
Abstract
Men who have sex with men (MSM) are disproportionally affected by the HIV epidemic. Self-efficacy is an important individual psychosocial factor associated with access to and use of health and HIV-related services. We estimated HIV testing prevalence and examined the relationship between HIV testing self-efficacy and self-reported HIV testing behavior among young MSM (YMSM) in Myanmar. We enrolled 585 MSM aged 18–24 years from six urban areas using respondent-driven sampling (RDS) technique. RDS analyses were performed to provide estimates for the key outcome of interest. More than a third (34.5%) had never been tested for HIV, whereas 27.5% and 38.0% had their most recent HIV test more than three months and within the past three months from the time of interview, respectively. Young MSM who reported high self-efficacy (adjusted relative risk ratio [ARR]=7.35, 95%CI = 2.29–23.5) and moderate self-efficacy (ARR = 8.61, 95%CI = 3.09–24.0) were more likely to report having tested for HIV in the past three months compared to their counterparts who reported low self-efficacy. Findings highlight a positive association between self-efficacy and HIV testing uptake, indicating a potential causal relationship. Further research is needed to examine the direction of this association and inform future public health interventions targeting YMSM in Myanmar.
Introduction
Compared to the general population, men who have sex with men (MSM) are at greater risk of HIV infection in nearly all studied contexts.1–4 Compared to their age peers in the general population, young MSM (YMSM) are more likely to engage in high-risk behaviors such as having condomless anal intercourse and are more vulnerable to HIV infection.5,6 Published data showed a global ongoing high HIV incidence—particularly among adolescents and YMSM, with an overall trend suggesting a greater burden of HIV infection in low- and middle-income countries (LMICs).7–11 It is recommended that MSM, including YMSM, who engage in high-risk behaviors should have an HIV test every three months. 12
Self-efficacy is defined as individual’s belief in his or her capacity to execute behavior necessary to produce specific performance attainment. 13 Perceived self-efficacy for specific health behavior is a social cognitive factor that has been highlighted in the Health Action Process Approach. This model of health behavior change stipulates that the adoption and maintenance of health behaviors require two distinct processes: motivation to change and self-regulation. Within these processes, different social cognitive predictors may emerge and self-efficacy appears as the only predictor that is equally important in both processes. 14 Previous research has shown that health-related self-efficacy contributes to the likelihood of having access to health care and is associated with health outcomes: higher self-efficacy is associated with having multiple points of connection to the health care system, 15 while lower self-efficacy is associated with higher burden of chronic diseases. 16
Recent studies have examined the importance of psychosocial factors in HIV testing uptake; 17 however, data on the relationship of self-efficacy and HIV testing behavior, particularly from low-resource settings, are limited and not consistent. This is partly because different measures of self-efficacy had been used among different study populations in different settings.18–20 For example, a study among HIV-negative incarcerated adult men reported that men with high HIV coping self-efficacy are more likely to be tested for HIV, 21 while another study among females using shelter services for intimate partner violence found that general self-efficacy for handling difficult situations, measured by 10 items general self-efficacy scale (GSE), has no effects on the acceptance of HIV testing. 22
Our previous study showed that self-efficacy was correlated with HIV testing uptake among YMSM in Myanmar, a LMIC with a concentrated HIV epidemic among key populations. 23 In this present analysis, we aim to estimate HIV testing prevalence and examine the relationship between different levels of HIV testing self-efficacy and self-reported HIV testing behavior of YMSM aged 18–24 years from six urban areas of Myanmar.
Methods
Study design
This is a cross-sectional study using data from the evaluation of the Link-Up project, a global HIV and sexual reproductive health project led by the International HIV/AIDS Alliance, with YMSM in Myanmar. The project implemented a combined community-based peer education and clinic-based service intervention to improve the health of YMSM. The interventions were implemented for six months from October 2014 and data for the evaluation study were collected between April and June 2015. Details of project interventions and the evaluation study design, including study population, data collection, and study measures have been reported elsewhere. 24 Briefly, potential participants who self-identified as YMSM aged 18–24 years, living in six urban areas (Pathein, Mawlamyine, Bago, Kalay, Magwe, and Thanlyin) of Myanmar and reported having sexual intercourse with other men in the past six months were recruited into the study using respondent-driven-sampling (RDS). 14 A total of 585 MSM were recruited by 33 seed respondents to participate in face-to-face interviews with a trained MSM data collector using study tools adapted from a validated questionnaire for a sexual health study among MSM in Kenya. 25 The questionnaire was translated to local language by a researcher who is fluent in both English and Burmese. The final questionnaire was reviewed by the research team to ensure clarity and consistency between English and Burmese versions.
