
Abstract
Continuous Positive Airway Pressure (CPAP) therapy is commonly prescribed for longstanding, acute cases of Obstructive Sleep Apnea (OSA) during which patients must wear a tight-fitting breathing mask overnight for the duration of the treatment. Because this condition frequently leads to the permanent use of CPAP masks, interface selection is a crucial factor influencing the treatment quality and effectiveness. Masks/interface selection is normally performed on a trial an error basis with clinicians informing their selection based on OSA-related factors with basic fitting feedback from patients. However, it is not uncommon for patients to abandon the treatment or request additional consultations due to ill-fitting CPAP mask with the main sources of discomfort being perceived air leakage and mask/strap overtightening leading to skin damage. This work introduces a novel system (Smart-Fit), for CPAP interface selection using advanced digital technologies, such as Reverse Engineering and Computational Modeling (Finite Element Analysis) which are paired to evaluate and determine the best fitting interface for each clinical case. The model simplifies the number of 3D facial landmarks to 12 and established that a 2 mm scan resolution is enough for accurate scans. The Von Mises stress map in ANSYS serves as an indicator of potential high-pressure areas, triggering the need for a chance of mask size. Current results indicate the Smart Fit System can enable a “best fit CPAP interface” to be selected considering individual’s physical characteristics and existing CPAP interface configurations. The development of the Smart Fit System is an evolution compared to traditional CPAP interface selection approach, which optimizes the CPAP interface selection process.
Introduction
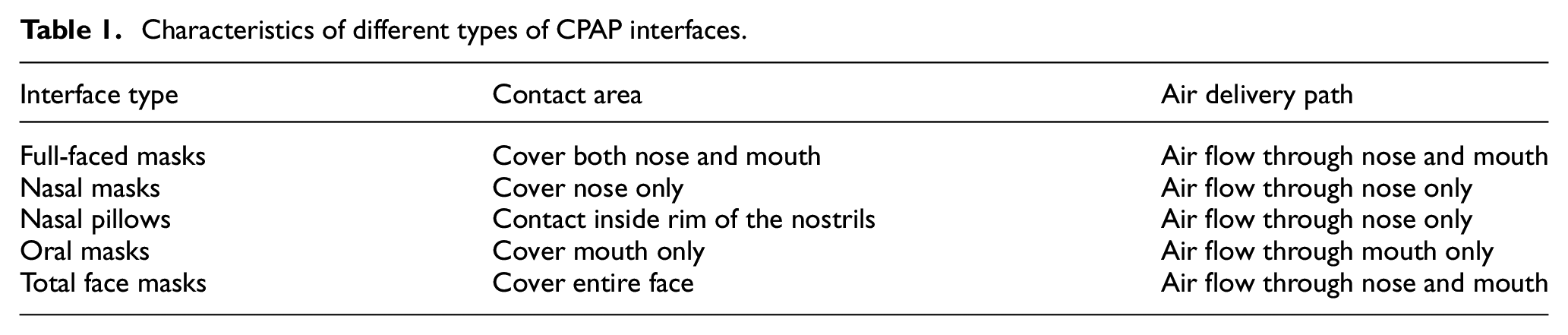
Continuous Positive Airway Pressure (CPAP) therapy was first invented by Colin Sullivan in 1980 1 and has since been widely used for the treatment of Obstructive Sleep Apnea (OSA) syndrome, currently considered as the golden-standard treatment. 2 A typical CPAP system comprises a pump, a flexible hose, a facial mask, and a headgear, 3 and it is the mask which creates the link between the user’s facial contour and the hose supplying pressurized air. Today, conventional CPAP interfaces are developed considering different requirements and possible breathing patterns, including: Full-faced (Oronasal) masks, Nasal masks, Nasal pillows, Oral masks, and Total face masks. 4 Materials used for shaping the cushioning side of mask interfaces employ a variety of typically soft formulations such as silicone, gel, air cushion or fabric. Table 1 shows the main types of commercially available CPAP mask configurations and airflow rationale.
Characteristics of different types of CPAP interfaces.
A CPAP mask is a prescription device which is either selected and adjusted as part of a dedicated “fitting session” with the relevant clinician 5 who provides it from stock by public healthcare systems (NHS, UK) or selected and purchased by patients directly who then obtain reimbursement via health insurance (US, Australia, New Zealand, and others). While sleep apnea is a highly prevalent condition, the typical cohort consist on older adults (above 55 years old) with common risk factors being obesity, smoking, and underlying disrupted sleep patterns such as snoring.2,6
Although CPAP masks greatly vary from configurations, materials, attachments, and cushioning, the design range is normally limited as a function of standard sizing. CPAP interface designs are normally based on average standard sizes (Small, Medium, and Large) with sizing templates provided by CPAP manufacturers focused on different characteristics on an idealized “average user.”
A sample Full-faced mask sizing template is shown on Figure 1 whose criteria considers the overall length from the eye corner to the mental crease. However other interface design will adopt different anatomic regions of reference such as the distance from the bridge of the nose to the corner of the mouth.
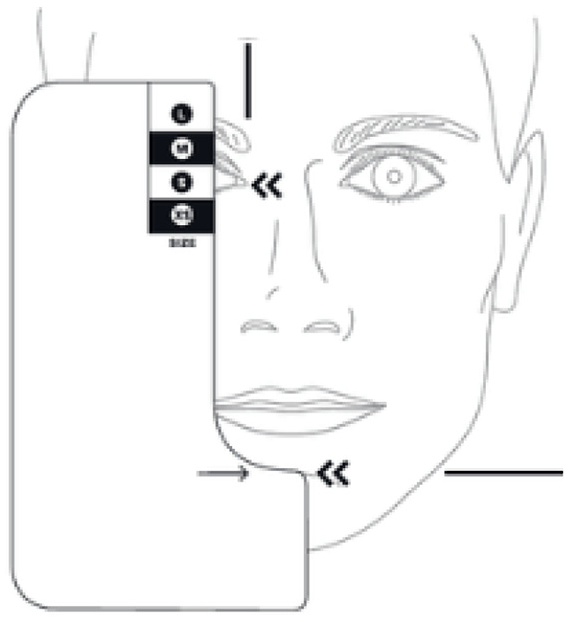
Sizing template for Full-faced mask considering distance from eye to chin crease, adapted from Resmed. 7
In this case, three different sizes (Small, Medium, and Large) of Full-faced masks are only classified by the distance between nasal bridge and chin. While similar sizing templates are commonplace and normally used as a primary fitting reference, there are a wide variety of unconsidered facial features that could lead to an ill-fitting mask if untested. Basically, most commercially available CPAP mask fitting guides rely on 2-dimensional (2D), normalized templates, which obviate the 3-dimensional (3D) nature of human facial features, usually leading to the rejection of the prescribed devices due to fitting and discomfort issues.6,8 Furthermore, with fit and comfort being a primary consideration, it has been reported that patients may exhibit low adherence or permanently abandon treatment if they perceive the intervention as uncomfortable and constraining.9,10
The current vast array of commercially available 3D capturing techniques, going from simple image photogrammetry to structured light projection, make it difficult to neglect the inherent 3D complexity of facial features, therefore the purpose of this work is to establish a system for the correct sizing and fitting of CPAP interfaces that acknowledges a more realistic user features’ scenario.
