
Abstract
We aimed to identify subgroups within age, racial/ethnic, and transmission categories that drive increased risk for late HIV diagnosis (LHD).
A 1996–2013 retrospective study of HIV-diagnosed individuals (N = 77,844) was conducted. The proportion of individuals with LHD (AIDS diagnosis within 365 days of HIV diagnosis) was determined, stratified by age, race/ethnicity, and transmission category. Logistic regression with interaction terms was used to identify groups/subgroups at risk for LHD during 1996–2001, 2002–2007, and 2008–2013.
Respectively, 78%, 27%, 38%, and 31% were male, White, Black, and Hispanic. Overall, 39% had LHD with a 6.7% reduction for each year increase (OR = 0.93, 95% CI = 0.93–0.94, p < 0.01). Older age was significantly associated with increased odds of LHD (OR range = 1.90–4.55). Compared to their White counterparts, all Hispanic transmission categories (OR range = 1.31–2.58) and only Black female heterosexuals and men who have sex with men (MSM) (OR range = 1.14–1.33) had significantly higher odds of LHD during 1996–2001 and/or 2002–2007. Significance was limited to Hispanic MSM (all age categories), MSM/IDUs (30–59 years), and heterosexuals (18–29 years) and Black MSM (30–39 years) during 2008–2013.
Older individuals and Hispanics (driven by MSM) are at increased risk for LHD. HIV testing interventions directed at seniors and Hispanic MSM can further reduce rates of LHD.
Introduction
Due to advances in medicine, human immunodeficiency virus (HIV) infection no longer poses the perilous social threat it once did. With appropriate care, people living with HIV (PLHIV) can both live a normal life with an average life expectancy1–5 and prevent further transmission.6–8 However, the benefits of HIV care can only be maximized when these persons are diagnosed early in the course of the disease and linked to care.
Late diagnosis of HIV (LHD) is a major impediment to ending the HIV epidemic. LHD allows the disease to progress uninterrupted to AIDS and also allows for an extended interval during which the person might transmit HIV unknowingly. LHD has been defined in various settings based on the timing of AIDS diagnosis (CD4 count <200 cells/mm3 or clinical presentation with an AIDS-defining illness) 9 relative to HIV diagnosis. Studies conducted within the United States typically operationalize LHD as having an AIDS diagnosis within 3 10 or 1211–14 months of HIV diagnosis. Such studies have found temporal declines in the rate of LHD whether measured based on three months 10 or 12 months. 14 However, rates still remain high, with a national rate of 24% recorded in 2012. 10
Interventions to reduce LHD can be efficient if they target groups with the greatest risk for LHD. 15 Previous studies have attempted to identify groups broadly at risk for LHD but these studies have left unclear whether the risk for LHD is uniform across identified at-risk groups. A CDC study found that LHD rates were higher among Blacks, Hispanics, and heterosexuals. 13 Another study found significantly higher rates of LHD among Hispanics and adults aged 45–64 years in California. Other studies have compared the risk of LHD among more narrowly-defined groups but tended to have statistical issues. For example, a 2012 study reported higher rates among male injecting drug users (IDUs), male heterosexuals, and older individuals but the results were mainly descriptive with no statistical comparisons. 10 Another study found that higher rates of LHD among the older group compared to the younger group. 12 They went further to report higher rates among Black men, Black and Hispanic women, and male IDUs. However, the second analysis was limited to older adults aged 50–65 years, limiting the application of the findings to the younger population due to range restriction. These studies, taken together, indicate that older individuals and racial/ethnic minorities have relatively higher rates of LHD, with diagnostic delays of three years or more estimated in other studies. 16 It is therefore necessary to look more closely at these groups and identify subgroups within them that may explain the relatively high rates of LHD in these groups as a whole.