In order to examine factors associated with uptake and the temporal nature of HIV testing among YMSM, we constructed an outcome variable for the main outcome of interest “HIV testing status” with three groups including never tester (never been tested for HIV), nonrecent tester (having most recent HIV test more than three months ago), and recent tester (having an HIV test in the past three months). Other study measures include: (i) main exposure “Self-efficacy for HIV testing” measured using a single-item response on a five-point Likert scale to the statement “I feel confident that I could get tested for HIV” (1 = strongly disagree; 5 = strongly agree), respondents with responses 1–3, 4, and 5 were coded as having low, moderate, and high self-efficacy, respectively; and (ii) potential confounders including socio-demographics (sexual identities: gay- and nongay-identified MSM, age, ethnicity, education, occupation, relationship status), sexual behavior (multiple sexual partners, engaged in transactional sex, reported sexually transmitted infection [STI] symptoms), and other psychosocial variables related to HIV testing (HIV-related knowledge, experienced social stigma due to sexual orientation, disclosure of sexual orientation, knowing sexual partners’ HIV status, having a close relative/friend infected with HIV).
Statistical analysis
Descriptive statistics were used to summarize the characteristics of study participants by outcome of interest (HIV testing status). Respondent-driven sampling (RDS) analyses for outcome of interest using RDS-II (Volz-Heckathorn) estimators 26 with final reported sample including seeds 27 were performed to provide population estimates 28 for coverage of HIV testing among YMSM in Myanmar. There were 12 participants including one seed who reported being HIV positive. To keep the sampling structure and recruitment matrix of the RDS sample intact, given a small number of HIV-positive participants, all self-reported HIV-positive participants were included in the analyses. A sensitivity analysis was performed to assess the potential impact of inclusion of seeds and self-reported HIV-positive participants on the final RDS estimates.
Nested multinomial logistic regression models were built to examine the relationship between self-efficacy and HIV testing status, with YMSM who had never tested for HIV treated as the outcome reference group. Cluster robust standard errors 29 were specified to account for clustering of the sample around the seeds. Independent effects for three specific groups of potential confounding variables—socio-demographic, psychosocial, and sexual behavior factors—were also estimated in multinomial regression modeling. We used univariable-filtering approach for variable selection. Only variables that were significantly associated with the outcome of interest at p < 0.1 in bivariate analyses were included in multivariate analyses. Post-estimation joint Wald tests were used to assess the statistically significant contribution of covariates across outcomes.
Interactions between self-efficacy and other covariates that might influence HIV testing status were assessed. More specifically, interactions between self-efficacy and sexual identity were assessed to examine whether the effects of self-efficacy on HIV testing status were moderated by sexual identity. A complete case approach to missing data was applied. All statistical analyses were undertaken using Stata version 13.1 (STATA Corp, College Station, TX, USA) and Stata user written command package SPost13. 30
Ethics
The study was approved by the Department of Medical Research in Myanmar, the Population Council Institutional Review Board in USA, and the Alfred Hospital Human Research Ethics Committee in Australia.
Results
A total of 585 MSM were enrolled in the study. Table 1 presents the characteristics of the study participants. The mean age was 20.8 years (SD = 1.9). Ninety-one percent of participants self-identified as Burmese ethinicity and had completed middle school or higher, 58% identified themselves as nongay MSM, and 42% as gay MSM. Eighty-four percent of participants who had never been tested for HIV (never testers) were nongay MSM, while only 43% of participants who had an HIV test in the past three months (recent testers) belonged to this sexual identity group. Among the recent testers, 58% reported moderate and 39% reported high self-efficacy. For the nonrecent and never testers, the percentages of YMSM who reported moderate and high self-efficacy were 54%, 41%, 45%, and 37%, respectively.
Characteristics of young MSM aged 18–24 years in six urban areas of Myanmar a disaggregated by HIV testing status, October 2014 to June 2015.
