
Abstract
In 2017, British Columbia (BC) transferred responsibility for healthcare services in provincial correctional facilities from the Ministry of Public Safety and Solicitor General to the Ministry of Health. This study explored how healthcare leadership perceived the impact of the transfer on services, work-life, and job satisfaction. We conducted one-on-one interviews (n = 8) with healthcare managers and medical and administrative leadership within Correctional Health Services. Using the Two-Factor theory of job satisfaction as a framework, we applied Interpretive Description methodology to analyse interview data. Participants identified changes to four areas of the working environment: (1) staffing, equipment, and resources (2) systems of supervision and support (3) standards, policies, and quality improvement and (4) culture and orientation. These changes predominantly affected motivational factors of job satisfaction and were described as enriching the roles of managers and staff. Participants described improved autonomy and recognition of providers, increased quality of services delivered, and a shift toward patient-centred care. The perspectives of healthcare leaders provide new insight into the potential impact of transferring healthcare services in custody to a public healthcare system. Discussion of changes and their affects also provide practical learning for jurisdictions seeking to improve healthcare under a variety of governance and service-delivery models.
Keywords
Introduction
Effective healthcare governance is essential to addressing health and healthcare inequities faced by people who experience incarceration1–3 and ensuring the clinical independence of healthcare providers working in these settings.1,3 However, there is a global lack of evidence concerning governance models for healthcare in custody 4 which affects the ability of jurisdictions to implement changes or align with relevant recommendations from bodies such as the World Health Organization.2,3 To understand the potential impact of models of governance and service delivery requires the perspectives of healthcare providers working in carceral settings.1,3,4
Globally, most systems of healthcare in carceral environments are under the authority of the ministry responsible for corrections. Limited research available on the experiences of healthcare providers in correctional facilities identifies ethical and structural challenges common to this model. Healthcare providers employed by corrections experience conflict between the cultures and priorities of healthcare and security which create barriers to clinical independence, 1 and directly affects care.1,5–7 In a small but growing number of jurisdictions worldwide, responsibility for healthcare in custody has been moved partially, or completely, to the ministry responsible for health.1,2,4 Increased oversight and engagement by health authorities is thought to reduce the risk of inappropriate intervention of correctional authorities in clinical care, foster equivalence with services in the community and improve working conditions.1,2,4 Currently, there is a lack of research examining this change in governance from the perspective of healthcare providers working in correctional facilities.
Our study aimed to address this gap by exploring the perspectives of correctional healthcare leadership in British Columbia (BC) where, in 2017, responsibility for healthcare in provincial correctional facilities moved from the Ministry of Public Safety and Solicitor General to the Provincial Health Services Authority (PHSA) under the BC Ministry of Health. In Canada, each province and territory provides medically-necessary hospital and physician services to residents through a universal public health insurance plan. 8 People incarcerated in provincial or territorial correctional facilities (which includes people awaiting trial or sentenced to less than 2 years) remain eligible for this insurance throughout their time in custody. However, in many jurisdictions healthcare services in custody are under the ministry responsible for corrections.
In BC, healthcare services are delivered by five regional and two province-wide health authorities. PHSA is a province-wide health authority that provides specialized services and programs such as BC Cancer. 9 Prior to the transfer, healthcare services in provincial correctional facilities were delivered by a private, for-profit company contracted to the Ministry of Public Safety and Solicitor General. The transfer responded to expert recommendations and calls for change10,11 including those from the World Health Organization, 3 BC Coroner’s Service 12 and Auditor General.10,13 The stated aim of the transfer was to improve quality and access to healthcare services and continuity of care between custody and community. 11 Through interviews with correctional healthcare leadership, we aimed to explore the impact of this transfer on healthcare providers working in provincial correctional facilities.
Methods
We conducted one-on-one interviews with healthcare managers of correctional centres and members of Correctional Health Services administrative and medical leadership teams.
KM sent email invitations to participate in a research interview to five leaders within Correctional Health Services who had key roles in the transfer. Invitations were sent to the seven healthcare managers by a member of Correctional Health Services leadership with KM CC’d. KM sent all follow-up invitations. Four people did not respond to the initial invitation plus one follow-up invitation.
