
Abstract
Unprotected sex, common among people who inject drugs, puts them and their partners at risk of sexually transmitted infections including human immunodeficiency virus (HIV). This analysis assesses the changes in sexual risk behavior with regular female partners (RFPs), among married men who inject drugs, before and after implementation of a HIV prevention intervention, and identifies correlates of unprotected sex. People who inject drugs (PWID) were assessed at three points: baseline, preintervention follow-up visit (FV)1, and postintervention FV2. Descriptive analysis was used for reporting changes in sexual behavior over time. Generalized estimating equation assessed the population-averaged change in self-reported unprotected sex with an RFP, attributable to intervention uptake. Multivariable logistic regression determined correlates of self-reported unprotected sex with an RFP at FV2. Findings suggest that the proportion of men reporting any unprotected sex remained high (baseline = 46.0%, FV1 = 43.5%, FV2 = 37.0%). A reduction was observed in unprotected sex after the intervention phase, but this could not be attributed to uptake of the intervention. Higher odds of self-reported unprotected sex with an RFP in the past three months at FV2 were associated with self-reported unprotected sex at baseline, living with family, and being HIV-negative. Married male PWID should receive counseling for safe sex with RFPs, especially those who are HIV-negative and live with their families.
Background
People who inject drugs (PWID) constitute a high-risk population at risk of contracting and transmitting human immunodeficiency virus (HIV) and other infectious diseases. 1 Globally, HIV prevalence among PWID is 28 times higher than among the rest of the adult population. 2 In India, there are an estimated 177,000 PWID 3 with an HIV prevalence of 6.3%. 4 While sharing of injection paraphernalia is a key risk factor for HIV among them, 5 it can be significantly reduced with increased availability of sterile injecting equipment and prevention interventions. However, unsafe sexual behaviors among PWID have been difficult to change. 6
Multiple studies have also shown relatively high prevalence of non-HIV sexually transmitted infections (STIs) among PWID, suggesting risky sexual behaviors. Uusküla et al. 7 in their study in Estonia reported more than a fifth of PWID to be positive for hepatitis B surface antigen, while in India, Saraswati et al. 8 reported 9.2% hepatitis B positivity. Ghosh et al. 9 highlighted high prevalence of other STIs such as human papillomavirus and coexisting STIs such as herpes simplex virus (type 2) and syphilis among them. Moderate prevalence of syphilis sero-positivity has also been reported among PWID in Estonia – 2.9%, 7 China – 5.4%, 10 Russia – 8–20%, 11 and India – 12.9%. 12
Globally, it has been documented that sexually-active male PWID often have non-injecting sex partners.13–16 The onward transmission of HIV and non-HIV STIs to female sex partners is facilitated by high rates of unprotected sex among PWID,14,17 especially with exclusive main partners.15,18 Niccolai et al. 19 reported high prevalence of unprotected intercourse at last sex (60%) and high HIV prevalence (15%) among non-drug-using sex partners of PWID. Similar high HIV prevalence among female partners has been reported in Kazakhstan (10.4%) and Vietnam (11.5%).20–22 In India, as per the National Integrated Biological and Behavioral Surveillance (IBBS), more than 40% of male PWID reported being married. Studies from Chennai and Manipur reported 5 and 45% HIV-positivity among female sex partners of male PWID, respectively.23,24 Thus, spouses of men who inject drugs represent a group of married monogamous women who are at higher risk for HIV and other infections due to their husband’s risk behaviors. 25
A few studies in the United States and Russia have explored correlates of unsafe sex among PWID. Unsafe injection practices, low self-efficacy for sexual risk reduction, and frequent interaction with the sex partner were independent predictors of inconsistent condom use.6,26,27 Further, sexual behavior in intimate partnerships such as marriage is influenced by additional factors such as intention to conceive, mutual trust, and desire for intimacy.28,29 Therefore, determinants of unprotected sex with regular female partners (RFPs) are more complex, but have largely remained unexplored for this high-risk population group.
In India, evidence indicates an increase in HIV prevalence in PWID in newer geographies such as Delhi which has an estimated population of 17,000 PWID 30 with HIV prevalence of 16.2%. 4 This analysis aims to describe the sexual behavior of PWID with their RFP before and after the introduction of select HIV prevention and care interventions – facility-based HIV counseling and testing, HIV prevention counseling by outreach workers (ORWs), and needle syringe programs – in Delhi. Correlates of unprotected sexual behavior with RFPs in the post-intervention phase are also assessed.
