
Abstract
Union communication and framing are important for how union members, as well as how unions as organizations, are represented. In the context of declining union density and therefore fewer direct union members, unions’ daily communication material on social media may be one of the most common interactions people have with unions. This case study focuses on United Nurses of Alberta, the union for most registered nurses in Alberta, Canada, where unionization rates are among the lowest in Canada. This case study shows how United Nurses of Alberta uses two collective action frames, nurses-as-distinct and nurses-as-advocates, in their daily communication to members and the public. In creating and promoting these frames, United Nurses of Alberta draws from and pushes against the industrial relations framework under which they operate and the historical narrative of nurses as caring and self-sacrificing, which may reinforce common understandings of nursing and also limit United Nurses of Alberta’s ability to represent their members.
Introduction
Canadian mainstream media communication about unions has been notoriously negative and often gives the perception that unions are no longer necessary or relevant (Kumar and Schenk, 2006). Kumar and Schenk (2006) argue that unions in Canada are presented as irrelevant, inefficient, undemocratic and at best a special interest group. However, this representation is inconsistent with the evidence that unions in most countries help to establish better wages, health and safety regulations and advance workers’ interests (Kumar and Schenk, 2006), along with evidence of the union premium for wages, scheduling and occupational safety (Campanella et al., 2014; Finnigan and Mhairi Hale, 2018; Wilmers, 2017). The ways that a labor union frames itself as an organization is important to how its members and other people evaluate its performance and its role in society in general. Framing could be particularly important considering the decline in union density over the past 40 years in countries such as Canada.
To change the tide of how unions are presented in societies, unions must actively participate in their presentation, and they must use framing that helps people understand unions in the context of their lives (Benford and Snow, 2000). This case study focuses on a unique case of the United Nurses of Alberta (UNA), which is the union for the vast majority of registered nurses in Alberta, Canada. Alberta has one of the lowest unionization rates in Canada and has a provincial government hostile to most unions. UNA has a strong communications record and a history of adopting new communications technology relatively quickly compared with other unions. The adoption of new technology includes the development of their own internal communication system in the early 1990s. UNA maintains a range of communications with members and the public where they focus on workplace issues and health care in Alberta and Canada. They use common social media platforms such as Facebook and Twitter, both of which have a demand for almost daily communications material. For these reasons, UNA is an especially interesting organization in which to study questions of communications and framing. The case study analyzes how UNA creates collective action frames that help people interpret events and promote certain collective actions. The two key frames identified in this research were nurses-as-distinct and nurses-as-advocates. The first speaks to the unique qualities nurses have in the health care setting while the second speaks to the role nurses play in both the health care policy as well as in their care work with patients.
This article builds on Benford and Snow’s (2000) work on collective action frames to show how social movement organizations attempt to mobilize support for their goals, as well as the work of Gahan and Pekarek (2012), who connected collective action frames and social movement theory to union renewal. This article draws from various researchers who have examined different aspects of framing in relation to unions such as Ross (2011) who used collective action frames to examine the politics of union-community mobilization in the Canadian AutoWorkers campaign Manufacturing Matters, as well as the work of Muir (2008) who analyzed the Your Rights at Work campaign in Australia, and lastly Yates (2010) who focused on how union framing mobilized prospective women members in the childcare sector in Canada.
This study addresses the question of what frames UNA uses, and interrogates how these frames operate in the Alberta industrial relations context. As this case study shows, UNA frames any collective action predominately as an activity nurses are doing for patients. This framing plays out in two related collective action frames: nurses-as-distinct and nurses-as-advocates. These collective action frames draw from the historical construction of nursing as a caring profession framed by traditional gender roles. These frames also introduce possibilities for union members and their union, such as an opening space for nurses to advocate for their patients based on their care work, education and skill. At the same time, the frames may also limit the ability for UNA to represent their members as deserving of rights based on their worker status. The primary contribution of this work is to demonstrate how the frames used by UNA play into the social and historical context of the nursing profession and potentially limit the ability for UNA to advocate for members as workers. Notably, this case study contributes to extant literature on union renewal and daily union communications by allowing more careful attention to collective action frames outside of the bounds of a set organizing drive or campaign period and the impact this has on how unions can represent their members.