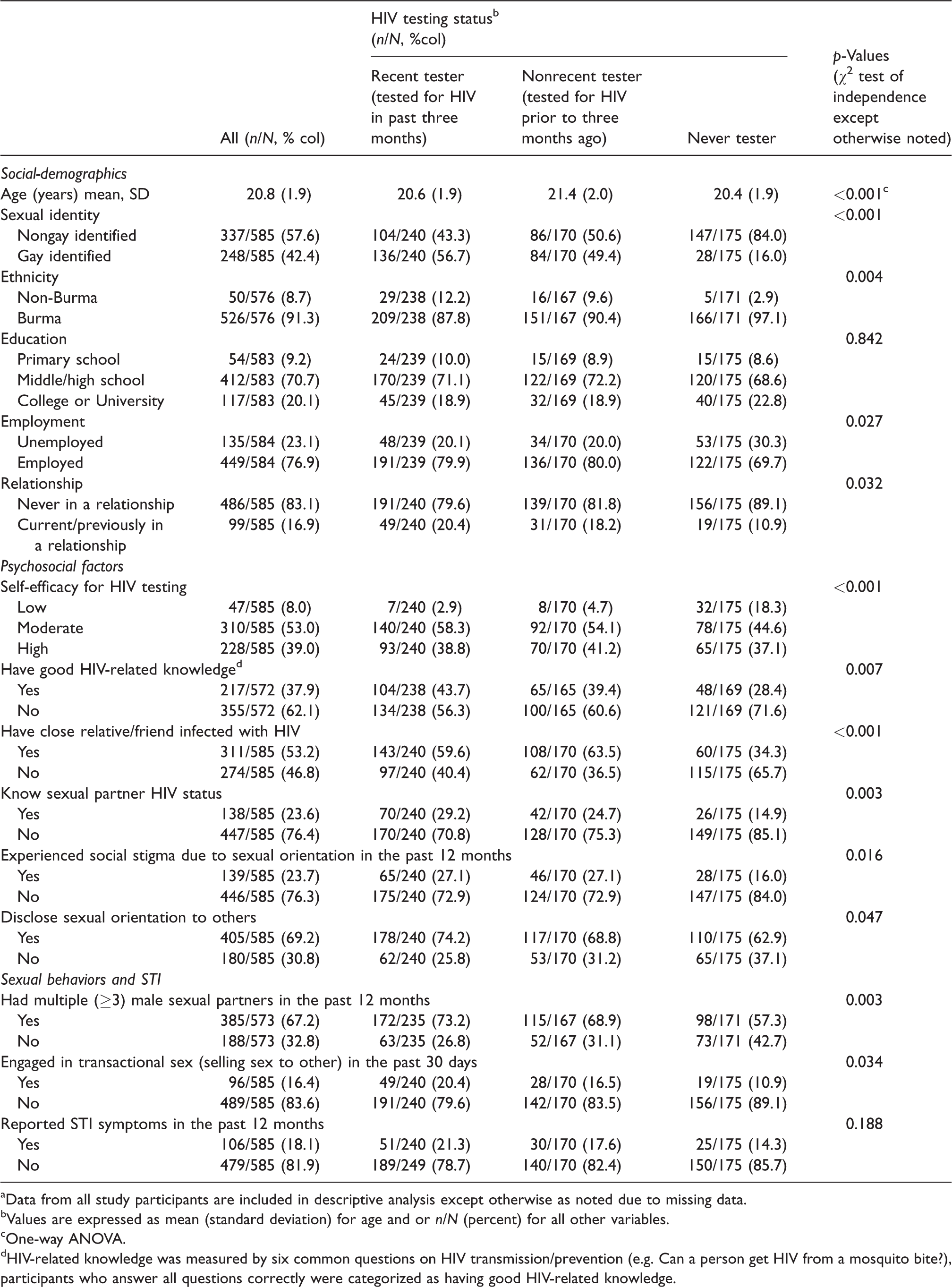
aData from all study participants are included in descriptive analysis except otherwise as noted due to missing data.
bValues are expressed as mean (standard deviation) for age and or n/N (percent) for all other variables.
cOne-way ANOVA.
dHIV-related knowledge was measured by six common questions on HIV transmission/prevention (e.g. Can a person get HIV from a mosquito bite?), participants who answer all questions correctly were categorized as having good HIV-related knowledge.
