
Abstract
Fostering Open eXpression among Youth (FOXY) is an arts-based HIV prevention program developed by Northern Canadians to address sexual health, HIV, sexually transmitted infections (STIs), sexuality, and healthy relationships among Northern and Indigenous youth in Canada. We conducted a pilot study with Indigenous and Northern young women aged 13–17 years from 17 communities in the Northwest Territories to evaluate whether, in comparison to pre-intervention, FOXY participants demonstrated increased knowledge of STIs, increased safer sex self-efficacy, and increased resilience. Wilcoxon test results indicated significant increases in STI knowledge scores and safer sex self-efficacy scores. Findings suggest that FOXY holds promise as an effective method of delivering sexual health information through peer education, and increasing STI knowledge, safe sex self-efficacy, and resilience.
Introduction
Sexually transmitted infections (STIs) cause a substantial and immediate threat to the health and wellbeing of young Canadian Indigenous women. While Indigenous populations (First Nations, Inuit, and Métis) comprise 4.3% of the Canadian population, this population accounted for 10.8% of new HIV infections in 2014. 1 The Public Health Agency of Canada also points to higher prevalence of other STIs, such as sevenfold higher rates of Chlamydia, among Indigenous adults in comparison with their non-Indigenous counterparts. 2 New HIV infections occur disproportionately among the adolescent and young adult population (15–29 years), representing 31.6% of HIV-positive cases compared to other age groups. 3 For Canada’s Indigenous women, the HIV infection rate is double that of the non-Indigenous population. 3 HIV infection among Canada’s young Indigenous women is influenced by factors such as mental health issues from historical trauma and racism, 4 alcohol and drug use,5,6 intergenerational poverty, 7 and limited availability of comprehensive and culturally relevant interventions to address these structural drivers of HIV. 8 While interrupting the transmission of HIV and STIs represents an urgent public health priority for the Northwest Territories (NWT), efficacious strategies for HIV and STI prevention among Indigenous young women in Canada remain an understudied area of research that also needs attention.
To slow down the spread of HIV and STIs among young people, public health researchers and service providers advocate for the development and implementation of innovative health promotion programs that better engage young populations. 9 These programs should encourage the incorporation of information on social and peer norms while leveraging protective health behaviors, thus empowering participants with the skills necessary to make informed sexual health decisions. 10 Specific to HIV and STI prevention programs, arts-based interventions are prominent in the literature as promising methods for reaching and engaging youth, modifying sexual behavior outcomes among adolescents, and addressing public health concerns among other marginalized populations.11,12
Current evidence on the public health impact of arts-based interventions among adolescents documents several positive outcomes. 11 Unlike didactic teaching methods, arts-based interventions provide an interactive environment while recognizing the knowledge, experiences, and contributions of program participants.13,14 This environment enables participants to engage socially and emotionally, while at the same time influencing behavior modification.14,15 Furthermore, arts-based interventions can address cultural considerations while providing participants with consistent messaging aimed at skill development tailored to influence specific behaviors for change.16,17 The use of peer educators who can easily identify with the developmental challenges of adolescents is praised as a strength of these interventions.18–20 Arts-based interventions allow for participants to learn in a fun environment where their personal experiences are welcomed and utilized to enhance sexual health education curricula. 11 Finally, adolescents who participate in arts-based interventions find them informative, inclusive, acceptable, fun, and memorable.12,21 Current literature indicates that there is a need to include rigorous evaluation while developing accessible, engaging, and culturally appropriate arts-based sexual health education to increase the replicability and generalizability of interventions.
Research on the public health impact of arts-based interventions among adolescents is still emerging. 13 There is a paucity of evidence regarding rigorously evaluated interventions utilizing samples of adolescents from Indigenous populations, where the incidence of HIV is increasing. 22 While arts-based interventions are gaining popularity among adolescent health researchers and practitioners, the impacts of these interventions on improving the sexual health of adolescents are less known. Through developing and testing a peer-led, age-specific, and culturally relevant arts-based intervention, the current study will add to the emerging literature on the effectiveness and generalizability of arts-based interventions among Indigenous adolescent women in Canada.
