
Abstract
Forrester’s proposed seventh style of reasoning – thinking in cases – functions as an analogous, dyadic relationship that, whilst indebted philosophically to the logical reasoning and semiotics of Charles Peirce, is prone to creating feedback loops between induction and deduction, precluding novel abductive hypotheses from advancing medical knowledge. Reasoning with a Peircean triadic model opens up the contexts and methods of meaning-making and reasoning through medical cases, and the potent influence of their genre conventions, to intellectual critical scrutiny. Vitally, it offers a third mode – abduction – that this article argues needs to be reintroduced into Forrester’s model of reasoning with cases. This article demonstrates this by applying a Peircean triadic model of reasoning to Forrester’s own model, tracing a shared genealogy but one in which the abductive element was lost. The article goes on to illustrate the explanatory and predictive potential of Peircean abductive reasoning and the necessary re-theorising of the case this entails. This argument is supported through an analysis of early case reports of what would become HIV/Aids, drawn from the Case Records of Massachusetts General Hospital series in the New England Journal of Medicine.
Abduction as syllogism
The surprising fact, C, is observed;
But if A were true, C would be a matter of course,
Hence, there is reason to suspect that A is true. (CP 5.189) 1
The above, by way of introduction, is a syllogistic expression of the nature of abduction by Charles Peirce, the American logician and semiotician who provides one of the two wholly unrelated lineages for the semiotics-suffused (post-)structuralist movements across a range of disciplines in the 20th century, including anthropology, literary and cultural studies, and continental philosophy. The other, and more famous, line descends from the linguistic semiology of Ferdinand de Saussure.
At the heart of this article’s argument is a conceptual position rendering the medical case (and its component facts, symptoms, treatment regimens, causes, and outcomes) as a semiotic sign, within a constellation of such meaning-generative signs, thereby casting discourses of medical knowledge and practice as a rhizomatic and dynamic semiotic. This represents a potentially radical new way of understanding not just the medical case or other medical narratives, but medicine itself. However, the clarion call for this epistemological shift has sounded before, most notably with Eugen Baer’s monograph on Medical Semiotics (1988) and papers such as Nessa (1996), Brands, Franck, and Van Leeuwen (2000), and Staiano-Ross (2012), yet there never follows any further rush onto the battlefield. Biosemiotics as an area of academic research certainly exists, as a slow-growing presence evidenced by the recent publication of Goli (2016), but it has little or no profile within the UK and has failed to materialise in clinical education, let alone influence clinical practice, in English-speaking countries (Tredinnick-Rowe, 2017). Cases, however, for all their anachronistic character and their openness to accusations of anecdotalism and ascientism, persist as a penumbral character on the dual scenes of medical education and clinical pedagogy and practice in the UK. By applying a semiotic approach to the medical case, and the thinking with cases described by John Forrester (2017a), this article will both answer and advance Forrester’s formulation and be a landmark instance of (bio)semiotic methods of thought in UK medical theoretical discourse, from there to prove a valuable step towards its inclusion in medical training and practice.
Very bluntly, a new holistic method of thinking about cases, about diagnoses, about the constitution of disease or (ill) health, about medicine itself – as an epistemology, as a healing craft, as an industry – is urgently required. The 20th century saw positivist assumptions – in politics, in the arts, in history, and throughout the sciences – troubled and overthrown. Not so, medicine. Whilst 21st-century thinking is increasingly pluralistic, polyphonic, responsive, relativistic, and dialectical across disciplines and sociopolitical practices, medicine as formally taught, practised, and conceptualised has continued a retrenchment, a calcification even, into structures of thinking and behaviours best described as bureaucratic, institutional, and technocratic. The medical semiotic revolution – only hinted towards in what follows – dynamites a monolithic edifice constructed on the ideologically motivated lie of supposed immutable fact, seeding in its place an organic rhizomatic growth assembled through layers of polyvalent and antagonist meanings. In this, medicine can be remade – both in structure and in content – in the image of that real life to which it must tend.
Although this will entail some involved semiotic theoretical thinking, what is at stake is far from abstract or just the playing-out of some niche Peircean logic game. This article will – by putting a Peircean semiotic reasoning method to work on published cases in the early years of HIV/Aids research – argue forcefully that an incomplete analogic method of reasoning inductively from case to case, as espoused by Forrester, allows (forces, even) medicine to retreat into vague untheorised circular thinking about new, paradigm-breaking diseases, where the a priori prejudices and uninterrogated habits and assumptions of thought are rediscovered as supposed facts and results. Behind the logical formulae and semiotic analysis is a heartfelt plea coming from common ground with Forrester: better medical thinking with cases is a matter of life and death.
For the reader unfamiliar with semiotics, it will be helpful first to explain the nature of the Peircean sign around which this medical semiotic is organised. For Peirce, the sign was simply ‘something that stands to somebody for something in some respect or capacity’ (Peirce, 1955c: 99), and he formalised this into an indivisible triadic sign, comprising a Representamen, an Object, and an Interpretant. In this, the Representamen in the position of Firstness, as a thing in itself, is the ‘something’, say a drawing of a tree. The Object in the position of Secondness, as a thing in relation to another thing, is the ‘that for which the something stands’, which would be the abstract concept of tree-ness. Finally, the Interpretant in the position of Thirdness, as a thing for which two other things are placed in a relation, is the ‘somebody to whom that something stands for something’. This would be any receptive mind suitably culturally situated and sensorily endowed to understand the image as corresponding to the concept (see Figure 1). To pre-empt this paper’s argument, the medical Peircean sign can be illustrated with reference to the clinical appearance of Kaposi’s sarcoma in a previously healthy young male homosexual – the Representamen – that ‘stands for’ the presence of the newly described HIV/Aids disease – the Object – to the medical practitioner at the specific epistemological, historical juncture of orthodox ‘Western’ evidence-based medicine circa 1985 – the Interpretant. For a model of this Peircean medical sign, see Figure 2.
