
Abstract
Gender and work are important social determinants of health, yet studies of health inequities related to the gendered and emotional intricacies of work are rare. Occupations high in emotional labour – a known job stressor – are associated with ill-health and typically dominated by women. Little is known about the mechanisms linking health with these emotional components of work. Using physiological and questionnaire data from Canadian police communicators, we adopt an embodied approach to understanding the relationship between gender norm conformity, emotional labour, and physiological dysregulation, or allostatic load. For high conformers, emotional labour leaves gendered traces in the flesh via increased allostatic load, suggesting that in this way, gendered structures in the workplace become embodied, influencing health through conformity to gender and emotion norms. Findings also reveal that dichotomous conceptions of gender may mask the impact of gendered structures, obscuring the consequences of gender for work-related stress.
Keywords
Introduction
All working bodies accomplish work through sensing and, as such, all work is an embodied practice (Hockey and Allen-Collinson, 2009). While the physical bodies of workers – for example, their strength, proximity, interactions, injury, or movement in space (Rajan-Rankin, 2018; Rydzik and Ellis-Vowles, 2019; Yates et al., 2018) – are given increasing attention in the sociology of work, the physiological bodies of workers – for example, their chemical stress responses and emotion-based neurohormonal pathways – have received little consideration. Work, however, consumes large portions of time throughout life, and is a significant social determinant of health (SDOH; Ahonen et al., 2018). As a SDOH, work is also understood to be manifestly gendered with gendered health outcomes (Milner et al., 2021). Notably, the salience of gender in sustained and growing divisions of labour across jobs (Adams, 2010; Milner et al., 2018) and within organisations (Acker, 1990) underscores the importance of understanding how gender – both in organising the work environment and in the details of the work itself – might shape the health of workers through internally-based, yet socially determined bodily stress and emotion processes (Gimlin, 2007). As such, matters of the physiological body are central to a sociological understanding of social relations of inequality, including stressful gendered work and its health outcomes (Freund, 2006; Pearlin, 1989).
Although the work-related health, illness and well-being of first responders is of increasing concern (Carleton et al., 2020; Regehr et al., 2021; Wagner et al., 2020), police communicators – otherwise known as emergency call handlers/takers and dispatchers – are often excluded from these studies because of their civilian, behind-the-scenes status. However, as the typical actual first responders in public safety, research regarding their unique workplace conditions and associated negative impacts on health, is warranted.
Working within a masculinised organisational imperative to remain calm and emotionally removed (Mann, 2004), it is through emotional labour (EL), we suggest, that communicators are able to conduct some of the most crucial aspects of their work (Birze et al., 2020, 2021). The emotion-based body work of communicators, often deemed women’s work, although typically characterised as disembodied, because the objects of their body work are not physically present (Rajan-Rankin, 2018), rather involves deeply embodied processes (Wang, 2020). The conflicting gendered nature of these tasks – feminine for caring and emotionality on the one hand, and masculine for self-reliance and rationality on the other – likely compounds the difficulty of communicators’ tasks. We believe an approach that centralises the embodiment of work might best reflect how it is that EL, as a form of stressful gendered body work, ‘gets under the skin’ (McEwen, 2012) to shape health.
While scholars have produced considerable evidence linking EL with poor self-reported mental and physical health (Hülsheger and Schewe, 2011), little research has addressed the physiological embodiment and health-related impacts of this stressful, gendered work. Specifically, we ask: How might gender – through emotional labour practices – become visible in the flesh of working bodies in high-stress and high-trauma contexts? We hypothesise that conformity to gender norms and the EL requirements of police communications work will be associated with the health of workers through embodied occupational stress processes (physiological dysregulation as measured through allostatic load; AL) in a sample of communicators from an urban centre in Canada. Following the ‘body/work/gender nexus’ conceptualisation of the connections between the working body and gendered bodily practices (Rydzik and Ellis-Vowles, 2019: 488), this work considers how non-binary gendered bodily practices in high stress working contexts might become visible in the physiological body with a specific focus on integrating EL as a form of stressful gendered ‘body work’ (Twigg et al., 2011) that is embodied (Mirchandani, 2015).
Thus, this observational study makes three main contributions. First, it provides a particularly ‘fleshy’ embodied perspective on working bodies (Hockey and Allen-Collinson, 2009: 218), thereby expanding traditional sociological notions of the material body (Freund, 2006). Second, it pushes the boundaries on the types of work that are traditionally appreciated for their profound body work and processes of embodiment by reconceptualising remote, telephone-based work as something other than disembodied (Rajan-Rankin, 2018). Third, it explores stress and emotion in gendered work in a non-binary manner that might better reflect how nuanced normative practices, typically masked within binary gender categories, might shape the experience of workplace stress inducing EL. While most studies explore the influence of sex assigned at birth or self-identified dichotomous gender (Bottorff et al., 2011; Hart et al., 2019; Westbrook and Saperstein, 2015), earlier research has demonstrated that femininity and masculinity are related to health in complex ways that are obscured by dichotomous measures (Annandale and Hunt, 1990). The extent to which we align ourselves with gendered norms might serve as a proxy for the expectations we have for ourselves and others in social encounters, including how we conduct and perceive workplace tasks like EL. Accordingly, we evaluate the impact of a more nuanced view of gender by exploring conformity to gender norms, uncovering nuanced variation within gender categories (Hart et al., 2019).