Smart fit method for CPAP interface selection
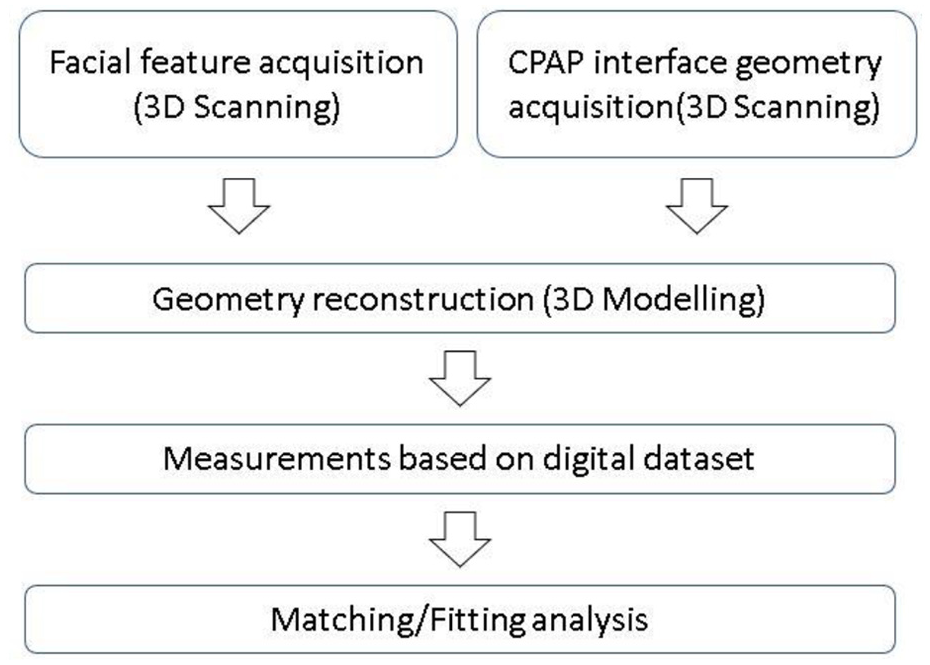
This study introduces a comprehensive mask selection procedure, named “Smart Fit System,” which can objectively and quantitatively indicate whether a specific mask, size, and material are the best fit for an existing OSA patient in need of CPAP interface selection. The system considers individual’s physical characteristics as well as specific CPAP interface configuration initially used or recommended by a clinician. The Smart Fit System consists of three main steps: (1) reverse-engineering (3D scanning) on a first instance in order to capture the patients’ facial features; (2) then a “3D superposition” stage is applied in order to fit a virtual representation of an existing mask design on the 3D face using a 3D scene environment; (3) computational modeling, based on Finite Element Analysis (FEA) is applied in order to estimate contact areas, skin pressures, and potential areas of noncompliance. Finally, the system is coupled with standard patient diagnose information as conventionally gathered during clinical appointments and visits in order to select a best fit CPAP interface: Age, Gender, breath pattern, sleep position, severity of OSA syndrome, treatment time, experience of the use of CPAP interface, known skin allergies. Figure 2 shows the general framework for the Smart Fit System.
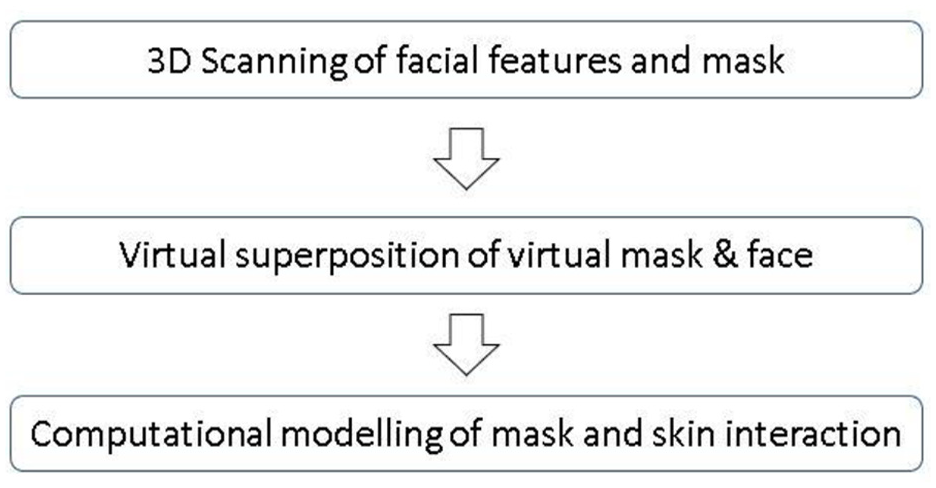
General workflow of Smart Fit System for CPAP interface selection.
Reverse Engineering allows the human facial anatomy and CPAP interface configuration to be converted into digital datasets which can be manipulated without requiring the patient to be physically present during the assessment. Measurement and facial features analysis can also be obtained based on digital markers located at the vertices and intersections of the mesh polygons, with the accuracy defined by the triangle-mesh size and the repeatability based on the measurement protocol. The interaction between facial skin and CPAP interface, for example, the contact area and pressure region, can also be predicted by applying a simple displacement condition on the “virtual mask.”
However, the “3D digital datasets” are only one half of the Smart Fit system, as the other part will still rely on capturing conventional clinical-case information. The aim is the digital technologies-driven system coupling with conventional patient data in order to create a smart system with potential of “learning” (Figure 3). This “conventional” system will rely on three main steps: mask type “shortlisting,” determining mask size, and linkage to patient records.
