
Abstract
Background
In Mexico, the number of people living with HIV (PLWH) receiving antiretroviral therapy (ART) has increased in the last 20 years. The elimination of a CD4 threshold to initiate publicly funded ART was a major policy implemented in 2014. The study objective was to assess the determinants of Virologic Failure (VF) in Mexican PLWH on first-line ART between 2008 and 2017 and to evaluate the effects of changes following the 2014 policy.
Methods
A 10-year patient-level data analysis was conducted using the Mexican SALVAR database. The main outcome was the proportion of PLWH with VF. A multivariable logistic regression was conducted to identify the association between covariates and VF before and after the 2014 policy implementation.
Results
We found a lower proportion of people with VF in 2014–2017 compared with 2008–2013 (50% vs 33%, p<0.001). The multivariable analysis showed a reduction in the odds of virologic failure after 2014 (Odds ratio: 0.50 [95% CI: 0.48–0.51]). Place of treatment and level of deprivation were significant predictors of VF in during 2014–2017, but not before.
Conclusion
This study indicates that, by lowering threshold levels of CD4 required for treatment initiation in Mexico, a higher number of PLWH initiated treatment during 2014–2017, compared to 2008–2013 and the odds of VF were reduced.
Keywords
Introduction
The primary goal of antiretroviral therapy (ART) is to achieve and maintain virologic suppression in people living with HIV (PLWH) and to reduce disease progression and eliminate transmission through the achieving and maintaining viral suppression.1,2 It has been shown that early diagnosis and full timely access to ART reduce the probability of disease progression and improve health outcomes among PLWH.1–5 In addition to timely diagnosis and treatment, adequate monitoring and timely identification and management of treatment failure are key to reducing the clinical impact of HIV.6,7
In Mexico, the number of PLWH receiving ART has increased in the last 20 years due to different public policies focused on expanding access to ART. Starting in 2007, Mexico launched a major initiative to provide universal access to ART conditional on several clinical criteria including CD4 counts ≤200 cells/mm3 and the presence of risk symptoms. 8 Following the World Health Organization (WHO) recommendations for early treatment initiation of PLWH in June 2013, 9 a major policy changed occurred when the Mexican HIV-clinical guidelines were modified in 2014 to expand universal access to ART to all PLWH irrespective of their baseline CD4 count and symptoms10,11 The performance of the program is monitored quarterly by the government, and has shown that, on average 80% of the PLWH in Mexico show viral load (VL) counts below 50 copies/ml (virologic success) during their routine checkups12,13 Clinical and observational studies have shown that maintaining VL under that threshold is a predictor of long-term health outcomes 14 Although VL is an important measure of disease progression, likelihood of transmission, and mortality, 15 as a policy measure, it is also important to document virologic failure (VF) following first line ART treatment initiation (independently of the treatment option) at the population level. This is because VF is the result of multiple and complex factors that go beyond treatment efficacy such as poor adherence, inadequate care or access to healthcare, and other sociodemographic factors and contextual variables.16–18
While an early study conducted in a third-level hospital in Mexico City in 2010 found that the probability of VF was 20% at 48 months after ART initiation and was higher among youth (individuals younger than 30 years old), 14 this study was published before the 2014 changes in clinical guidelines. In addition, the determinants of VF have not been explored in Mexico and the 2014 policy changes have not been evaluated. Providing information about the proportion of PLWH with VF in Mexico, as well as the influence of changes in clinical approach for treatment initiation following the 2014 Mexican policy change will generate evidence for further HIV-policy design and implementation in Mexico and elsewhere. Therefore, the objective of this study was to document the change in rates of VF and compare the determinants of VF in Mexico before and after the updated 2014 clinical guidelines.
Methods
Study design
We performed a retrospective population-based cohort study to assess virologic failure after receiving first line treatment in PLWH in Mexico. Data were accessed using the Mexican Administrative Health Data from the Antiretroviral Administration Logistics, and Surveillance System (SALVAR in Spanish).