RDS-population estimates including seed data showed that 38.0% (95%CI: 33.1–43.0) of YMSM in Myanmar have had an HIV test in the past three months, 27.5% (95%CI: 22.9–32.0) had their HIV test more than three months before the time of interview, and 34.5% (95%CI: 29.7–39.5) had never been tested (Table 2). Sensitivity RDS analysis without seed data provided similar point estimates with wider 95% CIs. Similar results were found with 12 HIV-positive participants dropped from the analysis.
RDS population estimates a of HIV testing prevalence among young MSM aged 18–24 years in six urban areas of Myanmar, October 2014 to June 2015.
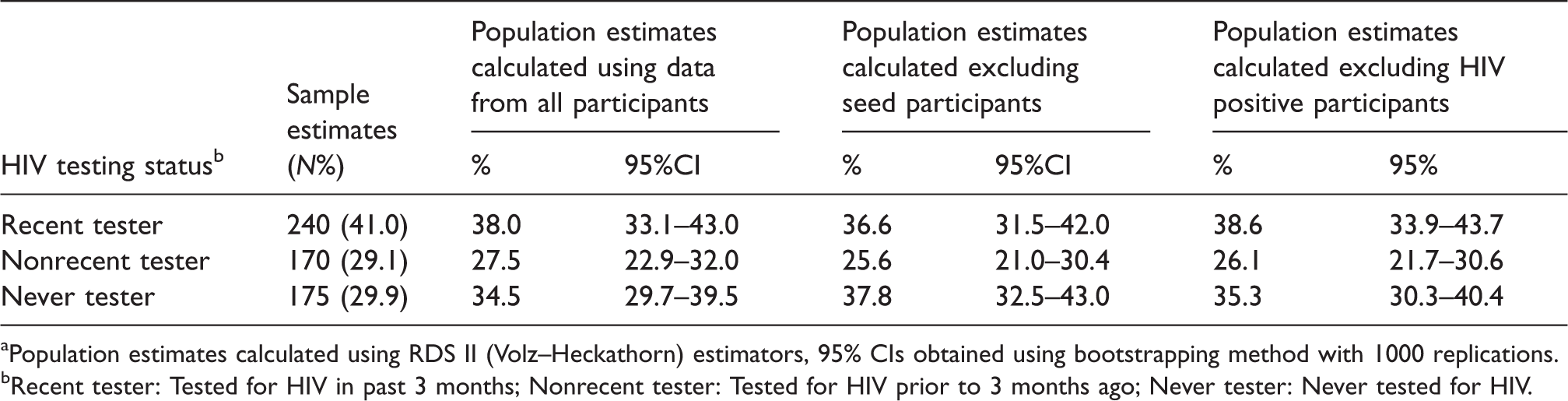
aPopulation estimates calculated using RDS II (Volz–Heckathorn) estimators, 95% CIs obtained using bootstrapping method with 1000 replications.
bRecent tester: Tested for HIV in past 3 months; Nonrecent tester: Tested for HIV prior to 3 months ago; Never tester: Never tested for HIV.
Bivariate analyses suggested that self-efficacy and all other variables except “education” and “reported STI symptoms in the past 12 months” were significantly associated with HIV testing status (Table 1). Results of multivariate multinomial regression analyses (Table 3) showed an association between self-efficacy on HIV testing status among YMSM. The introduction of potential confounders into the regression models did not attenuate the associations. In the final model, Joint Wald tests showed that self-efficacy (p = 0.001), socio-demographic (p < 0.001), and psychosocial factors (p < 0.001) were independently associated with HIV testing but sexual behavior factors were not associated with HIV testing conditional on the other factors (p = 0.067).
