
Abstract
Oral pre-exposure prophylaxis (PrEP) has the ability to curb HIV incidence worldwide and bring us closer to ending the HIV epidemic. Scale up of PrEP service delivery has many similar challenges to those faced by voluntary medical male circumcision (VMMC) services roll-out. This article outlines ten important lessons learned during the scale up of VMMC services in sub-Saharan Africa and their application to current oral PrEP implementation efforts to promote faster expansion for public health impact.
Introduction
Thirty-six years after the identification of HIV,1,2 the HIV epidemic has resulted in the death of 35 million people. 3 Although a highly-effective vaccine has yet to be developed, the intervening years have seen impressive advances in HIV-related diagnostics and treatment. A person with HIV today can expect to live a relatively normal lifespan if the infection is correctly diagnosed and clinically managed, primarily through treatment with antiretroviral (ARV) medications.4,5 Early detection and successful treatment has the added benefit of preventing onward transmission of HIV to others, thereby adding to the public health benefits.6,7
In 2012, the prevention benefits of ARVs were further expanded when the United States Food and Drug Administration approved the use of specific ARVs, a combination of emtricitabine and tenofovir disoproxil fumarate, as pre-exposure prophylaxis (PrEP) against HIV. 8 Randomized control trials demonstrated oral PrEP to be 85–92% efficacious against HIV acquisition when taken daily,9–12 while major demonstration projects showed oral PrEP to be 75–90% effective.13–17 In 2015, the World Health Organization (WHO) recommended that oral PrEP be made available to those at substantial risk of HIV infection.18,19 The Joint United Nations Programme on HIV/AIDS (UNAIDS) proposed an aspirational target of three million people to be started on oral PrEP by 2020 in order to reach the 2030 goal of an AIDS-free generation. 20 To date, service delivery of oral PrEP has yet to reach the scale to have public health impact in most settings, although PrEP services are now starting in a few countries, for a range of key populations in low- and middle-income settings (e.g. Kenya and South Africa), including among men who have sex with men (MSM) in North America, Europe and Asia.21–37
As the world embarks upon the initial stages of PrEP scale up, it is imperative to anticipate and proactively address key programming requirements and challenges. While some learning-by-doing is desirable and inevitable, oral PrEP scale up should look for lessons learned by other prophylactic clinical interventions that have been taken from research to public health scale. We proffer that, among such HIV interventions, the scale up of voluntary medical male circumcision (VMMC), a programme that to date has reached over 15 million out of the ambitious initial target of 20.8 million males circumcised by 2016, 38 has parallels with oral PrEP. The lessons of VMMC scale up can be leveraged to improve both programme efficiencies and safety in PrEP scale up.39,40
To begin, a brief comparison and contrast of the two interventions provides important context. VMMC is a one-time intervention that affords a greater than 60% reduction in HIV acquisition risk for heterosexual men.41–48 The VMMC procedure may be surgical or device based. It is permanent, as is the partial protection afforded. Interaction with the health system is limited, involving three to four appointments for a typical client. In contrast, oral PrEP can provide up to 90% reduction in HIV acquisition risk for both women and men, regardless of sexual orientation, only while the medication is taken as prescribed.9,10 Thus, an oral PrEP user may interact with the health system repeatedly for many years, whenever they face a period of risk and they choose to take oral PrEP.
At the same time, VMMC and PrEP have much in common. Both interventions serve to keep HIV-uninfected individuals free of HIV; in turn, they do not infect others. Both VMMC and oral PrEP are clinical services provided by trained, licensed health care practitioners, often in resource-constrained settings. Both VMMC and oral PrEP have a strong evidence base supported by WHO and UNAIDS.18,19,49 Perhaps most importantly, VMMC and oral PrEP can have a public health benefit by curbing the HIV epidemic, but that impact depends upon a high rate of uptake among those most likely to benefit. In other words, scale up among those at greatest risk is crucial for either to reduce HIV incidence.39,40
Here we describe the scale up of VMMC and draw parallels with oral PrEP to demonstrate how lessons learned from the former may benefit the latter. These lessons are summarized in Table 1.
