
Abstract
The study investigates whether sick leave for the unemployed is used to address problems of labour market integration – a process that can theoretically be conceptualised as the medicalisation of unemployment. Estimating a multilevel logistic regression model on a sample of N = 20,196 individuals from the German panel study Labour Market and Social Security (PASS) reveals that, on average, 18% of the unemployed are on sick leave due to poor health. However, given a comparable state of health, the probability increases for men, older individuals and those with lower educational levels. These findings are crucial as they reveal a dual role of sick leave in a context with limited access to disability pensions: as a protective measure for sick, unemployed individuals and as medicalisation of unemployment by excluding those who face non-medical barriers to labour market integration.
Keywords
Introduction
Social science research has long been interested in how boundaries between unemployment and sickness or disability are constructed (Stone, 1984). However, existing research examines such processes and their social policy implications exclusively in the context of disability pensions. In the economic literature, for example, the concept of hidden unemployment describes the use of disability pensions to deal with limited labour demand beyond the needs arising from severe impairments and health limitations (e.g. Beatty and Fothergill, 2002; Koning and van Vuuren, 2010; Westerhout, 2001). Sociological perspectives have instead employed medicalisation theory (Conrad, 2008) to describe how disability categories are constructed in different welfare states and to investigate how knowledge and power structures are linked to these construction processes at different societal or institutional levels (e.g. Buffel et al., 2017; Holmqvist, 2009).
This article examines the institutional categorisation of sickness in the context of unemployment, by analysing who is granted sick leave for the unemployed in the German minimum income scheme. Drawing on medicalisation theory, it argues that the medicalisation of unemployment is detectable if non-health-related barriers to labour market integration of unemployed individuals who share the same health status are associated with an increase in granting sick leave over time. While existing research provided valuable insights into the medicalisation of unemployment through disability pension schemes (e.g., Holmqvist, 2009; O’Brien, 2013; Stone, 1984; Wong, 2016), sick leave for the unemployed received little attention. However, this institutional category may be crucial given the reform pathways of many industrialised countries in recent decades: following the recommendations of international organisations such as the OECD (2010), many countries restricted access to (permanent) disability benefit schemes (van Kersbergen and Hemerijck, 2012) and instead sought to integrate more people into the labour market, focusing especially on those with health impairments (Duell et al., 2016). The result of these changes is that more people overall and especially those who are more difficult to integrate end up or remain in general unemployment and minimum income benefit schemes (Hollederer, 2009). These schemes were also restructured in recent decades to pressure the unemployed to overcome their need for assistance as quickly as possible (Clasen and Clegg, 2007; Dwyer, 2008). Given that unemployed people in different types of welfare states have worse health than employed people (Bambra and Eikemo, 2009), and about 14% report a disability (OECD, 2010), the question of how to deal with sick or disabled unemployed persons in these schemes remains high on the political agenda (European Network of Public Employment Services, 2020).
In this context, the article explores whether granting sick leave to unemployed individuals serves not only as a strategy to address the growing number of sick individuals in the German minimum income scheme but also as a response to obstacles hindering successful labour market integration. These barriers, and consequently the potential medicalisation of unemployment, can manifest at various levels (Gangl, 2003). At the individual level, characteristics like advanced age or lower education levels, which can impede finding employment, may contribute to the medicalisation of unemployment. Structural medicalisation of unemployment could occur if, for example, employment opportunities are restricted in regions with high unemployment rates. This could make it more difficult for employment agencies to match suitable vacancies with unemployed persons, leading to higher rates of unemployed being granted sick leave.
Existing qualitative studies interviewing unemployed persons and specialist advisors of the Federal Employment Agency or studying administrative documents provided evidence of such medicalisation processes (e.g. Hansen et al., 2014; Holmqvist, 2009) occurring in Germany as well (Dornette et al., 2008; Kupka et al., 2017). These studies indicate that intentional actions, both by unemployed individuals and by specialist advisors, as well as unintentional effects of institutional rules and organisational practices, can lead to both individual and structural medicalisation. This article goes beyond these findings by investigating whether such medicalisation processes are observable using representative data from the population of minimum income beneficiaries. The analysis therefore utilises longitudinal data from a sample provided by the Federal Employment Agency, encompassing N = 20,196 repeated measures over 11 waves (2008–2019). It specifies a three-level multilevel model, integrating time at level 1, individual health variables and variables related to labour market integration at level 2, as well as the district unemployment rate at level 3. The results therefore broaden our understanding of how sickness-related social policy categories influence the efforts of welfare states to integrate all non-employed individuals into the labour market. In addition, the study extends the existing literature on the medicalisation of unemployment, which has primarily focused on liberal and social-democratic welfare regimes, by examining the processes within the context of Germany as a case representing a conservative welfare state.
The article proceeds as follows: First, it explains why disability is a socially constructed category and how this connects to framing unemployment through a medical lens. It argues that viewing unemployment as a medical problem not only responds to an existing need but also generates one, particularly for individuals ineligible for disability pensions. The article then describes how the assumed medicalisation of unemployment can be empirically detected in the German minimum benefit system and postulates respective hypotheses. The article proceeds by describing the employed data, constructed analysis sample, as well as the details of the specification of the multilevel model Then, the results of the analyses are reported. Finally, the concluding section evaluates the findings and explores their implications for sociological theory and labour market-related social policies.
