
Abstract
Background: An optimal adherence to antiretroviral therapy (ART) is fundamental for suppression of HIV viral load and favourable treatment outcomes. Patient-reported outcomes (PROs) are effective tools for improving patient–provider communication and focusing providers’ awareness on current health problems. The objectives of this analysis were (1) to determine the feasibility of implementing an electronic screening tool to measure PROs in a Canadian HIV clinic to obtain information on ART adherence and related factors and (2) to determine the factors related to sub-optimal adherence. Methods: This implementation research with a convenience sample of 600 people living with HIV (PLWH) was conducted in a busy, academic, urban HIV clinic in Toronto, Canada. PLWH were approached to participate in PRO assessments just prior to their in-clinic appointments, including health-related domains such as mental health, housing, nutrition, financial stress and medication adherence, and responses were summarized on a single sheet available for providers to review. Feasibility of implementing PROs was assessed by quantifying response rate, completion rate, time taken and participation rate. Medication adherence was elicited by self-report of the percentage of prescribed HIV medications taken in the last month. Unadjusted and adjusted odds ratios were estimated from logistic regression models to identify factors associated with adherence of <95%. Results: Of the 748 PLWH invited to participate, 692 (participation rate: 92.5%) completed the PRO assessments as standard of care in clinic. Of these, 600 consented to the use of their PRO results for research and were included in this analysis. The average response rate to the ART-related questions was 96.8% and mean completion rate was 95.5%. The median time taken to complete the assessment was 12.0 (IQR = 8.4–17.3) min, adjusted 8.7 (IQR = 7.2–10.8) min. 445 (74.9%) of participants were male, and 153 (26.2%) reported dissatisfaction with ART. 105 (19.7%) of the PLWH reported ART adherence of <95%. Multivariable logistic regression identified the following risk factors for sub-optimal adherence: dissatisfaction with ART (OR = 2.30, 95% CI 1.38–3.83), not having a family doctor or not visiting a family doctor in last year (OR = 1.69, 95% CI 1.02–2.79). Conclusion: Collecting self-reported health information from PLWH through PROs in a busy urban clinic was feasible and can provide relevant information to healthcare providers on issues related to adherence. This has a potential to help in individualizing ambulatory care.
Introduction
Antiretroviral therapy (ART) has revolutionized the course of HIV disease, reducing premature HIV-associated mortality, morbidity and the risk of onward transmission. While regimens have improved over time and many are now more forgiving of some variations in adherence, maintaining adherence to ART is still required in order to maintain long term clinical success.1–4 Optimizing treatment adherence leads to suppression of HIV viral load, reduces rates of hospitalization, decreases the risk of treatment failure and minimizes the need to switch to more expensive, complicated or poorly tolerated drug alternatives. 5 Several studies have identified behavioural, social and clinical factors that shape adherence patterns among people living with HIV (PLWH).6–9 It is highly beneficial to identify the presence of sub-optimal adherence to ART in real time, during routine HIV clinic visits, so that individualized strategies can be implemented, to improve ART adherence, and thus patient outcomes.
Within brief clinical encounters, it can be challenging for healthcare providers to routinely screen, identify and explore all factors that may contribute to inadequate HIV medication adherence. 10 Eliciting responses to a clinical assessment of patient-reported measures and outcomes (PROs) just before appointments could assist with this process. This can enable screening of patients at the point of care to help address barriers to ART adherence. 11 Patient-reported outcomes directly assess how the patient feels or functions in relation to their health condition or therapy and can identify health issues experienced by patients, and help providers make appropriate referrals and direct decision-making. 12
Introducing PRO assessment into clinical practise has been demonstrated to offer benefits for both providers and patients.12–15 Patient-reported outcome results in HIV settings were observed to focus outpatient consultations on current health problems, ameliorate patient-centred care and support resource optimization.16–20 Even though advances have been made in approaches to assessing PROs, little is known regarding the feasibility and impact of implementing assessment of PROs including ART adherence and related information in routine clinical care in the current treatment era. Therefore, the present study aimed (1) to determine the feasibility of implementing an electronic screening tool (tablet-based assessment) of PROs in a busy Canadian urban HIV clinic among PLWH to obtain information on ART adherence and related risk factors and (2) to determine the factors associated with sub-optimal ART adherence.
Methodology
Study design and study site
This was a cross-sectional research study conducted among a convenience sample of 600 PLWH visiting an academic ambulatory HIV clinic at St. Michael’s Hospital (SMH), Toronto. The feasibility of tablet-based screening of health-related domains using PRO assessment to obtain information on ART adherence in the outpatient clinic is described. Factors associated with sub-optimal adherence to HIV medications were determined through analysis of data obtained during implementation. This work is part of a wider implementation research study, the ‘PROgress Study’ (see https://progresshivcare.org/), that was designed to evaluate the process, impact and added value of PROs in two North American HIV clinics. The St. Michael’s Hospital (SMH) clinic serves an estimated 1800–2000 PLWH. The study was approved by the SMH Research Ethics Board, and written informed consent was obtained from all the participants.
