
Abstract
Three simple and low-cost configurations of handheld scanning probes for optical coherence tomography have been developed. Their design and testing for dentistry applications are presented. The first two configurations were built exclusively from available off-the-shelf optomechanical components, which, to the best of our knowledge, are the first designs of this type. The third configuration includes these components in an optimized and ergonomic probe. All the designs are presented in detail to allow for their duplication in any laboratory with a minimum effort, for applications that range from educational to high-end clinical investigations. Requirements that have to be fulfilled to achieve configurations which are reliable, ergonomic—for clinical environments, and easy to build are presented. While a range of applications is possible for the prototypes developed, in this study the handheld probes are tested ex vivo with a spectral domain optical coherence tomography system built in-house, for dental constructs. A previous testing with a swept source optical coherence tomography system has also been performed both in vivo and ex vivo for ear, nose, and throat—in a medical environment. The applications use the capability of optical coherence tomography to achieve real-time, high-resolution, non-contact, and non-destructive interferometric investigations with micrometer resolutions and millimeter penetration depth inside the sample. In this study, testing the quality of the material of one of the most used types of dental prosthesis, metalo-ceramic is thus demonstrated.
Keywords
Introduction
Optical coherence tomography (OCT) 1 is a technique that uses principles of low-coherence interferometry to achieve images with micrometer resolution and millimeter penetration depth. While OCT was developed initially to investigate the retina, 2,3 it is nowadays used for several biomedical applications including, besides ophthalmoscopy, teeth, skin, and endoscopy.
Even though OCT has been first applied to in vitro studies, now is essentially used for in vivo investigations, as the challenge is to deliver images in real time—with video-frame capability. The modern OCT technology has evolved from time-domain (TD) OCT to spectral domain (SD) that offers higher acquisition speed and better sensitivity. SD-OCT has been developed along two directions to interrogate the spectrum at the output of the OCT interferometer, using either a broadband source and a spectrometer or a swept source (SS) and a photodetector. 4,5 OCT has progressively expanded toward other fields, such as non-destructive characterization of materials, 6 art conservation, 7 and profilometry. 8
In parallel with the development of OCT systems and applications, an expanding area of research is involved in moving the technique from the laboratory to the clinical environment. 9 This specific activity, as well as the material and art applications mentioned before, implies the use of handheld scanning probes to allow for the examination of different parts of the body or a larger sample. 10 –12 This work concerns the development of various handheld-based near-infrared optical imaging devices. 13 This is itself part of a more general trend of having and using handheld probes in portable instruments, 14 not only in OCT but also in other techniques, such as Raman spectroscopy, 15 or other types of applications. 16 These researches include devices developed for surgical procedures 17 and applied in a dedicated medical environment. Endoscopes have been designed 18,19 to meet different medical requirements; some variants couple handheld probes and endoscopes for a more reduced size and an improved ergonomy—despite of higher costs. 20
Various fully functional systems, including handheld probes with lower cost, and macroscopic scanners for OCT units have already been demonstrated, by example for primary care diagnostics, 21 with a gamut of applications targeted, for investigations of the eye, ear, mouth, and skin. Optical designs 22 as well as improvements in the instruments and the techniques have been approached. 23 –26
In response to the utility of this topic as demonstrated by the list above, the aim of this work is to develop different specific designs of handheld scanning probes. The descriptions and the layouts that will be presented allow for constructing such probes in any laboratory, with minimum effort and costs. To the best of our knowledge, such a detailed and practical description has not been done before yet, although various probes and applications have been reported. 10 –14,20 –22 We shall use in these probes a simpler and more un-expensive unidimensional (1D) galvanometer-based scanner (GS), in contrast to other handheld probes, which use bidimensional (2D) dual-axis GSs 21 or micro-electro-mechanical systems (MEMS). 27 Furthermore, this is, to the best of our knowledge, the first configuration of handheld probes for OCT that can be built almost entirely with off-the-shelf parts. Therefore, our designs are with different degrees of complexity, appropriate for different applications, including those that are targeted to be used for the various current researches of our groups, for example, OCT investigations of teeth, 28 or in art studies. 29
Even if a range of applications are expected for the handheld scanning probes we are currently developing, the first priority of our study was to take the technique to be user-friendly for specific clinical applications. The Applied Optics Group (AOG) of the University of Kent (Canterbury/Kent, UK) has already demonstrated a portable OCT system using both a scanning handheld probe that is a variant of one of the prototypes that will be described later and a catheter probe for primary care in an ENT (Ear–Nose–Throat) Department at the Northwick Park Hospital in London (London, UK). 30 As we have different on-going developments of the project, a dentistry application carried out at the Imaging Group of the School of Dentistry of the Victor Babes University of Medicine and Pharmacy of Timisoara (Timisoara/Timis, Romania) will be presented in this study. Metalo-ceramic prostheses will be considered in order to test the handheld probes presented; a comparison with metalo-polymeric prostheses will also be achieved. The handheld probes developed will be used with an SD-OCT setup developed by the AOG and installed in Timisoara. A few possibilities offered by the use of this non-invasive technique in dental applications will also be discussed.
Instrument design requirements
Several aspects had to be taken into account and solved for the handheld scanning probes in order to optimize both design and fabrication.
The material of the cage has to fulfill several requirements that have been satisfied for all of the probes. Thus, the material must be
Relatively light to make the probe easy-to-handle for a significant duration of time throughout the day (please see the “Discussion” section regarding the practical limits of the mass).
Appropriate for a clinical environment, thus potential toxic materials are excluded. This also implies the use of surface treatments of the probe to make it corrosion resistant.
Heat resistant for the heat dissipation of the GS. If the probe is manufactured of metal, this heat dissipation must not propagate through the entire probe to affect the patient or the person that handles the probe.
Easy-to-process and to fabricate with high precisions on the active surfaces of the probe.
Durable: the main issue is also related to the heat resistance over the entire lifetime of the assembly in order to maintain its structural integrity and its imposed tolerances.
Relatively low cost: a trade-off has to be made between the above necessary characteristics and the cost of the handheld probe. Therefore, a titanium alloy is not compulsory, but the probe cannot be manufactured entirely from plastic either—if GSs are used. Plastic probes could be employed for MEMS scanners included in the construction.
27
The choice is therefore between Al alloys and composite materials.
