
Abstract
Although healthcare managers make increasingly difficult decisions about health innovations, the way they may interact with innovators to foster health system sustainability remains underexplored. Drawing on the Responsible Innovation in Health (RIH) framework, this paper analyses interviews (n=37) with Canadian and Brazilian innovators to identify: how they operationalize inclusive design processes; what influences the responsiveness of their innovation to system-level challenges; and how they consider the level and intensity of care required by their innovation. Our qualitative findings indicate that innovators seek to: 1) engage stakeholders at an early ideation stage through context-specific methods combining both formal and informal strategies; 2) address specific system-level benefits but often struggle with the positioning of their solution within the health system; and 3) mitigate staff shortages in specialized care, increase general practitioners’ capacity or patients and informal caregivers’ autonomy. These findings provide empirical insights on how healthcare managers can promote and organize collaborative processes that harness innovation towards more sustainable health systems. By adopting a RIH-oriented managerial role, they can set in place more inclusive design processes, articulate key system-level challenges, and help innovators adjust the level and intensity of care required by their innovation.
Keywords
I ntroduction
Healthcare managers are steadily confronted with difficult decisions regarding the adoption and dissemination of new medical devices, digital technologies, and novel ways of delivering care (Marsilio and Prenestini, 2020). Although there is an important body of knowledge on the costs, benefits, and unintended consequences of new technologies and services (Martin et al., 2012; Soarez and Novaes, 2017), few scholars examined whether and how healthcare managers may interact with health innovators in order to foster innovation that adequately considers the needs, demands, and challenges of health systems. Although innovators’ decisions are made at an early stage in the innovation development process, the choices they make bear direct implications for the sustainability of health systems (Lehoux et al., 2008; Fasterholdt et al., 2017). For Fineberg (2012), sustainable health systems are characterized by: 1) a healthy population, 2) superior care (“effective, safe, timely, patient-centered, equitable, and efficient”), and (3) fairness, which implies that services are provided “without discrimination or disparities.” Healthcare managers are thus well positioned to inform health innovators’ decisions at an early stage and facilitate innovation development processes that foster more equitable and sustainable health innovation.
Within this perspective, the Responsible Innovation in Health (RIH) framework draws attention to the responsibility features an innovation should possess and to the contribution it may bring to health systems (Silva et al., 2018). More specifically, RIH emphasizes the importance of 1) setting in place inclusive design processes to gather the needs of diverse stakeholders; 2) designing a solution that is responsive to system-level challenges; and 3) considering the level and intensity of care required for the innovation to be used safely and effectively by intended users (Silva et al., 2020).
Drawing on RIH, the aim of this paper is to generate insights for healthcare managers about the way they can influence how health innovators define what problems their solution should tackle and how it may contribute to health systems. Nested within a broader case study, our study focuses on interviews (n = 37) with the leaders of 16 innovative for-profit and not-for-profit organizations from two Canadian provinces (Ontario and Quebec) and one Brazilian state (São Paulo). Our findings explore 1) how these innovators operationalize inclusiveness in their design processes, 2) what influences the responsiveness of their innovation to system-level challenges, and 3) how they consider the level and intensity of care required by their innovation. By highlighting the challenges faced by health innovators as well the practices that are conducive to sustainable health and social care innovation, these findings contribute to healthcare management research and practice. First, they clarify how innovations can be designed to support health systems. Second, they provide empirical insights on the way healthcare managers can promote and organize collaborative processes that harness innovation towards more sustainable health systems.
Health innovation in healthcare management research and RIH
With the aim to assist healthcare managers in implementing “innovative ways of working,” scholars shed light over the organizational challenges raised by health innovation (Martin et al., 2012). They also examined organizational readiness to change (Williams, 2011) and the impact of multidisciplinary collaboration (Alrabie, 2020; Giacomelli et al., 2019), employee involvement (Busch-Casler et al., 2020), and clinical leadership (Dickinson et al., 2013; Erskine et al., 2013; Lega et al., 2017; Storey et al., 2015) on the adoption of new technologies and services. Such research recognizes that healthcare managers’ decisions are constrained by “scarcity of resources” (Marsilio and Prenestini, 2020). Indeed, policymakers across industrialized countries increasingly emphasized the need to reduce spending growth. This resulted in pressure not only on workforce recruitment and service provision, but also on spending associated to drugs and medical devices. According to an international scoping review, the most frequently documented challenges faced by health systems relate to: governance (strategies, collaboration, and inter-sectoral coordination), service delivery (quality, access, and integration), and human resources (availability and competency) (Roncarolo et al., 2017). Thus, beyond the economic and organizational sustainability of specific innovations (Marsilio and Prenestini, 2020; Martin et al., 2012), healthcare managers should also consider how different types of innovation may affect governance, service delivery, and human resources.