PRO implementation
People living with HIV booked for routine care at the SMH HIV clinic first check in with the clinic clerical assistant and are escorted by the nurse to the examination room where vital signs and history are recorded on patient charts. They are then seen by other member(s) of the clinic team consisting of doctors, pharmacists, a dietician and a social worker, depending on their health status; the sequence of consultation varies to facilitate the clinic flow. After introduction of PROs as standard of care, PLWH were reviewed for their eligibility and English-speaking people, aged 18 years and older, were invited to participate. Those with psychiatric/cognitive impairment, those visiting the clinic for non-routine reasons (e.g. to receive an immunization only) and those visiting to see only a provider other than their primary HIV physician (e.g. social worker or dietitian) were excluded. People living with HIV who agreed to participate were then approached by the Research Coordinator (RC) who described the rationale for introducing PROs as a strategy for improving quality of care and offered them a tablet containing the PRO assessment. Participants could press a ‘help’ button on the tablet to alert the RC by text message in real time if they required assistance using the tablet or had any queries. After participants completed the assessment, a summary sheet was instantly generated, printed and attached to the respective patient chart by the RC. The clinic team members referred to the summary sheet to inform their discussions with the patients and to make appropriate referrals. Organizational infection control practices were followed by all staff and participants handling the tablets.
Health issues elicited by the assessment of PROs
The assessment contained PRO instruments relevant to HIV care. The assessment was developed by researchers from the University of Washington (UW) and ViiV Healthcare, using previously validated clinically relevant instruments and modified by the clinic team at SMH according to the local health needs of PLWH.17,19 The PRO platform (https://cprohealth.org) is open source software developed at the UW containing an automated decision support tool designed to make programmed decisions after the patient completes their PRO assessment and present the results in an actionable format. People living with HIV use touch-screen tablets over a wireless network. Network communications are encrypted and no patient data are stored on the tablets. The tool contained 41 core items, with a maximum of 120 items depending on skip patterns.
The PRO assessments included questions on various health-related domains including (a) demography (sex, gender), (b) adherence to ART, (c) ART satisfaction, (d) food insecurity (risk of malnutrition), (e) mental health (depression, suicidal ideation, intimate partner violence and anxiety), (f) financial stress, (g) behavioural risk (smoking, drug and alcohol risks) and (h) others (housing, having a family doctor and immigration status).
Information on adherence was elicited by a visual analogue scale item asking the percentage of HIV medication taken in the last month. Antiretroviral therapy satisfaction was assessed with items from the HIV/AIDS-Targeted Quality of Life instrument, with lack of satisfaction identified by an affirmative response to one of two items: Taking medicines in the last 4 weeks (a) ‘has been a burden’; (b) ‘makes it hard to live a normal life’. 21 Risk of malnutrition was determined by the Canadian Nutrition Screening Tool; persons reporting weight loss in the last 6 months along with eating less than usual for over a week were recognized as high risk. 22 Depression was defined as scoring >10 on the Patient Health Questionnaire, and suicidal ideation was defined as an affirmative response to the last question in that tool (‘Thought you were better off dead or hurting yourself in some way’). 23 Intimate partner violence was assessed by including questions about psychological, sexual and physical violence by a partner in the past year. If a participant reported suicidal ideation for more than 7 days in the last 2 weeks or physical/sexual intimate partner violence in the past year, both text message alerts and emails were automatically sent to the clinic team in real time to facilitate immediate intervention. The summary sheets included ‘red flags’ for suicidal ideation, partner violence or participants who self-reported weight loss in past 6 months.
The Multidimensional Sex/Gender Measure tool was used to ascertain sex and gender. 24 History of smoking was determined using the Center for AIDS Research Network of Integrated Clinical Systems Smoking questionnaire. 25 Alcohol use in the last year was measured using Alcohol Use Disorders Identification Test (AUDIT-C) with scores ≥5 for men and ≥4 for women. 26 Substance use was defined as any non-prescribed use of cocaine, methamphetamine, heroin, fentanyl, narcotics, sedatives, marijuana, stimulants, inhalants, hallucinogens or anabolic steroids (The modified Alcohol, Smoking and Substance Involvement Screening Test). 27 Questions were also included regarding anxiety status, housing type, citizenship, having a family doctor or visiting a family doctor in the last year, difficulty meeting housing costs and difficulty meeting medication costs. Age, race and viral load were not components of the PRO questionnaire; chart review was done for a subsample of 50% to obtain this information.
Data analysis
The analysis was done in three steps: Socio-demographic characteristics and health risks were summarized for the 600 enrolled participants using frequencies and percentages for categorical variables and mean (standard deviation) or median (interquartile range) for continuous variables. Feasibility of using tablet-based PRO assessment was evaluated by quantifying participation rate, response rate, completion rate and time taken. Participation rate was determined by the number of PLWH who agreed to answer the PRO assessment as a part of standard of care in the clinic, out of the total eligible that were invited to participate. Response rate was calculated as the average proportion of participants who responded (termed as respondents) to each individual item/question related to adherence and related factors in PRO assessments. Completion rate was determined by the average proportion of core questions (41 in number) that were answered by each patient.
