
Abstract
People living with HIV (PLWH) are more prone to severe respiratory infections. We used the severe acute respiratory infection (SARI) definition to describe the etiology, clinical, and epidemiological characteristics in this population. This was a prospective observational study including PLWH hospitalized with fever and cough. Those with symptom onset up to 10 days were classified as severe acute respiratory infection and 11–30 days as non-severe acute respiratory infection. Blood, urine samples and nasopharyngeal swabs were collected. Data were extracted from patient charts during their hospital stay. Forty-nine patients were included, median CD4 cell count: 80 cells/mm3, median time since HIV diagnosis and hospital admission: 84 months and 80% were antiretroviral therapy exposed. Twenty-seven patients were classified as SARI. Etiology was identified in 69%, 47% were polymicrobial. Respiratory virus (9 SARI vs. 13 non-SARI), bacteria (5 SARI vs. 4 non-SARI), Mycobacterium tuberculosis (6 SARI group vs. 7 non-SARI group), Pneumocystis jirovecii (4 SARI vs. 1 non-SARI), Cryptococcus neoformans (1 SARI vs. 3 non-SARI), and influenza A (1 SARI vs. 2 non-SARI). Dyspnea was statistically more prevalent in SARI (78% vs. 36%, p = 0.011) but the risk of death was higher in the non-SARI (4% vs. 36%, p = 0.0067). In the severely immunocompromised PLWH, severe acute respiratory infection can be caused by multiple pathogens and codetection is a common feature.
Background
People living with HIV (PLWH) are highly susceptible to respiratory infections. 1 Even in the antiretroviral therapy (ART) era, tuberculosis (TB) has fallen disproportionately among seropositive patients 2 and pneumonia remains five times more common among this population, despite achieving CD4 cell counts above 500 cells/mm3. 3 PLWH are also at increased risk for poor influenza outcomes, which may be particularly risky for those living in countries with limited resources.4–6
After the recent influenza A (H1N1, H5N1, and H7N9) and the Middle East Respiratory Virus (MERS-CoV) outbreaks, the WHO is encouraging and supporting countries to strengthen surveillance on severe acute respiratory infections (SARI) 7 but with limited information on PLWH regarding etiology and prognosis, despite their increased risk for respiratory infections and adverse outcomes.8–10 So, in this study, we described how SARI is represented, according to clinical presentation, epidemiology and etiology in a population of PLWH with respiratory infection residing in a high-prevalence TB area.
Patients and methods
Study design
A prospective observational study was conducted at the Instituto Nacional de Infectologia Evandro Chagas (INI-Fiocruz), Rio de Janeiro, Brazil, from May 2012 to December 2013. INI-Fiocruz is a national reference center for infectious diseases and has been a reference center for care, research, and training related to HIV/AIDS since 1986. The AIDS program at INI is one of the largest providers of primary, specialty, and tertiary care for PLWH patients in Rio de Janeiro State with a cohort of about 4000 patients in active follow-up.
Patients
We conducted surveillance of every HIV-positive patient hospitalized during the study period above. Every Monday, Wednesday, and Friday we carried out reviews of inpatient medical records and all PLWH hospitalized with respiratory symptoms were screened by the principal investigator, a physician specialized in infectious diseases. In the presence of fever and/or cough and onset of symptoms for less than 30 days, the patient was invited to participate in the study, which involved the collection of clinical material as detailed below in the sample collection and processing section. Patients were excluded if symptoms occurred more than 30 days ago or if no fever and/or no cough were reported by the patient. Patients were classified as SARI if the onset of symptoms was ≤10 days, according to WHO global standards for SARI definition. 7 Those with symptom onset greater than 10 days but up to 30 days prior were considered as non-SARI patients (Figure 1). Participants were screened by a physician regarding respiratory viral symptoms such as myalgia, diarrhea, arthralgia, coryza, and odynophagia. Data on dyspnea, respiratory frequency, and peripheral oxygen saturation (SpO2) using pulse oximetry were collected by a respiratory therapist. Patients were considered to have dyspnea if rated ≥5 on an ascending scale from 0 to 10.