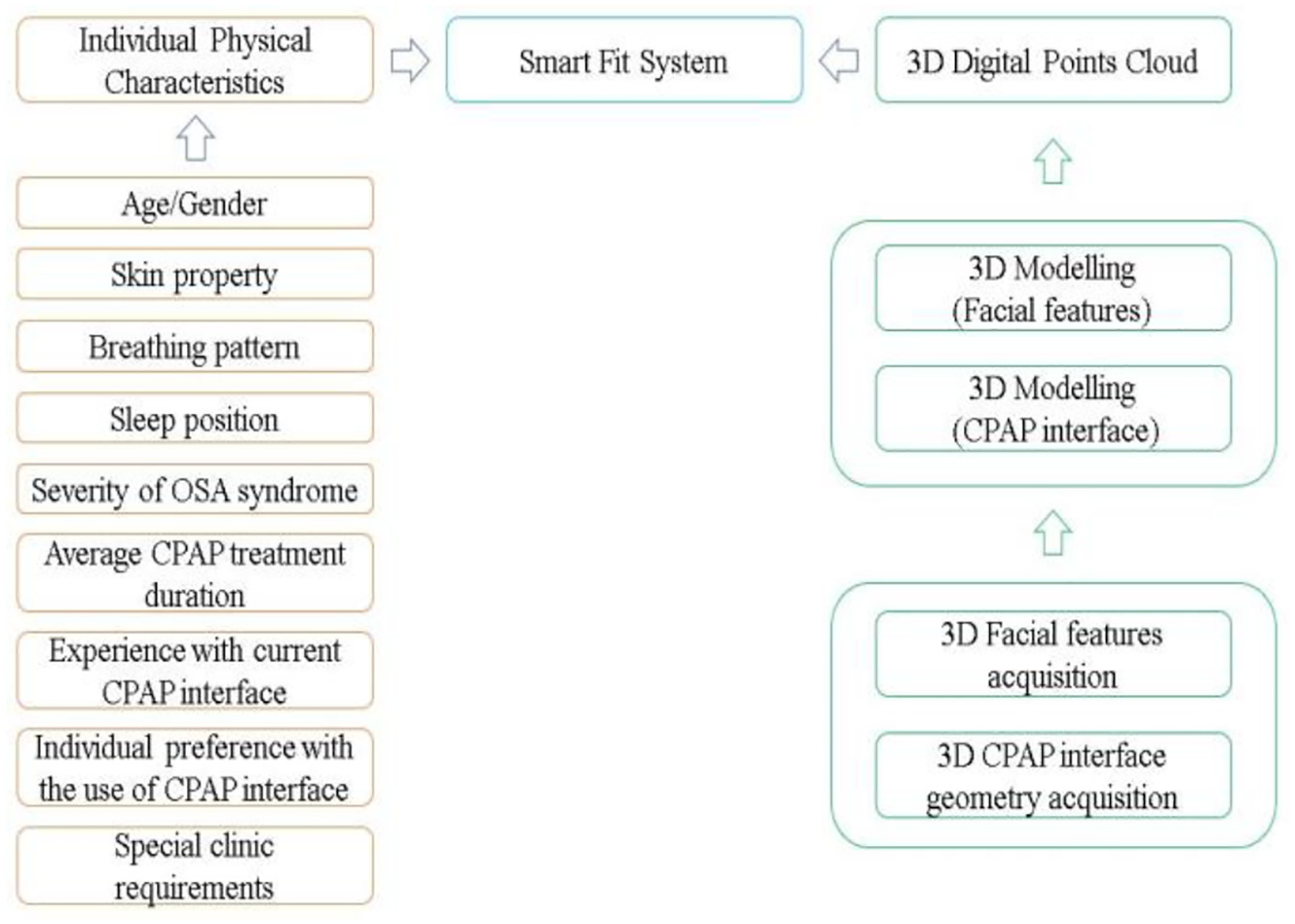
Development of Smart Fit System for CPAP interface selection.
CPAP interface shortlisting algorithm
Drawn from observation field work and consultations with local clinicians at the NHS-Newcastle trust Lung Function Department (Freeman Hospital, Newcastle upon Tyne), the mask types to be prescribed are dictated by the predominant breathing pattern of the patient; this is sometimes complemented by skin sensitivity indications, as well as potential allergies or declared issues with previous devices. Figure 4 illustrates the CPAP interface type selection process proposed by Smart Fit System.
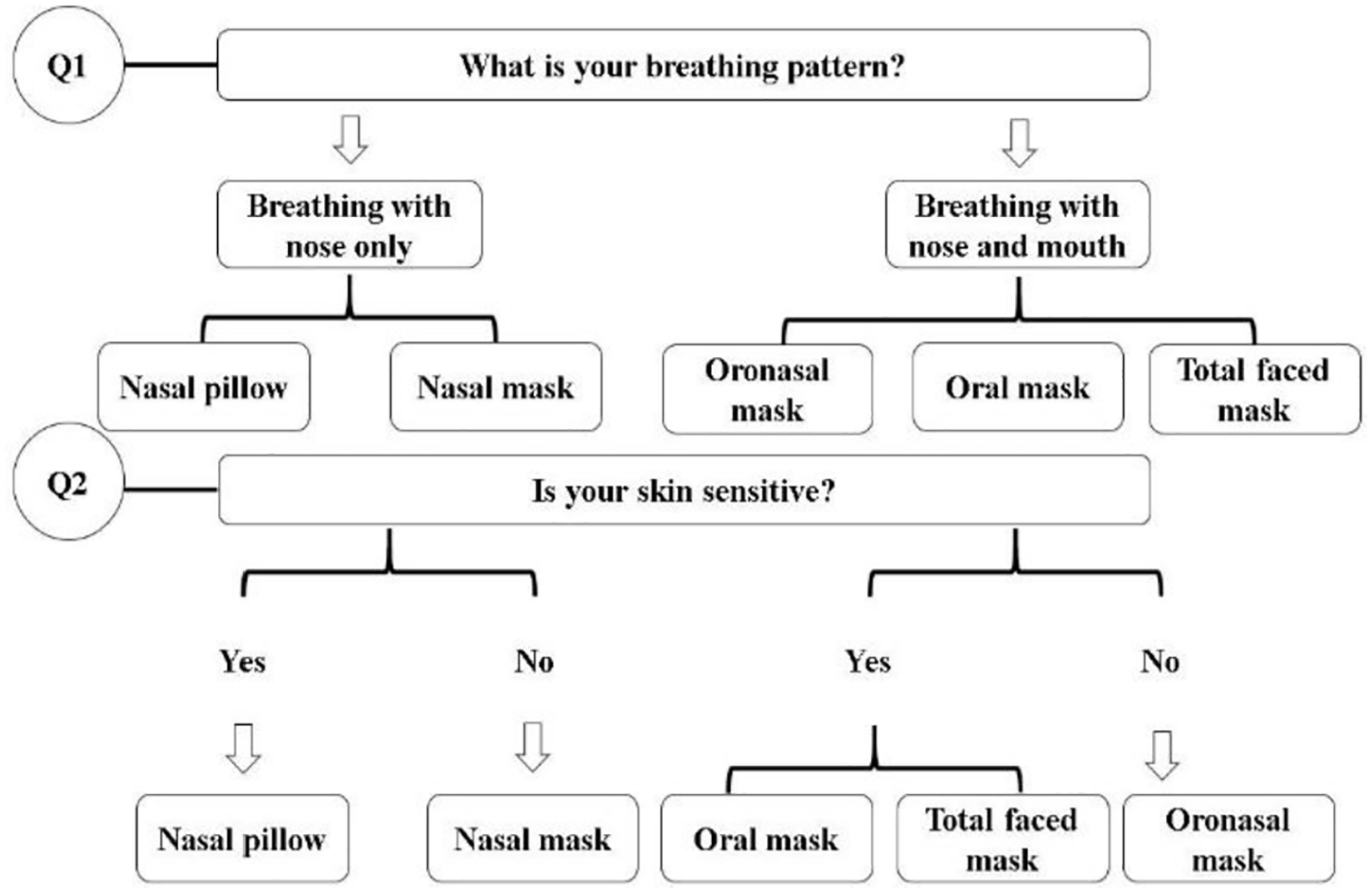
CPAP interface type selection strategy introduced by Smart Fit System.