Median time taken to complete the PROs by all the participants was assessed by the median of the difference between the time of the first and last questions answered by each participant, as tracked by the platform. Patients who answered at least 51 items of the PROs were included in the calculating median time and the rest were excluded. Time taken was adjusted for interruptions in the PRO sessions due to personal phone calls or visits by the clinic team including doctors, nurses and pharmacists for consultation, physical examination, etc., using 60 s suppression method with an assumption that if time taken to answer any item was more than 60 s, it was due to interruption in the session. 3. To determine the association of health risks and socio-demographic characteristics with sub-optimal adherence, unadjusted and adjusted odds ratios and 95% confidence intervals were estimated from logistic regression models. Participants who self-reported an adherence of <95% were defined as having sub-optimal adherence to ART.4,28–30 In the era of modern ART, 80–85% of ART adherence is associated with an undetectable HIV viral load.31,32 However, the cut-off of 95% selected for the study was due to the limitation of the methods and tools used in the study that had the potential of overestimation in reporting by the participants. Since the information on adherence was collected for the last 1 month, this long duration had the potential to overestimate reporting of adherence by participants. Additionally, participants might have felt pressured to overestimate adherence, as they were being questioned just prior to seeing their doctor. Only participants who answered the question related to adherence were included in this analysis (those not on ART do not receive those items).