Police communicators and their embodied work
In the Canadian context, police communicators are responsible for answering calls and dispatching services for both emergency and non-emergency calls from the public, as well as for internal requests for service. These are civilian roles and not normally filled by past officers. However, from behind the scenes, communicators are exposed to similar occupational stressors as those of frontline emergency workers and are also subject to additional, environment-specific stressors such as a close, confining workspace and controlled mobility, intense organisational scrutiny, prolonged interpersonal engagement and concentration, and rapid pace for extensive periods (Birze et al., 2020, 2021; Regehr et al., 2013). At all times – whether interacting with the public, frontline emergency service workers, co-workers, or supervisors – they are required to simultaneously manage their own emotions while evaluating and managing the emotions of others, in their ongoing efforts to discern pertinent public safety information in organisationally sanctioned ways (Birze et al., 2020, 2021). Thus, they routinely negotiate a variety of their own as well as others’ emotions – including anxiety, anger, guilt, disgust, indifference, empathy, sadness, helplessness – as a function of carrying out their occupational duties (Shuler and Sypher, 2000; Tracy and Tracy, 1998).
Although often characterised as disembodied, this highly skilled technological and telephone-based work profoundly engages sensory and emotional processes. Telephone-based or voice-to-voice work is both a form of ‘body work’ (Gimlin, 2007) and embodied work (Mirchandani, 2015; Wang, 2020). The few scholars examining the embodiment of telephone-based work or ‘voice workers’ have demonstrated this embodied work as done through both the transmission and reading of bodies – across time and space – through the use of voice and visualisation (Mirchandani, 2015; Wang, 2020). In a context with high uncertainty and risk, the embodied work of call-takers and dispatchers demands that the bodily experiences of the communicator are joined both with the bodily experiences of callers as well as frontline first responders through voice and visualisation in an effort to bridge the distance between all parties (Wang, 2020). Through voice and visualisation, the call-taker works to be there in the caller’s presence by interpreting the sensory experiences of the caller and controlling the flow of embodied information from them, while the dispatcher works to be there with the emergency response personnel at the scene, transmitting the callers’ embodied information and always sensing the ‘worst-case-scenario’ possible, in an effort to ensure the safety and security of frontline responders (Wang, 2020: 481). Working from the ‘zone’ – a mental space where communicators are ‘vicariously co-present on scene with people absent from them’ – communicators experience some of the ‘hardest, most emotionally intense’ aspects of their work (Wang, 2020: 481). Thus, although by distance, the work of communicators focuses both on their own bodies as well as the bodies of others – through sensorial experiences of voice, emotion, description, and visualisation – making those on the other end of the transmission objects of their ‘body work’, largely through demands for emotional labour (Gimlin, 2007; Mirchandani, 2015; Twigg et al., 2011; Wang, 2020).
Emotional labour and gendered work
Emotional labour (EL), as originally theorised by Hochschild (2003) in her influential work with women flight attendants and men debt collectors, examines the ways in which workers are required to cultivate certain emotional exchanges along gendered divisions of labour. An occupation requires EL when its performance involves relational contact with the public, the production of an emotional state in another, and/or when the employer has an incentive to control the emotional displays of its workers (Wharton, 2009). In order to present as falling in line with an organisation’s feeling rules and societal norms – including gender norms – feelings either have to be suppressed, changed or evoked in an effort both to behave appropriately and to engineer the desired response from others in the interaction (Wharton, 2009). The emotional dissonance required to perform EL may lead to feelings of inauthenticity, emotional exhaustion, and burnout (Meanwell et al., 2008).
While sometimes critiqued as insufficient for capturing the complexity of emotion in the workplace (Bolton and Boyd, 2003; Brook, 2009), EL is regarded as a significant source of on-the-job stress with the potential for serious health consequences (Hülsheger and Schewe, 2011). Although some researchers have provided evidence of the multidimensional nature of workplace EL that is not entirely predicated on organisational feeling rules (Bolton and Boyd, 2003), others have demonstrated important differences in the mental health outcomes associated with EL that is performed with the public, co-workers, or supervisors (Birze et al., 2021).
In that there are gendered patterns to who performs EL and how, feeling rules share ‘some formal properties with other sorts of rules, such as rules of etiquette, rules of bodily comportment . . . and reflect patterns of social membership’ (Hochschild, 1979: 565–566). Young (1980) uses the example of how some women are said to ‘throw like girls’ to demonstrate some of these social constraints on the body, describing them as ‘a space [which] surrounds us in imagination that we are not free to move beyond; the space available to our movement is a constricted space’ (p.143). Emotional spaces can be similarly constrained and women use and experience their bodies within different material, spatial, emotional, and discursive arrangements than men (Freund, 2006; Young, 1980, 2002).
Although work in emergency services is often recognised as requiring EL (Mastracci, 2015), it is rarely examined with specific attention paid to the gendered and embodied dynamics of EL. Assuming EL is a gender-neutral task however, may marginalise certain emotional responses, leading to further distress with potential consequences for long-term health inequities. For instance, Lois’ (2001) study of volunteer rescue workers demonstrates how, during the regular course of their high-risk search and rescue missions, adrenaline rushes occurring in response to stressful working conditions and decision-making are characterised as a sense of urgency in men and a sense of fear in women rescuers. Not only are the labels urgency and fear intricately woven into what are judged appropriate performances of masculinity and femininity respectively, but the sense of fear in women is less powerful and more stigmatised than is the sense of urgency experienced by and bestowed upon the men (Lois, 2001). In this masculinised context, feelings of fear are gendered feminine and marginalised, thus leaving more at stake with respect to judgements of emotional competence and job performance for women rescuers. Consequently, they worry more about losing emotional control – that is control over their emotional responses through EL such as suppression or display of emotions – and find the unpredictable nature of their work to be more stressful than do the men (Lois, 2001). Adrenaline rushes and their associated emotional responses are gendered through workplace interactions, thereby creating an embodied hierarchy of emotional competence with potential consequences for their health. Emotion practices among these rescuers serve to reinforce existing power structures as attempts by the women to step outside the bounds of this situated emotional hierarchy are either ignored or admonished outright (Lois, 2001).
Indeed, as Whalen and Zimmerman have pointed out, specifically in the police communications setting, other emotion labels such as ‘hysterical’ or ‘hostile’ are as much relational and organisational as they are emotional (Whalen and Zimmerman, 1998), possibly used to enforce embodied hierarchies of emotional competence, including through the gendered labelling of EL practices. Their close examination of the situated intersection of physiological arousal, display, and management of emotion also demonstrates the undeniably social construction of emotion (Whalen and Zimmerman, 1998), anchoring these processes in emotional labour and stress.
