
Abstract
Research innovations and breakthroughs are increasingly realised through collaborative networks amongst state and non-state actors. This article investigates the utilisation of such networks in the field of applied health services research, where policy narratives repeatedly emphasise the importance of collaboration between university researchers, clinical and health service leaders, patient representatives and industry. The translation of policy into practice suggests that these networks are not always designed and managed in line with policy aspirations. Taking a decentred approach, the study reported in this article examines how local policy actors translate national policies for collaborative health research networks in the context of their own histories of applied research, including local narratives and priorities for health research. The study shows that local actors face key dilemmas and opportunities for situated agency, as they experience three competing policy narratives, first, for carrying out world-class research; second, for ensuring research meets local needs and third, for developing new understanding about the implementation of research into practice. Although these expectations might appear coherent to policy-makers, at the regional level, they provide the basis for disagreement and negotiation amongst local policy actors through which the local narrative of collaborative research is framed to regional stakeholders. The study shows how the tensions between elite and local narratives can be reconciled through re-framing activities, especially the articulation of ‘parallel frames’ within a ‘cascade framing’ process.
Introduction
Research policies increasingly see technological innovations and research breakthroughs as realised through the formation of collaborative networks between state and non-state actors; commonly described as a ‘triple-helix’ between industry, universities and government (Bozeman, 2000; Etzkowitz and Leydesdorff, 2000; Gibbons, 1994; Powell et al., 1996). Such collaborations are exemplified in bio-medical, clinical and health services research where government funders, university academics, bio-tech industries and service providers work together to develop, trial and implement evidence-based therapies and interventions. A major factor in the promotion of collaborative research networks is the recognition that evidence-based interventions do not easily ‘translate’ into frontline care, with reports describing time-lags of up to 15 years (Grimshaw et al., 2012). In some cases, delays ensure the safety of new therapies, but where they become too long and systemic, there is potential for wasted investment and prolonged delivery of sub-optimal care. Such time-lags have been interpreted as ‘translation gaps’ between the discovery of basic science and its application (T1) in product testing, and then between proven interventions being implemented (T2) into routine practice (Cooksey, 2006). The networked model of health research aims to close these gaps by building closer links between knowledge producers and service users in the co-production of evidence-based interventions.
In the UK, a variety of networked research infrastructure has been established to close the translation gaps in health research, such as Biomedical Research Centres (BRCs) and Academic Health Science Networks (AHSNs). In this article, we examine the introduction of Collaborations for Leadership in Applied Health Research and Care (CLAHRCs) as regional multi-agency research networks. In 2008, nine ‘pilot’ CLAHRCs were introduced across England to bring together university researchers, NHS leaders and other public stakeholders to undertake ‘applied health research’ (T2), i.e. research that can directly impact on the way services are organised and delivered. A ‘second wave’ of 13 CLAHRCs was introduced in 2014, which provide the focus for our study. These initiatives received in excess of £200 m public research funding, with ‘match funding’ from NHS, industry and university partners. Although questions remain about their contributions to frontline services (Kislov et al., 2018), further funding was announced in late 2018 for a similar ‘translational’ research programme.
Research shows the formation of early CLAHRCs was shaped by how different healthcare and research leaders translated national policy in the context of local historical contingencies and competing local priorities (Caldwell and Mays, 2012; Lockett et al., 2014; Rycroft-Malone et al., 2013). Building on these ideas, our study looks closer at how local actors resolve the dilemmas of reconciling three (often competing) policy narratives, first, to carry out world-class research; second, to ensure research meets local needs; and third, to develop new understanding about the implementation of research into practice. Although this collaborative agenda might appear coherent to ‘elite’ national policy-makers, at the regional level, it provides the basis for disagreement and negotiation amongst university researchers and service providers and commissioners.
Just as health services research communities have come to realise that the translation and implementation of evidence into practice is often complicated, the interpretative policy literature shows how national public policies are rarely, if ever, neatly implemented into local service organisation and delivery (Yanow, 1996). Rather, they are subject to on-going re-interpretation and modification as they are translated and enacted in different arenas (Lipsky, 1968). To explore how health research policies are translated and implemented, we take a ‘decentred’ approach, as developed by Bevir and colleagues (Bevir, 2011; Bevir and Richards, 2009). The decentred approach attends to the ways governance arrangements are realised through, and are contingent upon, the interactions and meaningful practices of policy actors. These meaningful practices are guided by actors’ beliefs and customs that are rooted in different ‘traditions’. At the same time, these practices are the source of novel governance arrangement as actors confront ‘dilemmas’ when interpreting and enacting policies, for example where existing meanings and beliefs are contradictory or perceived as irreconcilable.