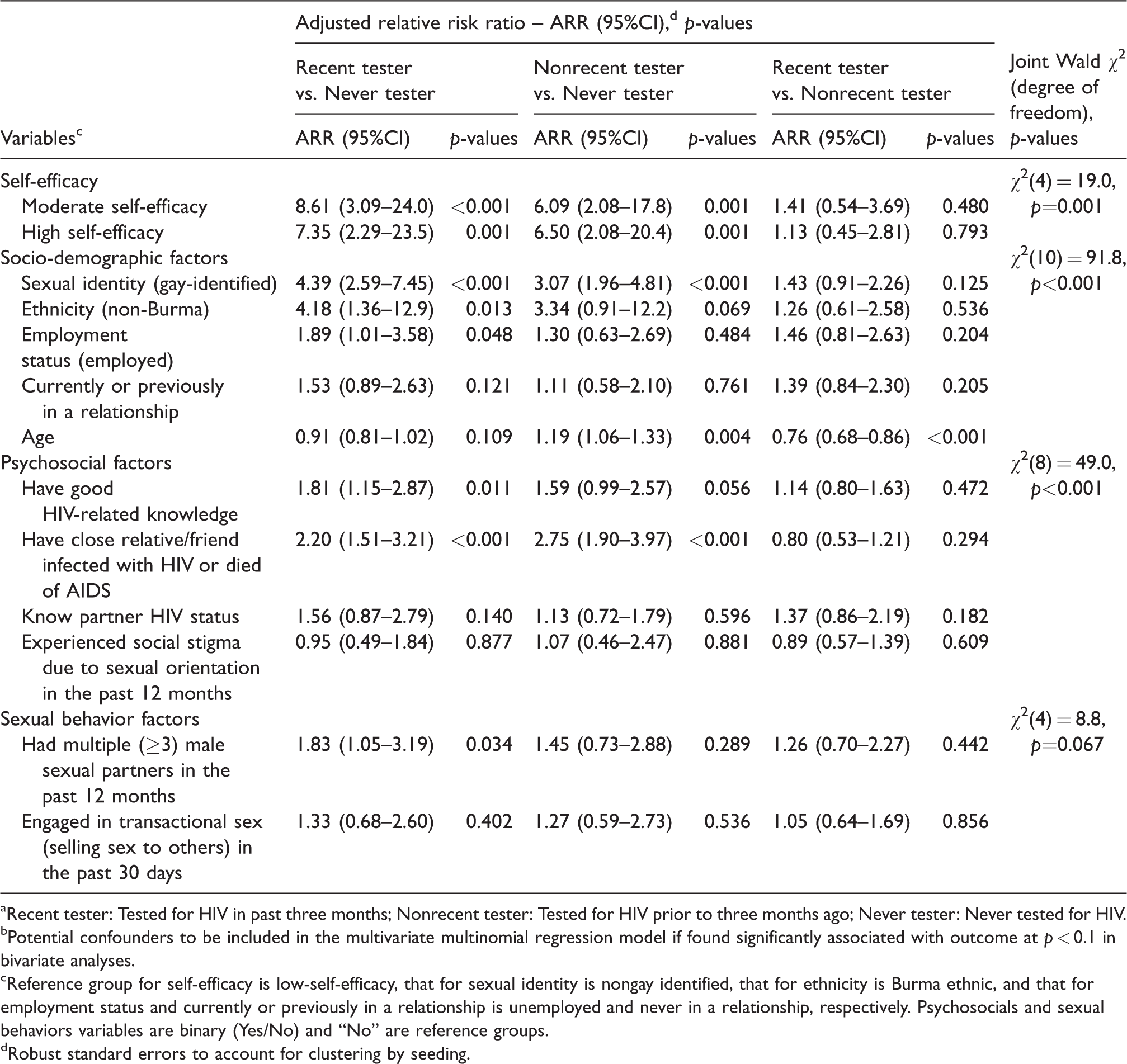
aRecent tester: Tested for HIV in past three months; Nonrecent tester: Tested for HIV prior to three months ago; Never tester: Never tested for HIV.
bPotential confounders to be included in the multivariate multinomial regression model if found significantly associated with outcome at p < 0.1 in bivariate analyses.
cReference group for self-efficacy is low-self-efficacy, that for sexual identity is nongay identified, that for ethnicity is Burma ethnic, and that for employment status and currently or previously in a relationship is unemployed and never in a relationship, respectively. Psychosocials and sexual behaviors variables are binary (Yes/No) and “No” are reference groups.
dRobust standard errors to account for clustering by seeding.
YMSM who reported moderate self-efficacy (adjusted relative risk ratio [ARR] = 8.61, 95%CI: 3.09–24.0) and high self-efficacy (ARR = 7.35, 95%CI: 2.29–23.5) were more likely to have tested for HIV in the past three months (recent testers) compared to their peers who reported low self-efficacy. Similarly, YMSM who reported moderate self-efficacy (ARR = 6.09, 95%CI: 2.08–17.80) and high self-efficacy (ARR = 6.50, 95%CI: 2.08–20.4) were more likely to report being a nonrecent tester compared to their peers who reported low self-efficacy.