A test of interaction is a useful approach to determine whether the effect of a risk factor for LHD is modified by another factor. A significant interaction effect suggests that the association between one risk factor and the outcome depends on the value of another variable. For example, the association between race/ethnicity and LHD could depend on the transmission category (transmission risk group) and vice-versa. In order words, a significant race/ethnicity by transmission category interaction exists. This would imply that racial/ethnic disparity in LHD is heterogenous across the different transmission categories. That is, racial/ethnic disparity in LHD may be higher or lower among men who have sex with men (MSM) compared to heterosexuals. Put a different way, transmission category modifies the effect of race/ethnicity on LHD. Therefore it would be of interest to know which of the transmission categories experience worse racial/ethnic disparities.
In our study, we applied tests of interaction to determine whether the risk of LHD is homogenous across age, racial/ethnic, and transmission categories in three time periods between 1996 and 2013. Our goal was to identify subgroups that drive the risk for LHD within age, racial/ethnic, and transmission categories experiencing disproportionate rates of LHD, in order to allow for the development of more efficient interventions that focus on those with the greatest need. In our report, we focus on determining whether there are worse racial/ethnic disparities within transmission categories and/or age groups identified as having disproportionate rates of LHD. Drivers of racial/ethnic disparities in LHD are of particular interest because racial/ethnic disparities in HIV are consistently found along the continuum of HIV care as well as in HIV risk and survival outcomes.17,18 Hence, interventions that address racial/ethnic disparities in HIV diagnosis have the potential to address downstream disparities along the continuum of HIV care and disparities in survival outcomes.
Materials and methods
This was a retrospective cohort study of adults aged 18–89 years diagnosed with HIV in Texas between January 1996 and December 2013 using Texas HIV surveillance data obtained from Texas Department of State Health Services. The dataset was de-identified and included the following variables: age at HIV diagnosis (years), gender at birth (male/female), race/ethnicity (White, not Hispanic; Black, not Hispanic; Hispanic; Other; Unknown), risk transmission category (MSM only; IDUs only; dual MSM and IDU (MSM/IDU); heterosexual; pediatric; adult other) and number of months between HIV and AIDS diagnosis. The surveillance data included a probability variable associated with risk transmission category so that more than one risk transmission category, each with a probability, could be assigned to an individual. All probabilities for each individual summed to one. For this study, we selected the risk transmission category assigned the highest probability as the transmission category for each individual and blended ‘pediatric’ and ‘adult other’ into a single value, ‘other,’ due to the categories’ small size. We combined ‘gender’ and ‘risk transmission category’ into a single variable, ‘transmission category,’ with the following categories: MSM, male IDU, female IDU, MSM/IDU, male heterosexual, female heterosexual, other males, and other females. In concordance with similar studies conducted in the US, LHD was defined as a difference between HIV and AIDS diagnoses of ≤12 months.11,14,19,20 Individuals with missing data on AIDS diagnosis were assumed to be AIDS-free as of December 31, 2013 since, at the time of data acquisition, Texas HIV surveillance data collection was complete up to this date.
Descriptive analysis was conducted using means (standard deviations) and frequencies (percentages). The proportion of patients with LHD was determined for each calendar year of diagnosis. The Wald test for difference between proportions was used to compare the difference in LHD between 1996 and 2013. 21 To quantify the trend in LHD, a logistic regression model incorporating year of HIV diagnosis and controlling for age (continuous variable), race/ethnicity, and transmission category was applied. Logistic regression analyses were also used to determine factors (age, race/ethnicity and/or transmission category) associated with LHD in three time periods – 1996–2001, 2002–2007, and 2008–2013. The analyses were done in time intervals to assess changes in risk of LHD over time. In order to determine whether the risk of LHD was homogenous across subgroups within age, racial/ethnic, and transmission categories, two-way interactions terms were initially tested in the models (age by race/ethnicity, age by transmission category, and race/ethnicity by transmission category). In the final models, the significant interaction terms were retained. Three-way interaction terms were included when two or more two-way interaction effects were significant to allow for the estimation of conditional odds ratio (OR) comparing groups within one factor given fixed levels of the other two factors. From an analytical standpoint, having two 2-way interactions among the three variables indicates overlapping interactions that can successfully be captured with a three-way interaction term. Because reporting a single group effect size where interaction exists introduces ‘wrong model bias’ by failing to account for the heterogeneity that exists within the group, 22 we report the effect sizes (as ORs) for subgroups within the interacting variables. In line with the goals of our study, we prioritize reporting racial/ethnic differences within subgroups.
