
Abstract
Guidelines highlight the need to increase HIV testing among men who have sex with men (MSM) and novel point-of-care testing provides new possibilities for delivery of care. However, it is unclear how point-of-care testing should be used to best effect. This study aimed to increase understanding of sexual risk-taking behaviour, service use, and attitudes to point-of-care testing among MSM sauna clients. Data were collected within two saunas for MSM in south west England using a self-completion survey (n = 134). Though this sample of MSM sauna clients are at high risk of acquiring a sexually transmitted infection, the testing frequency among the majority of those reporting unprotected anal intercourse is not in keeping with national guidelines. For almost all participants the introduction of rapid point-of-care testing for both genital and blood-borne infection was likely to increase testing and for the majority NHS specialist services was the preferred setting.
Keywords
Introduction
Gay, bisexual, and non-identified men who have sex with men (MSM) continue to be disproportionately affected by sexually transmitted infections (STIs), 1 including HIV. 2 Sex between men remains the principal mode of transmission of HIV infection in the UK, with the number of new HIV diagnoses among MSM in 2012 exceeding new diagnoses in heterosexuals for the first time in over a decade. 2 Gonorrhoea and chlamydia are the most commonly diagnosed STIs amongst MSM 1 and their rising incidence, 1 along with HIV, 3 suggest that current services are failing to provide appropriate healthcare. Increasing testing for HIV and STIs among MSM in the UK is a priority for the NHS.3–5 National guidelines advocate developing opportunities to increase testing in individuals not currently accessing mainstream services and recommends the use of rapid HIV point-of-care tests (POCT) via outreach in venues where there is high-risk sexual behaviour. 5 Previous research has demonstrated that saunas may represent important sites of HIV transmission among MSM.6–10
Providing STI testing in community settings is advocated as they can facilitate access to individuals at high risk of sexual infection who test infrequently or not at all and can be beneficial in certain environments, such as saunas. 6 The introduction of POCT is appealing as results, counselling, and treatment can be delivered in a single contact and individuals are more likely to receive timely and appropriate treatment. This provides an opportunity to reduce the likelihood of onward infections. Early economic modelling has suggested that the added cost implications for the use of POCT, compared to laboratory-based tests, are outweighed when the whole care pathway is considered. 11 With the development of simpler and more accurate rapid HIV POCT and POCT for gonorrhoea and chlamydia becoming available, the use of rapid POCT is likely to increase.12–14 There is variation in the reported acceptability of providing POCT in community settings, especially commercial sex-on-premises venues such as saunas,15–18 suggesting the need for further consideration of the most effective use of POCT.
Most acceptability studies of STI testing have been conducted with community samples of MSM 18 and it is not clear if MSM who are at increased risk of STIs find POCT acceptable and whether their introduction will have the potential to increase levels of STI and HIV testing. MSM who engage in STI risk behaviour are more likely to attend saunas than men who do not engage in STI risk behaviour.9,10,19 Therefore saunas provide an opportunity to examine the acceptability of POCT within this high-risk population. This study aimed to increase knowledge of types of risk taking, sexual health service use and views on rapid POCT among MSM sauna clients.
Materials and methods
Study design and data collection
An anonymous self-completion survey was developed on a tablet device. Piloting was undertaken through four rounds of cognitive interviewing with a convenience sample of 16 MSM, in order to evaluate the face validity of the survey. Piloting highlighted issues with question comprehension and interpretation, response problems, and the acceptable level of disclosure for participants. Following each round of cognitive interviewing the study team met to discuss the results and necessary refinements were made. The final version of the survey contained 63 questions which recorded socio-demographic characteristics, sexual health service use (location and recency of HIV and other STI testing), sexual behaviour in previous three months (number of sexual partners and frequency of protected and unprotected anal intercourse), and views on POCT. The study was approved by the Faculty of Medicine and Dentistry Committee for Ethics at University of Bristol.