Breathing habits during sleep are considered as the priority when selecting CPAP interface type. Theoretically, nasal delivery interfaces, such as Nasal masks and Nasal pillows, are indicated for nose-breathers 11 whereas Full-faced masks and Total face masks are considered as direct options for mouth-breathers.11,12 This initial mask screening based on user’s history and preferences is crucial, as it is intended to capture the main habits leading to the most accurate type of mask configuration, that is, if patients have demonstrated having over-sensitive skin around the nose or allergic reactions in the presence of silicone cushion, then a Nasal-pillow would not be indicated even if the subject is primarily a nose-breather. Hence the system can rule out specific masks such as Nasal masks and Nasal pillows and indicate a more neutral design with a different contact area and contour, thus reducing the likelihood of skin problems. 13 The selection must also consider the current severity of the OSA syndrome, treatment history as well as sleep position. If patients have severe OSA syndrome where a higher-pressure support is needed, Nasal mask is recommended with better performance compared to Nasal pillow. A relatively higher air pressure can be supplied with the use of Nasal mask. 14 In addition, previous experience with the use of CPAP interface and individual preference should also be considered in order to avoid interface associated side effects, such as dry nose, congestion, and skin damage.
Patients exhibiting both of mouth and nose breathing, will have Full-faced masks, Oral-masks and Total face masks normally indicated, however, Oral masks and Total face masks are less commonly used. 15 Full-faced masks cover both of mouth and nose area. It is worth noting that Full-faced masks also have various configurations, although pressurized air is supplied through both of mouth and nose path. Selection of Full-faced mask can be further decided by considering individual preferences, previous masks experience and sleep position.
CPAP interface size selection
After the CPAP interface type is shortlisted, the next step is to select an adequate size. Unlike traditional interface selection processes using 2D sizing templates provided by manufacturers, the Smart Fit System considers a 3D surface map obtained via 3D scanning to convert human facial anatomy and CPAP interface geometry into digital datasets.
It must be noted that any 3D scanning platform can be applied, provided the scan’s volumetric accuracy is not greater than 2 mm. This is to avoid potential leakage areas induced by large triangles on the post-processes point cloud.
Datasets for this work were acquired using the Creaform GoScan 50 (Levis, CA) coupled with VX-Elements post processing software. This is a white-light projection scanner suitable for acquiring facial features with resolution up to 0.5 mm. 16 Because there is currently not existing 3D digital repository of commercially available CPAP masks, we digitized a range of Fisher & Paykel Simplus Full Face Masks (Frame with cushion) in three sizes (small, medium, large), using the same scanner and post processing software above. The intention of this method is to undertake 3D measurements on digital mask datasets as opposed to 2D-measuring templates.
The final step is to record all information in Smart Fit System, information collected can be used as reference in future when patient’s physical condition changes. Figure 5 indicates the CPAP interface size selection process introduced by Smart Fit System.
CPAP interface size selection strategy introduced by Smart Fit System.
Patient record
Not only is the type of CPAP mask dictated by the patient background information, but also the air supply pressure levels as well as the duration of the treatment. While a Smart Fit System can be deployed based on the previous two elements, it is acknowledged that in order to have a comprehensive system, ideally patient dataset should also form part of the assessment. Relevant physical aspects consist of breathing habits (breathing with mouth and nose), sleep position (spine position and side position), skin sensitivity (Skin elasticity), severity of OSA syndrome, previous experience with medical device as well as individual preference.
Case study
Digital dataset acquisition
Facial anatomy acquisition
The Smart Fit System methodology was applied to a case study based on a healthy male participant, recruited as volunteer at Newcastle University School of Engineering following the internal Ethics procedure. 17 The volunteer’s facial anatomy acquisition was obtained using a structured-light projection scanner as described before, without the use of reflective markers. The scanning protocol set up and acquisition ran for less than 5 minutes. The raw point cloud was processed using VXelements in order to obtain a workable triangular mesh by trimming contours, removing floating island, filling mesh patches, and running once cycle of general smoothing (Figure 6).
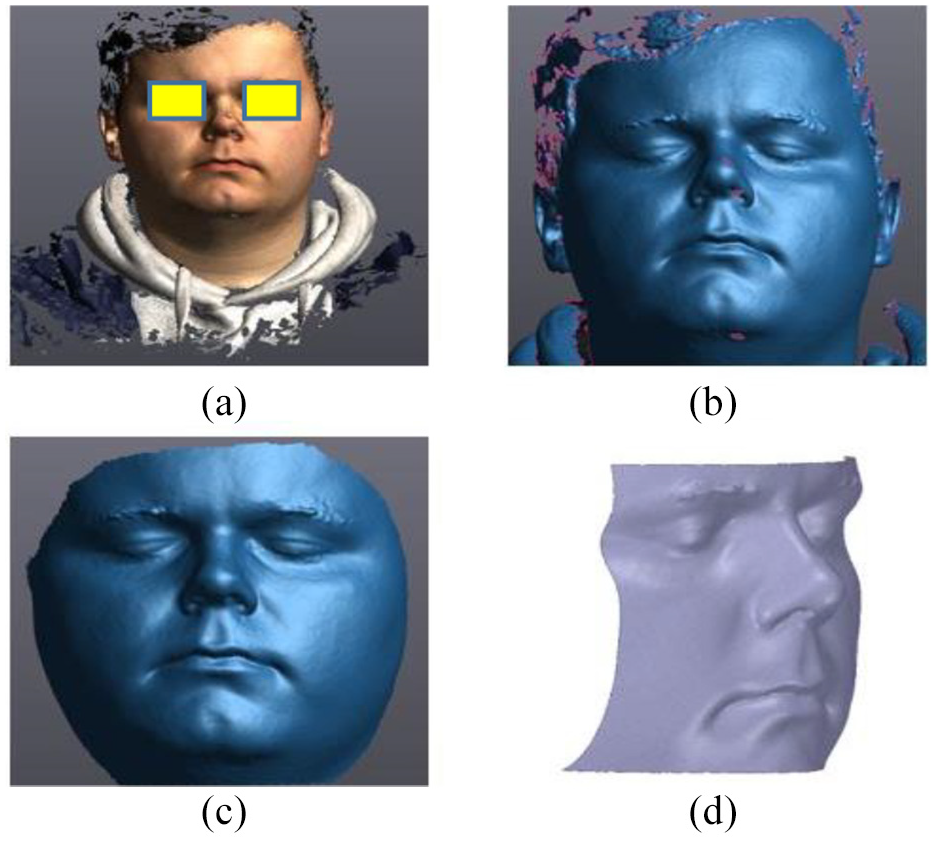
Facial anatomy acquisition: (a) Point cloud with texture. (b) Raw scan with noise. (c) Edited and patched mesh. (d) Modified 3D facial model.
CPAP interface geometry acquisition
In this study, three examples of Full-faced CPAP mask (Simplus, Fisher & Paykell Health), 18 were 3D scanned using the same scanner and post processing software. Because structured-light 3D scanners cannot easily capture translucent objects’ features, it was necessary to prepare the masks acrylic and silicone surfaces by coating them with a 3D scan spray SKD-S2 (Figure 7). After painting, the mask was left for at least 3 minutes to allow the liquid spray to be solidified. 3D scan spray can be easily removed without causing any physical damages to the original mask model. After scanning, the digital dataset of the Full-faced mask was also postprocessed via VX elements and exported as a STL mesh. In order to simplify the geometry for the purpose of Finite Element Analysis, only the mask’s cushion was extracted and imported into the computational modeling software, ANSYS2017-R2.