Variables selected for the multivariable model satisfied the following criteria: clinically relevant according to the literature or expert team or yielding p values ≤0.15 in the unadjusted analyses.33,34 Because of missing data in the risk factors (non-response rates), multiple imputation was also performed using the fully conditional specification method. The number of imputations was 20. 35 Finally, to avoid overfitting, we limited the number of variables to less than m/10 with m = minimum number (adherent and non-adherent participants). 36 Multiple imputed results were compared to those from complete case analysis. The area under the curve (c-statistic) was calculated for all models. p values <0.05 were considered significant for multivariable models. All analyses were performed using Stata (version 12) statistical software, except multiple imputation that was conducted in SAS 9.4 (SAS Institute Inc., Cary NC USA).
Results
The data collection was initiated in August 2019 and completed in December 2019. During this period, 795 PLWH met the inclusion criteria; 47 (5.9%) were excluded (Figure 1). A total of 748 PLWH were asked to complete the PRO assessments as a standard of care procedure at the clinic, of whom 692 (92.5%) agreed. The primary reasons for non-completion were lack of interest (N = 22, 2.9%) and language issues (N = 12, 1.6%). When asked for consent to use the information in their PRO assessments for research, 92 PLWH refused, leaving 600 unique participants in this analysis. Flowchart depicting enrolment of PLWH and reasons for refusal in the HIV Clinic. Note: PLWH: people living with HIV.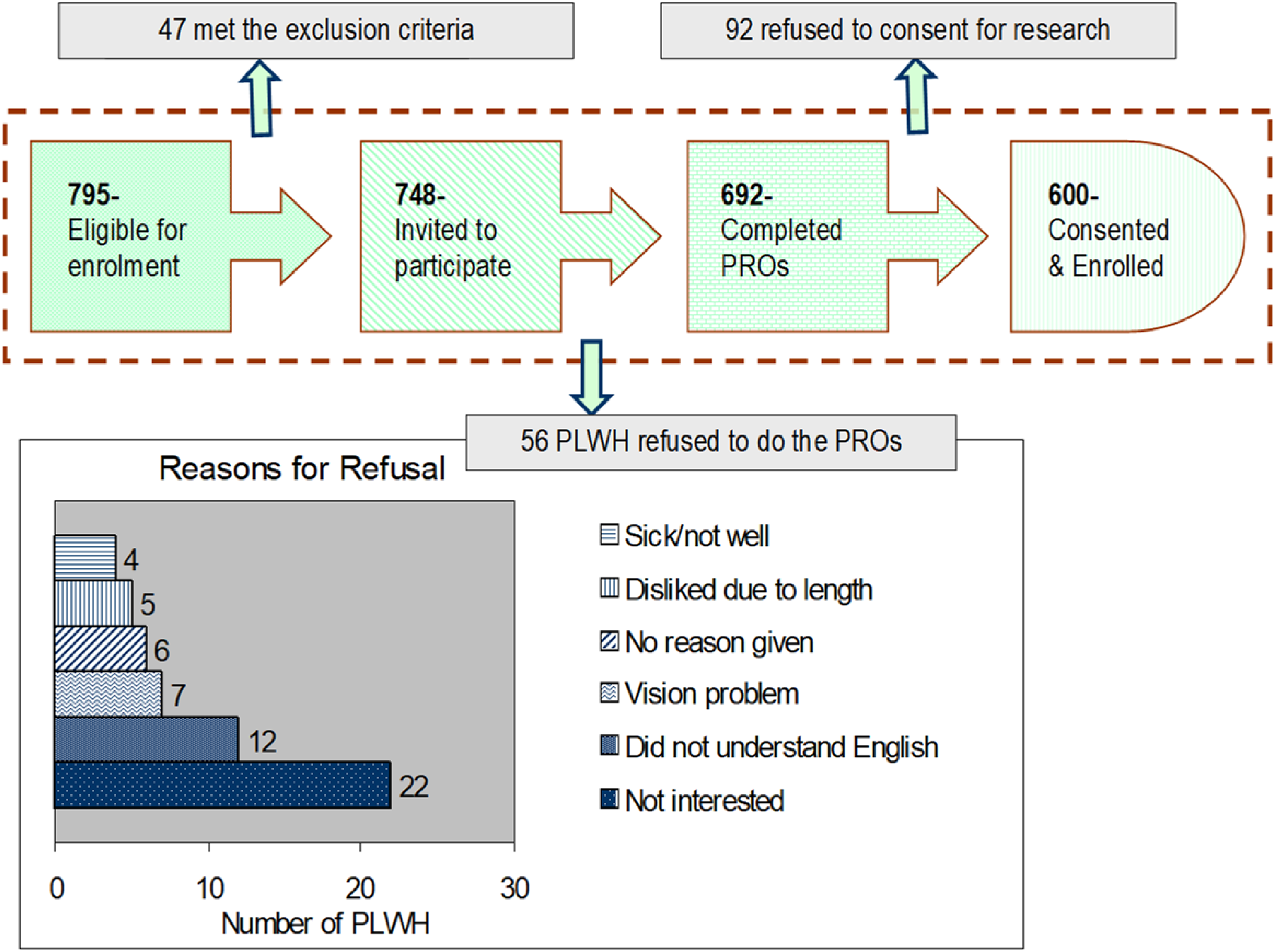
Socio-demographic characteristics of PLWH attending the HIV clinic obtained from PROs (N = 600).
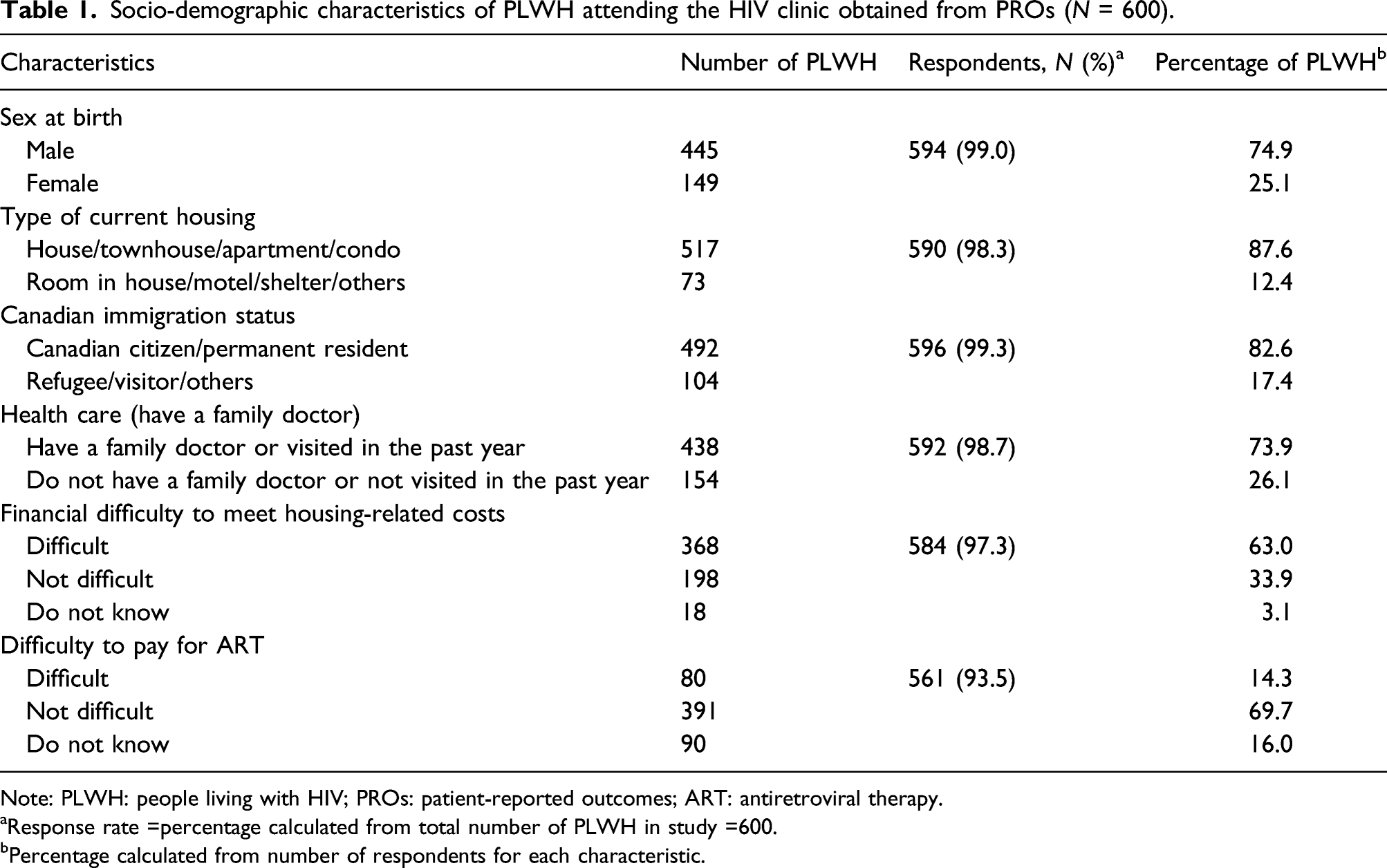
Note: PLWH: people living with HIV; PROs: patient-reported outcomes; ART: antiretroviral therapy.