Data source
SALVAR is an electronic system managed by CENSIDA (National Center for the Prevention and Care of HIV/AIDS in Spanish) and funded by the Mexican Ministry of Health. It contains clinical, biometric, antiretroviral therapy and demographic information of individuals enrolled in the national HIV/AIDS program. All patients provide consent for the use of personal information. 15 Data presented in this analysis was provided to the authors as a secondary anonymized dataset. Data in SALVAR began to be captured in 2006; however, it was not until 2008 that the system was fully implemented nationwide. Currently, it contains information on more than 140,000 PLWH on ART. 16
Study population
For this analysis, we included adults (18 years old and older) living with HIV who received their first ART after January 1st, 2008 and before September 1st, 2017. Given the purpose of the analysis, we only considered patients that had completed at least 12 weeks of follow-up,9,19 and at least three VL measures. Pregnant women, children, people who are incarcerated, and people receiving antiretroviral prophylaxis were excluded from the analyses. Individuals with incomplete information on gender, and age were also excluded.
Study outcomes
The primary outcome was the proportion of people with Virologic Failure following first line ART treatment initiation. As per the Mexican clinical guidelines definition, 17 VF was determined by one of the following two criteria: 1) individuals without a reduction of at least one log10 of VL count at week eight compared to baseline information; and 2) individuals who had reduced at least one log10 within the first 8 weeks, but after 6 months of ART initiation presented two continuous VL measures above 200 copies/ml at any further week. However, considering WHO recommendation and in order to include more individuals in our study, we considered at least 12 weeks of follow-up instead of eight.
First line treatment was defined as the first ART components prescribed to the patient based on the information reported in SALVAR. The database also provides the specific ART assigned at treatment initiation a well as switches in ART treatments. Patients changing their first line ART from a 3-pill regimen to fewer pills (i.e., a 2 or 1-pill scheme), but maintaining the same components (i.e., efavirenz/emtricitabine/tenofovir disoproxil fumarate [EFV/FTC/TDF)] and EFV+FTC+TDF) were not considered switching lines of ART treatment.
Independent variables
All variables such as gender (i.e., male, female, and trans), age (as a continuous and categorical variable), year of ART initiation, geographic information of facility (region and type of health facility), baseline virologic measures, and type of treatment were collected at the time of treatment initiation. Region was grouped following previous analysis on Mexican HIV population 20 as Central East, Central West, Northwest, Northeast, and South. For our analysis, Mexico City was stratified as another region (instead of being part of Central East) based on the number of people living and receiving treatment there. Health facilities were categorized by type as Specialized Clinic CONDESA (based on Mexico City), Tertiary level Hospitals or National Institutes of Health, and the Ambulatory Centers for Prevention and Attention for HIV/AIDS and Sexually Transmitted Infections (CAPASITS in Spanish). The marginalization index (high, medium, and low) estimated by the Mexican government for each Mexican municipality/location 21 was assigned to the location of each health facility where PLWH were treated to reflect social and economic differences among health facilities. 1
In terms of biologic measures, CD4 cell count at first line ART treatment initiation was divided into two groups by CD4 count lower than 200 cells/mm3 and higher or equal to 200 cells/mm3, based on prior evidence of an association of CD4 count with VF. 22 Baseline VL was classified as lower or equal than 100,000 copies/mL and higher than 100,000 copies/mL and was used as an adjustment for ART allocation based on clinical guidelines to reduce bias due to treatment selection. 23 We also grouped ART as the three most used and representative first line ART available in Mexico during the studied timeframe, reported in SALVAR database for the analysis: efavirenz/emtricitabine/tenofovir disoproxil fumarate (EFV/FTC/TDF), efavirenz + abacavir/lamivudine (EFV+ABC/3TC), boosted Protease Inhibitors + backbone (boosted PI), and other (including integrase inhibitors and all other regimens defined as a first line ART in SALVAR). Although today integrase inhibitors are an important treatment option for PLWH, their use represented less than 2% of total first line ART from 2008 to 2017 in the SALVAR database, and less than 1% before 2014. Therefore, they were included in the “other” category to avoid any estimation bias.