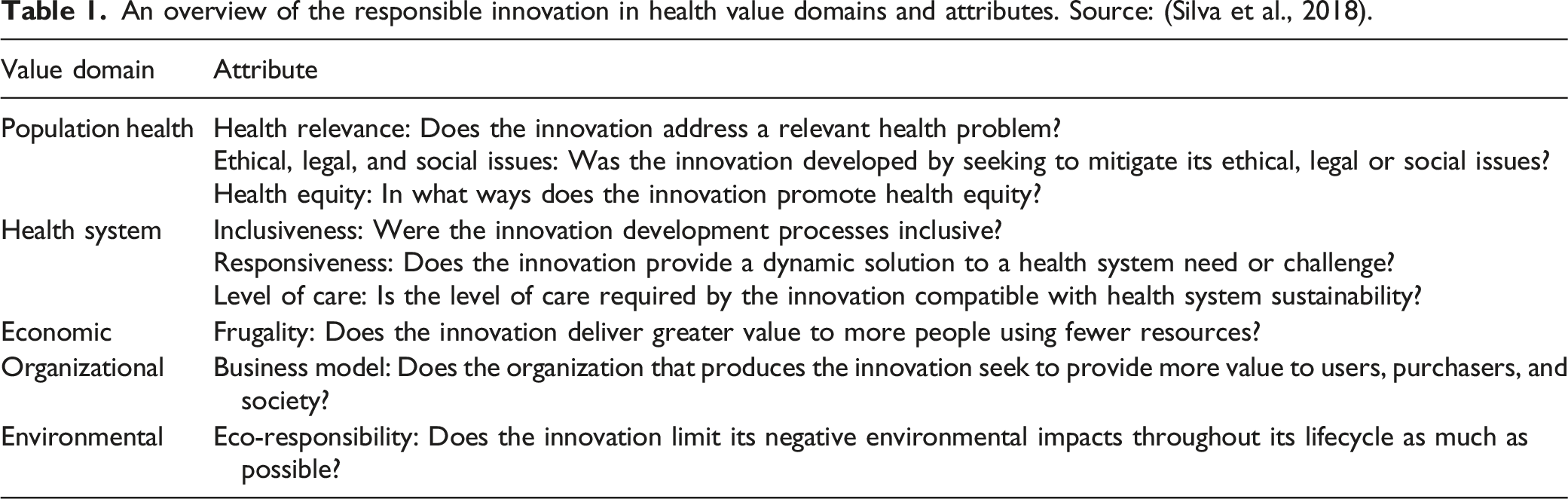
Responding to the call for new approaches to support managers in balancing “adequate innovation openness with the public budget allocated to health care” (Marsilio and Prenestini, 2020), this paper draws on RIH (Lehoux et al., 2018; Silva et al., 2018). For Silva et al. (2018), articulating “the supply of innovation to the demand of health systems” (and not vice versa) is imperative because the way new technologies are “financed, developed, and brought to market render health systems increasingly inequitable and unsustainable.” RIH is grounded within Responsible Research and Innovation (RRI), which seeks to steer innovation towards major social, environmental, and economic challenges (Stilgoe et al., 2013). To develop and validate responsibility constructs specific to healthcare, Silva et al. (2018) conducted an international Delphi study with RRI scholars, biomedical engineers, bioethicists, and Health Technology Assessment experts. As Table 1 summarizes, the RIH framework is comprised of nine responsibility attributes falling into five value domains. Our qualitative study focuses on its three health system value attributes because they are well-suited to examine how innovators and healthcare managers may collaboratively shape the solutions being offered to health systems. We empirically explore the following research questions: • How do innovators operationalize inclusiveness in their design processes? • What influences the responsiveness of their innovation to system-level challenges? • How do they consider the level and intensity of care required by their innovation? An overview of the responsible innovation in health value domains and attributes. Source: (Silva et al., 2018).
Methods
Study design
Our study is nested within a broader longitudinal case study that began in 2017. Its goal is to understand why and how innovative organizations in mature and emerging economies may develop and bring to market responsible health innovations. Our study focuses on three regions that can generate rich empirical lessons. Ontario and Quebec are, respectively, the first and second largest Canadian provinces, accounting for 38.5% and 19.8% of the country’s Gross Domestic Product (GDP). Health systems in Ontario and Quebec are publicly funded and the Canadian drug and medical devices industry is concentrated in these two provinces. Brazil has an extensive publicly financed health system and São Paulo is the most economically developed state, accounting for 33,9% of the country’s GDP.