The level of significance was set at p < .05. All analyses were conducted using SAS 9.4.
Results
A total of 77,844 individuals in Texas aged 18–89 years were diagnosed with HIV during 1996–2013, ranging from 3,289 to 5,218 persons per calendar year. A significant proportion were aged 30–39 years (34%), MSM (58%), and Black (38%) (Table 1). From 1996 to 2013, the proportion of HIV-diagnosed individuals who were White and IDU declined from 34% to 22% and from 17% to 3%, respectively, while the proportion who were Hispanic and MSM increased from 25% to 36% and from 53% to 71% respectively. Similarly, the proportion of HIV-diagnosed persons aged 30–39 years decreased from 45% in 1996 to 25% in 2013 while the proportion aged 18–29 years increased from 25%to 42%.
Characteristics of persons diagnosed with HIV and rate of late HIV diagnosis in Texas, 1996 to 2013 (N = 77,844).
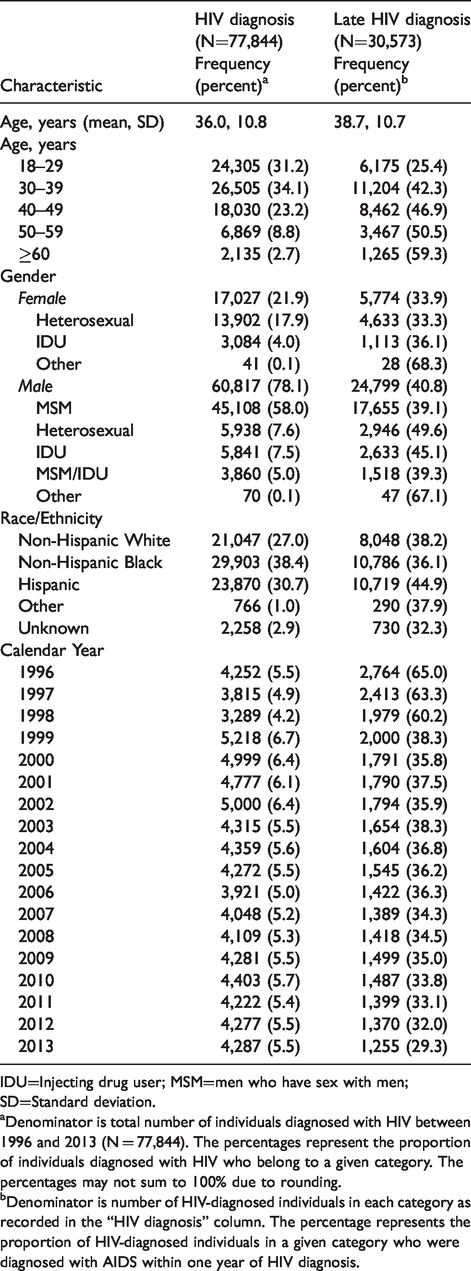
IDU=Injecting drug user; MSM=men who have sex with men; SD=Standard deviation.
aDenominator is total number of individuals diagnosed with HIV between 1996 and 2013 (N = 77,844). The percentages represent the proportion of individuals diagnosed with HIV who belong to a given category. The percentages may not sum to 100% due to rounding.
bDenominator is number of HIV-diagnosed individuals in each category as recorded in the “HIV diagnosis” column. The percentage represents the proportion of HIV-diagnosed individuals in a given category who were diagnosed with AIDS within one year of HIV diagnosis.