This manuscript describes the implementation of Fostering Open eXpression among Youth (FOXY), an arts-based intervention developed by Northern Canadians for adolescents across the NWT delivered by peer educators. Our primary objective was to evaluate whether, in comparison to pre-intervention, adolescent women who attended FOXY demonstrated increased knowledge of STIs. Our secondary objective was to examine if, in comparison to pre-intervention scores, participants who received the FOXY intervention would report the following changes in scores at the post-intervention evaluation: (1) increased safer sex self-efficacy and (2) increased resilience.
Methods
Participants
FOXY project staff recruited potential participants from secondary schools across the NWT from September 2015 to May 2016. Active recruitment methods were utilized to establish contact with potentially qualifying program participants, including school outreach, use of volunteers at high schools, and referrals from friends of participants. All potential program participants were screened to determine eligibility through the following criteria: individuals self-identifying as female, residing in the NWT, willing to attend FOXY, aged 13–17 years, and capable of providing informed consent.
Study procedures
The study consists of a multicenter nonrandomized pragmatic cohort pilot using a pretest/posttest design approved by the Ethics Review Board at the University of Toronto and the Aurora Research Institute. Eligible study participants completed a baseline assessment before attending a FOXY intervention. Immediately following completion of the FOXY intervention, participants completed a post-intervention evaluation. Trained facilitators and adolescent peer leaders on staff cofacilitated these sessions.
Intervention components
FOXY is an interactive arts-based HIV prevention program that addresses sexual health, HIV and STIs, sexuality, and healthy relationships among Northern and Indigenous youth in Canada. A unique component of FOXY is the use of arts-based methods and peer facilitation to educate without judgment. The FOXY intervention involves seven workshops lasting between 1 and 2 hours each and conducted over 1–2 days in communities across the NWT (see the study protocol for further details regarding content of a typical FOXY workshop). 23 Each workshop hosts 8–15 participants and is led by professional facilitators and trained peer leaders with expertise in sexual health education and arts-based HIV prevention.
Data collection
Cross-sectional surveys were administered directly before the FOXY workshop and directly following the workshops. We used venue-based sampling to recruit participants from Grade 7 to 12 classes at secondary schools in 17 communities across the NWT: Aklavik, Whati, Fort McPherson, N’Dilo, Lutselk’e, Fort Liard, Fort Simpson, Yellowknife, Ulukhaktok, Fort Resolution, Behchoko, Inuvik, Tuktoyaktuk, Hay River, Katlodeeche First Nation, Fort Smith, and Norman Wells. Self-administered structured surveys assessed sociodemographics, STI knowledge, safer sex self-efficacy, and resilience. Participants received remuneration valued at $25 (a FOXY branded t-shirt) for the baseline assessment and post-intervention assessment.
Outcome measures
Three primary outcome variables were used to assess the efficacy of the FOXY intervention in increasing STI knowledge, safer sex self-efficacy, and resilience. Since these measures were based on self-report, to enhance the validity of participants’ responses, the researchers collected posttest assessments immediately following the intervention to optimize recall of knowledge.
STI knowledge outcomes
Items regarding STI knowledge (Cronbach’s Alpha = 0.765, range = 1–14) were adapted from a previous study. 24 Participants were asked to indicate true or false to a 14-item scale (score range 1–14).
Safer sex self-efficacy outcomes
This scale measured participants’ current confidence in using condoms consistently in a variety of situations with different partners. 25 The measure consisted of five items assessed on a five-point Likert scale. We computed a mean score such that higher scores indicated greater safer sex self-efficacy (Cronbach’s Alpha = 0.864, range = 1–4).
Resilience outcomes
Using the Child and Youth Resilience Measure 26 (Cronbach’s Alpha = .875, range = 1–12), participants were asked to rate the availability of individual, relational, communal, and cultural resources. The measure consisted of 11 items assessed on a five-point Likert scale.
Statistical analysis
Descriptive statistics were used to explore the sociodemographic (e.g. age, sexual orientation, parents attended residential schools, dating relationship) characteristics of the sample. A Kolmogorov–Smirnov test was used to test for normality on all outcome variables. Due to the nonnormality of the outcome variables, a Wilcoxon test was conducted to evaluate whether participants had improved their STI knowledge, safer sex self-efficacy, and resilience before and immediately after the intervention. The data were analyzed using IBM SPSS 23.
