
Abstract
Institutional arrangements used to steer public policies have increasingly become layered. Inspired by the literature on institutional layering and institutional work, this paper aims to make a contribution to our understanding of institutional layering. We do so by studying an interesting case of layering: the Dutch hospital sector. We focus on the actors responsible for the internal governance (Board of Directors and Supervisory Boards) and the external regulation (the Healthcare Inspectorate) of hospitals. In the paper, we explore the institutional work of these actors, more specifically how institutional work results from and is influenced by institutional layering and how this in turn influences the institutional makeup of both healthcare organizations and their institutional context. Our approach allowed us to see that layering changes the activities of actors in the public sector, can be used to strengthen one’s position but also presents actors with new struggles, which they in turn can try to overcome by relating and using the institutionally layered context. Layering and institutional work are therefore in continuous interaction. Combining institutional layering with a focus on the lived experiences of actors and their institutional work makes it possible to move into the layered arrangement and better understand its consequences.
Keywords
Introduction
Institutional contexts in the public sector have become increasingly complex as they are built on different institutional arrangements that exist at the same time. For example, the introduction of regulated markets and other New Public Management (NPM)-like interventions were not accompanied by the elimination of other institutional arrangements such as professional self-regulation and consensus building between stakeholders. Instead, these preexisting arrangements have become incorporated in and conditioned by regulated markets. Therefore, the introduction of regulated markets in Western European countries meant that increasingly complicated mixed arrangements to govern public policies were created (Streeck and Thelen, 2005), which public service providers have to relate to. In this paper, we explore what this means for actors working in these organizations, how they respond to these layered arrangements, and how they in turn influence this institutional context. For this exploration, we draw on the concepts of institutional layering and institutional work.
The concept of institutional layering has been introduced to better understand complex arrangements and how they came about (Mahoney and Thelen, 2010; Streeck and Thelen, 2005). Institutional layering is a type of institutional change in which new institutions are added on top of or alongside existing ones. Institutional layering does not mean that new arrangements simply overlie others but that arrangements interact with each other, which can lead to large and unpredictable transformations (Mahoney and Thelen, 2010; Streeck and Thelen, 2005). These transformations can have important consequences for actors working in such a layered arrangement. Much literature on layering describes the historical process of layering and focuses on its consequences on policies and the actions of actors at the macro level (e.g. Beland, 2007; Parker and Parenta, 2008; Thatcher and Coen, 2008). However, in this article we take a somewhat different focus. Instead of researching the process of layering, we take layered institutional environments as our starting point and explore the undertheorized issue of how actors working in organizations that have to relate to such an institutionally layered context engage with this context.
The literature on layering acknowledges the important role actors play as change agents who strategically wish to bring about institutional change (Hacker, 2004; Mahoney and Thelen, 2010; Scheingate, 2010). In this article, we extend this actor approach by introducing the concept of institutional work from the Organization Sciences. This literature took a similar actor-focused turn as its Public Administration counterpart, by focusing on the work of actors that actively shape institutions (Currie et al., 2012; Lawrence et al., 2011). However, institutional work does not only comprise the strategic use of the institutional context in order to bring about certain changes, as is the focus in Public Administration literature, but also the daily coping and keeping up with institutional structures (Lawrence et al., 2011). Such daily work, as is shown for example in literature on organizational routines, both works to sustain and change prevailing institutional structures (Feldman and Pentland, 2003). Using the concept of institutional work in our study on institutional layering allows us to better understand the dynamics caused by institutional layering.
The Dutch hospital sector is an interesting case of layering and is used in this paper as our case study (Van de Bovenkamp et al., 2014). We focus on the actors responsible for the internal governance (Board of Directors and Supervisory Boards) and the external regulation (the Healthcare Inspectorate) of Dutch hospitals. Increasingly, these actors were given responsibility for quality of care as a consequence of institutional layering. In the paper we focus on the institutional work of these actors, more specifically on how institutional work results from and is influenced by institutional layering and how this in turn influences the institutional makeup of both healthcare organizations and their institutional context. We answer the following research questions: How does institutional layering influence the institutional work of actors responsible for the internal governance and external regulation of quality of care of Dutch hospitals and how does this institutional work lead to institutional change both within and outside these organizations?
In the following, we first elaborate on the literature on institutional layering and institutional work. Then, we describe the institutionally layered context of Dutch healthcare quality governance and regulation and the methods used to study our case. Thereafter, we present the results in terms of how the actors responsible for the internal governance and external regulation respond and relate to institutional layering through institutional work. We conclude with a reflection on the added value of combining the concepts of institutional layering and institutional work.