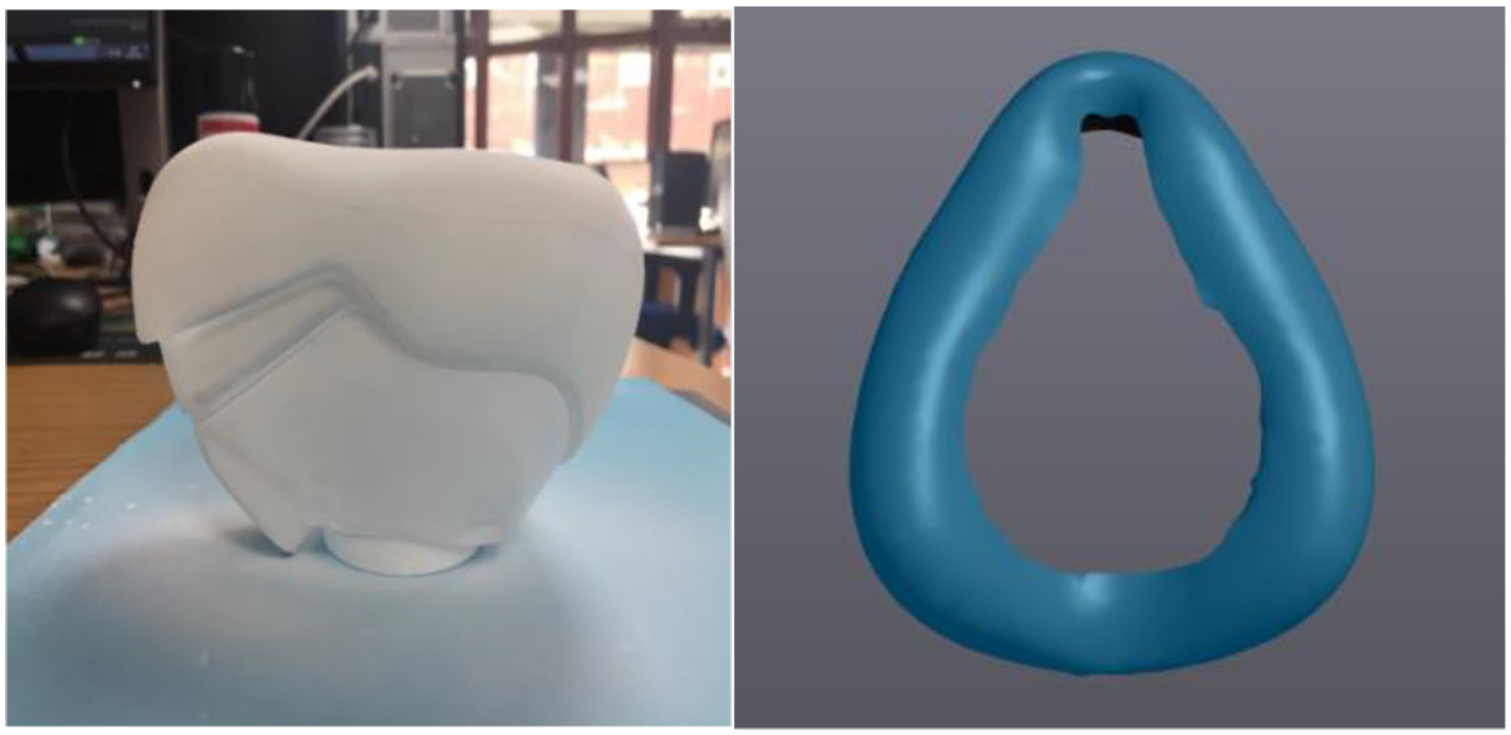
Painted Full-faced interface model (left) and 3D model construction of Full-faced interface cushion (right).
Following the same 3D acquisition method three sizes of Full-faced mask models (Small, Medium, and Large) were generated. Figure 8 shows the over imposed models of the flexible silicone region.
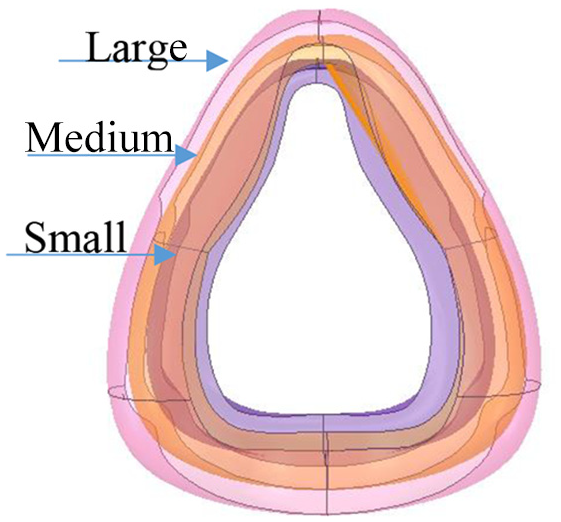
Three sizes for the Full-faced cushion geometry: Large (pink), Medium (orange), and Small (brown).
Virtual facemask superposition
Facial landmarks can be easily marked based on digital facial anatomy datasets; however, this will rely on the vertices generated by triangular 3D meshes, therefore the max resolution of 2 mm. As opposed to 2D-measurement templates, using a 3D mesh enables the measurement of detailed features that would be otherwise unknown, such as mouth to bridge of the nose distance, nose angle or the variation in depth of the cheek area. In this case, 22 points have been highlighted mapping the key facial features, including eyes, cheeks, nose and mouth as highlighted by previous state of the art on 3D facial landmark measurement,19–21 shown on Figure 9.
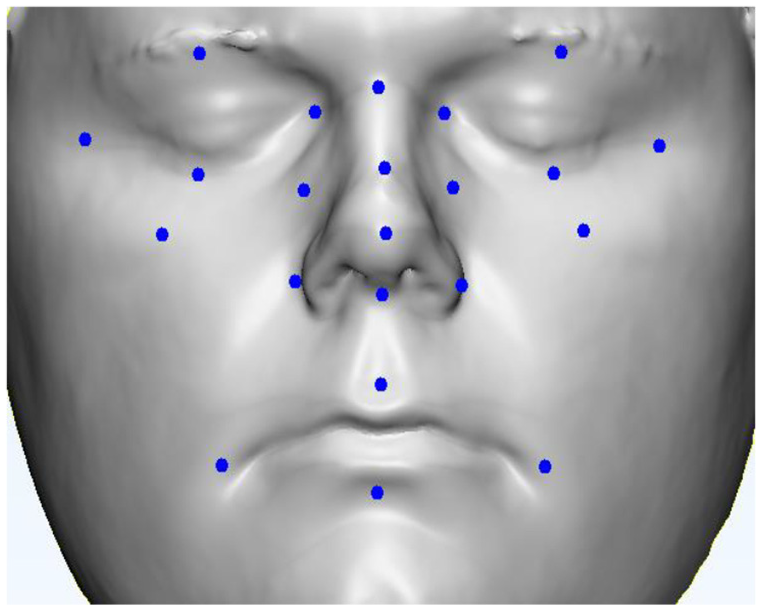
Facial landmarks on 3D canned facial dataset.