Design
Concept of the assembly: the handheld probe may be made from several parts or in a composite material injected variant. The latter is convenient only for larger scale production, as it involves expensive matrix for plastic injection, whereas the former is preferable from the point of view of the manufacturing costs and therefore more convenient for a few prototypes. In conclusion, this solution has been chosen for our scanning probes. By using this specific design, the handle can be made distinct from the main part where different scanners can be used to focus the laser beam at different distances in order to investigate various parts of the body. An interchangeable subassembly to be mounted on different handles is preferred. This subassembly can allow for different functions (and appropriate complexities) of the probe—with different scanners and for different applications. The central part of the handle, where the GS is mounted, must include a heat dissipating element.
Tolerances
Tolerances and appropriate adjustment possibilities must be utilized. The necessary protection for the optical fibers connected to the collimator and electric wires connected to the GS must be provided. Appropriate mounting solutions have to be designed for each type of GS used within the handheld probe.
All these aspects have been applied for the handheld probes that will be presented and their fulfillment will be discussed after that.
Handheld scanning probes with off-the-shelf parts
Figure 1 shows the design and the prototype of the first scanning probe, constructed almost entirely from available off-the-shelf (16 mm cage; Thorlabs™) optomechanical parts. The components of this handheld probe (but also of the next ones) are presented in Table 1, where in parentheses the Thorlabs components used in our particular device are pointed out—to allow for the easy duplication of these configurations.
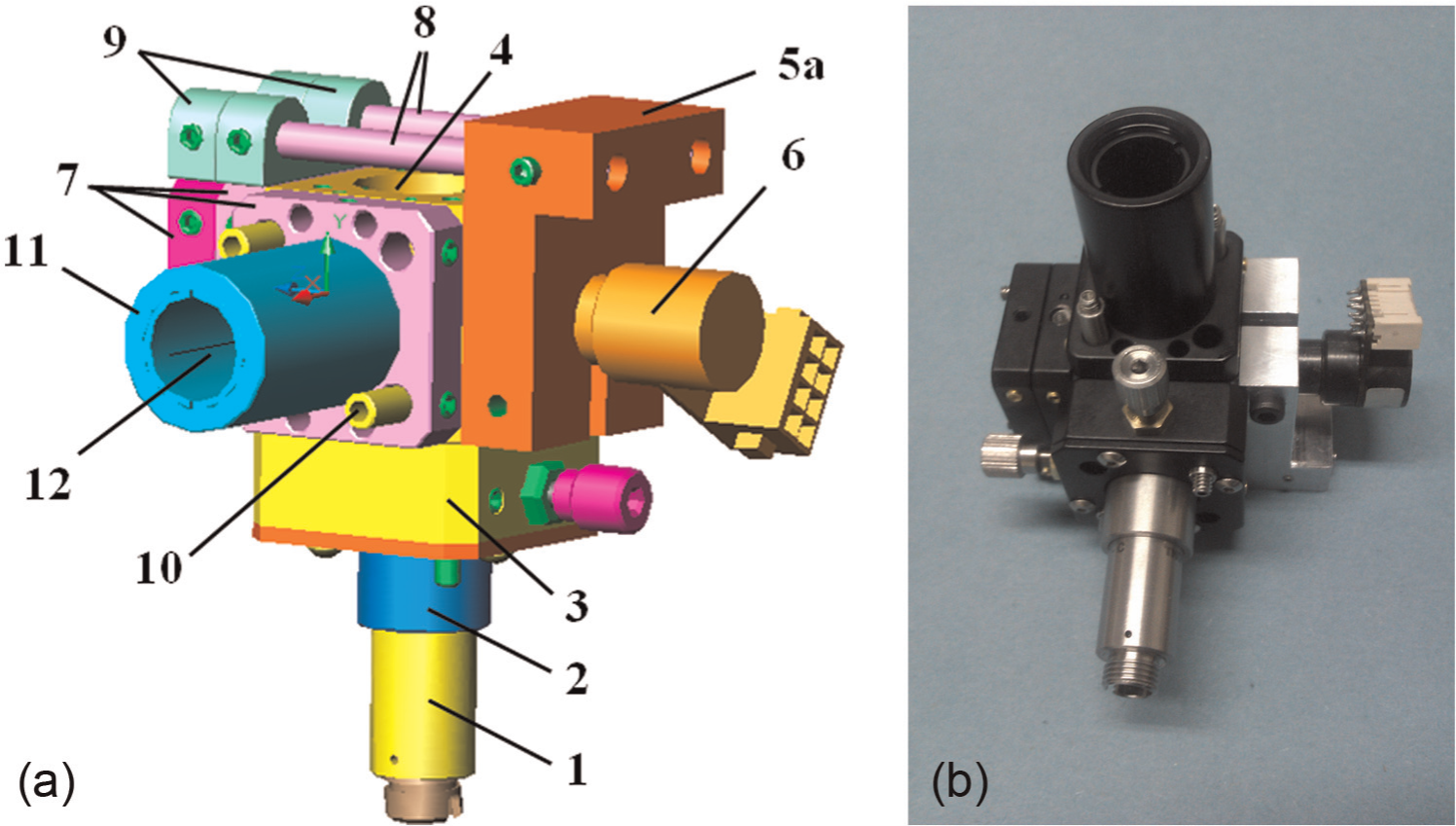
First configuration of the handheld scanning probe—constructed from off-the-shelf optomechanical parts: (a) design of the probe and (b) photo of the probe, with the GS. Notation (see Table 1 for details): (1) fiber collimator; (2) mount adapter for the fiber collimator; (3) X–Y translation stage; (4) six-way cage cube; (5a) GS mount; (6) 1D GS; (7) compact cage plates; (8) extension rods; (9) compact cage mounting brackets; (10) rods; (11) tube lens; and (12) objective lens.
