
Abstract
Objectives
The objective was to perform a survey-based service evaluation of our telephone PrEP clinic (Tele-PrEP), which was instituted during the COVID-19 pandemic, to inform future service delivery.
Methods
We administered parallel, web-based, anonymous surveys to PrEP-users who had a Tele-PrEP appointment between 13.11.2020 and 17.12.2020 and all healthcare professionals (HCPs) conducting Tele-PrEP clinics. We used descriptive statistics to summarise demographic and qualitative data, and thematically categorised free text responses using the Framework for a Systems Approach to Healthcare Delivery.
Results
62/117 (53%) PrEP-users and 8/9 (89%) HCPs completed the surveys. Tele-PrEP was rated ‘excellent’ or ‘good’ by 61/62 (98%) PrEP-users. All HCPs felt that Tele-PrEP allowed them to assess patients safely and confidently. 10/62 (16%) PrEP-users and 1 (11%) HCP expressed a preference for face-to-face care. Using the Framework for a Systems Approach to Healthcare Delivery we identified key areas important to respondents who highlighted the rapid changes as a result of COVID-19, which required an increase in dedicated resources. HCPs valued teamwork, support/supervision and convenience in achieving quality care for the patient, who in turn, valued convenient, holistic and individualised management to meet their sexual healthcare needs.
Conclusion
Tele-PrEP is feasible and acceptable. While most respondents rated the service highly, others identified a need/preference for face-to-face appointments.
Keywords
Introduction
Scotland implemented a national HIV pre-exposure prophylaxis (PrEP) programme in mid-2017. PrEP (oral tenofovir/emtricitabine) and associated monitoring is provided free of charge to people who satisfy risk-based eligibility criteria. 1 3354 individuals received at least one prescription for PrEP in the first 2 years and reduction in HIV transmission at population-level has been demonstrated in men who have sex with men.2,3
Our large urban sexual healthcare service provides PrEP care for around 1300 people, almost half of all those on PrEP at any one time in Scotland. 2 Prior to the COVID-19 pandemic, around 230 patients/month accessed PrEP though 30-min face-to-face appointments.
A national COVID-19 ‘Stay at Home’ order was imposed in the UK on 23/03/2020, with advice to limit non-urgent medical services. 4 While much routine sexual healthcare activity ceased, we continued to provide PrEP in line with national guidance. 5 To reduce face-to-face care, we implemented a telephone-based clinic (‘Tele-PrEP’) which involved a 20-min telephone consultation with a doctor or nurse specialist, followed by a short clinic attendance to collect the medication and for necessary tests (screening for sexually transmitted infection and blood borne viruses +/− renal function). A new online booking system for Tele-PrEP appointments was also introduced on 07/07/2020. People who contacted our service for ongoing PrEP care and those whose behaviours put them at high risk of HIV acquisition were appointed to the Tele-PrEP clinic. A small number of face-to-face appointments remained for patients who were medically or socially complex; during the study period, this represented only 4% of PrEP appointments. All patients seen face-to-face for PrEP had either limited English language, complex renal conditions, mental health conditions or had previously been identified as being in abusive/coercive relationships which meant telephone consultations were unsuitable.
Aims and objectives
To perform a survey-based service evaluation to determine whether Tele-PrEP meets the needs of PrEP-users and sexual healthcare professionals (HCPs) in order to inform future provision of PrEP services.
Methods
The survey period was a stable 5-week period, 13/11/2020-17/12/2020, in which there were no changes in Governmental restrictions or clinic provision.
Survey development
We developed web-based surveys combining modified Likert scale questions and free text responses, based on an existing questionnaire that had used validated questions wherever feasible. 6 We piloted them in paper form with three HCPs before refining them to ensure optimum readability and succinctness, leaving 16 and 13 questions for the PrEP-user and HCP surveys, respectively. The PrEP-user survey asked for basic demographic and sexual behaviour data, but no identifiable information to ensure that we could not link the survey to the individual. The HCP survey asked for limited demographic data to avoid deductive disclosure. We converted them into an online format using our Health Board approved online survey platform Webropol™.
Survey administration
During their Tele-PrEP appointment, HCPs offered the survey to patients who met our inclusion criteria (age over 18 years, able to understand and speak English, able to access an internet-enabled device, provide informed consent to participate and used the service for the purposes of accessing PrEP). We texted patients who agreed to participate using a link to the survey and sent one reminder message 7–14 days later.
We emailed all HCPs involved in Tele-PrEP delivery a weblink to the survey which was available for a 6-week period with 2 reminder emails.
Data analysis
We analysed quantitative data on MS Excel using descriptive statistics and thematically categorised qualitative data from the free text comments using the Framework for a Systems Approach to Healthcare Delivery. 7 This framework divides a healthcare system into four levels (individual patient, care team, organisation and political/economic environment) to describe its structure and to explore the interdependencies and dynamics within the system. 7 The free text comments were coded by authors LH and JQ, according to the aspect of healthcare delivery to which they related. Any disagreements were discussed with a third author and the themes agreed between all co-authors.