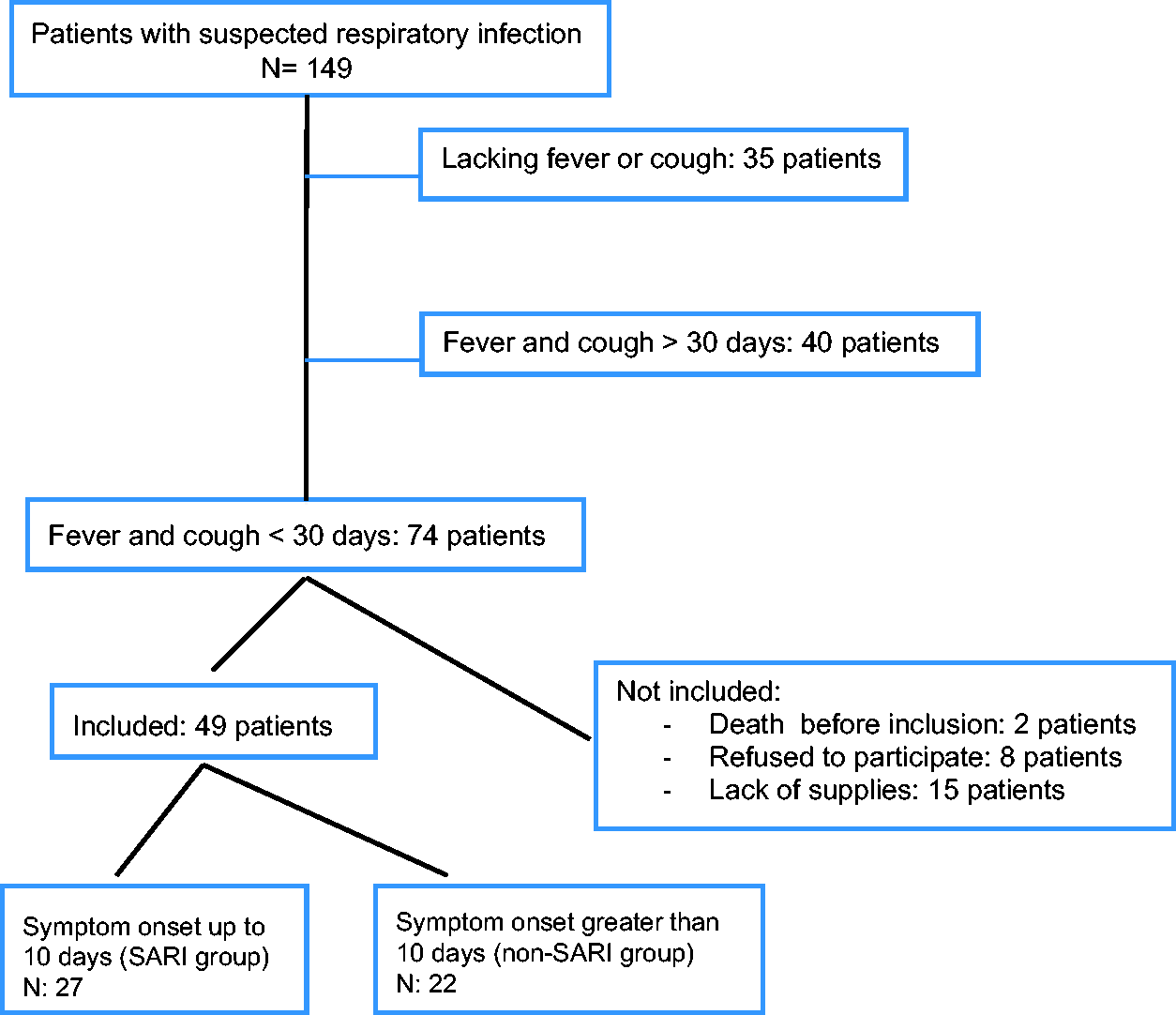
Flowchart of inclusion.