Theoretical framework and literature review
To fully understand the impact of union communications, this study uses a collective action frame approach. The collective action frame approach was built on the work of Goffman (1974) who defined a frame as a layout that helps individuals organize their experiences and gain meaning, and thereby function, in their lives. A collective action frame functions to help people interpret events by simplifying and condensing aspects of the world in ways that support a social movement or promote collective action (Benford and Snow, 2000). Snow and Benford (1992: 137) describe a frame as ‘an interpretive schemata that simplifies and condenses the “world out there” by selectively punctuating and encoding objects, situations, events, experiences and sequences of actions within one’s present or past environment.’ More specifically, framing is a term used by social movement theorists to describe the work done by people trying to maintain a social movement identity through articulating their goals, values, solutions and strategies (Monahan, 2013: 440). Through framing, social movements can also define the main players, including specifying who is responsible and who holds power in certain situations, as well as presenting possible solutions or actions the movement should use to achieve its goals (Ryan, 2004). ‘[To] be successful [though] frames must seek congruence and complementarity between the interests, values, and beliefs of the potential movement participants and the activities, goals, and ideologies of social movements’ (Franzway and Fonow, 2011: 292).
Franzway and Fonow (2011) claim that for unions to be seen as ‘mobilizing structures’ for collective action, unions must be discursively framed to make clear relevance in workers’ daily lives, and thus mobilize people to act. Depending on how a union frames itself, current and potential members can evaluate whether a union aligns with their own values and beliefs, which previous research has shown can influence member participation (Monahan, 2013: 440). Framing also helps workers to understand how unions can participate in and influence issues impacting their lives; in other words, framing can help to establish the relevance of an external organization in workers’ lives (Ross, 2011).
Frames are not created and do not function in isolation; therefore, it is important to examine the relationship frames have to the broader political and social context (Carragee and Roefs, 2004). Unions, their members, employers, community partners, government and the media all potentially impact framing. As Yates (1990) has shown, framing disputes can happen within organizations and the extent to which open debate and change can happen within organization depends on the form of mobilization structures. For example, Ross (2011) found the framing process for a Canadian Auto Workers (CAW) and community organizations’ campaign centered location over class as a unifying element and marginalized more anti-business and adversarial frames. In developing its framing the campaign tried to associate itself with what Benford and Snow (2000) refer to as ‘culturally resonant’ beliefs, which Ross (2011) reminds us are often connected to hegemonic assumptions. This study continues Ross’s (2011) inquiry into the implications of communications framing for unions in Canada. A key factor in how nurses specifically have been successful through unionization and various job actions is how they and their unions frame their relevance and how, in turn, they justify their militant, and sometimes illegal, actions. Instead of starting labor disputes for themselves, nurses have framed disputes in terms of their patients’ care and have worked to position themselves as public interest advocates improving patients’ conditions (Briskin, 2012; Brown et al., 2006; Jennings and Western, 1997; Strachan, 1997).
By framing relevance this way, nurses’ unions position their activities and goals as advocating for the general public in upholding a quality standard of care. This framing builds on the self-sacrificing characteristics of nursing and tends to allocate blame to hospital management and administration – sometimes even the government – and connects nurses’ working conditions to patients’ health outcomes. Frames in general are not static but an ongoing process, and different frames can compete or conflict with each other over how to interpret events (Benford, 1997: 416). The framing for nurses is fragile in the sense that it needs to be maintained and precludes important discussions about health care workers being deserving of rights for being workers. Since the nursing profession is dominated by women, a group often assumed to be caring based on their gender, they can also be presented during labor disputes as heartless and uncaring – failing not only as nurses but also as women (Briskin, 2012).
On an individual level, even when industrial relations activities help improve nurses’ working conditions and patients’ health outcomes, industrial action has historically been shown to cause personal issues for nurses when they try to reconcile these activities with their profession (Bessant, 1992; Hibbered, 1992; McGauran, 1999). Furthermore, Brown et al. (2006) demonstrate how nurses’ understanding of industrial actions change with their experience. Brown et al. (2006) found that before an Irish nurses’ strike, some nurses viewed the strike as responding to the government’s claims that the profession was weak and lesser-educated. At the beginning of the strike, nurses saw the action as making history through an expression of solidarity, then, as the strike continued, many nurses thought of strike activity like a job. In the final stages of the strike nurses were less positive and blamed the activity on industrial relations laws that forced them into certain allowable actions like strikes, which some nurses found incongruent with their profession.
Based on their ethnographic study, Brown et al. (2006) consider strategies that help nurses reconcile their self-image as a nurse with that of a striking worker. These strategies include: to reaffirm that both roles value caring; to link industrial action with patient advocacy; and to present strikes as a form of professional development, thus redefining what it means to be a professional nurse. To some extent, nursing unions have been successful with these strategies, as they realize nurses are more open to unionization when they feel unions are an avenue to address patient care (Clarke and Clarke, 2006). Nursing unions have focused on patient outcomes by linking them to nurses’ working conditions and trying to address the issues in collective bargaining agreements, and through legislation and regulations such as those of patient to nurse ratios (Clarke and Clarke, 2006).