In further analyses, we introduced an interaction term to explore whether the association between HIV testing and self-efficacy was moderated by sexual identity. Although we found the effect of self-efficacy on HIV testing uptake was more pronounced for those identifying as gay (nonrecent testing: moderate self-efficacy ARRs = 8.3 vs. 6.3, high self-efficacy ARRs = 8.6 vs. 6.1; recent testing: moderate self-efficacy ARRs = 23.1 vs. 4.1, high self-efficacy ARRs = 14.4 vs. 4.3); jointly these moderated effects were not statistically significant (p = 0.312).
Discussion
Findings from this study shows that HIV testing self-efficacy positively correlates with HIV testing behavior of YMSM aged 18–24 years in Myanmar. This finding is in line with findings from other studies among MSM conducted in high resource settings showing that self-efficacy was positively associated with acceptance and frequency of HIV testing among adult MSM.18,31–33 It is noted that in these studies, HIV testing self-efficacy was discussed; however, the measurements of self-efficacy were varied across these studies with authors using either a single-item statement to measure participant’s confidence in obtaining an HIV test if desired31,32 or an opportunistically constructed scale with five or eight items to measure the extent to which participant’s thought that having an HIV test was under their control if they choose to.18,33
Traditionally, the use of single-item measures of cognitive variables has been criticized due to concern regarding their psychometric properties. However, current research has shown that single-item measures of latent constructs such as self-efficacy, compared to well-established multi-item measures, has equal or even superior predictive utility in predicting health-related outcomes. A single-item measure of self-efficacy was found consistently correlated positively with a well-established 20-item measure and consistently predicted relapse to substance use in a sample of substance use disorder treatment-seeking young adults in the United States. 34 In another study among female university students in the UK, researchers found that a single-item measure of self-efficacy was a significant predictor of well-being as was the validated 10-item measure of general self-efficacy. 35 These findings suggest that using single psychometric measures may offer a valid approach to investigating overall well-being as well as other health-seeking behavior and health-related outcomes.
Previous research in low-resource settings has examined the correlations between self-efficacy related to specific behaviors with HIV testing practice among the general population and the results were mixed. A community survey in Namibia 20 reported that greater self-efficacy for HIV prevention behaviors (ability to enact behaviors preventing HIV infection) was associated with lifetime HIV testing. Similarly, one study found that HIV prevention self-efficacy was positively associated with previous HIV testing among the general adolescent and adult population in eight urban districts of Malawi. 19 However, another community-based study in 11 southern districts of Malawi reported that self-efficacy to protect oneself from exposure to risks of HIV infection was not associated with HIV testing in the past 12 months. 36 Studies among MSM in Australia, 33 Italy, 13 and Hong Kong 31 have shown that self-efficacy was positively associated with self-reported HIV testing. A study among young people aged 18–24 years in South Africa found that HIV risk reduction self-efficacy was not a determinant of HIV testing, 37 while another study among sexually active young people aged 15–24 years in Thailand reported that self-efficacy for HIV testing was associated with ever being tested for HIV. 38 These findings, although useful and indicative, cannot be generalized to YMSM populations in low-resource settings.
In this study, we found no clear evidence on the difference between the impact of high and moderate self-efficacy on HIV testing uptake. However, as different specific self-efficacy beliefs and measurements were employed and there is a paucity of available data on the relationship between self-efficacy and HIV testing among key populations in low-resource settings, consolidation of evidence for guiding public health interventions is a challenge. Therefore, future research may benefit from using standardized, validated self-efficacy scales 39 to measure self-efficacy as a global construct underlying a basic belief in one’s capabilities to exercise control over their own functioning in various challenging situations rather than self-beliefs related to specific behaviors or learnt behaviors. There is also a need to develop and validate a standardized self-efficacy scale specific to HIV testing for research examining the relationship between this psychosocial factor and HIV testing behavior. This may help to provide needed information and facilitate the synthesis of evidence to draw conclusions on effects of self-efficacy on HIV testing and inform the design of public health interventions to improve HIV testing uptake among target populations.