Data collection
Clinical and epidemiological data were collected during hospitalization using standardized forms, until hospital discharge or death (Table 1). Variables of interest were age, gender, time since HIV diagnosis based on the first HIV-positive result, CD4 nadir cell count, and CD4 cell count at hospital presentation or up to 2 months before, having had a previous TB diagnosis (pulmonary or disseminated) or any other previous opportunistic infection. Viral load was considered to be undetectable if less than 400 copies/mL, and we considered being ART exposed if patient ever used ART regardless of adherence. Prophylaxis of respiratory infection was recorded, such as Pneumocystis jirovecii pneumonia (PJP) prophylaxis and pneumococcal and influenza vaccines. Data about the respiratory infection included leucocyte count, C-reactive protein, pulse oximetry, and CRB-65 and the combined CRB-65 + O2 score at admission. Outcome variables of interest were: intensive care unit (ICU) admission, non-invasive ventilation use beginning within 72 h of hospital admission and death.
Clinical and epidemiological characteristics of patients with less than 10 days since symptom onset (SARI) vs patients with more than 10 days since symptom onset (non-SARI).
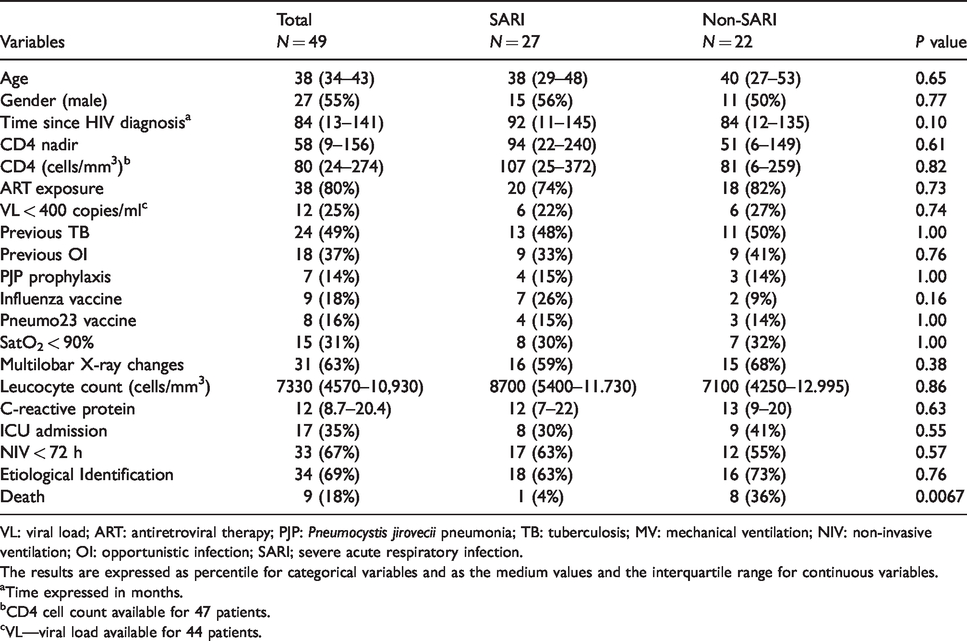
VL: viral load; ART: antiretroviral therapy; PJP: Pneumocystis jirovecii pneumonia; TB: tuberculosis; MV: mechanical ventilation; NIV: non-invasive ventilation; OI: opportunistic infection; SARI; severe acute respiratory infection.
The results are expressed as percentile for categorical variables and as the medium values and the interquartile range for continuous variables.
Time expressed in months.
CD4 cell count available for 47 patients.
VL—viral load available for 44 patients.
Microbiologically-confirmed pneumonia was defined as fever (axillary temperature) ≥38°C, (new) pulmonary infiltrate on chest X-ray or computed tomography scan plus an etiological agent identified through the tests mentioned below.
Sample collection and processing
For every patient included we collected blood cultures for bacteria, fungi, and mycobacteria processed with the automated BactAlert® system (Healthcare-bio Merieux), urine samples for urinary Streptococcus pneumoniae and Legionella pneumophila serogroup 1 testing (Binaxnow kit®) and triple respiratory swab (nasopharyngeal, one for each nostril and one for posterior pharynges). Respiratory swabs were tested for respiratory syncytial virus (RSV), adenovirus (Adeno), influenza A (FluA), parainfluenza 1–3 (PIV 1–3), human-metapneumovirus (HMPV), and rhinovirus (RV) using rt-PCR. Probes were labeled at the 5′ terminus with 6 carboxyfluorescein (FAM) and with quencher Blackhole-1 dT (Biosearch Technologies, Inc., Novato, CA).