Context
It is well established that for social movement communication to be effective, proper framing needs to be used so that people can understand the message and examine it against their understanding of the world and their lives (Benford and Snow, 2000). This contextual analysis discusses a brief history of the nursing profession, current knowledge about why framing matters for labor unions in the context of declining density as well as relevant details of UNA.
Brief history of nursing in Alberta
Canada’s early women’s movement helped carve out what were considered ‘appropriate professions’ for middle-class women, such as nursing (Villeneuve, 2014: 133). Often, these ‘appropriate professions’ were extensions of women’s traditional roles in the family and were constructed around an idea of a selfless, submissive woman (Villeneuve, 2014: 133). Nurses were trained, and women were taught, to put the needs of others before their own (Strachan, 1997).
This construction of nurses as a subservient group made it difficult for them to become a ‘profession’ in the early 1900s. The process of professionalizing nursing was like other professionalization processes in that it focused on service, education, certification and self-regulation (Adams, 2010). Part of this process also relied on nurses distinguishing themselves from other health care workers, often those who had less formal education or training. This historical construction of nurses, along with their efforts to become a profession made unionization and any job actions more difficult, as protests or strikes by nurses were sometimes labelled as unprofessional, unethical or selfish (Breda, 1997). David Coburn (1988) has pointed out that nurses’ professionalization was top-down and focused on their service to patients and subordination to doctors, while unionization focused on service to patients and generally came from nurses themselves.
The gendered history of nursing as an occupation and profession also causes nurses in Alberta and beyond to be seen as less important than other health care workers, such as physicians, and less knowledgeable about health care policy compared with administrators, which has led to struggles for fair pay and good working conditions (Adams and Nelson, 2009). Dahlke and Stahlke Wall (2017) also note the tensions nurses face as they attempt to articulate their knowledge skills as a profession, which are often discounted due to their gender, in addition to their caring skills.
Declining union density in Canada and Alberta
Many trade unions across the world are facing declining membership density. Union renewal is thus a critical issue and involves changes that can help to rebuild the labor movement, for example by attracting new members and increasing union density, but also by reinvigorating the movement (Kumar and Schenk, 2006). In Canada, union density has fallen in the private sector, but strength has been sustained by public sector growth (Krahn et al., 2020). In 2021 union coverage in Canada overall was 30.9% and ranged across provinces from a high of 39.9% in Quebec to a low of 25.6% in Alberta (Statistics Canada, 2022a). The variation in union density within Canada can be partly attributed to the different labor regulations across the provinces (Foster and Barnetson, 2011) and general differences in political culture (Fudge, 2006). Alberta is historically known to have more anti-union legislation and an anti-union popular culture (Foster and Barnetson, 2011; Yates, 2007).
Recent legislation in Alberta requires unions to divide their budgets into core and non-core activities that the government has defined broadly. Core activities include the basics of labor relations, such as filing grievances and negotiating collective bargaining agreements. The non-core activities include political advocacy and community donations. Any union dues payers would be required to opt-in to pay dues for these newly labeled ‘non-core activities’. The government can amend either of these categories as it sees fit. While the intent of this legislation appears to introduce American-style right-to-work legislation to Canada, it also fundamentally questions the role of unions in Canadian society. Owing to this recent legislative change, the framing of unions and their activities in Alberta has become more important than ever.
The United Nurses of Alberta (UNA)
The Alberta-based UNA has approximately 30,000 members comprised of registered nurses, registered psychiatric nurses and other allied workers. It is limited by the provincial labor relations board to only having registered nurses as members (except in a select few cases where they have a wall-to-wall agreement that includes all workers, such as clergy, food services or housekeeping staff). UNA has developed a reputation as a strong union willing and able to take a variety of approaches – both legal and illegal – in the face of concessions and government cuts. In Canada union coverage for professional occupations in nursing for 2021 was 82.8% (Statistics Canada, 2022b). In Alberta, there are just over 36,000 nurses (Canadian Institute for Health Information, 2021) and UNA claims to have over 30,000 members (UNA, n.d.), which aligns with national union coverage trends.
The requirements to become a registered nurse in Alberta are set by the College and Association of Registered Nurses of Alberta (CARNA). The requirements include a four-year nursing degree from an approved program. Under Alberta’s Health Professions Act and Registered Nurses Profession Regulations, nurses must be registered with CARNA to have an active practice permit.
