
Abstract
Falls are a leading cause of injury and disability among older adults, yet sex-specific differences in fall biomechanics and injury mechanisms remain underexplored. This narrative review synthesizes current evidence on how fall circumstances, intrinsic risk factors, and biomechanical responses differ between older males and females. A comprehensive literature search was conducted using PubMed, ScienceDirect, and Google Scholar, with search terms including “fall biomechanics,”“sex differences,”“older adults,” and “injury risk.” We screened peer-reviewed studies and included English-language, human-based research that examined sex-specific fall patterns, injury outcomes, and biomechanical factors. Our findings reveal that while males are more likely to fall from seated positions, females more commonly fall while walking and are prone to sideways and backward falls—patterns associated with increased hip and head injuries. In addition, biological differences such as lower injury thresholds, reduced muscle strength, and distinct soft tissue composition further elevate injury risk in females. Despite these differences, most injury models and prevention guidelines remain male-centric or do not consider sex differences. Our findings underscore the need to integrate sex-specific anatomical and functional characteristics into fall prevention strategies and injury prediction models to improve outcomes for both sexes.
Keywords
Introduction
Falls remain a leading cause of injury, disability, and loss of independence in older adults, with over one-third of individuals aged 65 and older experiencing at least one fall annually. 1 These falls often lead to secondary complications such as fractures, hospitalizations, and functional decline. 2 Emerging evidence suggests that sex differences play a critical role in fall patterns, injury locations, and outcomes. 3 Yet, these differences are seldom addressed in clinical guidelines or biomechanical frameworks, despite their implications for injury prevention.4–7 To understand how these sex-specific patterns affect injury risk, it is essential to first recognize that falls are fundamentally biomechanical events. A fall can be described as an unintentional collision with the ground due to the force of gravity. During such events, external forces distribute across various body segments and tissues, and if these forces exceed the tissue’s tolerance, injury occurs. 8 These outcomes are influenced not only by extrinsic factors (e.g. fall direction or surface type) but also by intrinsic characteristics such as body composition and tissue stiffness. Therefore, understanding how sex influences both the mechanics of falling and the body’s response to force is key to designing effective prevention strategies. Despite this, many injury biomechanics models continue to rely on male-centric data, particularly the “50th percentile male,” a standard derived from average male anthropometry and historically used in crash-test and safety engineering. 9 These models do not account for critical sex-based physiological differences (e.g. fat distribution, bone density, and soft tissue composition) which can significantly influence injury thresholds. 10 Furthermore, experimental and computational studies of injury disproportionately use male participants and cadavers, skewing biomechanical predictions toward male norms.7,11 As a result, injury mechanisms that may be unique to females (especially older females) remain poorly understood. Moving beyond these generalized models requires integrating sex-specific anatomical and physiological data into biomechanical research and injury prediction tools.7,11
The disconnection between biomechanical research and real-world diversity has practical consequences. Existing fall prevention guidelines from major organizations, such as the American and British Geriatric Societies, as well as initiatives like the Centre for Hip Health and Mobility, rarely incorporate sex-based differences in risk profiles, behavior, or biomechanics.12,13 Likewise, many assistive devices (e.g. hip protectors and wearable sensors) are designed using male-focused data and fail to accommodate sex-specific anthropometrics or movement patterns, reducing their efficacy for female users.14,15 Even targeted approaches like hormone therapy only partially address this gap, 16 while broader strategies continue to treat all individuals the same. To enhance the effectiveness of fall mitigation efforts, there is a pressing need for sex-specific guidelines informed by a deeper understanding of how fall circumstances and injury mechanisms differ between males and females. In this literature review, we will present a review of the sex differences in fall circumstances, with a deeper focus on sex-specific intrinsic factors and how they affect the biomechanics of falls.