The tests were done following Centers for Disease Control and Prevention (CDC) guidance. Sputum or induced sputum and bronchoalveolar fluid were tested for fungus and Mycobacterium spp. under direct visualization followed by inoculation into Sabouraud culture medium for fungi and BACTEC® MGIT™ 960 and Lowenstein–Jensen for mycobacterial culture. Mycobacterium spp. identification was performed under conventional techniques (Kent and Kubica, 1985, CDC Atlanta). All clinical samples were collected up to 72 h after hospital admission except for P. jirovecii detection which was done through staining and indirect immunofluorescence assay (IFL) on bronchoalveolar samples
Statistical analysis
We conducted a descriptive analysis of the convenience sample from the studied population. Categorical variables were presented as proportion and continuous variables summarized as median and interquartile ranges for SARI and non-SARI patients. We compared the distribution of continuous variables by using U or Mann–Whitney test, and categorical variables by using the Chi-squared or Fisher’s exact test when appropriate at univariate analysis. The analyses were processed using Statistical Package for Social Science (SPSS) and GraphPad Prism 3.0 for Windows (GraphPad Software, San Diego, CA, USA). Statistical significance was considered whenever p value was less than 0.05.
Results
A total of 149 patients were screened and 74 patients met our inclusion criteria. Among those, 8 patients refused to participate because of discomfort and pain during the nasal swab collection and 15 patients could not be included due to temporary lack of supplies. A total of 49 patients with fever and cough and symptoms lasting up to 30 days were included (Figure 1), of which 27 (55%) met the SARI case definition.
A profound and prolonged immunosuppression is reflected by the median nadir lymphocyte CD4 cell count (58 cells/mm3) and at hospital admission (80 cells/mm3) and time since HIV diagnosis with a median of 84 months, except for five patients with recent HIV diagnosis (in the previous three months). This finding is supported by the fact that 38 (80%) patients were ART exposed, but only 12 (25%) had an undetectable viral load. Prevention of respiratory infection was observed in only 7 (14%) patients taking prophylactic sulfamethozaxole–trimethoprim for PJP, 7 patients (14%) who previously received S. pneumoniae vaccine and 9 (18%) received influenza seasonal vaccine. About half of the patients had a previous history of TB and 18 (37%) had a history of other opportunistic infections.
Pneumonia was confirmed in 46 (94%) patients and 31 (63%) had X-rays with multilobar infiltrates. In the remaining three patients, the chest X-ray was normal and CT scan could not be done (data not shown). Pulse oximetry showed that 15 patients (30%) had SpO2 less than 90% and non-invasive ventilation was initiated in 67% of the patients in the first 72 h of admission. Twenty (41%) patients were classified as CRB-65 = 0 points, 19 patients classified as CRB-65 = 1 (39%) point, 9 (18%) as CRB-65 = 2 points and 1 as CRB-65 = 3 points. Although 39 patients had CRB-65 0–1, the majority required non-invasive ventilation (NIV) in the first 72 h of hospitalization and 25 had chest X-rays with multilobar infiltrates. The mortality risk for those 10 patients (20.4%) with CRB-65 2–3 points was 4.5 higher (95% confidence interval [CI]: 0.94–21.92) compared to CRB-65 0–1 points, p value = 0.069, with sensitivity (S) and specificity (Sp) of 85% and 44% and positive predictive value (PPV) and negative predictive value (NPV) of 87% and 40%, respectively. When combined with pulse oximetry, 15 patients (30.6%) had CRB65+O2 of 2–4 points and a 10.5 higher risk of dying (95% CI: 1.87–59.1), p value = 0.0051 with a S:75% and Sp:78% and PPV: 94% and NPV: 42% (data not shown). In total, nine patients (18.6%) died during hospitalization.
