
Abstract
There are increasing reports of antiretroviral therapy (ART) drug-related kidney dysfunction. Traditional markers of kidney dysfunction such as urine protein/creatinine ratio and estimated glomerular filtration rate (eGFR) have thus far proven ineffective at detecting some sub-clinical forms of ART-related kidney injury. This is a cross-sectional examination of 114 people living with HIV (PLWH), either naïve (N =104) or treatment experienced (N =10). Urinary kidney injury molecule-1 (KIM-1 ng/mg) thresholds were estimated using electrochemiluminescent assays from stored urine samples and normalised for urinary creatinine excretion (KIM-1/Cr). Correlation coefficients and predictors of kidney tubular injury were compared and derived for both adjusted and unadjusted urinary KIM-1/CR (ng/mg). In PLWH (both ART-naïve and treatment experienced) had a higher baseline unadjusted and adjusted median (≥3.7 ng/mg) and upper tertile (≥6.25 ng/mg) urinary KIM-1/Cr levels compared to either non-normal volunteers (0.39 ng/mg) or those with acute kidney injury in the general population (0.57 ng/mg). When upper tertile KIM-1/Cr (≥6.25 ng/mg) was utilised as a marker of kidney injury, eGFR (ml/min/1.73 m2), white Caucasian ethnicity, and protease inhibitor exposure were significantly associated with increased risk of kidney injury in multivariate analyses (odds ratio 0.91, confidence interval [CI] 0.68–0.98, P = 0.02; odds ratio 8.9, CI 1.6–48.6, p = 0.01; and odds ratio 0.05, CI 0.03–0.9, p =0.04, respectively). We found a significant degree of sub-clinical kidney injury (high unadjusted and adjusted KIM-1/Cr) in PLWH with normal kidney function (eGFR ≥60 ml/min/1.73 m2). We also found a higher baseline KIM-1/Cr (ng/mg) in our study cohort than reported both in normal volunteers and patients with kidney injury in the general population.
Introduction
Kidney disease in its various phenotypes has been reported to be amongst the fourth leading cause of mortality amongst people living with HIV (PLWH) exposed to antiretroviral therapy (ART) drugs.1–4 The range of ART-related extra-glomerular morbidities includes nephrolithiasis associated with the protease inhibitor (PI) atazanavir, and kidney tubular dysfunction (KTD) with tenofovir disoproxil fumarate (TDF)2,5 amongst others. Estimated glomerular filtration rate (eGFR) has been reported to be normal in the setting of up to five-fold increase in urine albumin:creatinine ration (ACR) in one study in PLWH. 6 Therefore, having a biomarker reporting sub-clinical kidney tubular injury early in PLWH exposed to ART will be important, as it will allow risk stratification of these patients before commencement of ART including monitoring whilst on them. A number of candidate low molecular weight proteins (LMWPs) excreted in urine have been proposed as potential surrogate markers of kidney injury in these cohorts of patients. 7 The role of kidney injury molecule-1 (KIM-1) in the diagnostic evaluation of kidney injury has been the subject of increasing attention in the general population but perhaps less so in PLWH. It has however continued to generate increasing mechanistic and clinical interest regarding its probable utilisation as an early reliable marker as well as risk-stratification tool for PLWH with suspected kidney tubular injury.8,9 It is expressed by several cells including kidney tubular cells following exposure to stress (including metabolic, infective, and inflammatory stress). 9 It is a trans-membrane glycoprotein with an ecto-domain which when cleaved and excreted in urine can be estimated and has been shown to correlate with kidney injury. 9 Urinary KIM-1 excretion has been shown to correlate with varying degrees of kidney injury in both mechanistic and systematic studies in the general population both as a predictor of adverse outcomes as well as a surrogate marker.9,10 However, the role of both HIV infection itself and secondary ART-related kidney injuries in the urinary kinetics of KIM-1 (adjusted for urine creatinine excretion) remains unknown and has continued to generate intense mechanistic debate. 10 Notably its total lack of expression in healthy kidneys makes it an elegant and potential useful biomarker of kidney injury in both PLWH on ART and the general population. Determining kidney tubular involvement early (before established change in traditional kidney biomarker kinetics) will be a desirable and potentially safer option for patients, because it will allow withdrawal of the offending ART drug. Much as this is the thrust of this study, the long-term utility of this strategy (i.e. use of novel kidney tubular biomarkers) will be dependent on outcome of high power prospective systematic studies.
In this report, we have explored the potential clinical utility of unadjusted urinary KIM-1/Cr (ng/mg) in reporting acute tubular injury vis-à-vis other established traditional markers of kidney injury (eGFR, urine protein/creatinine ratio [PCR]) in PLWH exposed to ART drugs. We have chosen to exclusively explore KIM-1’s diagnostic utility owing to relatively limited data in PLWH compared to other biomarkers.11–14 We hypothesise that establishing KIM-1/Cr as a reliable marker of acute sub-clinical kidney injury in this population could contribute in risk stratification before commencement of potentially nephrotoxic ART drugs.
Patients and methods
We recruited 127 consecutive PLWH attending outpatient’s clinics at Royal Liverpool University Hospital from October 2011 to March 2013. One hundred and fourteen HIV-positive patients were recruited for cross-sectional evaluation of the association between KIM-1 thresholds and various ART exposure. We utilised previously reported KIM-1 levels in PLWH with normal kidney function for comparison with thresholds reported from our study. 15 Inclusion criteria include PLWH (ART-naïve or treatment experienced), age ≥18 years old, any CD4 cell count or viral load, and ability to give consent. Patients satisfying these criteria were counselled and recruited into the study. Figure 1 gives the distribution of the study cohort. Demographic, clinical, and laboratory parameters were abstracted from patient’s case notes and electronic records. Ten millilitres of whole blood and random urine samples (10 ml) were collected for the determination of e-GFR, serum creatinine, urea, alkaline phosphatase, glucose, corrected calcium, inorganic phosphate, urinary creatinine, glucose, phosphate, KIM-1, and urinary albumin/protein (expressed as their creatinine ratios) (see Figure 1 for recruitment flow chart).