The decentred approach pays particular attention to the role of narratives in both informing, and unsettling, meaningful practice (Bevir, 2011). Narratives are understood as relatively coherent stories of problem-definition and problem-resolution that reflect prevailing systems of meaning and belief (Fischer, 2010). From the decentred perspective, narratives are both a source of tradition, i.e. stories about how services have worked, and a source of dilemma, i.e. when new policy narratives attempt to reshape local practices. In the context of such dilemmas, localised governance arrangements are formed as policy actors seek to reconcile competing or contradictory narratives through their meaningful practices. The decentred approach attends, in particular, to the ways ‘elite’ policy narratives, i.e. those constructed by political elites and policy-makers are received, filtered and negotiated through the meaningful practices of local policy actors operating in the context of their local traditions and narratives.
Taking a decentred approach, our article examines the tensions between (and within) ‘elite’ and ‘local’ policy narratives for applied health research, and how these tensions represent dilemmas around which meaningful practices translate, negotiate and enact policy into practice. Later within our article, we turn to the literature on ‘framing’ to develop our analysis of how policy actors, at different levels, seek to reconcile the dilemmas posed by divergent policy narratives. A ‘frame’ can be defined as a cognitive-cultural filter through which social actors perceive, organise and make sense of their experiences in the context of their interactions (Goffman, 1974). Within social movement and policy studies, ‘framing’ relates to the way actors interpret and communicate a policy issue, especially when seeking to influence how others will interpret and respond to it (Snow and Benford, 1992). In this respect, social actors can use ‘narratives’ or appeals to ‘tradition’ to both interpret and shape how people make sense of policies (Czarniawska, 2004; Fairhurst and Sarr, 1996). Although some subsume narratives within framing processes, Olsen suggests (2014) ‘frames’ and ‘narratives’ offer distinct but complementary insights, which we see as enriching a decentred approach. From a decentred perspective, narratives represent relatively broad discursive formations that articulate particular governing rationalities (Bevir, 2011), whereas framing focuses more on the interactive dimensions through which actors interpret and communicate policies in their meaningful practices. As such, we operationalise framing theory to analyse the meaningful practices of social actors as they confront and translate divergent policy narratives.
Drawing on a historical review of recent health research policy in the UK, the article first sets the context of the changing health research landscape and the emergence of a dominant ‘elite’ policy narrative for applied health research. It then develops a decentred analysis of the meaningful practice of translating policy in one regional context, drawing on documentary, observational and interview data collected over five years. Invoking the framing literature, we show how elite policy narrative becomes disturbed, transformed and mutated as it works its way through the health research landscape as a form of ‘cascading framing’. We suggest, in particular, that ‘parallel frames’ can emerge that reflect the different interpretations of policy and the localised agendas of stakeholders.
Collaborations for applied health research and care: Policy narrative
Throughout much of the 20th century, research priorities in the UK were based on the ‘Haldane’ principle; namely, that decisions about funding should be guided by the research community, not politicians. In the early 1970s, the Rothschild Report recommended that research should more directly contribute to policy-making and, since that time, the politicisation of research policy has continued with the alignment of funding to national economic and political priorities (Parker, 2016). In the health research context, this has seen government departments, quasi-governmental agencies and arms-length research council, coming together to prioritise and fund a broad portfolio of ‘bio-medical’ and ‘clinical’ research for the discovery, testing and implementation of new therapeutic interventions, as well as ‘health services’ research concerned with analysing and evaluating new modes of service organisation and delivery. It is increasingly the case that such funding is shaped by the expectation that health research should make a meaningful and substantial contribution to political and economic priorities.
In 2004, for instance, the UK Treasury called for health research to have greater economic impact through fostering partnerships between industry and clinical research teams (HM Treasury, 2004). Similarly, the Department of Health report Best Research for Best Health (DoH, 2006) recommended collaboration between industry, universities and NHS organisations to address national economic and health priorities. This included recommendations for streamlined research governance and funding through a National Institute for Health Research (NIHR). The combined aspirations for ‘health and wealth’ have carried through into a succession of policies that have shaped the national policy narrative for collaborative research activities, including CLAHRCs. For example, following the decision to ring-fence health research funding through agencies such as the NIHR, the UK Treasury commissioned the ‘Cooksey Report’ (Cooksey, 2006) to consider future funding options. This report is significant for highlighting the ‘first’ and ‘second’ translational ‘gaps’ in the research ‘pipeline’, as well as an apparent bias towards blue-sky ‘discovery’. It suggested ‘the UK is at risk of failing to reap the full economic, health and social benefits that the UK’s public investment in health research should generate’ (Cooksey, 2006: 1). Highlighting the achievements of international research institutions, such as the Canadian Institute of Health Research (CIHR), the report called for enhanced national leadership for ‘applied’ and ‘translational’ research based on collaborative partnerships between research and clinical communities. That is, collaborative research that determines how interventions, shown to be effective in trial conditions, can be implemented in ‘real-world’ healthcare settings.