Following a theoretical case sampling strategy (Eisenhardt and Graebner, 2007), we relied on the RIH framework to identify cases. We looked for innovations that were, for instance, aiming to reduce health inequalities by catering to vulnerable groups, enabling safe and effective care in the community or adopted eco-responsible design principles (Silva et al., 2018). The legal structure of the organizations and the type of innovation served as internal diversification criteria.
The case selection process unfolded between January 2017 and March 2018, using websites and social media accounts dedicated to health innovation and entrepreneurial activities pursuing a social or environmental mission. Following a personalized invitation, a research team member described our study’s aim to potential participants and gathered information to ascertain whether the case met our criteria. Overall, 14 organizations in Ontario were contacted, one did not meet our criteria and nine refused to participate, six organizations in Quebec were contacted and two refused to participate, and eight Brazilian organizations were recruited (none refused). A total of 16 organizations were thus recruited.
Interviews and data analysis
To fulfill this paper’s aim, we rely on two rounds of interviews (n = 37) with high-level managers (Chief Executive Officers, Chief Scientific Officers, and Chief Technology Officer). Initial interviews included more than one respondent per organization, lasted between 30 and 118 minutes and explored the genesis of the innovation, what problems it seeks to address, and how it interfaces with health and social care services. About a year later, we conducted a follow-up interview with one key informant per organization to take stock of the progress made and to validate a preliminary case description (Goffin et al., 2019).
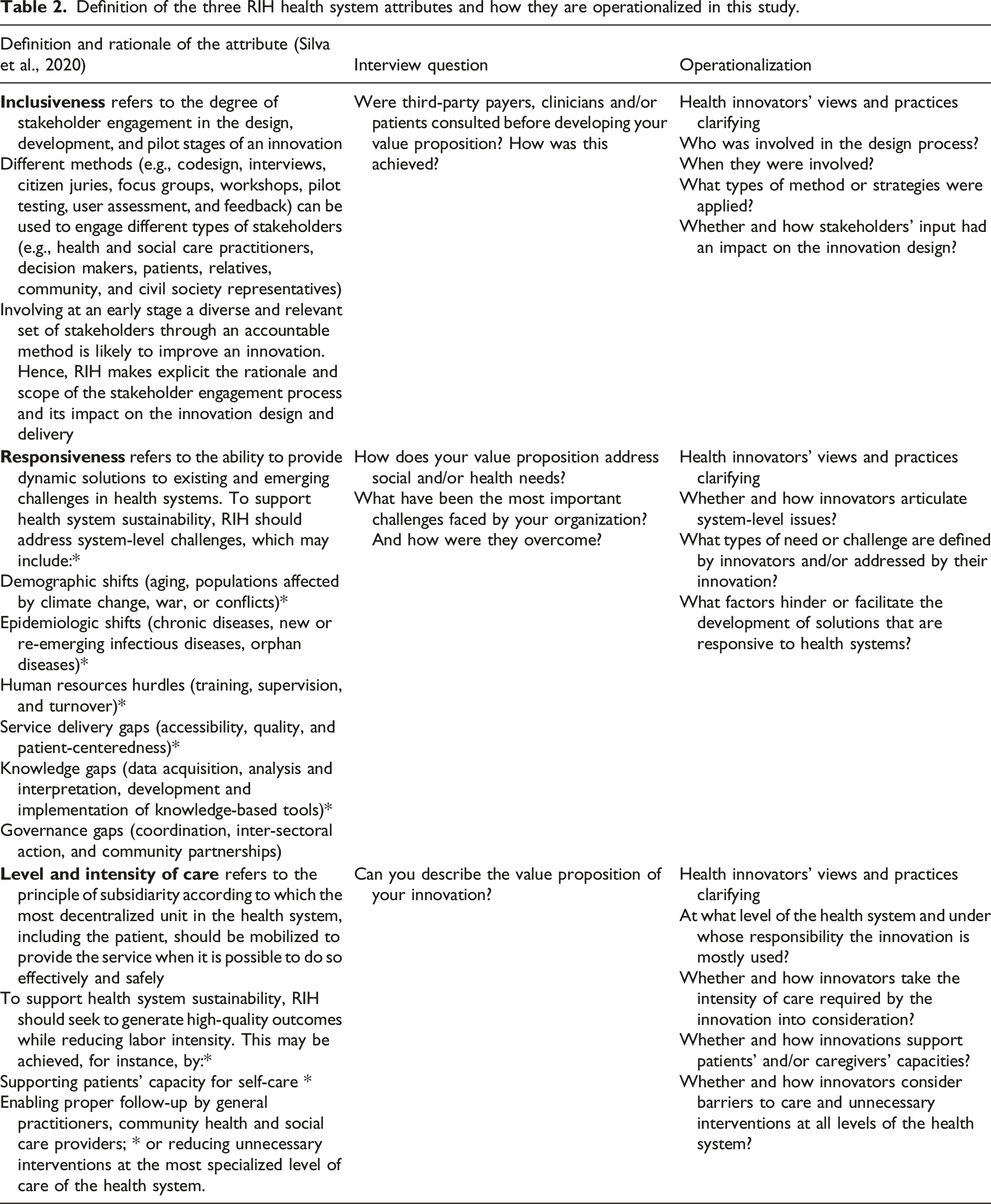
Definition of the three RIH health system attributes and how they are operationalized in this study.