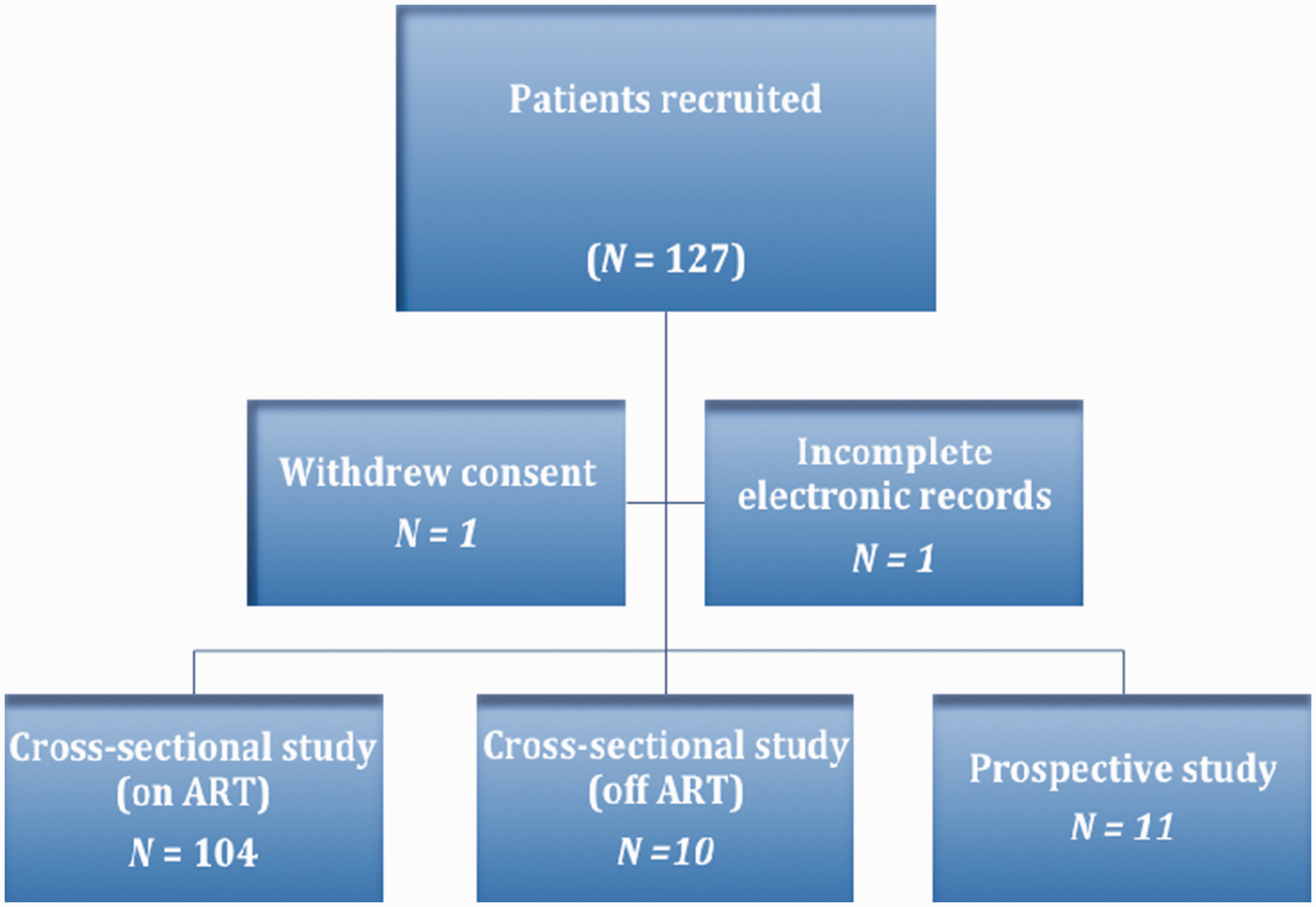
Study flow chart. ART: antiretroviral therapy.
Ethics approval and consent to participate
The study protocol, patient information, consent forms, available safety information, study participants’ recruitment procedures, information about payments, and compensation available to the subjects as well as documentation evidencing the investigator’s qualifications were submitted to the North Manchester Research Ethics Committee (reference: 12/NW/0448), Manchester, England for ethical review and approval according to local regulations, prior to commencement of the study. Following initial review of the study protocol, the study was approved for commencement.
Bio-analytical methods
Stored urine was thawed, mixed, and centrifuged at 3000 r/min for 1 min. Urinary KIM-1 levels in nanograms were then determined from the resulting supernatants using electrochemiluminescent assays (Meso Scale Discovery, MD, USA). These assays were run on a 96-well plate in accordance with the manufacturers’ protocol. Essentially these are sandwich immunoassays with the 96-well plate pre-coated with KIM-1 capture antibody, and utilised a detection antibody conjugated onto an electrochemiluminescent label. The upper limits of quantitation and lower limits of quantitation (LLOQ), respectively, on a seven-point calibration curve were 5000 and 1.22 pg/ml, respectively. Intra- and inter-assay precision were <6 and <7%, respectively, on three plates on different occasions, recovery of spiked samples was 104–107%, and dilutional linearity was shown at 1 in 10, 1 in 100, and 1 in 1000 dilutions in the assay diluentmc. The LLOQ was about 2 standard deviations greater than the background value of the diluent alone and the LLOQ is taken as the limit of detectionmc. Subsequently, derived KIM-1 values were normalised to urinary creatinine (as described elsewhere) 15 and expressed as KIM-1/Cr (ng/mg).
Definitions and kidney outcomes
In this study proteinuria is defined as urine PCR ≥20 mg/mmol Kidney injury was determined based on KDIGO classification
16
We additionally carried out additional comparative analyses between different sub-categories of urine PCR, eGFR, and thresholds of KIM-1/Cr (ng/mg)
Statistical analysis
Continuous variables were presented as median/inter-quartile range or means/standard deviation as appropriate (depending on distribution), and categorical variables as number/percentages. In view of skewed distribution of our dataset with non-sustained linearity of KIM-1/Cr (ng/mg) and urine PCR (mg/mmol) values, these variables were analysed before and after log-transformation. The means/medians of demographic and other laboratory parameters were described and compared with either Mann–Whitney U test (for two variables) or Kruskal–Wallis (for multiple variables). Correlations between unadjusted/adjusted urinary KIM-1/Cr and other demographic variables and markers of kidney function were determined by Spearman’s rho. We carried out linear regression modelling to ascertain the predictors of increased unadjusted urinary KIM-1/Cr excretion. Additionally, we explored the diagnostic value of upper tertile urinary KIM-1/Cr (≥6.25 ng/mg) as a marker of kidney injury by generating multivariate regression models with parameters that have p = ≤0.1 in univariate analyses serving as covariates. All statistical analyses were carried out with StatsDirect software version 2.7.9 (StatsDirect Ltd, Altrincham, Cheshire, UK).