Methods
The Population Council initiated a prospective cohort study at five drop-in centers in Delhi, to examine HIV incidence and behavior change among PWID before and after provision of internationally recommended HIV prevention interventions. 31 Before the study initiation, ORWs undertook a mapping exercise to identify hotspots and estimate the number of PWID who could be contacted at each hotspot. Study sites, were thus set-up near hotspots with high estimates of PWID in central, east, north-east, and north-west districts of Delhi. Study methods have been described elsewhere, 32 but briefly, participants were recruited through peer referral, targeted outreach by ORWs, and self-referrals. The study entailed three rounds of data collection: baseline, a preintervention follow-up visit after six months (FV1), and a postintervention follow-up visit (FV2) 12 months after FV1. At baseline, participants were tested for HIV, followed by repeat HIV testing at FV1 and FV2, if they were HIV-negative at the previous study visit. No HIV prevention interventions were provided during the observational control phase (baseline to FV1). However, PWID could still receive abscess care, outpatient medical consultations for common conditions, bathing facilities, and midday meals at drop-in centers, all of which continued through the intervention phase (FV1 to FV2).
Intervention
Returning participants who completed FV1 data collection received the internationally recommended HIV prevention and care intervention through the project. 31 These interventions included individual/group counseling sessions, needle syringe program, condoms, hepatitis B and C testing, counseling for STI prevention, STI screening, and symptomatic treatment. Referrals were also provided for opioid substitution therapy, deaddiction, and detoxification services. Access to project-related interventions ended after participants completed their last round of data collection (FV2). Throughout the study period, participants were free to access services available at government healthcare facilities or other community-based drop-in centers.
Study participants and procedures
To be eligible for study participation, participants had to be at least 18 years of age, must have injected drugs at least once in the last three months, and lived in Delhi at the time of study enrollment. For this analysis, male participants who reported being married or cohabiting (had an RFP – spouse or live-in partner) and returned for their postintervention FV2 were included. The study questionnaire was pilot tested for clarity of language, comprehension, content, and cultural sensitivity and was administered in Hindi. Face-to-face interviews were conducted by trained research interviewers conversant with quantitative data collection methods. All participants provided written informed consent for participating in the bio-behavioral survey and collection of blood samples. The HIV tests used for the study have been described in detail elsewhere. 8 Participants received INR 40 (approximately 80 USD cents) for participating in the behavioral survey at each round.
Study measures
Unprotected sex – the primary outcome variable was defined as self-reported sexual intercourse with no or inconsistent condom use, i.e. participants did not use condoms at all sexual encounters. Conversely, protected sex was defined as self-reported sexual intercourse with condom use at all sexual encounters. Participants who reported to be cohabiting were considered married for this analysis.
To evaluate the effect of the study intervention on change in sexual behavior, three key project interventions were considered – facility-based HIV counseling and testing, HIV prevention counseling by ORWs, and needle syringe services. These interventions were included as they promote safe behaviors - by providing free condoms and counseling about their correct and consistent use to prevent HIV and non-HIV STIs among PWID and further onward transmission to their sex partners. Also, studies have shown positive association between unsafe injecting and unsafe sexual behavior and hence access to needle syringe services was selected. 14
Data management and statistical analysis
All study related data were stored in password-protected computers and were accessible only to the project team. Analyses were done using STATA version 12.0 (College Station, TX, USA). Descriptive analysis described change in sexual behavior over three time points. To assess the population-averaged change in unprotected sex with RFPs from the control phase (baseline to FV1) to the intervention phase (FV1 to FV2), a generalized estimating equation (GEE) modeling approach was used. Subsequently, an interaction term was introduced to assess the impact of uptake of select interventions on unprotected sex with an RFP. Final models were adjusted for baseline covariates including age, education, recruitment method, and risky injection behavior index at FV2. Logistic regression, using a priori selected variables with potential effect on sexual behavior, and those which were significantly associated on the bivariate analysis, were used to determine correlates of unprotected sex with RFPs at FV2.
The study was approved by the Technical Resource Group and Ethics Committee of National AIDS Control Organization (NACO) in Delhi, the Research Ethics Committee of PATH, USA and the Institutional Review Board of the Population Council, USA.