The median time between symptom onset and hospital admission was 10 days (6–20). According to SARI classification, we saw that clinical and epidemiological characteristics were evenly distributed with no statistical difference between SARI and non-SARI patients, except for mortality rate, which was significantly more prevalent among non-SARI patients (Table 1).
Symptoms according to SARI classification
Symptoms related to respiratory viral infection were analyzed among SARI and non-SARI patients (Figure 2). Fever and cough were present in 100% of cases because they were used as inclusion criteria. Dyspnea was the only symptom that was statistically more prevalent in the SARI subgroup, p = 0.011 (Figure 2). Arthralgia, conjunctivitis, odynophagia, and coryza were all infrequent in both subgroups.
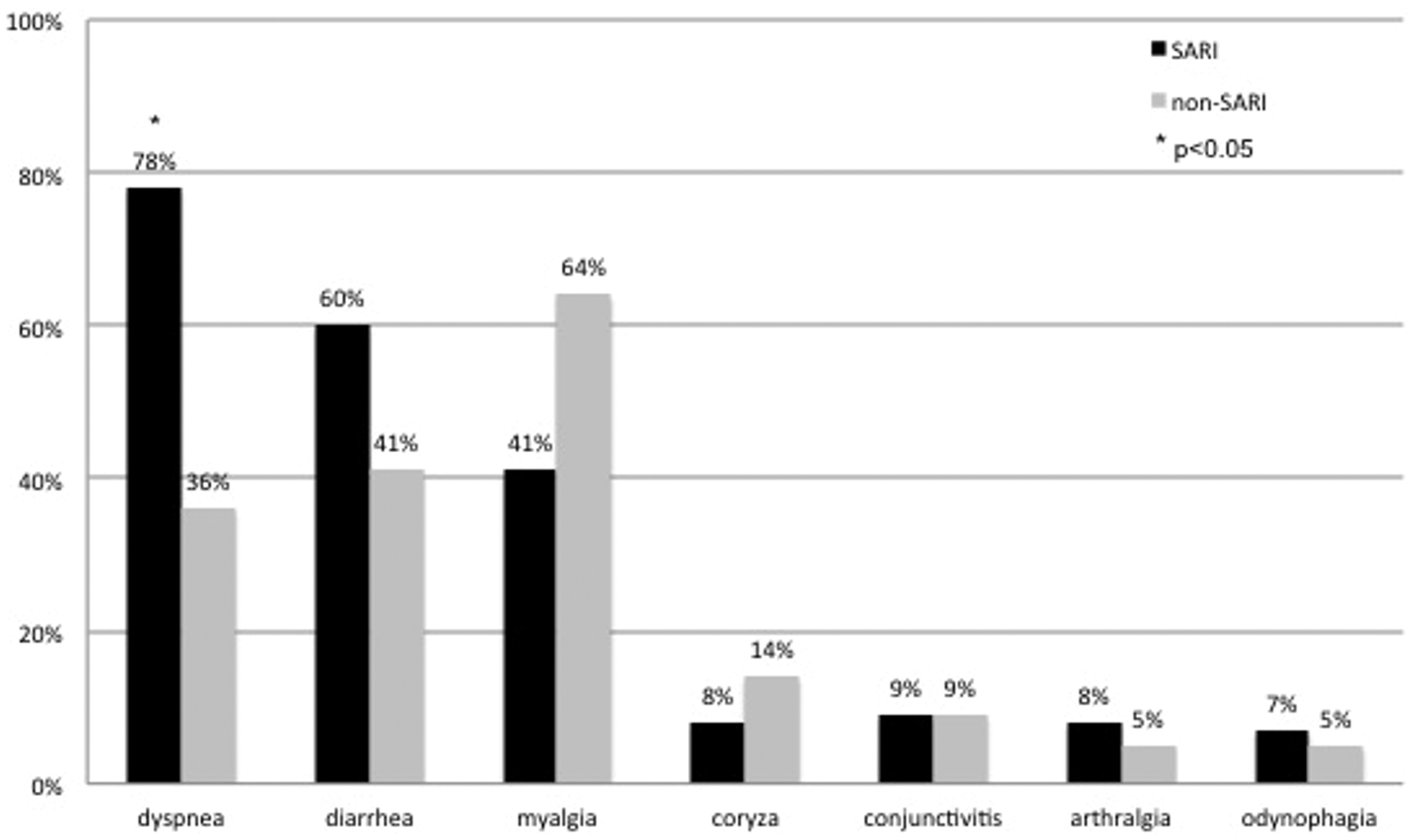
Symptoms (%) according to SARI and non-SARI classification.SARI: severe acute respiratory infection.