Findings
An overview of the innovations developed by study participants
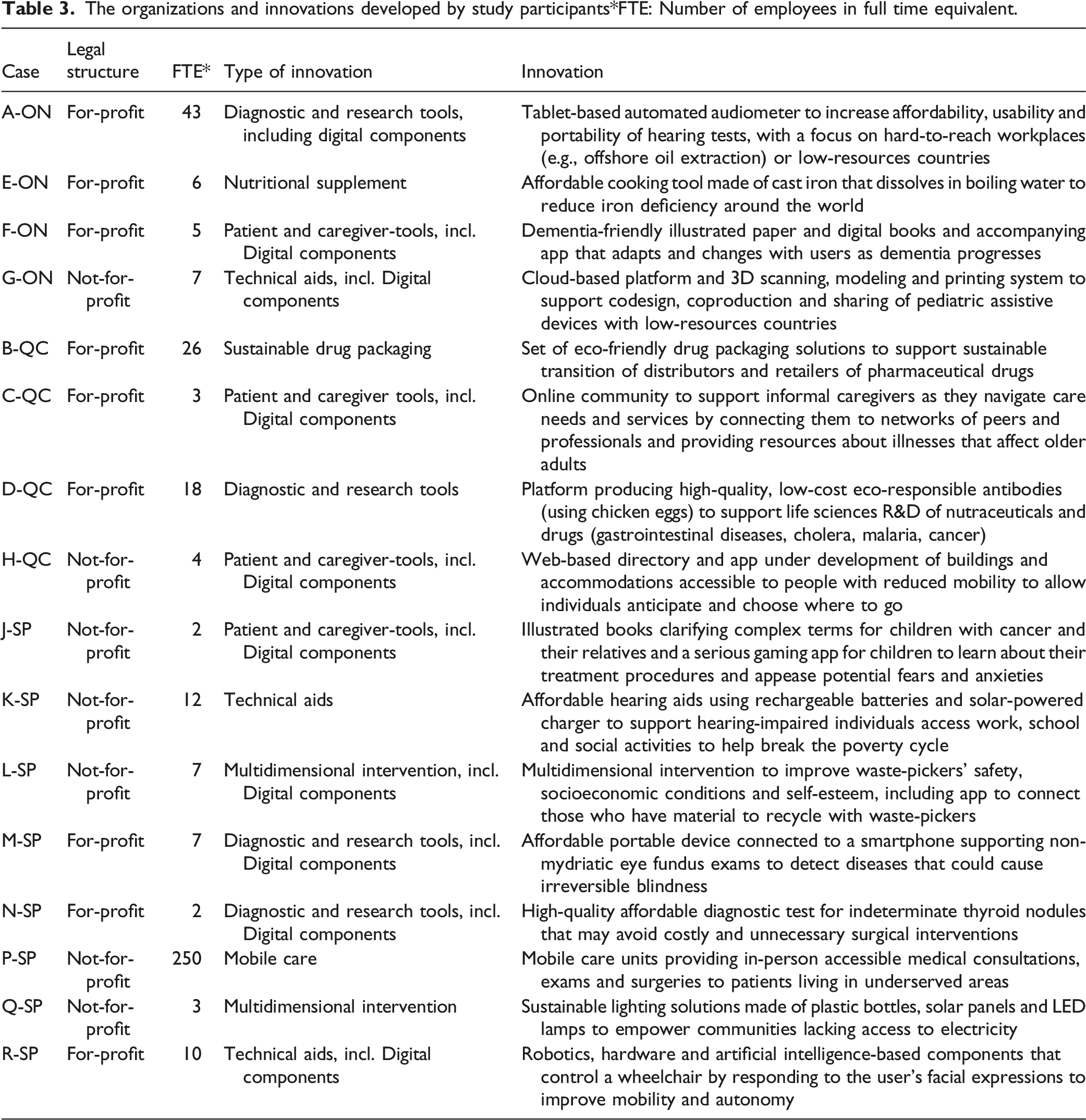
Table 3 provides an overview of the innovations developed by our interviewees as well as the legal structure and size of their organization. Following our internal diversification criteria, nine organizations have a for-profit structure and seven a not-for-profit one, and four innovations are diagnostic and research tools, four are patient- and/or caregiver-tools, three are technical aids, two are bottom-up multidimensional interventions, and the last three include a nutritional supplement, a set of sustainable drug packaging solutions and mobile care units. Up to ten innovations include digital components (e.g., apps and artificial intelligence-based solutions). How do innovators operationalize inclusiveness in their design processes? The organizations and innovations developed by study participants*FTE: Number of employees in full time equivalent.