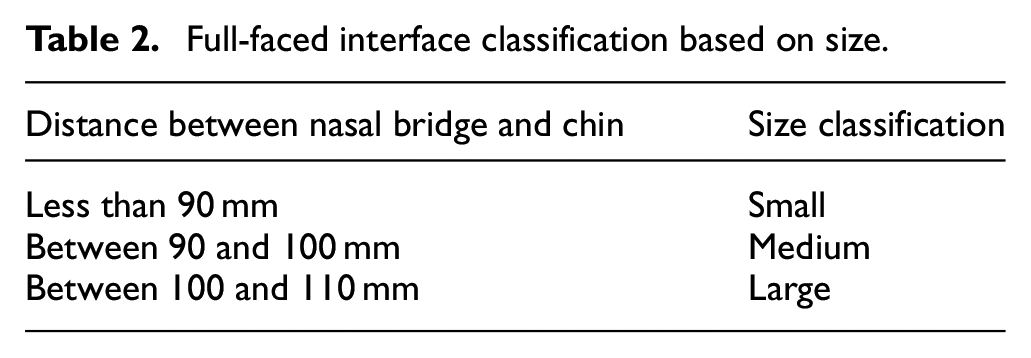
According to traditional Full-faced interface sizing templates, the three different sizes: Small, Medium, and Large, are classified by the distance between nasal bridge and chin. The classification is shown in Table 2.
Full-faced interface classification based on size.
Based on digital facial anatomy datasets, the distance between nasal bridge and chin can be easily measured (Figure 10). The distance between nasal bridge and chin for this volunteer was 90.76 ± 1 mm. According to the sizing template, both Small size and Medium size interfaces could be suitable. It is obvious that the best fit CPAP interface cannot be selected using this simple sizing template.
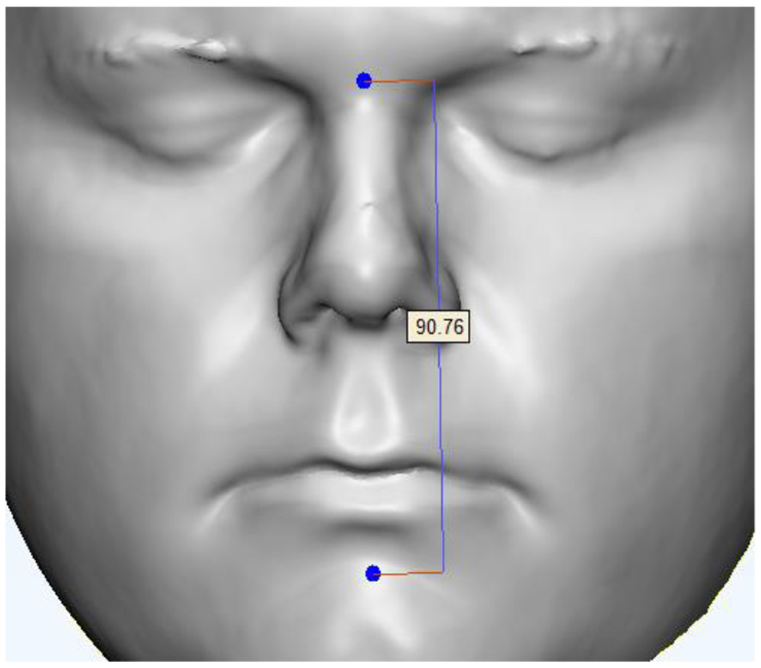
Measurement of facial feature (between nasal bridge and chin).
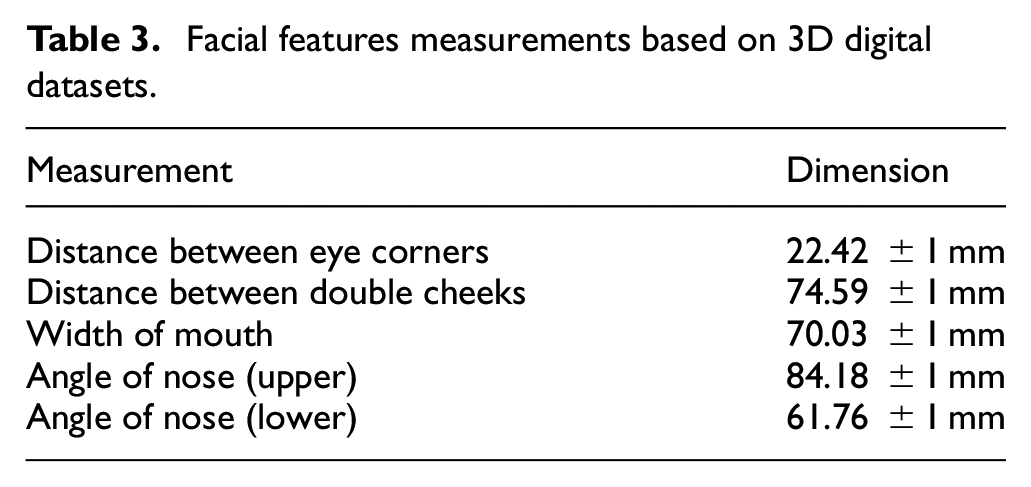
In order to let the best fit CPAP interface be selected, Smart Fit System requires more facial features measurements, for example, the distance between eye corners, distance between double cheeks, and width of mouth. This is because CPAP interface related side effects, such as discomfort and air leak can be easily developed around the eye corners if an ill-fitted mask is worn. Skin problems can be developed around the mask, particularly at the nasal bridge area and double cheeks area where fat is less. Detailed nose structure and overall facial layout have also been vital influencing the CPAP interface selection. Figure 11 illustrates the facial feature measurements required by Smart Fit System. In this case, more facial features measurements were obtained shown in Table 3.
Facial features measurements based on 3D digital datasets.
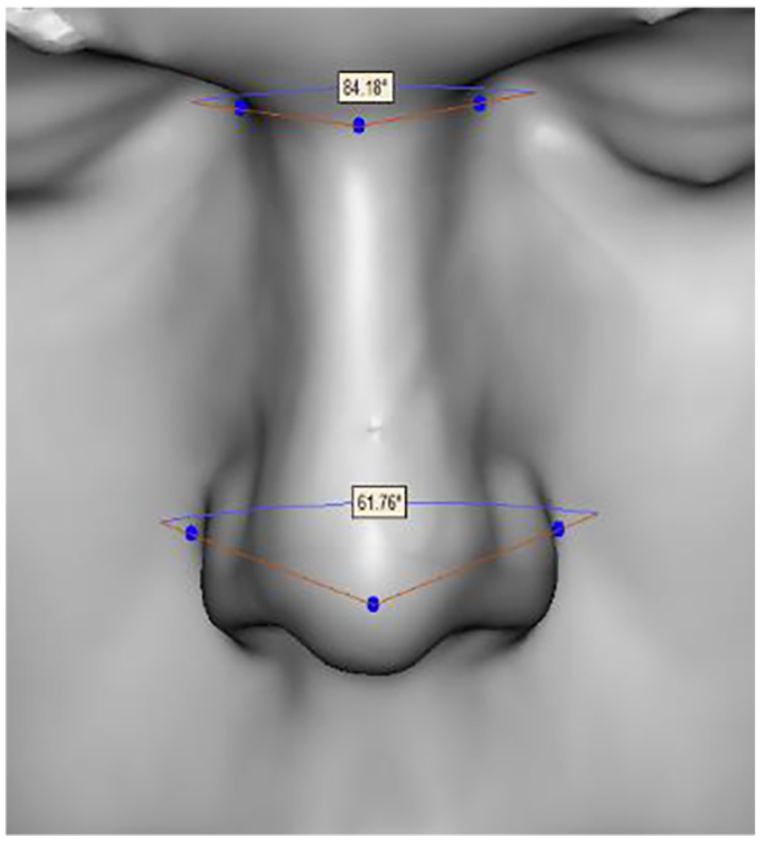
Measurement of 2D and 3D facial features.