Study recruitment
Men were recruited from the only two saunas for MSM in Bristol between July and September 2013 using time and location sampling to optimise representativeness of the sample. Each day of the week was divided into three four-hour recruitment shifts. Afternoon covered 2–6 pm, evening 6–10 pm, and late night 10–2 am. Shift selection was guided by the expected number of visitors at each sauna, with weekends (Fridays–Sundays) being sampled more frequently. Overall a total of 16 survey sessions were conducted across both venues.
Recruitment and survey completion occurred contemporaneously. All men were given a study information leaflet on arrival at the sauna by reception staff, and then later approached by researchers about survey recruitment. Men were not eligible if they were unable to read English, were unable to give consent due to cognitive impairment, or had already participated. The first screen of the survey reiterated study information and consent was provided by participants selecting the ‘start’ button. Participants were reimbursed with a £10 voucher for their time.
Statistical analyses
Data were analysed using descriptive statistics including frequencies and percentages. Chi square tests were used to assess associations of testing behaviour and views of POCT with high- and low-risk behaviour. Stata™ (version 13.0, 2013) was used for all analyses.
Results
A total of 134 sauna clients completed the survey, representing a response rate of 74%. The survey took a mean of nine minutes to complete. Two participants required a researcher to verbally administer questionnaires due to visual problems.
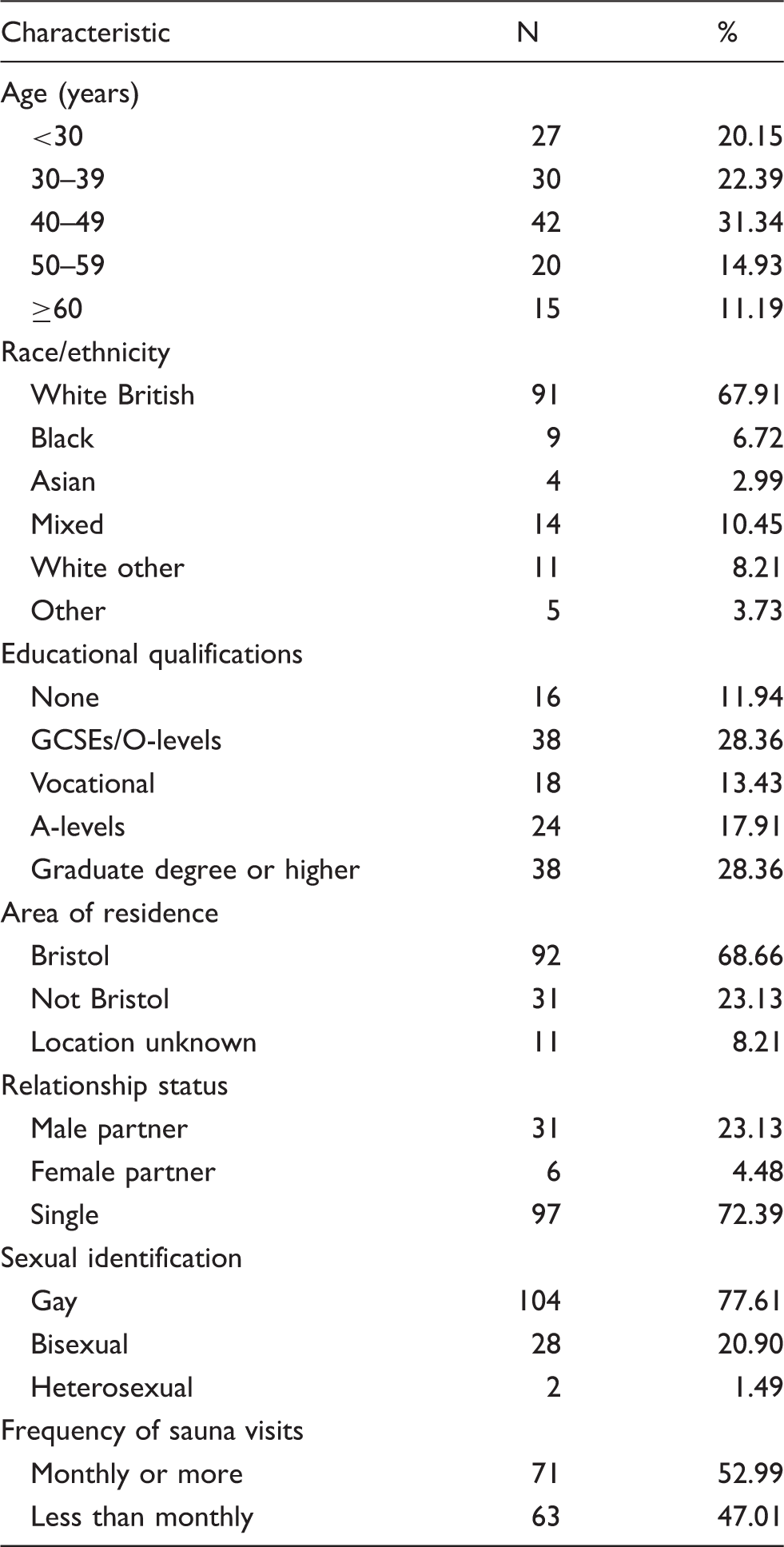
Participant characteristics
Demographic characteristics, N = 134.
