
Abstract
The novel coronavirus (COVID-19) pandemic is a major heath crisis that continues to impact healthcare organizations worldwide. As infection rates surged, there was a global shortage of personal protective equipment, critical medications, ventilators, and hospital beds, meaning that healthcare professionals faced increasingly difficult workplace conditions. In this conceptual study, we argue these situations can lead to healthcare professionals experiencing moral emotions - defined as specific emotions which relate, or occur in response, to the interest or welfare of others - towards their organizations. This paper explores the three moral emotions of contempt, anger and disgust, and their potential influence on healthcare professionals’ workplace commitment in the context of a pandemic. Drawing from the moral emotions and organizational commitment literature, we develop a process model to demonstrate how healthcare professionals’ affective and continuous commitment are likely to decrease while, paradoxically, normative, and professional commitment may become amplified. The possible potential for positive outcomes from negative moral emotions is discussed, followed by theoretical and practical contributions of the model, and finally, directions for future research.
Introduction
The COVID-19 pandemic has become an ongoing crisis for healthcare organizations since it emerged in 2019. 1 Healthcare organizations were uniquely affected by the pandemic as they had to not only care for those infected with COVID-19 but contend with the challenges of keeping their workplaces and employees safe. Healthcare organizations have had to cope with surges in patient numbers despite significant efforts to slow the spread of infection2,3 as well as critical shortages of physical space, equipment (e.g., ventilators), intensive care beds and key medications-particularly through the first wave of the of the pandemic.4–6 Frontline healthcare professionals, who have described themselves as “unwilling martyrs”, 7 have been heavily affected by these conditions and thrust into a distressing new normal in their workplaces. Using the COVID-19 pandemic crisis as an illustrative example of an external event that resulted in organizational crises (where organizational crisis is defined as an extraordinary condition that is disruptive and damaging to the existing operating state of an organization), 8 we examine how employees’ responses to their organizations’ management of crisis events affects their commitment. Specifically, in this paper we explore the potential for moral emotions to influence professionals’ commitment, behaviours, and performance in their workplace by asking: How do healthcare professionals’ crisis-driven moral emotions affect their organizational and professional commitment?
Moral emotions are emotions linked to the interest or welfare of others and are experienced in situations that are morally relevant. 9 Individuals perceive their workplaces as morally relevant when they, or their organizations, act in ways that influence the well-being and rights of others. 10 The moral nature of the workplace is highlighted for those working at the front of the COVID-19 pandemic, such as healthcare professionals, as it has been during past pandemics. 11 Moral emotions should be particularly salient in the context of the current pandemic for two reasons. First, although global pandemics have occurred in the past, the scale and scope of the current pandemic has left healthcare organizations in crisis, facing a lack of resources and escalating demands. However, the lack of planning displayed by healthcare organizations was somewhat surprising in light of guidance available from previous outbreaks such as SARS, MERS, H1N1 and Ebola in the last decade. 12 Healthcare professionals in these organizations have had to face the brunt of these effects, through no fault of their own, making them especially likely to experience negative affect towards their workplaces. Second, frontline healthcare professionals working in healthcare organizations such as hospitals means seeing the direct effects of (in)adequate care on patients. Although there are many healthcare professionals working globally during this pandemic, we focus on the organizational and political landscape affecting physicians and nurses in North America. In this conceptual study, we examine the potential influence of healthcare organizations’ responses during the first wave of the COVID-19 pandemic, from March to August 2020, 13 on healthcare professionals’ three moral emotions: contempt, anger, and disgust. We argue that experiencing these three negative emotions will serve to decrease affective and continuance organizational commitment but has the potential to lead to an increase in normative commitment and the commitment to one’s profession.
Organizational commitment, a construct defined as the psychological state which characterizes an employee’s relationship with their organization, has been examined for its ability to promote effective organizational functioning. 14 While there have been some studies into how employees’ organizational commitment may change in the face of external events such as economic crises,15, 16 there has not yet been considerable research into how, and by which mechanisms, employees’ organizational commitment may change during a pandemic. In terms of employees’ moral emotions, theoretical frameworks have conceptualized affective commitment as being motivated by emotions and feelings rather than individuals’ rational judgements 17 while other studies have found that moral emotions play a key role in the maintenance of physicians’ professional values and may drive institutional work (e.g., the effort to create and maintain one’s institution) at the micro level. 18 Antecedents of moral emotions in the workplace (e.g.,) 10 have been investigated and theories suggesting that emotions can energize (or de-energize) employees’ behaviours in organizational contexts have been proposed (e.g.,),19, 20 but little research has examined specifically how moral emotions could affect organizational commitment specifically. Professional commitment, the strength of an individual’s identification with and involvement in their profession, is often used in reference to self-regulated professions such as physicians, accountants, and engineers. 21 Tensions between professional and organizational commitment persist, and the effect of moral emotions and COVID-19 have not been investigated as factors affecting either type of commitment.