Results
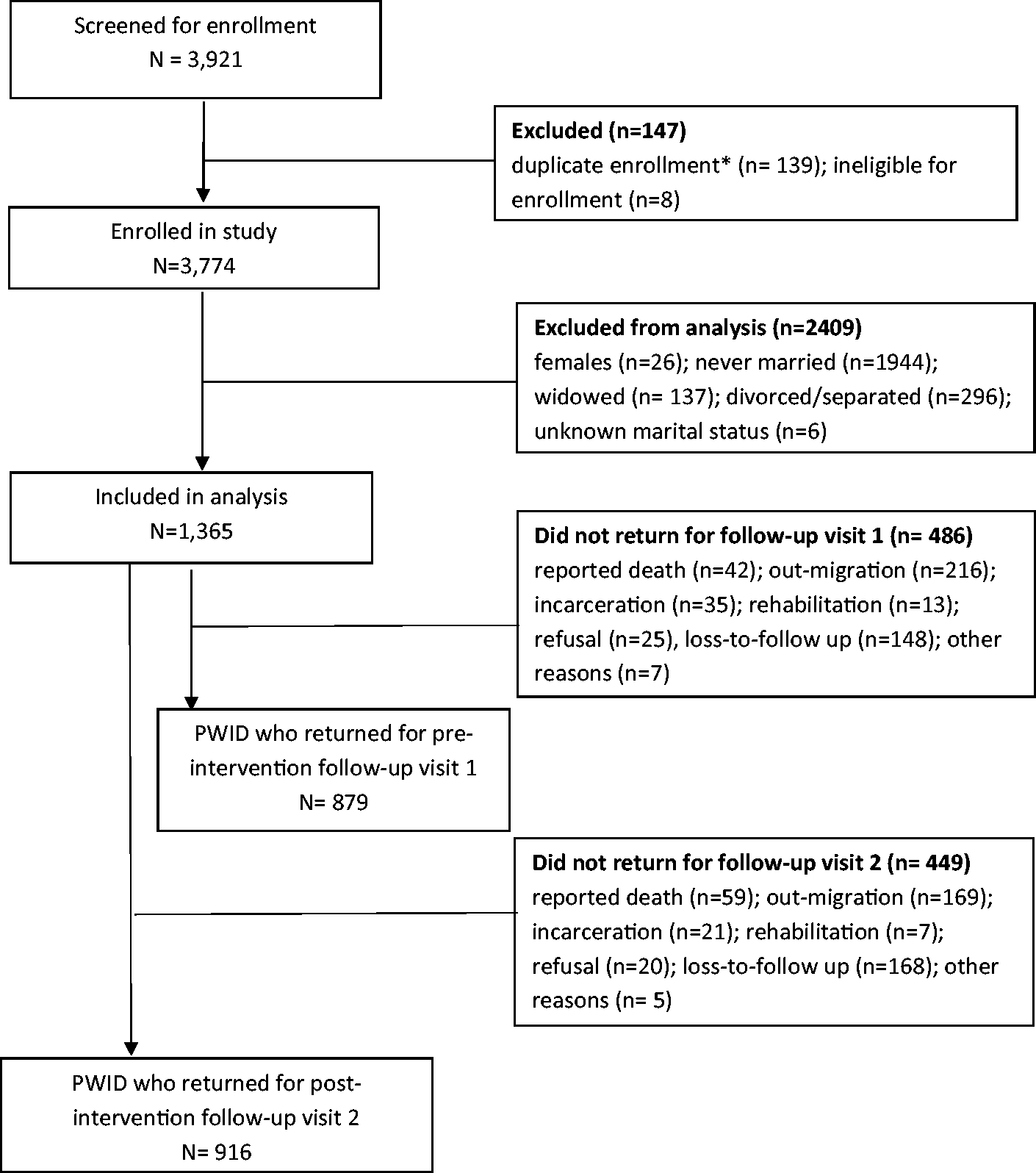
Among 3921 PWID enrolled in the study, 147 were excluded because of duplicate enrollment or ineligibility to participate (Figure 1). A total of 1365 male participants reported being married at baseline, and of them 916 (67.1%) returned for data collection at the postintervention FV2. Of those who returned at FV2, 879 (96.0%) had returned for data collection at FV1.
Two-year follow-up data of married male participants in the study cohort.
Among participants enrolled in the study, those who returned for the post-intervention FV2 visit, were more likely to be less educated (illiteracy 47.4% versus 43.4%; p = 0.002) and more likely to originate from Delhi (24.9% versus 17.0%; p = 0.002) compared to those who did not return for FV2 (Table 1). The two groups did not differ with respect to age, employment, HIV-positivity, injection practices, and sexual activity with women.
Comparison of sociodemographic and behavioral characteristics of married male PWID who returned and those who did not return at postintervention follow-up visit 2 (FV2).