Characteristics of the study population
Table 1 gives demographic and clinical characteristics of the study population. Unadjusted urinary KIM-1/Cr (ng/mg) values followed a non-parametric distribution. Amongst 114 cross-sectional patients examined, mean age was 43.1 years (SD ±9.9), 70.2% were males with a white Caucasian population of 73.7%. Significant proteinuria was present in 20.9% of the study population, with a higher proportion in older patients compared with their gender-matched cohorts (49.3 versus 41.4, respectively, P = 0.002). Median TDF exposure was 36 months (inter-quartile range [IQR] 22.5, 72). Median unadjusted KIM-1/Cr was 4.17 ng/mg (IQR 1.5, 8.2) with an upper quartile threshold of ≥8.6 ng/mg. Patients with urine PCR ≥20 mg/mmol had a higher median KIM-1/Cr (ng/mg) level than their comparable controls (5.9 versus 2.7, confidence interval [CI] 2.4–4.8; P = 0.0001). About 5.3% (N = 6) and 3.5% (N = 3) of the study cohort were hypertensive or had incident diabetes mellitus, respectively. The median nadir/current CD4 cell counts were 200 cells/mm3 (IQR 95, 298) and 565 cells/mm3 (IQR 401, 665), respectively. The median eGFR was 85 ml/min/1.73 m2 (IQR 75.5, 90), with 5.3% of the cross-sectional study cohort having incident chronic kidney disease stage 3. Baseline eGFR levels were significantly lower in males than their age-matched female participants (82 versus 90 ml/min/1.73 m2, respectively; CI 1.4–3.6; P ≤ 0.0001).
Baseline characteristics of the DETIKI (cross-sectional cohort) study population (N = 114).
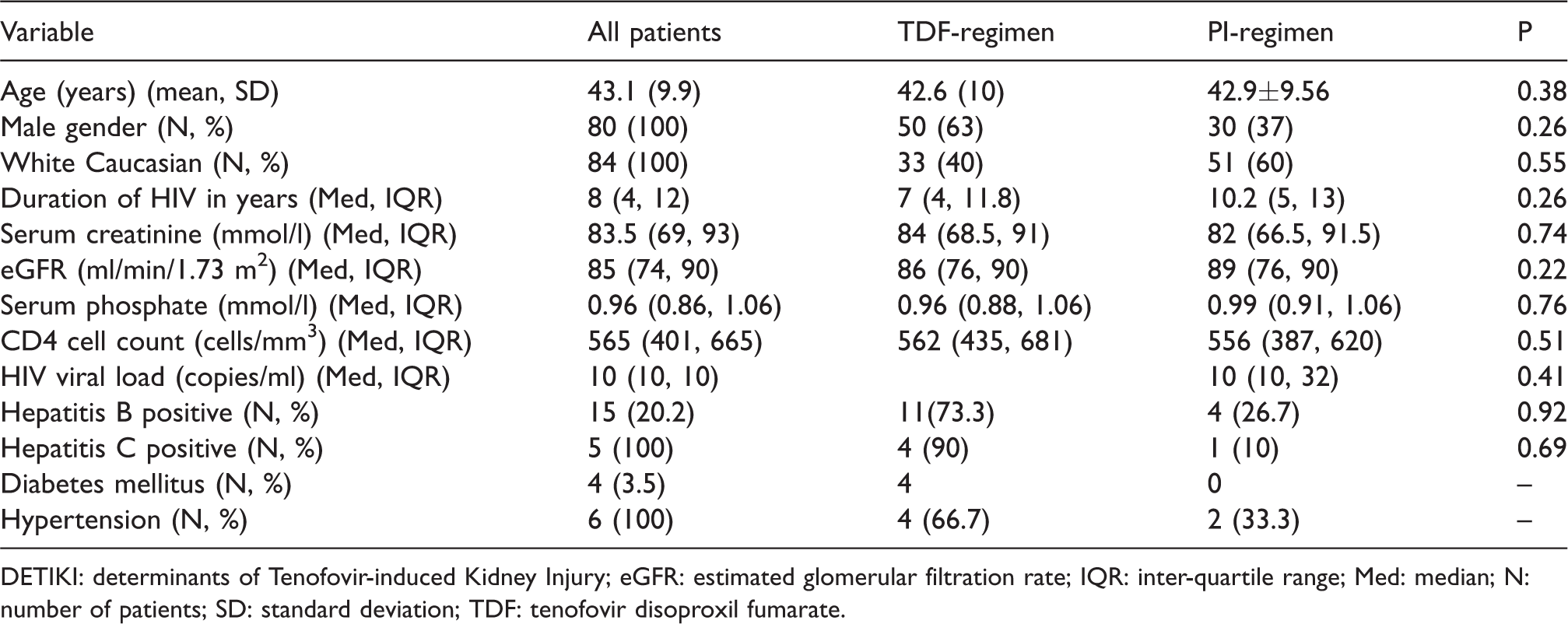
DETIKI: determinants of Tenofovir-induced Kidney Injury; eGFR: estimated glomerular filtration rate; IQR: inter-quartile range; Med: median; N: number of patients; SD: standard deviation; TDF: tenofovir disoproxil fumarate.
KIM-1/Cr levels and ethnicity
Baseline KIM-1/Cr (ng/mg) values were higher in patients of white Caucasian ethnicity (4.1 ng/mg) compared with patients from other ethnic groups (1.1 ng/mg, CI 2.2–3.9; P = 0.0001) (Supplementary material 1). When stratified based on ART exposure, Caucasian patients who were either ART naïve or treatment experienced had a significantly higher baseline KIM-1/Cr (ng/mg) values compared to other ethnicities (8.6 versus 2.1, and 2.2 versus 1.9, respectively).
ART exposure and kidney biomarker levels
Table 2 shows detailed comparison of kidney biomarkers as a function of ART exposure. Unadjusted KIM-1/Cr is uniformly distributed across ART drug regimens. When stratified according to TDF exposure, patients on TDF-containing regimens had a significantly higher median unadjusted KIM-1/Cr than comparable cohorts (Figure 2). Patients on PI-based regimens had higher median urine PCR compared to those on alternative regimens (P = 0.02) (Table 3).
Comparative distribution of kidney biomarkers by antiretroviral therapy regimen.