Etiology of respiratory infection according to SARI classification
Microbiological confirmation was possible in 34 (69%) patients and 16 (47%) patients had polymicrobial infections (Table 2). Viral pathogens were the most common agents, occurring in 17 (35%) patients with 22 isolates. RV was the most common virus among SARI (4; 15%) and non-SARI (7; 32%) patients, followed by RSV in (5; 10%); the majority (4/5) in the non-SARI group, influenza A in 3 (6%), HMPV in 2 (4%), and parainfluenza-2 in 1 (2%) patient. All three cases of influenza A happened in non-influenza-vaccinated patients, but since the vaccination was infrequent, we could not explore its impact. Influenza A(pdm09)H1N1 was confirmed in one patient classified as SARI, and the other two influenza viruses were identified among patients whose symptom onset was greater than 10 days ago, both seasonal AH3N2 strains. The two isolates of HMPV and the only PIV-2 were identified in patients with SARI.
Etiology and percentage of codetection with other pathogens among SARI and non-SARI patients.
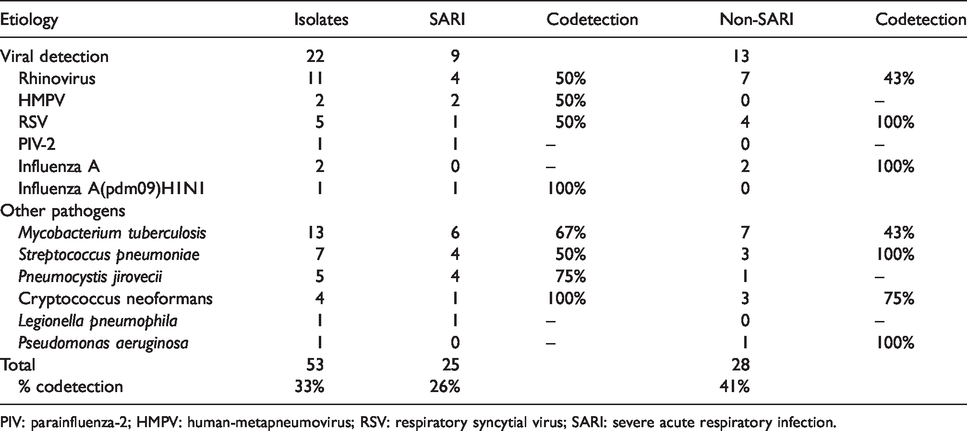
PIV: parainfluenza-2; HMPV: human-metapneumovirus; RSV: respiratory syncytial virus; SARI: severe acute respiratory infection.
Mycobacterium tuberculosis (Mtb) was the most common bacterial pathogen identified in 13 (27%) patients (Table 2). Among the 24 patients (49%) who had been previously diagnosed with TB, 8/24 (33%) were readmitted with Mtb infection the majority in the non-SARI group (7/8 patients, 88%).
S. pneumoniae was evenly distributed among SARI (four isolates) and non-SARI (three isolates), but PJP was more frequent in the SARI group, while Cryptococcus neoformans was more common in the non-SARI group (Table 2).
Among polymicrobial infections, 13 patients had 2 pathogens and 3 patients had 3 or more pathogens identified. Polymicrobial infection was more frequent in the non-SARI group, 9 (41%) vs. 7 (26%), but with no statistical difference. No single agent was significantly more prevalent according to this classification.