Clearly, gendered assumptions about jobs lead to specific ways of ‘doing’ and ‘seeing’ femininity and masculinity (Nentwich and Kelan, 2014). This has important implications not only for the women in high-stress emergency response such as communications, but also for the minority of men who perform this type of work. In policing, those who are able to harden emotionally, maintain a calm and dispassionate demeanour in the face of distressing events, and project an ever-functional working body, are perceived as ideal officers (Evans et al., 2013; Yates et al., 2018). It is unclear, however, whether this emotional hardening is perceived as appropriate and becoming among women officers or by extension, those in communications. For instance, it is also the case that women working in occupations dominated by men experience backlash and reprisals for adopting masculine ways of conducting their work and EL (Pierce, 1999, 2004). Engaging in work that is constructed as women’s work, men may perceive themselves and be perceived by others as violating normative expectations for masculinity (Nentwich and Kelan, 2014).
The nature of police communicators’ work is likely to create unique tensions, both conscious and unconscious, between altruistic intentions of providing compassionate, caring service for public safety – gendered feminine – (Shuler and Sypher, 2000) on the one hand, and workplace constraints in policing for calm, dispassionate, rational and controlled rapid response – gendered masculine – (Swan, 2016) on the other. The conflicting nature of these tasks likely compounds emotional difficulty, and potentially heightens communicators’ stress responses at work.
The allostatic load framework as embodied work stress
We wish to expand the scope and meaning of the ‘body/work/gender nexus’ (Rydzik and Ellis-Vowles, 2019) by paying particular attention to ‘fleshy’ matters of the body (Hockey and Allen-Collinson, 2009) – the physiological variables associated with chronic workplace stress – using AL as a way of operationalising the physiological embodiment of social life (Delpierre et al., 2016; Krieger, 2005). The AL framework was created as a way of assessing bodily ‘wear and tear’ due to chronic stress (McEwen, 1998). While its typical conceptualisation in the stress literature is not employed to interrogate the health implications of social relations and structures, it can be understood as a way of mapping – through explicit changes in neurohormonal pathways linked with stress and emotion processes (Freund, 2006) – the physiological impact and health-related outcomes associated with the material embodiment of social life, and thus the social gradient in health (Delpierre et al., 2016). While higher work-related demands, lower decision latitude and control, exhaustion, and burnout are associated with higher AL (Mauss et al., 2015), to the best of our knowledge, there is no research regarding the intersection of AL, EL, and gender.
Generally speaking, the cardiovascular, metabolic, immune, and central nervous systems all have wide ranges of activity that are involved in healthy coping and adaptation, or what is referred to as allostasis (McEwen, 1998). It is when the activation of these systems is recurring or not terminated that health is undermined through inefficiently managed or overactive responses to chronic stressors. These changes are assessed and an AL score is calculated using a battery of physiological indicators including neuroendocrine, metabolic, inflammatory, neurophysiological, cardiovascular, and anthropometric factors (Juster et al., 2010; McEwen, 2015). Over the long term, systemic dysregulation may manifest as clinical conditions such as hypertension, cardiovascular disease, diabetes, or obesity (Juster et al., 2010; McEwen, 1998, 2012, 2015), some of which may be disproportionately high among communicators (Lilly et al., 2016; Smith et al., 2019).
Methodology
Data presented in the current study are part of a larger mixed methods investigation on how stress, emotion, and gender shape embodiment and health outcomes in police communicators. Ethics approval was obtained from the University of Toronto’s Research Ethics Board. Permission to conduct the research onsite was granted by a large urban Canadian Police Service. All currently-working communicators in The Service were eligible and invited to participate on a voluntary basis. All individuals who wanted to participate were included with a total of 81 individuals enrolling throughout the span of data collection.
Upon providing consent, each participant was scheduled for one observation period while they worked, lasting approximately 3–4 hours. During observations, participants wore a heart rate variability monitor, and the first author took notes and talked with participants as their workload permitted. At the end of the observation session each participant received a set of questionnaires, along with cortisol awakening response kits, to be completed at home. The study comprised 80% women and is representative of the gender composition of communications employees across Canada (Conor et al., 2019). This, in itself, reflects the gendered segregation of certain kinds of labour. However, although representative, this is a very small cohort necessitating a cautious interpretation of these observational associations. Future studies with larger cohorts will help to refine and verify the theoretical implications of our findings.
Multiple visits to The Service comprised 400 hours over nine months. Towards the end of the nine months, separate visits were used to collect the additional physiological data for calculating allostatic load scores. Participants were temporarily relieved of their duties to complete this component. A certified phlebotomist conducted the blood draws and a research assistant helped with the additional anthropomorphic indicators. The physiological data collection only occurred during day shifts.
The Emotional Labour Scale-Revised (ELS-R) is job-centred and assesses the perceived variety, intensity, duration, and frequency of hiding, faking, and expression of emotion on an average workday (Brotheridge and Grandey, 2002; Brotheridge and Lee, 2003). Example items include ‘Try to actually experience the emotions that I must show’ and ‘Hide my true feelings about a situation’, which are endorsed on a scale from 1 to 5, reflecting never to always experienced. Cronbach’s alphas range from .69 to .95 (Lee et al., 2010) and convergent and discriminant validity are supported (Lee and Brotheridge, 2011). Using the ELS-R, workers can successfully be divided into different EL profiles that are generalisable across occupations, and can meaningfully predict outcomes such as, emotional exhaustion, psychological detachment, and job performance (Fouquereau et al., 2019), suggesting the scale’s sensitivity for assessing the impact the requirements for EL may have.