aResponse rate =percentage calculated from total number of PLWH in study =600.
bPercentage calculated from number of respondents for each characteristic.
Health issues reported by PLWH attending the HIV clinic obtained from PROs (N = 600).
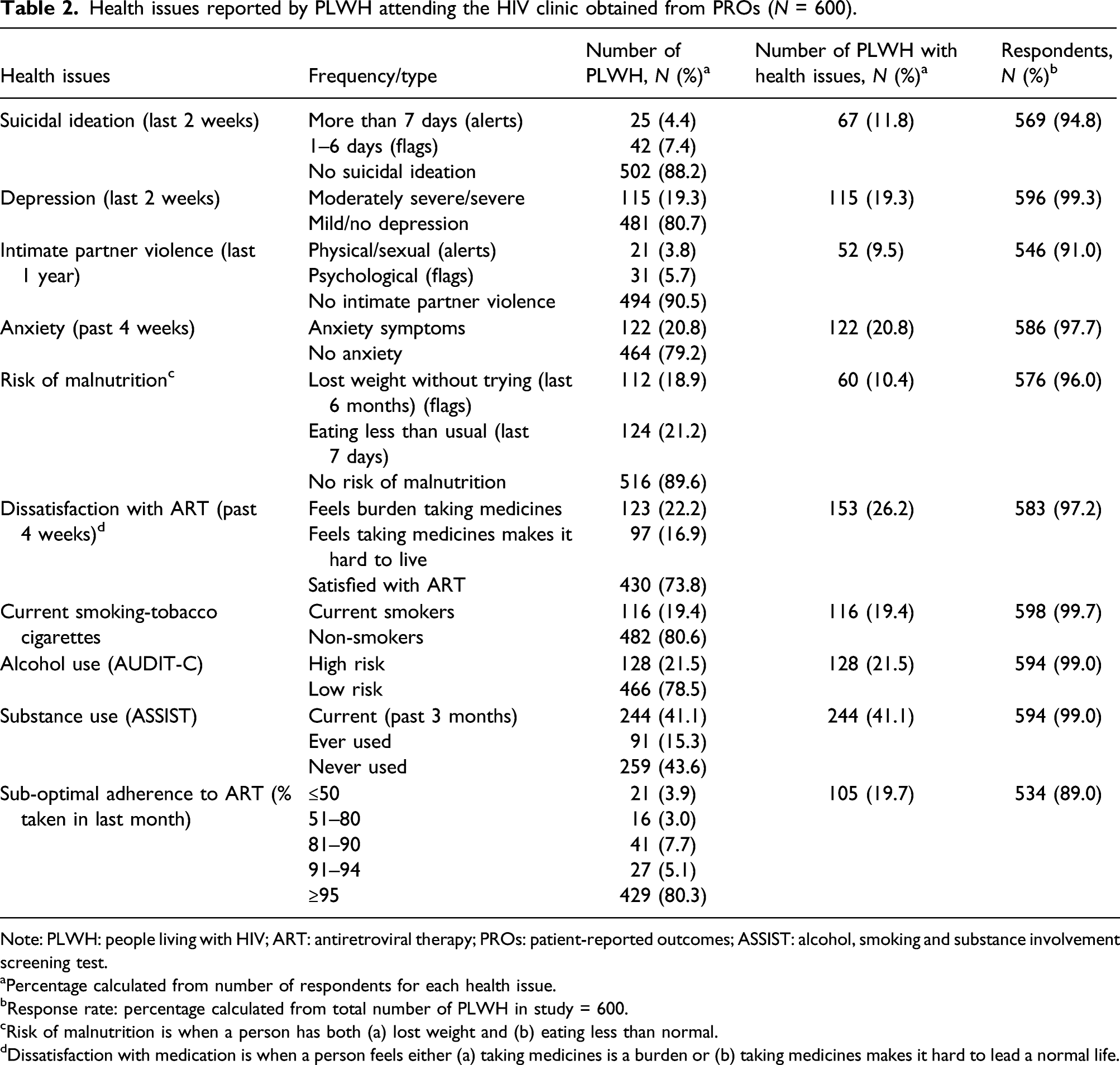
Note: PLWH: people living with HIV; ART: antiretroviral therapy; PROs: patient-reported outcomes; ASSIST: alcohol, smoking and substance involvement screening test.
aPercentage calculated from number of respondents for each health issue.
bResponse rate: percentage calculated from total number of PLWH in study = 600.
cRisk of malnutrition is when a person has both (a) lost weight and (b) eating less than normal.
dDissatisfaction with medication is when a person feels either (a) taking medicines is a burden or (b) taking medicines makes it hard to lead a normal life.