Ethical approval was not required as this was a service evaluation; the project was approved by the local Clinical Governance Board in September 2020.
Results
PrEP-user survey
During the study period 237 Tele-PrEP consultations took place; 23 patients did not meet the inclusion criteria, 97 were not offered the survey (the HCP omitted to offer it or it had been offered previously) and 5 declined. Of 112 patients who agreed to participate, 64 accessed the survey and two were excluded as ineligible (overall completion rate 62/117, 53%).
PrEP-user characteristics
The demographics of respondents were broadly representative of our whole PrEP-cohort (data not shown), all were aged 18 to 59 years (54% were 40 to 59 years), 60/62 (96%) identified as male, 54/62 (87%) reported having sex with men only, 51/62 (82%) were of White British ethnicity and 57/62 (92%) spoke English as their main language.
Patient experiences of Tele-PrEP
61/62 (98%) PrEP-users rated their overall care in the Tele-PrEP clinic as ‘excellent’ or ‘good’, and 49/62 (80%) would be happy to be assessed/managed by phone again. 10/62 (16%) would prefer face-to-face care. 51/62 (82%) would ‘definitely’ recommend the Tele-PrEP service to friends, 8/62 (13%) ‘probably’, 2/62 (3%) said they would not recommend it and one (2%) was unsure.
Healthcare professional characteristics
8/9 (89%) HCPs completed the survey; five were senior nurses and three were doctors (1 senior grade and 2 junior/training grade).
Healthcare professional experiences of Tele-PrEP
All HCPs felt that telephone appointments allowed them to safely assess patients for both PrEP initiation and continuation. 5/8 HCPs answered ‘yes, definitely’ when asked if they had been provided with enough support to undertake Tele-PrEP appointments, 2/8 ‘yes, mostly’ and 1/8 ‘no’. When asked how confident they felt providing PrEP over the phone, 2/8 HCPs and 6/8 felt ‘very confident’ and ‘somewhat confident’, respectively.
Qualitative analysis
A number of distinct themes emerged in the respondents’ free text comments regarding their experience and opinions of Tele-PrEP (Figure 1). Thematic categorisation of free text responses regarding Tele-PrEP using the Framework for a Systems Approach to Healthcare Delivery.
7
Themes from PrEP-user respondents are in italic, those from HCP respondents are in standard font and themes common to both groups are highlighted in bold.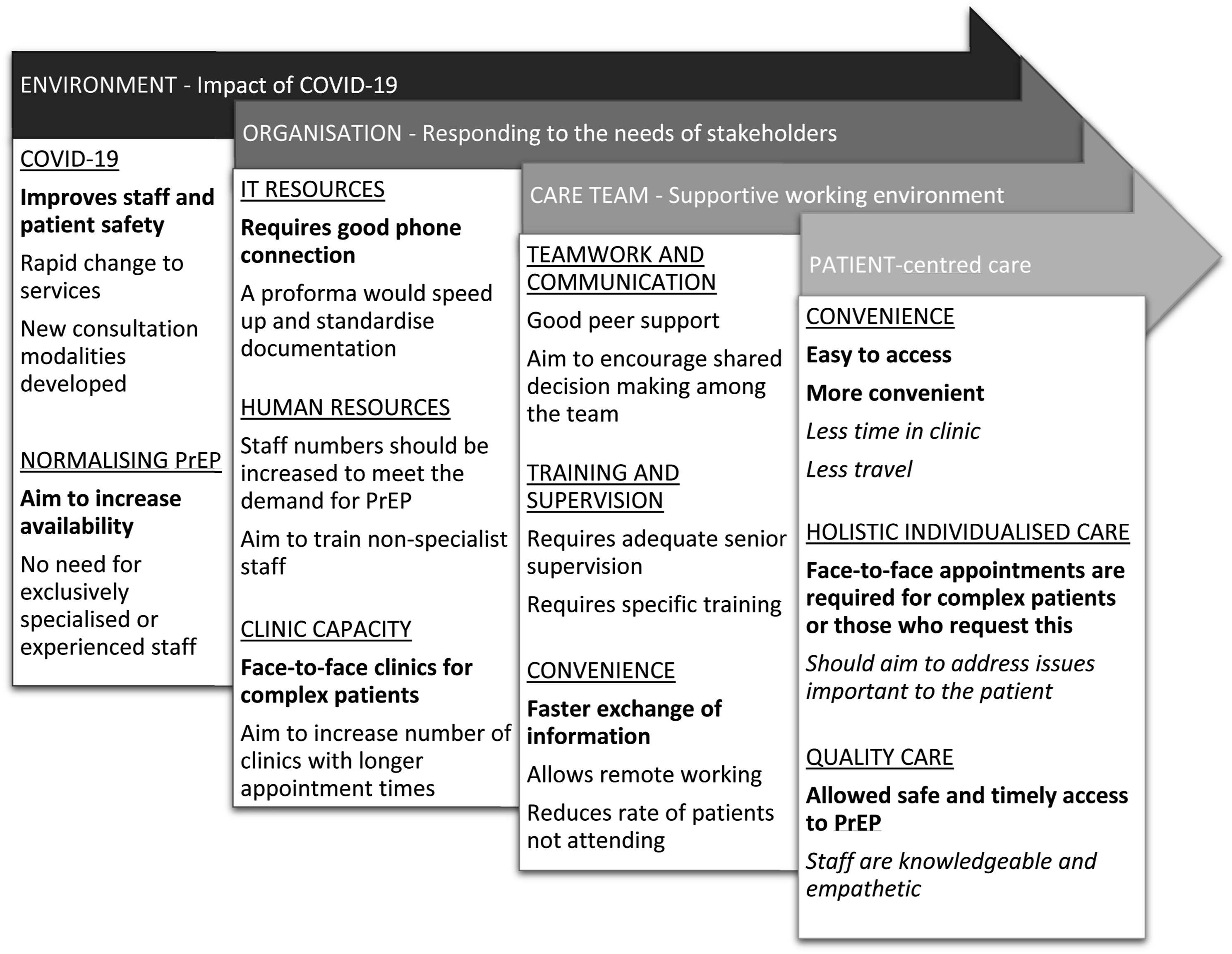
Patient and HCP responses highlighted the need for rapid change in the PrEP service to minimise COVID-19 transmission while still maintaining access to PrEP. HCPs stated that this needed an increase in resources such as adaptations to information technology systems, increased staffing/staff training and the ability to maintain adequate clinic capacity for both telephone and face-to-face appointments. HCPs strongly felt that Tele-PrEP could provide effective care for the majority of patients, however face-to-face capacity must be retained for more medically or socially complex patients.
Overall, HCPs valued teamwork, support/supervision and convenience in achieving high quality care for the patient; while patients valued convenient, holistic and individualised care to meet their sexual health needs.
Discussion
Tele-PrEP was highly acceptable to PrEP-users and HCPs and enabled ongoing provision of PrEP to those at high risk of HIV acquisition in the context of a global pandemic. The main identified benefits of the telephone service related to the improved convenience and accessibility of PrEP. However, a small but important proportion of PrEP-users and HCPs strongly preferred face-to-face care, especially when the patient may have more diverse or complex sexual health needs beyond routine PrEP provision.