Inclusiveness suggests that innovators should clarify which stakeholders contributed to the design of their solution, the methods deployed to gather their expectations and needs, and the way such inputs shaped the innovation. Our analysis indicates that stakeholder engagement mostly takes place at an early ideation stage and the methods employed are context-specific and include both formal and informal strategies (see Supplementary Material for examples of each thematic finding).
For G-ON’s leaders, bringing “a lot of players together upfront,” that is, before going to the “drawing board” was key (G-ON, 1). To develop their 3D-printed prosthetics for children living in Low- and Middle-Income Countries (LMICs), they worked closely with clinicians and “had conversations” with prosthetic wearers and “some of the payors.” To develop its thyroid cancer test, N-SP founder relied on his partnership with a hospital where he could “talk to the doctor, the nurse, the patient’s family.” He would ask “‘What’s the problem here?’, ‘Where does this sample go?’, ‘How long before the results?’” (N-SP, 1). By “seeing what was going on,” he could optimize the solution by using the sample already collected, thereby avoiding a second biopsy.
The founder of H-QC, which developed a digital platform to inform people with reduced mobility about the accessibility of public buildings, organized brainstorming sessions with ten community organizations because they “know more about user needs then herself” (H-QC, 1). The design process of K-SP’s low-cost pediatric hearing aids using a solar battery charger started in Botswana with hearing-impaired adolescents and young engineers. Because only users can articulate their problems clearly and find appropriate solutions,” the founder “wrote their hopes and dreams into a business plan, raised the money and told them ‘now go invent it’” (K-SP, 1).
Interviewees stressed the power relations and “hierarchy” (J-SP, 1) that prevail in healthcare systems and make inclusive design processes challenging. D-QC developed different products using chicken egg yolk (IgY) antibodies, ranging from nutraceuticals to antibacterial products. When working on a solution for Clostridium difficile bacteria, the co-founders discussed with infectious disease medical specialists and realized that “replacing antibiotics would be very difficult” because of their conservative clinical approach. Though “it’s sad to say,” they “don’t need to talk to patients” but to know “what causes the disease” (D-QC, 1). As vividly explained by C-QC’s founder, innovators who wish to ask vulnerable patients and their caregivers to identify design priorities must be well-prepared: if you give someone who’s drowning a baton or you give them a tennis racket, they’re going to grab it regardless. And when they’re drowning and [you’re asking] ‘is the tennis racket more valuable to you than the baton?’ it’s kind of asking a bad leading question (C-QC, 1).
For J-SP, communicating with children and their parents about pediatric cancer diagnostic procedures and treatments is part and parcel of its innovation, which consists in providing free illustrated books made with the help of children: “The kids were like, ‘Yeah, I know what an operating room is but I’m afraid,’ so let’s explain to the kids what an operating room is” (J-SP, 1). Such a codesign process requires “a lot of work” but makes “the material so persuasive” (J-SP, 1).
Overall, at an early ideation stage, innovators use different stakeholder engagement methods, ranging from informal discussions to structured group processes. The intensity and scope of these methods vary according to the purposes of the innovation but also depend upon innovators’ ability to access and interact with health and social care practitioners. What influences the responsiveness of innovators’ solutions to system-level challenges?
Responsiveness stresses the importance of providing dynamic, timely solutions to system-level challenges such as demographic and epidemiologic shifts, human resources hurdles, or gaps in service delivery, knowledge, and governance. Our data indicates that innovators may struggle with the positioning of their solution within a system they often describe as intricate, but all identified specific system-level benefits.