Conformity to Gender Norms Inventories: Gendered inequalities in health are not neatly dichotomous, prompting scholars recently to advocate for the use of femininity and masculinity scales as a way of adding nuanced gender variation that exposes hidden dimensions of inequality (Hart et al., 2019; Magliozzi et al., 2016). This is especially true with respect to health inequalities (Weber et al., 2019). Because social interactions evoke hegemonic gender beliefs, the salience of these beliefs acts as a background frame that shapes the practices and appraisals of self and others in predictably gendered directions (Ridgeway and Correll, 2004). Constant effort is required to conform to gendered expectations in every-day life and interactions with others, including at work; the degree or nature of this conformity may be stigmatised or subject to penalties if violations occur (Fisk and Ridgeway, 2018; Ragins and Winkel, 2011). For instance, Swan (2016) found that women police officers who report higher levels of masculinity also report lower job satisfaction because of their continued struggle to prove competence in a masculinist institution. Thus, assessing gender as the degree to which an individual conforms or not to culturally defined stereotypical beliefs about masculinity and femininity and then linking their gender conformity with health outcomes has the potential to reveal new relationships otherwise masked by binary gender identification approaches. Therefore, rather than assuming gender binaries and only administering the masculine and feminine conformity scales to their corresponding gender group, we administered both inventories to all participants, regardless of their self-identified gender. To reduce gendered social desirability biases, the conformity scales were combined to form a long-form gender norm conformity scale. This allowed participants to respond without being primed about social requirements and beliefs originally labelled by the scales as belonging to one gender group or another, thus supporting nuance and transcending typical gender binaries in measurement.
The Conformity to Masculine Norms Inventory-46 (CMNI-46) focuses on beliefs and behaviours and assesses the degree to which respondents adhere to nine hegemonic masculine norms reflecting winning, emotional control, risk-taking, violence, power over women, playboy, self-reliance, primacy of work, and heterosexual self-presentation (Parent and Moradi, 2009, 2011a). Sample items include ‘I bring up my feelings when talking to others’, ‘It bothers me when I have to ask for help’, and ‘In general, I do not like risky situations’. Cronbach’s alphas fall within the good to excellent range, from .77 to .91 (Parent and Moradi, 2009, 2011a). Evidence for acceptable convergent and discriminant validity are reported and additional validity checks support the psychometric properties of the CMNI-46 (Parent and Moradi, 2011a). Validity evidence also supports the use of this instrument with women (Parent and Smiler, 2013). Greater conformity to masculine norms is consistently associated with negative mental health outcomes (Wong et al., 2017).
Conformity to Feminine Norms Inventory-45 (CMNI-45) focuses on beliefs and behaviours and assesses the degree to which respondents adhere to nine stereotypically feminine norms concerning thinness, domestic, invest in appearance, modesty, relational, involvement with children, sexual fidelity, romantic relationship, and sweet and nice (Parent and Moradi, 2010, 2011b). Sample items include ‘Being nice to others is extremely important’, ‘I believe that my friendships should be maintained at all costs’, and ‘I always try to make people feel special’. Cronbach’s alphas fall within the fair to excellent range, from .69 to .92 (Parent and Moradi, 2010, 2011b). Additional supportive psychometric properties and evidence of convergent and discriminant validity are reported (Parent and Moradi, 2011b). Validity evidence also supports the use of this instrument with men (Lafferty et al., 2021). Research on conformity to feminine norms and the associated mental health outcomes has yielded mixed findings (Brady et al., 2016; Iwamoto and Mui, 2020).
Allostatic Load (AL), consistent with previous studies, was designed to summarise physiological dysregulation across multiple bodily systems by including the core subconstructs that support the AL metaconstruct (Juster et al., 2010; McEwen, 2015). Practicable indicators were selected based on their contributions to homeostatic functioning across multiple systems as demonstrated in the AL literature. The following components are included in our construct of AL:
Cortisol Awakening Response (CAR): Ambulatory baseline levels of salivary cortisol or the morning CAR were gathered from participants as a physiological measure of sustained stress and recovery (Chida and Steptoe, 2009). Participants used pre-labelled Sarstedt Salivettes (Sarstedt, Germany) to collect saliva immediately upon awakening, as well as 30 and 45 minutes after awakening on two different workdays. Several best practice strategies were used to increase reliability and adherence to the sampling protocol (Stalder et al., 2016). All collections took place between 3:00 and 11:45 a.m. and samples were stored in the freezer until returned to the PI. Samples were sent to Dresden LabService (Dresden, Germany) for immuno-assaying. Both Area Under the Curve with respect to Ground (AUC(G)) and with respect to Increase (AUC(I)) were calculated according to formulas outlined by Pruessner et al. (2003).
Heart Rate Variability (HRV): During observations, participants wore a Firstbeat BodyGuard2 (Parak and Korhonen, 2013) HRV monitor (Firstbeat). HRV data were analysed using the Kubios software package and the standard deviation of beat-to-beat intervals (SDNN), the root mean square of successive heartbeat interval differences (RMSSD), high frequency power (HF ms2), and total power (TP ms2) outputs were used. Reduced SDNN, RMSSD and HF are associated with anxiety disorders (Chalmers et al., 2014) and reduced SDNN, RMSSD, HF and TP are associated with clinical burnout (Lennartsson et al., 2016).
Blood Markers of AL: After the blood draw, blood samples were immediately delivered to a brokerage lab (In-Common Laboratories, ON) that treated and sent samples out for analyses of dehydroepiandrosterone-sulfate (DHEAS), high sensitivity C-reactive protein (hsCRP), insulin-like growth factor 1 (IGF-1), fibrinogen, total cholesterol (TC), high density lipoprotein (HDL), TC/HDL ratio, and glycosylated haemoglobin (HbA1c).