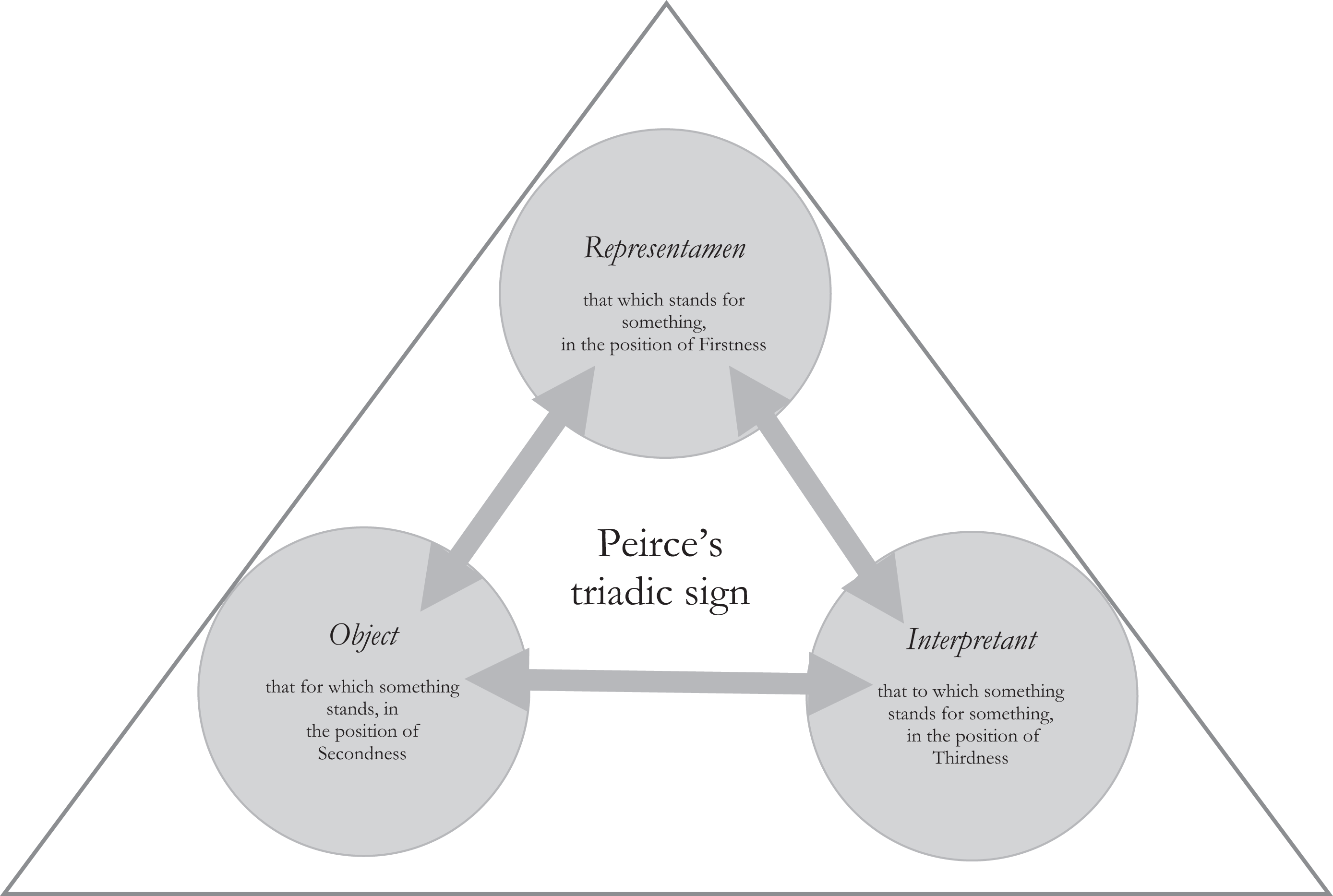
The indivisible tripartite structure of the Peircean sign.
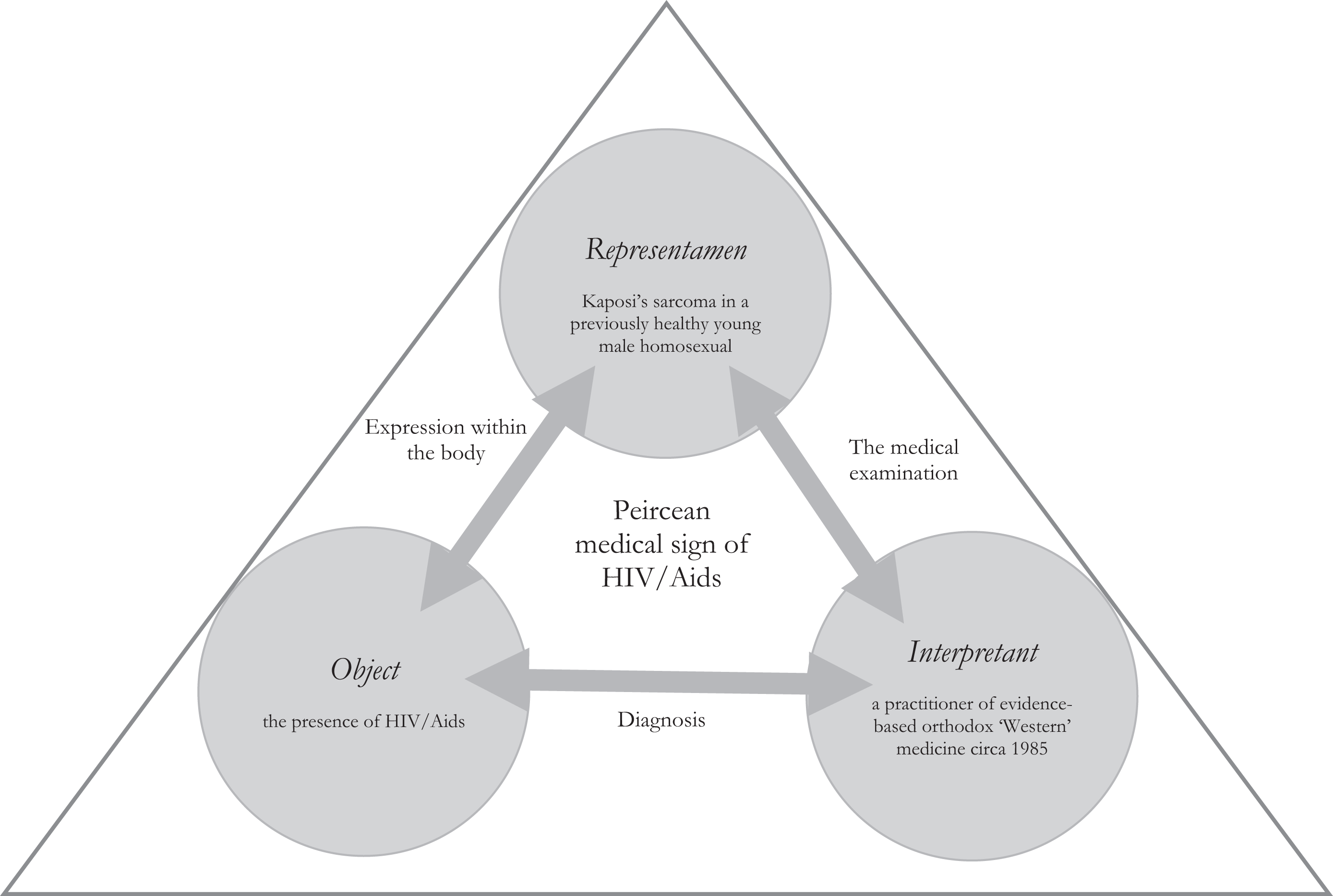
The dynamic structure of HIV/Aids as a Peircean medical sign. Of course, this is just one of very many different medical signs of HIV/Aids that could be formed, some complementing, some competing.