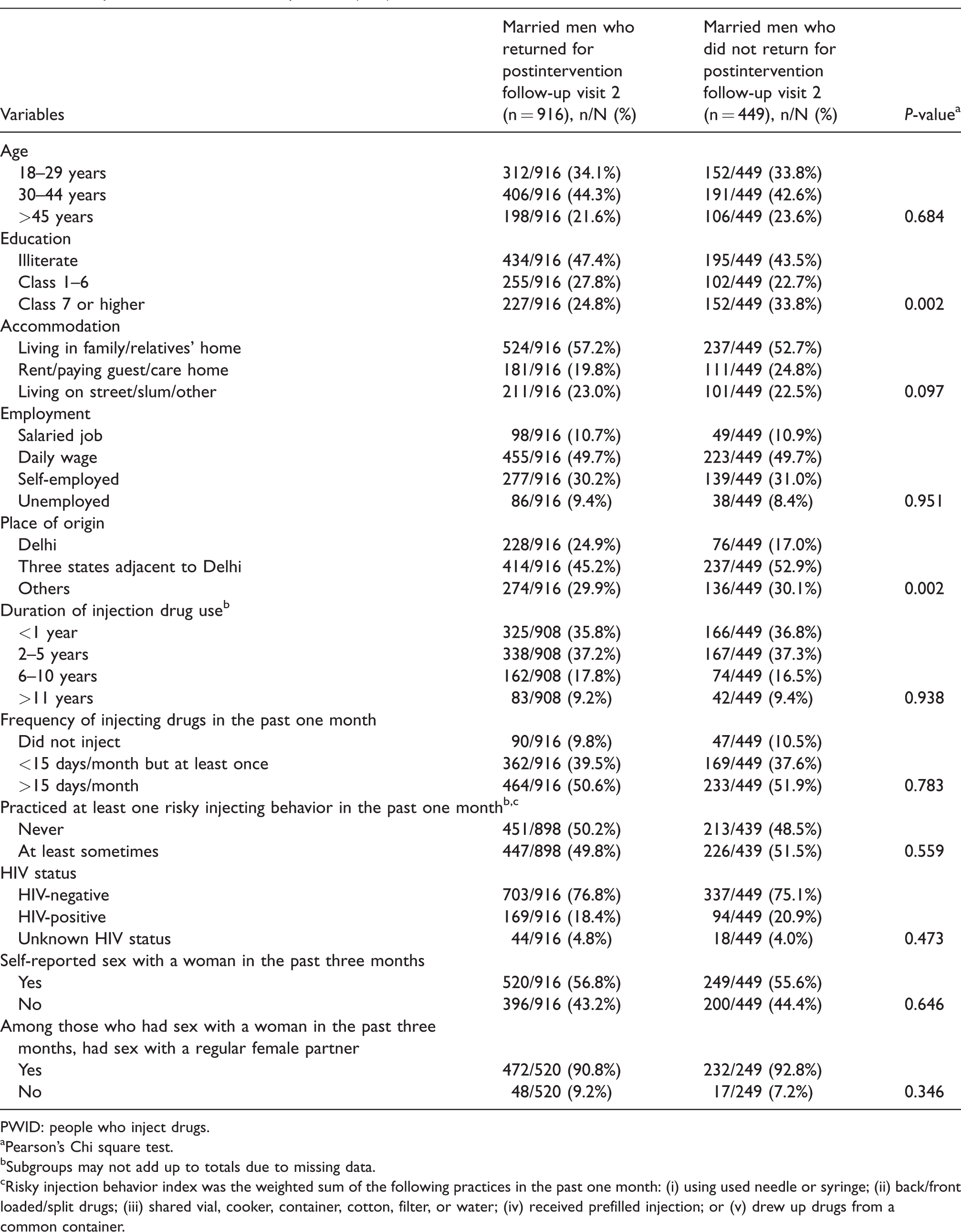
PWID: people who inject drugs.
aPearson’s Chi square test.
bSubgroups may not add up to totals due to missing data.
cRisky injection behavior index was the weighted sum of the following practices in the past one month: (i) using used needle or syringe; (ii) back/front loaded/split drugs; (iii) shared vial, cooker, container, cotton, filter, or water; (iv) received prefilled injection; or (v) drew up drugs from a common container.
Of 916 married men who returned for FV2, more than a third were aged <30 years (34.1%), and almost one-half were illiterate (47.4%). Steady means of income was infrequent as one-half (49.7%) were daily wage earners. Nearly one-half injected drugs on >15 days a month and a similar proportion reported risky injecting behaviors in the past one month. HIV prevalence was high at 18.4%. Self-reported sexual intercourse with a woman was low, as 43.2% did not have sex with any woman in the past three months.