Institutional layering and institutional work
Incremental change can count on growing attention of Public Administration scholars working in the field of institutional theory (Hacker, 2004; Mahoney and Thelen, 2010; Streeck and Thelen, 2005; Thelen, 2004; Van der Heijden, 2010). This strand of literature argues that institutions are not static and do not only change through exogenous shocks as punctuated equilibrium theory proposes, but incrementally change and evolve due to both exogenous and endogenous sources of change. Mahoney and Thelen (2010) identify four types of incremental change: displacement (the removal of existing institutions and the introduction of new ones), drift (the changed impact of existing institutions due to shifts in the environment), conversion (the changed enactment of existing institutions due to their strategic deployment), and layering (the introduction of new institutions on top of or alongside existing ones). It is the latter we focus on in this paper.
As the expanding literature that uses concepts drawn from the incremental change framework shows (e.g. Beland, 2007; Carboni, 2010; Horton, 2006; Parker and Parenta, 2008; Scheingate, 2010; Thatcher and Coen, 2008; Wallenburg et al., 2012), the framework provides us with language and tools to describe how and why a certain mode of change occurred. Aside from this, we argue that it can also provide insight into what this change means (Van der Heijden, 2010). It is this we focus on in this article; we argue that the concept of layering can be used to better understand policy reforms, the complex institutional arrangements they create, their consequences, and the way actors deal with these consequences. Therefore, in this article we do not focus on the process of layering but on how actors relate to a layered institutional arrangement. In order to do this, we first need to be clear about our use of the layering concept.
In his review on layering, Van der Heijden (2011) shows that the concept is used in terms of actors being added, in terms of instruments added, and in terms of adding both instruments and actors. In this paper, we follow this broader use by focusing on the layering of institutional arrangements. Institutional arrangements consist of both instruments and actors. Moreover, this broad approach allows for the recognition of the different institutional logics that can exist at the same time in a layered arrangement.
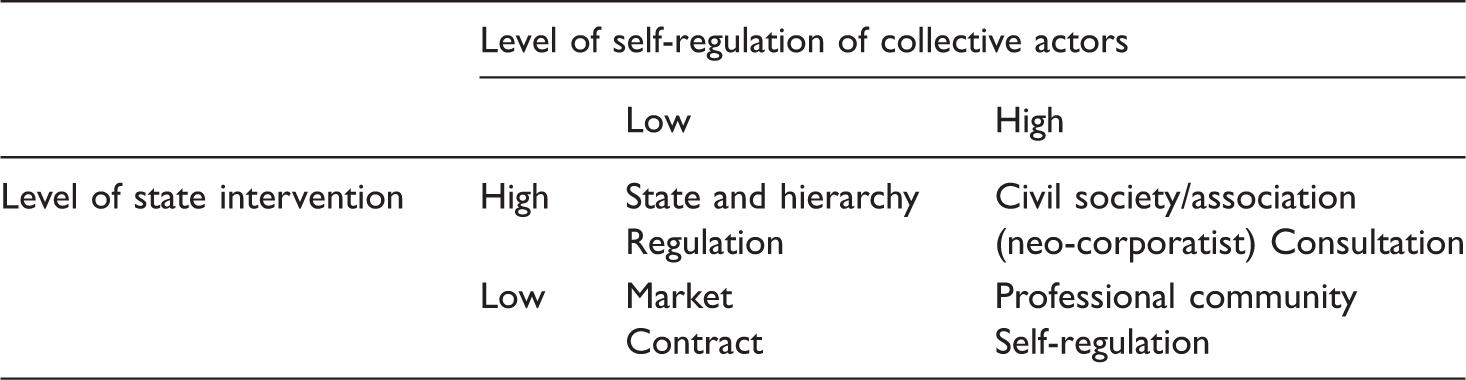
Ideal typical institutional arrangements (based on Bal (2008) and Helderman (2007))
An important feature of the incremental change literature is the active role attributed to actors who can influence institutional change (Hacker, 2004; Mahony and Thelen, 2010; Scheingate, 2010; Streeck and Thelen, 2005). Since rules allow room for interpretation, debate, and contestation, actors can operate strategically in their institutional environment, acting as change agents who can set in motion incremental change (Hacker, 2004; Mahony and Thelen, 2010; Scheingate, 2010; Streeck and Thelen, 2005). However, actors are confronted with the consequences of layering in their day-to-day activities as well. To better understand these consequences and how actors deal with those, we therefore want to extent this actor approach by not only focusing on actors as change agents but also on their day-to-day interactions with layering.