Although there is limited research in this area, our findings align with other surveys of patient and/or HCP acceptability of telephone consultations within various fields of medicine.8–10 In particular, Riba et al. (2021) performed a similar but smaller online survey of patients accessing PrEP via telephone or online assessment in Colorado, USA. 10 Over 90% (21/23) of respondents agreed that telephone/online PrEP appointments were easy to schedule and complete. 10 Over 90% of their respondents also preferred this method compared to traditional face-to-face appointments. 10
The COVID-19 pandemic resulted in a rapid shift to telephone consultations without the sequential evaluative process which would usually characterise such a dramatic change in practice. This service evaluation provides some of the first insights into the acceptability of Tele-PrEP which will be of interest nationally and internationally as sexual health services endeavour to continue high quality PrEP care during and beyond the COVID-19 pandemic; and locally to ensure we meet the needs of our PrEP-users. We took a robust approach using the validated Framework for a Systems Approach to Healthcare Delivery to identify key areas which are important to patients and HCPs and describe their interconnectivity such that the organisation can respond by providing the necessary resources and infrastructure to the care team in order to maintain high quality patient-centred care. 7
However, there are limitations to our evaluation. Although our response rate was acceptable, overall numbers of participants are small and from a single country. The generalisability of the findings therefore may be limited in settings without similar patient populations or healthcare delivery systems. There is also likely to be selection bias because we could only survey PrEP-users who had already navigated the new online appointment system, those who had use of an internet-enabled device and those who spoke English. This therefore excludes patients who are likely to be some of the most vulnerable and underserved and most likely to experience health inequalities.
Conclusion
This service evaluation, conducted during a period of very limited social mixing, suggests that a predominately telephone-based model of PrEP provision is highly acceptable to both patients and HCPs. However there remains a need for face-to-face appointments for patients who request this and for those with more complex needs. Looking to the future this could mean that Tele-PrEP becomes the main model of PrEP care. However, uncertainties remain, including the views of patients with low health literacy, the acceptability of remote care as COVID-19 restrictions ease, and whether this care model provides value for money.
Supplemental Material
sj-pdf-1-std-10.1177_09564624211068766 – Supplemental Material for Maintaining access to HIV pre-exposure prophylaxis in a pandemic: A service evaluation of telephone-based pre-exposure prophylaxis provision
Supplemental Material, sj-pdf-1-std-10.1177_09564624211068766 for Maintaining access to HIV pre-exposure prophylaxis in a pandemic: A service evaluation of telephone-based pre-exposure prophylaxis provision by Lindsay Henderson, Jo Gibbs, Jacqueline Quinn, Sharmini Ramasami and Claudia Estcourt in International Journal of STD & AIDS
Footnotes
Acknowledgements
We would like to thank all the patients and staff who took the time to complete the surveys.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.