Sexual behavior during study follow-up
About half of the married men reported to be sexually active with any female partner in the past three months – baseline (55.6%), FV1 (57.7%), and FV2 (52.1%; Table 2). Anal sex with female partners was reported by about 7–9% of PWID at each time point. Sex with male partners in the past three months was reported by 7.1, 2.7, and 6.2% of participants at baseline, FV1, and FV2, respectively (data not shown).
Sexual behavior at three time points among 916 married male PWID who returned for postintervention follow-up visit 2 (FV2).
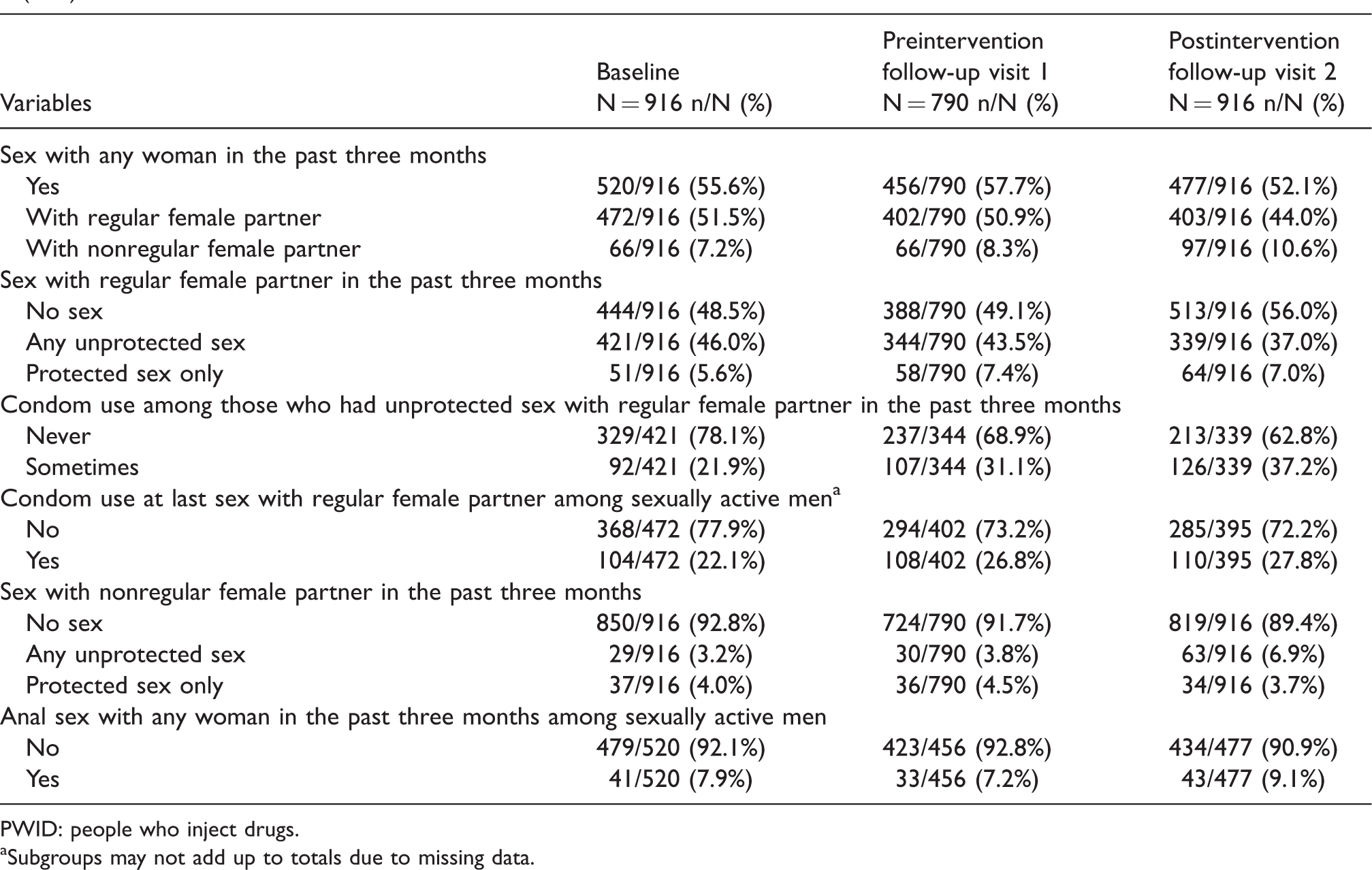
PWID: people who inject drugs.
aSubgroups may not add up to totals due to missing data.
Correlates of self-reported unprotected sex with regular female partners in the past three months among 916 married male PWID at postintervention follow-up visit 2 (FV2) (n = 916).
