
Abstract
An estimated 15% of patients seen by neurologists have neurological symptoms, such as paralysis, tremors, dystonia, or seizures, that cannot be medically explained. For a long time, such patients were diagnosed as having conversion disorder (CD) and referred to psychiatrists, but for the last two decades or so, neurologists have started to pay more serious attention to this patient group. Instead of maintaining the commonly used label of conversion disorder – which refers to Freud’s idea that traumatic events can be converted into deviant behaviour – these neurologists use the term functional neurological disorder (FND) and explain that the problems are due to abnormal central nervous system functioning. The situation that some patients with medically unexplained neurological symptoms are diagnosed with CD and treated by psychiatrists while others are diagnosed with FND and stay under the control of neurologists provides a unique case for analysing how neurological and psychological explanations affect subjectivity. In this article, I compare patient reports from English-language websites from the past 15 years to find out how minds, bodies, brains, and selves act and interact in the accounts of both patient groups. I conclude that the change in label from CD to FND has not only influenced ideas of medically unexplained disorders, but also affected ideas of the self and the body; of self-control and accountability.
Introduction
In October 2009, the former cheerleader Desiree Jennings became an American celebrity because of a rare movement disorder, believed to be caused by a flu shot. The 23-year-old woman came down with flu, ten days after the vaccination, and started to have seizures, which developed into severe movement disorders. According to the newspapers, she was officially diagnosed with dystonia – a disorder that causes involuntary muscle contractions – as a result of the vaccination (Chinn, 2009). On 16 October, the television news programme Inside Edition picked up the story and broadcast an interview with Jennings (Coffey, 2009). In the interview, it was shown how the woman had severe movement disorders while walking, but no problems while running; how she could not walk forwards, but was able to move backwards; how she had serious speaking problems, but spoke fluently when she was running. The fragment went viral on the internet and has been watched more than a million times. Many people soon began discussing the mysterious case, and several medical doctors decided that this could not be dystonia. 1 A few months later, Inside Edition published another interview in which Jennings was asked to respond to secretly filmed clips of herself driving a car and going shopping (see ‘Flu Shot Woman’, 2010; hopew213, 2010). Jennings answered with a strange accent and explained that she now had cognitive impairment due to her dystonia. This caused considerable uproar. In the media and on the internet, people discussed the ‘hoax’, and accused Jennings of ‘faking’ her problems (see Avila and Cohen, 2010). Videos were made to demonstrate that she was a liar, and to make fun of her – for example, by emphasizing her tremors and unusual movements with a rap rhythm (e.g. fadomon, 2009). Soon the diagnosis ‘psychogenic’ appeared. Jennings resisted the psychological explanation and persevered with her flu shot story, but the world laughed: it was all in her head, and she was denounced as faking her problems.
At a symposium on functional movement disorders for physiotherapists that I attended in 2017, Jennings’ case was presented and commented on by a neurologist as ‘quite a fuss that this happened after a vaccination, but this is clearly a functional disorder’. 2 Even in this setting, however, the case evoked some laughter from the audience, and one physiotherapist asked if these symptoms could also occur together with an actual neurological disorder such as multiple sclerosis. The neurologist confirmed this and added, ‘We have to leave the idea that this is different. This is also just a neurological disorder’. She noted that she told her patients, ‘If this was psychological, you would have stopped now’.
The presentation of Jennings’ case as a neurological disorder instead of a psychological problem illustrates a new way of thinking about medically unexplained symptoms. However, it also demonstrates some of the uneasiness: the laughing and the comparison with an ‘actual’ neurological disorder suggest a world with symptoms that are perhaps real, but not really real. The response of the neurologist emphasizes this; her addition that psychological problems can be stopped implies that neurological problems cannot. This suggests that there is less self-control in the neurological case then in the psychological. In this article, I compare self-reports of patients who see their (medically unexplained) symptoms as psychological with those of patients who see these symptoms as neurological. I focus in particular on how minds, bodies, brains, and selves act and interact in the accounts of both patient groups.
The patient, the mind, and the brain
The relation between neuroscience and understandings of self or personhood has been studied in different ways. Some neuroscientists and philosophers have presented the brain as the seat or the being of the self, and hence have argued that concepts such as consciousness or responsibility lose or change meaning (Churchland, 2013; Damasio, 2012; Swaab, 2014). Researchers in social studies of neuroscience have studied the impact of neuroscientific discourse on personhood and have argued that people who learn that behaviour is due to neurochemicals also learn to see themselves, their problems, and the causes of these problems in a neurochemical way (Dumit, 2003; Thornton, 2011). That is, neurochemical discourse – in neoliberal societies used not only by neuro-philosophers but also increasingly by doctors, schools, and the media – influences people’s subjectivity in the sense that it affects ideas of self, agency, and responsibility. Boldly stated, people are governed to become neurochemical selves (Rose, 2003, 2007), and personhood turned into brainhood (Vidal, 2009).
Other researchers, however, have relativized this effect on subjectivity and demonstrated that people who learn to understand their behaviour as neurological generally use a heterogeneous language of psychological and physiological statements (Bröer and Heerings, 2013; Broer and Pickersgill, 2015; Choudhury, McKinney, and Merten, 2012; Martin, 2010; O’Connor and Joffe, 2013; Pickersgill, Martin, and Cunningham-Burley, 2015; Rose and Abi-Rached, 2013; Singh, 2013; see also Brenninkmeijer, 2016). These discussions about the brain and the self are related to discussions about agency and responsibility: for example, because neurobiological explanations are believed to reduce responsibility for actions, or feelings of blame (Horstmann, 2017); because neurobiological discourse encourages people to improve their brains and hence makes them more self-responsible (Rose, 2007; Thornton, 2011); or, in a relativization of the reduction argument, because people with neurobiological diagnoses do in fact feel agency and responsibility (Singh, 2013). All these papers are fascinating, often empirical, studies on the influence of brain discourse on subjectivity. In none of these, however, has it been possible to actually compare neurological and psychological explanations in a single patient group. As I will show, the case of medically unexplained neurological symptoms does allow for such a comparative analysis.