The concept of institutional work, borrowed from the Organization Sciences is of added value here. The concept was introduced by Lawrence and Suddaby (2006) who recognized a similar actor focused turn in institutional theory in the Organization Sciences. Although the influence of actors on institutions has long been recognized in this field (e.g. Selznick, 1957), here institutional theory mostly focused on the way institutions govern action. However, since the seminal works of DiMaggio (1988) on institutional entrepreneurship and Oliver (1991) on strategic responses of organizations to institutional contexts, there has been a steady development in literature focusing on the role of actors in creating, maintaining, and disrupting institutions (Lawrence and Suddaby, 2006). By contributing agency to actors when studying institutions and institutional change, insights from institutional and political models are combined (DiMaggio, 1988; Lawrence and Suddaby, 2006). Institutional work includes the strategic use discussed in the incremental change literature described above. However, this work does not only comprise the strategic use of the institutional context in order to bring about certain changes, but also the everyday getting by; actors cope with, keep up with, shore up, tear down, tinker with, transform or create new institutional structures, which can create, maintain, or disrupt institutions (Lawrence et al., 2011). This way a broad vision of agency is used; avoiding seeing actors as cultural dopes who are trapped by institutional arrangements but also of depicting them as highly influential institutional entrepreneurs (Lawrence et al., 2009). This institutional work is enacted by individuals and groups who can reproduce the roles assigned to them by their institutional context but can also challenge, modify, and disrupt these roles (Lawrence et al., 2011). It is therefore important to study how actors respond to layering empirically. It is this working approach to institutional layering that allows us to move into the layered institutional arrangement and thereby understand its consequences for daily practices.
Setting the scene: Institutional layering in Dutch healthcare
Layered institutional arrangement of Dutch healthcare
Short history of institutional layering in healthcare governance
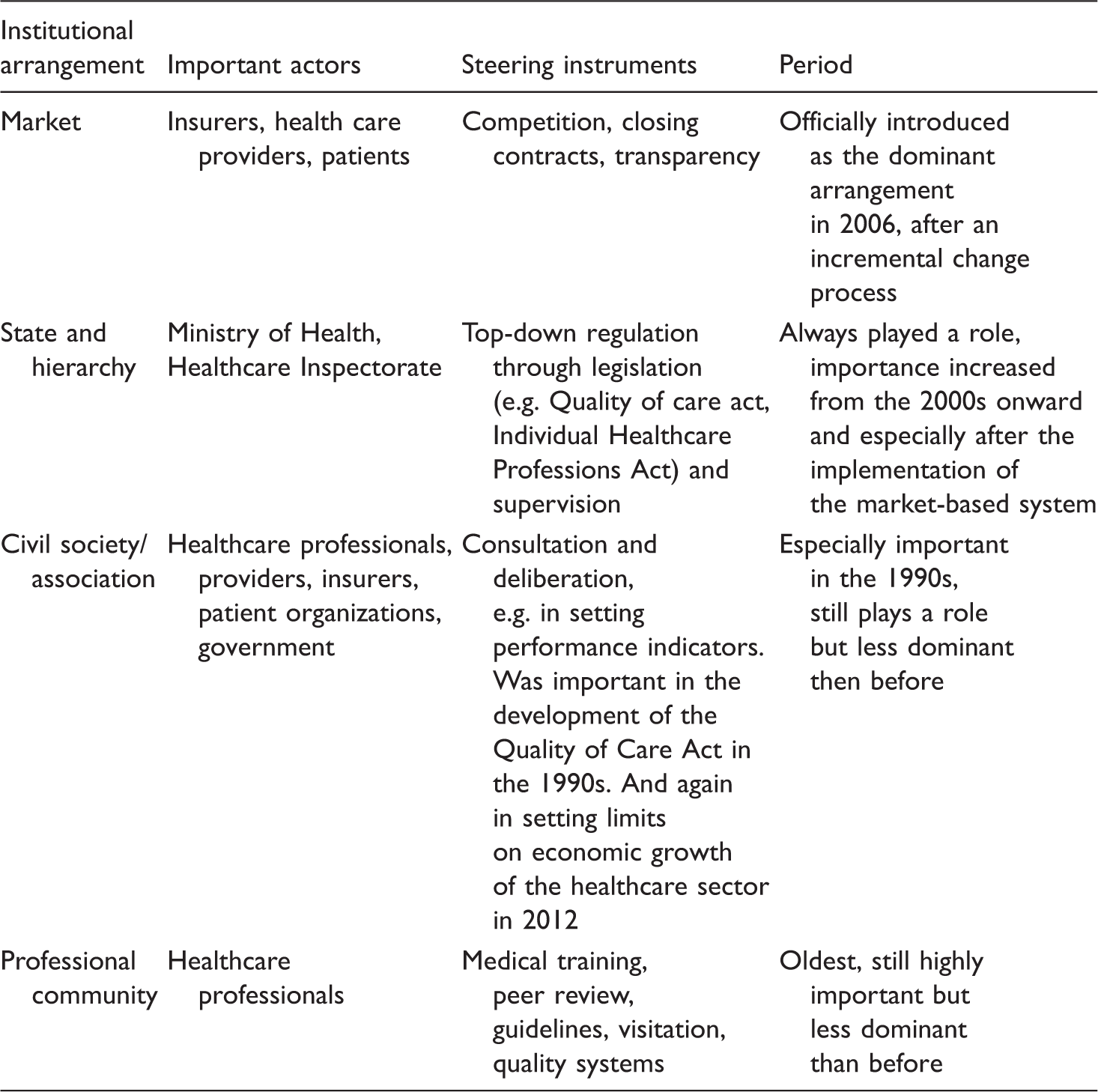
Originally, quality of care was based on self-regulation by the professional community, drawing on instruments such as medical education, peer review, clinical guidelines, visitation, etc. (Klazinga, 1996), complemented with a limited amount of state regulation, e.g. regarding academic training and the supervision of quality of care. The role of the state however was mainly to protect the boundaries of the medical sphere.
During the mid-1980s, a public discussion started on quality of care as part of the debate on getting a grip on rising healthcare costs. From the end of the 1980s onward, the associational arrangement in which consultation with societal actors involved in healthcare—professionals, healthcare providers, patient organizations, insurers, and government—played an imported role in bringing about change (Bal, 2008). This resulted in the implementation of several legal arrangements, such as the Individual Healthcare Professionals Act (1997) and the Quality of care Act (1996) which aimed to regulate quality of care.