Theoretical background
How welfare states deal with unemployed individuals who have health limitations is investigated primarily through studies on disability or incapacity pensions. The literature examined the temporal and geographic variations in the boundaries between unemployment and disability status (Beatty and Fothergill, 2015; O’Brien, 2015b) to understand how both economic and institutional factors determine who is considered disabled and who is not (Barnes, 2012; Jenkins, 1991; O’Brien, 2015a). While the category of being disabled changes with reforms of eligibility criteria (e.g. Autor and Duggan, 2003; Blomgren et al., 2021; Bratsberg et al., 2010; Koning and van Vuuren, 2010), the regulations of social policy programs (Angelini et al., 2012) provide the context for social interactions and practices in which unemployed persons, physicians and administrators construct the disability status and transform individuals into cases (Zola, 2017). These results illustrate that the disability status is socially constructed and not an easy translation of symptoms and bodily changes or a mere expression of an individual’s objective health status. Equally important in this context is the fact that ideas and interests influence these social constructions on the societal level. Clasen and Clegg (2007) for instance argued that ‘politicians have often changed directives and guidance they give to these professionals in an attempt to use the lever of category definition to impact on inflows into benefit receipt’ (p. 173). Resulting regulations therefore provide the context in which administrative staff and the unemployed communicate, (inter)act and produce the status of disability (Garthwaite, 2015; Hansen et al., 2014).
Up to this point, these regulations address a need for necessary social security for individuals who are unemployed and ill. If, however, such a category is granted to deal with difficulties of labour market integration other than health limitations, these processes can be interpreted as a medicalisation of unemployment (Conrad and Schneider, 1992; Holmqvist, 2010). The underlying theory of medicalisation is a social constructionist approach, which aims to explain why phenomena are defined and treated as medical problems (Conrad, 2008; Conrad and Barker, 2010). Medicalisation processes can be observed for many social phenomena, such as deviant behaviour (e.g. alcoholism), mood (e.g. depression), or life events (e.g. childbirth). In the course of welfare state reform towards activation and social investment, scholars have become increasingly interested in the medicalisation of unemployment and poverty (Holmqvist, 2009; Schram, 2000). Empirically, this research also focuses on disability pension receipt or the utilisation of health services. A key finding is that unemployed persons use significantly more professional care and antidepressants than employed individuals with a similar mental health status (Buffel et al., 2015a). Moreover, the medicalisation of unemployment has been related to macro-economic conditions (Buffel et al., 2015b) and welfare state institutions in several countries (Buffel et al., 2017; Hansen et al., 2014; Pulkingham and Fuller, 2012; Wong, 2016).
However, this literature does not address how the minimum income systems deals with unemployed persons who are also ill but do not qualify for disability pensions. This article therefore investigates how the German institutional category of granted sick leave for the unemployed is used for this group. The German case is interesting in this respect because in an international comparison of 36 countries Germany has a tight compliance regime with the highest score (4.5 on a 5-point scale) for ‘Job search and availability’ (Venn, 2012). These compliance measures foster an expectation from welfare recipients to overcome their unemployment as quickly as possible, shaping the responsibility for the self (Giddens, 1991; Riach and Loretto, 2009) to get out of unemployment and thus minimum income benefit receipt. This expectation might be difficult to uphold for unemployed persons with health limitations. Nevertheless, granting a temporary release from these obligations responds to a need within the minimum income system. This is particularly important as the route to disability benefits is closed for many unemployed persons in the German system. The prerequisite is that they have paid at least three years of compulsory contributions to the pension insurance scheme in the last five years prior to the onset of the reduction in earning capacity. The first expectation is therefore that the category of granted sick leave for the unemployed responds to an unmet need of ill health.
H1: Individuals with illnesses, health limitations and/or disabilities have higher odds of being granted sick leave for the unemployed (need hypothesis).
At the same time, the presence of such an institutional category holds the potential to medicalise unemployment (Holmqvist, 2009; Ford et al., 2000); thus, not only addressing a need, but also creating an additional need. For instance, Karlsson et al. (2008) demonstrated that certain socio-demographic factors such as advanced age, low income, unemployment, or prior sick leave significantly predict the likelihood of receiving disability pensions. Building on this notion, our study postulates that if there are individual barriers (e.g. limited education, advanced age, caregiving responsibilities) or structural obstacles (e.g. high district unemployment rate) hindering labour market integration, certifying physicians and/or Federal Employment Agency advisors might incline towards employing this category to grant sick leave for the unemployed to accommodate their diminished capabilities of finding or taking up a job. Existing evidence from Germany supports this assertion. Boockmann et al. (2010), for instance, showed that, in general, sick unemployed receive fewer appointments or integration measures from Federal Employment Agency advisors. Moreover, qualitative research highlights that older unemployed individuals, who have been granted sick leave often feel ill-equipped to meet job requirements, encounter difficulties in accessing job opportunities and lack support from the Federal Employment Agency (Wuebbeke, 2011).