Methods
This narrative literature review aimed to identify and synthesize peer-reviewed studies examining sex differences in fall circumstances and biomechanics among older adults. The literature search was conducted using Google Scholar, PubMed, and ScienceDirect to capture a broad range of peer-reviewed research. Additionally, the reference lists of selected articles were manually reviewed to identify relevant studies not retrieved in the initial search. Search terms included combinations of keywords such as “falls,”“older adults,”“sex differences,”“fall biomechanics,”“injury risk,”“bone density,”“muscle strength,” and “fall prevention.” No date restrictions were applied to ensure inclusion of foundational biomechanics research in the search results. Studies were included if they were peer-reviewed, published in English, focused on older human subjects, and addressed sex differences in fall circumstances, biomechanics, or injury outcomes. Exclusion criteria included non-English publications, animal or cadaver-only studies without a focus on sex differences, and opinion pieces or editorials lacking original data. Articles were selected based on their relevance to the review objectives, and an iterative process of keyword searching and reference screening was followed until no new relevant studies were identified.
Results
Fall circumstances
Both males and females experience falls due to an incorrect shift of body weight, but the circumstances differ between the sexes. Males are more likely to fall while seated or shifting positions, while females are more prone to falling while walking. 3 Falls involving walking devices and falls from furniture or stairs are more prevalent in females.3,17 Home is the most common location for falls among both males and females, with factors such as flooring, furniture design, and stairs contributing to fall and injury risks. 18 While sex differences in these factors are not extensively documented, it is important to consider the unique needs of older adults of both sexes when designing safe living environments. 19 Additionally, the direction of falls influences injury patterns, with males experiencing more forward falls and females encountering more sideways and backward falls.20–22 This variation in fall direction impacts the vulnerability of different body parts to injury, with older males more prone to upper limb injuries and females more susceptible to hip and head injuries.23,24
Intrinsic factors
Numerous intrinsic factors have been identified as contributors to fall and injury risk, including conditions such as cognitive impairment, 25 arthritis and chronic diseases,26,27 age,27,28 sex, 26 previous history of falls, 28 insufficient activity,27,29 limitations in activities of daily living,27,30 impaired gait, 27 impaired mobility and stability, 27 visual acuity, 30 muscle weakness,26,27 long reaction times, 27 low body mass, 29 and weak grip strength. 27 Some of these factors cause a loss of balance, while others limit a person’s ability to correct the loss of balance. 31
In this review, our focus is on intrinsic factors that distinguish falls leading to injury from those that do not. Specifically, we will explore the sex differences in factors contributing to load transfer through the body and the resulting injury risk from falls, examining both structural (tissue properties) and functional (strength and reactivity) variables.
Structural factors
Bone
Fractures resulting from falls are common and debilitating injuries in older adults, as bone fragility increases with age, 32 and the aging process disrupts the bone repair process. 33 Both males and females experience adverse effects of natural aging on bone strength, 34 area, 35 and mass, 36 which are biomechanical factors influencing injury outcomes from falls. However, the impact of aging differs between sexes, with females exhibiting a higher prevalence of osteoporotic bones compared to males.32,37
Osteoporosis is more prevalent in older females and contributes to sex-specific vulnerability to fall-related injuries. 38 This condition compromises bone strength and is associated with structural deformities such as spinal curvature, which can impair balance and mobility.39,40 These impairments, combined with reduced physical activity due to pain and functional limitations, may explain the increased risk of falls observed in osteoporotic females.26,41 Although spinal deformities are prevalent in both older males and females, the underlying causes differ by sex, with female deformities primarily related to osteoporotic fractures and male deformities associated with disk degeneration and spondylosis. 42 Consequently, older females with spinal deformities often experience compromised balance, functional ability, and an increased risk of osteoporotic fractures. 42
The biomechanical characteristics of bones, including density, area, and area moment of inertia, play a crucial role in determining the injury threshold, which represents the maximum mechanical state a bone can withstand before an injury occurs (Table 1). Extensive research has shown that females generally have lower injury thresholds compared to males. 43 Notably, smaller females, weighing less than 50 kg, exhibit significantly lower neck injury thresholds than males under various loading conditions. 44 Similar observations have been made for other bones such as the femur and radius, highlighting that injury thresholds for females can be approximately half of those for males,45–51 making females more susceptible to injury at lower loading conditions. 44
Injury threshold in the large males, mid-sized males, and small females.