Aligned with contemporary demographic shifts in Canada, C-QC’s online platform was created to provide informal caregivers with support and resources to address older adults’ needs: “if you’re not a caregiver now, there’s a good chance that you might be a caregiver in the future” and “everybody’s caregiving capacity” will have to be consolidated (C-QC, 1). Relying on a portable device connected to a smartphone to perform non-mydriatic eye fundus exams, M-SP responded to Brazilian epidemiological shifts, where diabetes “has increased 60% in the last ten years,” affecting “almost 10% of the population” (M-SP, 1). The co-founder underscored the “great opportunity” they had by working with a large hospital that clarified what the “demand was” and how patients at risk of retinopathy from more than a dozen cities had to travel to access diagnostic services (M-SP, 1). Generating “a bit of an earthquake” in São Paulo, the mobile care units of P-SP were located where they could bridge key service delivery gaps by providing “a large volume of care” through an innovative care delivery model (P-SP, 1).
Factors limiting innovators’ ability to provide responsive system-level solutions had to do with how public services are organized and funded. H-QC could hardly operate a viable business because she could not charge for services that are, in principle, under the responsibility of Quebec’s provincial government, though “nothing has been done” since 1978 (H-QC, 1). F-ON, which produces printed and digital recreational books for older adults living with dementia, was “trying to intertwine more with the current health system” in Ontario but had not yet succeeded. However, providing personal support workers with “a tool that’s easy to use” for reading a 20-minute story with the patient generates “good social outcomes” and represents “a better use of [staff] time for the health system” (F-ON, 1).
To summarize, though innovators seek to address system-level challenges, their ability to do so is influenced by how health systems are governed as well as their receptiveness to novel solutions. How do innovators consider the level and intensity of care required by their innovation?
According to the subsidiarity principle, the most decentralized unit in the health system should be mobilized to provide care when it is possible to do so effectively and safely. Our analyses indicate three ways in which innovators envisaged the level and intensity of care required by their solution.
First, they sought to mitigate staff shortages and reduce barriers to specialized care. A-ON and G-ON, respectively, took into consideration the lack of trained audiologists and prosthetists in rural, remote, or resource-constrained areas to develop their solutions. To improve patient access to care in hard-to-reach or underserved communities, P-SP’s mobile clinics offer mammography, endoscopy, and colonoscopy exams as well as dedicated spaces for minor surgeries (P-SP, 1). By taking a picture in a primary care facility enabling an ophthalmologist in an urban center to produce its clinical report remotely, M-SP’s eye fundus exam reduces obstacles in the patient care pathway (M-SP, 1, follow-up).
Second, innovators sought to strengthen the capacity of general practitioners and community care providers to locally attend to their patients’ needs. The motivation to develop A-ON’s tablet-based hearing test “was a problem encountered” in tertiary care practice where up to “90% of patients who consult a medical specialist” have normal results: Hearing loss is affecting 60% of people over age 75. And yet, the family doctor doesn’t deal with it. […] because they don’t have the equipment. […] the value of [our solution] for primary care workers is that it provides inexpensive and simple technology […] enabling them to provide complete care (A-ON, 1).
Third, innovators sought to increase the autonomy of patients and informal caregivers. F-ON’s digital books include reading level adjustments and automatic page turning as well as a “backend strategy” for relatives to receive notifications about the stories a loved one has read because “it’s a big problem when you’re not there, you’re worrying” (F-ON, 1). Lastly, K-SP’s mission also includes “generating decent jobs” for young deaf people who are recruited to work in the manufacture and trained in “micro welding, electronics, basic electronics” (K-SP, 2).
To summarize, innovators consider the level and intensity of care required when developing their solution, a process wherein gaps in health and social care services can be turned into opportunities to innovate.
Discussion
Contribution of our study
Though healthcare managers face persistent problems raised by health innovations that poorly meet the needs of patients and caregivers or neglect the context in which care is delivered, including clinical workflows and patient pathways (Kajamaa and Schulz, 2018), their role in harnessing innovation towards the challenges of health systems remains underexplored. Our study contributes to bridge this gap by providing novel insights for research and practice.
Firstly, we found that innovators set in place inclusive design processes at the ideation stage and this was facilitated by health and social care managers. This finding complements the study of Banda et al. (2018) who observed that regenerative medicine innovators were deferring “healthcare adoption” issues “further down the road.” For instance, our interviewees relied on formal engagement methods (e.g., advisory committees and bottom-up processes), informal methods (e.g., conversations and onsite visits), or a combination of both. These processes were context-specific, that is, conditioned by the purposes of their innovation and by the stakeholders they had access to, and with whom they were able to interact. This is compatible with studies indicating that innovation depends upon the quality and thoroughness of the interactions between innovators, health and social care practitioners, and healthcare managers (Martin et al., 2012). Though inclusiveness is aligned with the growing importance attached to health services co-creation, Busch-Casler et al. (2020) found that “lower level employees are often left out” of innovation processes at an early stage and this may be due to “top-down” governance. Likewise, our study highlights that the diversity and scope of stakeholder engagement is modulated by power relations affecting how innovators may have access to managers, providers, patients and their caregivers.