Summary of the ten key lessons learned during voluntary medical male circumcision scale up with application to oral HIV pre-exposure prophylaxis implementation.
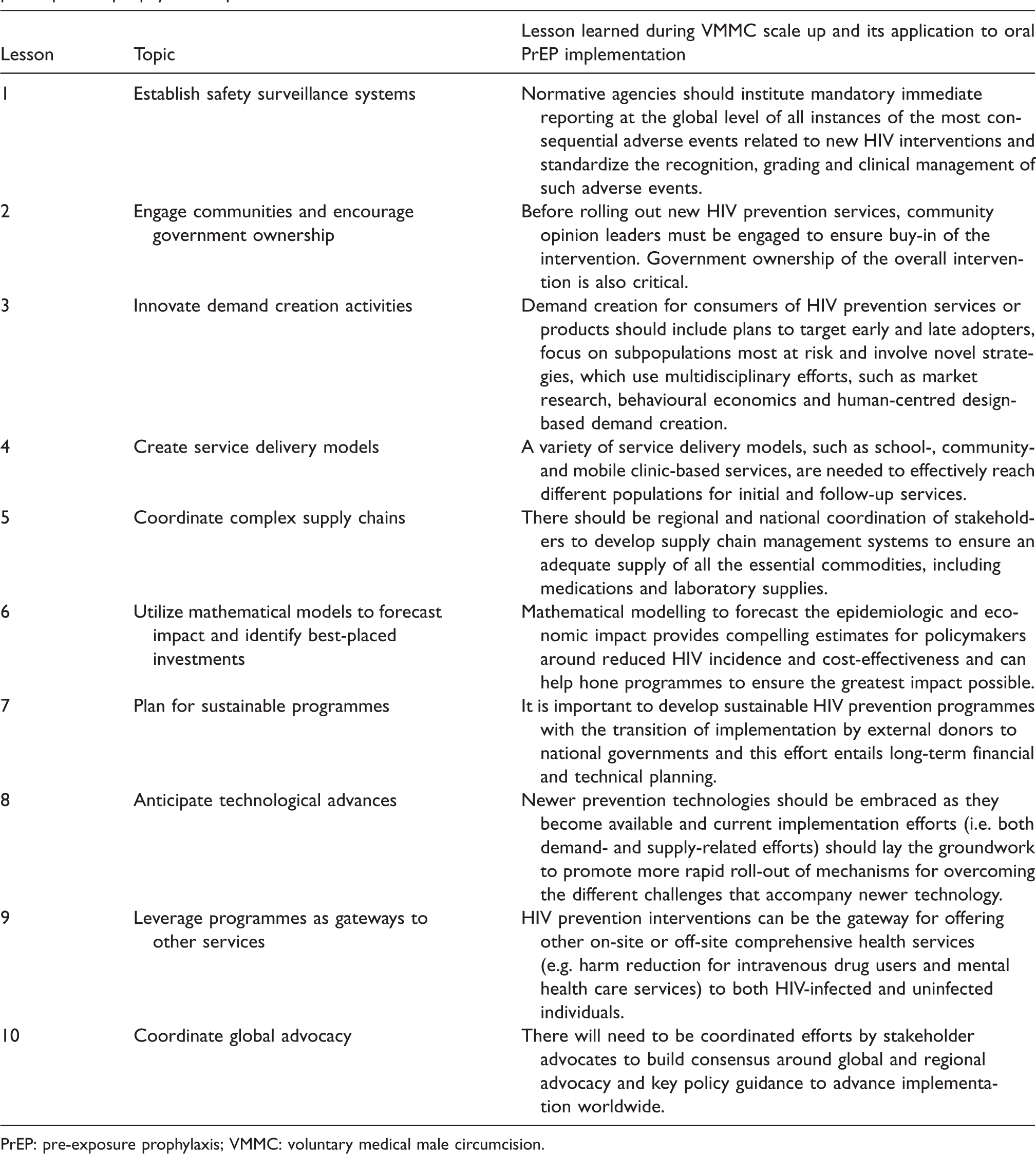
PrEP: pre-exposure prophylaxis; VMMC: voluntary medical male circumcision.