In this article, I first explain how unexplained neurological symptoms can be diagnosed with different labels: conversion disorder (CD), diagnosed and treated by psychiatrists, and functional neurological disorder (FND), diagnosed and under the control of neurologists. Next, I explain how I have studied how these two labels relate to ideas of self, agency, and responsibility. I have analysed patient accounts on English-language websites from the past 15 years to find out how people who identify themselves as having CD and those who identify themselves as having FND explain their problems and the causes of these problems. In my analysis, I especially focus on how minds, bodies, brains, and selves act and interact in the accounts of both patient groups. Hence, I demonstrate that patients who understand their problems as neurological attribute less agency to their minds, brains, bodies, and selves, and seem to feel less blame and accountability for their problems, as well as less self-control, than patients with CD. I conclude by explaining why I think this is an important contribution for CD/FND experts, as well as to social studies of neuroscience.
The phenomenon and the diagnoses
The fact that case studies such as Jennings’ seem to tickle the funny bones of experts, who surely attend these symposia to learn how to help such patients, demonstrates their unfamiliarity with medically unexplained neurological symptoms. According to neurologists, however, such symptoms are actually relatively common. Moreover, they belong to one of the most common patient groups treated by neurologists (Stone et al., 2010). About 15% of the patients seen by neurologists have severe neurological symptoms, such as paralysis, tremors, dystonia, blindness, or seizures, that are not medically explained (Hallet, Stone, and Carson, 2016). In an interview study with neurologists, however, the psychiatrist Kanaan and colleagues conclude that many neurologists see themselves as agnostics in the treatment of these patients. In line with the responses to Jennings, they see this kind of problem as a form of deception: the patients are perhaps not outright ‘malingering’, but at least feigning their symptoms. As a result, neurologists have to ‘trick’ these patients into doing things they say they cannot do. It is a matter of ‘finding out’ whether the weakness is ‘real or not’ (Kanaan et al., 2009: 2891). Hence, neurological treatments for patients with neurological symptoms that remain medically unexplained have long consisted of proving that the symptoms are not (medically) real, and of referring these patients to psychiatrists (Rosebush and Mazurek, 2011).
For the last two decades or so, however, neurologists have started to raise the alarm about this patient group.
3
For example, they have referred to the private and public costs of these patients (e.g. over $20 billion a year in the US; Evens et al., 2015), or called these disorders ‘a crisis for neurology’: The nature of the crisis is that there are many patients, we don’t understand the pathophysiology, we often don’t know how to make the diagnosis, we don’t know how to treat the patients, the patients don’t want to hear that they have a psychiatric disorder and they go from doctor to doctor, psychiatrists don’t seem interested anyway, and the prognosis is terrible. (Hallett, 2006: 269)
A subsequent problem is how and what to tell the patient. Doctors can use numerous labels to diagnose these patients. A simple analysis of terms used on Web of Knowledge indicates that clinical neurologists seem to prefer the use of labels that refer to the non-medical origin of the symptoms, with terms such as functional, psychogenic, non-epileptic, or pseudo-symptoms, while psychiatrists especially emphasize the physical nature of the symptoms with labels such as medically unexplained or psychosomatic. However, this is not a clear division; in fact, all labels are used by both groups of experts. 4 And because there are many different symptoms, there are also many different names for the specific problems, such as psychogenic epilepsy, functional seizures, non-epileptic attack disorders, conversion seizures, non-organic movement disorders, psychogenic parkinsonism, psychogenic dystonia, and so on.
None of these labels, however, seems ideal. Patients easily feel insulted when they understand that their doctor thinks their illness is not in their body but in their mind (Stone et al., 2002). Labels with the word psyche (or worse, pseudo) are therefore not recommended by clinicians. The term conversion (or somatization) expects a psychological trigger and is too closely associated with Freud and hysteria. Medically unexplained suggests that there may be an explanation in the future; non-organic refers to something that is not; and the term functional disorder is seen as confusing because patients see their complaints as dysfunctional, instead of functional (Edwards and Bhatia, 2012). All of these labels are objected to, but the labels that refer to the psychological character of these symptoms, such as CD, psychosomatic, or psychogenic, are obviously the most commonly used. 5
This is about to change. Since patients with medically unexplained symptoms are one of the commonest patient groups in neurology, and because they often refuse to see psychiatrists, some neurologists have started to pay more serious attention to this patient group (e.g. Carson et al., 2000; Edwards, Stone, and Lang, 2014; Hallett, Stone, and Carson, 2016; Stone, Carson, and Sharpe, 2005). These neurologists have mainly agreed on using the term functional to indicate the absence of a medical explanation, because that term appears to be the most acceptable to patients and side-steps the ‘illogical debate’ about whether symptoms stem from the mind or the brain (Edwards and Bhatia, 2012; Stone, 2009). According to these neurologists, functional neurological problems are due to abnormal central nervous system functioning, and they emphasize that psychological triggers are not necessary – or even typical – causes of such problems (e.g. Edwards and Bhatia, 2012). The label was confirmed with a mention in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5): the category ‘conversion disorder’ is now extended with the subtitle ‘functional neurological symptom disorder’ in parentheses (American Psychiatric Association, 2013a). The use of FND has been consolidated through its use in a neurological handbook (Hallett, Stone, and Carson, 2016), on a website with patient information (www.neurosymptoms.org), and in a society (the Functional Neurological Disorder Society).
The (new) neurological approach differs from the more traditional psychiatric approach that presumes that patients with CD have unmanaged psychological or childhood traumas (Roelofs et al., 2002). Moreover, in agreement (and consultation) with these neurologists, the DSM-5 suggests that the diagnosis CD(FND) no longer requires a psychological triggering factor for the problems, and it emphasizes the need for neurological examination to demonstrate incompatibility with neurological disease (American Psychiatric Association 2013a, 2013b; Edwards and Bhatia, 2012). As a result of neurological examination’s becoming the main diagnostic instrument for CD(FND), many neurologists and patients have started to use the FND label and see this disorder as part of neurology (Demartini, d’Agostino, and Gambini, 2016). However, others – especially psychiatrists and their patients – continue to use the name CD and emphasize the psychological or psychiatric relation (e.g. Roelofs et al., 2002).