Data collection
Interviews occurred between January and October 2019. KM conducted all interviews by phone or in-person. Interviews were audio recorded and transcribed verbatim. Transcripts were checked against audio recordings and de-identified. Each participant was assigned a single-letter identifier. Notes were taken during the interview and field notes were written after, though these were for reference and were not included as data. Approval for this study was granted by the University of British Columbia Behavioral Research Ethics Board (H17-02577) and the BC Mental Health and Substance Use Services Research Committee. Transcripts were managed using Nvivo 12.
Analysis
We used Interpretive Description methodology to structure study design, data collection tools and data analysis. 14 Interpretive Description was developed to generate grounded knowledge in the intersection of subjective experience and shared understanding of healthcare contexts in order to inform clinical practice.
All authors each independently coded three transcripts, then came together to discuss codes and develop initial themes. Within the context of these themes we applied Two-Factor theory as a framework to examine participant perceptions of effects of the transfer on their work-life and job satisfaction. 15 Two-Factor theory describes two parallel sets of factors which influence job satisfaction. 15 External factors affect job dissatisfaction and include interpersonal relationships, compensation, policies and administration, supervision, and working conditions. Motivation factors are intrinsic to the job and affect job satisfaction. They include advancement, possibility of growth, responsibility and authority, work itself, recognition, and sense of achievement. 15 The theory has been used in the nursing literature to understand the experiences of emergency department nurses, 16 psychiatric nurses, 17 and mental health nurses in an in-patient psychiatric ward. 18
KM coded all remaining transcripts and recoded the initial three, using this preliminary codebook and inductive coding. All authors participated in iterative discussion throughout the analysis. We developed initial themes into higher-order ideas until we reached consensus on final themes. No repeat interviews were conducted but participants had the option to review their transcript and/or the draft manuscript. One participant requested their transcript, and feedback was incorporated into the analysis. Five participants were sent a draft manuscript for comment.
Findings
Eight people participated in this study. Five were healthcare managers and three held leadership roles within Correctional Health Services. Three participants were women. Four participants were located in Vancouver or the Greater Vancouver Metropolitan Area, six were located across the province. Six participants had worked in provincial corrections prior to the transition. Interviews took between 45 min and an hour.