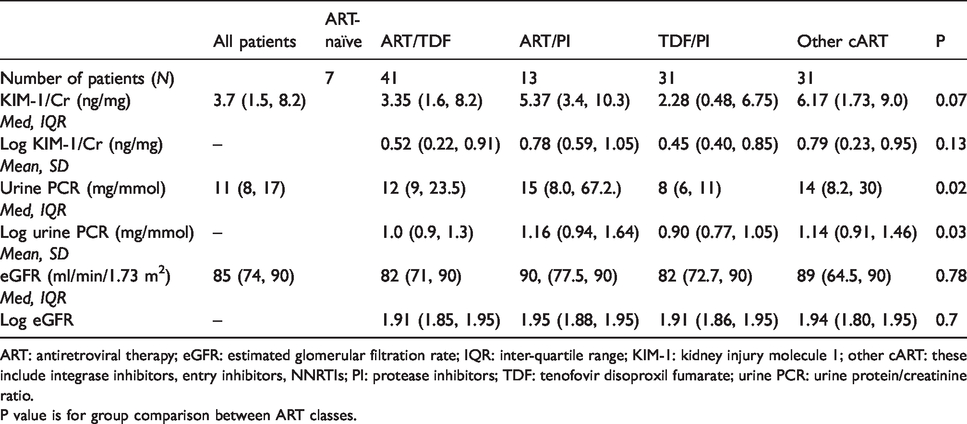
ART: antiretroviral therapy; eGFR: estimated glomerular filtration rate; IQR: inter-quartile range; KIM-1: kidney injury molecule 1; other cART: these include integrase inhibitors, entry inhibitors, NNRTIs; PI: protease inhibitors; TDF: tenofovir disoproxil fumarate; urine PCR: urine protein/creatinine ratio.
P value is for group comparison between ART classes.
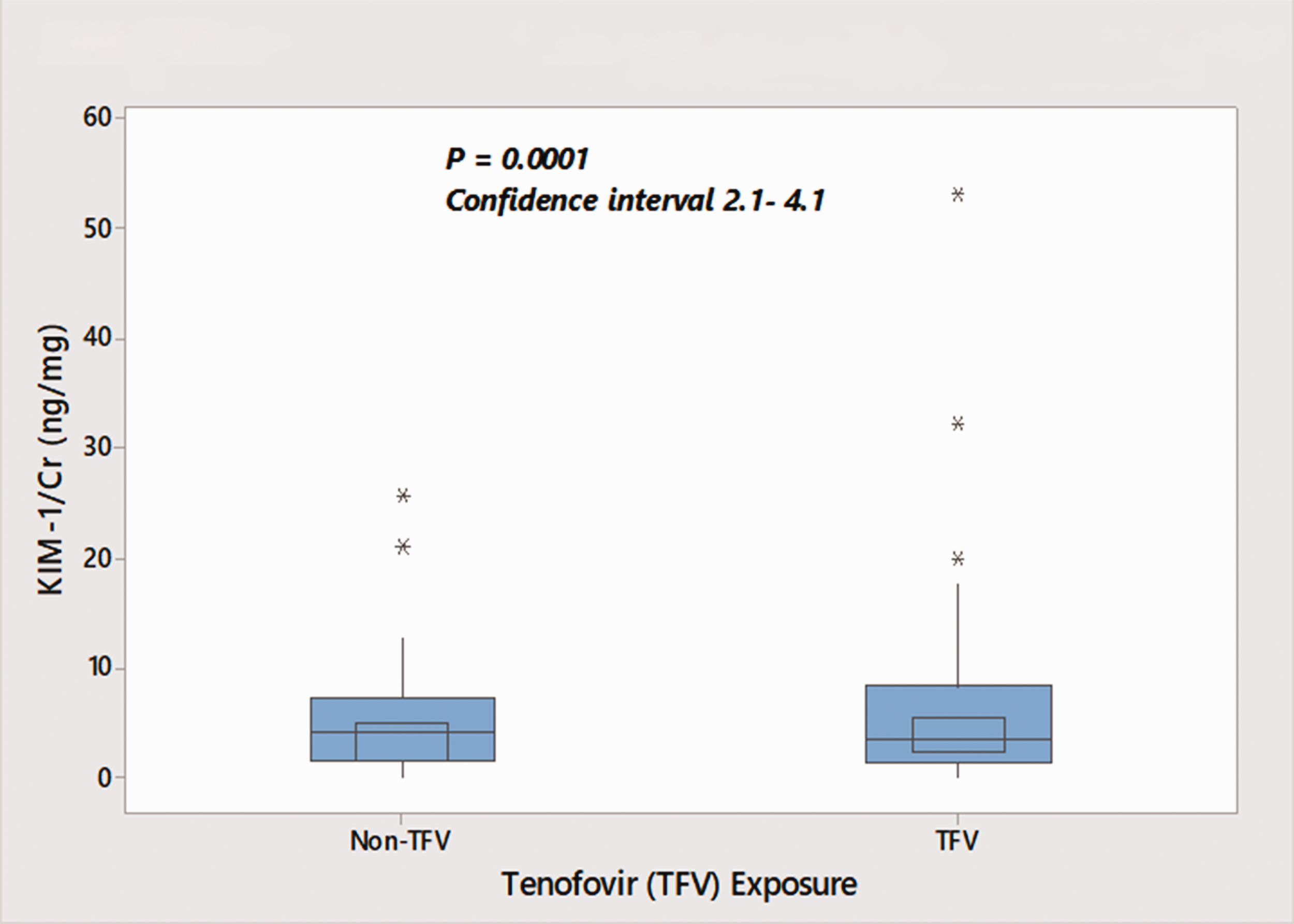
Box plot showing distribution of KIM-1/Cr stratified by tenofovir disoproxil fumarate exposure. KIM-1: kidney injury molecule 1.
Correlation between urinary KIM-1/Cr and traditional markers of kidney injury
There were statistically significant correlations between unadjusted urinary KIM-1/Cr with age, white Caucasian ethnicity, and urine PCR. When stratified into medians/quartiles/tertiles, age and white Caucasian ethnicity maintained significant positive correlations with median KIM-1/Cr (r = 0.3, p = 0.018 and r = 0.29, 0.02, respectively). It is noteworthy that unadjusted urinary KIM-1/Cr (ng/mg) showed a positive correlation with both adjusted and unadjusted urine PCR (a well-established marker of kidney injury in these cohorts of patients) (Figure 3). About 52 and 26.5% of our study population with eGFR greater than 60 ml/min/1.73 m2 had KIM-1/Cr values higher than the median and upper quartile thresholds, respectively (Figure 4). This may suggest a degree of sub-clinical kidney injury in patients with hitherto normal eGFR. Table 4 gives a summary of the correlation matrix of other variables.