Results of the PRO assessments are presented in Table 2. Adherence to ART varied: while 429 (80.3%) participants had taken ≥95%, 21 (3.9%), 16 (3.0%), 41 (7.7%) and 27 (5.1%) PLWH had taken <50%, 51–80%, 81–90% and 91–94% of their ART, respectively, in the last month. Around one-fifth of the participants reported moderate to severe depression while one-fourth were dissatisfied with ART. Behavioural data showed that 116 (19.4%) smoked tobacco cigarettes currently, 128 (21.5%) were at high risk of alcohol use and 244 (41.1%) had a history of substance use in the last 3 months.
Unadjusted odds ratios and 95% confidence intervals associated with sub-optimal adherence to ART a among PLWH (N = 534).
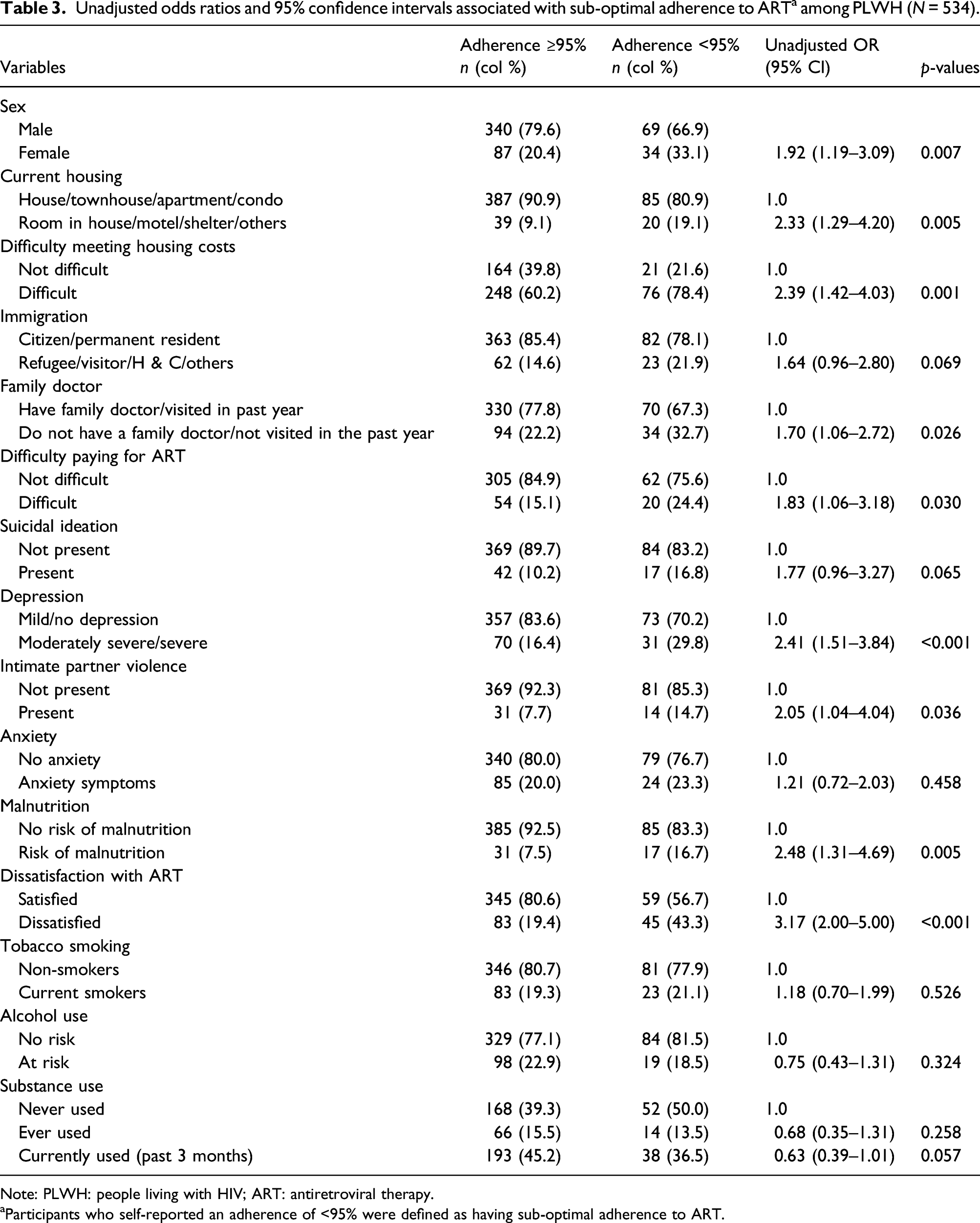
Note: PLWH: people living with HIV; ART: antiretroviral therapy.
aParticipants who self-reported an adherence of <95% were defined as having sub-optimal adherence to ART.