Toward the beginning of the 2000s, it was concluded that the implementation of this legislation was inadequate (Casparie et al., 2001) which resulted in more state regulation of quality through the Inspectorate. This happened alongside the implementation of the market-based system, which was introduced in 2006 as the official governance arrangement. Within this system, all Dutch citizens are obliged to buy private health insurance. The idea is that the parties in healthcare (providers, insurers, and patients) regulate healthcare through competition and closing contracts on three markets. In the healthcare provision market, hospitals (mostly private not for profit) compete for patients. In the healthcare insurance market, insurers compete for the insured. Both healthcare providers and insurers are active in the healthcare purchasing market. Here, insurers can buy care selectively on the basis of quality and price. Transparency of healthcare quality is seen as a crucial instrument for the market to work, since quality information is needed by patients, insurers, and providers alike.
So throughout the years, the Dutch healthcare system became increasingly layered. With the introduction of the market-based system it draws from all four of the governance arrangements described above (see Tables 1 and 2).
Interaction between layers
The different layers in the Dutch healthcare system do not just exist alongside each other; they interact. The introduction of the market did not result in the elimination of other institutional arrangements. These preexisting arrangements—professional communities, the state, and civil society—became incorporated in, were conditioned, or even strengthened by the new healthcare system (Van de Bovenkamp et al., 2014). For instance, the professional community still plays an important role through the mechanism of self-regulation based on professional norms, which are set by professional associations. However, these norms partly take on a different meaning because departing from them becomes more difficult as actors such as the Inspectorate and insurers turn to them for regulatory grip. In terms of Mahoney and Thelen’s framework (2010), layering therefore also resulted in institutional drift, since the impact of guidelines changed as a result of shifts in the environment.
Elements of a civil society arrangement and the mechanism of consultation can also still be identified. For instance, insurers, healthcare providers, and the government reached an agreement after a consultation process aimed at reducing the rise in healthcare costs through consultation (NVZ et al., 2011) and civil society actors consult on setting performance indicators.
Interestingly, rather than being opposites the market and the state have proven to be mutually reinforcing institutions; the transparency of healthcare quality accompanying the market-based system also renewed emphasis on top-down steering. Examples of this include giving the healthcare inspectorate a more dominant role, setting up national quality and safety programs, and setting up a national quality institute in order to gain control over quality instruments (Van de Bovenkamp et al., 2014).