Overall, 30,573 individuals (39%) had LHD, with 18,651 individuals (41%) having both HIV and AIDS diagnoses in the same month. Sixty-five percent, 63%, and 60% of persons diagnosed with HIV in 1996, 1997, and 1998, respectively, had LHD. The proportion fell sharply to 38% in 1999 and then gradually declined to 29% in 2013 (Figure, Supplemental Digital Content 1). The Wald test showed that the difference between 1996 and 2013 was statistically significant (risk difference (RD) = 35.7%, 95% confidence interval (95%CI) = 33.8%–37.7%). Times series logistic regression showed that for each calendar year increase, the odds of LHD reduced by 6.7% (OR = 0.933, 95% CI = 0.930–0.936) (Table 2).
Logistic regression model of late HIV diagnosis on year of diagnosis controlling for risk factors.
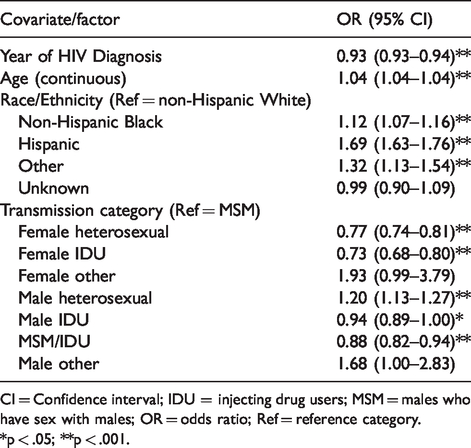
CI = Confidence interval; IDU = injecting drug users; MSM = males who have sex with males; OR = odds ratio; Ref = reference category.
*p < .05; **p < .001.
The trend of a sharp decline in 1999 followed by a gradual slope to 2013 was consistent across age, gender, race/ethnicity, and transmission categories (Figure, Supplemental Digital Content 1; Table, Supplemental Digital Content 2). The Wald test showed that the difference between 1996 and 2013 was also statistically significant for each age, gender, race/ethnicity, and transmission category (p < 0.001 in each case). However, the change was greater among non-Hispanic Whites (42%, 39%–46%) than non-Hispanic Blacks (34%, 95%CI = 31%–38%) and Hispanics (35%, 95%CI = 31%-38%). Among men, the change was as follows: MSM (41%, 95%CI = 39%–44%), IDUs (38%, 95%CI = 28%–49%), MSM/IDUs (34%, 95%CI = 23%–45%) heterosexuals. (26%, 95%CI = 18%–24%). Among females, the change as follows: IDUs (22%, 95%CI = 6–37%), heterosexuals (15%, 95%CI = 10%–21%). By age group, the change was as follows: 18–29 years (30%, 95%CI = 26%–33%), 30–39 years (36%, 95%CI = 33%–40%), 40–49 years (37%, 95%CI = 33%–42%), 50–59 years (29%, 95%CI = 22%–36%), ≥60 years (39%, 95%CI = 28%–49%).
We used logistic regression with interaction terms to identify subpopulations that drive LHD. Interaction effects were evaluated and used to guide the comparison of homogenous subgroups. Logistic regression modeling with two interaction terms showed significant race/ethnicity-transmission category interaction for time periods 1996–2001 and 2002–2007 and significant age-transmission category and race/ethnicity-transmission category interactions for periods 2008–2013. The race/ethnicity-transmission category interaction term was retained for the 1996–2001 and 2002–2007 models. A three-way interaction term was added to the 2008–2013 model in order to fully capture the multiple interactions occurring between age, race/ethnicity, and transmission category.