Results
Descriptive characteristics
As shown in Table 1, among participants (n = 199), 20.5% (n = 39) identified as sexual minorities; most participants 79.4% (n = 154) identified as Indigenous. More than half of the participants reported depressive symptoms (59.8%; n = 119), and over one-third of participants reported food insecurity (31.7%; n = 63). Approximately one-quarter (27%; n = 53) were in a dating relationship. About 34.5% (n = 67) used one or more substances (e.g. alcohol, weed, coke, speed, ecstasy) in the three months prior to the survey. Regarding sexual practices, 12.1% (n = 24) of adolescent women reported engagement in oral sex, while 17.7% (n = 35) engaged in vaginal sex. When asked if they perceived themselves to be at risk for either HIV or STIs, 14.6% (n = 29) of participants believed they were at risk for HIV and 18.6% (n = 37) believed they were at risk for STIs.
General characteristics of Northern adolescent women at baseline (N = 199).
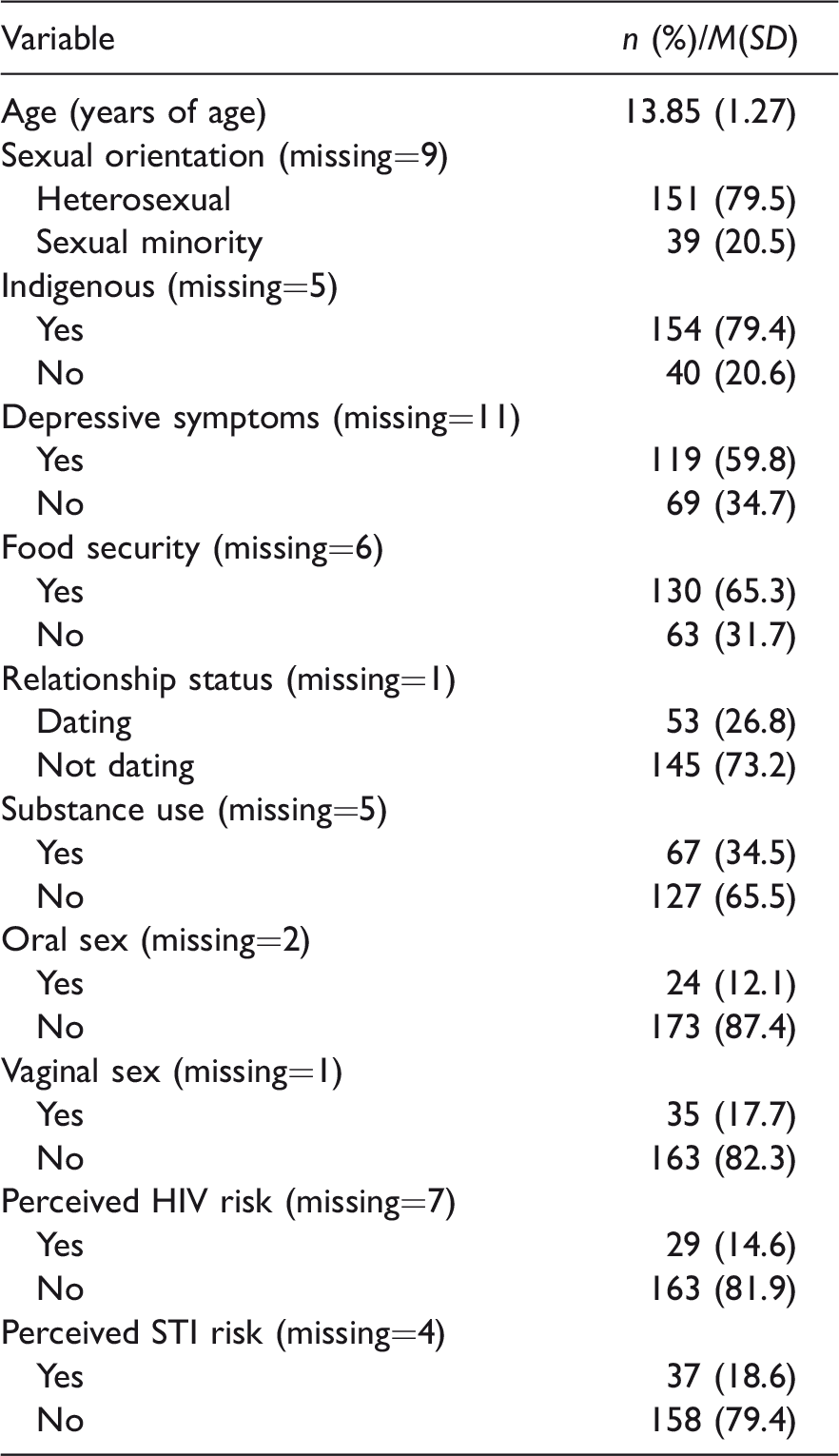
STI: sexually transmitted infection.