Most nurses practicing in Alberta are unionized under UNA. The union has all the major contracts for nurses in the province, including those working in the province-wide health bodies, such as Alberta Health Services, which covers acute care hospitals, public psychiatric facilities, as well as several continuing and community beds, mental health and addiction support and community health centers. UNA also has contracts with Covenant Health, which is a Catholic health care provider in Alberta with approximately 17 hospitals and nursing homes. Further, they have collective agreements with several private nursing homes across the province. Nurses working in private non-unionized nursing homes or in out-of-scope positions, such as management, would not be covered under UNA. Also, nurses working for the federal Canadian government are unionized with the Professional Institute of the Public Service of Canada. Most nurses working in Alberta are automatically dues-payers to UNA as a requirement of their employment contract and their collective agreement.
UNA is well-integrated with the Canadian labor movement, with association to the Canadian Federation of Nurses’ Unions, which is the national umbrella organization for nurses’ unions across Canada, and representation at the Canada Labour Congress. UNA is also affiliated with the provincial Alberta Federation of Labour, as well as with the various municipal labor districts throughout Alberta.
Over the years, UNA has also collaborated with different partners to (a) fight against provincial and federal legislation, (b) ensure that nurses are heard during trade deals and (c) make connections with other labor and social groups in Canada. UNA has also provided strong financial support for other unions in Canada going through industrial disputes. In terms of communication, UNA is committed to multiple platforms to inform and update its members and the public. These platforms include traditional ones like news adverts and billboards, but also new technology and social media. UNA can be considered an early adopter of developing technology to communicate.
A key service that UNA provides its members is negotiating and servicing collective bargaining agreements that cover salaries, benefits, schedules and working conditions. UNA also participates in matters related to occupational health and safety, pensions and retirement, matters before professional and regulatory bodies, as well as the Workers’ Compensation Board – Alberta. UNA members fund UNA with 1.3% of their gross monthly income through union dues.
Methodology
By building from the work of previous union renewal research, this research uses a qualitative case study design (Foster and Barnetson, 2011; Fowler and Hagar, 2013; Kumar and Schenk, 2006; O’Neill, 2007; Ott and Milkman, 2014; Ryan, 2004; Sullivan, 2010). The research examines the question of what frames UNA uses in its communication materials and considers how the frames function for UNA members.
Research design
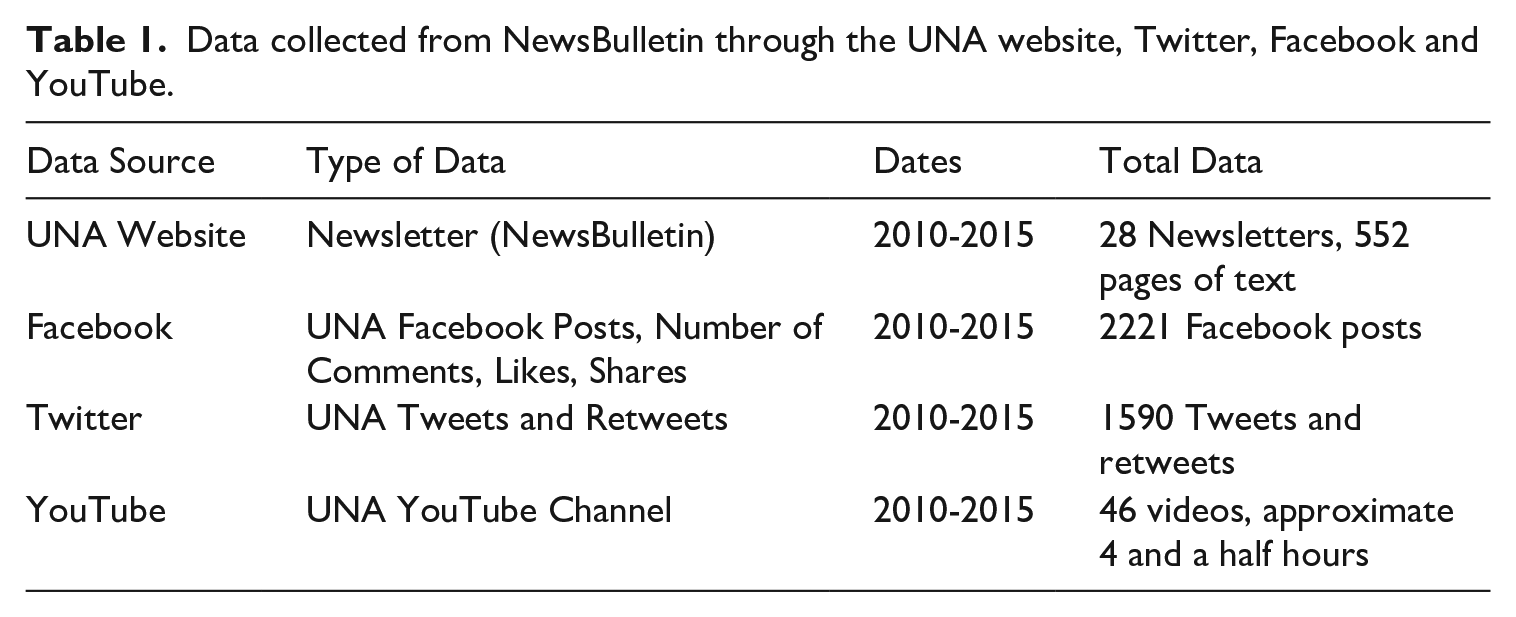
Typical of most case studies, this study draws from multiple data sources (Yin, 2009), including a wide range of communications documents from UNA as well as a rich set of 23 semi-structured interviews with union employees and members. The research began in 2015 by collecting information about UNA and its history. In the next stage UNA’s communication data was collected, starting first with the newsletters, which were readily available on the UNA website, then Facebook data, followed by Twitter data, UNA videos from YouTube and finally a website analysis (Table 1). The qualitative data used includes that produced by UNA and does not include comments from UNA members or the public through social media sites. The data from this study offers original evidence from the Canadian context concerning the collective action frames used by UNA.