Secondly, though all the health innovators we interviewed articulated contextualized system-level challenges, our findings showed the difficulties they encountered when seeking to interface their solution with health and social care systems. What is understood and managed as falling within or outside public health systems (e.g., aging, socioeconomic vulnerabilities, informal caregiving, and resilient communities) (Barr et al., 2003) may hinder sustainable health system-oriented innovation where the population health, superior care and fair service provision “regardless of age, group identity, or place” should prevail (Fineberg, 2012). Because our sample was comprised of innovators operating both not-for-profits and for-profits, our findings also highlighted how healthcare management receptiveness to diverse forms of entrepreneurship (Santos et al., 2015; Giacomelli et al., 2019) could help to “think outside the health system box” (Busch-Casler et al., 2020).
Thirdly, health innovators considered the likely impacts of their solution on human resources, service delivery, and patient access to care. Both Canadian and Brazilian innovators were conscious of the specific challenges patients living in rural, remote or resource-constrained neighborhoods, and communities face. As observed by Alrabie (2020), the “inherently small patient populations found in rural areas” raise unique challenges for healthcare managers who must consider the breadth of services to be offered as well as varying geographical constraints. Several of our interviewees turned such obstacles into opportunities to innovate, bringing support to the notion that increased collaboration with local practitioners could help orchestrate complementary resources for patients living outside well-serviced areas (Alrabie, 2020).
Overall, our study shows how innovations can be purposefully designed to contribute to health system sustainability and provide novel empirical insights on how healthcare managers can promote and organize collaborative processes that harness innovation towards more sustainable health systems.
Implications for healthcare managers
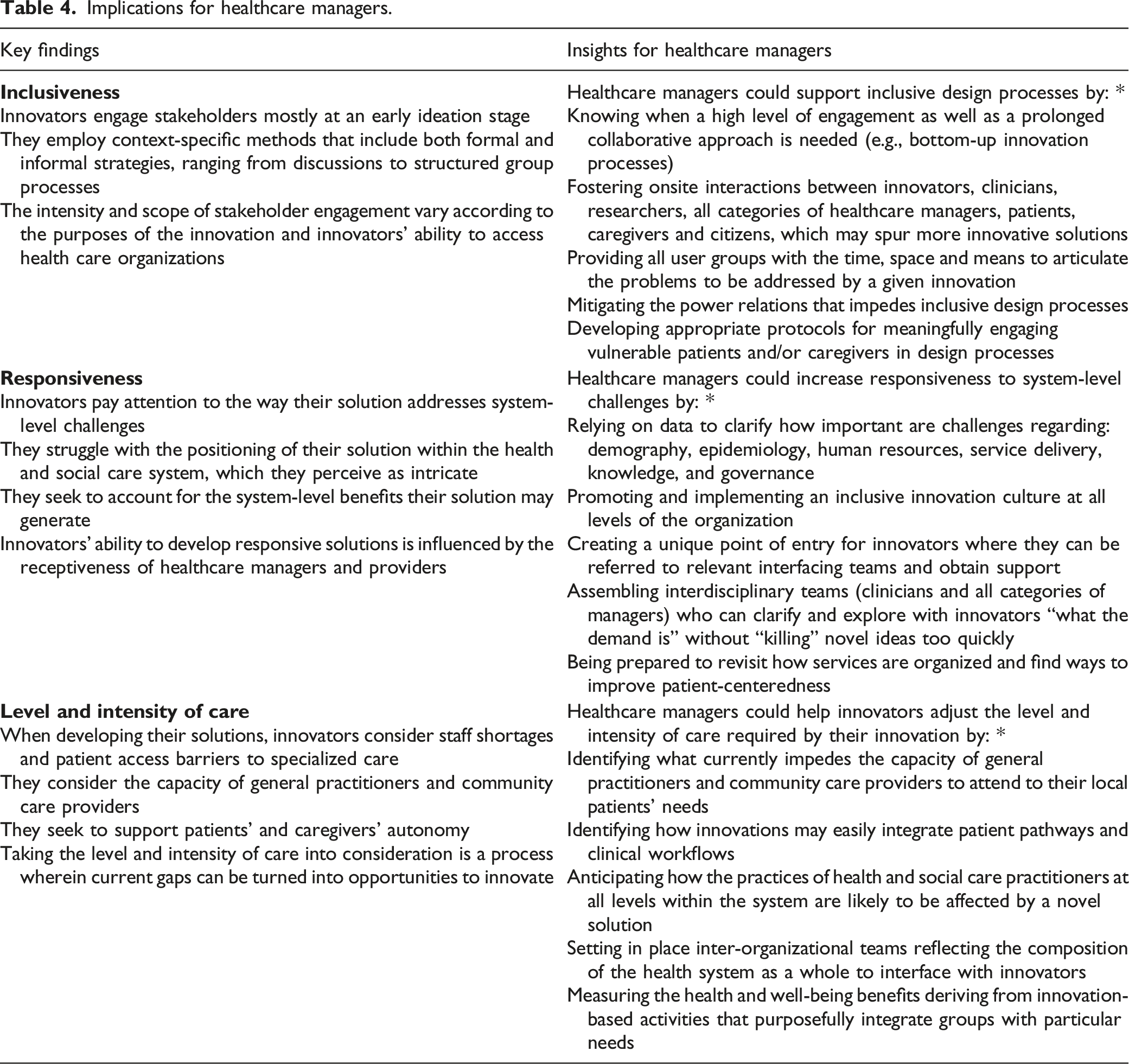
Implications for healthcare managers.