This study aims to contribute to two streams of management literature in three ways. First, we expand the moral emotions literature by attempting to understand how experiencing moral anger, contempt, and disgust may affect perceptions of one’s workplace and behaviours within it, and in doing so, respond to recent calls to further understand moral emotions in management scholarship (e.g.,).
22
Second, we attempt to contribute to the organizational commitment literature by illustrating how different types of commitment (affective, continuance, and normative) may be differentially affected by the same organizational crisis event. Third, we propose to contribute to the broader workplace commitment literature by examining how moral emotions may have opposing effects on professional and organizational commitment - suggesting that negative moral emotions may, in some cases, result in positive outcomes. Our process model is depicted in Figure 1. Process model illustrating the impact of healthcare professionals’ more emotions (contempt, anger, and disgust) on their professional and organization commitment during the COVID-19 pandemic.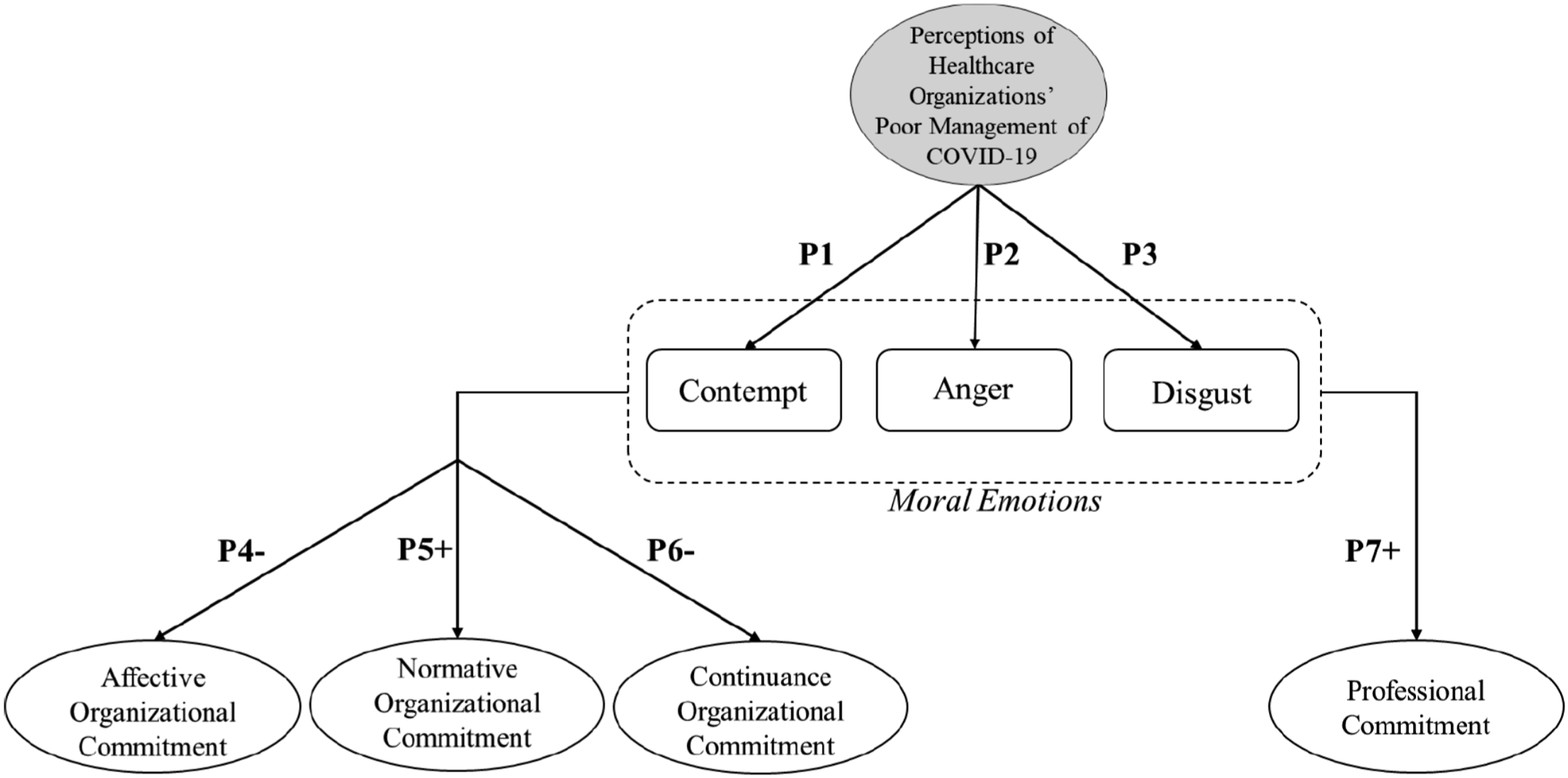
The impact of negative moral emotions on healthcare professionals’ workplace commitment
Moral emotions
While there is no neat division between moral emotions and their nonmoral counterparts, Haidt explains that emotions become moral when experienced in the specific material conditions of moral issues linked to the interest or welfare of others, or to society as a whole. 9 These emotions serve to efficiently alert individuals to when they, or others, have not upheld the moral standards of society.9,22 Moral emotions have origins in biology and previous experiences 23 and can be learned via social situations. 22 Individuals experience moral emotions in response to immoral events and the mistreatment of themselves or others 24 – e.g., in the case of healthcare workers, mistreatment may be suffered by employees, patients, or their families. There is evidence to suggest that the capacity to experience moral emotions may be automatic 25 and that moral emotions serve as motivators for individuals’ behaviours, such as preventing unethical conduct 26 and promoting prosocial behaviour. 22 Moral emotions are those that respond to moral violations or motivate moral behaviour. 9 For example, moral anger would be the feeling of anger resulting from experiencing a moral violation, such as anger in response to witnessing discrimination, versus anger resulting from a non-moral violation (e.g., a flight cancellation). We use this terminology in order to denote the emotions discussed occur in response to questions of morality.27,28
Moral emotions are grouped into families of emotions which share similar characteristics. These families are differentiated based on the focus of the emotion (i.e., the transgressor or the victim) and whether the behaviour violates or transcends moral standards. 9 These families include the following moral emotions: other-praising, other-suffering, other-condemning and, self-condemning. 9 In this paper, we focus on other-condemning emotions, which are defined as those that are experienced in response to others’ moral transgressions and are commonly considered to be composed of the trifecta emotions of contempt, anger, and disgust.9,22,25,29 We take the view of the victim – that is, the healthcare worker – where the transgressor is the healthcare organization. We concentrate on other-condemning emotions because healthcare professionals are likely to feel that they are tied to the choices of their organizations which have resulted in subjecting them to detrimental workplace conditions. Contempt is defined as a feeling of disdain towards those who have violated a moral norm or the ethic of a community, 29 in this case, the norms of the health services community. Moral anger describes the indignation that occurs when a moral standard has been violated without justification. 