The collaborative (and economic) agenda was developed in the report of the The High-Level Group on Clinical Effectiveness (Tooke, 2006). This brought attention to the different rates at which evidence-based interventions were implemented into routine practice, and again called for more applied and translational research, emphasising community-wide research collaborations between clinicians and academic researchers and the translation of evidence into practice (Tooke, 2006). The report was careful to define ‘applied research’ as having practical application for patient benefit, with the proviso that patient gain should be realised within three to four years.
It was within this context that the national policy narrative for translational health research was crafted. Significant was the framing of a particular problem related to the translation of biomedical and clinical research into frontline patient care because of a disjointed research landscape where academic research was decoupled from clinical practice (and industry). The narrative also raised concerns about the culture of established research models, which appeared to be dominated by ‘blue-sky’ university research, rather than ‘applied’ research. Although the CLAHRC narrative is ostensibly concerned with the ‘second’ translational gap, the underpinning policy narrative reflects wider political imperatives. First, there is a strong economic agenda centred on the wasted resources associated with implementation delays and the lost potential for wealth creation from developing new therapies with industry. Second, the policy narrative claimed the UK was falling behind other OECD countries and hence should emulate the successes of these world-leaders in introducing translational research networks (notwithstanding a lack of evidence). Third, there was an aspiration to transform the culture of the NHS with an emphasis on creating a research-led service in which both staff and patients participated in research.
In October 2007, the NIHR called for proposals to establish research collaborations that would ‘forge a mutually beneficial, forward-looking partnership between a University and the surrounding NHS organisations, focused on improving patient outcomes through the conduct and application of applied health research’. The first CLAHRCs were framed as ‘pilots’ and then ‘experiments’, suggesting that policy-makers were uncertain how these networks should ‘close the gap’ between research and practice (Rowley et al., 2012). The call required a single NHS organisation to lead the collaboration, with the quality of the application assessed on the track record of ‘applied research’ with university partners. A significant feature was the expectation for CLAHRCs to secure ‘match-funding’ from NHS, academic and industry partners to the equivalent value of NIHR funding. As well as designating ‘clinical’ research themes, reflecting local and national priorities, it was expected that at least one theme would deal with the science of ‘implementation’; that is, understanding how evidence can be more effectively translated into practice. In 2008, nine ‘pilot’ CLAHRCs were established each with up to £10 m funding for five years.
Reflecting the narrative that the initial wave of CLAHRCs were ‘experiments’, the NIHR commissioned a programme of formative evaluations to review how the different collaborations were formed and to appraise their relative success in closing the second translation gap (Walshe and Davies, 2013). The findings of these evaluations (summarised below) informed the ‘second call’ for CLAHRCs issued in August 2013. On this occasion, the NIHR announced that £124 million would be allocated for 13 new CLAHRCs. As with the first call, the collaborations needed to ‘close the second translation gap’, but there was more explicit focus on national clinical priorities for dementia, long-term conditions and public health; and that research should be generalisable to the wider NHS, not only local service needs. It was also clear that the new CLAHRCs would be tailored to the changing NHS landscape following the Health and Social Care Act (2012), including more focus on industry partnerships. The new CLAHRCs were intended to: Develop and conduct applied health research relevant across the NHS and to translate research findings into improved outcomes for patients. Create a distributed model for applied health research that links those who conduct applied health research with all those who use it in practice. Create and embed approaches to research and its dissemination that are specifically designed to take account of the way that health care is delivered across the local AHSN. Increase the country’s capacity to conduct high-quality applied health research focused on the needs of patients, and targeted at chronic disease and public health interventions. Improve patient outcomes locally and across the NHS. Contribute to the country’s growth by working with the life sciences industry.