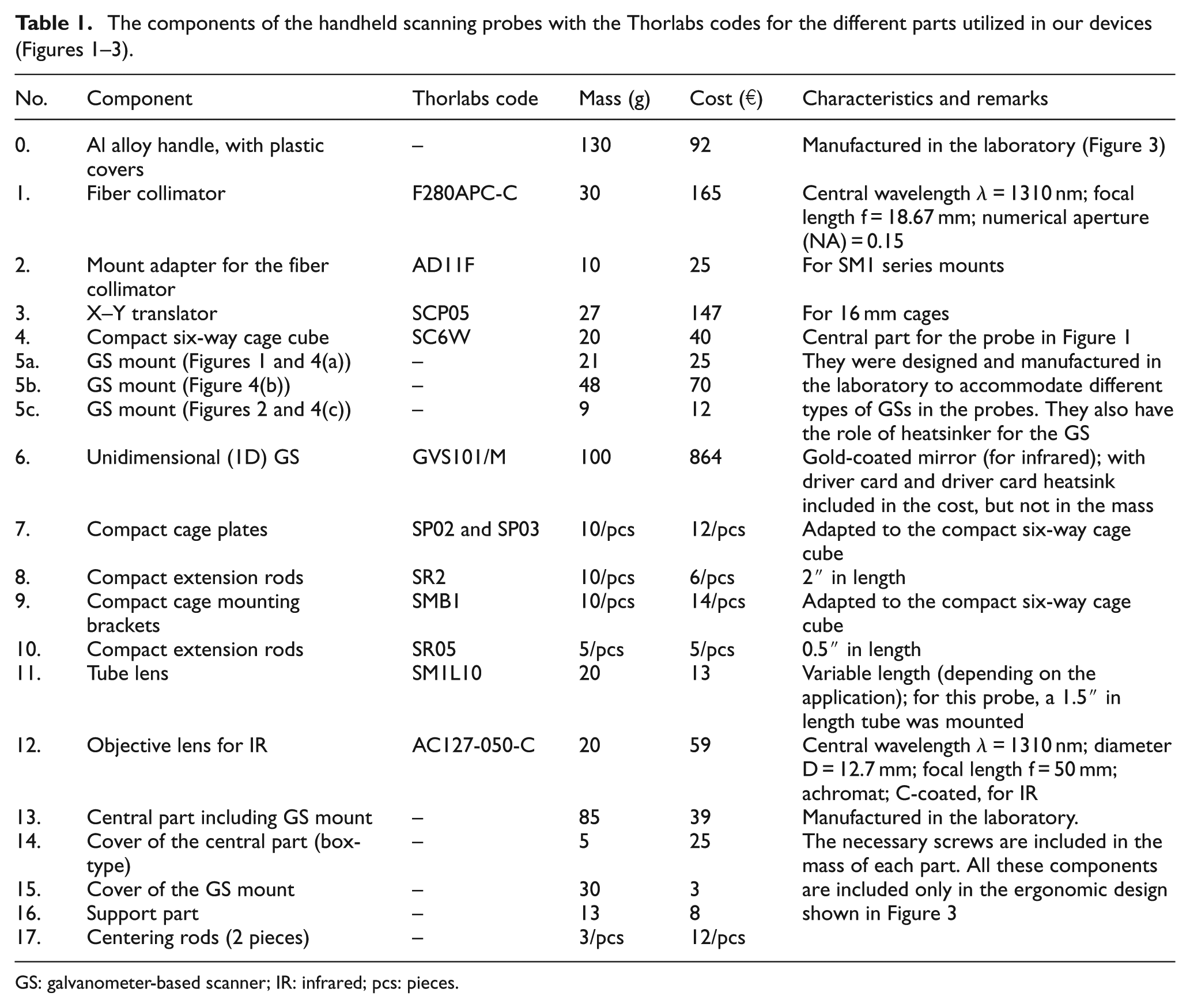
GS: galvanometer-based scanner; IR: infrared; pcs: pieces.
Due to the variety of scanning devices that may be employed in OCT, 31 we used the most common configuration for these handheld probes: a 1D GS that has to be optimized with regard to the scanning/input function to produce artifact-free images 32 and the highest possible duty cycles. 33 As discussed in recent developments on handheld probes with MEMS, 27 GSs have certain advantages that make them of interest, especially for 1D devices (which provide B-scans of the samples 3 ). Among these advantages, there is the possibility to drive them with triangular signals, so to obtain distortion-free OCT images 32 without any images post-processing. 27 This scanning regime is employed in the SD-OCT system used in this study.
The X–Y mini-translation stage (Figure 1, (3)) allows for the alignment of the optical axis of the components: the X-axis adjustment allows the placement of the axis of the fiber collimator (Figure 1, (1)) on the axis of the exit lens (Figure 1, (12)); the Y-axis stage allows the positioning of the axis of the collimator (and of the incoming laser beam) on the oscillatory axis of the GS (Figure 1, (6)).
A controlled eccentricity of the beam with regard to the galvo mirror axis included in the handheld probe for TD-OCT setups could be used for producing the modulation function without a translation stage. 34
This first prototype had been initially attached to the optical table for preliminary studies by using a TD-OCT setup. With this configuration, it can be used as the scanning head of the sample for the OCT system. The probe had been then provided with an adapted, commercially available, and low-cost handle (Figure 2) to be used together with a mobile, portable SD-OCT system.