The MOS 36-Item Short-Form Health Survey (MOS SF-36) measures aspects of physical and mental health across eight health constructs: physical functioning, bodily pain, role limitations from physical health problems, role limitations from personal or emotional problems, general mental health, social functioning, vitality, and general health perceptions (McHorney et al., 1993; Ware and Sherbourne, 1992). Higher scores indicate better self-reported physical and mental health. Evidence of acceptable predictive, concurrent, content, criterion, and construct validity have all been reported (Ware, 2000).
Statistical analyses
Allostatic Load Scoring: Using the most common calculation method in the AL literature, we determine the high-risk quartile cut-offs for each marker (except for cortisol, which included both high and low octiles in the high-risk group) based on its distribution in our samples (Juster et al., 2010; Mauss et al., 2015) after disaggregating the data by sex (see online Appendix 1). Sex-specific cut-offs, although not standard practice, are an important recent development in the AL literature because they are thought to capture both sociocultural gender variation and within-sex diversity (Juster et al., 2016). Each participant’s AL score is calculated as the sum of the number of high-risk quartiles they are in. In accordance with prior research, participants taking medications for high blood pressure or high cholesterol have a point added to the corresponding markers if they fall below the high-risk threshold (Geronimus et al., 2006; Schulz et al., 2012). In order to account for the use of additional medications for the treatment of other chronic conditions, each participant receives an additional point for further medication use (Juster et al., 2016). To determine how the scoring for the use of additional medications affects the association between AL and stressors, we test additional models where the definition of AL does not include medication use. Main findings are unchanged, so the use of medications to treat chronic conditions remains a component of the AL score.
Independent sample t-tests were run to look for any underlying differences in the reported demographic backgrounds of women and men. Correlation analyses were then used to test for associations among AL, EL, self-reported health status and possible demographic covariates (e.g. age, sex). To assess the relative independence and contributions of the demographic and health status variables for AL, a linear multiple regression was run including any variables that had a significant correlation with AL. To measure and interpret gender as a more nuanced continuous and non-binary variable (Magliozzi et al., 2016), the sample was divided into four conformity groups according to their scores (defined in section ‘Relationship between gender norm conformity, emotional labour and allostatic load score’ below). Separate linear regressions were then run for each of the four different gender conformity groups using EL as a predictor of the outcome, AL.
Results
Demographic backgrounds
Table 1 provides the descriptive statistics for this sample. Eighty-one communicators participated: 65 self-identified women and 16 self-identified men. Participants ranged in age from 22 to 55 years (M=39) and had been working as communicators for .33 to 28.5 years (M=10.08). Women and men did not differ by demographic characteristics, apart from shift schedules. Men were more likely to work the 12-hour shift schedule and women, the 8-hour. Seventy percent of the sample had a college or university degree or higher and 66.7% were either common-law or married. Seventy-five percent reported having some chronic health complaint over the past 12 months with the highest complaint rates being for headaches (39.5%), fatigue (35.8%), backache (28.4%), insomnia (24.7%), and gastrointestinal issues (22.2%). Seventy-five individuals completed all questionnaire data; 63 individuals provided sufficient physiological data to calculate their AL scores. Of these, 59 individuals (46 women and 13 men) provided
Descriptive statistics for demographic characteristics of participants.