Of relevance to our article, there were important changes in the policy narrative for second-wave CLAHRCs. The first related to the need for alignment with a changing regional infrastructure, specifically AHSNs, that were introduced to accelerate the spread and scale-up of evidence-based innovations. Second, there was more explicit emphasis on the importance of collaborating with industry and demonstrating a contribution to economic growth: ‘NIHR CLAHRCs will facilitate improved outcomes for patients and the NHS, and also contribute to the country’s economic growth by working with the life sciences industry’ (p.3). Third, there was a drive towards building ‘a critical mass’ of people engaged in applied health research, with stronger emphasis on the track record of ‘world class’ research teams. This involved, for example, numerical measures of research quality in terms of academic outputs, grant capture and PhD completions, which in many ways reinforced traditional university research, rather than translational or applied research. Fourth, NIHR funding was reserved primarily for ‘applied research’, with the expectation that match-funding would be allocated for the ‘implementation’ of evidence into practice, which could be seen as re-introducing a separation between research and implementation.
The language of policy reveals various meanings of what health research ‘is’ reflecting different ‘scientific’ or ‘disciplinary’ traditions, i.e. ‘bio-medical’, ‘clinical’ ‘applied’ and ‘translational’ research. In one regard, the policy narrative for both first- and second-wave CLAHRCs emphasises the importance of ‘applied’ and ‘translational’ research, i.e. implementing and testing interventions in real-world settings that are already evidence based. Yet, in other ways, assessments of research capacity and quality are based on more traditional ‘bio-medical’ or ‘clinical’ lines. And at the same time, political interests continue to promote the importance of economic benefits and working with industry. It might be argued, therefore, that a coalition of ‘elite’ political, industry and scientific interests shaped both the wider health research policy landscape and the particular CLAHRC agenda. Yet, the heterogeneity and incoherence between these perspectives could also be seen as creating dilemmas or opportunities for subsequent policy translation where local actors interpret the different elements of the policy narrative according to their pre-existing frames or traditions.
Collaborations in context: Research commentary
In their analysis of changing health research policy, Walshe and Davies (2013) describe CLAHRCs as creating a research infrastructure to meet the strategic needs for innovation within the NHS. Research on the first-wave CLAHRCs offers important insight into the translation of policy. Of note, Caldwell and Mays (2012) analyse the translation of policy from expert reports, through national policy-makers, to one regional CLAHRC team. Their review suggests that there was a broad degree of alignment amongst national policy-makers and local CLAHRC leaders in the aspirations for translational health research.
In contrast, comparative case study research shows that CLAHRCs have translated policies along different lines according to regional priorities and the influence of clinical and service leaders. Rycroft-Malone et al. (2013) describe how differences in stakeholder engagement, funding and formal governance arrangements shaped the strategies for collaboration. Significantly, the local history of university/NHS collaborations pre-conditioned CLAHRC formation, while differences in power, especially between clinical and academic groups, impacted the potential for collaboration (Currie et al., 2013).
Similarly, Lockett et al. (2014) delineate five ‘archetypes’ of the different relationships between research and practice. For example, the ‘modular’ archetype describes a separation of research and implementation activities that work in connected, but distinct domains; another describes CLAHRCs as ‘collaborating through loose networks’ derived from pre-existing research partnerships between universities and healthcare organisation, whilst another sees CLAHRCs as characterised by ‘centrally controlled service improvement projects’ with a high-level core team monitoring local project teams embedded in service settings. More significantly, however, Lockett et al. suggest that policy translation was shaped by prevailing ‘field’ conditions, especially the influence of local leaders in framing the opportunities for applied research: with ‘clinical’ leaders adopting a more service-facing approach, ‘clinical-academic’ leaders favouring more traditional models of (trial) research, and ‘social science’ academics favouring implementation strategies. They argue that ‘who’ defines the problem locks in the resulting solution, or model of collaboration (Currie et al., 2013).
In their recent review, Kislov et al. (2018) further argue that the local context (and history) of relationships between NHS and research communities shapes the regional organisation of CLAHRCs. Building on this view, our article develops a decentred analysis of the way national or ‘elite’ CLAHRC policies are translated into local context, focusing on the influence of history, dilemma and meaningful practice in the selective translation, (re-) framing and enactment of policy. Narratives are treated as reasoned stories that are formed in the context of particular histories, traditions and interests that affect the meanings, behaviours and identities of social actors (Fischer, 2010; Shuman, 2012; Yanow, 2007). They are also sites for conflict, as divergent traditions and meanings compete to shape social practices, and the dilemmas created by this conflict creates opportunities for novel forms of meaningful practice (Bevir, 2011). For instance, elite policy narratives articulated by state actors reflect particular historical interests and agendas that are not always consistent in themselves or consistent with those of non-state actors. How local actors interpret and translate elite narratives in the context of their own histories creates both dilemmas and opportunities for meaningful agency, potentially re-making the local and resisting the elite.