In short, although ‘FND’ appears as a label in parentheses after ‘CD’ in the DSM-5, in practice FND and CD are often used as separate labels. Some patients with medically unexplained neurological symptoms meet doctors who diagnose them with CD, caused by stress or a traumatic event, while other patients with comparable complaints are diagnosed as patients with FND due to abnormal central nervous system functioning. So, although the DSM-5 revisions were made partly to undermine mind–body dualism, not only the problems of CD and/or FND patients (physical problems without physical defects), but also the labels (FND or CD), and the causes (nervous system or trauma) implicate a certain form of mind–body dualism.
Methods
For this article, I analysed patient accounts on English-language websites from the past 15 years to find out how people who identify themselves as having CD and those who identify themselves as having FND explain their problems and the causes of these problems. As already explained, CD(FND) encompasses a range of very diverse problems and labels such as psychogenic epilepsy, functional blindness, non-epileptic attack disorders, non-organic movement disorders, psychogenic parkinsonism, and psychogenic dystonia. In studying the difference between CD and FND patient accounts, it is almost impossible to include all these labels – especially because they all have their own history and connotations. Hence, I decided to focus on the difference between the words conversion and functional. This means that I included only those patient reports that mention the words conversion or functional – or those that are found in the context of these words: for example, on a website about functional movement disorders or a blog entitled ‘Conversion Disorder’. In other words, I searched for patient websites and blogs on conversion and functional seizures, but not on non-epileptic attack disorder or pseudo-seizures – although these terms all refer to the same kind of problem. Patient reports on non-epileptic attack disorder and pseudo-seizures found on a functional/conversion website, on the other hand, were taken into account. Because of the overwhelming amount of information, I focused only on English-language websites, I did not include videos or vlogs, and I decided to exclude patient reports in newspaper articles – because these might have been affected by the journalists’ points of view.
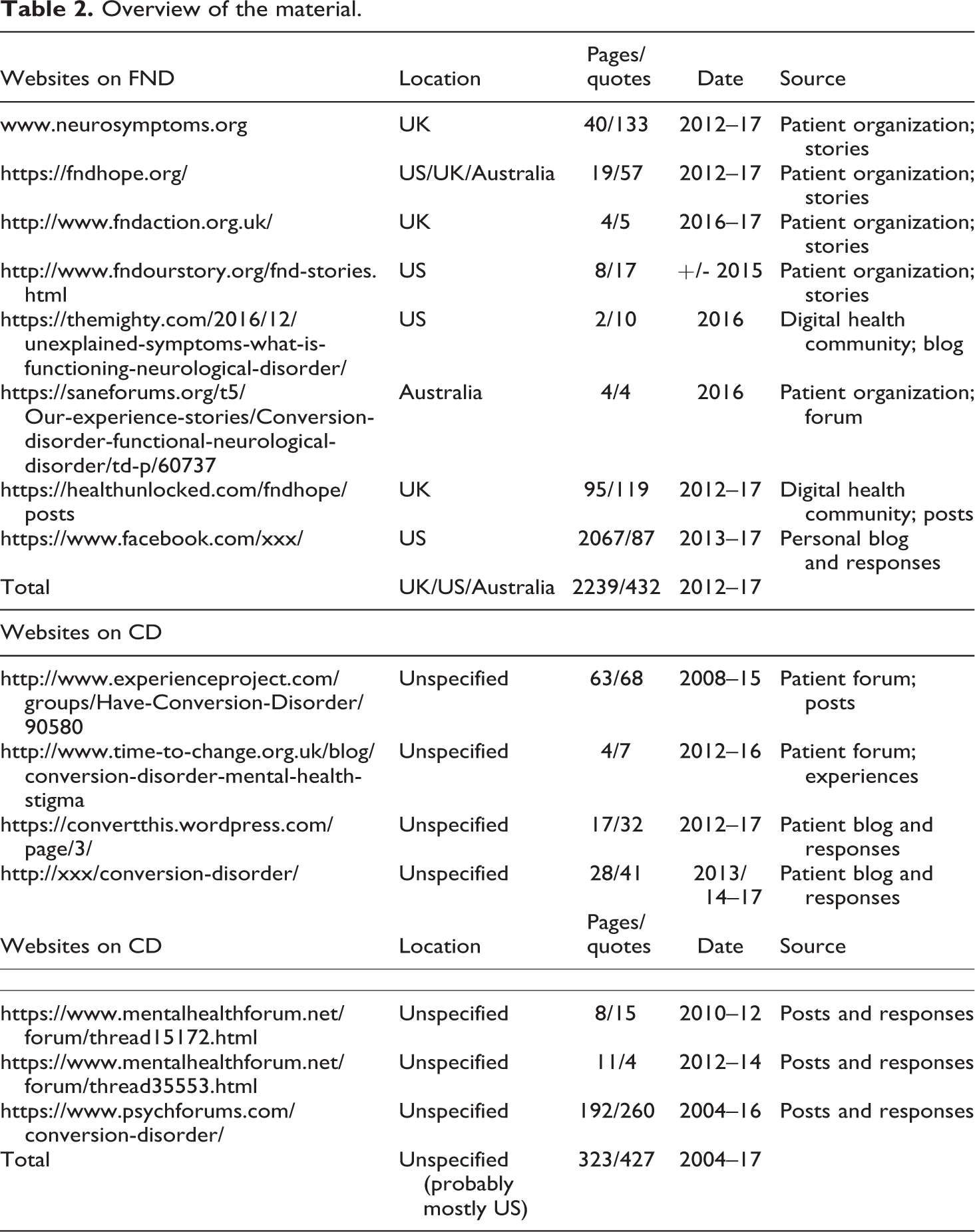
Since there are no clear ethical protocols for digital analysis, researchers generally develop their own guidelines, an approach that is also called ‘personal ethics’ (Ross, 2020; Samuel and Derrick, 2017). For this article, this means that I used only websites that were publicly available, that is, accessible without any form of registration. I searched for user guidelines to see if there were any restrictions with regard to the use of quotes, and if required, I asked the owners of the websites for permission. 6 To ensure the anonymity of the patients, as well as the readability of this article, I have not directly connected the patient quotes to their sources, but have listed all websites used in an appendix (see Table 2). Also, I did not use any quotes that could be harmful to the patient or that revealed any personal information. For this reason, I have also removed (family) names from the addresses of personal blogs listed in the appendix (replacing them with ‘xxx’). Spelling mistakes in the quotes were corrected.