Statistical analysis
Population baseline characteristics were presented for the overall study period and separately for the periods between 2008–2013 (i.e., before policy change) and 2014–2017 (i.e., after policy change). Discrete variables were presented as percentages, while continuous variables were described in terms of mean, standard deviation (SD), median, and Inter-quartile range (IQR). Chi-Squared test for categorical variables and two-sample Welch tests for continuous variables, were used to compare the population characteristics and outcomes between the two time periods (e.g., before and after the change in policy). VF, our primary outcome, was also presented for the overall study period, by time period and by category of 1st line ART.
To identify the factors associated to VF, a multivariable logistic regression was conducted adjusting by previously mentioned variables in addition to a dichotomous variable indicating the period of policy change in 2014. Furthermore, two models were performed stratifying by time periods (2008–2013 and 2014–2017) allowing a deeper understanding of the association between covariates and the main outcomes before and after the introduction of the 2014 policy. Results are presented as Odds Ratios (OR) with a 95% confidence interval (CI). Goodness-of-fit of the logistic models was estimated using the c-statistic.
Results
Study population
SALVAR dataset contains information about first line ART of 134,860 individuals during January 2008 and September 2017. Of those, 7005 were younger than 18 years old, pregnant women or deprived of their liberty. 29,612 did not have information about VL or CD4 at treatment initiation, and 18,488 did not have at least three VL measures or established time of follow-up. The final sample shown in Figure 1 consisted of 79,755 individuals. Sample Flow for Analysis.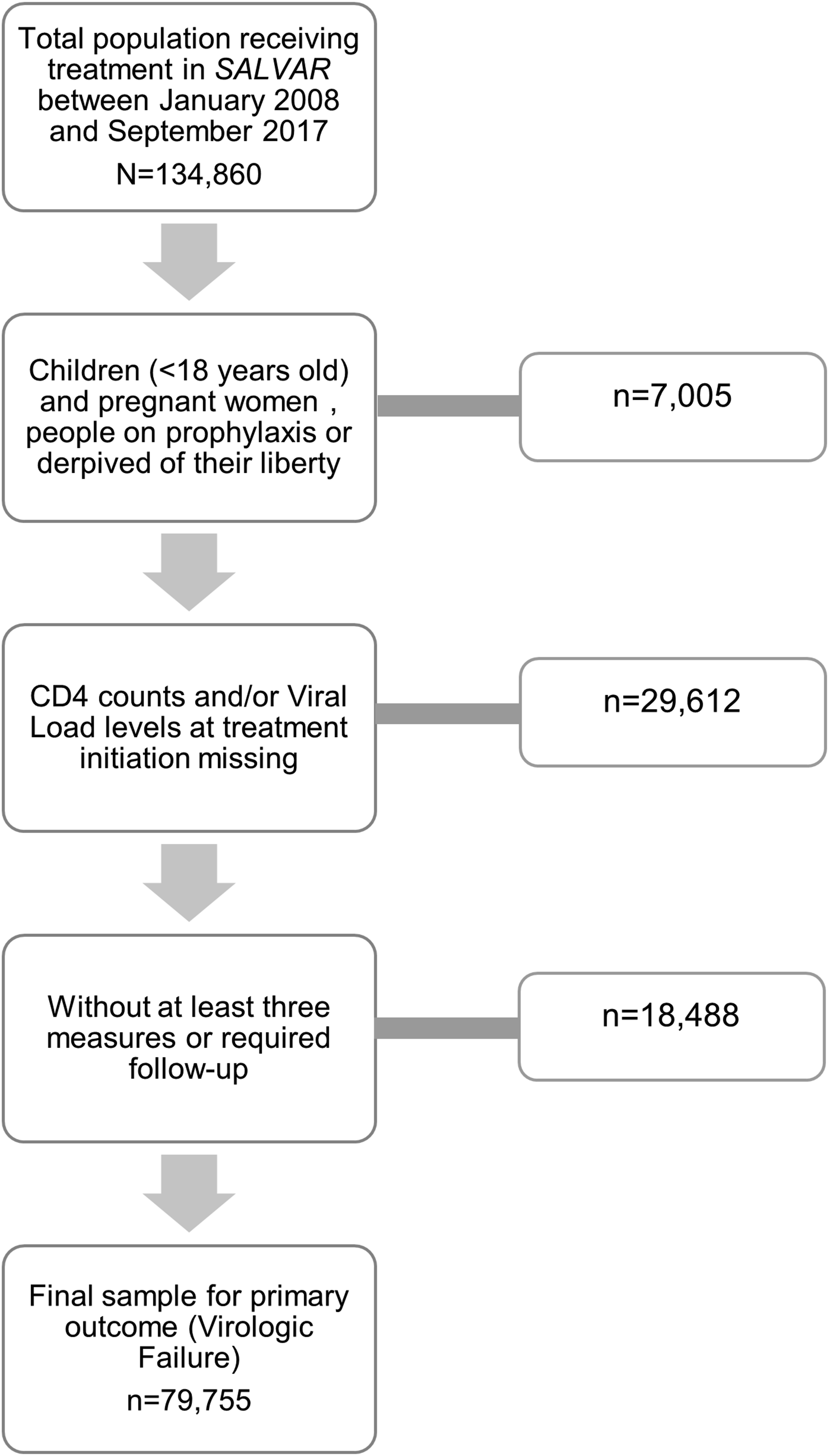
Summary Statistics and Patients’ Characteristics at treatment initiation, January 2008–September 2017.
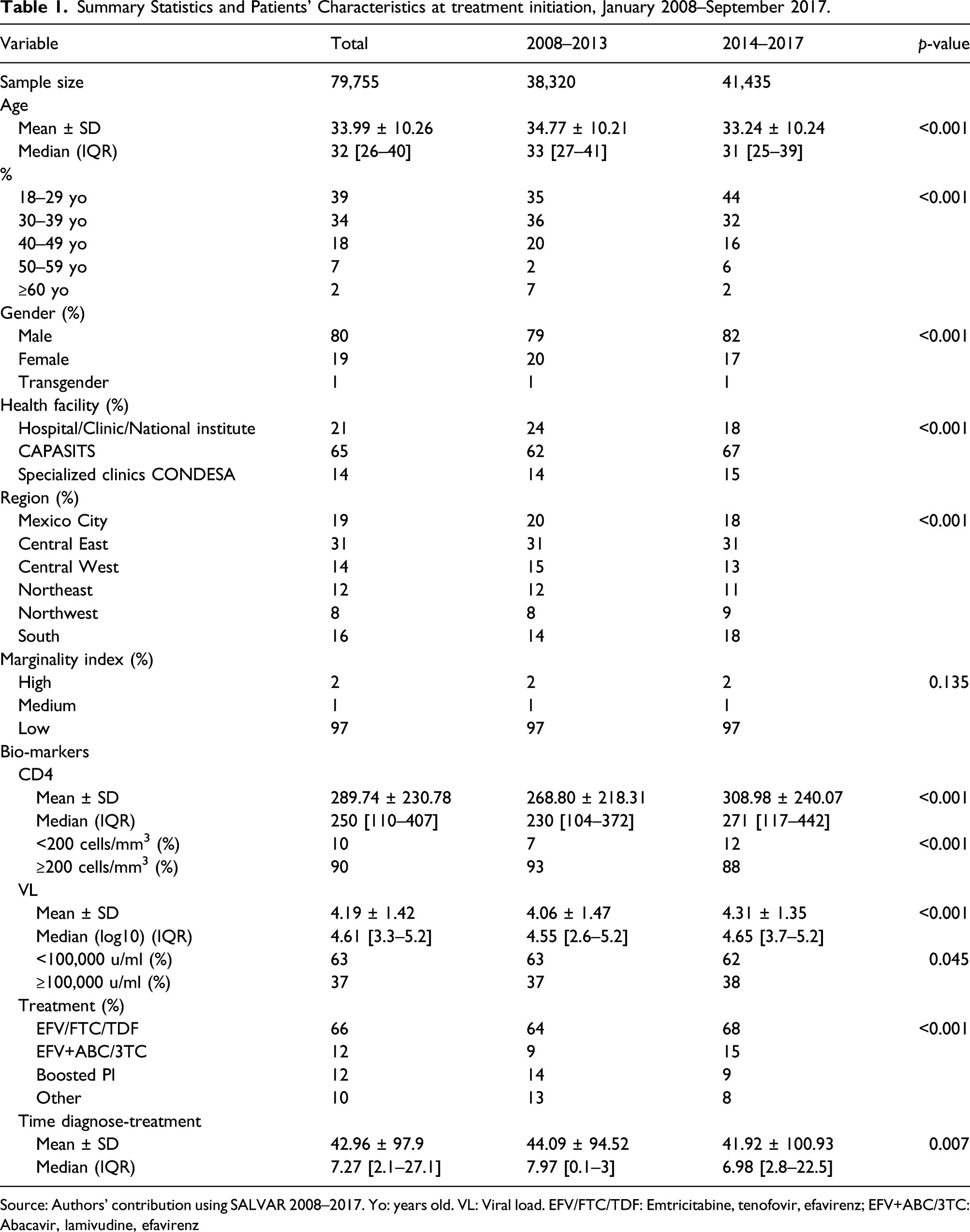
Source: Authors’ contribution using SALVAR 2008–2017. Yo: years old. VL: Viral load. EFV/FTC/TDF: Emtricitabine, tenofovir, efavirenz; EFV+ABC/3TC: Abacavir, lamivudine, efavirenz
Virologic failure
Virologic failure (%) of adults in 1st line ART. 2008–2017.
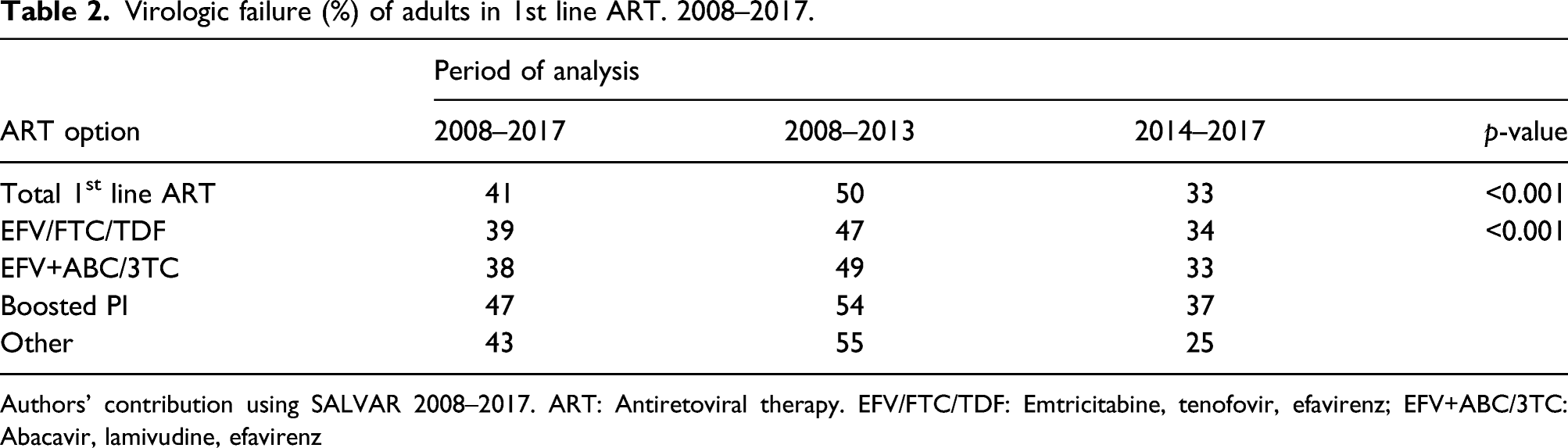
Authors’ contribution using SALVAR 2008–2017. ART: Antiretoviral therapy. EFV/FTC/TDF: Emtricitabine, tenofovir, efavirenz; EFV+ABC/3TC: Abacavir, lamivudine, efavirenz
Determinants of VF
Multivariate logistic regression for virologic failure, 2008–2017.