In the context of health research, the prevailing elite policy narrative is composed of multiple and, at times, competing scientific, political and economic imperatives that might represent ambiguities and inconsistencies to local actors; this includes, for example, the perpetual quest to provide high-quality services with in the constraints of limited fiscal resources. Rather than focusing on the social position and influence of CLARHC leaders (Lockett et al., 2014), our analysis focuses more broadly on how coalitions of local actors work through their divergent interpretations and negotiate the translation of policy in the context of local histories. In particular, it explores how local narratives not only reflect (and resist) some of the expectations of national policy but also represent divergent views, expectations and agendas, which find expression in the ambiguities and dilemmas created by policy and in the interactive practices of local actors.
As outlined above, our analysis focuses on the ways both national and local policy narratives (as expressions of tradition and meaning) are articulated, enacted and resisted through the framing activities of different policy actors and resources (Fairhurst and Sarr, 1996). In particular, our study considers how policy actors, at different stages of policy translation, framed and re-framed the policy narrative in the process of negotiated and mediating divergent interests.
Study methods
We initially developed a genealogy of health research policy in the UK from the late 20th century to the present, which forms the basis of the background section of this article. We regard policy documents, reports and other announcements as inherently discursive in that they reflect and articulate particular political ideologies, modernist assumptions and are constitutive of relations of power (Fischer, 2010; Foucault, 1984; Gale, 2001; Yanow, 1996). In practical terms, this involved identification, collation and critical interpretation of reports, policy documents and policy evaluations, and the underpinning source materials and evidence. Following Yanow (1996), these were subject to a relatively structured narrative analysis to delineate the key historical moments and turning-points, the underlying assumptions, motives and interests at play, the symbolic meanings and metaphors and the prescriptive elements of policy.
We also carried out in-depth qualitative research with local policy actors involved in the formulation and implementation of one ‘second-wave’ CLAHRC, with the aim of understanding the local translation and enactment of policy. Given resource constraints, only one CLAHRC could be researched over a four-year period with data collection commencing in the preliminary stages of CLAHRC formation and continuing until past the mid-point of the funded activity. The CLAHRC was interesting because of its specific historical circumstances, which were identified as a ‘dilemma-potential’ in the translation of policy; namely, the CLAHRC was formed from the merger of two ‘pilot’ CLAHRCs, each with different leadership arrangements, regional demographic priorities and histories of research collaboration. As such, it was a relatively unique case (Stake, 1995) for investigating how different histories within a region can shape assumptions about applied and translational research, the interpretation of policy and the creation of a new regional narrative.
The qualitative research involved non-participant observations and semi-structured interviews. Over a period of nearly four years, observations were undertaken of CLAHRC governance and executive meetings, research theme management groups, project meetings and public engagement activities. In excess of 200 hours of observations were undertaken, with data recorded in hand written field journals. The observations revealed the interactive processes and negotiations through which the CLAHRC was formulated and operationalised, ‘zooming in’ on key issues and dilemmas faced by local actors. As part of the observations a large number of in situ, ethnographic interviews were undertaken to explore and clarify observed events. In addition, semi-structured interviews were conducted with 20 individuals, including senior CLAHRC executives (6), administrators (3), theme leaders (4), and project team leads and members (7). The interviews elicited participants’ personal experiences and interpretations of the CLAHRC ‘story’ with a focus on how different actors translated and negotiated policy aspirations in the context of local histories.
Summary observation records and interview transcripts were subject to interpretative narrative analysis (Yanow, 1996) that focused on how participants reflected on the ‘story’ of the CLARHC, including the history of the two preceding collaborations, the processes of bid development and the new arrangements for research governance and project management. In examining these narratives, we analysed how these stories revealed common and divergent meanings, beliefs and interests. In practical terms, interview transcripts were subject to close reading and coding by two authors, identifying key events and issues, around which common and distinct ‘stories’ and prevailing ‘scripts’ were crafted. These were then discussed and debated with the wider study team with the goal of developing a critical interpretation of policy translation.
The local experience of CLAHRC
Regional legacy and parity
In the months before the formal NIHR funding call was announced, senior research leaders within the region began to mobilise local collaborators in anticipation of a future CLAHRC bid. In the absence of policy detail, local actors were uncertain about the expected size and scope of the new collaboration, especially the anticipated research priorities and their relationship with the changed NHS infrastructure. A major issue was whether the two existing ‘pilot’ CLAHRCs would be permitted to continue independently, whether they should submit competing bids, or whether a combined application should be proposed. As such, multiple groups mobilised around these options in advance of ‘the call’. The eventual invitation to apply required proposed collaborations to align with the regional ‘footprint’ of the relatively new AHSNs, thereby requiring the submission of a combined regional bid.