Furthermore, once administrative classifications are established, there tends to be an increase in their utilisation as various actors in the system become accustomed to them. This usage is not only observed among Federal Employment Agency advisors, who can concentrate on individuals with higher prospects for labour market integration (Kupka et al., 2017), but also among individuals to whom the status is granted. For instance, Mather et al. (2019) found that being granted sick leave status raises the risk of recurrent sick leave within two years, irrespective of individual circumstances. The authors concluded that inactivity exacerbates disease symptoms and negates the benefits of employment, such as a structured daily routine, social interactions with colleagues and having a meaningful task. Therefore, prolonged sick leave could set in motion a progression towards labour market marginalisation (Hultin et al., 2012), as individuals are unable to further accumulate the necessary skills and abilities demanded by the ever-evolving labour market, causing them to lag other job applicants, particularly those who are employed. Consequently, we expect that in the sample of minimum income recipients it will be difficult to revoke sick leave for the unemployed once it has been granted, as sickness may prevent individuals from persisting in the labour market. This is likely to explain, at least in part, the supposedly ever-increasing proportion of sick leave among the unemployed as a percentage of the total number of unemployed. As such, our second hypothesis is as follows:
H2: On average, the number of persons granted sick leave for the unemployed is increasing over time (trend hypothesis).
A precise differentiation of the cases in which an actual need is met by granting sick leave for the unemployed category and where unemployment is medicalised, therefore requires the consideration of additional individual and structural characteristics that may impact the granting of the status. Medicalisation should then be identifiable where additional barriers to successful labour market integration exist (Buffel et al., 2015a). Generally, women and older and lower-educated individuals are overrepresented among the non-employed (Fernandez et al., 2020) because, in addition to health limitations, a low level of education, low job-related qualifications, lack of experience, care responsibilities or a combination of these factors are major obstacles to entering the workforce. In addition, unpaid care responsibilities in particular create an interrupted employment biography, which is an obstacle to finding a job, even though women are predominantly willing to work (Ferrant et al., 2014). Moreover, there is evidence that employers discriminate against women (England, 2005) as care responsibilities are perceived as barriers leading to lower productivity and more frequent sick days, which is subsumed under the term of ‘family responsibility discrimination’ (Williams and Bornstein, 2008). Young individuals are struggling to enter the labour market if they left the educational system without obtaining a degree, have not acquired skills needed for the specific job, or employers perceive them to not have experience (OECD, 2015). Older persons face multiple barriers to reemployment and discrimination by employers (Wanberg et al., 2016), often stereotyped as poorer performers, less motivated, less willing to change or participate in training measures and less healthy (Ng and Feldman, 2012). Finally, the longer someone is unemployed, the lower is the chance of reemployment. The main reason lies in the deterioration of human capital, self-esteem and health, as well as the resignation that is associated with periods of unemployment (Machin and Manning, 1986; Paul and Moser, 2009). These considerations lead to the third hypothesis:
H3a: Controlling for health status, young persons, persons near the standard retirement age, with a low level of education, or with a longer unemployment history have higher odds of being granted sick leave for the unemployed (individual medicalisation hypothesis).
Finally, barriers to labour market integration are not only found on the individual level, but also on the structural level (Gangl, 2003). One important limitation for labour market integration poses the district unemployment rate. If these are high (Duell et al., 2016), integration for all unemployed individuals, but even more so for those with additional individual barriers, is difficult. Therefore, in regions with more tight labour markets, sick leave for the unemployed might be granted more frequently by Federal Employment Agency advisors to focus on people with lesser reemployment barriers. Thus, the expectation is that given the same health status and characteristics of the individuals considered, a higher unemployment rate within the district might be associated with a higher likelihood to be granted sick leave for the unemployed:
H3b: Controlling for health status, the higher the unemployment rate in a district, the higher the odds of being granted sick leave for the unemployed (structural medicalisation hypothesis).
Data and methods
The article used data from the Panel Study ‘Labour Market and Social Security’ (PASS). 1 To analyse the dynamic as well as the effects of receipt of social benefits on the economic and social situation of affected households and individuals, PASS utilises two subsamples: a sample of households with at least one recipient of minimum income benefits drawn from the recipient registers of the Federal Employment Agency and a sample of the resident population in Germany in which low-status households are oversampled. In both samples, PASS surveys the same individuals annually, creating a longitudinal data set with repeated measures. The response rate, measured as the proportion of personal interviews in realised households, is 74.8% across the entire longitudinal survey (Berg et al., 2021). Both subsamples can be extrapolated to the respective target population using cross-sectional weights. The recipient sample is updated every year to include new entrants. It can be used to analyse access cohorts separately or to identify determinants of access to the minimum income system (Trappmann et al., 2013). To examine district differences, the original PASS data were linked to administrative data on annual unemployment rates. 2 The district units for the study are 154 Federal Employment Agency 3 districts, which are larger than administrative districts.
The analysis focused on the sample of the Federal Employment Agency and therefore excluded households without benefit recipients. Since no information on granted sick leave for the unemployed was available in the first wave of data collection in 2007, these observations were also excluded. After this, only those individuals who had at least two observations during the entire observation period were considered for the analysis sample to model a consistent time trend. 4 After preparation of the data, the analysis sample contained N = 20,196 unemployed individuals who met the inclusion criteria across PASS waves 2–13 (2008–2019). Sampling weights for longitudinal analyses were used according to the PASS User Guide (Bethmann et al., 2013; Trappmann et al., 2013) for descriptive analysis. A test proposed by Dumouchel and Duncan (1983) found no significant difference (F10, 8 = 1.65, p = 0.2436) between weighted and unweighted estimates in the three-level model, which is why the latter are reported in the multivariate analysis.