The main agents associated with severity and ICU admission were PJP in 80% (4/5); Cryptococcus neoformans in 75% (3/4), S. pneumoniae in 43% (3/7), and Pseudomonas aeruginosa in 100% (1/1) of the cases. Infections were polymicrobial in 41% vs. 30% of the patients being admitted to the ICU (p = 0.52) and in 44% of the patients who died vs. 25% among survivors (p = 0.25).
Discussion
We found that PLWH hospitalized with fever and cough, with less than 30 days of symptoms were mostly young, with severe and prolonged immunosuppressed caused by HIV infection. There were no clinical or epidemiological aspects that could distinguish the classification of SARI and non-SARI. In terms of etiology, SARI was represented by a broad range of infectious agents in this population and much of the lung infections were polymicrobial. In one-third of the cases, we found viruses in nasopharyngeal samples and two out of three influenza viruses were detected in non-SARI patients.
Our findings highlight the importance of viral pathogens in community-acquired respiratory infections: viruses were implicated in 35% of respiratory symptoms in PLWH and RV was the most common one. This may be due to the fact that the RV is present throughout the year regardless of specific seasonality.11,12 Although being historically related to the common cold and to mild respiratory illness,13–15 recent data suggest that RV can be related to more severe cases. 16 According to Cohen et al. it was the principal agent of SARI during a hospital surveillance period 2009–2012 in South Africa, where 74% were PLWH 9 and also an important agent in elderly hospitalized with SARI in Chile 17 as well as the causal agent of more severe cases requiring ICU treatment, in co-detection with S. pneumoniae. 18 Most of our cases were found in co-detection with another agent suggesting that RV may contribute to more severe cases but the possibility of only being a bystander cannot be rule out in this context. In accordance to our findings, HMPV remains an infrequent cause of SARI even in PLWH. 19
Apart from viral detection, S. pneumoniae is reemphasized as the main bacterial pathogen found in patients with CAP who presented with SARI, regardless of the CD4 lymphocyte count as shown by López-Aldeguer et al. 20 Another important aspect of our study was the fact this pyogenic bacterium was found in patients with late onset of symptoms (non-SARI) and three out of seven patients presented with bacteremia and all three of them died, a feature often correlated with poor prognosis. 21 L. pneumophila remains an uncommon cause of community-acquired lung infection but we acknowledge that some cases might have been missed since the urinary antigen test can only detect type 1 infections and up to 14 days of onset.20,22
We found a high frequency of Mtb in patients with few days of symptoms and in a population with a previous history of pulmonary or disseminated TB, suggesting that prolonged immunosuppression may reactivate the bacillus.22–24 Our findings are in agreement with Coelho et al. who showed that TB was the most common opportunistic infection in the total cohort followed at our center. In high TB prevalence settings, such as the one observed in our context, this diagnosis should be pursued in PLWH regardless of symptom duration. 25
Another important aspect of our findings was to emphasize the polymicrobial aspect of respiratory infections in this population. Co-detection of multiple pathogens can occur in the context of HIV infection20,25,26 but also in the general adult population as recently demonstrated by Karhu et al. (39% of severe acquired pneumonia patients) and in children with SARI.26–28
In our sample, coinfection could be associated with death (44% vs. 25%, p = 0.25) but did not reach statistical significance, probably due to the small sample size.