9 Disgust has been conceptualized as a defensive emotion that protects individuals against potential sources of contamination and is often linked to moral judgment. 30 We focus on these three emotions because they are the negative moral emotions experienced in response to others’ moral transgression, thus making them particularly relevant for healthcare professionals during the COVID-19 pandemic – we suggest that such workers would be experiencing emotions related to circumstances largely outside of their control and dictated by their organizations’ responses. These three emotions, named the CAD triad, have been proposed as guardians of the moral order as they motivate people to change their relationships with those that have violated it. 29 Although there has been empirical support for combining contempt, anger, and disgust into a single construct of negative moral emotions, 31 we take the view of Greenbaum et al. (2020), to consider and examine each emotion in isolation since they each have unique antecedents and outcomes. 22
Moral Emotions during Pandemics
Contempt
Contempt involves a judgement of another party’s moral character and values, where the evaluator finds the other party lacking. 9 Contempt can be experienced in nonmoral situations, 22 but the pandemic creates a moral context in the workplace by creating moral issues for healthcare professionals as they are required to make decisions and perform actions that may harm or benefit others. 32 Greenbaum and colleagues (2020) suggest this can frame feelings of contempt in a moral light. We suggest that healthcare professionals will experience contempt towards their organizations’ management of the pandemic for three reasons.
First, studies have shown the performance of undesirable job tasks acts as a driver of moral contempt.10,22 Healthcare professionals are asked to care for patients infected with COVID-19 under undesirable conditions since hospitals are overcrowded and resource-scarce, leading to unsafe environments. 33 A lack of critical resources (e.g. PPE, ventilators, medications, hospital beds) as experienced during the pandemic34,35 makes for distressing work environments where ethical and moral dilemmas create unnecessarily traumatizing experiences that can breed contempt for their organization.
Second, poor compensation is known to act as a source of moral contempt in the workplace.10,22 Pay inequities evoke feelings of frustration and resentment in employees because they feel mistreated and that their employers are defaulting on their obligations. 36 The situation for healthcare professionals, particularly in the United States, continues to be paradoxical. As COVID-19 cases rose, many healthcare professionals initially found themselves either out of work, furloughed or taking significant pay cuts of up to 70% of their salary. 37 While this was not the case for all organizations (for example, some organizations offered pandemic pay or increased employee bonuses),38–40 healthcare organizations that did make cuts attributed them to the financial difficulties caused by the cancellation of elective and non-emergent procedures. 37 However, some large healthcare companies, such as HCA Healthcare in Tennessee, received billions of dollars in federal emergency stimulus funding while simultaneously warning their nurses that they might face layoffs if they did not agree to wage freezes and reductions. While HCA Healthcare was cutting the pay of its front-line healthcare providers, it did not reduce its executives’ million-dollar salaries. 41 We argue that such wage cuts are demoralizing to healthcare professionals who were still required to put themselves at risk for lower pay, fewer benefits, and less security 37 while hospital executives remain fully remunerated, leading to feelings of contempt against such organizations.