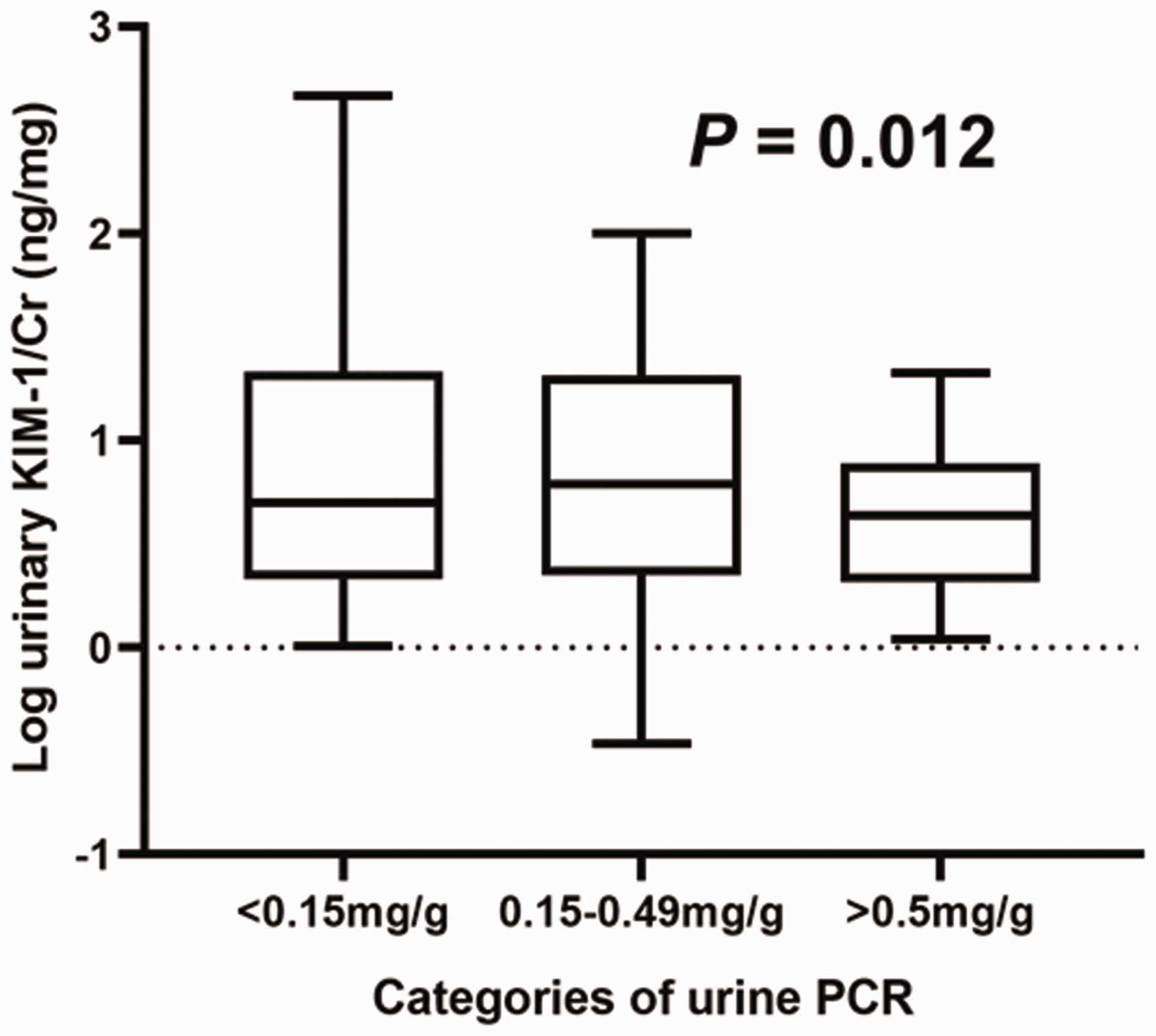
Relationship between unadjusted KIM-1/Cr and stratified urine PCR. Log KIM-/Cr (ng/mg) examined as a function of stratified urinary protein excretion in HIV-positive patients. Patients with urinary protein excretion below diagnostic thresholds have significantly high levels of urinary KIM-1 (corrected for urinary creatinine excretion). KIM-1: kidney injury molecule 1; urine PCR: urine protein/creatinine ratio.
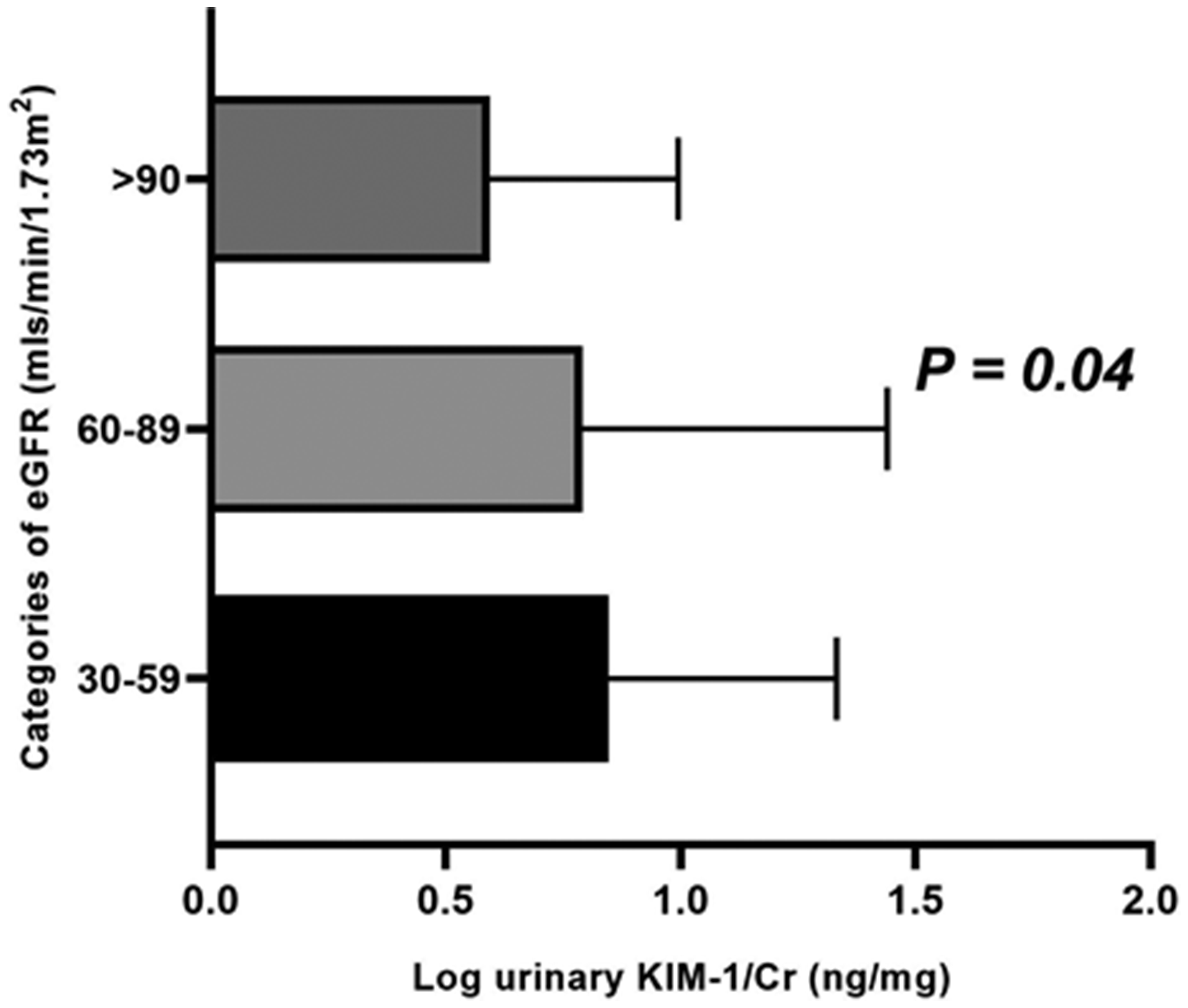
Relationship between log KIM-1/Cr and categories of eGFR. HIV-positive patients with >60 ml/min/1.73 m2 had significant urinary KIM-1 (corrected for urinary creatinine excretion). eGFR: estimated glomerular filtration rate; KIM-1: kidney injury molecule 1.