Peirce produced varying typologies of signs, but this paper will use only the simplest triad, his ‘second trichotomy’ (Peirce, 1955c: 102): the iconic, the indexical, and the symbolic. In the iconic sign, the relationship between the Representamen and the Object is one of resemblance: for example, a diagrammatic rendering of a flame to represent a fire, which indicates the Object through analogy. In the indexical sign, the relationship between the Representamen and the Object is one of physical contact: for example, the smoke from a fire, which indicates the Object through a material gesture. In the symbolic sign, the relationship between the Representamen and the Object is one of cultural meaning: for example, when referring to a fire with the letters ‘f i r e’, which indicates the Object through a mutually agreed convention.
The argument of this article will be made by applying Peircean rules of reasoning by abduction, and in doing so will also function as an explicative exploration of abduction’s explanatory and predictive potential in relation to medical diagnoses. In the first section, the ‘surprising fact’ of C will be defined and reformulated into an ordering question. Although this question will be expressed mathematically, maths is used in a way comparable to how Mary Morgan – in her contribution to this special issue (Morgan, 2020) – employs rhetorical permutations and combinations of the syntax of, as well as the connotations and denotations of, p in Forrester’s (2017a) initial proposal: if p, then what. The objective of this paper is to open up Forrester’s formula for reasoning with cases to greater theorisation, specifically addressing how the case, as a generic type for recognising other cases, is dialectically constructed in tension with individual instances of that case. In particular, this argument expresses a deep dissatisfaction with Forrester’s use and characterisation of induction and deduction, and especially, through his counterpointing of Aristotle with Mill’s critique, the implicit yet unavoidable reduction of reasoning to a balancing calibration between countervailing yet complementary inductive and deductive manoeuvres. In the second section, this paper will examine a genealogy of influence extending from Peirce (in critical response to Mill and Aristotle himself) to Forrester’s paper, via Richard Cabot and Thomas Kuhn, who feature so prominently within it. Delineating this genealogy will serve to make the argument that the vital third form of reasoning – abduction – has been excised from these formulations of reasoning with cases, and stands as a palpable absence in Forrester’s outline of how reasoning with cases might work. In the third section, the errors resultant from reasoning with cases without an appreciation of the role of abduction will be illustrated though an examination of the construction and description of HIV/Aids through early case reports.
Peircean abduction will be framed as the rupture constitutive of Kuhn’s ‘exemplar’, and powering what Forrester summarises as ‘the discontinuous character of science, of its revolutionary mode of transformation, and of the ubiquity of crisis rather than rational debate in such transformations’ (Forrester, 2017b: 47). After laying out the theoretical, semiotic groundwork to justify critically re-theorising Forrester’s thinking in cases in such a way, the argument will proceed to demonstrate the practical potential of applying such a reworked method of case-based reasoning to a specific new ‘exemplar’: the appearance, identification, and classification of HIV/Aids during the 1980s. It is precisely this normalising of the surprising, of the inserting into a meaningful time-bound semiotic of medical diagnoses, that constitutes the core value of reasoning with cases. It is worth adding that Rachel Ankeny (2011: 266) – discussed in more detail by Morgan (2020) – identifies ‘the surprise’ as the essential motivating fact behind the publication of the case study, in an analysis based partly on an examination of the identification and medical description of HIV/Aids through an accumulation of cases.
In terms of working with Forrester, the single most significant contribution this semiotic re-theorising has to offer is its correction of a linearity in the development of the case (any case) as Forrester conceives it; a linearity signifying more the chronological bias of historiographic modes of thought than the nature of the case itself. Adding Peircean abduction to this theory of the case disrupts any simple lineage. The abductive leap of faith (a phrase used both later in this argument and by Morgan elsewhere in this collection) is necessarily a leap in time also. In working only with the post-abductive altered timeline of the case, and in treating this as an ever-steady, ever-simple line of progression, Forrester ignores the dialogic, dynamic reverberations along the chain of a case series. These disruptive reverberations are the essential component in their temporary and contingent alignment into what appears, from a certain junctural perspective, to be a thing that can be called a case. Whereas Forrester presents a fixed firmament, reintroducing Peircean abduction into his model of thinking with cases allows for a Copernican revolution to set the semiotic stars spinning.
The surprising fact, C, is observed
Let p be an almost infinitely small number – that is, a decimal point, an almost infinite number of zeros, and then a five-digit series. Let this infinitely small probability represent a never-before-recorded medical case. Indeed, functioning as a Representamen in the triadic sign of Peirce (1955c), the probability both represents and describes the case; the probability of the case, expressed as a number ratio, is a mathematical sign of the case. Kuhn (1977: 299) makes an analogous distinction between the symbolic generalisation in pure mathematics and the symbolic generalisation in the sciences; in the latter, ‘they are not so much generalisations as generalisation-sketches, schematic forms whose detailed symbolic expression varies from one application to the next’. Beyond wholly abstract mathematics, then, the symbolic generalisation is not a universal constant, but rather is a description of a way of practically applying some (quasi-)rules, rules that by definition must be contingent (as in variously applicable, or applicable with non-trivially varying results). So, p therefore has a threefold relationship to the case of which it is a sign: iconic, as a predictive description (the probability of occurrence) that resembles the case’s rarity; indexical, as a material consequence (in the form of the string of digits comprising p) resulting from the case; symbolic, as an exemplar for the ways of thinking about p and its future series of occurrences.
To schematically formalise that series, given that the probability of that first case is p, then the probability of further cases – or instances (or icons, as the resemblance constitutive of a series of cases is a Peircean iconic relationship) of the same case qua syndrome – follows as p n (where n = number of cases). 2 Footnoted caveats aside, what is important is that p exists as an ‘Occurrence, a slice of the universe’ (Peirce, in Rosenthal, 1994: 5). And, as Peirce observes in these terms, it is from such an ‘Occurrence’ that fact(s) through the application of thought can be mined. What is telling about Peirce’s language here is that the particularity of the ‘Occurrence’ is conceptually inseparable from the generality of ‘the universe’. The rhetoric of the ‘slice’ problematises Forrester’s posited relationship between induction and deduction as packing and unpacking specific instances into a governing universality; the slice both destroys and constitutes the whole.