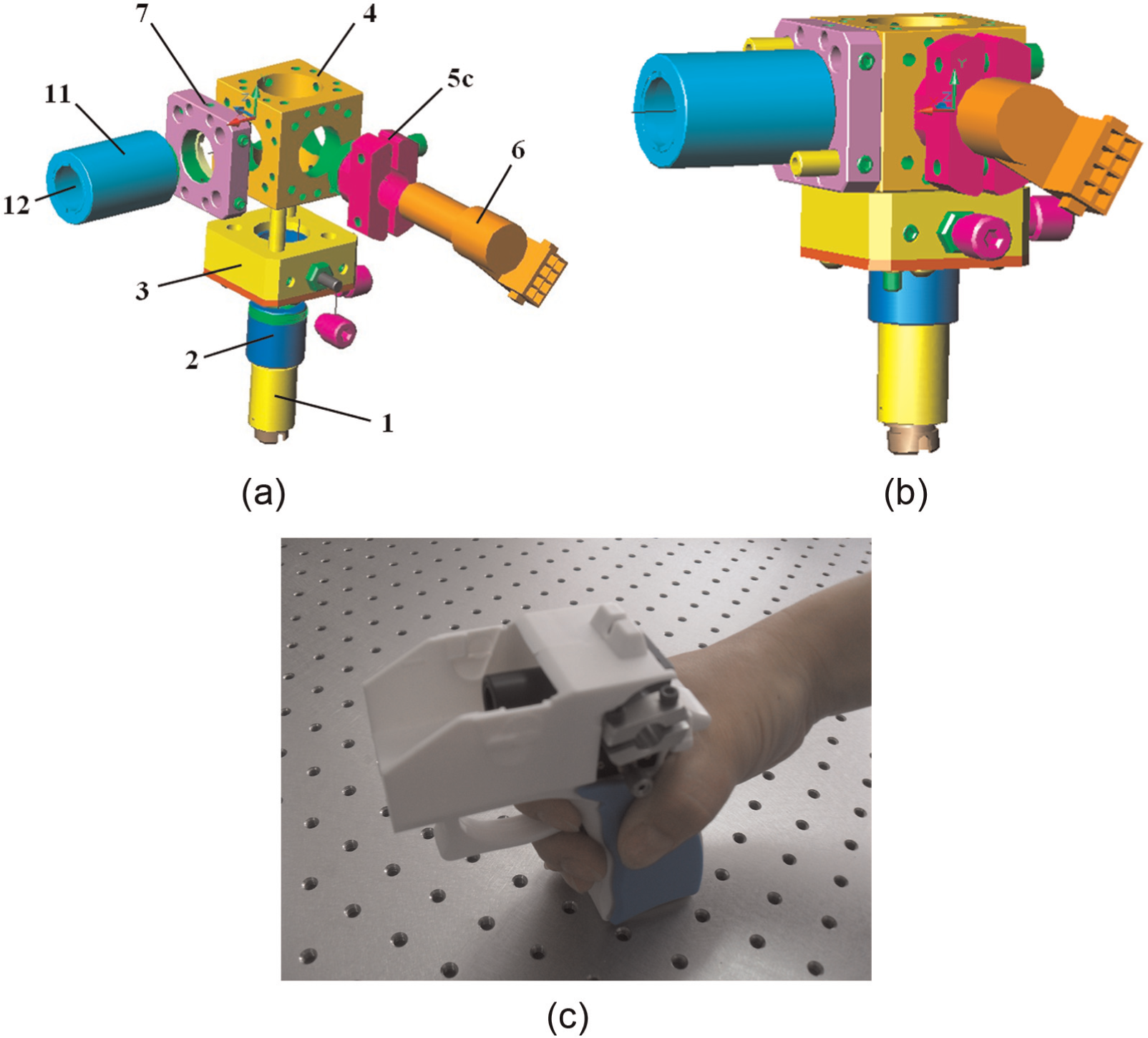
Second configuration of the handheld probe: (a) exploded view of the device (without the handle), with the same annotations as in Table 1 and Figure 1, except for the different mount (5c) of the GS; (b) assembly of the probe; and (c) probe mounted in a plastic handle (GS and cover removed for a better view of the GS mount).
One may see from the design shown in Figure 2 that such a handheld probe can be easily and rapidly assembled in any lab. Apart from the GS (Figures 1–3, (6)) and the fiber collimator (Figures 1–3, (1)), there are not any other components with significant costs. These optomechanical setups are thus suitable also for educational purposes, so to accommodate students with the internal anatomy of handheld scanning probes that they can build themselves and then employ with OCT systems in the laboratory.
Ergonomic prototype of a 1D GS handheld probe
Figure 3 shows another configuration of handheld probe, built with the same functionality but assembled with fewer components, in order to make it simpler, more robust, and less costly.
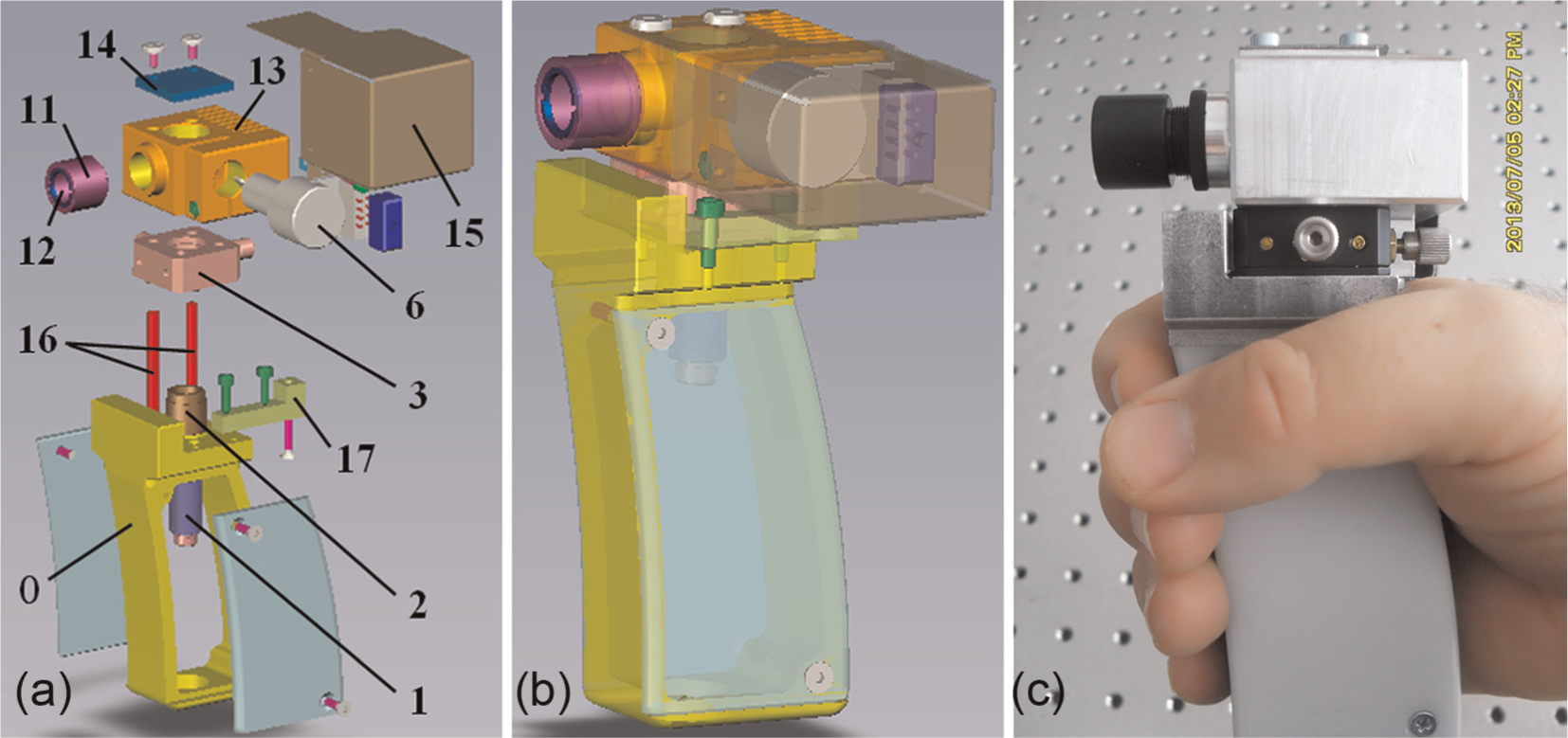
Final prototype of the OCT handheld scanning probe with the 1D GS, suitable for small scale production: (a) exploded view, with some of the same annotations as in Table 1 and Figures 1 and 2, but with a manufactured handle (0) and with a central part (13) that is both a mount and a heatsinker for the GS; (b) design of the assembly; and (c) manufactured handheld probe.