Lesson 1: Establish safety surveillance systems
Like all medical procedures, VMMC involves an inherent level of health risk to the client. While the United States President’s Emergency Plan for AIDS Relief (PEPFAR) was quick to suggest definitions for common adverse events (AEs) seen in clinical trials and national programmes around AE monitoring, evaluation and corrective action remained piecemeal throughout early scale up of VMMC programmes. 50 To assist, the College of Surgeons of East, Central and Southern Africa developed a guide to standardize the recognition, grading and clinical management of AEs. 51 Although programmes had guidance on monitoring the common anticipated AEs from clinical trials, little effort was made to distinguish the most consequential AEs or to ensure that transnational surveillance systems were in place to continuously monitor, collate and evaluate the rare but most severe AEs. 52 For example, an association between VMMC and tetanus had not been anticipated. Two cases of tetanus that occurred in 2012 went unnoticed by the global community and, therefore, unrecognized as a potentially serious concern until two years later when WHO uncovered a cluster of tetanus cases in the area of Lake Victoria.52,53 WHO called upon programmes to systematically report all tetanus cases thereafter. Collaboratively, WHO and PEPFAR instituted mandatory immediate reporting to the global level of all instances of the most substantial AEs (e.g. AEs resulting in death, permanent disability or deformity, or prolonged hospitalization).54–56 Simultaneously, national VMMC programmes were strongly encouraged by WHO to convene oversight committees to monitor and act upon AEs occurring in their countries, to ensure rapid national awareness of such events as well as to promote client awareness of signs and symptoms that warranted heightened caution.
Although to date they have been more benign, AEs resulting from the use of oral PrEP in demonstration projects and non-research settings have occurred and will continue to occur. Rare and severe AEs associated with oral PrEP, for example, may include new onset renal insufficiency, among others.10,13,57–67 In addition, some individuals acutely HIV infected immediately before or while taking PrEP develop resistance mutations impacting their subsequent HIV treatment options. Though modelling studies suggest that PrEP use contributes to less than 5% of the total burden of ARV resistance,68–71 laboratory surveillance activities should monitor for drug resistance among PrEP users who seroconvert so that they may be appropriately clinically managed. Normative agencies must endeavour to issue guidance to national programmes that standardize the recognition, grading and clinical management of PrEP AEs. The most consequential of oral PrEP-related AEs, even hypothesized AEs, should be defined and surveillance systems should be created to ensure mandatory immediate reporting of AEs at the global level, including to drug manufacturers. Every country instituting an oral PrEP programme should prioritize convening committees, at both facility and national levels, to continuously review and act upon AEs among oral PrEP users.
VMMC scale up has taught us that, once an intervention is scaled up to reach millions of people, rare and consequential AEs will occur. For oral PrEP it is important to anticipate those events now, provide guidance on their identification and management, institute surveillance systems to monitor and collate findings globally and nationally, and act upon the findings so as to refine global guidance that defines the appropriate measures to characterize those events that may occur and prevent those that may be averted.57–59,67
Lesson 2: Engage communities and encourage government ownership
Following the WHO recommendation of VMMC for HIV prevention in 2007,72,73 initial progress was slow, and countries differed in their enthusiasm for implementation. Overcoming social and cultural norms in non-circumcising communities and governments taking ownership of their VMMC programmes were hallmarks of early success. 74 In addition, local champions (e.g. parliamentarians in Zimbabwe and traditional leaders in Zambia) have been important in many settings, advocating for VMMC in their communities.75–77 For PrEP a similar pattern is emerging, with a few countries at the forefront (e.g. Kenya and South Africa), and others showing caution.21–25
Engaging opinion leaders within various communities early to ensure their understanding and endorsement of the proposed HIV prevention approach is critical to broadening acceptance.