Predictors of kidney injury
We tested the performance of both unadjusted and upper tertile KIM-1/Cr (≥6.25 ng/mg) as a predictor of kidney injury in PLWH exposed to various ART drugs. By backward logistics regression (likelihood ratio), eGFR (ml/min/1.73 m2), White Caucasian ethnicity, and PI exposure were significantly associated with risk of kidney injury in multivariate analyses (odds ratio 0.91, CI 0.684–0.98, P = 0.02; odds ratio 8.9, CI 1.6–48.6, p = 0.01; and odds ratio 0.05, CI 0.03–0.9, p =0.04, respectively) (Table 5).
Distribution of kidney biomarkers in the two cross-sectional study arms.
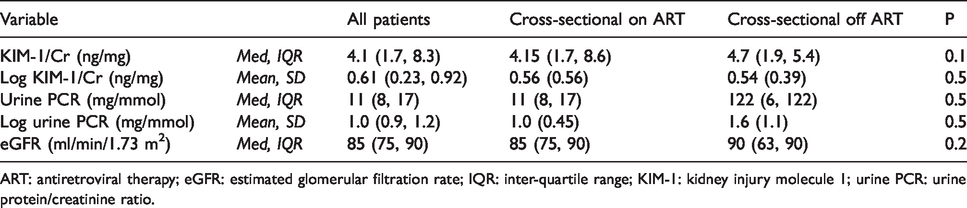
ART: antiretroviral therapy; eGFR: estimated glomerular filtration rate; IQR: inter-quartile range; KIM-1: kidney injury molecule 1; urine PCR: urine protein/creatinine ratio.
Key correlation matrix between unadjusted/adjusted urinary KIM-1/Cr and other markers of kidney function.
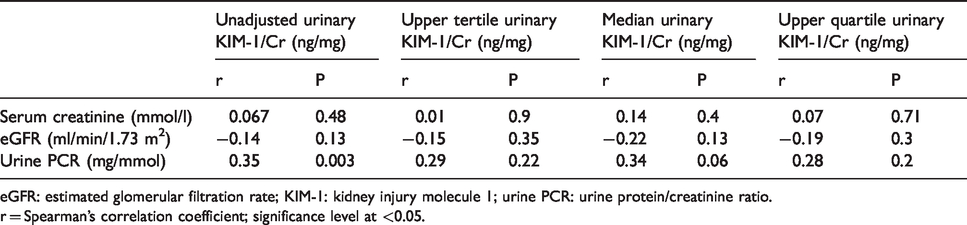
eGFR: estimated glomerular filtration rate; KIM-1: kidney injury molecule 1; urine PCR: urine protein/creatinine ratio.
r = Spearman’s correlation coefficient; significance level at <0.05.
Univariate and multivariate adjusted odds ratios of upper quartile urinary KIM-1/Cr (ng/mg).
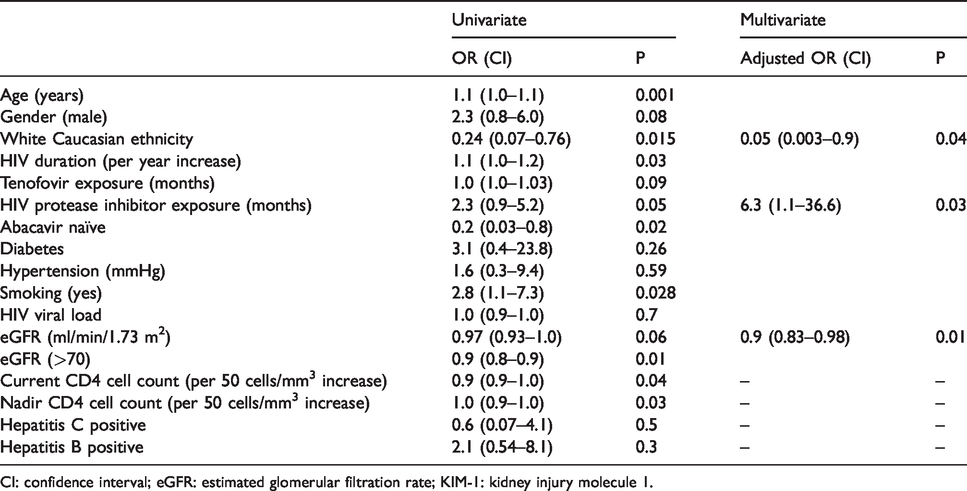
CI: confidence interval; eGFR: estimated glomerular filtration rate; KIM-1: kidney injury molecule 1.
Diagnostic value of unadjusted KIM-1/Cr
Supplementary material 2 gives a summary of predictive coefficients of unadjusted KIM-1/Cr. Notably, duration of TDF exposure (in months) and eGFR were significantly associated with unadjusted KIM-1/cr. The AUC-ROC for predicting significant urinary protein excretion based on plasma KIM-1/Cr concentration was 0.86 (95% CI: 0.81–0.90), and sensitivity and specificity of 94 and 60%, respectively (Figure 5).