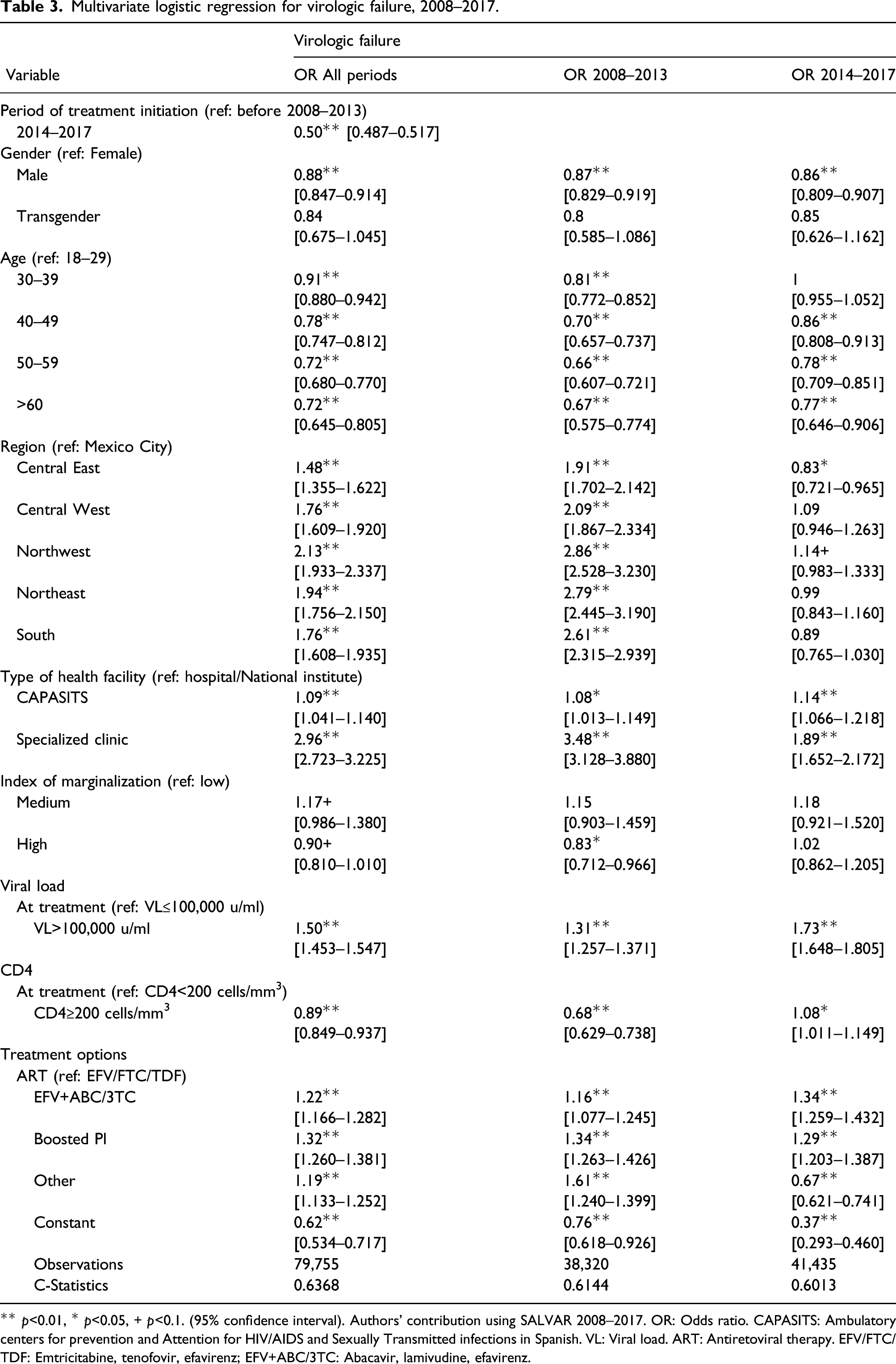
** p<0.01, * p<0.05, + p<0.1. (95% confidence interval). Authors’ contribution using SALVAR 2008–2017. OR: Odds ratio. CAPASITS: Ambulatory centers for prevention and Attention for HIV/AIDS and Sexually Transmitted infections in Spanish. VL: Viral load. ART: Antiretoviral therapy. EFV/FTC/TDF: Emtricitabine, tenofovir, efavirenz; EFV+ABC/3TC: Abacavir, lamivudine, efavirenz.
Discussion
Based on 10 years of national data of PLWH in Mexico, this study has provided new information on the determinants of virologic failure and treatment success between 2008 and 2017 and clinical guideline changes for treatment initiation since 2014 eliminating the CD4 threshold previously established (CD4 ≤ 200 cells/mm3). Compared to the 2007–2013 period, individuals treated during 2014–2017 were younger, a higher proportion was male, more were initially treated in CAPASITS, a higher proportion were in the South of Mexico, and (as expected) with baseline CD4 was higher, compared to the period 2008–2013. The proportion of individuals with VF decreased from 50% in 2008–2013 to 33% in 2014–2017, suggesting that more adults were responding better to treatment. The multivariate analysis indicates that actions in 2014, eliminating the CD4 threshold for treatment initiation, reduced the odds of VF by 50%, after controlling for other variables. When analyzing VF by period, it was shown that being initially treated in another region than Mexico City or in a medium or highly deprived area was not a significant predictor of VF during 2014–2017. These could be explained by the national distribution of health facilities in the whole country which almost doubled from 2007 to 2013 24,25 and changes into a more integrated and centralized approach to HIV treatment and care in Mexico, 10 including testing for all high and not high-risk population was expanded, the CD4, lowering the threshold for treatment initiation, and starting massive prevention campaigns as the result of the 2013 implementation of the National HIV plan.10,26
It is difficult to compare our analysis with other studies conducted in Mexico given that this is the first study analyzing VF in these settings for all PLWH receiving care through the MoH. However, there is a governmental publication reporting that of all people enrolled in SALVAR living in Mexico City or the State of Mexico, 46.8% have acquired-resistance to efavirenz. 27 Our results showing a higher likelihood of VF among female are consistent with the results showed by Mata-Marín et al. 28 in a hospital in Mexico, who explained the findings because of a lower educational level and a higher probability of being unemployed for women as well as lower resources and social insurance to access ART compared to men. Regarding our findings for age, similar results were found in Latin American and Caribbean countries including Mexico,29–31 where the older population had a lower risk of VF, possibly