Lesson 3: Innovate demand creation activities
Following the initial release of the WHO recommendations for VMMC in 14 African countries, a high level of latent demand 78 kept circumcision clinics fairly busy in the early period of scale up. This led to a false sense of high overall demand for circumcision and, as a result, relatively little effort was devoted to innovative demand creation activities. The early, conventional communication methodologies touted the HIV prevention benefits of VMMC and were focused primarily on likely early adopters. 79 However, as the more easily persuaded individuals were successfully reached with VMMC services, the harder-to-convince individuals remained uncircumcised. As a result, many service providers went underutilized. The Bill and Melinda Gates Foundation was pivotal in promoting and implementing novel methodologies to generate demand for VMMC among consumers, which included bringing together experts in consumer market research, communication, behavioural economics and human-centred design.80,81
Scale up of oral PrEP will, likewise, require more than just making services available to communities who will benefit the most. As a case in point, in the United States significant expansion of oral PrEP has taken longer than expected,21,82 although PrEP use is currently increasing in some states. Among high-risk MSM in Washington State, those who reported ever taking PrEP increased from 5% in 2012 to 31% in 2015. 83 However, uptake of PrEP has been limited among racial and ethnic minority MSM, who often have the highest risk of acquiring HIV. 84 In addition, knowledge about the benefits of PrEP remains very limited in many parts of the world where there are those at substantial risk of HIV infection and would benefit from oral PrEP.85,86
VMMC scale up has taught us that it is challenging to engage healthy, HIV-uninfected people, many of whom are young, and encourage them to consider a medical intervention to prevent something that may or may not happen at some future date. Demand creation innovations in the space will be required to create and sustain demand for oral PrEP among the intended subpopulations (i.e. those most at risk of acquiring HIV infection). Market research complemented with innovative methodologies like behavioural economics and human-centred design may be beneficial to reaching harder-to-reach priority populations with sufficiently sophisticated content through messaging channels to drive demand. 80
Lesson 4: Create service delivery models
Developing different VMMC service delivery models enabled programmes to reach different subgroups of boys and men. Outreach programmes, whereby VMMC services are brought from the clinic setting directly to the people through mobile, temporary service locations, have reached high numbers.74,76,87–91 Some service delivery locations have offered after-hours and weekend services to attract older males, rather than adolescents, who might otherwise forego VMMC due to employment considerations. Campaigns during holiday periods have reached younger males during school breaks.89–91 Likewise, concerted short-term campaigns to boost awareness and intensify services for a limited period have succeeded to reach different populations. 92
Oral PrEP may differ from VMMC in supply and demand because oral PrEP is likely to be a more integrated service than VMMC and will require longer periods of engagement with health care services. Despite the differences, lessons from VMMC still apply in the context of needing to prioritize and reach often marginalized populations. Therefore, like VMMC, it will be important to plan for creative and innovative oral PrEP service delivery and outreach models, from the start of implementation, to bring PrEP to where the individuals who need it most are.
VMMC has taught us that even a surgical procedure can be safely performed in a tent or retrofitted space, availing services to those otherwise unable or unwilling to access them. Given that oral PrEP is less invasive, service delivery points may be as varied as the populations they serve, provided that follow up for prescription refills is carefully coordinated. Different at-risk populations will likely require bespoke oral PrEP service delivery models in order to achieve high coverage rates. In addition, concerted short-term campaigns to promote oral PrEP services may help to normalize this prevention intervention, catalyse demand and, thereby, intensify service uptake over a targeted time period.