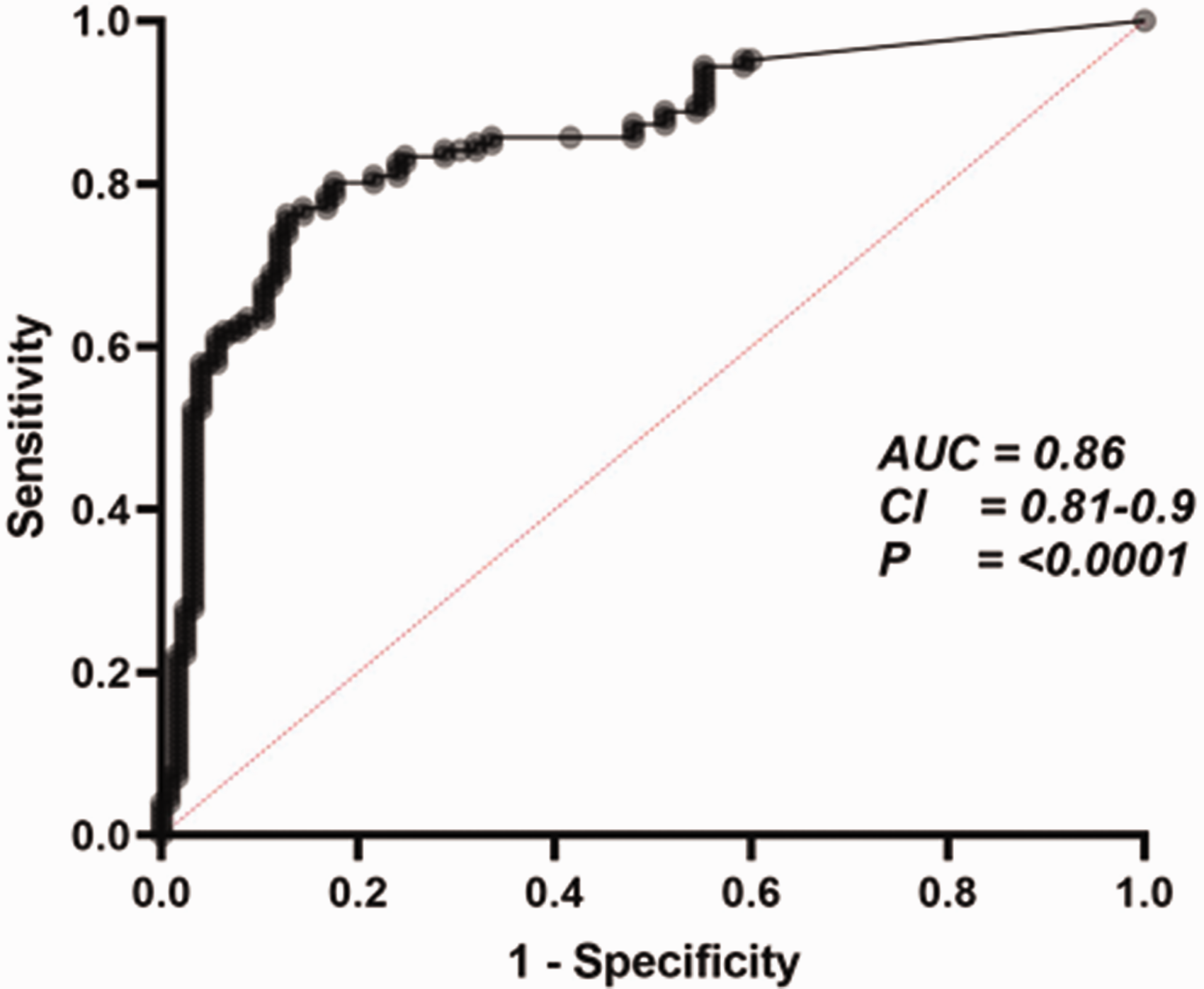
Diagnostic potential of KIM-1/Cr in HIV-positive patients on ART. Urinary KIM-1/Cr predicts the risk of kidney injury as defined by increased urinary protein expression (urine PCR). AUC 94% sensitivity at 60% specificity is given with statistical significance. AUC: area under the curve; CI: confidence interval.
Discussion
Traditional markers of kidney injury such as eGFR have increasingly been shown to report kidney impairment later than tubular proteinuria in PLWH exposed to ART drugs. 17 The increasing prevalence of ART-related drug-induced kidney morbidities meant that there is an urgent need for novel surrogate markers that report sub-clinical levels of kidney injury before routine kidney function tests (such as eGFR and urine ACR/PCR) become abnormal. Recently low molecular weight proteinuria such as retinol binding protein, 5 KIM-1,1,10,18 neutrophil gelatinase associated lipocalin (NGAL),15,19 fatty acid binding protein, 20 and other LMWPs have been proposed as reliable early markers of kidney injury in both PLWH on ART and the general population. 15 In this cross-sectional study, we have evaluated the association between traditional markers of kidney injury (such as eGFR and urine PCR) in PLWH on ART drugs with a novel marker KIM-1/Cr (adjusted for urinary creatinine excretion) that has increasingly been shown to report kidney tubular injury earlier in the general population. We observed higher median urinary KIM-1/Cr levels in these PLWH (3.7 ng/mg, IQR 1.5, 8.2) regardless of ART exposure compared with either healthy volunteers (0.097–0.39 ng/mg)1,10,21 or patients with acute kidney injury in the general population (0.57925 ng/mg, IQR 0.3997–0.82972). 21 The median KIM-1/Cr, for example, for ART-naïve PLWH in our study cohort was 5.1 ng/mg. Although the exact reason for this remains uncertain, it may suggest a degree of sub-clinical kidney injury in this cohort of patients with normal kidney function (eGFR ≥60 ml/min/1.73 m2). Several reasons may account for this. The natural history of HIV-related kidney involvement may be associated with up-regulation of KIM-1 synthesis in kidney tubular cells with resultant increased excretion of KIM-1 independent of exogenous injury (including ART drugs). This is supported by data from mechanistic studies that suggest tubular injury of diverse aetiologies resulting in up-regulation of this putative cell adhesion molecule (KIM-1). 10 Additionally, previous reports have shown that both glomeruli and distal convoluted tubules were early target sites for the HIV virus 9 further supporting the role of direct effect of the virus in up-regulating KIM-1 expression. Whilst the exact role of the natural history of HIV in KIM-1 kinetics remains a matter of pathogenetic debate, we hypothesise that it may (in common with other yet to be identified factors) account for its high baseline urinary excretion in PLWH either ART naïve or treatment experienced. Median KIM-1/Cr (ng/mg) levels were uniformly distributed across all classes of ART exposure. There was however a trend towards higher median levels in PLWH on TDF- and PI-based regimens. TDF22,23 and HIV PI5,24,25 exposures have both been independently associated with increased risk of KTD from various mechanistic and systematic studies. Higher median KIM-Cr values in these cohorts of patients may reflect its potential role both as a marker and predictor of adverse outcomes in patients on these treatment regimens, but this will need validation by more robust prospectively recruited patient cohorts.