Data collected from NewsBulletin through the UNA website, Twitter, Facebook and YouTube.
Data analysis
Over 3500 data points were collected and analyzed from the vast communication UNA uses, as well as interviews with staff and members. The documents were analyzed using a qualitative approach of developing consistent themes through different iterations of data review and from previous literature. The communication analysis began with the UNA newsletter, then the social media material grouped based on the platform and lastly the UNA website. The themes were expanded and refined as new material was analyzed through this iterative process.
After finishing the communication analysis, semi-structured interviews with UNA staff and elected officials were conducted to further understand their communications methods and strategies. The first round of interviews included seven elected officials and staff. The second stage of interviews involved six highly involved UNA members who simultaneously receive communications from central UNA and produce some of their own communications for members. The last stage of interviews was with 10 UNA general members who are largely receivers of UNA communications. Like the document analysis, interviews were analyzed in groupings and themes developed through an iterative process that included multiple reviews of the material, insights drawn from previous literature (Rubin and Rubin, 2012; Strauss, 1987) as well as the codes developed from the prior communication analysis. The overall themes were then developed out into the main collective action frames, which focused on who the major players are, who is responsible and holds power in the situation and the presentation of possible solutions (Ryan, 2004).
UNA’s collective action frames
This section discusses the data analysis, which resulted in two main frames UNA used to discuss the work that nurses do, and UNA in turn builds from these two frames to discuss their own relevance.
The frames of nurses and UNA
The first frame is nurses-as-distinct, which is based on their education, skill and regulated status. The second frame is nurses-as-advocates – firstly, advocates for their patients, clients and residents and secondly, advocates for a good health care system in general. These frames used by UNA impact how nurses understand themselves as a profession and as workers. The frames also shape how UNA presents itself as relevant for its members, this in turn shapes how UNA members evaluate and understand their union.
Nurses-as-distinct
A central frame for UNA messaging was that nurses are distinct from other health care professionals, especially from non-regulated health care workers (example, health care aides). This message was repeated in videos where elected officials discussed evidence from studies that show there are better health outcomes when patients are cared for by an adequate number of registered nurses. The message also features in UNA videos that emphasize the lack of extensive education for health care aides. Several Facebook posts and tweets repeated this message. For instance:
Are you wearing white today? Each Wednesday, UNA members are encouraged to wear white or wear their Registered Nurse, Registered Psychiatric Nurse, and Licensed Practical Nurse pins to show their patients, residents, and clients that they are a Nurse. (Facebook, UNA) [Employers] are replacing educated skilled nurses, whose profession is regulated, with non-professional and unregulated Health Care Aides. This contradicts all evidence of the best way to run a safe and effective health care system. Eliminating nurses and replacing them with non-professional aides lowers the quality of health care and increases the risk for patients. (Facebook, UNA) Stop nurse job cuts, replacement by unregulated aides, @CFNU President Linda Silas tells #unaagm delegates: http://bit.ly/1h5MAfZ #abhealth. (Twitter, UNA)
In this frame, important players are identified and include groups such as nurses, health care aides and health care employers. Nurses are presented as a group that is more skilled and prepared and are uniquely held accountable through professional regulation for the care they provide. Moreover, within this frame, health care employers are routinely presented as the ones having power, in this case the power to hire a specific mix of employees within legislative minimums that would require specific staff-to-patient ratios.