My material on FND consisted of patient reports from the websites of patient organizations in the UK, the US, and Australia; posts on health forums; and posts on patient blogs. My material on CD consisted of posts on patient forums and patient blogs. If there were too many posts to analyse, I selected posts based on relevance (inclusion of ‘CD/FND’ in the title, posts written by patients instead of relatives, etc.) and replies/popularity. The countries of the patients posting these accounts were not always mentioned, but those specified were the US, the UK, Australia, or Canada. There was a slight difference in the material regarding time and sources. FND is a relatively new label and over the last few years, a number of patient organizations have been founded to raise awareness. As a result, all FND reports were posted after 2012, and about half of the FND material derives from the websites of patient organizations. The CD material, on the other hand, is collected from health forums and blogs, with most posts from 2011 and later, and some older posts starting in 2004 (see Table 2 in the appendix for an overview of the material).
In total, I analysed hundreds of pages on FND and CD with the help of ATLAS.ti, and this resulted in 432 quotes for FND patients and 427 quotes for CD patients (about 50–60 pages of quotes for each condition). 7 In these documents, I coded all relevant quotes with the words mind, body, brain, or self. For the body and brain codes, I did not include all general pains, feelings, or sensations in the body or brain, but focused on those quotes that expressed ideas, feelings, and so on concerning the body or brain. I added the code mind to sentences in which the mind (or subconscious, psyche, head, or soul) was discussed as a mental thing, different from the brain and the body, as in phrases such as ‘my mind never gets a rest’, ‘the body and the mind’, ‘the trauma/judge in my head’, and ‘my subconscious fear’ – but I did not include phrases such as ‘I don’t mind’ or ‘in your head’ in the sense of ‘making something up’. The code self was used for those quotes that discussed the self/myself/me/I in the context of identity (‘I know myself’, ‘I am a shadow of my former self’), or in relation to the brain, body, or mind (‘I can regain control over my body’). Simultaneously, I coded the documents with code words that indicated emotions and feelings (e.g. shame, frustration, confusion, in or out of control), experiences (rude professionals, ignorance, symptoms), and the ideas or explanations of patients (ideas about causes and treatments, metaphors). One quote could have (and most did have) several code words, and hence there were many more codes (1640) than quotes (860). The most frequently used code words are presented in Table 1: 8
Codes.
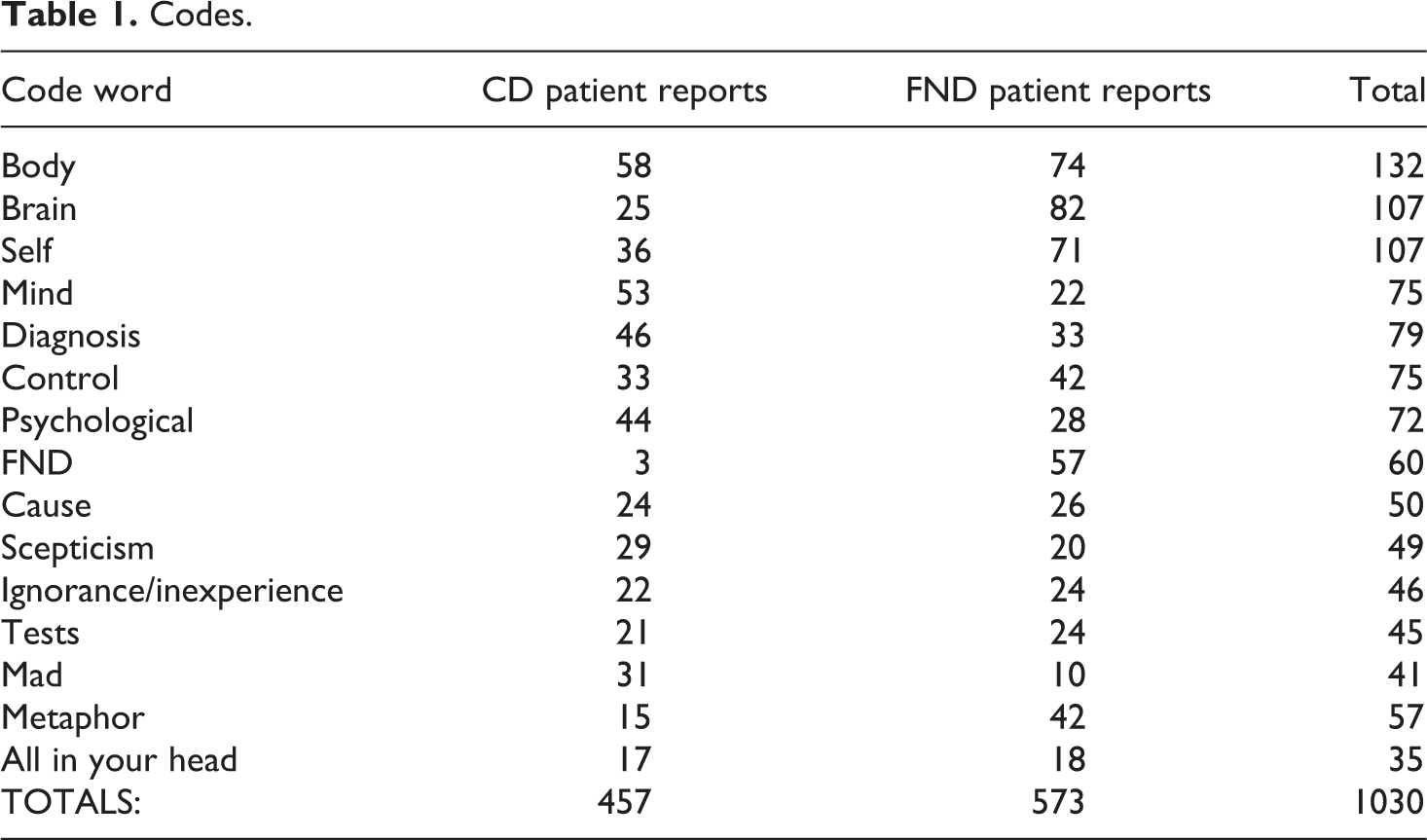
For this article, I mainly studied the quotes with the codes body, mind, brain, and self, and I used the other codes (such as control, blame, guilt, all in your head, mad, and scepticism) to see if there were any clear differences between the two conditions (FND and CD). 9 I especially focused on how minds, bodies, brains, and selves appeared in the accounts of these patients. Did these entities do something (e.g. say something) in a sentence? And if so, were their actions passive or active? How did these entities interact? Who or what (the self, the brain?) was appointed as accountable in these quotes? In the next section, I present my findings regarding brain, body, mind, and self struggles in FND and CD patients.