Participants identified multiple activities and initiatives implemented by PHSA that changed the work-life of healthcare staff and affected job satisfaction. Most changes were described as affecting motivational factors and enriching the roles of healthcare managers and staff.
We developed four categories of changes to work and working conditions highlighted by participants: (1) staffing, equipment, and resources, (2) systems of supervision and support, (3) standards, policies, and quality improvement, and (4) culture and orientation (Figure 1). In most instances, initiatives and activities implemented by PHSA were described as affecting multiple factors of job satisfaction. Themes of changes identified in interviews with healthcare managers and Correctional Health Services leadership in British Columbia.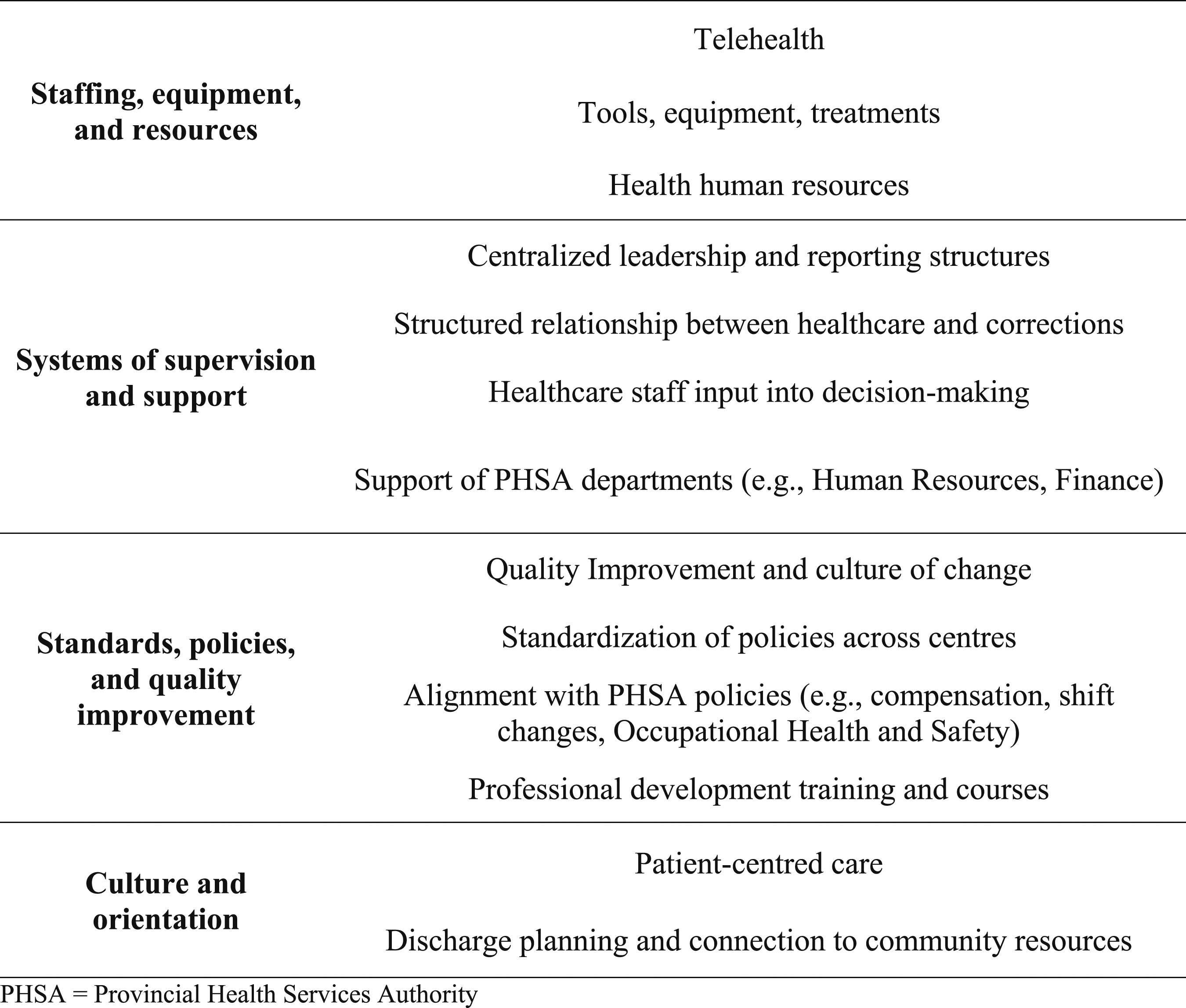
Staffing, equipment and resources
PHSA introduced new positions to each facility including access and transition nurses, mental health nurses, and concurrent disorder counsellors. Participants highlighted that increased staffing had affected “the whole team because now we’re not working short all the time” (P). They described these new positions as enriching the work of others in the department by increasing time available to staff to complete their work and by supporting specific components of care such as discharge planning.
We never had anybody for discharge planning. We kind of just had to roll it into the roles that we already had[...] Now we’ve got all these other roles that allow our healthcare department to flourish in ways that we haven’t before. (W)
Participants described increased access to physicians as improving the ability to provide efficient, high-quality services. All participants highlighted that the introduction of telehealth had increased access to physicians including specialist care such as for Hepatitis C and transgender clients. These resources increased autonomy and control for staff and supported higher quality care.
Though most participants acknowledged recruitment and retention as an ongoing problem, many felt the status of PHSA had helped to increase interest in positions and attract high-caliber candidates. PHSA also opened doors for advancement as seniority was now transferable to positions across PHSA’s other services.
Before I’d go through six, eight, ten people and then I’d find one diamond in the rough. Where now it’s, like, oh, my god, I have all these people that I’m interviewing and I have to pick the best out of a bunch of really great people. (W)
Participants also discussed increased access to equipment and treatments, such as pharmaceuticals to treat Hepatitis C. These resources helped to provide to high-quality patient care and increased feelings of autonomy and control.
Now we’re getting all these tools to work with patients. So patient care and quality of care’s going up. You’re able to provide them with things that you couldn’t provide[…] I mean, you feel empowered to do this job. (P)
Access to equipment and treatments also changed how participants saw their role and their ability to make a meaningful, long-term impact for clients.