Note: The percentages are calculated to exclude missing values.
Pre-intervention outcome measure scores differed by certain sociodemographic characteristics: depressive symptoms, Indigenous identity, sexual orientation, and food security. Participants with depressive symptoms reported increased STI knowledge (M = 4.59, SD = 1.54) compared to participants without depressive symptoms (M = 4.06, SD = 1.42). Adolescents who identified as Indigenous reported lower resilience scores (M = 38.57, SD = 9.51) compared to non-Indigenous participants (M = 41.97, SD = 9.43). Sexual minorities reported lower STI knowledge (M = 3.82, SD = 1.27) compared to their heterosexual counterparts (M = 4.51, SD = 1.62). Adolescents experiencing food insecurity reported lower resilience scores (M = 36.41, SD = 9.21) and higher STI knowledge scores (M = 4.69, SD = 1.53) compared to participants who did not report food insecurity.
Pre- to post-intervention outcome differences
Table 2 reports the significant STI knowledge score median differences before (Mdn = 4) and after (Mdn = 9) the intervention (z = 9.740, p <0.001, r = 0.490). STI knowledge scores were significantly higher following the intervention. Safer sex self-efficacy scores were significantly higher following the intervention (Mdn = 88) in comparison with pre-intervention scores (Mdn = 82), z = 4.110, p < 0.001, r = −0.220. After attending the FOXY intervention, participants reported slightly higher resilience scores (Mdn = 41) compared to pre-intervention (Mdn = 40), z = −2.820, p < 0.010, r = 0.140.
Differences in outcome scores from pre- to post-intervention.
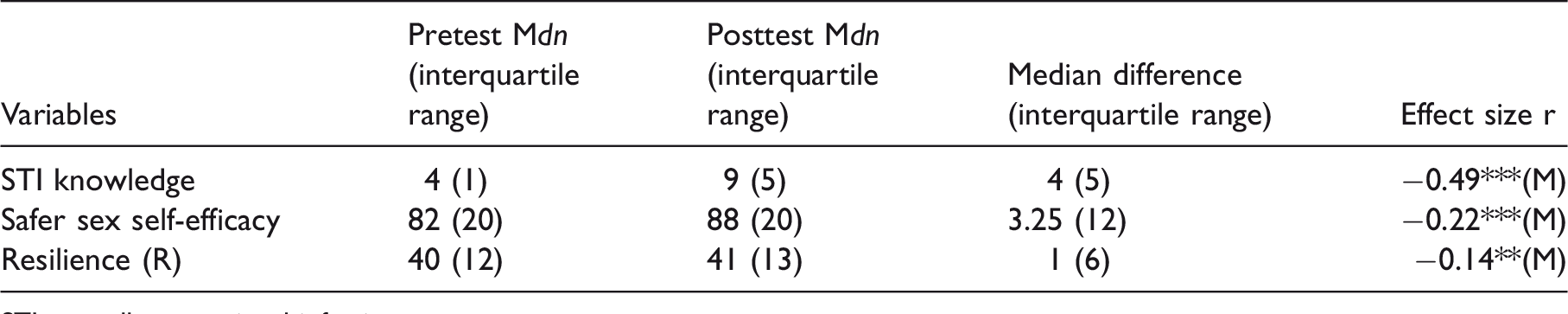
STI: sexually transmitted infection.
*p < .05, **p < .01, ***p < .001 for asymptotic two-tailed Wilcoxon Signed Ranks Test.
(M) = moderate effect size with r smaller or equal to −0.3 but larger than −0.5; (L) = large effect size with r smaller or equal to −0.5.
Median difference is calculated based on postscores minus prescores.