Measured variables
The binary dependent variable indicated whether a person was unemployed (0) or unemployed and granted sick leave for the unemployed (1). Before the status was granted, individuals were, on average, unemployed for 2.64 (SD: 0.06) years. However, individuals on granted sick leave for the unemployed had at least the possibility to enter another status again. After an average of 2.25 years of observation (SD: 0.04), 42.59% of observed individuals transitioned back to regular unemployment without sick leave. Apparently, the status of sick leave for unemployed had been withdrawn, so individuals were again considered unemployed and available to the regular labour market. Nevertheless, it is also possible that the status sick leave for unemployed was granted again by advisors. Of those who had previously received the status of sick leave for unemployed, 17.85% were granted the status at least once more during the observation period. To integrate the repeated measures of different timepoints in the model, a categorical wave variable (0–11) reflected the specific year participants were interviewed (Table 1).
Descriptive statistics for the respondent characteristics.
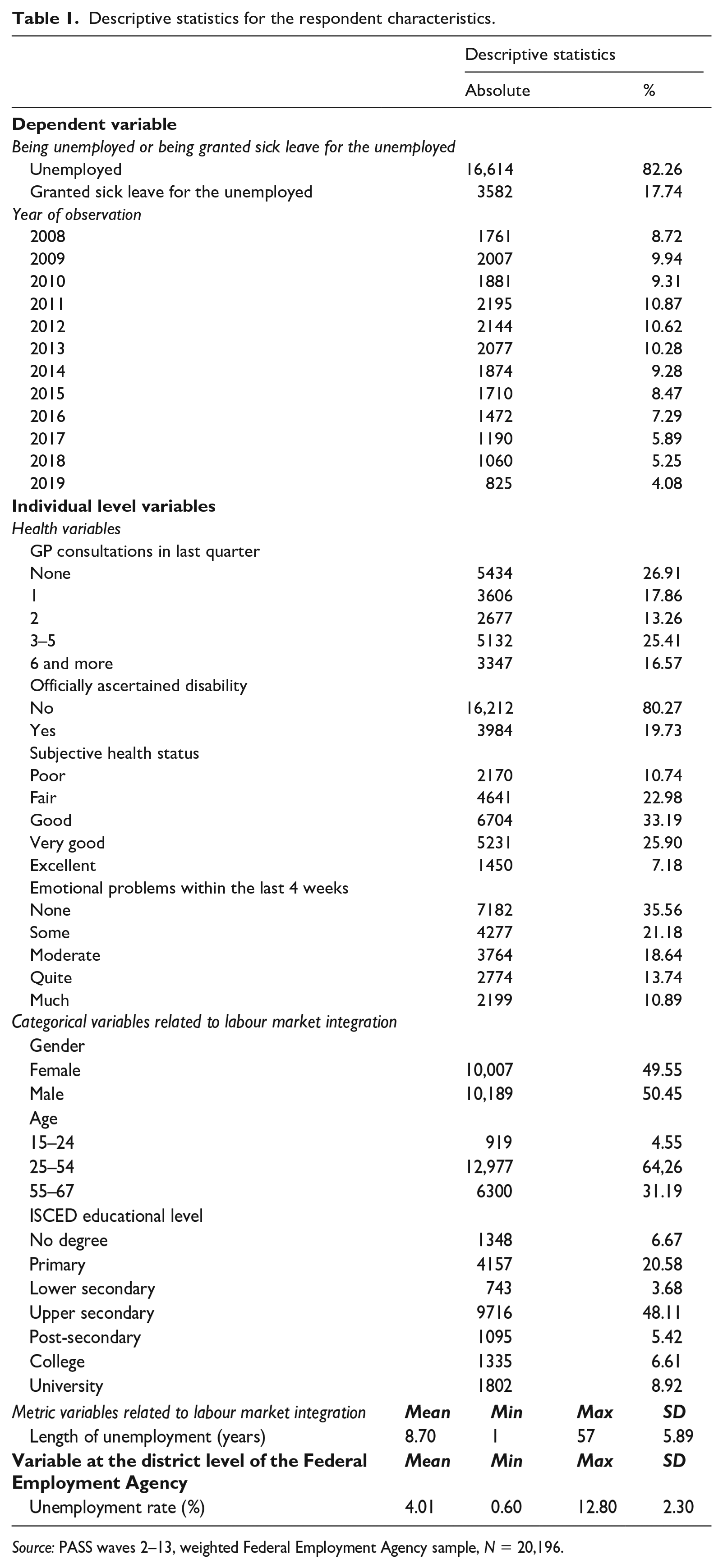
Source: PASS waves 2–13, weighted Federal Employment Agency sample, N = 20,196.
Individual health status was operationalised using four self-assessed indicators: (1) the number of consultations with a general practitioner in the last quarter (none up to six or more consultations); (2) whether respondents had an officially ascertained disability (yes/no); (3) subjective health (poor/fair/good/very good/excellent); and (4) the intensity of emotional problems during the last four weeks (none/some/moderate/quite/much).
To test the individual medicalisation hypotheses, variables for individual characteristics that may impede labour market integration were integrated. Age was included categorically (15–24, 25–54, 55–67), since integration measures of the Federal Employment Agency differ between these age groups: for younger individuals (15–24 years old), the Federal Employment Agency must attempt to facilitate integration into employment suitable for training as soon as an application for benefits is filed. To date, under-25s are also sanctioned more severely in the event of non-compliance (Boockmann et al., 2014), while older persons (55–67) are generally treated more leniently (Wuebbeke, 2011). In addition, the model took gender (female/male), the ISCED educational level (no degree/primary/lower secondary/upper secondary/post-secondary/college/university education) and the length of unemployment at the time of observation into account. Finally, the unemployment rate (in percent) within the Federal Employment Agency district was used as a third-level variable to test the structural medicalisation hypothesis.