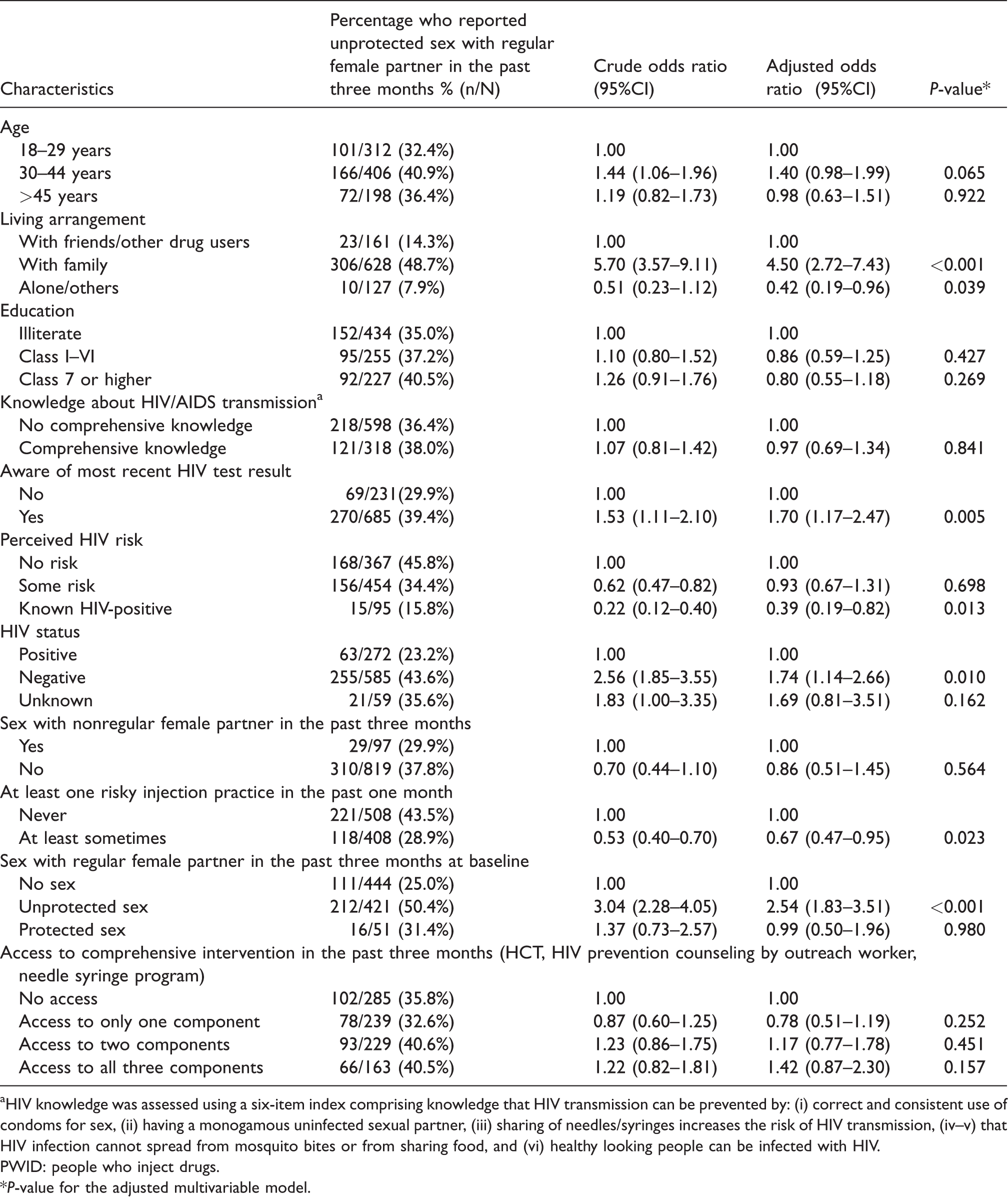
aHIV knowledge was assessed using a six-item index comprising knowledge that HIV transmission can be prevented by: (i) correct and consistent use of condoms for sex, (ii) having a monogamous uninfected sexual partner, (iii) sharing of needles/syringes increases the risk of HIV transmission, (iv–v) that HIV infection cannot spread from mosquito bites or from sharing food, and (vi) healthy looking people can be infected with HIV.
PWID: people who inject drugs.
*P-value for the adjusted multivariable model.
The proportion of men who reported sexual activity with an RFP in the past three months decreased over the study period: 51.5% (baseline), 50.9% (FV1), and 44.0% (FV2) (Table 2).