Our findings showed that the practical needs and problems that are brought to innovators’ attention depend upon who contributes to the design process, which in turn influences “where” in the health system the solution will be used and by whom. Interestingly, compared to frontline employees, physicians and top-level managers are more likely to see innovation as part of their job and career development goals (Busch-Casler et al., 2020). If healthcare managers wish to support patients’ and caregivers’ autonomy and consolidate primary care through innovation, they will have to set in place innovation-centered structures and processes that counter-balance established specialized care-centered dynamics (Lehoux et al., 2018).
Academic teaching centers play a key role in health innovation because of their expertise, skills and active involvement in clinical research (Lega et al., 2017; Storey et al., 2015). Yet, as our interviewees underscored, a hierarchical governance and physician-centered culture limit their capacity to engage a diversified set of innovation stakeholders (Busch-Casler et al., 2020). To reduce such obstacles, healthcare managers could promote and implement an inclusive innovation culture at all levels of the organization. A unique point of entry for innovators should be created so they can be swiftly referred to a specific interdisciplinary team that would be mandated and equipped to contribute to the innovation process (e.g., hosting onsite visits, organizing ideation activities, articulating problems, engaging vulnerable patients and caregivers). Such teams should reflect the health and social care system as a whole, foster inter-sectoral collaboration and create a shared commitment towards community and primary care innovation (Alrabie, 2020). It is also important to clarify “what the demand is” while avoiding to “kill” novel ideas too early. The task for RIH-oriented healthcare managers is thus to provide their teams with the tools and skills needed to revisit how services are organized and be prepared to bring changes. The diversity of the innovations included in our case study empirically shows that there is “a lot of untapped potential” for innovation in and around health and social care organizations (Busch-Casler et al., 2020).
Limitations of the study and conclusion
Our case sampling strategy led us to recruit small- and medium-sized organizations already engaged into the production of responsible health innovations and emerging from regions where health systems are publicly funded. The views and practices we reported are thus not transferable to a broader set of health innovators (e.g., growth-driven start-ups, large multinational companies) or who mainly interact with privately funded health systems. Though a greater number of organizations in Ontario declined our invitation, the internal validity of our findings was consolidated by having all team members cross-checking the relationship between the data associated to each case (variations) and our interpretations for the sample as a whole (commonalities). This process led us to provide conceptually consistent and empirically robust answers to our three research questions.
In several countries around the world, health inequalities persist and the sustainability of their health system is at stake (Roncarolo et al., 2017). By recognizing that healthcare managers can influence innovators’ decisions as well as innovation development processes, RIH provides them with a novel lens to look at the value different innovations may bring to health systems and it opens up new managerial avenues to better harness innovation towards sustainable health systems (Abrishami and Repping, 2019; Peine, 2019; Stahl, 2019).
Supplemental Material
sj-pdf-1-hsm-10.1177_09514848211048606 – Supplemental Material for Responsible innovation in health and health system sustainability: Insights from health innovators’ views and practices
Supplemental Material, sj-pdf-1-hsm-10.1177_09514848211048606 for Responsible innovation in health and health system sustainability: Insights from health innovators’ views and practices by Pascale Lehoux, Hudson P Silva, Robson Rocha de Oliveira, Renata P Sabio and Kathy Malas in Health Services Management Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research leading to this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.