Consequences for the internal governance and the external regulation of hospitals
Layering has caused many actors to be involved in governing quality of care. They all use their own instruments and draw from different logics to try to get a grip on and steer quality of care. By consequence, hospitals find themselves in an increasingly fragmented institutional context, which makes them an interesting subject of study (Van de Bovenkamp et al., 2014). Although many actors are now involved in governing quality, the actors responsible for the internal governance (Board of Directors and Supervisory Boards) and the external regulation (the Healthcare Inspectorate) of hospitals have increasingly been given responsibility for quality of care. The process of layering also impacted the role of these actors in important ways. For example, the introduction of the Quality of Care Act in 1996 obligated healthcare organizations to have a quality system in place and gave Boards of Directors the final responsibility for quality in their hospital (Legemaate et al., 2013). The introduction of the Quality of Care act therefore affected the internal governance of quality of care since it transferred responsibilities within hospitals from professionals to the Board of Directors of healthcare organizations. The Healthcare Inspectorate, as the external state regulator of quality of care, was meant to supervise whether this responsibility was taken up in practice. At the same time, these actors have to relate to the self-regulation of professionals and participate in consultations in the civil society arrangement.
Moreover, the introduction of the market-based system meant that Boards of Directors have to negotiate contracts with insurers, whilst at the same time having to relate to quality demands of professional bodies, patient organizations, etc. Because of the central role of Boards of Directors, Supervisory Boards, and Inspectorate, in the layered governance arrangement they will be the focus of our study. In the rest of the paper, we further explore their institutional work, how this work results from and is influenced by institutional layering, and how this in turn can spur further institutional change.
Methods
A qualitative research design was used to conduct this study. First, interviews were conducted with actors (n = 18) who have played or play a role in the internal governance and the external regulation of the quality of care in Dutch hospitals: directors of hospitals (n = 5, some of them were also healthcare professionals), a quality manager (n = 1), a representative of the association for healthcare directors (n = 1), and a representative of the association for internal healthcare regulators (n = 1). Next to these, (former) inspectors of the Healthcare Inspectorate (n = 5) and policy makers of the Ministry of Health (n = 2) were interviewed. In addition, we interviewed governance experts and senior advisors (n = 3, one of them a former inspector), who were key players in the development of governance of hospitals in the last 20–30 odd years. All respondents operate from a profound and “experienced” understanding of the governance of quality in hospital care.
We tried to keep the conversations as open as possible, yet beforehand we distinguished four topics that we wanted to discuss during the interviews: (1) the meaning given to the governance of quality in hospitals throughout the years, especially focusing on the years building up to and after the introduction of the market-based system, (2) the background of the discussion on governance, (3) the role division of actors involved in healthcare quality and the instruments used by these actors to steer quality of care, and (4) views on, experiences with and responses to the interactions between actors within the different institutional arrangements. The first two authors undertook all the interviews. The interviews lasted between 60 and 90 min and were conducted in the respondents’ own environment in an open “conversational” way—known as narrative interviewing (Czarniawska, 1998). The interviews were recorded, after first seeking the respondent’s consent, and transcribed verbatim.
Second, we collected and analyzed policy documents on the topic of healthcare governance from the Ministry of Health, Welfare and Sports; reports from the Healthcare Inspectorate; evaluations of quality legislation and reports of the Dutch Safety Board that according to our respondents had a great influence in transforming the regulation of the quality of hospital care. In addition, we analyzed empirical studies (research reports, academic articles) on the governance of healthcare quality in the Netherlands.
Data analysis was a combination of induction and deduction. First, we coded our data inductively, which eventually led to the following four key codes: (1) the roles and responsibilities of actors in healthcare quality (e.g. who is responsible for quality of care, in what way and how do these responsibilities relate to each other), (2) the meaning of governance (e.g. what do actors mean when they talk about governance and what does this subsequently mean for the role division and activities of actors both within the hospital and its external environment, (3) the instruments to steer quality (e.g. what instruments do actors use to steer quality and how do they relate to each other), and (4) interactions between institutional arrangements (e.g. how do actors, steering mechanisms, and institutional logics interact). We then iteratively compared these “grounded” codes deductively with the theoretical concepts: governance of quality, institutional layering, and institutional work. The typology of institutional arrangements (Table 1) served as a theoretical framework for the deductive part of the analysis.
Results
In this section we show how layering has put the internal governance of quality of care on the agenda and how the actors, Boards of Directors, Supervisory Boards, and Inspectorate, engaged in institutional work, which enabled them to strengthen their position while at the same time confronting them with new problems in gaining control effectively. At the end of this section, we describe how these actors respond to these problems and how this in turn leads to institutional change.