Table 3 shows the results of the final logistic regression models of the odds of LHD during 1996–2001 and 2002–2007 comparing age groups and comparing racial/ethnic groups with transmission category as an effect modifier. Table 4 shows the results of the final multivariate logistic regression models of the odds of LHD during 2008–2013 comparing race/ethnicity with age and transmission categories as effect modifiers (i.e. Blacks and Hispanics were compared to Whites of similar age and transmission categories). There was a trend of increasing odds of LHD with increasing age during both 1996–2001 (OR range = 1.90–3.95) and 2002–2007 (OR range = 1.97–4.55).
Odds of late HIV diagnosis comparing age and racial/ethnic groups with transmission category as an effect modifier, 1996–2007.
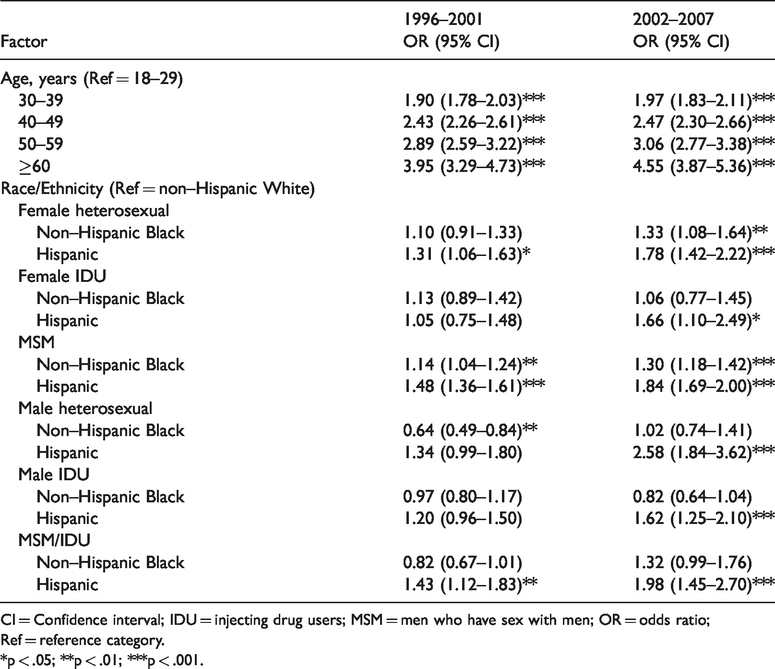
CI = Confidence interval; IDU = injecting drug users; MSM = men who have sex with men; OR = odds ratio; Ref = reference category.
*p < .05; **p < .01; ***p < .001.
Odds ratio of late HIV diagnosis comparing racial/ethnic groups with age and transmission category as effect modifiers, 2008–2013.
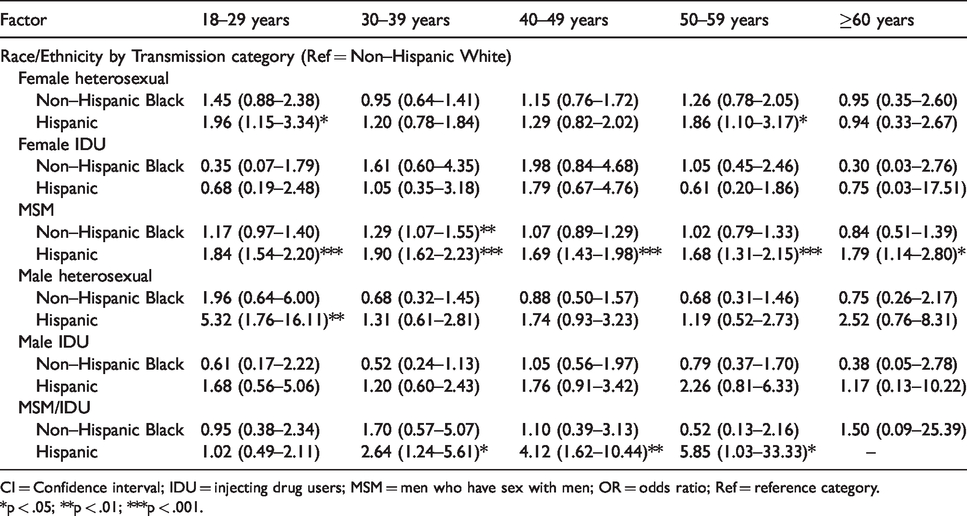
CI = Confidence interval; IDU = injecting drug users; MSM = men who have sex with men; OR = odds ratio; Ref = reference category.