UNA is also typically positioned in this frame as being an organization that helps to ensure that nurses are there for patients to provide quality health care. UNA is given a role in supporting nurses who, when supported by UNA, can provide the unique care that nurses as a regulated, skilled profession are equipped and able to provide. Other less lengthy statements supporting this framing include slogans such as ‘We’re here for nurses. . .and Alberta’s nurses are here for you!’ Slogans such as this rely on the relevance of nurses to justify the relevance of UNA. This theme is echoed on UNA’s Twitter page with tweets stating, ‘Safe staffing saves lives, and unions fight for safe staffing’ (Twitter, UNA). Acceptable actions for UNA members in this frame include filing Professional Responsibility Concerns (PRCs) when staffing is not appropriate, rallying, information pickets and wearing white to identify themselves as a nurse to patients and their families, thus setting themselves out as distinct from other health care workers.
Nurses-as-advocates
Nurses-as-advocates was a frame repeated across all the media platforms. This frame branches into two divisions of advocacy work that nurses are encouraged to be involved with – firstly, as an advocate for their patients, and secondly, as an advocate for improving the health care system.
This frame was presented in YouTube videos on UNA’s channel when there was confusion over a potential Alberta Health Services (AHS) policy that would punish nurses for publicly criticizing AHS. In this video, the message was clear that nurses needed the ability to be advocates and their employer should not silence them. The frame was repeated on Facebook with posts such as the following:
Alberta’s nurses are dedicated to your health and the health of your family. We advocate for a properly staffed and supported public health care system so that we can always provide the care you need when you need it. (Facebook, UNA) Members of UNA Local 301 stood up for safe patient care by holding an information walk outside of the University Hospital yesterday. The walk was held to raise awareness about the impact that ongoing nurse layoffs will have on safe patient care in Alberta hospitals. (Facebook, UNA) If you have a concern about a patient, client, or resident safety or staffing levels in your workplace, you should fill out a Professional Responsibility Concerns (PRC) report as soon as possible. Through this process, the concerns of Registered Nurses and Registered Psychiatric Nurses are documented and can be addressed at the highest levels of your organization. (Facebook, UNA) In good times and bad, that’s exactly what United Nurses of Alberta and its 30,000 members do: Advocate for quality care when Albertans require it, properly funded and universally accessible. (Facebook, UNA)
These messages were repeated in the newsletter with headlines such as, ‘UNA’s Superheroes lead the fight to make sure Save (sic) Staffing Saves Lives’ (NewsBulletin, UNA) and ‘File a PRC! When it’s unsafe, protect your patients, protect yourself!’ (NewsBulletin, UNA). These frames were repeated on Twitter with tweets such as ‘Alberta’s nurses are committed to the best care for our patients, and to public health care, available to every Albertan’ (NewsBulletin, UNA).
Nurses were also occasionally presented as advocating for specific changes to improve health care, such as advocating for a pharmacare program in tweets such as ‘A national prescription drug plan could save Canada +$1 billion in admin costs’ (Twitter, UNA).
In this frame, the major players are UNA, nurses and the government or employer. Nurses are positioned as an intermediary between patients and the government or employers, and nurses are given a guardian role in ensuring patients receive quality health care. The government and employers are positioned as having the power to give or restrict the care to which Albertans have access.
UNA is then positioned as backing up nurses and helping them ensure they can be advocates. The President of UNA, Heather Smith, is quoted in the UNA newsletter stating:
When unions like United Nurses of Alberta fight to preserve public health care and for the creation of new programs like a national pharmacare plan, we are working on behalf of all middle-class Canadian families. When we enforce our contracts, to ensure all employees are treated equally within their bargaining units, we are fighting for women’s rights, workers’ rights, and civil rights. And when we struggled successfully over the past 15 months for a fair collective agreement in the face of strong efforts by some of our employers and political forces to roll back our wages and working conditions, we were supporting the rights of every working person. (NewsBulletin, UNA)
This frame is also used on UNA’s Facebook with statements such as, ‘UNA’s new radio ad is playing across Alberta. UNA is speaking up about health care in Alberta on behalf of its members, their patients, families, and all Albertans’ (NewsBulletin, UNA).
Often these acceptable forms of action are accompanied by motivations for the nurses – for example, that if nurses take action to advocate for themselves or a better health care system, they are by extension advocating for their patients. Acceptable or recommended activities for people to take under this frame are limited to labor relations activities such as filing PRCs, grieving collective bargaining agreement infractions, rallying and taking part in information walks to educate the public. The most often recommended activity was to tell patients you are a registered nurse. UNA did not often suggest nurses talk to their families, friends, or neighbors as advocates, rather the focus was on communication with patients. On rare occasions, a labor strike is presented as an acceptable way of responding to the power of an employer or government. However, strikes are almost always presented as the last resort option, considered only once all other options have been tried and failed.