Analytical strategy
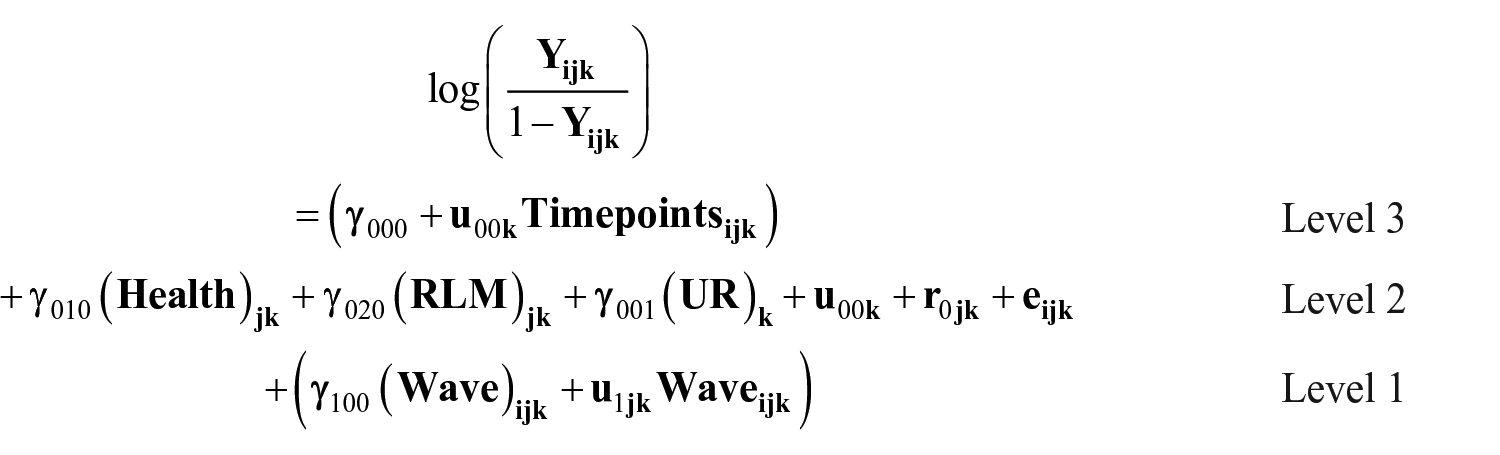
The variables described above were available at different hierarchical levels, which potentially influence each other. In general, the longitudinal model analysed the same people at 12 points in time over a period from 2008 to 2019 on the base level. On the second level, for each point in time – or in each observation wave – measurements on individual variables (e.g. educational level or health status) were available. Moreover, the individual measurements were bundled in the working districts on a third level to include possible influences resulting from differences between the respective districts in the model. The study therefore used a mixed multilevel logistic regression model accounting for the hierarchal data structure of repeated observations in timepoints (level 1) nested in variables related to labour market integration and individual health (level 2) nested in the working districts (level 3). Thus, a three-level model was specified in Stata 16 on the following general formula:


In a second step, the wave variable itself was added on level 1 and a random-intercept-random-slope-model (M1) with random slopes
6
and a corresponding error term (

Third, the contextual model (M2) integrated individual fixed predictors for health (
All models used an α = 0.05 for hypothesis testing and results are reported in odds ratios (ORs). In line with the recommendations made by Hox et al. (2018), model comparison is based on ICC (variance partition coefficient) for different levels, AIC and BIC values, as well as McKelvey & Zavoina-pseudo-R2 for random and fixed effects.
Results
Descriptive findings
First, descriptive results are briefly discussed. On average, 18% of the unemployed were on granted sick leave throughout the observation period. Over the years, the share of individuals on granted sick leave for the unemployed tripled from 9% in the first year of the survey to 34% in 2019 (Figure 1, Panel A). Moreover, granted sick leave for the unemployed was strongly related to health status; 57% of the individuals on granted sick leave for the unemployed rated their health as fair or poor compared to 28% in the group of unemployed respondents (Figure 1, Panel B).