We similarly found a high baseline KIM-1/Cr levels in patients of white Caucasian ethnicity compared to other cohorts. When stratified based on ART exposure, Caucasian patients maintained higher KIM-1/Cr values compared to other ethnic cohorts regardless of ART exposure. This will suggest an influence of ethnicity both in the expression and possibly increased excretion of KIM-1 from the kidneys. In the women's multi-agency study for example, black ethnicity was associated with significant albuminuria as well as an independent risk factor for increased excretion of tubular biomarker proteins including interleukin-8, NGAL, and α-1 microglobulin in patients on ART. 26 Additionally, McWilliam et al. 17 reporting in a paediatric population showed a higher urinary KIM-1 threshold in Caucasian patients compared with their black counterparts. A probable explanation for this observation might be the role of genetics in influencing the adverse effects of ART on the kidneys. TDF-induced KTD, for example, has a higher prevalence in white Caucasian males compared with other gender-matched ethnic cohorts.11,27,28 Although association between TDF exposure and risk of KTD remains speculative, recently both mechanistic and pharmacogenetic studies have increasingly implicated the role of single nucleotide polymorphisms (SNPs) of genes encoding proteins involved in the bio-disposition of TDF.29–33 It is probable that there might be an ethnic bias in the genes associated with synthesis and expression of KIM-1 on tubular cells. SNPs of these genes therefore account for either increased or decreased expression of this putative glycoprotein on kidney tubular cells.
We also observed a significant positive correlation between advancing age, white Caucasian ethnicity, and higher urine PCR levels with unadjusted KIM-1/Cr. In PLWH, higher urine PCR levels are associated with and utilised as a point-of-care marker of tubular dysfunction in those on ART.30–33 The positive correlation reported by our study supports a potential role of KIM-1/Cr as a reliable alternative marker of kidney dysfunction in this cohort of patients.
It is noteworthy that in our study urine KIM-1/Cr kinetics maintained an inverse relationship with eGFR. The latter is a well-established surrogate marker of kidney injury in both PLWH cohorts and the general population, with lower levels associated with worsening kidney impairment. This may additionally support a possible role for urinary KIM-1/Cr as a marker of kidney injury in PLWH exposed to ART drugs. Furthermore, we have shown that a significant number of patients in our study cohort with hitherto normal kidney function (eGFR >60 ml/min/1.73 m2) have both median and upper quartile KIM-1/Cr (ng/mg) values significantly above diagnostic thresholds for kidney injury in the general population. This may suggest some degree of sub-clinical kidney injury that has been masked or not reported by normal eGFR (≥60 ml/min/1.73 m2). The novelty of our approach is the identification of these patients with significant values of KIM-1/Cr (suggesting some degree of kidney impairment) even when eGFR in these patients was reported as normal.
Serum creatinine, eGFR, and thresholds of urine PCR have remained the main diagnostic markers for acute kidney injury both in the general population and PLWH. Despite this, unadjusted KIM-1/Cr (ng/mg) had a larger significant AUC (0.86 [Figure 5]) in our study. This may suggest a diagnostic role for KIM-/Cr in these patients, and perhaps its ability to identify kidney injury earlier in these cohorts of patients than traditional markers of kidney injury. Our finding of a protective effect following HIV PI exposure appears at variance with recent published reports in this area. Whilst no conclusive explanation could be advanced for this, it may have to do with the relatively small sample size of the study population. We know from recent studies that PIs such as darunavir have a more favourable kidney safety profile compared to lopinavir or atazanavir. 33
Admittedly, our study has several limitations including its relatively small sample size and cross-sectional design meant that direct causality could not be established based on our report. We therefore advise caution in interpretation and application of our findings without further validation.
Conclusion and future perspectives
In conclusion, we have demonstrated that unadjusted and upper tertile KIM-1/Cr (≥6.25 ng/mg) positively correlates with and predicts risk of kidney injury in HIV-positive patients on ART. PLWH regardless of ART drug exposure have urinary KIM-1/Cr values well above diagnostic thresholds for either normal volunteers or patients with AKI in the general population. This may suggest a probable role for KIM-1/Cr as an early diagnostic biomarker in PLWH.
Hypothesis
There has been increasing morbidity associated with ART drugs. Traditional markers of kidney injury such as eGFR have been shown to predominantly report glomerular injury and may not report early ART drug related kidney dysfunction. Novel markers such as KIM-1 have been proposed as reliable early markers of kidney injury in the general population. We hypothesise that thresholds of urinary KIM-1 normalised for urinary creatinine excretion are a reliable and effective early marker of kidney injury in PLWH exposed to ART drugs especially Tenofovir.
Supplemental Material
sj-pdf-1-std-10.1177_0956462420918515 - Supplemental material for The utility of kidney injury molecule-1 as an early biomarker of kidney injury in people living with HIV
Supplemental material, sj-pdf-1-std-10.1177_0956462420918515 for The utility of kidney injury molecule-1 as an early biomarker of kidney injury in people living with HIV by Mohammed I Danjuma, Shaikha Al Shokri, Nadia Bakhsh, Mohammed A Alamin, Mohamed GH Mohamedali and Igbiks Tamuno in International Journal of STD & AIDS
Footnotes
Acknowledgements
Dr Steve McWilliams assisted with urinary KIM-1 and urinary creatinine assay validation.
Authors’ contributions
MID was involved in study conceptualisation, study design, patient recruitment, data/statistical analyses, and manuscript writing. Additionally, MID was involved in study data preparation (including protocol development), ethics defence, study sample extraction, bio-analytical assays, and collation/preparation and cleaning of study data. IT was involved in study sample classification, data cleaning, sample analyses, and manuscript writing. NB and SNA were involved in study data cleaning, classification, and manuscript writing.
Availability of data and materials
The datasets used, analysed, and presented in this report are available from the corresponding author on request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study benefited from infrastructural funding from the MRC centre for Drug safety science. The publication of this article was funded by the Qatar National Library.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.