The surprising fact, C, mentioned in the abductive syllogism above, can be extracted from this particular slice of the universe. Mathematically prior to p
1 is p
0. Whereas p
1 = p, p
0 = 1, as any number to the power of zero equals one. This probability ratio (p
0 = 1) is the closest probability offers to certainty. As Peirce observes, this ‘1’ presents an extreme of knowledge in relation to the particular hypothesis: There are two conceivable certainties with reference to any hypothesis, the certainty of its truth and the certainty of its falsity. The numbers one and zero are appropriated, in this calculus, to marking these extremes of knowledge. (Peirce, 1955d: 157)
So, in the real world, what is first identified is a case series in which the early instances of the disease p (appearing as a run of p 1… p n-x) are conceived as some other condition(s), represented by the series l … m. This was famously the case with HIV/Aids, where early cases were seen as variant examples of other diseases, such as Kaposi’s sarcoma. Only as the series passes some recognition point (p n-x) does (l … m)n become recognised (and re-cognised) as earlier cases within the same series (p 1… p n-x) to create the coherent series of p 1… p n. This point of recognition most likely comes after the moment at which the new disease entity, formulated as that certainty of p 0 = 1, is identified. What happens often is a new name emerges and reclaims the misnamed prior cases, and the idea of an initiatory outlier case (p 1) as a tangible, readable text proves irretrievably lost in the disease prehistory. Furthermore, the disease hypothesis (p 0) would have already been present in some provisional form to provide unity to the series p n-x … p n (prior to the incorporation of the earlier misdiagnosed or misread cases of p 1… p n-x). Obviously, p 0 must be in dialectic with the adjusting series of p, bringing new cases in and responding to reflect this changing definitional set. It is important to note that as p 0 comes increasingly into focus, p 1 vanishes like the horizon. The truth is no paradigm-breaking case is ever really seen, or seen to be such.
In Kuhn’s (2012) account, the series constitutes a body of shared examples that mutually reify and, in conjunction with a dialectically responsive disciplinary matrix, constitute a new scientific paradigm. The series is the conduit for the analogous reasoning from problem to problem. But it is important to note that the exemplars, unidentified as such at that moment, provide the evidence for the new paradigm of which they are exemplars. In the case of the medical case, then, cases emerge as cases before there is a described disease of which they are a case. It is absolutely impossible to approach any disease without thinking through them as cases first. Similarly, and this is the novel observation produced by the mathematical formula, cases (p n-x… p n) emerge before the originary case p, and the dynamic, fluctuating p 0 – which has structural fixity as p 0 = 1 but ranges in terms of the p value – embodies the specificities of the case series p, whilst all the individual cases (especially in the earlier formulations of p 0 = 1) offer vague, generalised approximations at the indistinct hypothesis.
Here in full is C, the surprising fact observed: for any paradigm-breaking revolutionary medical case of extreme unlikeliness there is a hypothesis with a probability ratio of absolute certainty, and this hypothesis exists as a mutable but tangible specific, whereas the paradigm-breaking case is vague, invisible, and unverifiable. The empirical particular (p) is a metaphysical and absent generality, whereas the hypothetical universal appears as a solid presence. So, whilst thinking in cases might make one presented with p 1 ask, Then what?, it ought contra Forrester to provoke the question, If p 1, then p 0 = 1, so what? Crudely, Forrester is exactly wrong: cases are not real-world specifics for precise analogic reasoning. The ‘surprising fact’ of C is that cases, and certainly the case exemplar p, are lost, and are only the foggy particles, the primordial soup, from which sudden, crystallised hypotheses can rise up – sudden but temporary; transitorily solid.
But if A were true, C would be a matter of course
So, given that, this section now needs to recover the set of circumstances and evidence (A) that make the C observed and described in the previous section not a ‘surprising’ jolt but a ‘matter of course’. This is vital. If A can be established to make C a matter of course, then the proposed revision to Forrester and this Peircean abductive method of working with cases will stand, and from there bolder moves towards a medical semiotic can be taken.
Resolving C and outlining A requires: first, a tracing of Peircean semiotics as ‘tacit knowledge’ or ‘knowledge embedded in [the] shared examples’ of Kuhn’s reasoning from cases and Forrester’s thinking in cases (Kuhn, 2012: 191); second, a demonstrative and productive account and application of Peirce’s model of abductive reasoning (hypothesising) and its relation to inductive data (cases), as well as formulations of probability in relation to hypotheses; and third, some hints to the practical deductive value of C for working with medical cases. These three elements comprise A, in the three Peircean modes of Firstness, Secondness, and Thirdness, and specifically and respectively as aesthetics, ethics, and logic, the ‘three normative sciences’ detailed in Peirce’s Harvard Lectures of 1903 (CP 5.36). 3 Peirce does not use aesthetics, ethics, and logic esoterically: aesthetics is what is admirable, ethics is what is right, and logic is deliberate, controlled thought. The material or ideals come from aesthetics. Ethics forms principles based on these aesthetic ideals. Logic is thought according to these ethical principles. In A, aesthetics relates to the presence and object form of the posited Peircean-Kuhnian-Forresterean ‘knowledge’, and will here require only some verification of its contours and content, beyond the traces already made. Ethics relates to the (re)action this form can exert on secondary objects, in this case, the medical case report. Logic is the final (though provisional) truth or otherwise of the entire relation, and for Peirce it should comprise future-orientated propositions of real-world utility, of ‘reasoning how things really and truly are’ (Peirce, 1955b: 18). For all the intricacies of the argument here, the end goal is this real-world utility. The specific medical cases worked with in the following sections demonstrate viscerally how thinking better with cases, and thinking with Peircean abduction and a medical semiotic framework, could make the difference in what are literally matters of life and death.