Lesson 5: Coordinate complex supply chains
At the outset of VMMC programmes, supply chains had to be built to deliver surgical equipment, other commodities and, in certain cases, clinical infrastructure to some of the most remote sectors of the health system. The advantages and disadvantages of utilizing reusable versus disposable supplies had to be weighed, giving consideration to issues such as the environmental impact of waste management and sustainability. The introduction of oral PrEP and the complementary laboratory testing components also will pose obstacles to supply chain management, particularly where PrEP services are delivered in non-clinical settings. While supply chains for the management of ARVs are widespread, those for laboratory testing commodities (e.g. for creatinine and hepatitis B testing) may not be readily available.93–95
VMMC has taught us that it is important to engage with product manufacturers, service delivery organizations and health centres, and governments to ensure that there are regional and national supply chain protocols in place to mitigate commodity stock-outs. In the case of oral PrEP, pharmaceutical companies will also need to be engaged in this process.93–95
Lesson 6: Utilize mathematical models to forecast impact and identify best-placed investments
Mathematical modelling to forecast epidemiologic and economic impact was pivotal in securing political buy-in for VMMC as a priority HIV prevention intervention. Modelling was undertaken not only to show the overall curbing of the epidemic by reaching population saturation, but also, at a more granular level, models estimated the number of VMMC procedures needed to avert a single HIV infection within ten years. In sub-Saharan Africa, this number turned out to be approximately nine. 96 Results were purposefully framed in multiple ways to speak to varied audiences, and thus health policy leaders as well as economists could readily appreciate the substantial benefits of VMMC, not just nationally but also at the community and even facility levels. Following initial modelling results early in the intervention, more refined models helped to hone demand creation and service delivery models to reach individuals who were the most at risk for HIV infection in order to heighten impact and cost efficiencies.97,98
In this same way, mathematical modelling is being exploited, and should continue to be, to quantify the epidemiologic and economic impacts of scaling up oral PrEP. For example, recent modelling from Kenya suggests that PrEP adds additional benefit to the current HIV prevention measures employed, especially for MSM.25,57,96,99–102 In the United States and Europe, where only high-cost, branded PrEP is currently available, PrEP could be cost effective with drug price reductions or use of generics.103,104 However, modelling studies in the United States also predict a 70% reduction in the number of new HIV infections nationally with the use of oral PrEP and treatment as prevention. 105
VMMC has taught us that mathematical modelling can forecast future epidemiologic and economic benefits that may affect health policy decisions today. As with VMMC, modelling the impact of PrEP highlights the importance of focusing services in geographic areas and subpopulations that stand to gain the most from PrEP services and ensure sufficient coverage among them to achieve epidemic impact.99,101,106
Lesson 7: Plan for sustainable programmes
Long-term sustainability of any public health programme, VMMC, oral PrEP or others, depends upon purposeful and well-timed transfer of financial and oversight responsibilities from donors to national governments. 38 Institutional capacity building and the integration of VMMC services into routine adolescent and adult service delivery systems should remain a priority.38,107 Only a few VMMC programmes have reached levels of maturity, by achieving predetermined circumcision coverage targets among older adolescent and adult males, such that long-term sustainability has become a topic of wide interest. 101 Much of the debate on planning for sustainability remains theoretical at this point, with smaller demonstration projects pointing out which sustainability strategies may or may not meet the mark.
For oral PrEP, as services are just beginning in a few countries, planning for the long-term financial and technological trajectory of programmes may better happen in parallel. In this way, questions about sustainable financing and programmatic oversight will not linger as excuses for failing to begin at all.
Lesson 8: Anticipate technological advances
The lion’s share of VMMC procedures performed to date have used conventional surgical methods. However, medical manufacturers had been developing prototypes of male circumcision devices for adults that could help circumvent surgical programme challenges related to both supply and demand. Following numerous clinical trials and demonstration projects, WHO concluded that male circumcision devices could reduce rates of AEs from conventional surgical methods, offer less invasive and potentially more affordable alternatives, and facilitate greater scale up delivery efforts.108,109 However, varying degrees of re-engineering of the devices and device-based techniques have been necessary to optimize their safe and efficient use, and ongoing uncertainties and unexpected complications have hindered wide-scale use. Some of the risks and negative consequences of new, alternative methods became known only after relatively large numbers of individuals underwent device-based circumcision (i.e. cases of tetanus), and well after there were large initial financial investments in development and research.50–53 Early VMMC implementation efforts using older technology has laid the groundwork to implement newer technologies more rapidly when they become available and safety is assured.
Similarly with PrEP, as daily oral options are being introduced and scaled up, the research pipeline is already replete with alternative delivery methods, such as alternative oral preparations and longer-acting injectable formulations, rings and implants.110–113 These alternatives have the potential to circumvent some of the difficulties with oral, daily formulations, namely uptake and adherence. At the same time, new PrEP delivery systems will almost certainly come with their own challenges, some known already and others yet to be discovered.