Becoming active as a result of layering
The introduction of the market-based system was accompanied by an increased focus on transparency (Bal and Zuiderent-Jerak, 2011). In order for the market-based system to work and for actors to play their designated role, information about quality of care is seen as “absolutely essential” by the Ministry of Health (Schippers, 2011a, 2011b). As a result of this transparency the fact that mistakes are made and things can and do go wrong becomes broadly known as well (Klink, 2009). This resulted in extensive media attention in several major incidents. Our respondents emphasize the important role this transparency and the resulting media attention for quality incidents played in getting the subject of governance of quality on the agenda.
The responsibility for the content of care was completely assigned to professionals for which they did not have to be accountable. This was changed legally with the introduction of the Quality of Care Act in 1996. The Boards of Directors legally carry the final responsibility for everything in the organization. That includes the quality and safety of the care process. That has been duly noted for a long time. Nothing happened with that. Until, and that is the first time this was exposed, the Radboud case [case concerning high mortality rates on a cardiology ward]. (governance expert and former chief inspector)
As a consequence of this increased external public and political attention for the internal governance of quality, respondents point out that a shift can be seen in practice; Boards of Directors and Supervisory Boards have put quality firmly on their agenda. This feeling of urgency is generally felt by Boards of Directors and not only present in hospitals where quality incidents that received media attention occurred. And this transparency, with the paradox that is accompanied by it of course, has set a lot in motion. That goes for the Board of Directors and that goes for the Supervisory Boards. Supervisory Boards cannot hide in the attic anymore. Everything is transparent. (Healthcare Inspector)
So although the Board of Directors was assigned the legal responsibility for ensuring quality of care already in the mid-1990s and, by consequence, the responsibility of internal and external regulators to supervise if they had taken up this responsibility, this was put into practice only much later. The layered institutional arrangement of quality of care seems to have served as an impetus for these actors to take up their role. Only in the mid-2000s, when transparency had become a dominant value in the market-based system, were the agreements made under the institutional arrangement of the associational order implemented. Moreover, top-down state supervision of the implementation of this act was developed during that period. The introduction of the market-based system therefore served as a means to hold actors accountable for their designated role alongside a strengthening of state actors. As a result these actors indeed took up their role, thereby contributing to, in terms of Lawrence and Suddaby, the creation of their role regarding quality of care (Lawrence and Suddaby, 2006). We explore how they did this further in the next paragraph.
Using layers to gain control over quality
Above we saw how institutional layering influenced Boards of Directors, Supervisory Boards, and the Inspectorate to take up their role, thereby showing the influence of the institutional context on actors. Here, we focus on their institutional work to gain control over quality and how they use the layered institutional context in this work, thereby changing their institutional position within the hospital (Boards of Directors, Supervisory Boards) and in relation to the hospital (Healthcare Inspectorate). This analysis therefore shows how actors’ activities in turn shape institutions (Lawrence et al., 2009).
The governance of hospitals is mostly talked about in terms of trying to get clarity about the responsibilities of actors and relationships between those actors regarding the subject of quality of care. Despite the myriad of actors involved in quality of care as a result of layering, a clear division of responsibility is sought for. Respondents translate being responsible into the question whether the Board of Directors is “in control” of quality and safety within the hospital. The Supervisory Board needs to check whether this is indeed the case. The Healthcare Inspectorate in turn needs to supervise whether this internal governance system works. So, increasingly, Boards of Directors are attributed an important role in ensuring the quality of care, which strengthens their position vis-à-vis healthcare professionals, a relationship which can be a continuous struggle. If the relationship [between Board of Directors and medical professionals] is bad, then the medical staff will say to the director: quality in the consultation room is our thing. [I] agree when this concerns the one-on-one contact with the patient. [I] disagree when this concerns what happens next. I don’t need to know what happens in the consultation room but I do need to know how the individual specialist and his group of specialists work on quality and how they ensure the quality provided in that consultation room. (Former hospital director and former inspector) Throughout the years you step in earlier, you can nip it in the bud. That helps. Because there is more information, we now at least have the HSMR [Hospital Standardized Mortality Rate], well we did not have those eight years ago. (hospital director) They had a big fight with the internists and the intensive care specialists and they did not manage to solve that, so then the Inspectorate had to say ‘boo’. That is what they did and then you have them at your side. (quality consultant 3)
Struggling with layers
Above we saw how layering is used by actors in their institutional work to take up their role. However, layering can also blur responsibilities and have a burdening effect (Van der Heijden, 2011). This can also be seen in our case; actors are struggling with layers. They may use layering to strengthen their role within their organization or in relation to each other. At the same time it causes problems in their relation with external actors and as a result in the way they are forced to take up their role.