Like, we can make a difference in people’s lives. Dentures, for instance... we can now get them a set of dentures that can maybe allow them to get a job. (W)
Systems of supervision and support
Structures of supervision and reporting implemented by PHSA were cited by participants as having a positive effect on the morale and working conditions of healthcare staff. The support of new leadership structures was contrasted with the isolation that healthcare managers felt prior to the transfer.
It was the manager that carried the ball at each centre, that ensured that the health services would carry on. And we would provide the best service we could. But it wasn’t because of leadership from the contractor. (L)
An important distinction was that PHSA leadership are experts in healthcare which supported perceptions that strategic directions and policies aligned with the values and goals of the professionals providing care. This alignment in turn supported a sense of ownership and control over services.
We’re not contracted to provide the service. We are the service. It’s our service. We’re not reporting to Corrections on our health outcomes. We report to the Ministry. We report to the PHSA Board. We’re health and we’re an entity on our own. (E)
Healthcare managers highlighted both benefits and challenges of integrating with PHSA departments such as human resources and finance. All managers described these departments as increasing bureaucracy. In some cases, managers felt that challenges were created because PHSA departments were unfamiliar with the context of corrections. Most managers said that despite the bureaucracy, these departments had relieved administrative burden and helped them focus their time and energy on staff and patient care. One health manager felt the increased administrative burden had reduced time spent with staff.
Even though sometimes it can make it seem like everything is further removed, having the specialists managing a lot of these elements has really made it easier for us to focus on the patient care. (D)
All participants highlighted that throughout the transfer healthcare staff had a voice in policy and decision-making. This engagement was seen as recognition of the expertise of healthcare providers as specialists in care in the carceral environment. It was also viewed as a fundamental part of improving working conditions and services and supporting providers to feel empowered in their work. All healthcare managers reported that PHSA continued to ask for advice from healthcare staff after the transfer and several were members of committees working on specific policy areas. This ongoing role for staff in decision-making was described as a marker of positive leadership from PHSA.
Standards, policies, and quality improvement
Nearly all participants identified increased access to training and professional development opportunities under PHSA as having a positive effect on staff and on quality of care.
I think it makes them feel a little bit more valued as employees. But it also makes them feel more qualified to deliver care. (D)
Healthcare managers were also offered training in leadership and clinical skills and helped them to feel well positioned to support staff.
Participants also identified negative effects of centralized PHSA policies. One such effect was that standardization of compensation rates meant that some staff lost monetary incentives previously paid by the contractor.
Some people had to take pay cuts, which has since been addressed. But that impacted I think their morale. So we had low morale for a while. (D)
Another was that centralized human resource policies meant the previous four-on-four-off rotation did not fit the PHSA definition of a full-time position (37.5 h). In some sites this was an ongoing source of staff frustration. In others, healthcare staff had been able to elect to go down to part time (0.93 FTE) to return to this rotation. The availability of this choice was credited to advocacy by individual leaders.
Centralization of policies was also highlighted as contributing to the standardization of care. Healthcare delivered under the Ministry of Health must be accredited by Accreditation Canada. Most participants reported that policies implemented to prepare for accreditation had raised expectations around standards and quality improvement. They also reported that the standardization of policies across centres had improved working conditions as well as care provided to clients. Measuring progress toward these standards helped to empower people with data and provided a means of recognizing areas of achievement. Focus on quality improvement and accreditation also increased feelings of recognition and professionalism among providers.
If we’re wanting to provide the best possible care to our clients, then that’s a way we can say that, hey, we meet all the professional standards that are required. So I think that’s really important, and I’m kind of looking forward to that. (W)
Participants highlighted the relationship between Corrections and PHSA as a key facilitator of improving and standardizing policies. The relationship between the two organizations meant healthcare staff felt supported in their work and that reporting structures provided a means of exerting more control and influence over working conditions and patient care.
It’s not just me now going to the warden and saying ‘we’re going to do this’ and hope for the best. They’re having these discussions and they’re collaborating to make it work for both sides. (D)
Culture and orientation
Participants identified a top-down shift in the orientation of healthcare services toward a focus on patient centred-care. This included a requirement that healthcare staff use the word ‘client’ when referring to people receiving care. This change in language was viewed as both signaling and contributing to a larger shift in culture. Participants felt that it changed the way staff viewed clients and their relationship as providers.