Sexual behaviour in the previous three months
Sexual behaviour in previous three months.
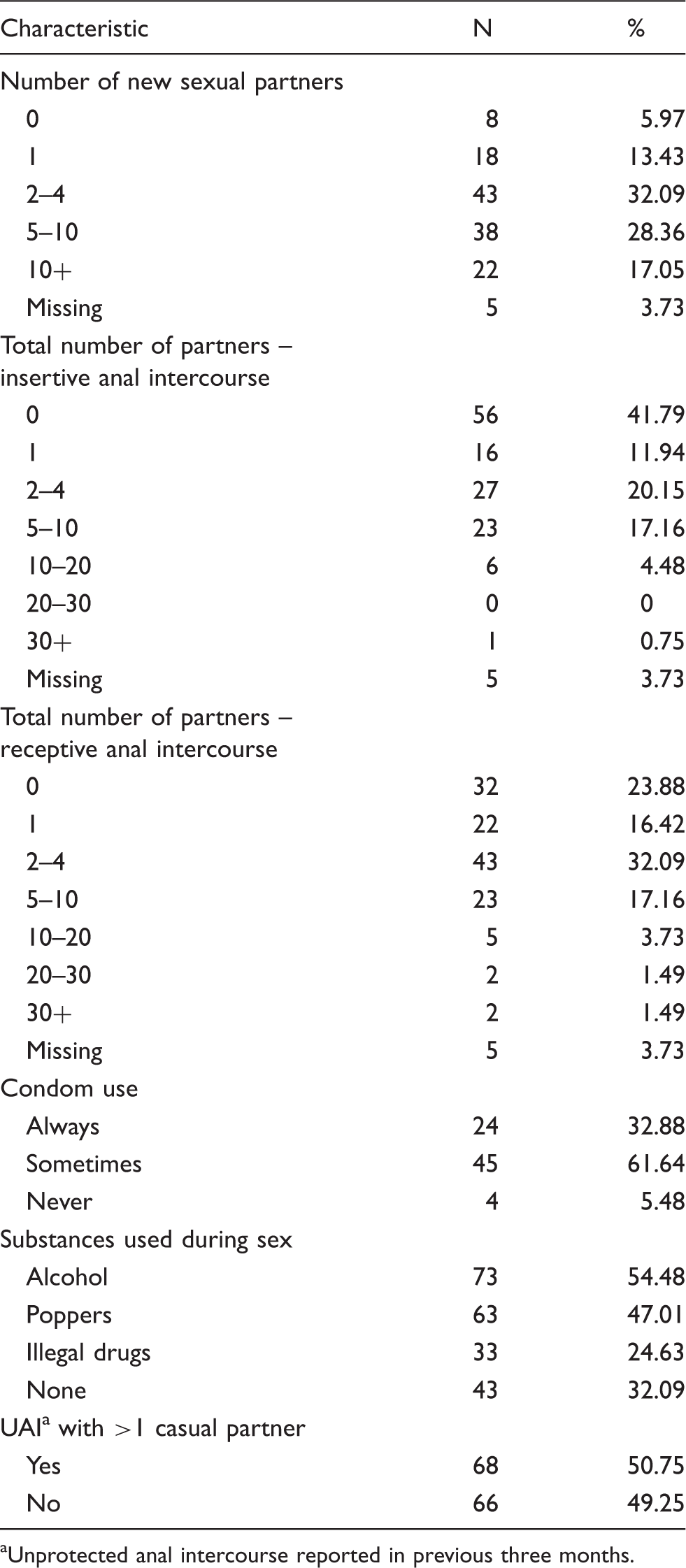
Unprotected anal intercourse reported in previous three months.