Whether the presence of multiple pathogens leads to a more severe presentation with increased risk of poor outcomes is still unclear. 29 When looking at coinfection involving bacteria plus a respiratory virus, mortality seems to be higher in the bacterial coinfection subgroup,30,31 as shown by Walaza et al. with TB and influenza and by Crotty et al. in pneumonia patients.32,33 But these findings may not be applied to viral–viral coinfection. 34
Since SARI and non-SARI were similar according to clinical and epidemiological aspects, the delay between symptom onset and the demand for care (non-SARI group) could have contributed to the higher mortality observed in our findings, as shown previously by several authors.6,35,36 Although 39 patients had CRB-65 of 0–1 points and could have been sent home with oral antibiotic therapy, the majority required NIV in the first 72 h of hospital admission and 63% had X-rays with multilobar infiltrates, another predictor of unfavorable prognosis. Similar findings were found by Almeida et al. in 49 PLWH admitted with pneumonia in an emergency department with a median CRB65 score lower then HIV-negative patients but which were also associated with a higher risk of mortality. 37 In the paper of Yone et al., 54 out 62 PLWH admitted with community acquired pneumonia (CAP) had CRB65 of 0–1.38 In our study, adding the pulse oximetry to CRB-65 score, as suggested by the Consensur II, the Latin America Pneumonia working Group, increased the ability to confidently predict the 30-day in-hospital mortality. 39
In the context of SARI surveillance target at influenza, a possible explanation for our late detection relies on the fact that immunosuppressed and critically ill patients there seems to be prolonged viral shedding. 40 The median CD4 cell count in this study population was 80 (24–274) cells/mm3 and the proportion of patients with undetectable viral load was 25% despite 80% being exposed to ART. Compared to the whole cohort followed at our center for the period 2012–2013, where 69.5% were male and the median age was 42.5 years, the median CD4 cell count was higher (542 cells/mm3), and so was the proportion who had undetectable HIV viral load (69.5%) and ever being exposed to ART (90.8%). 41 This shows that the population in this study is severely immunocompromised and found it harder to adhere to ART at the time. We observed two cases of influenza in the non-SARI group, respectively 20 and 30 days after symptom onset, and both patients developed respiratory failure that led to death (data not shown). This highlights the fact that immunosuppressed PLWH with respiratory symptoms may not seek hospital attention in time to be captured by SARI surveillance.
Finally, regarding symptom frequency, we found a low percentage of sore throat, runny nose and conjunctivitis and a high percentage of dyspnea, diarrhea, and myalgia. In fact, dyspnea was the only symptom more prevalent in the SARI group (p < 0.05). Although gastrointestinal involvement may have been influenced by the advanced immunodeficiency syndrome, other authors studying the symptoms of influenza in less-immunocompromised PLWH reached similar results.42,43 It is important to note that our study tried to address viral symptoms in a context of multiple pathogens. On one hand, it is difficult to assign a symptom to a specific virus or bacteria but on the other hand, it may reflect what actually happens in clinical practice, because as already highlighted above, a significant percentage of respiratory infections, especially in PLWH are of mixed type.
Our study has limitations. The small sample size conducted at a single center does not allow generalization of the results and the detection of respiratory viruses from the lower respiratory tract would have been more representative of the etiology of respiratory infection. Patients with advanced HIV infection may have multiple infections at the same time and an overlap of signs and symptoms is frequent, so the need for hospitalization may not be attributed exclusively to the respiratory infection per se. All cases in this study occurred in a 19-month period at a single institution, and viral epidemiology at this site and during this timeframe may not be representative of all seasons and locations. Finally, due to the constraints of the respiratory viral kit used, we may not have identified all possible and important viral infections such as adenovirus, coronavirus and bocavirus and PCR technique may detect a virus that is representative of several conditions such as the true agent itself, a bystander or facilitating bacterial superinfection. 44
Conclusion
In severely immunocompromised PLWH, SARI can be represented by a wide variety of respiratory pathogens and the codetection of multiple pathogens is common. Viruses must be considered as a common cause of respiratory infection either alone or in combination with other pathogens and in scenarios where TB is endemic, this agent should be pursued regardless of cough duration.
Footnotes
Acknowledgments
We thank Rogerio Valls and Jorge Salluh for their valuable suggestions during the study period.
Authors’ contribution
ACP collected data, performed the analysis, interpreted results, and wrote the manuscript. RTA contributed to data management, performed the analysis and drafting the figures and tables. FAB and AJ participated in the conception of this study and revised the manuscript. AJ and JCN participated in the interpretation of the results and writing. MS and MLO processed the respiratory samples. DCM participated in the data collection. All authors read and approved the final manuscript.
Availability of data and materials
De-identified data and materials are available on a case-by-case basis. Please contact the corresponding author with requests.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all patients prior to any study-related procedure. The National Institute of Infectious Diseases Review Board approved study protocol (INI, CAAE 0014.0.009.000–08). Participants who refused to participate or were excluded by exclusion criteria were not harmed by not participating in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.