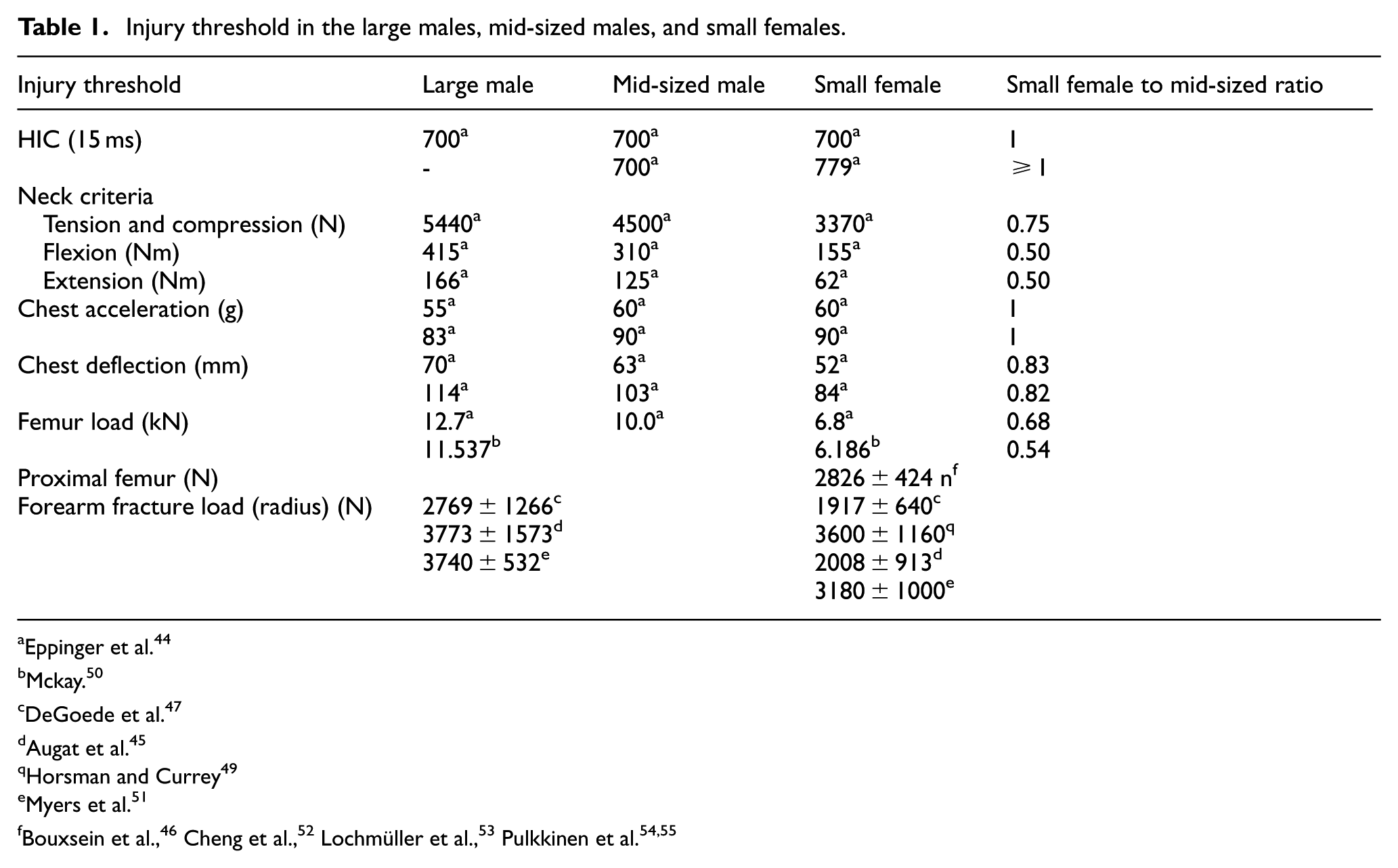
Eppinger et al. 44
Mckay. 50
DeGoede et al. 47
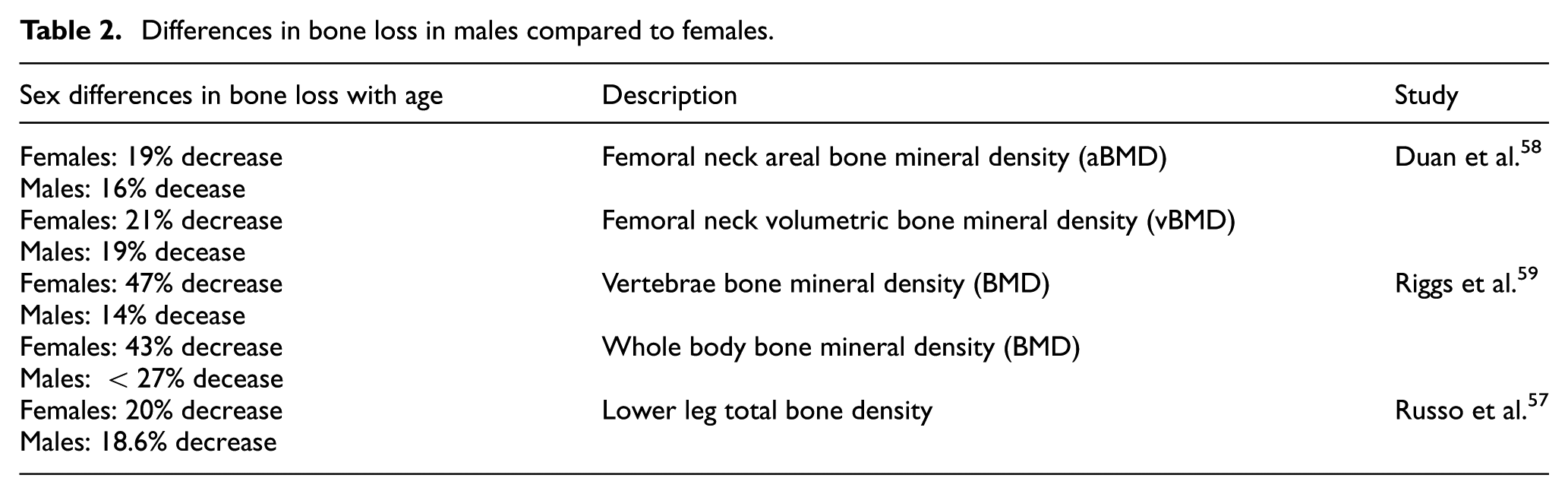
Previous research has consistently observed higher rates of bone loss in females compared to males. For example, studies conducted by Riggs et al. 56 and Russo et al. 57 reported sex-specific differences, with females exhibiting a greater rate of bone loss. However, it is noteworthy that Duan et al. 58 found a higher rate of bone loss in females compared to males, although this difference was not statistically significant (Table 2).
Differences in bone loss in males compared to females.
Soft tissues
In the context of low-loading impacts, such as falls, the significance of soft tissues cannot be overlooked, unlike high-loading impacts like automotive crashes. 60 These compliant soft tissues play a crucial role by deforming and absorbing the kinetic energy during a fall, thereby reducing the loading on bones, and the risk of injury. For instance, even a 1 mm increase in trochanteric soft tissue thickness can lead to a 71 N decrease in peak femoral forces exerted on the body. 61 Moreover, it was found to enhance tissue energy absorption by 1.7 J while reducing the body’s stiffness by approximately 50%.
Aging has been observed to impact the properties of these soft tissues, particularly in females. Older adults exhibited lower stiffness and damping characteristics of soft tissue over the hip compared to their younger counterparts. 62 This alteration in tissue properties can influence their ability to effectively absorb and distribute forces during a fall, potentially increasing the vulnerability to injury.