Sexual health
Sexual health and HIV.
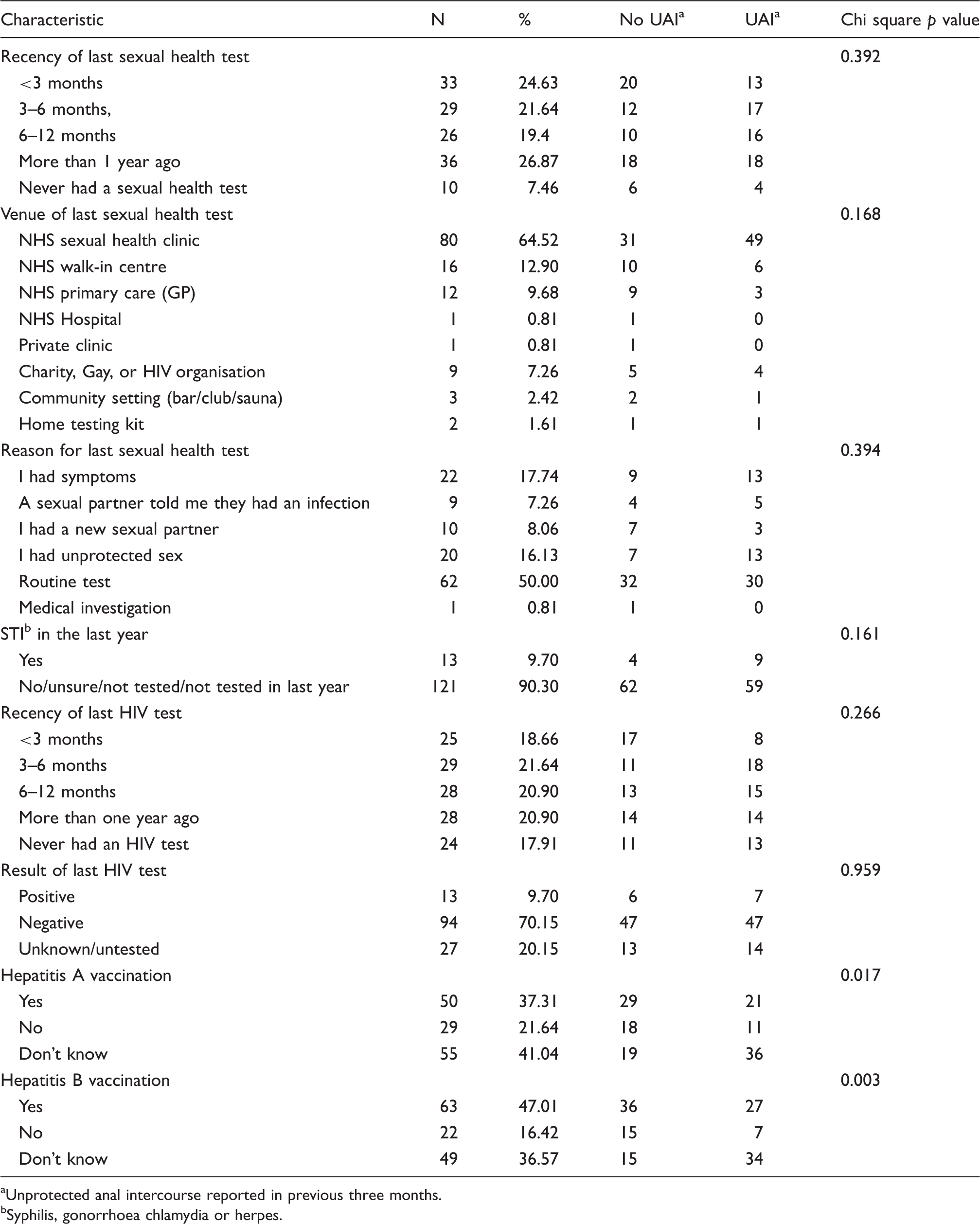
Unprotected anal intercourse reported in previous three months.