The assembly is mounted in a specially designed handle (Figure 3, (0)). This solution is more versatile, as it can include various and rather complex setups with 1D or 2D scanners, built on the same support of the translational stage (Figure 3, (3)). Apart from this handle (Figure 3, (0)), the central part (Figure 3, (13)), and the additional components (Figure 3, (14–17)), the same annotations as in Table 1 and Figure 1 have been used for the different components of the probe. The optical fiber (not shown in Figure 3) is connected to the collimator (Figure 3, (1)) which transmits the light beam to the objective lens (Figure 3, (12)) which focuses the beam on the sample. The laser beam is then backscattered and recollected by the collimator and the fiber.
We have already demonstrated the use of a type of this handheld probe in an OCT system in clinical applications, 30 with a similar design; however, this is the first presentation of its design.
Evaluation of the fulfillment of the instrument design requirements
The several aspects presented regarding the requirements of the instrument design were taken into account for all the three handheld probes.
The cage is made of an Al alloy (light and non-toxic), while the handles are made of plastic—totally (Figure 2) or in part (Figure 3). The probes are thus relatively light, as requested by users: 0.348 kg for the first probe (Figure 1), 0.276 g for the second (Figure 2), and 0.336 kg for the third probe (Figure 3). In comparison, commercially available probes are, for example, 1.5 kg (Envisu; Bioptigen, Morrisville, NC, USA), while a recent report pointed out MEMS-based probes with a minimum mass of 0.42 kg. 27 However, the latter costs higher and also require post-acquisition image correction due to the sinusoidal regime of the MEMS scanners. In contrast, the GSs are less costly, their frequency can be adjusted, and they can employ triangular scanning (linear on the active portions of the scan), which provides distortion-free images. 32 They are also employed anyway in most OCT setups to achieve lateral scanning; therefore, the effort to construct these configurations is minimal.
The testing of the probes has been done in the ENT Department of the Northwick Park Hospital in London (UK), for the OCT investigations of the ear, nose, and throat—as it has been presented in a former study, 30 and in the Imaging Group of the Victor Babes University of Medicine and Pharmacy of Timisoara (Timisoara/Timis, Romania), in dentistry applications—as it will be presented in an example in the next section of this study. It has thus been demonstrated that the probes are light enough and easy to handle for a significant duration (a few hours) in a medical environment throughout the day.
The material chosen was easy to process using conventional mechanical technologies: turning, milling, cutting, drilling, and wire cutting, the latter for the more complex components (Figure 3, (13)) and (Figure 3, (0)). Manufacturing with high precisions was possible on the active surfaces of the probe (e.g. on the inner cylindrical surface of the mount in Figure 4(d)). The robust design has allowed for the heat resistance, the structural integrity, and the maintaining of the imposed tolerances over more than 1 year of functioning of the product. A similar conclusion is expected for the lifetime of the probes, of at least 3–4 years. One also has to remark that because of the concept and of the simplicity of the handheld probes, they can be employed with any type of TD-, SD-, or SS-OCT systems.
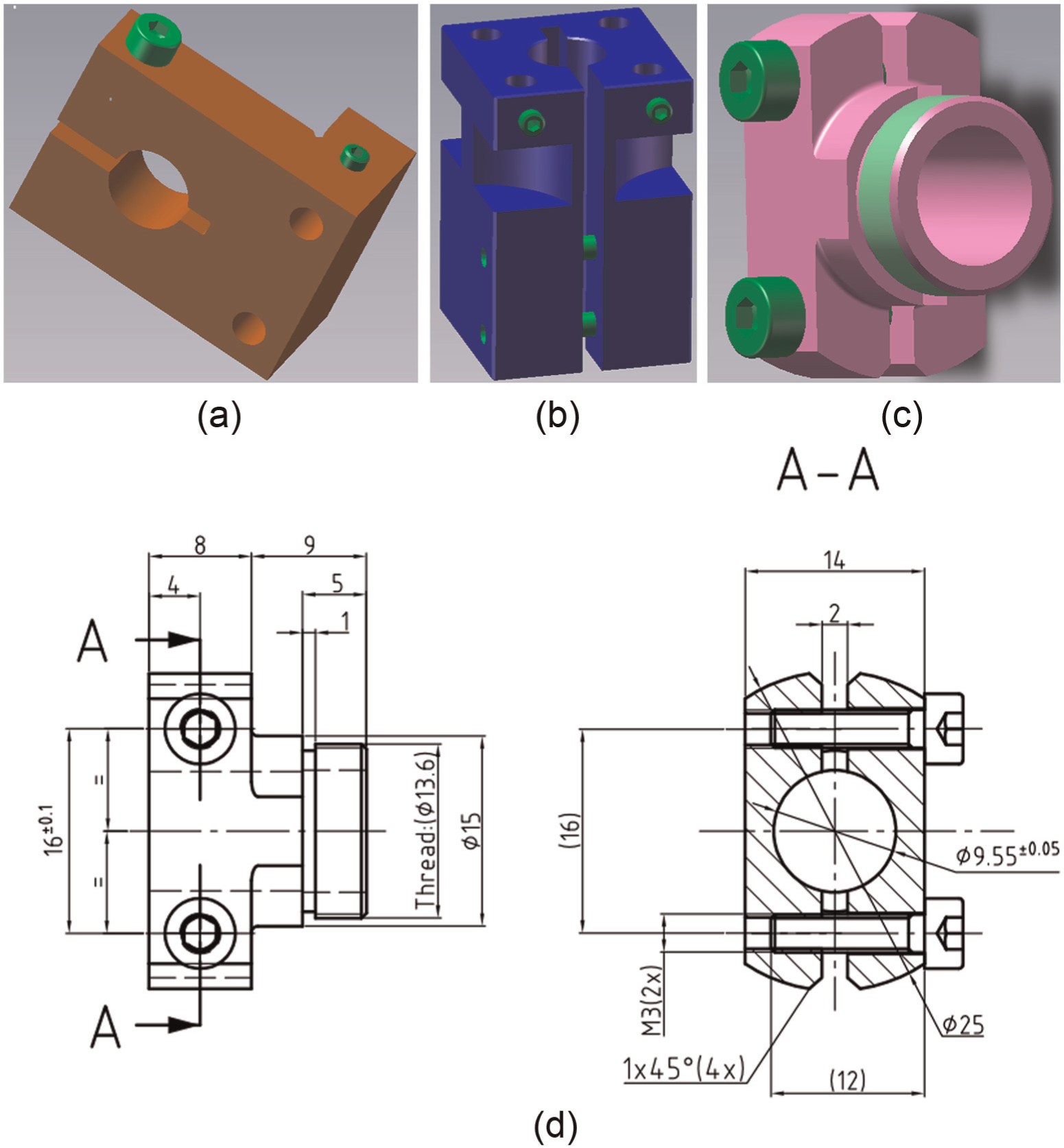
Mounts designed and manufactured to accommodate different types and sizes of GSs in the different handheld probes developed (a) for the first variant of handheld probe (Figure 1) and for a Cambridge Technology (Bedford, MA, USA) GS with a 4 mm aperture of the galvo mirror and (b) for a GS of the same type, but with a 5 mm aperture. (c) The mount used in the second design (Figure 2) with a Thorlabs (Newton, NJ, USA) GS with a 5 mm aperture. (d) Blueprint of the latter mount.
From the point of view of the necessary heat dissipation, a special part (Figure 3, (13)) was used to mount the scanner and somehow isolate it thermally. This part is also a heatsinker for the scanning device. The design was made to avoid the heat dissipation to propagate through the entire probe to affect the patient or the person who handles the probe.