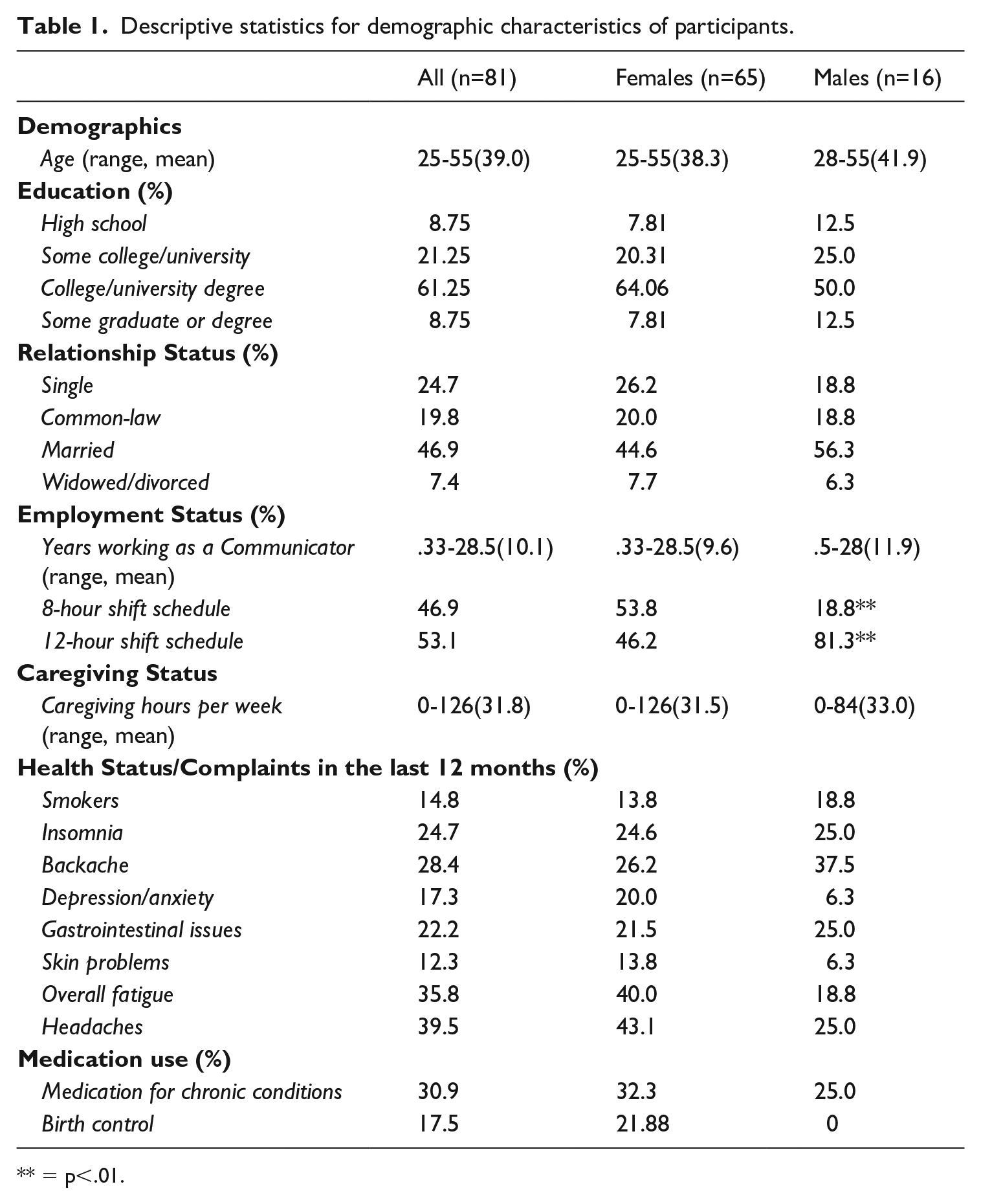
** = p<.01.
complete survey and physiological data. Appendix 1 online provides a breakdown of the physiological markers that are entered into the AL metaconstruct, each receiving a score of one if they fall within the high-risk range.
Correlations among demographic, predictor and allostatic load variables
Online Appendix 2 provides the correlation matrix for AL, predictor, and demographic variables. Importantly, birth sex (which aligns with self-reported gender in this sample) was unrelated to AL. Further, there was a significant positive correlation between AL and the number of years employed as a communicator (r=.284, p=.025), chronological age (r=.344, p=.006), and the number of hours spent caregiving during an average week (r=.276, p=.030). Those with better self-reported physical health (–.356, p=.006) had lower AL scores.
Online Appendix 3 provides the results of the multivariate regression that was run with the number of years working as a communicator entered as a predictor, in addition to variables that were found to correlate with AL: chronological age, caregiving hours, and self-reported physical health. The model predicted a significant amount of variance in AL (F(4, 51) = 6.139, p<.000), with an R square of .325. Only the physical component summary of the MOS SF-36 was a significant independent predictor of AL. Those reporting poorer physical health had higher AL scores, suggesting some degree of accordance between self-reported physical health and multisystemic dysregulation (see online Appendix 3).
Relationship between gender norm conformity, emotional labour and allostatic load score
In examining the nuanced influence of gender in a non-binary manner, the sample was separated into four gender norm conformity groups, differentiated by their degree of conformity to feminine and masculine norms (Figure 1): low or high conformity to feminine norms, low or high conformity to masculine norms. Group 1 (n=17; LF/LM) consisted of the overall low conformers, falling below the mean on both the femininity and masculinity scales. Group 2 (n=20; HF/LM) conformed high to feminine norms but low to masculine norms. Group 3 (n=20; LF/HM) conformed low to feminine norms but high to masculine norms. Finally, group 4 (n=17; HF/HM) consisted of those who were high dual-conformers, scoring above the mean on both femininity and masculinity scales. Each gender norm group comprised women and men, suggesting that patterns in gender norm conformity are not always predicated by birth sex.
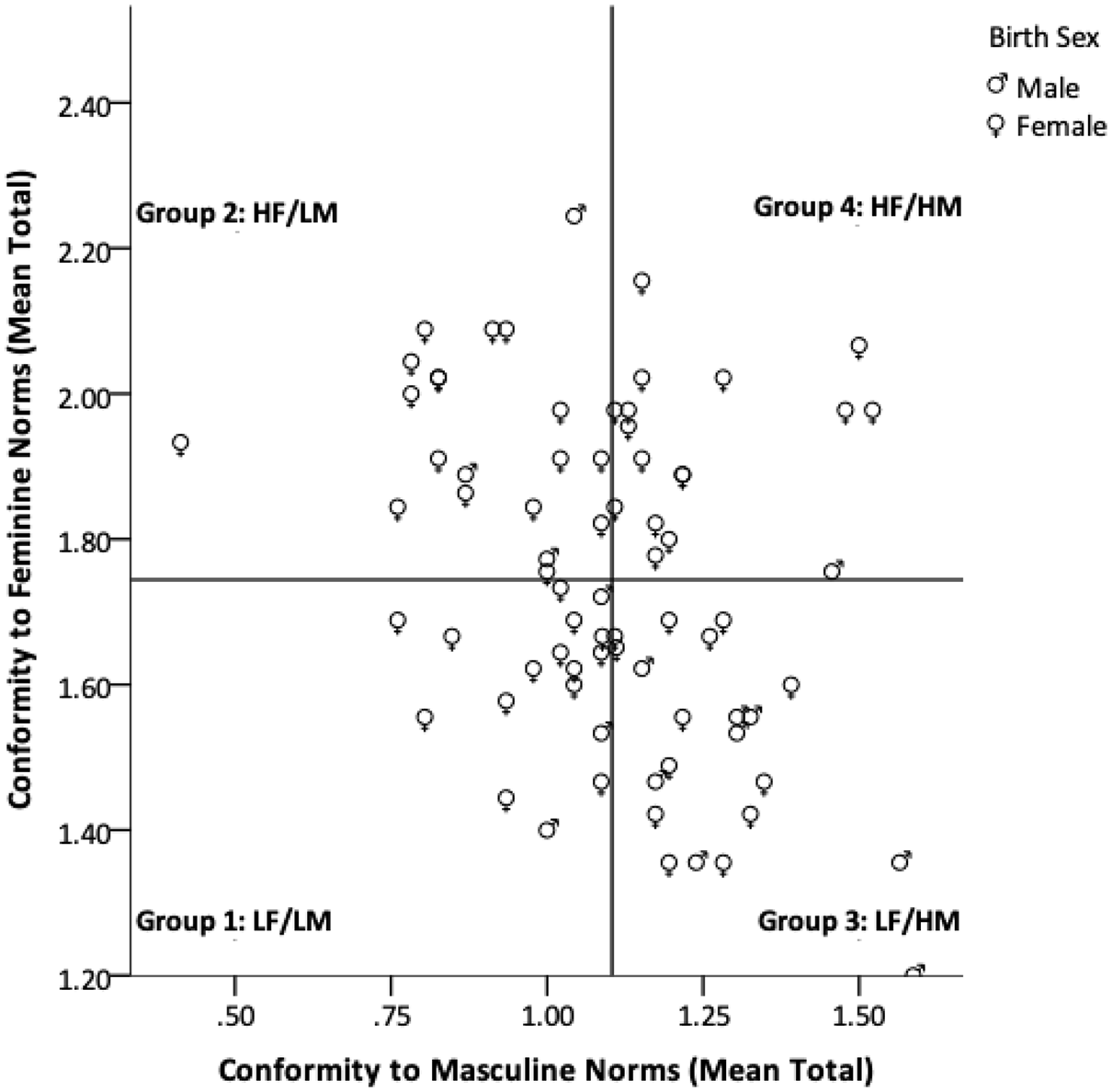
Conformity to feminine and masculine norm groups split by mean score.