Through a series of preliminary ‘behind the scenes’ discussions, brokered by the managing director of the AHSN, with representatives from major hospitals and university research leaders, it was decided a single application was the most appropriate path. Quickly within this process, research leaders crafted a collective narrative of a ‘mature’ CLAHRC (rather than ‘new’) that built on the ‘track record’ of the existing ‘pilots’ to offer an unprecedented model of synergy and collaboration. As such, a ‘master frame’ started to emerge that played on both the national and regional narrative of ‘collaboration’ and helped to galvanise and coordinate subsequent local action. For some, however, this was more of an ‘arranged marriage’ with complex geo-political considerations and long-term ramifications for CLAHRC governance. We knew we had to be collaborative because we didn’t have the scale in [City A] or in [City B] or in [Town A] to do it all ourselves. And that’s the idea of it you know, CLAHRC stands for Collaboration. (NHS Partner) When the call came out it turned out there would be one CLAHRC per AHSN area and therefore a very hasty marriage was convened…. And we had a number of meetings over several months then to basically put together a joint CLAHRC to bid. (Academic Project Lead) …the main thing was to convince the funders that we had an organisation that was capable of meeting the brief. So, there was a fusion of the old [CLAHRC A] and the old [CLAHRC B]. And there was the selection of people with a good enough H-index to be able to be seen to lead work streams. I’m sure that’s why… I got involved, mainly because I had the numbers, rather than I was necessarily all that appropriate. (Research Theme Lead)
The emerging narrative, or master frame, of the ‘mature’ CLAHRC was therefore shaped in the context of multiple competing agendas, including the need to show national funders that the ‘new’ CLAHRC was building on a proven track record of applied health research; the need to ensure geo-political fairness to regional partners who were providing financial resources to the collaboration; and also the need to ensure the engagement of local researchers and service providers. As described below, there remained tensions around what types of ‘applied’ research the CLAHRC would undertake and what role regional partners would have in shaping this work.
Determining research priorities
Early within the process of drafting the CLAHRC proposal, regional research leaders commenced a consultation exercise with local NHS commissioners, care providers, universities and industry partners to determine the future research priorities. This reflected the policy expectation for research to address local service needs and to demonstrate both engagement with and commitment from regional actors, especially in the form of ‘match-funding’. The key priorities identified included: dealing with complex conditions, integrated care, access to care, inequalities/prevention, patient safety and public health. Part of the requirement was that participating organisations, both NHS and academic, need to bring in an equal amount of funding to that that was passed over from NIHR….that added up to several million pounds…but in doing that I guess it’s to a greater or lesser extent the collaborating organisations felt they had some ownership of the CLAHRC. (University Research Manager) So, the legacy projects carried forward into the new CLAHRC. And there were various criteria that we used for example to select what sort of new projects would make a good CLAHRC project. And were stakeholders on boards? Did you have a strong implementation plan? Does it align to a pre-identified health need or priority? (Research Manager) In an idealised world, the CLAHRC is a unique vehicle for bringing together a whole range of different people who want to make a difference in making healthcare better through actually researching … doing research on interventions, on practices, on procedures, on anything that can make healthcare better. And it’s almost like a hook or a nexus point and it brings all these people together and they should work in this kind of dynamic mode two way of kind of interdisciplinary problem-solving. (Research Theme Lead)
Mobilising the new network
In concert with bid development, the regional leadership team commenced merging pre-existing CLAHRC governance and administrative arrangements so they would ‘hit the ground running’ if funded. it allowed the two CLAHRCs to unfreeze and so … because they’d both been running for five years, they’ve both developed systems and structures that they thought were right…We spent a lot of time telling our funders how good we were but you know, we might have some things we were doing that probably weren’t working as well. (NHS Partner) I’ve done quite a lot of mergers and they can be quite difficult. I said we needed an integration plan for the CLAHRC, which built on the strengths of both CLAHRCs, that’s actually in the prospectus. And produces something else