First, the aesthetic question: can the fact of Peirce be extracted from the Occurrence of Forrester’s paper? There is no direct documentary evidence that Forrester ever read Peirce. There is, though, much to suggest that Forrester wrote in the wake of Peirce. He writes both of and under his influence, sub rosa. It is not solely an intellectual debt, transferred through Kuhn; thinking in cases, as detailed by Forrester, is an exemplar of the paradigm of scientific thought woven throughout Peirce’s writing. (Forrester is p n to Peirce’s p 0.) It seems unlikely, but not impossible, that Forrester did not engage with Peirce directly when preparing his 1996 paper. The first quoted text in the paper is Ian Hacking’s The Taming of Chance (Forrester, 2017a: 2), and Forrester also makes passing reference to Carlo Ginzburg’s comparison of Sherlock Holmes’ detective method and medical diagnosis (ibid.: 14). The Taming of Chance (Hacking, 1990) concludes with a chapter devoted to Peirce; Peirce features in the title of the collection of essays from which Ginzburg’s paper (Ginzburg, 1983) is taken.
Of course, this is not an historical argument but an aesthetic one, and looks for traces suggestive of an influence, rather than documentary evidence of a verifiable connection. But nor is this an exercise in fanciful citational play. Hacking’s styles of reasoning – to which Forrester wishes to add his seventh type, ‘reasoning in cases’ (Forrester, 2017a: 2) – are already strongly informed by Peircean modes of reasoning. It is therefore of great value to do some necessary post hoc Peircean reasoning about this proposed seventh style of reasoning, to refine it and to ensure and validate its inclusion alongside these other a priori Peircean styles. It is particularly important to address the loss of abduction as a necessary element of a tripartite reasoning structure, alongside induction and deduction; a loss that occurs somewhere between Peirce and Forrester. The abductive leap already taken that Peirce influenced Forrester has been (partially) justified through inductive testing for the presence of potential moments of contact. This unarticulated influence needs to be brought out into the light and reasoned through, to understand not just the role that Peircean thought has already had in formulating Forrester’s proposed seventh style of reasoning, but also how by putting this style of reasoning back into dialogue with its Peircean antecedents, an abductive temporal leap can be taken to restructure Forrester’s under-theorised model of the case, and his by implication under-theorised mode of reasoning in cases, and can bring abductive reasoning actively into Forrester’s thinking with cases.
Consider the history. Peirce, already in his lifetime a ghostly precariat researcher avant la lettre, plays Banquo at the feast of thinkers in cases, in the genealogy presented by Forrester. Peirce was a close friend of Oliver Wendell Holmes Jr and Josiah Royce; both wrote letters in support of Peirce’s (rejected) funding application to the Carnegie Institution in 1902 (Peirce, 1997: 5). Ella Lyman was a student of Royce’s at Radcliffe College from 1887 to 1891, and their productive working friendship was to last until Royce’s death in 1916. At the same time as attending Royce’s lectures, Lyman began a ‘vibrant intellectual dialogue’ (Kaag, 2008: 136) with Harvard professor of medicine Richard Cabot (so vibrant, they later married). 4 Peirce’s exclusion from Harvard coincided with the appointment of Charles William Eliot – who ‘encouraged’ case-based teaching (Forrester, 2017b: 54) – as president of the university in 1869, and the subsequent appointment in the following year of Christopher Columbus Langdell as dean of Harvard Law School. Peirce had lectured in logic at Harvard in 1868 and 1869, but Eliot, with personal animus towards Peirce, blocked his proposed course in 1871 (Bergman, 2012), and Peirce would not return to Harvard until William James arranged for him to give a series of lectures on pragmatism, held in a private house rather than on the campus from which he was ‘banned’ (Menand, 2002: 232). These Harvard lectures provide one of the last and most comprehensive formalisations of the Peircean scientific method of thought, including his final-stage formulation of abduction as a creative methodology, a ‘first phase of inquiry with which ideas are generated’ (Paavola, 2005: 132). It is from the seventh of these lectures that the famous abductive syllogism structuring this paper is taken. As this quick historical tracing shows, Peirce was part of the intellectual milieu from which Forrester’s genealogy of case-based reasoning is drawn, and intersected with its key protagonists, without appearing explicitly in Forrester’s account. Biographically, Peirce echoes through Forrester’s history of thinking in cases. Is it any surprise if his semiotics reverberates too?
Kuhn’s relationship with Peirce has been explicitly articulated in the literature. Some argue for continuity between the two: see Rosenthal (1994) or Jacobs (2006), who traces Peirce’s influence, through Royce, in Kuhn’s conceptualisation of the scientific community.
5
Others see opposition, specifically over whether the course of scientific knowledge proceeds by cohering Pericean continuity, revealing a transhistorical narrative of progress, or by discontinuous Kuhnian revolutions, exhibiting an incommensurability across epochs and disciplinary matrices that smacks of nominalism to the Peircean (Haack, 1992; Skagestad, 1979). Consider Kuhn’s (2012) account of puzzle-solving within normal science, which he characterises as a finite set of easily exhausted ‘mopping-up operations’ (ibid.: 24) directed at three limited ‘foci’ (ibid.: 25): the paradigm’s foundational facts; theoretically relatable additional facts; a set of empirical procedures in support of these facts. Here, ‘the most striking feature of normal science research problems…is how little they aim to produce major novelties, conceptual or phenomenal’ (ibid.: 35). This description mirrors the helpless see-sawing between induction and deduction Peirce believes would endure without the creative potency of abduction, as he explains in his Harvard lectures: Abduction is the process of forming an explanatory hypothesis, It is the only logical operation which introduces any new idea; for induction does nothing but determine a value, and deduction merely evolves the necessary consequences of a pure hypothesis. (CP 5.171) When one’s purpose lies in the line of novelty, invention, generalization, theory – in a word, improvement of the situation – by the side of which happiness appears a shabby old dud – instinct and the rule of thumb manifestly cease to be applicable. (CP 2.178)
There is then an analogous relation of incomplete resemblance between these three theories of reasoning with cases, in the sense of the Peircean definition that ‘Analogy is the inference that a not very large collection of objects which agree in various respects may very likely agree in another respect’ (CP 1.69). The fact that ‘On Kuhn’s Case: Psychoanalysis and the Paradigm’ could be very easily rewritten to demonstrate the implicit (not unconscious; unconscious to whom?) guiding presence of Peircean semiotics is actually sufficient proof both that it should and that it need not be. That Kuhn’s innovation in the philosophy of science appears psychoanalytic to the Freudian and semiotic to the Peircean accords with the Peircean understanding of quasi-objective objects of knowledge and truth as dialectically self-constructing with the collective subjectivities’ ways of ‘grasping’ (CP 5.182). 6
Tracing Peirce through Kuhn and Forrester challenges the Aristotelean opposition between ‘the universal and…practical wisdom’ (Forrester, 2017a: 4). Whether the thinker in cases employs the phronesis applied to recognise the ‘particular figure’ of the triangle in Aristotle’s account (ibid.: 5) or that applied within Eleanor Rosch’s prototype theory, they recapitulate this opposition. However, the particular figure of the triangle cannot be recognised in the practical case in question; the case of the figure before the perceiving individual will be an approximation of the triangle only, exhibiting some but not all of the generic features. The moment of phronesis, the thinking with the case, will be analogous to the hypothetical p 0, because whatever is present as raw percept (or, in the medical encounter, the physical presence of the patient, the welter of laboratory data) is redacted into a perceptual judgement that gains its specifics and particulars from analogy with p 0 as an accumulation of genre conventions. As a result, recognition is an active act of ascribing features both ways across the equation between the perception or case in hand, and the case qua syndrome (or triangle) that makes sense of that recognition. In this analogous exchange, it must be that p 0 or the supposed universal is functionally the same as the case or specific instance or percept. Against Forrester’s understanding, it might be said that every act of phronesis is actually an invocation of an absent particular and the erasure of a present, but intangible, vagueness. Such an invocation is inherent to the triadic sign described earlier and, in its indivisibility, argues against any simple separation of universals and particulars.