I see people being a lot more engaged than they were before. Before, it was really-- not everybody, not everybody was like this before -- but it was like, oh, inmate, inmate, inmate, stigma, stigma, stigma. Now we call them clients. […] And I feel like my staff in a sense are looking at our clients more like people than just inmates. (W)
This culture change also included modifying specific policies that had previously been dominated by security concerns, such as medication diversion, to a focus on client needs. It also contributed to a new understanding of the role of healthcare providers within the context of corrections and the purpose and meaning of their work.
Going from being a paid-for-by-corrections contractor, so basically, you’re answering to Corrections, to being a public health authority who works with Corrections but is paid through the province and not through Corrections. It’s a different relationship. And it also brings a different lens. (H)
Participants frequently identified the new focus on discharge planning and continuity of care as transforming their work and its impact in the lives of clients.
So even if [we] are providing excellent care while the client is with us, it doesn’t mean anything if there’s nothing after they leave […]. So, I think that is one of the biggest things that I think that the health authority has brought into that model of care is the continuity of care (E)
Participants saw this shift toward trauma-informed client-centred care, in combination with increased access to resources and treatment, as changing the relationship between healthcare and clients.
To be honest, and this is really hard to define, but there is different attitude about who we are now. Meaning if somebody asks for something healthcare wise, we typically will do our best to try to meet that need. And we go out of our way. I think we just take an extra step in anything that we do to make sure that we’ve addressed everything that we possibly can for that patient. (D)
Participants highlighted that the new orientation toward connection and integration with community services changed the relationship with community organizations.
One of the biggest complaints with community partners was the discharge plan historically was ‘here’s a bus ticket to Greyhound and off you go’[….] Or they’d just get released at court and they’re not our problem anymore. So that all changed the day PHSA took over. (P)
Participants discussed how PHSA’s status as a health authority and the relationship of the organization to community services improved information sharing and access to community services for clients in custody and after release.
The amount of doors that have opened for our clients and also us-- and when I say that I mean we’re not shut down when it comes to calling the hospital or calling a doctor’s office or trying to get them in with a specialist. And information sharing from our community […] we now actually have clout behind our name. (W)
Finally, many participants discussed feeling hopeful and excited about the culture of change and quality improvement that they felt under PHSA.
I just think that there’s endless possibilities […] we’ve got all the right people in the right places, and I’m just really excited for the future. I don’t know what it holds, but I think it’s going to be pretty good. (W)
Discussion
Healthcare leadership in BC’s provincial correctional facilities identified many ways in which the transfer to PHSA improved important factors of work-life and job satisfaction for healthcare providers. Participants also felt these changes had made a difference in the quality of care they were able to provide for clients and the impact of their work on health outcomes. These improvements are important from both an individual and health systems perspective; in addition to promoting retention and a healthy workforce, job satisfaction among providers has been linked to quality, safety, and patient satisfaction with care. 19
Participants in this study identified increased staffing and access to equipment and treatment as improving their control and autonomy over their work, as well as quality of care. Inadequate access to staff and equipment is commonly reported by healthcare providers in correctional settings in the US5,7,20 and Canada. 6 As part of the transition to PHSA there was a reported 40% increase in per-capita spending for healthcare services delivered in custody. 21 This study highlights the benefits of investing in health resources in correctional facilities, not just on patient care, but also on providers and their working environment.
Improved supervisor support and participation in decision-making were also highlighted frequently by participants in this study. Other studies in carceral contexts have identified ineffective leadership7,20,22 and/or perceived lack of respect for healthcare services and providers6,7 as an obstacle to quality care and job satisfaction. On the other hand, recognition, trust in managers and having a voice in decision-making have been linked with retention of nurses in other healthcare settings. 23 The reported impact of changes to authority, policy and staff supports in BC provide valuable insight for other jurisdictions and evidence arguments around the importance of governance in shaping these structures.