Analysis of FND and CD patients’ accounts
Reading the quotes about CD and FND shows many similarities. Patients suffer from very serious complaints, but they find it difficult to explain the causes behind these symptoms. They have generally seen many doctors and done many tests, and are looking for coping mechanisms or ways to accept their problems and to feel accepted by others. Patients who present their worries on CD forums talk much more about emotions and life events (trauma), and patients on FND forums talk more about brain paths and brain wiring. Moreover, if patients try to explain the causes behind their problems in more detail, the FND patients explain their brain mechanisms in terms of their reactions to food, gluten, or medicines, or they describe themselves as more vulnerable because of their genetic make-up. CD patients make fewer attempts to explain how their emotions or life events cause their physical problems, but they sometimes bring up a (de)activated amygdala, or a blocked chakra. It therefore appears to me that CD patients keep their explanations closer to their selves, while FND patients look for mechanisms outside themselves. Metaphors used by FND patients are often more technical: they talk about computer software, wires, crashes, and communication systems, while CD metaphors include cages, prisoners, shields, and dead animals. Since most explanations and metaphors concerned the brain, body, mind, or self, I closely analysed how these entities performed in both patients’ accounts.
Brains
Analysis of the quotes that mention the word brain reveals several ways in which the brain is used in sentences. Especially in the case of FND, the brain is frequently presented as an entity that is broken or does not work (or communicate) properly. Examples of this are comments that the brain (or its wiring) has ‘shut down’, or sentences such as ‘My brain can no longer handle all stimuli coming in – it says “time out” and shuts down my ability to move’. Other examples are sentences such as ‘My brain is broken which causes a paralysis of my body’, or structures like: the brain is ‘damaged’; ‘no longer works’; ‘crashes’, has ‘stopped communicating’, sends ‘incorrect messages’; ‘misfires’; or ‘can’t compute everything’. In most cases, there is no control over this brain (‘It felt like someone was playing swing ball with my brain’), but in other cases, the self tries to retain control: ‘[I have to press] the reboot button within my brain and take back control by reconditioning my brain’; (I have to) ‘reprogram’/‘retrain’ the brain. In other words, the FND brain is presented as a brain that does not function, work, or communicate properly (often due to a software problem). 10 It is a clear actor, but for the most part it acts passively or by malfunctioning. Only very few quotes (less than 10% of all FND brain quotes) express the idea of a brain that really acts, for example by making a decision or doing something (e.g. imploding or punishing).
In the CD reports, the word brain is far less prevalent than in the FND reports. But if the term is used, it is sometimes described as a memory reservoir: ‘This sort of thing can just sit there in the brain until it peaks’; ‘I was opening my brain’; ‘You have to destroy everything out of your brain’. In about half of the quotes, however, the brain functions as a clear actor. The brain is seen as a ‘powerful tool’; it ‘does’ something to the body; it tries to ‘warn you to slow down’; or it says, ‘Nope. Not doing that’. Other quotes reveal uncertainty about who or what is the persecutor in the situation: ‘Who’s lying my body or my brain?’; ‘Is it me myself making me ill or my brain that [is] doing it?’ And in a few quotes, the brain is just a passive thing – an intermediary, which may be causing the problem but without any intention (‘changes taking place in the brain that affect sensory & motor functions’); or which is expressed as a stranger (‘My brain is so weird’) or as an entity that can be cured (‘rewire your brain’).
This shows that the brain has a slightly different function in the FND and CD reports. In the FND patient reports, brains are often broken or do not communicate well. Metaphors often relate to a computer with malfunctioning software or as a miscommunicating element between brain and body. In the CD reports, the brain emerges as an actor, actively doing something, or it functions as a reservoir full of problematic memories that can cause trouble. In sum, the FND brain acts mainly by doing nothing, while the CD brain is powerful, and somewhat apart from the self.
Bodies
Studying the FND quotes regarding the code word body reveals images of a stranger: a body that does not respond, is not under control, is not understood, and is somewhat alienated from the person. Patients talk about ‘a very strange sensation’, ‘a fuzz’, or ‘feeling really weird in my body’, or note that the body ‘felt as though it was in shock’. They describe their body as an entity that is not controllable, that ‘didn’t want to work’, does not cooperate, makes ‘involuntary movements’, and acts in ways that are ‘not normal’ or not natural. The alienation is expressed in phrases such as ‘my body that isn’t mine’ and descriptions of a feeling that ‘someone else is in charge’ or ‘controlling’ the body; in one quote, the body is even described as ‘a separate entity to myself’. The body is mainly assigned a passive role. It is an entity that does not receive or respond to messages from the brain/person: ‘There was NO messages going to my right leg’; ‘The messages just don’t seem to want to tell my legs to move’; ‘I can’t remember how to do it no matter how hard I visualize my muscles working’. In other quotes, however, the body is assigned a more active role – it is seen as a hindrance (‘My body never stops throwing obstacles in my way’), a trap (‘slowly shutting down from the inside out’), or an actor acting against the person (‘My body seemed to go on strike’). In only a few sentences is the body described as the key to recovery: you have to ‘strengthen the body and mind’, accept your ‘new physical limitations’, or get to ‘know and understand your own body’.