that’s a step up. An integration plan actually looks at the two entities before they integrate and what the new entity is, that’s about organisational development and communications, keeping the good people, moving on one or two people who haven’t quite performed. (NHS Manager) We did have a slightly torrid time in the beginning because we worked very, very differently. [CLAHRC A] had done a lot of work one set of priorities. So, we’ve taken some of the projects forward. [CLAHRC B] had done quite a lot on other issues and also in terms of the implementation strategy it was very strong. So, we’ve capitalised on that you know. (Research Theme Lead) Well it’s interesting and the CLAHRC works very well. We probably have the best partnerships of all the AHSN-CLAHRCs in the country. And this is historically because they understood CLAHRCs. (Research Theme Lead) First of all we shouldn’t be doing implementation, NIHR were clear about it. We should not be doing implementation. AHSN are the people to do the implementation. Having said that, we do help to facilitate implementation, so we get the product ready for implementation. We don’t implement ourselves. We do have this disconnect that you know, we’re trying to do implementation but NIHR doesn’t pay for implementation at all. We are supposed to do world-class research and then work with our partners to get that implemented and disseminated. (Research Theme Lead)
For some, the narrative that ‘researchers don’t implement’ became a prominent sub-frame within the CLAHRC, reflecting the different research cultures that persisted across the region. ‘Because I’ve always said this: researchers don’t implement, that’s not their skillset, and I think to expect researchers to come in to CLAHRC, take a two-year contract, do some funding to do a piece of research, then implement as well, it’s very unrealistic.’ (Network Manager)
Discussion
Our study examines how the ‘elite’ CLAHRC narrative, as articulated by national policy-makers and manifest in official reports, was interpreted by regional actors in the context of their local histories and narratives of applied health research, and how the interplay between these elite and local narratives presented both dilemmas and opportunities for meaningful practices in the translation of policy into practice. In developing our analysis, and offering a more relational view of 'narratives-in-practice' we draw upon the 'framing' concept as used, for example, within the field of social movement research. Specifically, we use the framing concept to understand how policy actors (re-)frame the translation of policy into practice occurs through a succession of framing and re-framing activities through the communicative and interactive practices of policy actors. In other words, we suggest that it is through the interactive practice of framing that policy and local narratives are brought together, translated and re-made.
As outlined above, the national policy narrative brought together multiple competing imperatives (i.e. world-class research, local health benefit, economic benefit) in what might be seen as a ‘master frame’ (Snow and Benford, 1992) of ‘collaboration’ that set the broad parameters for how ‘local’ policy actors were expected to make sense of and enact national policy. We found, for example, that the broad narrative of ‘collaboration’ (along with ‘maturity’) was operationalised by regional policy actors both in their ‘upwards’ relationship with national funders and their ‘downwards’ (or lateral) relationships with local policy actors. However, as this master frame permeated through the regional research landscape, it was re-interpreted in the context of pre-existing frames and also re-framed as policy actors, operating at different levels, negotiated the rationality and meaning of collaboration in the context of their diverse traditions (i.e. regional NHS and university leaders, CLAHRC senior leadership and project teams). Although the master frame of collaboration might appear coherent, it was refracted and split into multiple ‘parallel frames’ that seemed simultaneously consistent with the overarching frame, while also allowing for the divergent interpretations of local stakeholders according to their own traditions.
Elaborating this idea, we interpret the implementation of national policy into local contexts as a form ‘cascade’ framing, whereby the policy ‘master frame’ sets the broader direction of change (or ‘flow’), but where the meaningful practices of local actors repeatedly transform or divert elements of this frame in the context of their local traditions, resulting in the formation of parallel ‘local action frames’ (or ‘streams’). These parallel local frames flow in the same broad direction of policy implementation through adhering, in part, to the overarching master frame whilst also enabling groups of actors to mobilise in parallel ways according to their local customs (see Figure 1).
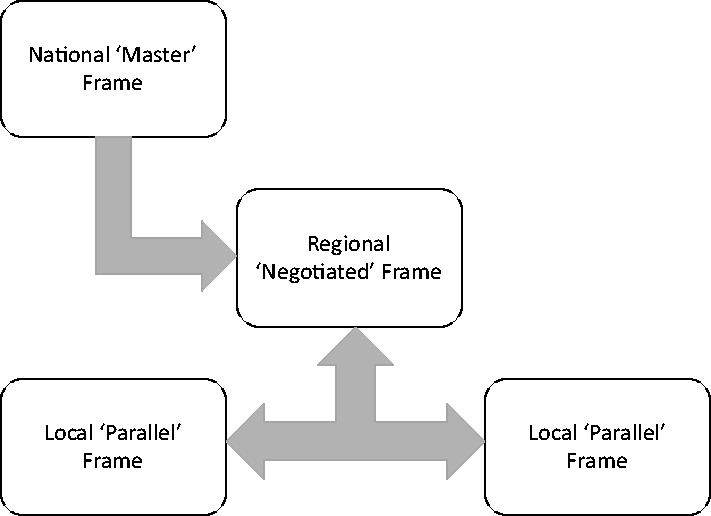
Illustration of cascade and parallel framing.