*p < .05; **p < .01; ***p < .001.
Comparing Blacks to their White counterparts, Black MSM had higher odds of LHD during both 1996–2001 (OR = 1.14, 95%CI = 1.04–1.24) and 2002–2007 (OR = 1.30, 95%CI = 1.18–1.42). Black female heterosexuals had higher odds of LHD during 2002–2007 (OR = 1.33, 95%CI = 1.08–1.64). On the other hand, Black male heterosexuals had lower odds of LHD during 1996–2001 (OR = 0.64, 95%CI = 0.49–0.84). During 2008–2013, only Black MSM aged 30–39 years had higher odds of LHD (OR = 1.29, 95%CI = 1.07–1.55) compared to White MSM aged 30–39 years.
Comparing Hispanics to their White counterparts, Hispanic female heterosexuals (OR range = 1.31–1.78), MSM (OR range = 1.48–1.84), and MSM/IDUs (OR range = 1.43–1.98) had higher odds of LHD during both 1996–2001 and 2002–2007. Also, Hispanic female IDUs (OR = 1.66, 95%CI = 1.10–2.49), male heterosexuals (OR = 2.58, 95%CI = 1.84–3.62), and male IDUs (OR = 1.62, 95%CI = 1.25–2.10) had higher odds of LHD during 2002–2007 compared to their White counterparts. During 2008–2013, significance was limited to Hispanic MSM (all aged categories), MSM/IDUs aged 30–59 years, female heterosexuals aged 18–29 and 50–59 years, and male heterosexuals aged 18–29 years (Table 4).
Discussion
In this study on LHD among HIV-diagnosed individuals during 1996–2013, we observed an overall decline in LHD over time. The sharpest decline occurred in 1999 when LHD fell by 22%. This period coincides with the introduction of combination antiretroviral therapy (ART) in the U.S which has been shown to be superior to mono- or dual- therapy in delaying clinical progression to AIDS. 23 Combination ART was first recommended by the U.S. Department of Health and Human Services in 1998. 24 The sharp decline in LHD may therefore reflect advances in drug management of PLHIV in the US. The observed decline in LHD may also have been due to the success of HIV testing programs, 17 which are an evidence-based approach for promoting early HIV diagnosis.
We also observed progressively increased risk of LHD with increasing age with the disparity gap increasing over time. Adults ≥60 years, in particular, were four or more times more likely than those aged 18–24 years to have LHD. These results support findings from other studies10,12,25 and may jointly be a reflection of delayed HIV testing 16 and repressed immune recovery 26 with increasing age. Past 12-month HIV testing rates have been estimated to be 40% lower for older adults ≥50 years compared to adults <50 years with testing rate at 4% for those aged 50–64 years.25,27 As part of the strategies to end the HIV epidemic, CDC HIV testing guidelines recommend routine voluntary HIV screening for adults aged 13–64 years and repeat testing for individuals at high risk of HIV infection. 28 Based on this recommendation, many older adults are likely to be missed for HIV testing. Further, identifying older adults at high risk for HIV infection presents some challenges in regular healthcare settings as providers are less likely to probe about the sexual behaviors of older adults. 29 Targeted HIV testing programs for older adults may circumvent this challenge. Such programs can be implemented in settings where older adults are likely to congregate such as senior centers. These would be similar to HIV prevention interventions for IDUs at substance use treatment centers. 30
Significant disparities in LHD were also observed for Hispanics. Compared to Whites, Hispanics had higher risk for LHD. This was observed among MSM, MSM/IDUs, and female heterosexuals during 1996–2001 and all transmission categories during 2001–2007. Hispanic MSM (all age categories) and MSM/IDUs (30–59 years) retained higher rates of LHD during 2008–2013. Other studies have observed higher rates of LHD among Hispanics.11–13,31 But our findings further suggest that Hispanic MSM may be driving the disparities among MSM. Past 12-month HIV testing for Hispanics significantly increased from 11% to 12% during 2000–2010 based on National Health Interview Survey (NHIS) data. 17 The same statistic increased from 17% to 18% during 2011–2017 based on Behavioral Risk Factor Surveillance System (BRFSS) data. 32 However, this change was not significant, suggesting little progress in improving early HIV diagnosis among Hispanics. Culturally-sensitive evidence-based HIV testing initiatives are, therefore, recommended to reach the Hispanic population. But these need to be tailored according to transmission category or age level. For example, the social network strategy has been shown to be effective in increasing HIV testing rate among high-risk populations like MSM. 33 This can be tailored to the Hispanic MSM population by coaching Hispanic MSM to recruit other Hispanic MSM.