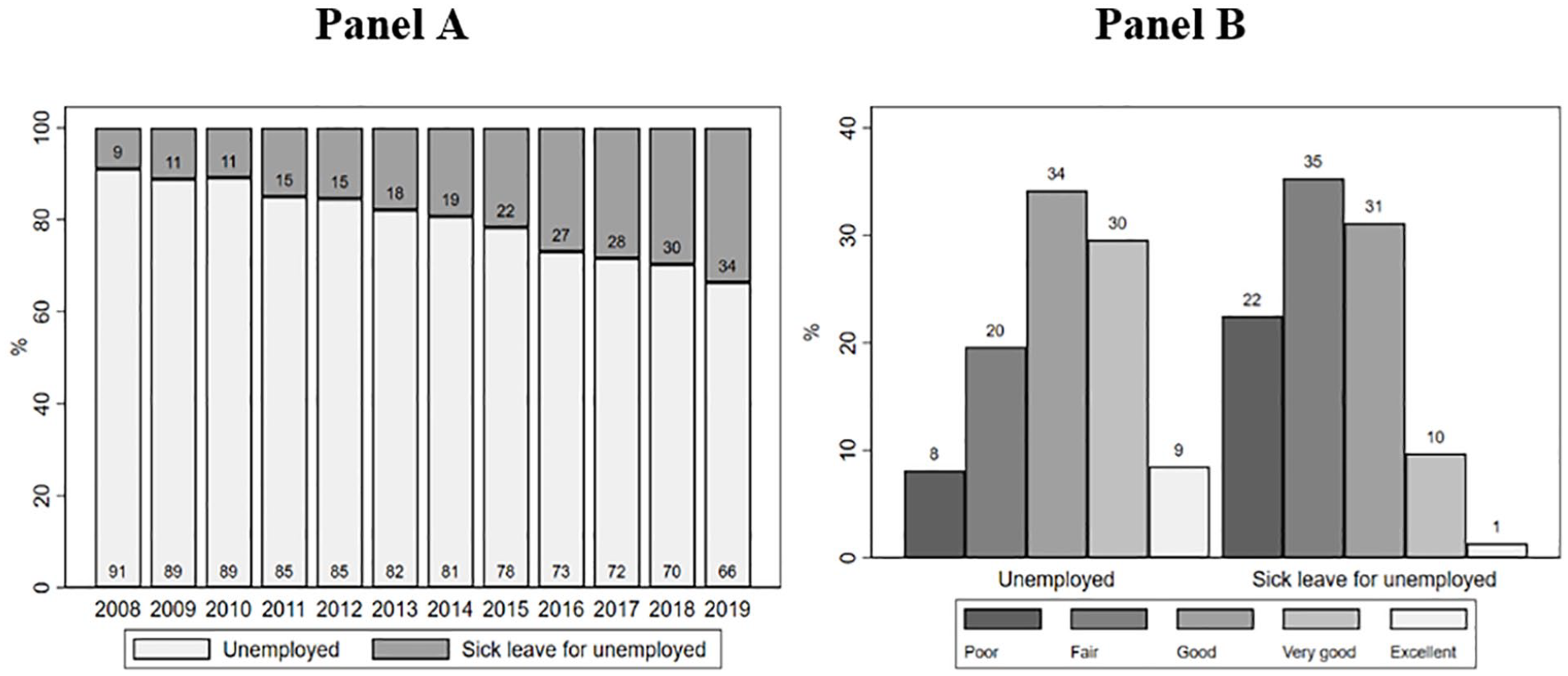
Proportion of individuals who are either unemployed or granted sick leave for the unemployed in the German minimum income system over time (Panel A) and by subjective health status (Panel B).
Multivariate findings
Table 2 shows the multivariate findings from the three-level logistic regression models. The variance decomposition of the random-intercept-only-model (M0) revealed that the district level explained 1.3% of the variance in granted sick leave for the unemployed, while the majority (66.5%) was explained by variance between individuals followed by variance over time (32.2%).
Multilevel mixed effects logistic regression models of the odds of being granted sick leave for the unemployed.
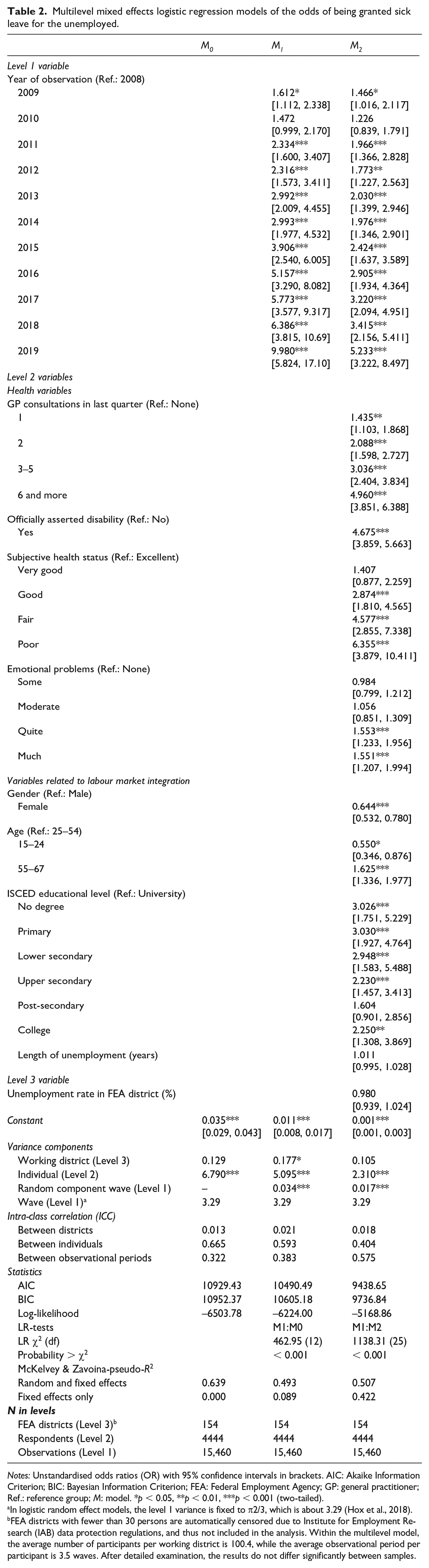
Notes: Unstandardised odds ratios (OR) with 95% confidence intervals in brackets. AIC: Akaike Information Criterion; BIC: Bayesian Information Criterion; FEA: Federal Employment Agency; GP: general practitioner; Ref.: reference group; M: model. *p < 0.05, **p < 0.01, ***p < 0.001 (two-tailed).aIn logistic random effect models, the level 1 variance is fixed to π2/3, which is about 3.29 (Hox et al., 2018).bFEA districts with fewer than 30 persons are automatically censored due to Institute for Employment Research (IAB) data protection regulations, and thus not included in the analysis. Within the multilevel model, the average number of participants per working district is 100.4, while the average observational period per participant is 3.5 waves. After detailed examination, the results do not differ significantly between samples.