Working in a layered institutional arrangement means having to relate to many external actors, mostly by giving account of one’s actions. The transparency accompanying the market-based system not only served as a window for the internal governance and external regulator of hospitals to strengthen their role, but it also gives external actors the means to gain control over the internal governance of hospitals and the external regulation thereof. The result of this can best be described as a struggle between having to relate to external parties that are active in the different layers and at the same time to be in control over the quality of care in the hospital.
In the layered arrangement, market parties are attributed an important role in holding hospitals to account for quality of care (Klink, 2009; Schippers, 2011b). Patients should critically choose their provider and insurers should buy their care selectively. As we have noted above, in order to do so hospitals have to provide these actors with a lot of quality information. So far however, patients use quality information to choose their provider to a very limited extent (Van de Bovenkamp et al., 2013). Insurers, who do ask for quality information from the hospitals, hardly use that data either: respondents feel that in practice insurers do not steer on quality but on price (see also Zuiderent-Jerak et al., 2010): They poor out this bureaucracy all over you and you have to comply with that. So that keeps your organization busy. And subsequently the health care purchaser [insurer] comes by and you just talk about money. (Hospital director) We have to deal with insane legislation, a completely instable government policy and an enormous amount of organizations that have an opinion. (Governance expert) The biggest problem is the enormous pressure of the media and politics: if something goes wrong the Inspectorate failed. (Inspector IGZ) I have a kind of adage that the moment you make a decision, you have to do that according to the formal rules (…) but especially the preparation of such a decision has to be done as informal as possible, because you don’t hear what is really going on in the meetings and you have to get a feeling about the expected effect and that can only be done (…) in an informal way. (Member of Board of Directors hospital) You cannot use checklists for the informal things, these are too soft. There is a lot of ‘soft’ information to check. That is actually the core of everything. The governance of each organization is different because it is so situational, because it is so dependent on the type of institution, the kind of people… (Healthcare Inspector)
We can conclude that although the discussion on governance in Dutch healthcare was meant to clarify the distribution of roles and responsibilities for the quality of care, this clarity is threatened by the layered context. In case of incidents, for example, the state rushes in, thereby disturbing the market-based arrangement as well as other state arrangements like the Inspectorate and the internal governance of quality. The everyday getting by (Lawrence et al., 2011) with institutional layering, therefore also means struggling with layers. However, we have also seen examples where actors engage in institutional work by actively relating to the layered context to overcome these problems, the subject we turn to next.
Responding to problems by relating to layers
Actors respond to the problems described above and to having to manage the fragmented quality demands put on them by the market, state, and professional community through institutional work, showing once again the interaction between actors being influenced by their institutional context and their active engagement with this context. They do this both in response to the problems caused by the myriad demands from the external system and the nature of the instruments used by external actors. We discuss them in turn.
A first response to deal with the multitude of quality demands is simply to defy them (Oliver, 1991). This strategy of refusing to comply with certain requests of the Ministry (in case of the Inspectorate) or of other actors such as insurers (in case of Boards of Directors) is sometimes used in practice. Then in April or May we got this package of extra stuff of Zorgverzekeraars Nederland [association of healthcare insurers] and a week after that of the individual insurers. Then you had to retrospectively provide information on last year which was just a bit different than what we had to provide the Inspectorate with. Then I asked to find out how much energy this would cost, I had to clear the schedule of two people for six weeks for just one insurer (…). Then I refused. (respondent from association of healthcare directors) They made an inventory about the number of guidelines, regulation etc. they had to follow and they came to the number of 1400. His [director] proposition is that you have to make a well-argued choice about where you focus your attention on, because 1400 subjects is a pointless exercise (…) that you pick ten themes and as Board of Directors you decide to work on those. (healthcare Inspectorate)
Hospital boards and the Inspectorate also engage in institutional work in response to the problems identified regarding the nature and focus of the quality instruments that they are forced to use. They actively try to change these instruments, a strategy earlier dubbed by Oliver (1991) as manipulation. For instance, they try to gain control and prevent having to react to all kinds of outside ad hoc pressure by building quality and supervision systems that allow them to deal with quality more proactively. Moreover, these systems incorporate both formal and informal aspects of governance work. This way these actors try to reshape and (re)gain control over the governance of quality. Hospitals actively engage in discussions, in professional journals and elsewhere, to argue for a more strategic approach to quality in which they can take the lead. The Inspectorate, recognizing this call, developed a method to supervise the internal governance of hospitals called system-based supervision in which they look at the hospitals’ integrated prospective quality and safety systems and also walk around and talk to staff more informally in order to perform “reality checks.” Then the only thing you have to explain in Parliament is that you have [insight in] the system of the hospital. And that looked good and that also means that a hospital has a prospective risk management system, of which as the Inspectorate you think it is trustworthy. (hospital director)
What these examples show is that this type of institutional work can be a way for the actors involved to influence their position and the way they relate to the institutional context. This working with layers through strategies of defying and manipulation (Oliver, 1991) consists of trying to create manageable expectations, shift responsibilities, and influence the layered institutional arrangement.