Figure 2 demonstrates that gender norm group, rather than sex (analyses not reported), moderated the relationship between AL and EL. A separate regression was run for each group and EL was a significant predictor of AL only for the high feminine/high masculine dual-conformers (group 4). The model for the high dual-conformers was significant with an R square of .74 and F of 24.99 (p=.001), which suggests a strong relationship between the strength of individuals’ conformity to potentially conflicting hegemonic gender norms, their experiences of EL, and AL.
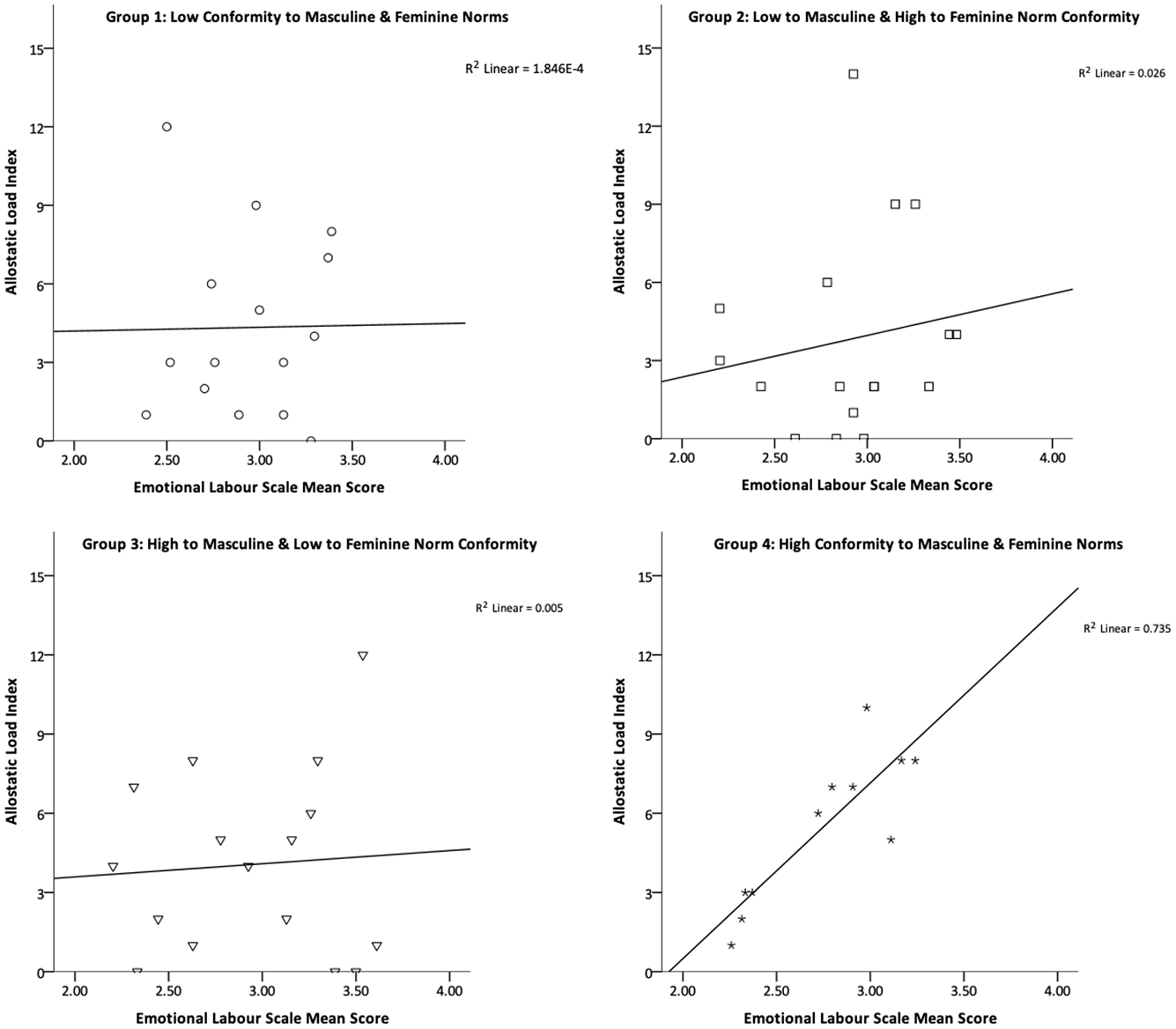
Emotional labour and allostatic load for the four gender norm groups.