VMMC has taught us that continued investments in research and development are necessary to realize maximum benefits, which is true for PrEP alternative delivery systems, as well.18,19 Implementation of presently available modalities and formulations are crucial to pave the way for newer alternatives. Demand creation messaging and service delivery and supply chain protocols should be adaptable to the newer technologies that lie ahead.
Lessons 9: Leverage programmes as gateways to other services
In the 14 priority African countries where VMMC programmes have been successfully scaled up, men lag behind their female peers in accessing HIV services (e.g. timely diagnostic testing and treatment); however, VMMC programmes have been remarkably successful in reaching millions of men with HIV testing.45,114 In general, men seek health care less often and at a later stage than women, with resultant worse health outcomes for HIV, other infections and non-communicable diseases.115–117 Learning from their success in reaching men, VMMC programmes are now considering how they can broaden and increase their impact from HIV to include other men’s health conditions and look at issues such as masculinity and gender-based violence. 38
Similarly, for maximum impact, oral PrEP services should be integrated with other health and social services (e.g. sexually transmitted infections testing and treatment, hepatitis B and C virus screening and treatment, provision of contraception, harm reduction for injecting drug users, other substance use counselling, and evaluation and treatment for mental and emotional health illness).118,119 Furthermore, people who seek PrEP services will likely do so because they are at risk for HIV infection, and significant proportions may already be HIV infected; thus, HIV testing conducted prior to starting PrEP can provide an earlier entry point for early diagnosis and immediate linkage of those who test HIV positive to treatment for viral suppression.4,5
VMMC has taught us that offering a service within a comprehensive preventative package may extend the health benefits well beyond those of the discrete service itself. Particularly for populations that rarely engage with the health sector, men in general and key populations, both VMMC and PrEP provide unique opportunities for holistic health assessments and treatment or referral for co-morbid conditions.
Lesson 10: Coordinate global advocacy
The saying that ‘there is strength in numbers’ is true whether the debate centres on VMMC, oral PrEP or other biomedical interventions. More progress is made when advocates speak in a consistent voice to national policymakers and donors. While the focus on specifics of population prioritization, service delivery models, innovative techniques and funding may, and likely will, wax and wane, progress is predicated on some degree of unison. 120 Ministries of Health, international normative bodies (e.g. WHO and UNAIDS), national normative bodies (e.g. Centers for Disease Control in the United States) and other organizations (e.g. AIDS Vaccine Advocacy Coalition) played key roles in building consensus around global advocacy and key policy guidance on VMMC to encourage partner country governments to adopt and act on the guidance provided. This resulted in the creation of a clearing house with the intent to share information and resources among stakeholders.121,122 Similar efforts for oral PrEP will be necessary to advance the agenda for implementation worldwide, including engagement with community key populations groups and networks, such as the Asia Pacific Coalition on Male Sexual Health and others. 123
Conclusion
VMMC and PrEP are not one and the same. Different segments of the population can benefit differentially from these two HIV prevention interventions. Also, while VMMC is a one-time intervention with lifelong benefits largely devoid of daily adherence considerations, oral PrEP effectiveness depends upon consistent adherence. Such differences must be appreciated. Nonetheless, as VMMC and oral PrEP are both biomedical interventions intended to attract HIV-uninfected individuals in the common interest of remaining HIV-negative, there are important similarities that should be identified and leveraged as much as possible. Also, both rely upon awareness of HIV status, an aspect whose importance should not be underestimated, given the UNAIDS 90–90–90 strategy.
We have presented ten key lessons learned from over a decade of VMMC implementation efforts, which can be applied to current PrEP initiatives for faster and safer scale up and public health impact. National governments, implementers and community advocates are encouraged to delve into the learning synergies that exist to improve the effective implementation of both programmes.
Footnotes
Acknowledgements
We would like to thank John Crane for his assistance in preparation of the manuscript and formatting the references.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RRP receives compensation for consulting from Gilead Sciences and ViiV Healthcare. The other authors declare no competing interests.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.