Conclusion
Institutional contexts in the public sector have become increasingly complex as they are built on different institutional arrangements that exist simultaneously (Streeck and Thelen, 2005). We have shown that throughout the years the institutional arrangement to steer Dutch healthcare quality has become layered with different institutional arrangements placed on top of or next to each other, forming a sediment-like structure; self-regulation of professional communities, neo-corporatist consultations in the associational order, state-based regulations and negotiations at the healthcare market have been laid on top of each other and exist at the same time, interacting with each other to different effects. While sometimes conflicting, these institutional structures also are dependent on each other, e.g. the market could not function without guidelines made in professional societies.
Institutional layering has important consequences for actors who have to relate to an institutionally layered context. For example, they can be confronted with institutional fragmentation (Van de Bovenkamp et al., 2014). Because of these consequences it is important to gain more insight in how actors are influenced by institutional layering. However, using the concept of institutional work (Lawrence and Suddaby, 2006) we showed that in turn actors’ responses to layering can also cause further institutional change both within organizations and in their institutional context. Whereas literature on layering mostly focuses on the macro level and the literature on institutional work mostly focuses on the meso level, combining the two concepts allowed us to gain a better understanding of the interaction between the two levels. More specifically, insight is gained into how layering influences and is influenced by institutional work.
This interaction between layering, shaping the activities of actors and actors using and relating to layering in their institutional work is nicely shown in the governance and regulation of hospital quality as studied here. Our approach allowed us to see that layering changes the activities of actors in the public sector, can be used to strengthen one’s position but also presents actors with new struggles, which they in turn can try to overcome by relating and using the institutionally layered context. Layering and institutional work are therefore in continuous interaction. For example, the introduction of a market-based system with a focus on transparency urged Boards of Directors to increase their control over quality of care, thereby creating the opportunity for these boards to strengthen their position within the hospital and to get a stronger grip on their healthcare professionals. Therefore, the institutional arrangement of the market helped implement a structure that was in fact the result of an associational effort in creating quality policies. Moreover, the myriad of quality instruments that have been invented and implemented are used by Boards of Directors, Supervisory Boards, and the Inspectorate in their institutional work aimed at gaining control of quality of care. This way, layering enabled these actors to gain control and steer quality, albeit that dependency on other institutional arrangements, like professional self-regulation, still stays in place. The layered context also introduced problems such as having to relate to myriad actors and instruments that shape activities in terms of what it means to be “in control” in a specific way. The interplay of the layered institutional arrangements with their emphasis on different types of instruments and actor roles can thus also produce dysfunctional effects for quality of care. Again, we saw that actors respond to these problems presented by layering through institutional work aimed at influencing their institutional context. Through this work, actors try to reshape the governance of quality by influencing the institutional structures in which they work and their relation to other actors within and outside their organizations (Lawrence et al., 2011). Such institutional work is both strategic—as already recognized within the public administration literature—but also involves the day-to-day practice of getting things done.
The layering concept can enable our understanding of institutional change and its consequences. One of the advantages of the concept is that it focuses on both exogenous and endogenous sources of change, thereby acknowledging the important role actors play in bringing about change but at the same time acknowledging how their actions are influenced by the institutional context (Hacker, 2004; Mahoney and Thelen, 2010; Van der Heijden, 2011). Besides explaining institutional change, we feel that the layering concept can also help to better understand complex institutional arrangements and how they influence the activities of actors having to relate to such a context. The concept of institutional work helps to gain insight into how layering works out in practice further by focusing on the actions of actors in relation to layering. Combining institutional layering with a focus on the lived experiences of actors and their institutional work makes it possible to move into the layered structure of public governance and better understand the consequences of layering for, in our case, healthcare practices.
Footnotes
Acknowledgements
The authors wish to thank the respondents who participated in the study. They also like to thank the two anonymous reviewers, Iris Wallenburg and the rest of the Health Care Governance group of iBMG for their valuable comments to earlier versions of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research this article is based on was funded by ZonMw, the Dutch organization for Health Research and Development, project number 80-83505-98-001 and 70-70582-98-004.