In place of Rosch’s ‘generators or prototypes’ offered by Forrester (2017a: 9), Lev Vygotsky’s chain complex, informed by Soviet semiotic thinking, should be favoured as a model for the cognitive psychology of thinking with cases. Instead of positing remarkable (and commonly shared and static) originary qualities – as Rosch’s theory requires – the chain complex is a relational network, which alters dynamically as new ‘concrete objects’ are united within the complex (Vygotsky, 1986: 127). A child using generalisations rather than concrete examples is not evidence of ‘an early mastery of abstract thinking’ (ibid.: 143), as the opposition between specific cases and tyrannical rules presented by Forrester might suggest. Rather, the specific is general in the experience of the child. In the face of the new disease, the clinician (and medical science by extension) is in the position of the child. And this is similarly how genres (literary, medical, or any other) build too: from specifics as the general. The symbolic generalisation sketch already given of the relationship between p 0 = 1, p 1, and the series p 1… p n describes the formation of a genre: a series of exemplars is observed first (p n-x… p n); secondly, the genre form is abducted (p 0 = 1); thirdly, earlier exemplars are incorporated into the series, modelled against the genre form (p 0) to create the genre canon of p 1… p n. This structure can easily be tested against case studies of literary genres.
To place Forrester’s use of Wittgenstein’s account of the standard metre in Paris into this account of the relationship between the abducted hypothesis qua medical diagnosis, it becomes apparent that Wittgenstein’s language games can be read as a translation of the Peircean probability formula. Once any standard length is established – necessarily from a series of real-life incidences of measurement (p 1… p n) – then p 0 is revealed as having always been there, not only in an Ideal form but in an actual, real form. (This would not be true only if the length exceeded the limits of the spatial dimensions of reality, but then it would not have been possible to observe in series p 1… p n.) When the general rule, or p 0, is seen so evidently as being a product of the series of particulars, or p 1… p n, then to talk of ‘the tyranny of the universal, the tyranny of the rule’ (Forrester, 2017a: 9) sounds almost paranoid. This is not sophistry. Cases have generalised features, and generalised patterns of creating meaning. They have shared, general routes of dissemination and modes of application.
These traces allow finally for the construction of a Peircean triad for the method of thinking in cases (P). Forrester offers only a dyadic analogous reasoning: an inductive/deductive see-sawing between generalised, woolly, and tyrannical universals and specific, real-world particulars, and an attempt to draw meaningful inferences from comparisons between cases on the basis of (sometimes only supposed or even fabricated) similarities. Articulating the Peircean triad now and reapplying it to reasoning with cases amounts to a reintroduction of the vital creative component of abduction that has slipped from Forrester’s genealogy. The value of P as a Peircean triadic method for thinking in cases will be demonstrated inductively in the next section, but this section will conclude with its explication. P: in Firstness, the perceptual judgement or case or perceived triangle as Representamen; in Secondness, the percept or patient or raw data as Object; in Thirdness, the hypothesis or disease entity or so-called Ideal triangle, as Interpretant. So much for aesthetics.
Hence, there is reason to suspect that A is true
Now that A is established as an abductive hypothesis to explain the surprising fact of C, this can be inductively tested against some actual cases (and the product of thinking in these cases). In this inductive experiment, C will be the surprising fact of an epidemic of unusually fatal cases of various illnesses (most infamously Kaposi’s sarcoma) amongst gay Americans at the start of the 1980s. To maintain a direct link with the Peircean-infused Harvard method of case-based reasoning, the inductive analysis will draw upon cases published in the New England Journal of Medicine (NEJM). This journal is used here for its long-standing reputation as the pre-eminent publisher of medical case reports, and as home to the series of case studies established by Cabot and described by Forrester (2017a: 17). Cabot himself is a suitable exemplar for the ambivalence of the man of phronesis. Certainly, he was a rigorous advocate for and architect of a materialist, empirical, and systematised thinking with cases, transporting this methodology from Harvard Law School to the teaching hospital. Simultaneously, Cabot was also a man of pronounced religiosity, with all the metaphysics and universalising this implies. In his works, this arch medical thinker in cases repeatedly attributes medical efficacy to the supreme universal, God, who overwrites His supernatural power onto ‘nature’ or medicine or humanity, and by implication all the Case Records of Massachusetts General: ‘so instead of “vis medicatrix naturae” we should say “vis medicatrix Dei”’ (Cabot, 1937: 835; see also Cabot, 1909: 146). It need hardly be said that this much metaphysical transcendence, such establishment of meaning through the imposition of an ineffable, unanalysable guarantor, such inversion to offer as the foundation for a material, reasoned science of inductive analogies a supernatural, celestial fiat, rather troubles the intellectual framework of thinking with cases here. Can it be philosophically possible (let alone consistent) to reason from particular instances when men are numbered like dust against a boundless Thirdness?
The NEJM’s thinking in cases about the p 0 = 1 that would become HIV/Aids begins breathlessly in medias res. In the wake of the Centers for Disease Control’s (CDC) pronouncements of 1981 – themselves a response to case reports accumulating in New York and San Francisco – the medical community finds itself already within a proliferating series p n-x … p n, and in search of establishing p 1… p n-x and p 0. It is a nice historical quirk that in the mythology of HIV/Aids, the abductive originary case is already the zero case; the letter O attached to an index case resident ‘outside’ California – the area of an early CDC study into HIV/Aids – was misread as the digit zero (McKay, 2014). The genre demands of epidemic exemplars made the so-called ‘Patient Zero’ a stigmatised, sociopathic villain of contagion, as a Typhoid Mary of the gay bathhouses.