Furthermore, the decline in muscle mass, strength, and the development of sarcopenia significantly contribute to compromised coordination in daily activities.63,64 This age-related process substantially heightens the risk of falls and fractures, with nearly three times higher incidence compared to healthy adults.65–67 Both males and females experience a reduction in muscle mass as they age, with a higher rate observed in the lower extremities. 68 Notably, males exhibit a more pronounced decline in leg muscle mass compared to females, 69 while females generally have lower overall skeletal muscle mass compared to males. 70 Importantly, individuals with weaker leg muscles face a significantly higher risk of injury following a fall, 26 underscoring the crucial role of muscle strength in mitigating fall-related injuries.
Body mass index
Low body mass index (BMI) has been linked to a higher risk of hip fractures in both males and females. Those with a higher center of gravity are more likely to exert greater forces on their proximal femur during falls. 71 Studies have demonstrated that older adults with a higher BMI are less susceptible to hip fractures in the event of a fall, as the additional protective tissue around the hip provides coverage.62,72 Furthermore, the presence of increased gravitational forces, resulting from higher BMI and consequently higher forces on the bones, has been proposed as a contributing factor to the protection against hip fractures, particularly in females.73,74
The presence of sarcopenic obesity, characterized by reduced muscle mass and higher fat content, has direct implications for falls and fractures. 75 Sarcopenia itself is recognized as a risk factor for falls. 76 However, there are conflicting findings regarding the sex-specific rates of sarcopenic obesity. While Oh et al. reported higher rates in females, Batsis et al. found the opposite trend, albeit with higher mortality related to sarcopenia in females.77,78
Aging is associated with a significant increase in body fat, primarily observed in females. 69 However, both males and females experience an increase in the percentage of body fat as they age. 79 In males, there is a tendency to accumulate fat throughout their 50s, followed by a decline in both fat and lean mass after the age of 60. 76 Numerous studies consistently demonstrate fat gain in females, except for those aged over 80.80–86 Males are more likely to accumulate fat around the abdomen, while females tend to accumulate it in the lower extremities, particularly the hip region.75,87 The decline in basal metabolic rate over the years, with a steeper decrease in males compared to females, may contribute to increased fat deposition around the abdomen.79,88–90 Individuals with a higher distribution of fat around the abdomen are at a greater risk of falls due to the anterior location of their center of mass. 91
Functional factors
Numerous studies have emphasized the crucial role of muscle strength as a risk factor for falls.92–94 Strong muscles not only help prevent balance loss but also improve balance recovery and provide better support during grasping movements. 95 Notably, older adults with greater muscle strength exhibit enhanced balance recovery after tripping incidents. 96 The contribution of specific muscle groups to fall risk has been investigated by researchers. Studies have found that reduced hip and knee extensor strength significantly increased the risk of falling, with knee flexor and ankle plantar flexor strength also playing a role. 97 Interestingly, individuals with stronger knee flexors and ankle plantar flexors had a higher fall risk, possibly due to their higher walking velocity at the time of the trip, as observed in fallers compared to non-fallers. Stronger knee extensors and plantar flexors were associated with higher walking speed and, consequently, an increased risk of falling.97–99
Muscular strength plays a central role in fall risk through its influence on gait speed and balance recovery. 100 Muscle weakness often leads to slower gait and impaired balance—both established risk factors for falls. 100 Studies show that each 0.1 m/s reduction in an older adult’s usual walking speed is associated with approximately a 7% increase in fall risk, and individuals who fall tend to walk more slowly than non-fallers. 100 Conversely, greater lower-limb strength may paradoxically increase fall risk by enabling higher gait speeds at the time of a stumble. Pavol et al. 97 found that both the weakest and strongest older adults were at elevated risk of trip-induced falls: weaker individuals lacked the force to recover, while the strongest fell due to their higher walking speed and forward momentum. Sex differences in muscular strength and body composition further compound these risks. Frontera et al. and Sperling et al. reported that older females exhibit significantly lower strength in elbow flexors and extensors—approximately 60% and 48% of male strength, respectively.101,102 This pattern extends to lower-limb musculature. Aniansson et al. 103 showed that older females’ knee extensor isokinetic peak torque was roughly 55% of that of males, with Murray et al. and Borges observing similar differences in both extensors (∼74%) and flexors (∼53%).104,105 These sex-based differences limit women’s ability to arrest a fall or recover from balance loss. 24 Although stiffness differences between sexes normalize when adjusted for height and weight, females still tend to exhibit lower absolute stiffness—likely due to their smaller body size. 106 Taken together, the interaction between strength, speed, and sex-specific biomechanical factors highlights the importance of individualized fall prevention strategies.