Third, healthcare professionals are likely to experience contempt targeted at healthcare organizations due to organizations’ lack of preparedness for COVID-19. Although the impact and severity of the pandemic could not have been predicted, the significant lack of foresight displayed by hospitals may be considered surprising in light of guidance stemming from previous outbreaks such as SARS, MERS, H1N1 and Ebola in the last decade. 12 Further, the World Health Organization (WHO) had been warning of a “Disease X”, a new and unknown pathogen capable of an outbreak of epidemic or pandemic proportions since 2016 and advising governments and healthcare systems to start creating preparedness plans. 42 Hospitals in the United States were struggling to prepare for the potential onslaught of COVID-19 patients and at that time, only 30% of nurses surveyed reported that their organizations had sufficient equipment inventory to respond to a COVID-19 surge. 12 Moreover, fewer than half of nurses felt that their employer had provided them with necessary information about how they should respond to the virus. 12 One physician likened her experience to being “played for a fool” because as infection rates and case severity rose, she was told to use lower levels of protection (e.g., using a surgical mask instead of an N95) and re-use single-use PPE. 43 Further, some healthcare workers in the United States stated that they faced termination for publicizing their poor working conditions and inadequate personal protective equipment due to their corporations’ efforts to maintain a corporate image. Physicians voiced that they have a duty to speak up about threats to patient safety and were unfairly punished by their organizations for doing so. 44 Given that contempt arises when a party’s (in this case, the healthcare organization) values and priorities are deemed lacking, we argue that each of these failing actions (i.e., forcing undesirable job tasks upon staff; providing low compensation; and lack of preparation) will incite feelings of contempt towards these workplaces.
Healthcare professionals’ will experience moral contempt related to their organizations’ response to the COVID-19 pandemic.
Anger
Employees experience moral anger when their organizations break with moral standards or commit transgressions without justification. 22 Throughout the pandemic, healthcare professionals have raised the alarm about inadequate and improper PPE that puts themselves and their patients at risk. 34 We argue that if healthcare professionals are going to risk their lives, there exists a reciprocal obligation, both on the principle of fairness and legislated through occupational health and safety acts, that their healthcare organizations will keep them safe. This perspective is supported by social exchange theory, which proposes that powerful, albeit ambiguous, rules dictate behaviour in situations where there are exchanges of resources such as time, money, energy, and other intangibles. We posit that healthcare professionals are likely to experience moral anger due to their organizations continuing to expect them to perform their duties with inadequate personal protection. For example, during the SARS pandemic, one study found that nurses expressed less anger when appropriate PPE was supplied as it was understood to be a display of organizational preparedness and support. 45 Although it may be argued that organizations are justified in their transgressions due to the scarcity of resources across the industry, we suggest that workers will perceive themselves to be unfair victims of this transgression, thus making the transgression unjustified. For example, when Kious Kelly, a nurse manager at a Manhattan hospital, succumbed to COVID-19 after having to wear a garbage bag in lieu of proper protective equipment, his colleagues were angry, calling his death preventable, and blaming the hospital system for failing to protect their innocent colleague. 46
Research has suggested that perceptions of unfairness can lead to moral anger. 22 Quarantine requirements of up to 14 days had been a near universal recommendation for COVID-19 positive individuals. While guidance from public health departments have evolved over the course of the pandemic, one thing has remained constant: if you feel sick, stay home. CDC recommendations included self-isolation mandates for those who are sick, those with known or suspected exposure to COVID-19, as well as individuals who have tested positive. 47 However, some hospitals forced COVID-19 positive healthcare professionals back to work sooner than public health guidelines suggested may be safe by suggesting that they would be fired if they did not return to work. 48 Further, employees who were sick with COVID-19 were instructed to return to work as long as they did not have a fever. 48
In another example of unfairness, when COVID-19 vaccines became available, there were instances in the rollout where non-patient facing staff, administrators or those working from home received vaccines before frontline doctors and nurses. In the case of Stanford Health Care, young frontline physicians and trainees were largely excluded from the first round of vaccinations in favour of senior staff or specialists who were not directly involved in patient care. 49 Similarly, in Toronto, a public relations specialist posted a photo of themselves getting a vaccine, which lead to widespread accusations of “queue jumping” by administrators ahead of those at the highest risk – frontline healthcare providers. 50
We argue that such inequality imposed upon employees by their healthcare organizations - particularly those that appear contrary to public health and CDC guidelines - are likely to lead healthcare workers to experience a sense of broken moral standards, resulting in moral anger.
Healthcare professionals will experience moral anger related to their organizations’ response to the COVID-19 pandemic.
Disgust
Disgust, in its primordial form, is a defense against contaminants. 9 Although healthcare professionals are potentially exposed to pathogens in the everyday practice of patient care, the working conditions surrounding COVID-19 are unique and have served to elevate these exposures. Healthcare professionals are trained in universal precautions (i.e., standard guidelines aimed at preventing infection), which involves the routine use of PPE and handwashing to prevent the transmission of disease. 51 However, during the current pandemic, a lack of adequate PPE left healthcare providers unable to protect themselves in keeping with their knowledge and training of effective infection control protocols. 11 For example, healthcare providers have been asked to re-use PPE intended for one-time use until it is “visibly soiled” or “no longer retains structural integrity” in efforts to conserve dwindling supplies, 34 effectively increasing their risk of infection. Researchers have illustrated that concerns regarding hygiene, cleanliness, or death, act as antecedents to disgust, 22 suggesting that the conditions created by healthcare organizations are likely to incite feelings of disgust related to physical contamination.