Reading through the quotes coded with the word body in the CD category initially yields many images of a dead body. Sometimes literally: ‘I felt like a dead body waiting to be taken to the morgue’; ‘kinda like animals that play dead’. Other times more figuratively: ‘My eyes were usually open, staring blank’; ‘My legs go grey and cold’; ‘an out-of-body experience’. Other expressions symbolize the body as a cage: patients feel ‘trapped in their bodies’; ‘It’s like being a prisoner in your own body’; ‘My body just goes into the shutdown mode’. Some quotes reveal that there is no control, and that the body acts against the will of the person. The body ‘does not work properly’; is ‘odd’; is ‘flaking out’; there is ‘no understanding’; the patient feels ‘betrayed’ by their own body. What is especially notable in comparison to the FND quotes, however, is that the body is often assigned a much more active role: problems occur because the body ‘received’, ‘relives’, or ‘handles’ a trauma – the body ‘counteracts’ fear or responds to specific actions (‘I stopped my body from doing what it wanted to do. Big mistake. The numbness started in my legs, then arms’). The body is ‘trying to tell’ the person something; ‘protects’ the person; does not want the person ‘to remember what’s happening’. It ‘doesn’t know how to deal with it anymore’; it ‘is mirroring your consciousness’ and ‘expresses memories’. Symptoms are therefore often seen as bodily flashbacks of traumas. And this seems to point to another actor (self? mind?) that is accountable for the problems with the body.
FND bodies are often seen as unresponsive and alienated. CD bodies, on the other hand, are quite active. They respond to the person, for example by causing problems, or they function as a cage, keeping the self imprisoned. In some situations, the body is experienced as so dysfunctional that the image of a dead body arises. Compared to the brain, however, the body appears to be more powerful in the CD than in the FND reports.
Minds
Regarding the word mind (and related terms such as subconscious and psyche), FND patients do not use these terms very often. If they are used, it is often in combination with the body, indicating a dualistic way of thinking: ‘strengthen the mind and body’; ‘My mind and body doesn’t get into stress’; ‘[Everyone wants] our old mind and body back’. On one occasion, the word mind is combined as ‘mind and soul’, and in another quote, the brain and mind are contrasted with the body: ‘The problems are to do with the brain and mind, not the arm or hand’. Sometimes the mind takes on the role of a troubled psyche: ‘a whole weight of my mind’; ‘it was difficult on my psyche’. In other quotes, the mind becomes a passive or indirect actor: ‘The veil descends over my mind and I am disconnected from the world around me’; ‘[I needed to] take back control by reconditioning my brain and ultimately my subconscious’. And in a few sentences, the mind emerges as a clear actor: ‘that enabled the subconscious mind to access basic movements’; ‘my mind finally decided’; ‘Can my own mind cause this?’.
Patients classified as having CD, on the other hand, mostly present the mind as an active agent: the mind ‘manages’, ‘chooses’, is ‘telling your body’ or ‘telling you’ something, ‘fights’, acts as ‘a judge’, ‘causes’ pain or paralysis, ‘defends you’, ‘stops you’, ‘hides something from you’, ‘make[s] you believe’, ‘deals’, and ‘thinks’. It is described as ‘a mystery’ and as a ‘mysterious and fascinating thing’. In some quotes, the self openly struggles with the mind: ‘If it is a mind issue, why doesn’t me wanting it to go away work?!!!!’; ‘My mind is mine, I am not my mind’. In other explanations, the mind is more integrated – part of the self: ‘I lay here, on my couch, fighting with all my mind, soul and heart to keep the seizures away’; ‘I can’t fly physically, but my mind has perfected the art of running away by dissociating’. And in some sentences, the mind is more passive, or functions as a reservoir: it is the place where ‘psychological traumas’ or ‘illnesses’ originate; it picks things up ‘subconsciously’; and to get better, you have to ‘destroy anything in your mind’ or ‘figure out as much about one’s mind as possible’. In quite a few quotes, the mind is mentioned in combination with the body, but often in a more interactive way than in the FND quotes. Although some quotes simply refer to the mind and the body (‘feeling through your mind and body’; ‘My mind/body reacted’), many others express the idea that the mind ‘influences’ the body, or that they are ‘interlinked’, ‘connected’, or ‘working as one’.
FND minds are not particularly active, and they mainly appear in dualistic relations with the body or self. The CD mind, however, is expressed as a very active agent: it does all kinds of things (fighting, saying, stopping), struggles with the self, and interacts with the body. Occasionally, it functions as a reservoir, comparable with the brain reservoir. Also, when the CD mind emerges in a dualistic relationship, it does so in a more active way than the FND mind.
Selves
FND quotes regarding the self (or myself/me/I) are often about control, and in most of these quotes the self is not in control. People express surprise (‘Apparently I was cursing which I never had done’), confusion (‘I knew very little about what was going on in my body’), and powerlessness (‘There was nothing I could do to make myself move’). Sometimes people feel defeated (‘I was trapped inside a body’), or they see the self as an entity that has disappeared (‘The person I was has gone’). This feeling of powerlessness often appears as an internal conflict. The self struggles with the body or the brain. In other words, the self is involved in a dualistic conflict (‘My leg wouldn’t want to walk when I wanted to’; ‘My brain goes into shock if I try’), or even in a tripartite conflict (‘I was told to stop concentrating so hard because my brain was getting in the way of my body’s natural ability to move’; ‘If I bend my wrists my brain implodes like I have broken a bone’) (emphasis added).