Discussion
This study reports on an assessment of the feasibility and efficacy of FOXY, an arts-based HIV and STI prevention intervention implemented with young women in the NWT, a region with Chlamydia rates ten-fold that of Canada’s national prevalence. 27 This study provides the first statistical support for the feasibility and initial indicators of the FOXY intervention, demonstrating increases in participants’ STI knowledge, safer sex self-efficacy, and resilience. We had high study completion (90%), suggesting acceptability of FOXY among Northern and Indigenous young women. Though evaluative data on the effectiveness of arts-based interventions among Indigenous young people are scant, our study demonstrates that the application of interactive approaches appears to hold much promise for HIV and STI prevention among young Indigenous and Northern women in Canada.
According to Coyle et al., 28 for an HIV or STI prevention program to be efficacious, the intervention should be interactive, age specific, and geographically and culturally relevant in order to increase the uptake and retention of sexual health information. To our knowledge, there is a dearth of studies that have evaluated the effectiveness of arts-based HIV and STI prevention interventions among Indigenous and Northern young women, particularly in the Canadian context. Our pilot findings suggest that FOXY holds promise as an effective method of delivering sexual health information, and increasing STI knowledge, safer sex self-efficacy, and resilience. 29 In addition, our study is consistent with prior research on the importance of peer educators on providing an encouraging environment for adolescents to share potentially sensitive information about their sexuality and sexual practices.19,21
This study has limitations, and therefore, the results should be interpreted with caution. First, the nonrandom sample and lack of a control group limits the generalizability of our findings. The use of a convenience sample may have biased the evaluation toward overestimating the benefits of FOXY. Furthermore, the risk of measurement error might be high due to reliance on self-reports, raising the risk of social desirability. However, our team of trained researchers and peer leaders implemented several measures at the outset of the study to minimize the limits of self-report, including expert review of the instruments and pilot testing surveys with peer leaders. Since this study reports preliminary findings of the FOXY intervention, it is too early to assess whether the effects of the interventions hold over time. Therefore, there is need for longitudinal studies to evaluate the long-term outcomes of the FOXY arts-based HIV and STI prevention intervention.
Furthermore, there were several challenges with implementing the intervention. Sexual health can be a sensitive subject for some individuals, so great care was taken during the development of the intervention to ensure that it was developmentally and culturally appropriate for Northern youth. This attention to detail prolonged the development phase of the intervention. Also, delivery of the intervention occurs in a dynamic environment with logistical challenges such as limited airline schedules, weather delays while traveling, and unforeseen complications such as community events or funerals that may interrupt the delivery of interventions in the NWT or require flexibility for facilitators to accommodate community needs.
Despite these limitations, this study offers strong preliminary evidence on the feasibility of arts-based interventions as an HIV and STI prevention approach and provides foundational details to inform the improvement and future scale-up of the FOXY intervention. 23 We demonstrated the importance of combining peer education with arts-based approaches in advancing HIV and STI prevention with young Northern women. Our sample’s demographics were representative of adolescent females in the NWT, with rates of depression and sexual practices similar to national health surveys.5,7,8 This suggests that the findings from this pilot study may be applicable to other Northern and Indigenous adolescent women who may face similar experiences in other regions of Canada outside the NWT. With limited evaluations of arts-based interventions in Canada focusing on sexual health, we compare our findings to interventions implemented in the United States, United Kingdom, South Africa, and Australia that reported similar findings regarding increases in STI knowledge, safer sex self-efficacy,10,12,30 and resilience.21,31,32
In Canada, Indigenous peoples have HIV infection rates 2.7 times higher than their non-Indigenous counterparts. 1 This high rate of HIV infection underscores the urgency for building an evidence base of efficacious, innovative, and comprehensive HIV/STI interventions that are developed and led by Indigenous peoples.4,7,23,33 Scant published research has evaluated the effectiveness of arts-based interventions among Indigenous adolescent women in the Canadian North and this pilot research adds to the knowledge base of promising approaches to HIV and STI prevention with Northern and Indigenous young women. 23 HIV and STI prevention interventions that are tailored for the unique needs and lived realities of Northern and Indigenous young women are interactive, engage with peers in a group-based format, leverage the protective factors of resilience, and take into consideration the developmental and cultural context of participants have potential to promote sexual health and wellbeing in the NWT.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the Canadian Institutes of Health Research and the Public Health Agency of Canada for the research of this article. CM was also supported by an Ontario Ministry of Research & Innovation Early Researcher Award.