It is hard not to find a NEJM editorial’s excitement at the ‘tantalizing questions raised by this new syndrome’ (Durack, 1981: 1467) distasteful, though this certainly demonstrates the anomalous, paradigm-breaking rupture the syndrome already represented. Perhaps even more distasteful, routes of investigation endorsed by the CDC establish the locus of disease in the lives of the cases presented: Case-control studies to single out possible risk factors, such as promiscuous life styles and nitrite inhalation are underway. Patients are being HLA-typed…in a search for a possible genetic predisposition. Examination or re-examination of the immunosuppressive potential of recreational drugs has begun. (ibid.)
Early abductive attempts are quickly apparent from the case studies. In an assessment of 11 atypical cases of pneumocystis carinii pneumonia, the theoretical tail wags the empirical dog visibly (Masur et al., 1981). The abductive explanation is that this is a ‘community-acquired’ (ibid.: 1431) outbreak, yet the paper has to actively create the community in question. When the paper notes that ‘all 11 men were drug abusers or homosexuals or both’ (ibid.), the scientific mind might object that only those who were both represent a meaningful community. When it parses the ‘community’ further, only two are both drug users and homosexual, and the drugs abused range across heroin (four of the patients), methadone (one), alcohol (one), and cocaine (one); it is surely permitted to Whiggishly note that if drug abuse and homosexuality had been disaggregated and the researchers had worked with two different ‘communities’ (intravenous drug users and homosexual men), they would have struck closer to the truth of this outbreak. By the time the paper remarks that ‘all patients were residents of New York City who had no social or occupation contacts with one another’ (ibid.: 1433), the supposed community has clearly evaporated. The paper then reincorporates this fictive community (as the disease’s aetiological agent) into its own experiment, inserting its own conclusions into the premises, through its definition and selection of the control: ‘(matched for age, but not for sex or race) who were not known to be drug addicts or homosexuals and who were not taking medications’ (ibid.: 1432). To be clear, the only serious problem here in terms of scientific method is the ‘or’ that creates a fictitious community to suit p 0’s genre demands. In Peircean terms, there is the right kind of wrong hypothesis – the just wrong – and the wrong kind, which is unscientific and pernicious in bending facts to its theory. This failure to use abduction and this violation of the facts constitute an ethical problem. For Peirce, ethics entails self-critical reflection on a practice of conduct with the aim of modifying and correcting any bad habits. This is triply wrong, in fact: wrong in its results, wrong as a practice, and wrong as no self-reflection has taken place. To abuse facts to fit a wrong theory is an ethical failure. In the case of HIV/Aids, this meant earlier, more painful deaths for people with the disease for many years.
Consider the correspondence provoked by Case 11-1982 in the NEJM. Clinicians wrote in with cases related to heterosexual men. As homosexuality has, through the cases presented (or through the cases as presented), become part of the differential diagnosis for the new syndrome, the clinical response is to challenge the validity of the raw data as a case; the act of constructing the case drives (unsuccessfully) to recreate its genre generalities over the particular person presenting. The correspondence states: He had a 14-year history of addiction to cocaine and intravenous heroin, but he denied using amyl nitrate. On repeated questioning he denied having any homosexual partners. The sexual history was confirmed by independent discussion with several of the patient’s friends. (Gold, Thomas, and Garrett, 1982: 498)
Thinking only in cases, or too greatly in cases, or with too strict adherence to the specific genre conventions of a case series, can foreclose any creative abduction. This can be demonstrated by examination of a potential case within the series p
1… p
n-x excluded from the p case series through the dictates of a then current formulation of p
0. When the case report dismisses a potential diagnosis of what was then cytomegalovirus (CMV) infection with Kaposi’s sarcoma, and would now be HIV/Aids, because the young male presenting is not (or does not admit to being) homosexual, it is evident that the case has, through the strength of genre, hardened from a collection of particulars into an un(der)theorised generalisation. This weak induction – that only homosexuals can have this novel immunodeficiency – is, whilst superficially more grounded in the empirical facts and reality of the cases, actually further from the epidemiological truth of HIV/Aids, which would require some abductive leaps of faith to reach. Forrester’s reasoning in cases without employing abduction necessarily refuses a movement from case to broader theory and back, through refinement, to further cases (in this instance, of non-homosexual men with HIV/Aids) and then back again (or on again) to a better abduction; this is exactly the kind of reasoning that would be structurally unavoidable if the Peircean triad P were used rather than the dyadic analogous reasoning from case to case. What is particularly remarkable in this case is the acknowledgement within the very same paragraph that an elderly woman (who was presumably not also a young homosexual man) had a similar clinical presentation to this supposedly exclusively gay male disease: If this young man was homosexual a consideration would be Kaposi’s sarcoma, one of the unusual diseases, including Pneumocystis carinii infection, that have been described in homosexuals.…There is a lymphadenopathic form that may be associated with few skin lesions and occurs in younger patients, and this form of the disease has been found in homosexuals.…This link to CMV may be important since infection with this agent is very common in the homosexual population.…In addition, we have seen a 68-year-old woman with the nephrotic syndrome due to membranous nephropathy who six months later was found to have a vaginal lesion that on biopsy proved to [sic] Kaposi’s sarcoma. (Scully, Mark, and McNeely, 1983: 891) On the contrary, he entertains hypotheses which are almost wildly incredible, and treats them with respect for the time being. Why does he do this? Simply because any scientific proposition whatever is always liable to be refuted and dropped at short notice. A hypothesis is something which looks as if it might be true and were true, and which is capable of verification or refutation by comparison with facts. The best hypothesis, in the sense of the one most recommending itself to the inquirer, is the one which can be the most readily refuted if it is false. This far outweighs the trifling merit of being likely. For after all, what is a likely hypothesis? It is one which falls in with our preconceived ideas. But these may be wrong. Their errors are just what the scientific man is out gunning for more particularly. (CP 1.120) (original emphasis)
Space precludes further analysis, but for any wedded to the specificities of the case contrasted to the vague generalities of the hypothesis, a quick look at any NEJM case reports of possible HIV/Aids prior to the isolation of HIV (Barre-Sinoussi et al., 1983) in particular demonstrates how the investigation and reasoning move from poorly read presenting symptoms and through inductive fits of tests and examinations before hitting upon an abductive collapse, with the text imploding in the final paragraphs under the accumulated weight of numerous diagnoses, peppered with question marks (for a perfect exemplar, see Scully, Mark, and McNeely, 1982). Most often, the patient himself has quietly vanished off to die sometime between the drawing of his blood and the diagnosticians’ stroking of their chins. So much for the ethics of recognising the case in its singularity.