While nurses advocating for patients may be a ‘safe’ form of advocacy that people have come to expect from nurses and is therefore seen as an acceptable task, the other forms of advocacy for the health care system, in general, may not be seen as acceptable. Joining advocacy for patients with advocacy for the health care system may help to depoliticize advocacy solely for the health care system that often involves lobbying the federal and provincial governments. On its own, political lobbying may be seen as too overtly political and therefore an inappropriate use of mandatory union dues as is suggested by the new Alberta legislation.
By intertwining these two different kinds of advocacy, UNA is pushing the boundaries on what is acceptable for nurses’ advocacy by expanding nurses’ duty and responsibility ‘to care’ while also justifying UNA’s political advocacy efforts. UNA is also promoting the different forms of advocacy as potentially helping patients. So, nurses are motivated to advocate for themselves and a better health care system in the political realm, all in the name of providing better care for their patients.
Discussion and conclusion
This study seeks to identify and analyze the collective action frames used by UNA and interrogates how these frames advance the interests of members and the union. Collective action frames are important for how union members, and the public, understand nursing work as well as UNA and their roles in society. As discussed earlier, UNA uses two frames to organize their communications: nurses-as-distinct in the health care setting, and nurses-as-advocates for patients and the health care system. These two frames reinforce the power dynamics that nurses and their union operate within, including the industrial relations context and the recommended courses of action available to the parties, echoing how Monahan (2013) describes frames as articulating goals, values, solutions and strategies. In using these two frames UNA may be entrenching traits such as self-sacrificing, regardless of compensation, which is arguably not ideal for any worker in the power imbalance often found in employment relationships.
The nurses-as-distinct frame emphasizes and distinguishes nurses based on their education and skill. This frame is often used to counter moves by government and employers to replace nurses with health care aides who receive lower compensation. This frame harkens back to some of the same messaging that was historically used when nurses were first forming their professional associations – mainly that they were a distinct profession because of their skill and education (Gray, 1989; Ross-Kerr, 1998).
Despite some of the potential benefits of this frame, UNA staff and elected officials are aware that some UNA members are uncomfortable differentiating themselves from their coworkers based on their nursing designation. This frame does not always sit well with nurses in their actual practice, especially when they are part of collaborative health care teams or when they have been trained to be invisible in the workplace, as argued by Adams and Nelson (2009). The use of this frame also appears to be disconnected from the experience of some nurses seen in other research such as Boateng and Adams (2016) who found that racialized and young nurses had their professional experience and knowledge discounted by other nurses and were vulnerable to workplace bullying and discrimination. Still, UNA uses this as a frame for communications presumably because the benefit of emphasizing the distinctness of their own members enables them to advocate for them better during collective bargaining negotiations and political lobbying efforts.
In the nurse-as-advocate frame, nurses have been cast as guardians of public health care and their patients. Nurses are seen to not only provide care to patients, but to also keep the system functioning effectively, and hold politicians and bureaucrats accountable to the public, ensuring quality care for patients. UNA condenses the complex matter of quality health care into a simple message that promotes nurses as advocates and also promotes UNA in supporting nurses to be advocates. As found by Benford and Snow (2000: 614), condensing and simplifying complex matters into collective frames allows social movements to promote their goals and more easily engage potential supporters. This frame plays well with the common rhetoric of nurses and women as caring and self-sacrificing for their patients, which has historically been associated with the nursing profession. This again supports Benford and Snow (2000: 622) who assert that movements will often attempt to connect their framing to ‘culturally resonant’ perspectives, which tend to mobilize people more effectively. However, as Ross (2011) points out, perspectives that have cultural resonance often have unacknowledged assumptions attached to them.
The nurse-as-advocate frame also does not always pan out. Not all nurses advocate for their patients or the health care system. When there are inconsistencies between how nurses are framed by their union and nurses’ actions it can cause issues for the public, who may come to expect all nurses to behave or carry themselves in a self-sacrificing manner. This may also cause issues for nurses who feel pressured to maintain this role despite pressures from their employer to save costs on supplies, finish tasks quickly, or nurses who have limited interest in being an advocate on top of their nursing duties.