explained by higher adherence, lower risk behaviors, and general awareness of better health care. Also, consistent with international literature, studies in Latin America and Africa, show that to initiate treatment with CD4 ≥200 cells/mm3 reduces the odds of VF. These effects could be explained because CD4 count at treatment initiation is a biological predictor of a better immunological function and slower disease progression.32–35 However, our stratified analysis indicated that CD4 levels increase the odds of VF after 2013, but the association is marginal (OR of 1.08; 95% CI of 1.01–1.15). Although the association of CD4 levels and VF after 2014 is counterintuitive, it could be explained by a few reasons. First, as identified as one of our study limitations, SALVAR data do not include information on treatment adherence, which may create some bias. Second, in addition to eliminating in 2014 the CD4 threshold to initiate ART treatment, a year before other measures were implemented including diagnosis and awareness campaigns, increasing access to HIV care by targeting low-risk individuals could partially explain this result as we were not able to control for these unmeasured confounders. For example, it has been shown that individuals with a lower perception of risk have a poorer adherence 36 which could be the case for those PLWH with higher CD4 count (fewer symptoms and warning signs for disease progression) 36,37 Besides the direct association of poor adherence and VF, intermittent ART adherence has also been associated with CD4 variability, which is also associated with VF. 37 In contrast, lower VL levels at treatment initiation are associated with better prognosis and successful viral responses 32 This could be explained because VL is a predictor for disease progress. Patients with higher levels at treatment initiation presented a more complex and advanced disease than patients with lower levels.38,39 When observing the stratified analysis for VF, our results are similar to a previous analysis concerning Mexican regions and different periods. 26 The effect of being treated in a region different than Mexico City losses significance after 2014. This could also be explained to changes in policies regarding diagnosis, where late testing is the main reason for a late and unsuccessful treatment, 40 as well as an expansion of the Mexican health system. 10 Compared to studies previously performed in Mexico around PLWH, our study gives information based on national-wide patient-data and evaluated changes in treatment initiation policies after modifications in international and national clinical guidelines.