One limitation of our study is that data were limited to one state. However, Texas has the fourth highest number of PLHIV in the US and the demographics of the HIV population in Texas closely reflects the national distribution.34,35 Hence, we can make inferences about the US with some degree of confidence. The period covered in our study presents another limitation. At the time of data acquisition, complete data from all reporting sites was only available up to 2013.
Our study has some strengths. Although previous studies had identified subgroups at risk for LHD, they do not account for heterogeneity within these subgroups. Our study is the first study to address such heterogeneity. The lack of significant age by transmission category and age by race/ethnicity interactions during 1996–2001 and 2002–2007 implies that the effect of age was similar across transmission categories and race/ethnicity during this period. Our approach of evaluating risk in time blocks, which has not previously been done, allowed for the observation of temporal trends in risk factors. Our results showed overall improvements for most subgroups except Hispanic MSM. This historical perspective can inform the future deployment of resources for HIV testing to prioritize the Hispanic MSM population.
Conclusions
Despite the decline in rate of LHD, almost 30% (N = 1,255) of HIV-diagnosed individuals were diagnosed late in 2013. From a clinical perspective, late presentation with HIV leads to poor prognosis for the infected individuals in terms of rapid progression to AIDS36–39 and lower survival probability37–42 which could result in higher direct medical costs and productivity loss for the health system and society, respectively.43–45 From a public health perspective, LHD results in missed opportunities to prevent HIV transmission.44,46–48 From our study, we identified older individuals and Hispanics as groups at risk for LHD, with MSM driving the disparity among Hispanics. We recommend HIV testing interventions directed at senior centers, and Hispanic MSM to further reduce the rate of LHD since individuals in these settings are more at risk for late diagnosis.
Supplemental Material
sj-pdf-1-std-10.1177_0956462420947567 - Supplemental material for Identifying subgroups within at-risk populations that drive late HIV diagnosis in a Southern U.S. state
Supplemental material, sj-pdf-1-std-10.1177_0956462420947567 for Identifying subgroups within at-risk populations that drive late HIV diagnosis in a Southern U.S. state by Sabina O Nduaguba, Kentya H Ford, James P Wilson, Kenneth A Lawson and Robert L Cook in International Journal of STD & AIDS
Supplemental Material
sj-pdf-2-std-10.1177_0956462420947567 - Supplemental material for Identifying subgroups within at-risk populations that drive late HIV diagnosis in a Southern U.S. state
Supplemental material, sj-pdf-2-std-10.1177_0956462420947567 for Identifying subgroups within at-risk populations that drive late HIV diagnosis in a Southern U.S. state by Sabina O Nduaguba, Kentya H Ford, James P Wilson, Kenneth A Lawson and Robert L Cook in International Journal of STD & AIDS
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.