The first frame is about nurses as a profession while the second frame is about the advocacy role that nurses have. UNA uses these frames together: nurses are a distinct profession, and, on that basis, they are able to be advocates. In these frames the role of advocate could be seen as a code for caring, an attribute that has historically been associated as natural, yet often devalued economically, for women. Changing the language from caring to advocate may make caring more compatible with being a professional. Being an advocate, although perhaps still drawing from predominately feminine characteristics, is a recognized role in the public sphere complete with compensation and at times legal standing in certain systems. These findings connect to those from Dahlke and Stahlke Wall’s (2017) – namely, that nurses are often not given the proper vocabulary to talk about their knowledge skills alongside their caring skills – and findings from Yates (2010) that caring labor can be framed by unions as skilled work that has social and economic value – and thus, the use of advocate could be UNA’s attempt to provide a different vocabulary that is more compatible with presentations of what a professional nurse is. However, pushing the frame of nurses-as-distinct and building to nurses-as-advocates may actually move nurses further away from being conceived of as workers. An advocate role, although different from the role of a caregiver, still risks playing up traits such as self-sacrificing and going above and beyond, regardless of compensation, which does not appear helpful for any worker in the power imbalance often found in employment relationships. Playing up the advocate role may indeed make it more difficult for nurses to assert their rights as workers, especially in the face of pressure from management and perhaps the public. Overall, a conception of nurse-as-worker is arguably better for nurses as it comes with legislated protections and is more aligned with the overall goals of the labor movement.
The frames used by UNA impact how nurses understand themselves and this impacts the services the nurses think they need from unions, which is reflected in how UNA positions itself as relevant for members. For example, by presenting nurses as advocates for patients and the health care system, UNA is also outlining roles for nurses and in turn, roles for UNA to support nurses. A key example of this is the PRC process that UNA describes as a way for nurses to alleviate their moral distress caused by the incompatibility of their CARNA professional expectations and the reality of their working conditions – for example, being unable to provide adequate care because of short-staffing. UNA provides a tool, the PRC process, for nurses to use in these situations that aligns with the frame of nurses-as-advocates. The PRC process is typically done during a nurse’s personal time and may push nurses away from being conceived as workers and pull them more towards being selfless advocates. This process, however, does help make UNA relevant regarding the conflict of CARNA professional expectations and the reality of working in health care in Alberta.
As previously mentioned, the courses of action recommended by the frames fall well within the parameters set out by Alberta industrial relations legislation including rallies, informational lines, pickets and strikes all of which promote collective actions. This promotion of collective action reinforces Benford and Snow’s (2000) description of social movement frames that aim to achieve collective action from participants. The specific action promoted also reinforces the power structures between the state, workers and their unions, by following the prescriptive steps set out in Canada’s labor relations laws.
The frames unions use for their communications matter, not just for themselves as organizations but also for how they present the work and workers they represent. For collective action frames to gain traction in our societies they must have cultural resonance and it helps if they can easily connect with already established ideas, such as nursing as a caring profession for UNA. The frames used by UNA in its communication materials strongly play into the historical and social history of nursing as a profession, and by playing up this history they set expectations for good nurses and a good nurses’ union while at the same time restricting how nurses and their union can advance nurses’ interests. By presenting nurses as distinct health care providers who can uniquely advocate for patients, expectations are set for nurses that align with a selfless feminine caregiver, which is arguably not in the best interests of nurses as workers in a patriarchal medical system and capitalist economy. These frames also set up the value and relevance of UNA itself. UNA is now defined by how its members, nurses, live up to their role as distinct health care providers who are advocates for their patients and the health care system. This may mean UNA is able to ensure its members are both distinct and advocates, which in turn may place UNA in tension when they may have to defend members who do not perform as ideal nurses under these frames or under their conditions of labor in the Alberta health care system. It is therefore important for unions to understand and plan how their collective action frames tap into already established ideas, if those frames indeed promote unions to advance the interests of their members, and if the frames entrench assumptions that harm union members or if a mixture of benefit and harm are the outcome. This planning needs to take place not just for more organized campaigns around specific issues or organizing drives but for the now daily social media communications that many unions are using.
This research leads to more questions the author will pursue in future research and publications such as: is there any dissonance or tension between these frames used by UNA and their members? and how do members influence the frames UNA uses? Another line of questioning would be how UNA’s framing impacts the work of other unions operating in the health care sector. Overall, this case study provides valuable empirical insights into the activities and communication practices, as well as both the possibilities and limitations of current collective action frames, of a Canadian health care union. It also provides solid groundwork for future studies examining the role of union communications, how various historical and current factors impact communications and how union communications can impact how unions are evaluated as relevant for their members.
Footnotes
Acknowledgements
I wish to thank the participants and organization for sharing their knowledge and time during this research. I also want to thank my dissertation committee for their guidance and support. Preliminary versions of this article were presented at the 2021 Canadian Association for Work and Labour Studies and I would like to thank the organizers and participants. Lastly, I want to thank the three anonymous reviewers at Work, Employment and Society for their invaluable remarks and recommendations.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Joseph-Armand Bombardier Canadian Graduate Scholarship Doctoral from the Social Sciences and Humanities Research Council in Canada.