M1 – the random-intercept-random-slope-model – provided the main effects for the wave variable. The random component variance for wave was significant with OR = 1.193 (CI: 1.010; 1.411), the McKelvey & Zavoina-pseudo-R2 for random and fixed effects combined decreased by 14.6 percentage points and the ICC between individuals decreased by 7.2 percentage points. Those findings along the significant likelihood-ratio (LR)-test (p < 0.001) between the random-intercept-only and the random-intercept-random-slope-model indicate that the total variance was partially explained by time. The increasing odds of the wave variables indicate that granted sick leave increased over the observation period (OR2009 = 1.612 to OR2019 = 9.980). Compared to the reference category (2008), the odds of being granted sick leave for the unemployed in 2019 were almost 10-fold.
The contextual model M2 included all explanatory variables on the individual level 2 as well as the Federal Employment Agency district level unemployment rate on level 3. The model fit statistics (AIC, BIC, LR-test with p < 0.001) indicated an improvement. In addition, the McKelvey & Zavoina-pseudo-R2 for only fixed effects increased by 33.3 percentage points, while the ICC on the individual level decreased by 18.9 percentage points, implying that the individual variables were able to explain a significant part of the total variance within the model. All health measures were significantly associated with being granted sick leave for the unemployed: The odds were higher the more consultations respondents report with a GP (OR1 = 1.435 to OR ⩾6 = 4.960), when having an official asserted disability (ORYes = 4.675), indicating a worse subjective health status (ORVery good = 1.407 to ORPoor = 6.355) or having more emotional problems (ORSome = 0.984 to ORMuch = 1.551).
After controlling for health-related measures, the odds of being granted sick leave for the unemployed were also associated with socio-demographic indicators that are relevant for labour market integration. The odds were lower for women (ORFemale = 0.644) than for men. Age also had a significant association, with higher odds of being granted sick leave for the unemployed for individuals aged 55 and older (OR55–67 = 1.625) compared with the reference group of 25–34 years. Young respondents (< 25) had lower odds to be on granted sick leave for the unemployed (OR15–24 = 0.550) in comparison with the reference category. In addition, the level of education is associated with being granted sick leave for the unemployed. Compared with a university degree, lower educational degrees (especially no degree, primary and lower secondary degree) had higher odds of being granted sick leave for the unemployed (ORNo degree = 3.026 to ORCollege degree = 2.250). The odds furthermore increased with each additional year of being unemployed (ORLength of unemployment = 1.011); however, the effect is not significant. Finally, the Federal Employment Agency district level unemployment rate on level 3 was not significantly related to the odds of being granted sick leave for the unemployed.
Discussion and conclusion
In recent decades, there has been a growing interest in understanding whether and how unemployment is medicalised to address individual or local difficulties in labour market integration or deal with existing gaps and ambivalences in social policy programmes (e.g. Buffel et al., 2017; O’Brien, 2013; Wong, 2016). This article seeks to extend this existing research by investigating with a quantitative longitudinal design, whether the granted sick leave is used to medicalise unemployed individuals in the context of the German minimum income scheme.
Sick leave exists in the minimum income scheme as a response to the inability of unemployed persons to look for work due to (temporary) sickness. As access to incapacity pensions is very restrictive in Germany, minimum income recipients on sick leave may also include a significant number of people with long-standing health limitations and disabilities. If the granted sick leave for the unemployed is used only for these sick individuals, it can be assumed that it covers the intended need. The results provide support for this need hypothesis (H1), as all of the four health measures were independently significantly associated with being granted sick leave for the unemployed. However, controlling for health status, being granted sick leave was also associated with other variables which suggest that medicalisation processes may also have been present. This confirms findings from other countries on disability pensions or similar benefits (e.g. Buffel et al., 2017; O’Brien, 2013; Wong 2016). In line with the trend hypothesis (H2), results show that the number of people being granted sick leave for the unemployed has increased significantly over time in the sample, suggesting that granting sick leave has become more important in this scheme. Moreover, certain socio-demographic groups are significantly more likely to be granted sick leave for the unemployed: men, older persons and persons with a low level of education. Except for men, these groups are known to face higher barriers to labour market integration for various reasons, including employer discrimination (e.g. Berger, 2009; Carlsson and Eriksson, 2019; Mooi-Reci and Ganzeboom, 2015). Thus, the individual medicalisation hypothesis (H3a) is supported, except for young people who were less likely to be granted sick leave. In contrast, the results were not consistent with the structural medicalisation hypothesis (H3b), as the district unemployment rate did not show an association with sick leave status and the overall district variation was rather small.