Syphilis, gonorrhoea chlamydia or herpes.
HIV
The majority of participants (82%, n = 110) reported having tested for HIV. For 82 (61%) men the most recent HIV test was within the previous 12 months, and for 25 (19%) within the previous three months. Of the 110 men who reported having had an HIV test, over half (55%, n = 60) described this as part of a regular STI test, and 13 (12%) reported knowing they were HIV-positive, 94 (85%) HIV-negative, and for three (3%) the results of the tests were unknown. Considering the sample as a whole, 27 (20%) men did not know their HIV status, 13 (10%) were HIV-positive, and 94 (70%) HIV-negative according to their most recent test results. HIV tests were performed most frequently within NHS sexual health clinics (70%, n = 77). Among the 68 men reporting UAI in the previous three months, 41 (60%) reported having an HIV test in the previous 12 months and eight (12%) in the previous three months. A fifth of the men reporting UAI did not know their HIV status (21%, n = 14), while seven (10%) were HIV-positive and 47 (69%) HIV-negative according to their most recent test results. Among the 121 men who reported having had a new sexual partner in the last three months, 20 (17%) reported that they had been tested for HIV in the previous three months.
Views on rapid point of care tests
Views on point-of-care testing (POCT).
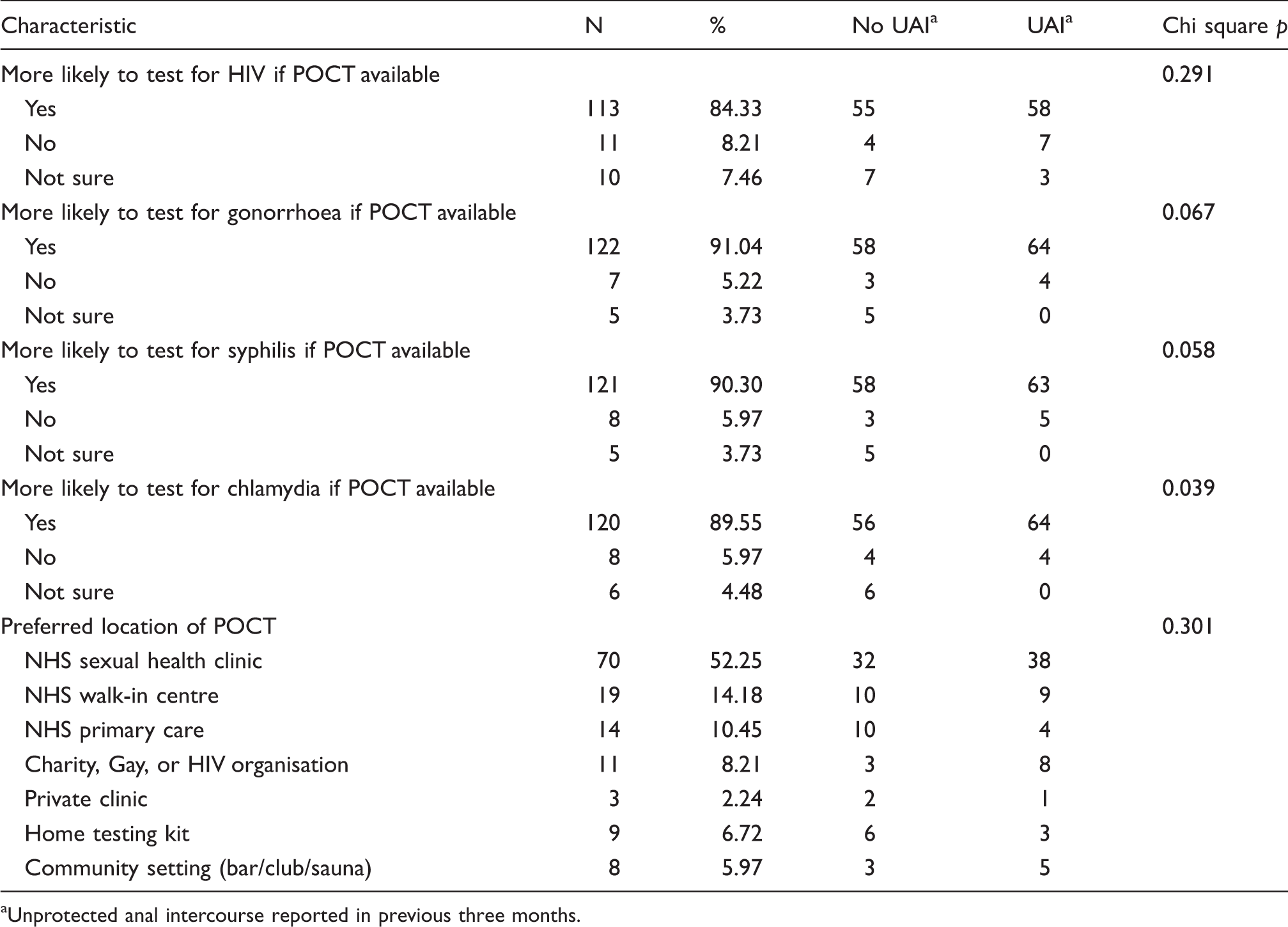
Unprotected anal intercourse reported in previous three months.
Discussion