Second, the sociomoral aspect of disgust is elicited by hypocrisy and disloyalty. 29 We argue that demonstrations by healthcare organizations and governments alike touting the heroism of healthcare workers while expecting them to work with inadequate PPE 52 is likely to result in employee perceptions of organizational hypocrisy and betrayal. The prevailing narrative of healthcare heroism centers around healthcare workers sacrificing themselves, like soldiers, for the good of others. 53 Healthcare workers have expressed that the more dangerous the working conditions, the more the “hero” moniker has been used. 54 As suggested in the popular press,12,54 we argue that this moniker draws attention to the bravery and altruism of healthcare workers rather than the continued existence of hazardous working conditions that may have been avoided with proper planning, adequate PPE, and staffing.
Healthcare professionals will experience disgust related to their organizations’ response to the COVID-19 pandemic.
Influences of moral emotions on organizational commitment
Organizational commitment: Affective
Affective organizational commitment relates to employees’ emotional attachment and identification with an organization. 14 Healthcare professionals, notably nurses, are increasingly exhibiting low levels of affective commitment towards their healthcare organizations, 55 making them more likely to suffer decreased affective commitment when faced with negative moral emotions. Given that moral anger is an emotion that condemns others’ behavior and judges that behavior offensive, 56 we suggest that this experience will decrease any felt affection or warmth towards one’s organization. Second, Haidt 9 describes contempt as a cool emotion where the object of contempt is treated with less warmth, respect, and consideration in future interactions. Contempt leads individuals to distance themselves from the source of this emotion, particularly when they believe that the source is to blame for its actions. 56 This leads us to suggest that experiencing contempt towards one’s organization, particularly when healthcare professionals blame their organization for an inability to deliver the quality of patient care they desire, is likely to reduce their sense of organizational identification. Lastly, studies have shown that disgust often triggers avoidance behaviours since individuals do not want to be in proximity, physically or otherwise, to a disgusting object or idea. 9 We suggest that the negative moral emotions of anger, contempt and disgust will lead healthcare professionals to lose their emotional attachment to their organizations.
Healthcare professionals’ moral emotions of anger, contempt and disgust will result in reduced affective organizational commitment.
Organizational commitment: Continuance
Continuance commitment is often seen in employees who have few or no other job alternatives. 14 Based on the idea that employees have made an investment in the organization and leaving would result in losses, 57 continuance commitment occurs most commonly for those working in low demand sectors and is focused on the employer-employee economic exchange relationship. 58 Given that hospitals have suffered from understaffing for some time, and the pandemic has only served to exacerbate these effects, 59 continuance commitment is likely to have been low for healthcare professionals even without resource deficiencies and mismanagement. Moral anger is associated with a tendency to want to punish transgressors (in this case, one’s place of employment). 56 We argue that this desire to punish may result in the consideration of leaving one’s organization, or at least reducing commitment to working within that organization long-term. Further, since morally relevant feelings of contempt can arise in response to poor compensation and benefits, 10 we argue that when positions offering higher compensation both in terms of monetary and non-monetary benefits arise, healthcare professionals are likely to view their own organizations’ values as lacking by choosing to prioritize other concerns over their well-being.
Healthcare professionals’ moral emotions of contempt, anger and disgust will result in reduced continuance commitment.
Organizational commitment: Normative
Normative organizational commitment is a rational attachment to an organization characterized by employees’ feelings of obligation to remain. 14 These feelings of obligation can result from the internalization of normative pressures exerted on individuals prior to or after entry into an organization and generally denote an acceptance and identification with organizational goals. 17 The goal of most healthcare organizations is the care of the patients that they serve 60 and this organizational goal overlaps with the ethical duties and responsibilities of healthcare providers to treat patients, even during extreme circumstances. 61
While there has been some debate about the limits of healthcare providers’ duty to serve during a pandemic, 11 most healthcare providers believe they should continue to provide care even in highly adverse conditions as a result of their specialized knowledge and training.62,63 This is particularly salient for physicians, who take an oath to serve the public good. 11 Healthcare professionals have consistently demonstrated their normative commitment by continuing to perform their duties and treat patients regardless of hospital working conditions.
Negative emotions play a critical role in individual’s cognitive activation process - raising awareness and directing an individual’s attention. 64 We argue that the negative emotions of contempt, disgust and anger will increase commitment to the organizational goal of patient care, and that healthcare professionals will be increasingly aware of the difficulty faced by these patients in pandemic conditions. We suggest that the lack of resources (in terms of time, energy, and protective equipment) which results in negative feelings will also act to increase empathy and awareness of patients’ suffering due to this same lack of resources. This experience could result in increased commitment to those being cared for by healthcare professionals, and thus, increase normative commitment to organizations which allow them, to the best of their ability, to provide care to patients.
Healthcare professionals’ moral emotions of contempt, anger and disgust will result in higher normative organizational commitment.