Like health systems around the world, burnout is a growing crisis in Canada’s healthcare workforce. A 2013 study among healthcare providers in Ontario’s provincial correctional facilities found that 67% of healthcare managers and 39% of nurses had scores of emotional exhaustion that indicate burnout on the Maslach Burnout Inventory-Human Services Survey. 6 The Job Demand-Control model posits that employee mental health and wellbeing are influenced by the intersection of job demands, such as workload and emotional strain, and job control. 24 Many of the changes to work-life identified by participants in this study directly addressed elements of workload, autonomy and control. Understanding how models of governance affect work-related stress for providers in correctional facilities may provide opportunities to support health, wellness and job sustainability.
To our knowledge, ours is the first study to examine the impact of this type of governance through the lens of job satisfaction and working conditions of healthcare staff. However, some of the changes identified by participants echo views of providers in UK who described the transfer of responsibility for healthcare in custody to the NHS as resulting in more patient-friendly care, a greater say for nurses in how services should be delivered and reduced feelings of professional isolation. 25 Our study provides greater breadth and novel insights into how governance models may affect healthcare providers.
The transfer to PHSA changed both governance and service delivery models. Prior to the transfer, healthcare services were delivered by private, for-profit contractors. Privatized healthcare delivery in custody is increasing in some jurisdictions and is particularly prevalent in the US. 26 Arguments and studies around this model have examined tradeoffs in costs, quality of care, health outcomes and oversight.26–28 Our study adds to this literature by offering insight into the impact of moving from a privatized delivery model to a public healthcare system on the working conditions and satisfaction of healthcare providers working in corrections.
Participants’ comments were predominantly positive, though some discussed periods of low morale as the transfer was underway. This is consistent with the Change Curve model of organizational change 29 based on Kubler-Ross’ stages of grief. 30 When the idea of change is introduced, people commonly respond with denial and remain committed to the status quo. As change is initiated people may fear or identify negative effects for themselves or their work resulting in anger and frustration. More than a year after the transfer occurred, when we conducted interviews for this study, most people would have moved into the final stages of acceptance and commitment.
Limitations
A strength of this study is that most participants had worked in corrections prior to the transfer and therefore had a comprehensive understanding of changes. Though interview questions probed for challenges and difficulties, most comments reflected positive perceptions of the transfer. Since participants candidly discussed challenges that were identified, we do not have reason to believe negative effects were deliberately omitted.
Limited research about models of governance for healthcare services in custody limits our understanding of the generalizability of findings. For example, we do not know what effect the centralized structure of PHSA may have had compared to a decentralized model under the Ministry of Health. Similarly, prior to the transition, healthcare services in BC’s provincial prisons were provided by a private, for-profit company. Further research is needed to understand and compare different models of service delivery within similar structures of governance.
Interviews were conducted with healthcare leadership and their views may not reflect the experiences of frontline staff. In a Scottish report, healthcare managers were “generally more positive about the transfer than frontline staff,” 22 though it is not clear how generalizable this discrepancy might be. Additionally, the focus of interviews was the transfer process and outcomes related to patient care; the absence of specific questions about job satisfaction may have missed key components. However, member-checking provided opportunities to identify gaps. Finally, interviews reflect early outcomes and potentially, optimism. Future research should seek to understand outcomes in the medium and long-term.
Conclusions
Healthcare leadership perceived the transfer to PHSA as having a positive effect on services and on the job satisfaction and work-life of healthcare providers. Many changes addressed challenges identified by healthcare providers in other correctional settings indicating that lessons learned in BC may be valuable to efforts to improve services and healthcare provider work-life in other jurisdictions. Governance models that support clinical independence through separated structures of supervision and support, resourcing and integration with community services may enable meaningful improvements to the work-life of providers in carceral contexts and to help address health equity for people who experience incarceration. Future research should examine and compare the impact of governance models on healthcare providers under different service delivery models and in the context of other systems of community healthcare.
Footnotes
Acknowledgements
All authors respectfully acknowledge that they live and work on the unceded traditional territory of the Coast Salish Peoples, including the traditional territories of xʷməθkwəy̓əm (Musqueam), Sḵwx̱wú7mesh (Squamish), and Səl̓ílwətaɬ (Tsleil-Waututh) Nations. Our sincere thanks to the participants for sharing their experiences and expertise. K McLeod is supported by the University of British Columbia Public Scholars Initiative.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.