In addition to strength, sensory and neuromuscular response factors show sex-specific differences relevant to falls. Visual acuity declines and slower reaction times are independent risk factors for falls, as they impair balance correction. For example, decreased visual acuity predicted approximately a 20% higher risk of falls and injurious falls in older adults. 107 Notably, older females experience more vision impairment than males. This greater visual deficit may partly explain women’s higher fall rates, since even among patients with poor vision, being female and having worse acuity markedly increase fall risk. 108 Likewise, reaction speed tends to be slower in older females. Males generally exhibit faster and more consistent reaction times than females across the lifespan, 109 and older females often require more time to regain balance during sudden gait disturbances. 110 Consequently, a slow postural reaction can prevent timely recovery from a trip or slip, elevating fall risk in older females relative to males. 27
Discussion
Falls among older adults are not only influenced by extrinsic factors such as environmental hazards but also by intrinsic factors that are sex-specific. The occurrence of falls and subsequent injuries vary between males and females, highlighting the need for sex-specific considerations in fall prevention strategies. Current fall prevention guidelines typically focus on addressing extrinsic risk factors and implementing interventions such as exercise programs and home modifications. Exercise interventions commonly include activities that improve balance and strength, while home modification interventions aim to identify and address potential hazards within the home environment. However, these guidelines often overlook the sex-specific differences in fall risk and injury patterns.
It is essential to recognize that sex differences play a significant role in both the occurrence of falls and the resulting injuries. While the guidelines for fall prevention do not currently incorporate sex-specific risk assessments and preventative strategies, it is crucial to acknowledge the impact of intrinsic factors specific to each sex.13,111 Individualized fall prevention strategies have been found to be more successful than standard approaches, taking into account the specific needs and lifestyles of individuals. 112 Several studies have highlighted the importance of incorporating sex-specific considerations into fall prevention interventions. By tailoring interventions to address sex-specific risk factors, such as differences in muscle strength, body composition, and anatomical structures, we can design more effective and efficient preventative measures.113–116
Considering the findings of this review, it becomes evident that incorporating sex-specific fall prevention strategies can lead to significant improvements in both the effectiveness and cost-effectiveness of interventions. By identifying sex-specific fall locations and understanding the sex-specific intrinsic risk factors, we can develop targeted and tailored strategies that address the unique needs of individuals. The current review highlights the sex-specific fall locations and body structures that require sex-specific interventions to lead to a time and cost-saving strategy design while improving the effectiveness of interventions. All the extrinsic and intrinsic sex-specific risk factors reviewed in the current paper suggest a sex-specific method to design preventative designs and safety standards.114,117
Conclusions
In conclusion, the current review emphasizes the importance of sex-specific fall prevention guidelines. While existing guidelines primarily focus on extrinsic factors, our review highlights that sex-specific intrinsic factors also significantly influence the occurrence and severity of injuries resulting from falls. The most pronounced sex differences identified include bone properties and injury thresholds, muscle strength and mass, and the properties of soft tissues. Females generally have lower injury thresholds and muscle mass, as well as distinct soft tissue properties compared to males, making them more susceptible to fall-related injuries. By incorporating these sex-specific considerations into the design of preventative measures and safety standards, we can create more efficient and effective strategies that ultimately reduce the burden of falls and their associated injuries among older adults.118,119
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Discovery Grant from the Natural Science and Engineering Research Council of Canada (NSERC RGPIN-2018-06382) and a Discovery Accelerator Supplement Grant from the Natural Science and Engineering Research Council of Canada (NSERC RGPAS-2018-522659).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.