Similarly to the FND reports, the self quotes in the CD reports are often about control, and on most of these occasions, the self is out of control. However, in comparison to the FND reports, CD patients talk more about getting control, finding ways to recovery, or accepting the situation, and less about losing control or losing the self. 11 In relation to the FND-self, the CD-self actually emerges as quite a resilient entity:
In other sentences, however, there is no control at all: ‘My will is swallowed up in mechanisms I can’t control’; ‘I kept begging my body to stop shaking’. Sometimes, this feeling of uncontrollability results in confusion: ‘[I] feel totally confused by my own body and mind’; ‘I can’t trust me any more cos I don’t know who’s lying my body or my brain’. It even evoked a form of aggression: ‘I’m starting to hate me’; ‘[It’s] a form of auto-aggression, I hate myself for feeling whatever is beyond that, I am “beating myself” per the movements’. However, in contrast to the FND reports, there are no signs of losing the self, apart from one quote in which a patient questions the agency of the self (‘Do I exist in that moment?’). And only few sentences reveal a self–body–brain interaction in comparison to the FND quotes: ‘I do not understand how my brain can do this to my body’.
In the FND reports, therefore, the self/me is often overruled by other entities (mind, body, brain), or struggles with them. The CD-self is relatively optimistic. It is a resilient self, striving for control. In some quotes, there is no feeling of control, and the self is confused or even aggressive, but in none of these quotes is the self defeated or lost.
Agency and control
In the CD reports, the brain is not presented as an entity that is broken – as in the FND reports – but, peculiarly enough, as an entity that acts against the body, mind, or self. This suggests that in the neurological case, the brain is more often seen as an organ that is damaged or does not work sufficiently well, while in the psychiatric focus, the brain is a reservoir of threatening memories (which can pop up in various forms), or an entity that actively acts against the self: ‘It says: “Nope. Not doing that”’. The brain seems to have more agency in the psychiatric setting than in the neurological setting. Bodies in both sets of reports show a comparable trend: FND bodies are experienced as something strange and out of control, while CD bodies act upon or respond to the person. Moreover, the body seems to be more related to the self in the case of CD than in that of FND: it is expressed as a reservoir (or dead body) that handles the patient’s traumas or an alienated entity that does not respond. FND minds have almost nothing to contribute, while CD minds are active, working to handle traumas, telling the patient things or protecting them. Comparing the self quotes in both kinds of reports, it appears that in both sets most quotes are about feelings of not having control, but the proportion of quotes that express attempts to retain control is higher in the CD than in the FND group. In comparison, the CD quotes appear to be more about getting control, while the FND quotes are more about losing control.
This suggests that people who see their physical problems as a result of their broken or miscommunicating brain do experience less control over their behaviour than people who see their physical problems as a result of a struggling mind (e.g. stress or trauma). In the following quote, from a (sceptical) patient on a CD forum, this difference is specified: I was hospitalised for 4 days two weeks ago where I underwent my 5th MRI in a year and a half and a brain scan. Again the docs are sure that it is conversion BUT are contradicting themselves. Before this episode I was under the impression that CD was triggered by stress and so I was involuntarily paralysing myself. Now they tell me that it’s not my fault, that I have no control over it and that CD is due to a chemical imbalance. Have you ever heard this kind of diagnosis before? In my layman’s interpretation what I now understood was that my brain was not diseased, nothing had physically broken, however sub conscious communication had broken down, automatic responses had become overloaded by corrupt messages and now my brain had gone into red alert, causing my body to over react and therefore swinging between extremes. There was nothing I could do to rein in control, in fact the more I consciously tried to overcome the situation the more my symptoms would become exasperated. It was not my fault, it had just happened. Have you ever had someone ask you if you want a cup of tea and you have to stare at them for five minutes before your brain has processed the appropriate response? During a hospital stay, I was repeating my symptoms to every nurse and aide with each shift change so they were clear. I know they [health professionals] communicate, but that doesn’t stop a panicked nurse from waving smelling salts under my nose when I’m staring blankly, unresponsive, while inside I’m saying, I smell it! Get it away, please! I beg you! I’m awake!
In the CD reports, in sum, the brain, the mind, the body, and the self all play a relatively active role, but the role of these entities in the FND reports is much more passive. The result of this appears to be that FND patients do not only experience less control over their situation, but also feel less accountable for their problems. Hence, it can be assumed that while CD patients experience more agency, and perhaps more control, they also experience more feelings of blame or guilt. Analysing the quotes coded with blame, guilt, and faking supports this. Of the 47 quotes for these codes, 13 belong to the FND reports, and 34 to the CD reports. Of the FND quotes, only 4 are about feelings or doubts about blame (‘I had no one else to blame but myself’), while the other quotes confirm that blame is out of the question (‘I am not making myself do them [seizures]’) or belongs to the past. Of the 34 quotes in the CD group, most are about others who blame the patient or accuse them of faking (‘The doctor I saw totally thought I was faking’). Other quotes directly reveal feelings of accountability (‘I am responsible for all this and I can’t stop it’), and only a few confirm that the person is not faking or to blame (‘I am NOT faking this’). This suggests that people who identify themselves as having CD do indeed seem to have more problems with feelings or accusations of blame than people with FND.
In general, CD patients seem to use more emotional terms (angry, alone, confused) than FND patients, and in particular, they more frequently report being seen as crazy or being told by doctors they could not help them (‘No doctors have done anything for me’; ‘My physician has never treated anyone with CD and he refers to my problem as being “goofy”’). Both groups report that their problems are seen as ‘not real’, but the FND accounts demonstrate that this idea of reality is closely connected to biology: ‘This article says it may not be all in your head, but in the temporoparietal junction in the brain.…Take that with you as proof you’re not faking it!’ While CD patients make more frequent mention of not being taken seriously, FND patients generally show relief that their problems are not in their head but in their brain.