Influences of moral emotions on professional commitment
Professional commitment
Professional commitment describes the congruency between an individual’s personal beliefs and the goals of their profession, where greater congruence leads to greater efforts to help the profession and its members. 65 We suggest that negative feelings towards one’s organization will serve to increase engagement within one’s profession. First, negative emotions direct behaviour towards victims, and anger in particular leads to actions of victim-directed support. 25 Healthcare professionals have demonstrated considerable support for each other during the pandemic since they are all similarly victims of the same situation. For example, with PPE in critically short supply, healthcare professionals took it upon themselves to either make PPE (e.g. fabric masks, eye-protection and scrub caps), petition their governments, or organize public drives for protective equipment on social media.34,66 Healthcare professionals are also mindful of ways that they can protect each other from unnecessary exposure to the virus. This has included using unconventional protective equipment, such as covering patients with large plastic bags during aerosolizing procedures 67 or changing established procedures. 68 The latter has included limiting the frequency of high-risk procedures (e.g., bronchoscopy), where medically appropriate, to limit disease spread and exposure to their colleagues. 68 Nurses have likened the COVID-19 experience to that of working on a battlefield and acknowledge the importance of caring for their coworkers and sharing the load. 69
Research has shown that shared difficult experiences bring people closer together. 70 COVID-19 has presented a collective challenge for all healthcare professionals such that nurses in Wuhan reported a heightened sense of professional collegiality during COVID-19. 62 Increased collegiality between nurses is consistent with reports from previous pandemics.71,72 Extant research has shown that stronger collegial ties result in stronger professional commitment. 21 Knowing that others within their profession are suffering from the same negative pandemic organizational experiences, we would expect that healthcare professionals would feel more strongly tied to their colleagues and feel a stronger sense of commitment towards them.
Being part of profession and/or professional association brings certain privileges, resources, and powers.73,74 For example, studies have found that being part of a nursing association brings nurses social benefits and support for their ideas.75,76 As noted earlier, the moral anger, contempt and disgust experienced by healthcare workers is likely to, at least partially, emerge from feeling undervalued and unappreciated by their organizations. Thus, we secondly argue that if one’s sense of value is diminished within one’s own place of work, one may search for other sources of strength – such as within one’s profession.
In terms of the effects of moral anger, the experience of anger as an emotion is subject to moderation. For example, when witnessing a mobbing in the workplace, the degree to which others experience moral anger was moderated by the how much they believed the victim was deserving of the mistreatment. 77 Given that healthcare professionals are unlikely to view others in their profession as deserving of their difficult workplace conditions, we suggest that anger will make suffering colleagues appear more deserving of sympathy and thus increase felt commitment towards them. Contempt can arise due to disdain of those who have violated the norms or ethic of a community. 29 In this case, workers who feel that their organizations have breached the norms of the medical and health community may search for a community that retains these ethical norms – most immediately, their peers. In this way, we suggest that the emotion of contempt towards one’s organization may lead to increased commitment to one’s profession. Finally, in terms of disgust, caring for another’s personal hygiene or bodily functions elicits this emotion. 78 Disgust is often applicable to occupations that are considered to be dirty, as is in the case of coroners or undertakers. 22 Most healthcare professionals are accustomed to disgust in their everyday work life, 79 as part of their profession – however, they are less likely to be familiar with suffering from sociomoral disgust arising from the hypocrisy and betrayal shown by their organizations. We argue that this novel experience is likely to cause such individuals to seek support from those who are in similar, sympathetic situations – their professional peers.
Healthcare professionals’ moral emotions of contempt, anger and disgust will increase their professional commitment to each other.
Discussion
Theoretical implications
The current study contributes to our understanding of the antecedents and consequences of workplace emotions during times of crisis. We build on, and extend, existing literature in emotions and workplace commitment in three ways. First, this study contributes to our knowledge of how moral emotions may directly affect workplace attitudes and outcomes. The impact of employees’ affective commitment to organizations has been investigated, as well as the influence of employees’ moral judgements and virtues. 17 However, to our knowledge, moral emotions have not yet been specifically considered as potential antecedents of organizational commitment. There has been much ongoing debate about the emotions of anger, disgust, and contempt as separate constructs,29,31 our study advances the line of thought that each of these emotions can be examined in isolation as we show that each may result from unique workplace antecedents. For example, we suggest that ignoring public health rulings and asking employees to continue to work when rules are transgressed may trigger anger; that showing weak character during times of crisis may result in contempt; and that the use of the ‘hero’ moniker to describe workers forced to operate in unsanitary conditions may lead to disgust.
Second, the current conceptual study contributes to a growing body of literature that illustrates how “feeling bad can do good”. 80 Previous literature around the benefits of negative emotions in the workplace showed that the sharing of negative events lessened and mitigated individuals’ unpleasant feelings. 81 Negative moral emotions have been frequently studied and cited for their deleterious effects, but our study argues that they can also have positive consequences for group members. For example, negative moral emotions could be a mechanism through which in-group loyalty, solidarity and connection is fostered in employees.