Adjusted odds ratios and 95% confidence intervals for the association of socio-demographic factors and health issues with sub-optimal adherence to ART among PLWH.
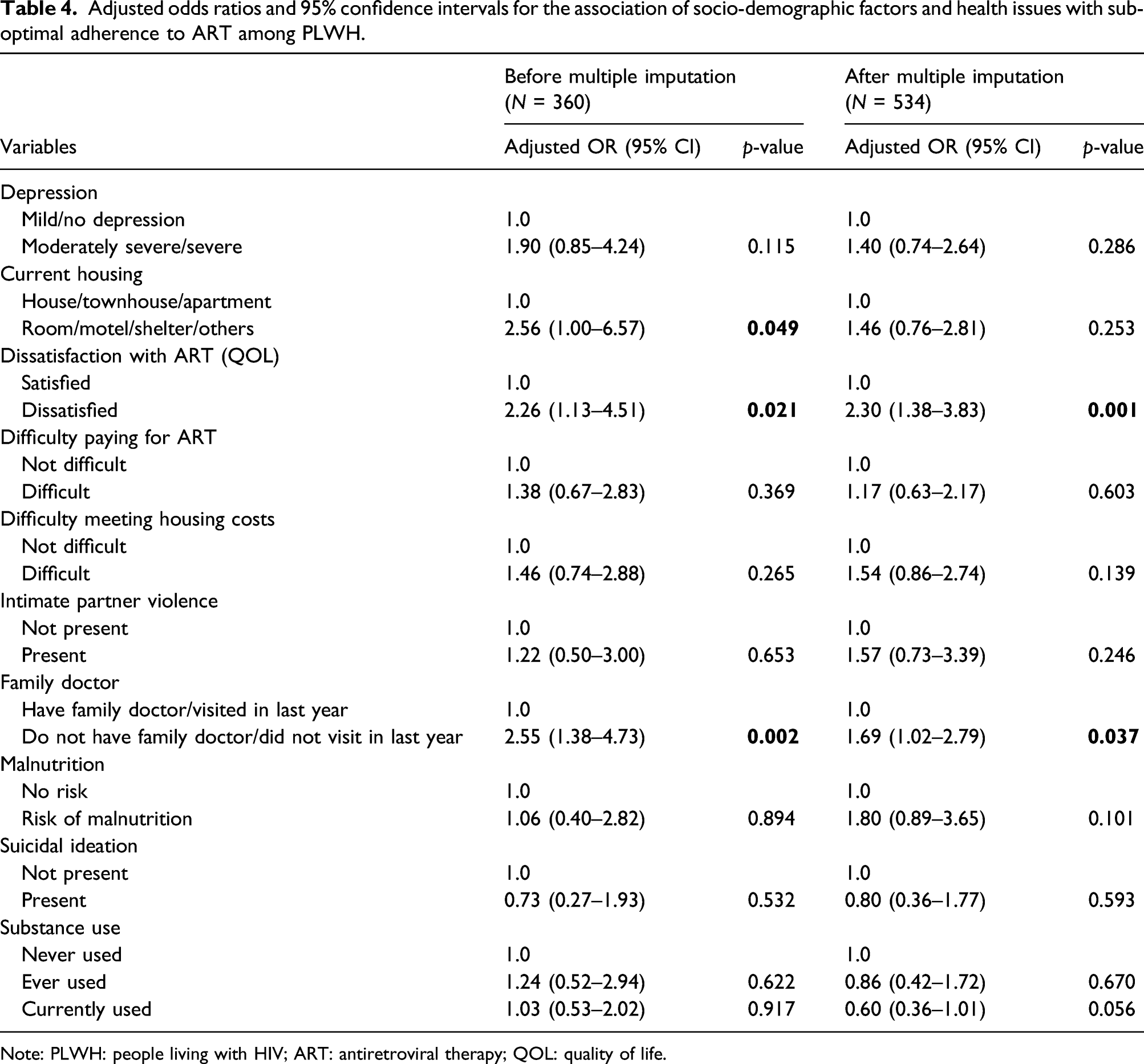
Note: PLWH: people living with HIV; ART: antiretroviral therapy; QOL: quality of life.
Discussion
This study investigated the feasibility of using tablet-based PROs in a busy ambulatory HIV clinic as a screening tool to systematically collect and document a wide range of health-related information associated with adherence to ART. The high participation rate of using PROs (92.5%), high completion rate (mean =95.5%) and high response rate to the individual PRO questions (mean =96.8%) suggests that this approach was feasible. Dissatisfaction with ART and not having a family doctor were significantly associated with inadequate adherence in multivariable analysis.