It is also possible to fully characterize the CPAP interfaces by establishing measurements on the soft and hard mask regions in order to relate those to actual facial characteristics (Figure 12).
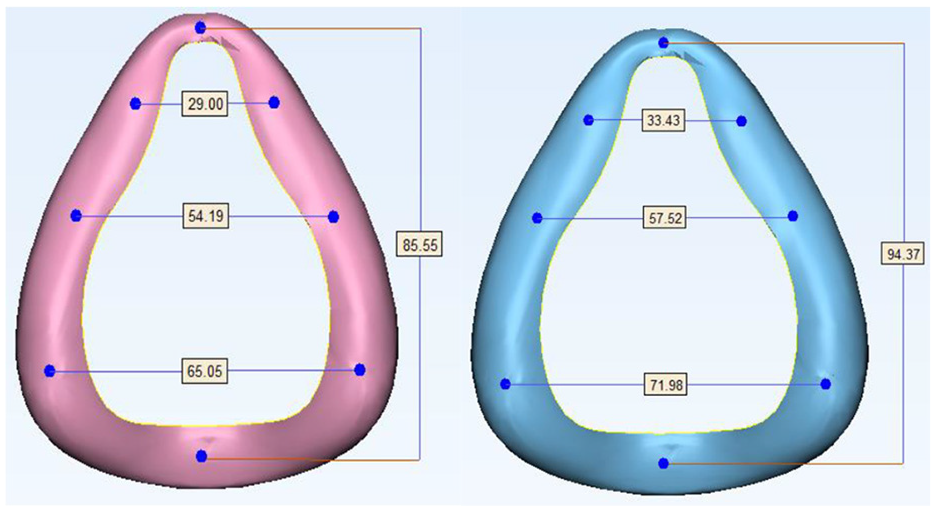
Measurement on Full-faced masks: Small (left) and Medium (right).
Finally, the facial features measurements obtained were compared to existing CPAP interface configuration. The most suitable CPAP interface should be selected based on several principles.
Full-faced interface should fully cover both mouth and nose area.
Vulnerable facial areas where interface related skin problems are often caused, such as, nasal bridge and double cheeks, should be avoided or minimized to contact with.
Mask should avoid any close contact with the naso-lacrimal area, as besides being a sensitive skin area it is prone to leakages.
In this case, size Medium presents more suitable for the volunteer, as the width of the mouth is fully covered by the Medium size mask.
Computational modeling (Pressure and Fit simulation)
While 3D-measurements are an instrumental feature afforded by digital scanning, it is possible to exploit 3-dimensional datasets even further in order to establish detailed interactions between mask and interface. This is done via computational modeling in the form of FEA which enables the application of forces, pressures, and contact areas controlled by the user.
The aim of conducting this simulation modeling is to deeply understand the interaction between mask interface and facial skin, therefore choosing a best fit mask for patients by predicting the contact area and peak pressure region. This simulation was conducted using Finite Element Analysis (ANSYS). Both models were meshed into Triangles, with the size of 3 mm. In this simulation, facial model was assigned as soft tissue material. Young’s modulus is 15 KPa, and Poisson’s ratio is 0.49.22,23 Full-faced mask cushion was simulated as silicone rubber. Young’s modulus is 2 MPa, and Poisson’s ratio is 0.49.5,24,25 Alignment of models is important to achieve accurate simulation results. Figure 13 shows the assembled models.
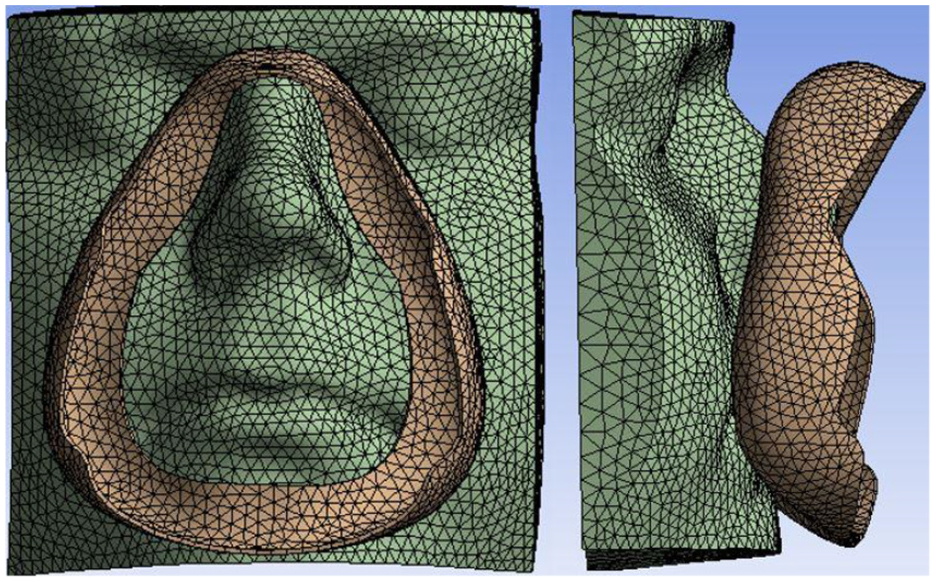
Front (left) and lateral view of alignment of facial model and Medium CPAP Full-faced interface cushion model.
In this simulation, the mask model was displaced toward to facial model using a series of displacements (27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, and 39 mm). Figure 14 illustrates the simulation results where displacement applied was 39 mm. It can be observed that Medium Full-faced mask covered the volunteer’s nose and mouth area, which meant that Medium mask selected can function suitably for this case. High stresses are recorded around the contour contact area as expected. A different result could indicate a higher stress concentration at localized regions; this can be particularly true for patients exhibiting pronounced facial asymmetries.
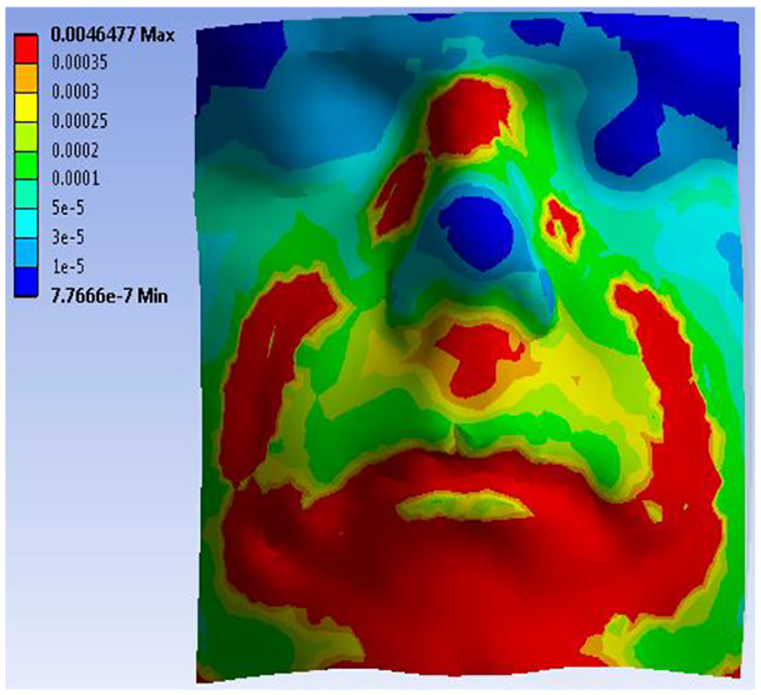
Stress (MPa) on facial model (left) and Medium mask model (right).