Third, our model contributes to the workplace commitment literature with separate implications for affective, normative and continuance commitment. There have been studies demonstrating the impact of moral distress and moral injury on healthcare professionals’ affective commitment, 82 but little consideration of the impact of moral emotions on commitment. Our study offers a contribution to the affective commitment literature by way of exploring additional antecedents to healthcare professionals’ affective commitment, which are of particular salience to organizations during the COVID-19 pandemic. Studies have found that breaches in psychological contracts or exchange relationships between employees and their organizations have resulted in decreased affective commitment.83,84 In our model, we used the failure of some healthcare organizations to provide the PPE for their healthcare workers as an illustrative example of a breach in their psychological contract and would predict ensuing decreases in healthcare professionals' affective commitment.
Current understanding and research of normative commitment has highlighted the importance of employees’ feelings of obligation to their organization14,85 with investigations into the effects of organizational trust, managerial relationships, work structure and justice. 86 However, our study suggests healthcare professionals’ normative commitment can be increased, not necessarily as a result of intra-organizational factors, but as a result of their professional commitment and their duty to the public. Healthcare professionals need the environment and resources that healthcare organizations provide in order to continue to serve the public. Thus, they remain at their organizations, not from a perceived obligation to the organization itself, but rather because it is a way for them to maintain their duty to the public. Healthcare organizations may benefit from increased normative commitment in this way, as they will maintain a normatively committed workforce despite less-than-ideal organizational conditions.
Our study also has the potential to contribute to the organizational citizenship behaviour (OCB) literature. Previously investigated antecedents to OCBs included employee, task, organizational and leadership characteristics. 87 There has been little investigation to date on how moral emotions might lead to OCBs. Researchers have investigated the effects of employees’ discrete emotions, moods, and dispositional traits on organizational outcomes (e.g., performance, creativity, group dynamics and leadership). 88 These investigations showed that positive moods and positive affect demonstrated greater influences on workplace outcomes than their negative counterparts.88,89 The influence of negative affect on organizational life is complex and substantial given how strongly negative emotions are experienced. Our study would argue that negative moral emotions may have opposing effects on OCB-I (individual-focused OCBs) and OCB-O (organization-focused OCBs), 90 such that healthcare workers are more likely to act pro-socially towards fellow employees within their organization or profession and less likely to engage in positive, voluntary behaviors that help their organizations during a pandemic.
Practical implications
This paper has important practice implications for healthcare organizations during COVID-19, as well as for any future health crises. Some sources of healthcare workers’ negative moral emotions cannot be easily or immediately fixed (e.g., global PPE shortages), but managers within healthcare settings can take concrete steps to temper the sequalae that these moral emotions have on their employees and stakeholders.
Managers should take decisive steps to remedy the underlying causes of their healthcare professionals’ negative moral emotions. Healthcare management learnings from previous pandemics have touted the importance of providing emotional and psychological support to healthcare professionals to foster emotional resilience and the ability to deal with stressful situations. 91 We have three suggestions for managers. First, the provision of positive feedback – both at the direct and senior manager level - can act as a proxy for organizational support to help diminish employees’ feelings of anger. 45 Second, contempt may be diminished through the clear communication of the values of the organization and detailing how the division of resources aligns with these values. Third, changing the rhetoric used by hospital administrators concerning the heroism of healthcare professionals, and instead acknowledging the difficulties they face, and outlining steps that the organization has, and will, take to reduce these difficulties, may serve to decrease feelings of disgust.
Our study suggests that the strongest risk of current pandemic working conditions is to employees’ continuance commitment. This is demonstrated by 22% of nurses indicating that they intend to leave their current position, which is up from 15.9% in 2019 prior to the pandemic. 92 With lucrative travel contracts available to healthcare professionals, coupled with low or decreased pay at certain organizations, healthcare professionals’ perceived costs of leaving their current organizations will likely be lower than pre-pandemic conditions. Additionally, having experienced workplace exposures to COVID-19, particularly without adequate PPE, leaves healthcare workers unwilling to share physical space with their families and loved ones after work62,93 due to fears of being contaminated and acting as a disease vector. This is likely to also contribute to healthcare professionals’ inclinations to leave frontline workplaces. As research has shown repeatedly that perceived inequities result in greater employee attrition and turnover 94 and pay cuts and job losses have been reported to disproportionately affect front-line workers during the pandemic,37,41 managers must become cognizant that these healthcare professionals are likely to take concrete actions to minimize these occurences or leave the frontlines altogether.
Another practical implication of the current study is that healthcare organizations and healthcare leaders should recognize and harness the paradoxical benefits that shared negative experiences may have for their employees in terms of group cohesion commitment. In order to do this, healthcare organizations should understand the actions that are needed to achieve positive outcomes out of negative work events. This includes reinforcing the pattern of professional commitment that healthcare workers develop with one another. Commitment to a professional group does not eliminate the possibility of concurrent organizational commitment 21 and rather, should be beneficial to the organization as well, particularly when employees perceive low conflict between the two.95–97 Building on Hadley’s (2014) findings on emotional disclosure at work, healthcare organizations should foster environments and opportunities in which their workers can process and share their negative moral emotions. This could include promoting weekly or monthly staff meetings that allow for a diverse display of emotions and supporting those displays in a non-punitive manner.