Design and tolerances: In the concept of the assembly, the handle of the probe is distinct from its main part where not only 1D but also 2D GSs, as well as different lenses (Figures 1–3, (12)), may be used in the tube (Figures 1–3, (11)) to focus the laser beam at different distances, for example, for different parts of the body. This issue appears when switching from imaging the skin to imaging the ear 29 or the oral cavity (as it will be presented in the next section). The flexibility of the design thus allows for different functions and complexities of the probe: with a 1D GS B-scans are obtained (as shown in the following section); with a system of dual-axis 2D GSs mounted on the handle (Figure 3, (0)), both 3D reconstructions of the samples and C-scans (en face images) can be obtained. 3, 35
Tolerances as well as appropriate adjustment possibilities have been utilized—as discussed related to Figure 1 with regard to the role of the X–Y translation stage that aligns the optical axis of three components: the fiber collimator (1), the GS (6), and the objective lens (12). Thus, the main tolerances of the design refer to the collinearity of the axis of the collimator and lens, the perpendicularity of these two axes and of the GS, and the concentricity of the cylindrical mount of the GS and of the inner cylindrical surface where the GS is mounted (inner surface that has to be large and precise enough to allow for a tight, stable, and precise mounting of the scanner).
Mounting solutions have been designed for each type of GS used in the different configurations shown in Figures 1–3. They are different for each type of GS producer, and they also differ with regard to the necessary aperture of the galvo mirror. The three mounts we have developed are presented in Figure 4, as well as the drawing of the one used for the GS employed with the ergonomic design in Figure 3. This blueprint is provided because for the first two designs (Figures 1 and 2), these parts are the only ones that are not off-the-shelf components. This presentation therefore allows for the fulfillment of one of the aims of this work: to provide a complete design of the OCT handheld probes.
Testing of the handheld scanning probes on dental constructs
Two testing procedures of these handheld scanning probes have been completed so far. The first one has been carried on in the ENT Department of the Northwick Park Hospital (London, UK), as it has been previously reported. 30 An SS-OCT system developed in-house by the AOG of the University of Kent (Canterbury/Kent, UK), working at 1300 nm, has been coupled with both an endoscope probe head and a handheld probe (Figure 2). The latter configuration proved better transversal resolution and larger image size; it was used for either ex vivo OCT imaging of excised tissue or in vivo OCT imaging of directly accessible areas of skin and mucosa of the scalp, face, neck, and oral cavity. 30
The second OCT testing, which will be presented in the following, was performed in the School of Dentistry of the Victor Babes University of Medicine and Pharmacy of Timisoara (Timisoara/Timis, Romania) by using one of the variants of handheld probes developed. An SD-OCT setup developed in-house 36,37 by the AOG and installed in Timisoara was used to host in its sample arm the handheld probes. According to the protocols of the School of Dentistry, an extensive ex vivo testing has to be performed previous to passing to in vivo researches in the oral cavity. An example of such an ex vivo investigation is presented in the following. Its goal is to assess the functionality and the ergonomy of the probes (lightness, ease of handle for at least an hour), as well as to evaluate the OCT images obtained using the probes and to compare them with the OCT images obtained with a fixed scanning unit mounted in the SD-OCT setup.
The procedure for testing the handheld probes has been simple: they replaced the fixed scanning unit in the SD-OCT setup. The wires of the GS driver were coupled to the GS (Figures 1–3, (6)), and the optical fibers were coupled to the fiber collimator (Figures 1–3, (1)) in the probe. The switch from a fix to a mobile scanning unit has been thus demonstrated to be easy for all the designs.