Our study has some limitations. The analysis was constrained by the list of variables captured in SALVAR, which do not include possible confounders, such as employment situation, risk behaviors and access to HIV healthcare (e.g., some individuals in remote areas could never know their HIV status). Second, there was some missing information from 29,000 adults, which might not be random. However, we did not find any differences on gender, age or region between those with complete information and those without CD4 and VL measures. The data did not allow for capturing adherence to treatment, which could be a determinant of treatment success, and therefore VF.41,42 Some studies have shown that two of the main determinants of non-adherence are access to ART and financial constraints.43,44 However, the Mexican government started providing free treatment to all PLWH in 2003. 40 Besides, to our knowledge, no widespread or national programs to improve adherence were implemented during the time of analysis. Therefore, we assumed that adherence rates did not change significantly from one period to another. Finally, the first line ART used for the analysis are mainly based on a backbone + EFV, which does not reflect current treatment options and ART use in Mexico where integrase inhibitors are the preferred ART option in clinical guidelines. 45 However, this work presents the Mexican situation during 2008–2017 and evaluates the modification on national clinical guidelines after 2014. The findings of our study could also increase awareness, improvement of HIV-specific health care, and changes in treatment options by informing decision-makers about trends and outcomes of the current HIV program. Despite the limitations, our study has several strengths. We performed a national-wide analysis with a large sample of patient-data representing 64% of PLWH in Mexico and a long follow-up period. This is the first analysis studying determinants of virological failure in Mexico with this sample size and a 10 year study period.
Derived from our analysis, some hypotheses can be made. We identified key indicators and determinants of treatment success that could inform future policies and programs targeting PLWH in Mexico. Further research is required to evaluate the association between early treatment initiation, time from diagnosis to treatment, and virologic outcomes. Furthermore, this analysis highlights the need to record adherence in the SALVAR database for a deeper understanding of VF determinants.
Conclusion
This study indicates that, by removing threshold levels of CD4 required for treatment initiation in Mexico, combined with an expansion of ART access through provision of more clinics country-wide, a greater number of PLWH initiated treatment and fewer had virologic failure. Identifying sociodemographic determinants of VF could enhance policy development and facilitate the achievement of policy objectives, improving national indicators of the Mexican epidemic of HIV.
Footnotes
Acknowledgments
The authors acknowledge to the Center for Aids Prevention and Control in Mexico (CENSIDA) the authorization to use the information for the analysis performed. Analyzed data is from an anonymized database.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.