The survey findings indicate high levels of sexual risk-taking among sauna clients. The majority of participants reported multiple sexual partners and half reported UAI in the previous three months putting them at high risk of acquiring an STI. Whilst the majority of men reported having an STI and HIV test in the past year, only a minority of those reporting UAI had been tested in the previous three months. The introduction of rapid POCT for HIV and STIs received overwhelming support from participants.
Survey participants reported more new casual sexual partners and higher frequency of UAI than UK community samples of MSM recruited from gay bars 21 or national surveys. 22 Over half of the men reported engaging in UAI in the previous three months and therefore at high risk of acquiring an STI and HIV infection. This is in line with previous estimates of frequency of UAI by sauna clients of 30%–64%.6,7,10,19
Previous research has linked higher frequency of UAI with new partners for men who attend saunas, but provides conflicting estimates of UAI in relation to where sexual behaviour took place. Some studies report higher frequency of sexual risk behaviour in saunas, 23 while others demonstrated that men may be less likely to engage in UAI on sauna premises than in a private home. 19 However, our data confirms that men who attend saunas are likely to engage in sexual risk behaviour with multiple casual sexual partners which can facilitate disease acquisition. As participants were asked to report all sexual behaviour during the previous three months, we cannot demonstrate that sexual encounters that took place in saunas were more likely to result in UAI than encounters with partners that took place elsewhere.