As the simplest scanning solution, implying a 1D GS was used in the probe, only transversal images through the sample were acquired. Figure 5(a)–(c) shows three such OCT images (B-scans, in the terminology imported by OCT from ultrasound imaging) 35 obtained for metalo-ceramic dental prostheses. Several remarks can be drawn from these investigations:
There is a strong difference that can be easily identified between the metalo-ceramic (Figure 5(a)–(c)) and other types of prosthesis, such as metalo-polymeric (Figure 5(d)), because of the significant lower porosity of the ceramic material with regard to the polymeric one. This aspect helps the dental surgeon to recognize (using the OCT system plus the handheld probe) immediately the type of the prosthesis a new patient has in his/her mouth when coming for treatment for the first time.
Defects (D) in the depth of the material can be clearly seen on the OCT images in the metalo-ceramic prosthesis ((Figure 5(a)–(c)). The clinician can thus estimate the lifetime expected for a certain prostheses: if the defects are in critical areas of the prosthesis (top, root, or interface (I) between the teeth), then it is likely that the survival rate of the dental work will be low.
Open defects (DS), on the vestibular surface, are also clearly seen—simultaneously with those in-depth (Figure 5(c)).
The OCT images obtained using the probes were similar to the images obtained with the scanning unit mounted in the SD-OCT setup.
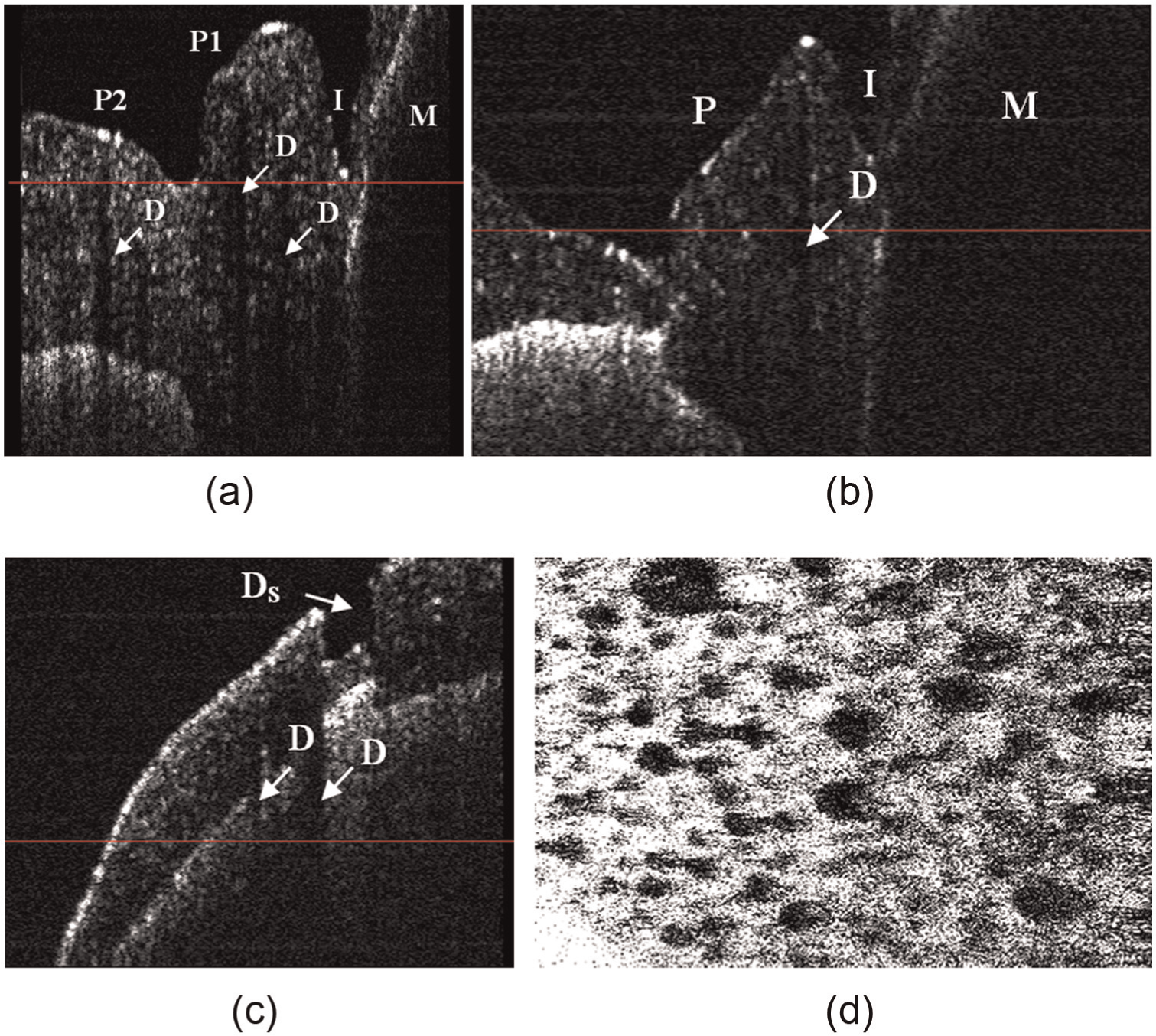
OCT investigations of metalo-ceramic dental prosthesis using the first type of handheld probe and a SD-OCT system: (a) B-scan of metalo-ceramic partially fixed prosthesis on the first molar (M) and on the first premolar (P1), investigated in vivo—defects (D) in the depth of the ceramic layers at the level of the interface (I) between the first molar (M) and first and second premolars (P2); (b) B-scan interface (I) of a metalo-ceramic partially fixed prosthesis with five elements pointed out an aeric insertions in the depth of the ceramic layers (one defect is shown as an example in the figure); (c) B-scan investigation of metalo-ceramic partially fixed prosthesis with an open defect on the vestibular surface (DS), but also with several defects (D) in the depth of the material; and (d) en face OCT image of a metalo-polymeric prosthesis obtained using the TD-OCT setup in our group (example considered to show the different porosity of the polymeric material).
Discussion
Three simple, easy-to-built, and low-cost OCT handheld scanning probes with 1D GSs have been designed in this study, manufactured as prototypes, and then tested. With their use on dental construct, the SD-OCT system allowed for a rapid, low-cost, and non-destructive evaluation of dental prosthesis. An entire range of other biomedical imaging applications in different parts of the body is also possible, as demonstrated by the previous OCT investigations in the ENT Department of the Northwick Park Hospital (London, UK). 30 To gain access in these areas, handheld probes are needed.