Change in unprotected sex with an RFP during intervention phase
Self-reported unprotected sex with an RFP in the past three months remained high throughout all three study visits: 46.0% (baseline), 43.5% (FV1), and 37.0% (FV2). Overall, unprotected sex with an RFP decreased over the study period – by 2.5% during the control phase (baseline to FV1), and by 6.5% during the intervention phase (FV1 to FV2). After controlling for age, education, recruitment, and risky injection behavior index, a 13% reduction in odds of unprotected sex with RFPs was observed during the intervention phase compared to the control phase, though this was not statistically significant (GEE adjusted odds ratio (AOR)=0.87; 95% confidence interval (95%CI) =0.66–1.14; p = 0.310; data not shown). On further exploration, those who reported uptake of any select intervention were more likely to have unprotected sex with an RFP (GEE AOR = 1.20; 95%CI = 0.87–1.66; p = 0.261) compared to those who did not access any intervention, and therefore the additional reduction in unprotected sex with RFPs may not be attributed to the self-reported uptake of the select study interventions (data not shown).
However, among men who practiced unprotected sex with their RFP, a consistent reduction was observed in the proportion of men who never used condoms with their RFP: 78.1% (baseline), 68.9% (FV1), and 62.8% (FV2).
Correlates of unprotected sex at postintervention follow-up
In multivariable analysis, factors independently associated with unprotected sex at FV2 were living with their family (AOR = 4.50; 95%CI = 2.72–7.43), awareness of their most recent HIV test result (AOR = 1.70; 95% CI = 1.17–2.47), HIV-negative status (AOR = 1.74; 95%CI = 1.14–2.66), and unprotected sex with an RFP at baseline (AOR = 2.54; 95%CI = 1.83–3.51). Alternatively, risky injection practices in the past month had a protective effect on unprotected sex compared to those who reported no risky injection behavior (AOR = 0.67; 95%CI = 0.47–0.95). Access to select study interventions was not significantly associated with unprotected sex with RFPs (see Table 3).
Discussion
To the best of our knowledge, this is the first study in India to assess change in sexual behavior of men who inject drugs with their RFP, before and after the introduction of select HIV prevention interventions. Additionally, an understanding of the correlates of unprotected sex among male PWID may provide guidance for designing future interventions to prevent onward infection transmission to RFPs.
Despite being married, male PWID reported low sexual activity as only about one-half of them reported sex with any woman across the study period. Grover et al. 33 reported an adverse effect of drug use on the endocrine system and higher rates of sexual dysfunction (low sexual desire, inhibited orgasm, painful sex, and inhibited sexual excitement) with heroin addiction (34–85%), Methadone Maintenance Treatment (14–81%), or Buprenorphine Maintenance Treatment (36–83%) compared to the general population. 34 Project staff (some of who were former drug users) also mentioned that PWID are either preoccupied with arranging for drugs or are under heavy influence of drugs, both of which makes them unavailable for sexual intercourse. Poor hygiene due to preoccupation with drug use further deters them from making any sexual contact.
Although consistent condom use with RFPs did not improve over time, an overall reduction in those who never used condoms with RFPs was observed. It may be that participants attempted behavior change by using condoms on certain occasions but could not sustain this safe behavior. Furthermore, it is possible that RFPs may have had an increased exposure to healthcare services, which may have altered certain behaviors and consequently resulted in a reduction in unprotected sex during the intervention period. Other reasons, besides chance, could be the Hawthorne effect, wherein individuals modify an aspect of their behavior in response to their awareness of being observed. McCambridge et al. 35 reported that answering questions on drinking in brief intervention trials appeared to alter subsequent self-reported behavior and found these findings to be relevant to evaluations of any interventions to change behaviors which involve participant self-report.