Working on the frontlines of a pandemic is distressing for healthcare workers and they experience high rates of fear, sadness, depression and anxiety. 98 Healthcare professionals are at high risk of poor mental health outcomes and may need psychological resources and support. 99 In previous studies, actions directed towards colleagues were found to negatively impact job stress, increase job satisfaction, and act as a surrogate for organizational support. 100 Performing altruistic or helping acts generates positive emotions in individuals who receive help and creates an urge to reciprocate in a similar fashion.101,102 Experiences in helping or gratitude form a self-renewing basis for cooperative relationships and communal support. 102 Healthcare professionals helping one another during COVID-19 is a way in which they can create positive emotions for themselves. In the broaden-and-build model of positive emotions, it was proposed that positive emotions act as an antidote to negative emotions by dismantling their psychological and physiological effects. 102 Healthcare professionals could use the positive emotions they receive from helping their colleagues as a way to cope and recover from their psychological and emotional distress induced by the COVID-19 pandemic. Managers should foster and encourage opportunities for colleagues to support one another, perhaps in the form of peer-support groups.
Haidt (2003) described anger as the most underappreciated moral emotion because it is typically associated with motivations to attack, humiliate, or get revenge. Anger is frequently used as an exemplar of a negative emotion due to its connection with adverse effects in the workplace such as aggression, violence, bullying and, deviance. 103 However, anger can serve as an important catalyst for prosocial change. Moral anger propels individuals to stop perpetrators of misconduct, 31 promotes victim-directed support, leads to reconciliation, improves relationships, and can lead to whistleblowing.22,103 Managers should try to harness the power of this emotion to create an ethical organizational climate that creates opportunities for voice and speaking up to make positive changes, particularly in times of crises.
Lastly, managers should address the inequities in the exchange relationship between themselves and their employees that can lead to negative moral emotions. Since the psychological contract inherent in organizational commitment involves equal exchanges, healthcare organizations could implement strategies that would help to allay their workers’ fears around COVID-19 infection. This could involve policies that redeploy healthcare workers at elevated risk of COVID-19 infection away from high-risk areas or creating programs that provide supplementary housing to healthcare workers wishing to protect their families, 104 thus providing an increased sense of balance between the efforts and inputs asked of employees and their working conditions and compensation.
Limitations and future directions
The work presented here is theoretical in nature. Empirical testing of this model is required to determine its validity and ability to predict how healthcare workers organizational commitment has changed due to COVID-19. Since we suggest that it is possible for healthcare professionals to have reasons to increase their normative and professional commitments while also experiencing potentially large decrease in their affective and/or continuance commitments, an avenue for future research would be to determine the relative size and magnitude of these relationships and how those leaving their organizations or professions experienced reductions or increases in their types of commitment. In particular, given the duration of the COVID-19 pandemic and its prolonged impact on healthcare organizations, investigating how organizational and professional commitment changes over the course of the same crisis event should be studied. We also consider only healthcare professionals, primarily in hospital environments, as the experience of caring for COVID-19 patients has been largely experienced there or other acute care settings; we acknowledge that professionals' experience in other healthcare or non-healthcare settings may be different. Cultural variations on the experience of emotions and organizational commitment were not explored here. There is evidence to indicate that the experience of emotions, particularly moral ones, is cross-cultural, 22 but this is not sufficient to conclude that changes in organizational commitment will be uniform worldwide. Similarly, how employees may be affected by the pandemic as individuals outside of the employment context (e.g., suffering from anxiety, worry or depression in their personal lives 105 ) and how those experiences would then impact their professional experience, was beyond the scope of the current study, but interactive effects would provide a worthwhile venue for examination. Moral events may simultaneously activate multiple emotions from different moral emotion families, so future studies should investigate the impact of other moral emotions such as guilt or shame. Pandemics have also been shown to evoke non-moral emotions such as fear, sadness, anxiety, and depression. Subsequent studies can examine the effects of these nonmoral emotions on healthcare professionals’ organizational commitment. Exploring the differences between moral and non-moral anger in organizational contexts is another promising direction for future research. From a standpoint of theoretical contributions, we suggest that exploration of pandemic-specific situations such as the impact of unpredictability and munificence would be worthwhile avenues of future consideration.
Exploring other organizational outcome variables would also be valuable. For example, the impact of the pandemic on unethical behaviours (e.g., theft) as well as the effects of solidarity between specific roles on interprofessional teams on professional commitment may be worth further study. Increases in professional commitment and in-group solidarity may have unintended negative consequences (e.g., tribalism), which warrant investigation. These variables can be investigated at the individual, group, and organizational level. Understanding the outcomes of healthcare professionals' moral emotions will provide practical information for organizations in order to sustain and improve their performance through not only the COVID-19 pandemic but various other unpredictable, complex organizational crisis events in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.