The data used in this analysis have limitations. First, health was operationalised via mainly subjective information provided by respondents, as no other variables are available within the sample. This can lead to unconscious bias as respondents misremember their health status (e.g. in the number of doctor visits) or deliberate bias because respondents do not want to jeopardise their granted sick leave for the unemployed status. Future analyses might integrate more objective measures of health, such as the 12-Item Short Form Survey (SF-12) as a measure of the Physical and Mental Component Summary scores (Jenkinson et al., 1997). Second, literature on the associations between unemployment and health proposes a strong negative causal effect (Paul and Moser, 2009), while becoming unemployed increases the probability of receiving disability benefits (Harkko et al., 2018; Støver et al., 2012) or, in the sample, being granted sick leave for the unemployment. Unemployment itself may therefore negatively affect health and the likelihood of being granted sick leave for the unemployed over time, a phenomenon usually subsumed under the term endogeneity (Semykina and Wooldridge, 2010). The standard modelling approach for data that might contain endogenous variables is to run a fixed effects regression model. However, this approach would out-control independent variables that are of central research interest and almost completely time-invariant (e.g. education). Bell and Jones (2015) argue in this context that instead of controlling-out context, one should model it. By integrating a random effect for the timepoints on level 3, the models separated the between and within effects associated with the timepoints, thus controlling for the specific context dependency. Finally, one could argue that with an ICC on level 3 ranging between 0.013 and 0.021, a more parsimonious multilevel architecture should be applied. However, Sommet and Morselli (2017) argue that even if the residuals are independent (which may explain a low ICC), this does not mean that variation in the effect of a lower-level variable is not present. Several researchers (Muthen and Satorra, 1995; Sommet and Morselli, 2017) suggest calculating the design effect (DEFF) in this situation, defined as ‘the ratio of the operating variance to the sampling variance if a simple random sample were conducted’ (Huang, 2018: 494). Calculating the DEFF supports the use of a multilevel approach, as DEFF values exceed the threshold of 2, indicating the importance of considering the clustering structure of the data. 8
Notwithstanding these limitations, the findings highlight the relevance of medicalisation theory in understanding the use of sickness-related categories in the context of unemployment. Who is sick and who is not, and how many persons are granted sick leave for the unemployed is the result of societal definitions, organisational routines and individual interactions. Certainly, health status plays a role in this assignment, but as our study shows, it does not determine it. There are very sick or disabled people who receive minimum income benefits and (must) actively look for work, and there are relatively healthy people on sick leave. More importantly, there are systematic effects of non-health factors that seem to be considered in this assignment process. At the individual level, these are gender, age and education. That older people are more likely to be medicalised and put on sickness-related benefits is in line with existing research (e.g. Beatty and Fothergill, 2013; O’Brien, 2013). This may be because sickness is taken more seriously at older ages, may be considered as less reversible or old age is itself seen as a form of disease (Fletcher, 2021). There are also alternative or supplementary explanations. Until 2007, the Federal Employment Agency did not require unemployed persons aged 58 and older to actively look for work due to their age. It seems possible that after age was no longer considered a justification for exemption, sick leave was used. However, existing research on this group suggests that a majority of the older unemployed want to work, but rather do not feel equipped to deal with job requirements, do not receive job opportunities or do not receive support from the Federal Employment Agency (Wuebbeke, 2011). Given the lower chances of re-integration of older unemployed people, granting them sick leave could also be a deliberate decision within employment agencies to focus on clients with higher chances (Kupka et al., 2017). Similarly, higher rates of granted sick leave for the unemployed were found for individuals with lower levels of education – another major barrier for labour market integration. However, length of unemployment was not associated with the receipt of sick leave. That men are more likely to be granted sick leave for the unemployed is surprising considering that women experience greater barriers to the labour market (Fernandez et al., 2020; Neumark et al., 2019). A potential reason could be that care responsibilities are another reason why the Federal Employment Agency may exempt persons from the obligation to actively look for work, which is more frequently applied to women. Future research should therefore examine the role of gender in this context. Pulkingham and Fuller (2012) have, for instance, shown that in Canada, where social policy reform has limited access to benefits for lone mothers on the grounds of caring responsibilities (in contrast to Germany), has led to a ‘medicalization of lone motherhood’.
In contrast to other research which has shown sickness-related benefits to be associated with unemployment rates (Buffel et al., 2015a; 2017), this analysis did not find support for structural medicalisation as district unemployment rates were not associated with granting sick leave. This is encouraging because it indicates that, unlike earlier analyses on disability pensions, granting sick leave does not seem to be used in a systematic way to deal with local labour market difficulties. However, it needs to be noted here that Germany experienced a strong labour market for most of the observation period. It is important that future research continues to investigate the presence of structural medicalisation considering the aging populations and declining levels of working-age populations in most advanced, industrialised nations.
Most importantly, this article has shown that a restrictive disability pension system may be accompanied by medicalisation in other benefit systems such as the minimum income scheme. This might be related to the inability of the system (until recently) to provide targeted services for older and sick, unemployed persons (Dornette et al., 2008; Kupka et al., 2017; Wuebbeke, 2011) despite the explicit goal of integrating this group into the labour market. Investigating medicalisation processes therefore remains important in understanding the complex, country-specific and historically dynamic construction of sickness as a legitimisation for unemployment.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Support Network for Interdisciplinary Social Policy Research (FIS) of the German Federal Ministry of Labour and Social Affairs (Grant Number: Ia4-12141-1115).