The National IBBS data for India shows high prevalence of unprotected sex among PWID as less than one-fifth reported consistent condom use with their RFPs in past 12 months; although it was relatively higher for Delhi at 23%. 22 We report similar findings as over a third of PWID reported any unprotected sex with their RFP in the past three months. The GEE analysis showed a trend towards lower odds of unprotected sex with RFPs at the population level during the intervention phase, though this was not statistically significant. Also, further exploration of the association showed that uptake of select study interventions was not associated with lower odds of unprotected sex. It is possible that the services were accessed by participants who intended to practice safe behavior i.e. consistent condom use but could not execute the desired behavior change as it may have been more difficult than anticipated. Further, the extent to which the actions required for behavior change have been deliberated also determine the actual change of behavior. 36 There are other potential reasons why uptake of the interventions did not reduce unprotected sex with RFPs – first, HIV prevention counseling for PWID is mostly targeted toward encouraging safer injection practices as it is their most critical HIV risk. Second, sexual risk behavior counseling often emphasizes condom use with non-RFPs such as paid sex workers who have high STI rates (including HIV), and less often addresses how to stay safe within steady relationships. In India, women involved in steady relationships with men who inject drugs are mostly monogamous and noninjecting15,23,37 and thus, present low risk to their male injecting partners. Further, intention to conceive or use of nonbarrier methods for birth spacing or birth limiting also discourages condom use, and this is especially relevant in India, where condom use among the general population is low (<10%). 38
Logistic regression identified important determinants of unprotected sex and may assist to identify strategies to reduce risk to RFPs. Unprotected sex at baseline was positively associated with unprotected sex at the postintervention phase, indicating that the past condom use behavior can predict future condom use intentions. Other studies have also reported predictability in intended condom use based on an individual’s prior history of condom use.39–41 Living with family was also associated with higher odds of unprotected sex, as men were likely to be sexually active when living together with their RFP. Other factors which increased the odds of unprotected sex with RFPs included awareness among men about their HIV-negative status. This could be because of no perceived risk of onward HIV transmission, although it would put their partners at risk of STIs and unintended pregnancies. This is consistent with findings from other studies 42 and our own baseline study which showed that safer sexual practices were more common among HIV-positive study participants than HIV-negative participants. 1 Information about their own HIV status, which could be a proxy indicator of being aware of their HIV-negative status, was also associated with higher odds of unprotected sex. Therefore, it is essential that PWID undergo repeat HIV counseling and testing and comprehend the importance of safer sexual behaviors, especially if they are HIV-negative.
At least one risky injection practice in the past one month reduced the odds of unprotected sex with RFPs. It is possible that men who engage in risky injection practices were heavy drug users and may have abstained from having sex with their RFPs; hence the reduced odds of unprotected sex with them.
Marriages are based on a shared desire for intimacy and mutual trust. Therefore, introducing condoms into the relationship is often unwanted and difficult to navigate. 43 However, considering the high risk of HIV and non-HIV STI transmission from men who inject drugs to their RFPs (with over a third of PWID reporting any unprotected sex in the past three months), there is an urgent need to reduce unprotected sex among them. It is recommended that married male PWID, especially those who live with their families or are HIV-negative, should receive regular counseling for safe sex with RFPs with adequate emphasis on dual benefits of condom use. Couple counseling can be an effective way to introduce and collectively address potential challenges in condom use. Use of condoms, irrespective of other non-barrier contraceptive methods, should be strongly promoted. Public health programs may also consider proactive outreach to women with injecting male partners as they have low perceived risk and inadequate agency to negotiate safe sex. 44
Study limitation
There was a sizeable loss-to-follow-up among the study population – 35.6% at FV1 and 32.9% at FV2, potentially introducing a selection bias. However, married male PWID who returned at FV2 practiced similar (baseline) behaviors compared to those who did not return. Moreover, although the select intervention was anticipated to reduce unprotected sex, it was not specifically designed to do so. Also, self-reported behaviors may be subject to social desirability, although prior studies have confirmed their validity among PWID. 45 The study recruited close to one-fourth of the estimated PWID in Delhi; however, representativeness of the sample cannot be ascertained as there may be differences in PWID in other districts of Delhi. Also, we may not have reached PWID who did not disclose their injection use behavior or were not a part of drug-using networks.
Conclusion
Our study findings highlight that despite exposure to key HIV prevention services, unprotected sex with RFPs continued to be high among married male PWID. While, focus on reducing drug-use and paid-sex related risk behavior is necessary, it is equally imperative to emphasize on sexual risk reduction within marriage through couple counseling and direct outreach to RFPs (wherever possible).
Footnotes
Acknowledgements
We would like to thank Dr Neeraj Dhingra, former - Deputy Director General, National AIDS Control Organization and Mr JK Misra, Joint Director - Targeted Interventions, Delhi State AIDS Control Society for their guidance and support to the project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this project was provided by ARISE – Enhancing HIV prevention for at-risk populations, through financial support provided by the Canadian Government through Foreign Affairs Trade and Development Canada, and via financial and technical support provided by PATH (CID.1450-02135-SUB). The ARISE project implements innovative HIV prevention initiatives for vulnerable communities, with a focus on determining cost-effectiveness through rigorous evaluations. We also gratefully acknowledge the contribution from the Victorian Operational Infrastructure Support Program received by the Burnet Institute, and Australia's National Health and Medical Research Council (NHMRC) for the Career Development Fellowships of SL.