Both optomechanical design and practical construction of the probes were described in detail, to allow for their easy reproduction in any photonics laboratory, including for educational purposes. Indeed, they are suitable to be built by students, to accommodate them with OCT investigations using handhelds probes in various parts of the body. To the best of our knowledge, this is the first time such a detailed design was described—although there are numerous reports of functional handheld probes. The two initial designs described were made almost entirely from off-the-shelf components that are available in any photonics laboratory. Finally, these designs led to a simpler, more robust, and more ergonomic variant of handheld scanning probe for OCT, suitable for use in clinical environments.
Several aspects should be pointed out regarding the probes:
The mass of our devices ranges from 0.28 kg (for the probe in Figure 2—with a plastic handle) to 0.35 kg (for the one in Figure 1). In comparison, commercially available handheld probes for OCT range from 1.5 kg (Envisu; Bioptigen) to 2.2 kg (iVue; Optovue, Fremont, CA, USA). However, one has to point out that the latter two are not actually handheld devices, as they are placed on supports with several degrees of freedom. They can be moved around on these supports and thus they are placed in front of the area of interest, but they are not actually held in the hand; their degrees of freedom as well as the actual accessibility in any area of the body are actually limited. Such devices also include several parts of the interferometer, so they are integrated only with a specific OCT system, that is, those developed by each of the companies mentioned before. Therefore, our designs should more likely be compared with the most recent ones that have reported such probes with masses of 0.42–0.5 kg. 27
The costs of these latter probes have not been reported, but as they include MEMS, they are higher than those of our solutions, which include the less costly GSs. As it can be calculated from the data provided for the components in Table 1, the total costs of our handheld probes are €1434 for the probe in Figure 1 and around €1340 for the probes in Figures 2 and 3. It must be remarked that these costs include GS as the most significant part, which costs more than €850 (with driver card and driver card heatsink, both of them mounted on the fixed part of the OCT setup). The remark that has to be made is that this GS has to be included anyway in the OCT system, as well as the fiber collimator (1) and the objective lens (12); the latter two components have an overall cost of €250. Therefore, the additional cost of the handheld probe to the OCT setup is only around €250.
From a functional point of view, the handheld probes with MEMS scanners developed recently 27 require a post-acquisition image correction due to the sinusoidal regime of the MEMS scanners. These devices are also limited by the fact that they are resonant scanners, therefore they have a fixed scan/oscillatory frequency. In contrast, using GSs for the lateral scanning of the sample in the OCT system has certain advantages (besides lower costs): the scan frequency of the GSs is adjustable; they can employ triangular scanning, with constant scan speed on the active portions of the scan. As demonstrated, 32 the latter aspect provides images with fewer artifacts (i.e. distortion-free).
A limitation of our devices is the fact that they include only a 1D GS, therefore they can achieve only transversal images/B-scans (as demonstrated in Figure 5). To perform 3D reconstructions, one needs dual-axis MEMS 27 or 2D GSs; 21 the latter devices are the aim of our current and future works. However, for the designs developed in this study, the aim of our design has been to obtain probes as simple and low cost as possible. Even more, these handheld probes, which include only the scanner, can be utilized in any OCT configuration (TD, SD, or SS), which is also a plus. In fact, we have already demonstrated in our groups the use of these probes in a fixed TD and in a mobile SD-OCT system—in this study, as well as in an SS-OCT system in a previous study. 30
Different wavelengths can also be used with OCT systems coupled with these probes by properly replacing only three of their components: (1) fiber collimator, (6) 1D GS, and (12) objective lens (Table 1, Figures 1–3). Specifically, these components have to be C-coated for the 1050–1620 nm wavelength interval (as presented in this article for our 1050 nm and our 1310 nm OCT systems) and B-coated for the 650–1050 nm wavelength interval (as necessary for an OCT system centered at 780 nm).
The designs, as well as the manufacturing methods for the parts that are not off-the-shelf, were chosen in order to offer the readers the possibility to built easily their own OCT handheld probe: (a) almost entirely from off-the-shelf components (Figures 1 and 2), with only one adaptor, that is, the GS mount shown in Figure 4(d); (b) in a more ergonomic configuration, but with more parts to be manufactured (Figure 3). This aim of our work was the reason for not choosing manufacturing methods that could be more easily applied, such as rapid prototyping. 27
Testing of the probes was performed in this study on dental prosthesis with a mobile SD-OCT setup developed in our labs. The defects in the material were clearly identified, as well as the type of material used in the dental construction. We have done another, previous demonstration of the feasibility and ergonomy of one of the probes (i.e. the one shown in Figure 2) for OCT investigations in ear, nose, and throat, 30 as mentioned before. Future work will continue towards in vivo investigations in the oral cavity, both on hard tissue (teeth) and soft tissue (gums).
This research will also continue in our groups with other applications and with other handheld scanning probes with different complexities, appropriate for various biomedical imaging techniques. Of particular importance is the development of handheld probes that correlate OCT with confocal microscopy, 36 or with laser scanning ophtalmoscopy. 38 The scope is to take advantage of the conjugated performance of two techniques at once, especially in en face imaging. Endoscopic scanning probes included in the OCT handheld probes are also a main direction of research in our groups, for different applications of OCT. 39,40 This work places itself in the frame of our efforts to build 41,42 low-cost, precise prototypes of particular interest for photonics and biomedical applications.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by a grant of the Romanian Authority for Scientific Research, CNDI-UEFISCDI project PN-II-PT-PCCA-2011-3.2-1682 (![]() ). Cosmin Sinescu acknowledges the support of the TE 101/2010 CNDI-UEFISCDI grant. Adrian Gh Podoleanu acknowledges the support of ERC 7th Framework Programme, Advanced Grant “COGATIMABIO” 249889, of the NIHR Biomedical Research Centre at Moorfields Eye Hospital NHS Foundation Trust, and of the UCL Institute of Ophthalmology.
). Cosmin Sinescu acknowledges the support of the TE 101/2010 CNDI-UEFISCDI grant. Adrian Gh Podoleanu acknowledges the support of ERC 7th Framework Programme, Advanced Grant “COGATIMABIO” 249889, of the NIHR Biomedical Research Centre at Moorfields Eye Hospital NHS Foundation Trust, and of the UCL Institute of Ophthalmology.