Recent UK guidelines recommend annual HIV testing for all MSM5,24,25 and every three months if changing partners regularly 25 or ‘at highest risk’ of HIV infection. 24 Our data demonstrate that the guidelines are not being met despite the high level of risk of sexual infection in this setting. Although the majority of men in our survey reported an annual HIV test, only around one in ten of the men who reported UAI had taken an HIV test in the previous three months. Therefore current services are failing to provide appropriate care to large numbers of MSM at high risk of ill-health. This is particularly pertinent in relation to our finding that a fifth of the men reporting UAI had never been tested for HIV and were unaware of their status. Although community samples of MSM indicate a higher proportion of men untested for HIV compared to our sample, 26 the higher reported frequency of multiple sexual partners and UAI21,22 within our sample suggests a greater risk of HIV infection. Strategies to increase HIV testing and normalise HIV testing amongst MSM are a priority to reduce undiagnosed and late diagnosed HIV and are vital in improving individuals’ prognosis and reducing onward transmission of infection.3–5,26
Our data demonstrate strong support among MSM sauna clients for the initiation of POCT for both genital and blood-borne infections, including HIV, with many participants commenting that POCT testing would be more attractive and less stressful than the current one to two week wait for test results. Previous research indicates that people are more likely to attend for HIV and STI testing if results and post-test services, including treatment, are available during the same visit and the service is delivered by staff with specialist knowledge. 13 The introduction of POCT has been demonstrated to make HIV testing more acceptable and increase the uptake14,17 and even be a motivating factor for individuals to attend for screening. 27 The performance of some POCT technology for detecting gonorrhoea and chlamydia, the two most common treatable bacterial STIs in MSM, 1 has been disappointing, but recently more reliable POCT for gonorrhoea and chlamydia 12 have become available. Although this requires the purchase of new equipment, this opens up the opportunity for same day complete sexual health screening for MSM, with results available in about an hour. By attempting to increase testing and reduce time to treatment, the introduction of POCT can provide an opportunity to reduce onward transmission of disease and ultimately prevalence of HIV.1,5,12,13,15,17,28,29 However, although it has been demonstrated that the introduction of HIV POCT may increase HIV testing in MSM, it has not resulted in a sustained increase over time. 30 Therefore the introduction of POCT needs to be part of a wider health promotion strategy.5,26
The UK National Institute for Clinical Excellence (NICE) has advocated offering rapid POCT via outreach in community venues, including venues that facilitate sex between men such as saunas, to increase uptake of HIV testing amongst MSM. 5 The majority of MSM in our survey demonstrated a preference for the introduction of rapid POCT within NHS specialist sexual health services rather than community and commercial venues such as saunas. The majority of participants were familiar with NHS specialist sexual health services and currently attended for hepatitis vaccinations and STI and HIV testing, but not within guideline frequency. Our findings are in line with previous research which has also reported that community samples of MSM find existing NHS sexual health services setting more acceptable for STI screening than community venues. 18 Previous research has suggested that a preference for STI screening in traditional NHS specialist sexual health services over community-based outreach could be due to concerns in relation to the suitability of sex-on-premises environments for rapid POCT for HIV, apprehension about the ability to ensure confidentiality, a preference for maintaining boundaries between sites of sexual pleasure and healthcare, and the possibility of testing with a negative result leading to disinhibition or unprotected sex. 16
Our findings could have implications for the cost effectiveness and suitability of providing POCT for MSM in community venues because this was the preferred location by only a minority of our participants. However, our study only provides preliminary evidence and further research is needed to investigate whether the introduction of a same day complete sexual health screening at NHS specialist services results in sustained increases in testing amongst MSM.
We found limited differences between men who reported UAI and those that did not report UAI. This may be due to there being no association or because the study was not powered to find an association due to the small sample size which is a limitation of the study. However, the use of time and location sampling method to recruit participants ensured sauna clients attending at different times and days an equal probability of inclusion in the survey and our study surveyed a range of sauna clients in relation to age, ethnicity, educational level, and frequency of sauna attendance. However, the narrow inclusion criteria of our sample may limit the generalisability of our findings to the wider population of MSM.
In conclusion, this study indicates that MSM attending saunas remain at high infection risk. HIV testing within the group was less frequent than guidelines recommend and the majority of sauna clients said they were more likely to test for HIV, gonorrhoea, chlamydia, and syphilis if rapid POCT were available. The data suggest that MSM attending a sauna prefer STI and HIV testing within NHS specialist sexual health services rather than community settings. Therefore, introduction of rapid POCT within these services may improve healthcare for this group.
Footnotes
Acknowledgements
We would like to thank the sauna owners and staff and all the men who took part in the study. Without them, this study would not have been possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the David Telling Trust [grant number 303].