If p, then p 0 = 1, so what?
The shortcomings of these weak inductions of analogous reasoning between cases spring from a tendency to reduce the case to a quasi-unit, and to imagine calculations are being performed, when in fact they are estimations. In the cases examined, this occurs on the micro and macro levels. The macro level is simple quantification: a certain proportion (y) of p has a certain feature (z), and therefore identify z clinically to establish with a certainty of y:p that this is a case of p. Within the case, qualities are overtly quantified. Male homosexuality, for example, is reduced to a unit that is either present or absent; again, the specific case is seen to be structured by the genre traditions (the macro-level quantification). The narrative is predetermined by these ratios of units, but the case report’s claim to qualitative narrative belies this generalising predetermination inherent in the inductive process. This is a very important problem with Forrester’s thinking. In taking these cases as rich qualitative narratives dealing with specifics, he has ignored how the form and content of these case reports – not just in their formal composition for publication, but even in the process of thinking them through when experienced by clinicians – are bounded in their possibilities and already structured in their range of exploration, innovation, and insight by the genre conditions within which they have been constructed. Again, this is equally true whether the clinician or researcher is moulding material for a published paper or whether they are only mentally transforming (and internally narrativising and rewriting) the raw perceptual data of an encounter with a patient or research participants into a medical case for their own grasping of it.
By contrast, the self-consciously partial nature of abductory induction does not blind it to its limitations and to its reliance on instinct and guesswork: So long as the class sampled consists of units, and the ratio in question is a ratio between counts of occurrences, induction is a comparatively simple affair. But suppose we wish to test the hypothesis that a man is a Catholic priest, that is, has all the characters that are common to Catholic priests and peculiar to them. Now characters are not units, nor do they consist of units, nor can they be counted, in such a sense that one count is right and every other wrong. Characters have to be estimated according to their significance. The consequence is that there will be a certain element of guess-work in such an induction; so that I call it an abductory induction. (Peirce, 1955a: 152)
To return to the triangle introduced by Forrester, or the unrealisable Platonic Ideal triangle, it is possible to discern a process not at odds with Peirce’s account of abduction. Deleuze – a 20th-century Stoicist philosopher who often deployed semiotic and structuralist modes of thought to explore and reconfigure experiences of disease and the clinic – argues that in relation to the images generated from the Ideal: Plato divides the domain of the image-idols in two: on the one hand the iconic copies (likenesses), on the other the phantasmatic simulacra (semblances).…The Platonic motive…is a matter of choosing claimants, of distinguishing the good from the false copies, or even more, the always well-founded copies from the simulacra, ever corrupted by dissemblance. (Deleuze, 1983: 48)
This is too much mathematics and too little medicine. And ‘mathematics is only busied about purely hypothetical questions’ (CP 1.53; emphasis in original). In terms of logic, abduction clearly provides an account of the progressive development of knowledge of p – in a way that a circular reasoning through cases only logically could not. It is certainly theoretically true that case studies can be read as ‘exemplary knowledge…viewed and heard in the context of another’s experience – another’s horizon…but used in the context of one’s own…interpretable only in the context of one’s own experience – in the context, in other words, of one’s phronesis, rather than theory’ (Thomas, 2010: 578). But this stumbles on an obvious pragmatic point. What possible use could there be for knowledge ‘interpretable only in the context of one’s own experience’ (emphasis added)? This is phronesis idiosyncratic to the point of solipsism. It is Hamlet as king of infinite space, bound in a nutshell. (The bad dreams are presumably all the rest of reality that has no interest in dancing to the solipsist’s tune.) Leaving aside whether anyone has experience so unique and so absolutely self-referential and context-free, so hermetically sealed off from all others, there is the more important question of how the result of the individual’s rumination (surely not free of the generalising influences of a network of shared contexts and overlapping and dynamically interacting intersubjective experiences) could possibly exist and not contribute socially and intersubjectively to a generalising abduction. Theory, like shit, happens. In the genre of medical case reports, and the practice within medicine of thinking in cases, the individual’s phronesis is caught in the established genre conventions of the case (both the general conventions of case reports and the specific medico-literary conventions of the particular case series). As a case becomes a case, a myriad other contexts, encapsulated through other cases into genre conventions, mould the new exemplary knowledge, setting its boundaries of possibilities. Similarly, this case leaves the two genres altered (perhaps infinitesimally).
It is vital to understand the culturally inflected genre construction of any disease and the cases (published or merely ‘written’ through intersubjective clinical encounters) that dialectically mutually construct. Forrester’s thinking in cases has pointed the way, but by losing sight of abduction as the only means of thinking beyond the dominant paradigm, and by fundamentally missing the ‘already genre’ nature of any case used within dialogic case reasoning, and the restrictions this imposes on the potential for creative, correct hypothesising, his approach is caught in a cul-de-sac. This paper offers a refinement currently absent from the literature, by bringing a semiotic expression of the problem (inductive analogic reasoning from case to case is a closed circuit incapable of addressing a paradigm-breaking event such as a new disease) and a complementary semiotic, in the form of the reintroduction of abductive hypothesising. This involves a semiotically informed reappraisal of the status and the nature of the case, as construct and building block of medical knowledge. The case is not an impartial Object in its perfect particulars. Rather, it is a Representamen and a generalisation from specifics. It is not the particular or the singular, but the singular overlaid with and translated by the universal principles for understanding these singularities. 9 These universal principles in turn must obviously abductively and dialectically evolve in response to the assimilated singularities. To revert to Kuhnian terms, the exemplar and the disciplinary matrix are both indivisible components of the paradigm. Only through this syllogism of abduction could Forrester’s proposed seventh style of reasoning, thinking in cases, be generalised out to have practical utility, a function of the disciplinary matrix and not the shared exemplars. p 0 = 1 serves as a reminder that there is no thinking out cases; thought renders the case and the case encapsulates its rendering thoughts for communication. It also states clearly that the specific and particular, in the form of medical cases, are – counter to superficial consideration – mutable, vague, contestable, and generalised; conversely, the theory to which these particular cases point is singular, practical, inevitable, and (for a time) truthful. So much for logic.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Notes
This article was developed partly from research done with Professor Brian Hurwitz, King’s College London, and would not have been possible without his support and guidance. We intend to publish further on the genre of the medical case report.