We observed that 80.3% participants reported HIV medication adherence of ≥95%. Two other Canadian studies have reported optimal medication adherence among 55% and 67% among HIV patients, respectively.37,38 Our participation rates were higher than those reported in the literature in outpatient clinics using tablet-based PROs as standard of care.16,20,39,40 Kjær et al. described the implementation of PROs in HIV clinics in which an invitation letter with a link to PRO was sent to patients 14 days prior to their scheduled appointment and patients could respond to the questionnaire through a web-based interface from home. They reported that 52% of patients submitted their PRO results. 20 Jamilloux et al. implemented PROs through monthly emails, and they observed that the monthly participation rate ranged from to 77%–89%. One of the reasons cited by 31% of non-responders was ‘away from home internet access’. 40 Since participation has been shown to increase when patients are approached face-to-face, the presence of a coordinator to facilitate the PRO data collection, by actively recruiting participants and supporting individuals might have improved uptake in our study. 39 Moreover, the fact that participants were completing PRO assessments at their clinic appointment might have added to the high participation rates. The major reasons for refusal in our study suggest that response rates could potentially be further improved by translating the questionnaire into different languages based on the patient population. Since this study, the PRO assessment has been translated into Spanish and Creole to address this issue.
Our study revealed that not having or not visiting a family doctor in the past year was associated with non-adherence to ART. Kendall et al. reported in a population-based study that 47.2% of PLWH in Ontario had co-management by a family physician and specialist which indicates that the lack of primary care is a systemic problem for PLWH. 41 The model of HIV care delivery at our centre and others in Canada is that family physicians provide primary healthcare services and refer to HIV specialists to provide HIV care when required. Since the HIV patients are seen by a specialist at our clinic twice a year on an average, having a family doctor provides another opportunity to review health status, screen for complications and antiretroviral tolerability and discuss the importance of adherence on a more regular basis. 42 Another factor observed to be linked to adherence was dissatisfaction with ART. This study highlights that an assessment of quality of life related to ART can be valuable since it is associated with medication adherence.43–45
Our study has several limitations that warrant consideration. First, we did not quantify all unintended consequences of the PRO intervention, such as formally timing changes in the duration of clinic visits and impacts on clinic workflow. Provider perceptions however were positive in this regard within the PROgress Study and will be reported at a future date. Another limitation is that adherence was measured at a single time point, whereas adherence is a dynamic process that may change over time. While the collection of longitudinal information could provide a more accurate understanding of patients’ adherence, we feel this issue is unlikely to compromise our overall findings about feasibility and the correlates of sub-optimal adherence. Information on the specific ART agents taken, which might influence treatment satisfaction and adherence to ART, was not collected as a part of this study. Also, this screening tool was accessible only to patients who attended the HIV clinic, were engaged in care and demonstrated their need of support services. Therefore, the applicability to those patients not engaged in routine care (and whose adherence may be the lowest of the population as a whole), is limited. Further, the cross-sectional nature of our study design precludes us from determining causality. Finally, the generalizability of the findings was somewhat limited by our restriction to English-speaking individuals with no cognitive deficits in an urban, high-income country setting.
Conclusion
Patient-reported outcomes provide important self-reported information that involves patients as active partners in their care and gives healthcare providers real-time information about adherence and related risk factors. Collecting PROs before a consultation is a feasible strategy for providing new relevant information that can improve the quality of care.
Supplemental Material
sj-pdf-1-std-10.1177_09564624211032796 – Supplemental Material for Feasibility of implementing a same-day electronic screening tool for clinical assessment to measure patient-reported outcomes for eliciting actionable information on adherence to HIV medication and related factors in a busy Canadian urban HIV clinic
Supplemental Material, sj-pdf-1-std-10.1177_09564624211032796 for Feasibility of implementing a same-day electronic screening tool for clinical assessment to measure patient-reported outcomes for eliciting actionable information on adherence to HIV medication and related factors in a busy Canadian urban HIV clinic by Shivali Suri, Deborah Yoong, Duncan Short, Darrell HS Tan, Mark Naccarato, Heidi M Crane, Alexandra Musten, Rob J Fredericksen, William B Lober and Kevin Gough in International Journal of STD & AIDS
Footnotes
Acknowledgements
We would like to thank the staff of the Positive Care Clinic at St. Michael’s Hospital for their assistance in carrying out the study and, most importantly, to the patients at St. Michael’s Hospital who gave generously of their time and experience during their clinic visits. We also thank Dr Rosane Nisenbaum for the guidance and support in creating and selection of logistic regression models and imputations.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Duncan Short is an employee and shareholder of ViiV Healthcare/GSK. Darrell H. S. Tan (DHST) is supported by a Tier 2 Canada Research Chair in HIV Prevention and STI Research. DHST’s institution has received investigator-initiated research support from Abbvie. Gilead and ViiV Healthcare. DHST is a Site Principal Investigator for clinical trials sponsored by Glaxo Smith Kline. Heidi Crane is also supported by grant funding to her institution from the NIH, AHRQ and ViiV Healthcare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by a grant from OHTN received through ViiV Healthcare LLC and the GlaxoSmithKline group of companies (Project Number: 209144).
Supplementray material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.