An important finding from our study was the apparent lack of clarity in the national ‘master frame’ which allowed for subsequent parallel re-framing at regional and local levels. The high-level narrative was unclear in at least three areas. Firstly, there was ambiguity about whether CLAHRCs should be concerned with undertaking world-class research (which often equates to large trials) or applied research that focuses on making a difference to local service providers. Secondly, there was a lack of clarity about whether research should address national priorities for health improvement and economic growth, or the local service priorities and health needs. Thirdly, there ambiguity about whether translation and implementation activities are something that occur independent of, and often at the end of the research process, or rather whether implementation should be integrated into the co-production of research. As such, internal contradictions and inconsistencies in the elite narrative, as framed within policy, created the dilemmas around which re-framing occurred (Kaplan, 2008).
Some commentators suggest that CLAHRCs can reconcile these tensions through a coherent narrative in which they undertake world-class research that simultaneously addresses national and local priorities, and where this research is developed and implemented in a variety of local contexts (Caldwell and Mays, 2012). Our study suggests, however, that these tensions were not always easy to reconcile, and that evident variations in how CLAHRCs have evolved across the country (Rycroft-Malone et al., 2013) might be explained by how policy actors working at different levels interpret and reconcile these tensions. In our study, this was manifest through the persistence of parallel frames at the regional and local levels that continued to drive local practices in different directions, but which offered a coherent, albeit unstable, overriding narrative to satisfy the expectations of national elites. Despite the potential for these parallel frames to disrupt the national mobilisation of CLAHRCS, regional leaders were successful in weaving together the national and local narratives to iteratively create a modified regional frame that would allow local ‘parallel frames’ to co-exist whilst still meeting national expectations. The blending of these parallel frames was evidenced through the creation of the ‘integration and knowledge management plan’.
Although the idea of cascade framing might lead to a view of policy translation that implies a linearity in the ‘downward’ implementation of national policy objectives at the local level (Caldwell and Mays, 2012), our study shows that this is a recursive re-framing process, especially at the meso-regional level, where national policy imperatives and local parallel frames are continually mediated and aligned through creative re-framing. Looking beyond our case study, our article brings to light the need to look at how national and local narratives for research can be inconsistent in themselves and at odds with one another. Local narratives are influenced by distinct interpretive frames that reflect and create internal and external dilemmas around which different meanings and agendas become mobilised as sites or opportunities for crafting new governing arrangements. Although senior research leaders clearly have an influential role in shaping the resultant narrative (Lockett et al., 2014), what seems equally important is the interplay of meanings amongst multiple networked actors, such as university and NHS leaders and other research partners. More than this, however, are broader social, cultural and political imperatives, especially the need to be seen as fair in the distribution of roles and resources, and legitimate in terms of reflecting the best interests of local people and drawing on the best talents within the region. These issues extend the range of contextual factors previously shown to influence the formation of collaborative research networks (Rycroft-Malone et al., 2013). Looking outside of healthcare, the study also suggests that large-scale research infrastructure and programmes, in which the state is one of multiple actors, can be interpreted as sites in which divergent meanings about the purposes and processes of knowledge creation and application are contested, not only around different methodological traditions but also around the desired economic and commercial benefits of research to the state (and national economy) and to industry (and shareholders).
Finally, our article demonstrates how the framing perspective can enrich a decentred analysis of narratives (Bevir, 2011). The concept of frames brings to light the webs of belief or traditions through which actors interpret and enact policy developments, whilst framing also highlights the interactive and communicative practices of ‘narrative-in-practice’ through which policy actors seek to influence others around policy agenda (Benford and Snow, 2000; Snow et al., 1986). In one respect, therefore, attention to framing offers a lens for looking at the interplay between narratives and meaningful practice (Olsen, 2014), where narratives are both source of tradition and dilemmas. The framing literature highlights, for example, the role of ‘narratives’ or stories as rhetorical devices, whilst appeals to tradition and custom are also used to align actors to particular agenda (Fairhurst and Sarr, 1996; Snow et al., 1986). As such, we suggest that framing theory offers an important lens for understanding how meaningful practices experience, translate and enact policy narratives.
Footnotes
Authors' Note
Bridget Roe is now affiliated with University of Birmingham, Birmingham, UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.