Results of our study support the argument that the inclusion of seed data in RDS analyses can provide unbiased estimates. We show that when using RDS estimator II, the inclusion of seed data in the final analysis can produce accurate population estimates. We estimate that only 38% of YMSM in Myanmar have been tested for HIV in the past three months while more than a third (34.5%) has never been tested. This finding raises an alarm for the national health policy makers in Myanmar where the majority of newly-diagnosed HIV-infected cases were found among young key populations, particularly YMSM aged less than 25 years who experience an HIV infection rate five times higher than that of their peers in the general population. 40 This is also an indication that the reported HIV prevalence of 6.6% among MSM in Myanmar 41 may be underestimated and innovative approaches to improve HIV testing coverage among this marginalized population are urgently needed if the first 90 of the 90-90-90 target (90% of HIV infected people are diagnosed) is to be achieved. Recent studies have shown that new approaches to HIV testing such as home-based or HIV self-testing could be effective and efficient in reaching more first time testers and promoting frequent testing among MSM who were unreached by conventional testing methods.42–45 Such approaches may well be worth considering for Myanmar in the years to come.
Our study findings add to the evidence that self-efficacy for HIV testing is positively associated with HIV testing behavior of YMSM who are at higher risk of HIV infection but have limited access to HIV services they need.46,47 The positive association found in this study may indicate a potential causal relationship between self-efficacy and HIV testing and public health interventions to improve self-efficacy may help to promote HIV testing behaviors among YMSM in Myanmar. Our findings warrant further research to determine the effects of individual psychosocial factors, particularly self-efficacy on HIV testing practice among high-risk populations in LMICs. This is an important area of research because improving HIV testing coverage and increasing the proportion of people at elevated risk of HIV infection who know their HIV status is a key strategy to reach the 90-90-90 targets in countries with concentrated HIV epidemics among key populations. 48
The cross-sectional design of this study does not allow us to determine the impact of self-efficacy on HIV testing behavior. It limits our ability to generalize the findings and draw conclusive causal relationship between self-efficacy and HIV testing among YMSM in Myanmar. The direction of this relationship and its implications for public health interventions are subjected to further examinations in future studies. Our data are self-reported and therefore can suffer from recall and social desirability bias. The measure of self-efficacy using a single-item statement specifically related to HIV testing behavior does not allow us to make direct quantitative comparisons with findings from other studies. Nevertheless, this study provides much-needed data related to HIV testing behavior of a young population at high risk of HIV infection in Myanmar. It contributes to the pool of evidence on self-efficacy and HIV testing behavior of YMSM and offers directions for future HIV research in Myanmar as well as other countries in similar contexts.
In conclusion, we found that more than a third of young MSM aged 18–24 years in Myanmar have never tested for HIV. HIV testing self-efficacy positively correlates with HIV testing behavior and future research is needed to determine the direction of this association and inform public health interventions targeting YMSM in Myanmar.
Footnotes
Acknowledgements
The authors would like to acknowledge the International HIV/AIDS Alliance and Marie Stopes International for their kind collaboration and support, and the Dutch Ministry of Foreign Affairs (BUZA) for their financial support of the Link-Up project, which aims to improve the sexual and reproductive health and rights (SRHR) of one million young people affected by HIV across five countries in Africa and Asia. The project was implemented by a consortium of partners led by the International HIV/AIDS Alliance. The Population Council, in partnership with Burnet Institute implemented this research in Myanmar. Our special thanks go to participants involved in the study and the screeners from the study sites. We also acknowledge the data collection team from Myanmar Business Coalitions on AIDS (MBCA) and the Burnet Institute Myanmar research team. The authors gratefully acknowledge the contribution to this work of the Victorian Operational Infrastructure Support Program received by the Burnet Institute. Stanley Luchters is a recipient of National Health and Medical Research Council of Australia (NHMRC) Career Development Fellowship. Minh D Pham received support via an International Postgraduate Research Scholarship (IPRS) from the Commonwealth of Australia and the Victorian International Research Scholarship (VIRS) from State Government of Victoria, Australia.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Government of the Netherlands’ Ministry of Foreign Affairs through its Sexual and Reproductive Health and Rights (SRHR) Fund through a subcontract from the International HIV/AIDS Alliance under the Link-Up project.