12
One FND patient report clearly illustrates this difference: I kept asking the doctor, but his answer was always, we did all kinds of tests and there is nothing there, believe me it’s only in your head, go to see psychiatry. Every time I stepped out of the doctor’s office, I was so frustrated. I felt so humiliated, how could my problems be only in my head? I was not making them up, I couldn’t walk, not talking about other symptoms going with it. My problems were real.…Finally I had a doctor who believed me, who said yes your symptoms are real, you are not making them up, there is more people like you, it is not in your thoughts, your brain under some circumstance doesn’t work like it should. What a relief it was!
Conclusion
In the DSM-5, the label CD was extended to FND: the diagnosis no longer requires a psychological trigger, and the need for neurological examination is emphasized. In practice, however, there seem to be two patient groups: CD patients, who are diagnosed mainly by psychiatrists and learn that their problems are due to psychological triggers; and FND patients, who are diagnosed mainly by neurologists and who learn that their problems are due to a problem with the functioning of the nervous system. CD is still the label most commonly used, but FND is advancing, especially because of a group of neurologists raising awareness of the disorder. In their information, the term CD is rarely used, and they emphasize that there is no difference between the mind and the brain: ‘It is the stuff between your ears’. 13 My comparative analysis, however, has demonstrated that in practice, it is not that simple. There are minds, brains, bodies, and selves all over in the accounts of both patient groups, and patients using the FND label assign less agency than CD patients not only to their minds, but also to their bodies, brains, and selves. They seem to experience not only less blame and accountability for their problems, but also less self-control.
Although the transition (or extension) of CD to FND was made to improve healthcare for CD/FND patients, therefore, something has also been lost. Feelings of agency, self, and having (some sort of) control are reduced and replaced by the introduction of the autonomous brain and nervous system that sends and/or receives messages incorrectly. This explanation reduces feelings of blame, guilt, and making things up, because the brain and the nervous system seem to make the disorder more ‘real’. However, the downside of this brain interpretation is that it also emphasizes the idea that only what can be found in the body or brain should be considered ‘real’. As a result, instead of taking the problems, experiences, and feelings of patients as the ‘evidence’ on which to base a diagnosis, the brain is used to give these patients a ‘real’ disorder that they are not accountable for (see also Hustvedt, 2013).
The case of CD/FND is illustrative of what is happening with many classifications in psychiatry, which are being increasingly related to the brain. Patients seem to prefer biological above psychological problems, but the search for biological substrates also emphasizes the idea that ‘real’ problems have to be anchored in flesh. This assumes that those problems that are not biological are not real. The neurologist’s remark at the FND conference – ‘If this was psychological, you would have stopped now’ – illustrates this. Again, this suggests that we do have control over, and are responsible for, what is psychological, but not what is neurological. And this is exactly how FND patients seem to relate to the brain in their accounts: as an uncontrollable, unaccountable entity.
The findings in this article may complicate the idea of FND experts who hoped to undermine mind–body discussions, but they also seem to complicate contemporary ideas in social studies of neuroscience about the neurochemical self that is especially addressed for its self-responsibility and self-management (e.g. Broer and Pickersgill, 2015; Pitts-Taylor, 2010; Rose and Abi-Rached, 2013). Moreover, in addition to what is often assumed (Racine et al., 2017) but not really demonstrated (e.g. O’Connor and Joffe, 2013), the comparison between CD and FND patient accounts suggests that neuroscientific explanations do challenge our notions of free will (or self-control) and moral responsibility. FND patients ascribe less agency and control not only to their brains and minds, but also to their bodies and selves. Metaphors of the brain as a computer with hardware and software not only influence ideas of medically unexplained disorders, but also affect ideas of the self and the body; of self-control and accountability.
Footnotes
Appendix
Overview of the material.
| Websites on FND | Location | Pages/quotes | Date | Source |
| www.neurosymptoms.org | UK | 40/133 | 2012–17 | Patient organization; stories |
| https://fndhope.org/ | US/UK/Australia | 19/57 | 2012–17 | Patient organization; stories |
| http://www.fndaction.org.uk/ | UK | 4/5 | 2016–17 | Patient organization; stories |
| http://www.fndourstory.org/fnd-stories.html | US | 8/17 | +/- 2015 | Patient organization; stories |
| https://themighty.com/2016/12/unexplained-symptoms-what-is-functioning-neurological-disorder/ | US | 2/10 | 2016 | Digital health community; blog |
| https://saneforums.org/t5/Our-experience-stories/Conversion-disorder-functional-neurological-disorder/td-p/60737 | Australia | 4/4 | 2016 | Patient organization; forum |
| https://healthunlocked.com/fndhope/posts | UK | 95/119 | 2012–17 | Digital health community; posts |
| https://www.facebook.com/xxx/ | US | 2067/87 | 2013–17 | Personal blog and responses |
| Total | UK/US/Australia | 2239/432 | 2012–17 | |
| Websites on CD | ||||
| http://www.experienceproject.com/groups/Have-Conversion-Disorder/90580 | Unspecified | 63/68 | 2008–15 | Patient forum; posts |
| http://www.time-to-change.org.uk/blog/conversion-disorder-mental-health-stigma | Unspecified | 4/7 | 2012–16 | Patient forum; experiences |
| https://convertthis.wordpress.com/page/3/ | Unspecified | 17/32 | 2012–17 | Patient blog and responses |
| http://xxx/conversion-disorder/ | Unspecified | 28/41 | 2013/14–17 | Patient blog and responses |
| Websites on CD | Location | Pages/quotes | Date | Source |
| https://www.mentalhealthforum.net/forum/thread15172.html | Unspecified | 8/15 | 2010–12 | Posts and responses |
| https://www.mentalhealthforum.net/forum/thread35553.html | Unspecified | 11/4 | 2012–14 | Posts and responses |
| https://www.psychforums.com/conversion-disorder/ | Unspecified | 192/260 | 2004–16 | Posts and responses |
| Total | Unspecified (probably mostly US) | 323/427 | 2004–17 |
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.