Data recording
The final step to complete the CPAP interface selection using Smart Fit System is to record all necessary data including individual physical characteristics, 3D digital datasets of individual facial anatomy and conventional CPAP interface geometry, measured data from facial anatomy and CPAP interface configuration, simulation results indicating contact area and pressure regions between facial model and CPAP interface model, as well as the information of the CPAP interface selected using Smart Fit System. All these data can be saved and will be further used to either trace patient’s CPAP treatment condition or improve the current CPAP device development.
Discussion
Features afforded by the Smart Fit System for CPAP interface selection
At present the Smart Fit System is presented as an algorithm which makes use of existing digital technologies for the analysis, fit assessment, and recommendation of suitable CPAP mask interfaces. The main objective is to introduce objective and quantifiable elements so that the CPAP interface selection and prescription can be an informed process, rather than relying on patient’s opinions and physician’s experience.
The development of Smart Fit System exhibits great potential to help patients selecting a best fit CPAP interface by objectively offering supporting data obtained from analysis of facial anatomy and conventional CPAP interface configuration. Furthermore, interaction between facial skin and CPAP interface such as contact area and pressure region, can be observed via simulation modeling. While at present, the case studies are being modelled on an individual basis, there is potential to automate the computational modeling scenarios by (1) adding intelligence to the system (automatic alignment, automatic measurement, and facial feature extraction) and (2) increasing the CPAP mask digital database, so that a wider range of models can be assessed, measured, and compared.
If the best fit CPAP interface can be theoretically suggested depending on results from professional analysis and simulation modeling, the selection process can become more efficient and could potentially be either outsourced, or preformed outside the clinic, hence liberating staff time and reducing the waiting time for mask-fitting appointments, which in some healthcare systems translates to weeks of waiting. An additional benefit is the potential of prescribing a mask which tends to minimize the possibility of leakage, which can affect the overall CPAP treatment by affecting the air pressure levels that are effectively supplied via the interface. Finally, Data processed and saved can further be used both in medical care trace for patients and in improving conventional CPAP interface design and manufacture.
Patient involvement in CPAP interface selection process
Traditional interface selection via sizing templates has the compromise of not catering for specific individual facial features while focusing on an “ideal average.” Consequently, the chance of selecting an ill-fitted CPAP interface increases due to inaccurate or insufficient facial features analysis. In addition, a system that can embed a more comprehensive logic for the selection of the right interface could potentially include more factors into the equation such as patient’s age, gender, breath pattern, sleep position, severity of OSA syndrome, treatment time, experience of the use of CPAP interface, individual preference, and special clinic requirement, should all be considered in CPAP interface selection.
Use of Reverse Engineering in CPAP interface selection process
Reverse Engineering is a quick method to accurately acquire human facial anatomy and can have multiple forms (laser, white-light, photogrammetry, IR); it can also be instrumental for digitizing commercially available masks for a quicker fit-analysis without the need of physical patient evaluation. It can be argued that facial datasets can have an expiration date as tissue density and features may change over time, therefore there may not be a need to store patient’s 3D data if the acquisition system is automated in a similar fashion as it is now for other fields such as foot orthotics design based on 3D scan data of plantar surface.26,27 Issues on accuracy, repeatability, and measurement error can be mitigated by the implementation of repeatable 3D scanning protocols which dictate: (1) 3D scan resolution, (2) 3D mesh triangle size defined by postprocessing, (3) definition of facial features relative well defined landmarks (nose bridge, tip of nose, nostrils width, etc.), and (4) a “rule of thumb” to define which vertex to choose for each datapoint (lower-left vertex for right-half of the face, and lower-right vertex for left-half of the face if split along the sagittal plane).
Modeling interaction between face and CPAP interface
The most suitable CPAP interface should present less contact on vulnerable facial zones, such as the eye corners and double cheeks. The simulation results can be as reliable as the material model data entered to analyze them; therefore, these can currently be considered close approximations to facial skin data and silicone material data. Facial contact pressures reported in literature 5 do not seem to follow a standardized approach with core differences in the way FEA models, loads meshes and boundary conditions are applied. 25 These variability in literature may be caused by:
Various material properties set up in simulation models. Material properties can significantly influence the simulation results however the only method to realistically represent human facial tissue interactions is to develop detailed multi-layer tissue model.
Geometry reconstructed and contact method. In this case, contacts, mesh, and boundary conditions can be set up differently. Most importantly, geometry used in each simulation modeling is also different.
Model limitations
The Smart Fit System presented in this work is delivered as a series of analysis steps or algorithm to follow in order to virtually assess the fit of a wide variety of commercially available masks as opposed to having to manually test every single mask option, brand, and size. A number of current limitations are to be addressed for a future widespread application of this or similar systems:
Access to a database of 3D virtual masks, or manually digitizing the most relevant models.
Clinicians access and use of FEA suit is not a straightforward option, therefore this analysis must be automated by the use of a library of previous analysis knowledge base.
Facial measurement and landmark selection are currently performed manually, and it is to be expected that an algorithm is developed which can accurately recognize, select, and measure the required landmarks.
Current 3D scan postprocessing is also manually done, so further algorithmic development is expected to overcome the multiple steps involved in remeshing, cleaning, smoothing, etc.
Finally, the ultimate aim of such a system is to be available as a self-contained semi-automatic suite or app which can automate all 3D and engineering analysis in order to provide clear selection criteria.
Conclusion
CPAP interface selection process can be optimized using the Smart Fit System proposed in this study. Compared to traditional CPAP interface selection, Smart Fit System, which be a technology-based evaluation, analyses both individual’s physical characteristics and existing CPAP interface configuration to objectively suggest a best fit interface for patients. Reverse Engineering enables the duplication of complex object’s geometry including facial anatomy and existing CPAP interface configuration. Digital datasets obtained are precise to be further used into measurement and analysis process. Furthermore, interaction between facial skin and CPAP interface can also be predicted through computational modeling. Results generated from computational modeling, such as contact area and pressure region at facial skin and CPAP interface, can be considered as supporting evidence to select the best fit CPAP interface. Further work is being undertaken in order to automate different parts of the system including the orientation, alignment, and loading scenarios so that multiple masks can be batch-compared. We foresee not only CPAP masks, but other types of breathing and respiratory devices going into digital workflow for the precise fitting, selection, and eventually for the generation of custom digital-design alternatives.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.