Discussion
Guided by our intentions to further broaden the scope of the ‘body/work/gender nexus’ laid out by Rydzik and Ellis-Vowles (2019: 488), the primary objective of this study was to determine whether allostatic load – a framework for assessing the physiological embodiment of social conditions – might visibly link gendered workplace stressors with the physiological health of workers in non-binary ways. As might have been expected of this stressful work, the number of years working as a communicator is positively correlated with allostatic load (AL), while self-rated physical health is negatively correlated with AL. Although emotional labour (EL) was not independently associated with AL, gendered norm conformity – rather than birth sex or self-identified gender – appears to play a role in the relationship between the two. In those communicators who scored high in both masculine and feminine norm conformity, there was a strong association between EL and AL, suggesting a gendered emotional ‘double bind’ where ‘individuals can display or suppress emotions in ways that satisfy either gender or work role expectations, but not both’ (Ragins and Winkel, 2011: 382), thus creating dissonance and further distress.
Perhaps because of the gendered nature of emotional work requirements that are situated within the gendered organisation, EL becomes a powerful predictor of AL in the communications context. As the amount of EL among the dual feminine and masculine conformers increases, the greater the bodily wear-and-tear they experience, suggesting conformity to sometimes-contradictory social norms can lead to greater work-related distress and a greater burden of disease. Performing this EL requires extensive emotional expression and suppression, both of which are at times in conflict with closely-held gender beliefs for appropriate emotional behaviour among the high dual-gender-norm conformers. Importantly, the dissonance resulting from EL is most distressing when behaviours are in conflict with perceptions of the self (Grandey and Gabriel, 2015). As such, communicators may be experiencing elevated emotional dissonance in the workplace, as they aim to perform two sets of gendered and sometimes-conflicting norms with sometimes-contradictory workplace prescriptions. Notably, the same relationship between EL and AL is not present for low or polarised gender conformers.
While it is not known whether these high masculine and feminine norm conformers are perceived by others or perceive themselves as gender nonconforming, perhaps rather than being inherently harmful, gender nonconformity is distressing when it conflicts with the strictly dichotomous norms for men and women that are enacted by the surrounding social or organisational context (Heise et al., 2019; Zentner and von Aufsess, 2020). Similar findings regarding the distressing aspects of gender nonconformity show that masculine women are forced to navigate stigma and devalued gender-based expectations in the workplace (Dozier, 2017; Ragins and Winkel, 2011). Similarly, men who engage in work that is constructed as women’s work may perceive themselves – and be perceived by others – as violating normative expectations for masculinity (Nentwich and Kelan, 2014). For instance, other research has demonstrated that among men, endorsing items on the Emotional Control subscale of the CMNI-46 (used in this study) is associated with higher stress appraisals for expressing tender emotions (Yeung et al., 2015), which are sometimes required in communications work. Perhaps not surprisingly, these individuals may experience poorer mental health as a result of these distressing conditions (Yeung et al., 2015).
Policing is a hyper-masculinised occupation that can pathologise emotions and push emotional work to the margins – defining it as women’s work (Shelley et al., 2011; Swan, 2016), as we see in communications and other feminised work. For instance, other masculinised forms of labour, such as the trial attorney, have pushed emotional caretaking work to the margins into less powerful, more deferential feminised roles such as the paralegal or legal assistant (Pierce, 1999). Nonetheless, the masculinised requirement for stoicism and rational ways of thinking, feeling and doing that are evident in policing (Lumsden and Black, 2018; Yates et al., 2018) are organisationally extended to communications employees (Shuler and Sypher, 2000), who are also regularly exposed to distressing and traumatic events (Birze et al., 2020; Carleton et al., 2019) for which they must repeatedly project empathy and authority while working to calm and control their own and others’ emotional responses (Lumsden and Black, 2018). In other hyper-masculinised contexts with high trauma exposure, the distress associated with conforming to strict masculine norms is associated with the experience of traumatic stress and symptoms of post-traumatic stress disorder among men and possibly women (Christiansen and Berke, 2020; McDermott et al., 2017; Neilson et al., 2020). Interestingly, individuals working in other feminised occupations that include high demands for emotional labour as well as frequent trauma exposure, but may not be situated in a hyper-masculinised organisational context, such as child protection services, score higher on professional quality of life and wellbeing at work if they endorse both masculine and feminine gender roles, the combination of which is thought to be protective (Dufour et al., 2021).
When enacting gender creates dissonance or perceptions of threat, these dynamic short-term changes in both physiology and behaviour highlight the relational nature of stereotypical gender and associated emotional interactions that work beyond fixed identity-based characteristics. These short-term changes can, in turn, affect physiological dysregulation over the long term. As such, gender differences in stress response patterns commonly reported in the literature are less likely a story of inherent sex or gender differences per se. Rather, they are more likely a result of the salient gender dynamics and context, both in the short term and over the long term. This shift from differences to dynamics allows for a conceptualisation of gender and work as social determinants of health that are based in social relations rather than individual characteristics.
In the communications context emotional labour is realised as a form of gendered and embodied ‘body work’, extending Wolkowitz’s definition – ‘the work that human beings do on their own and others’ bodies’ (Wolkowitz, 2011: 177) – to bodies that are physically distant from one another. Communicators ‘work on their own bodies’ in accordance with workplace requirements for emotional control as they manage potentially traumatic incidents, as well as a myriad of other emotion-inciting interactions, while simultaneously working on ‘other people’s bodies as a component of their jobs’ by bridging the gap between bodies through the voice transmission of critical embodied information (Wang, 2020; Wolkowitz, 2011: 179).
Conclusions
As Krieger (2005) argues, embodiment is a process whereby our ‘terms of engagement’ with the social world are translated into bodily characteristics over time or, as Einstein (2012: 160) says, ‘the world writes on the body’. Unfortunately, most stress and health research does not conceptualise gender as a social structure that is more complex than a binary trait that matches one’s sex assigned at birth. However, as Young (2002: 422) states, ‘an important conceptual shift occurs when we understand the concept of gender as a tool for theorizing structures more than subjects’. Given that the conditions often associated with feminised work – like high emotional demands, low work-time control, and exposure to violence – have particularly striking effects on health (Roelen et al., 2018), gendered discrepancies in exposure to work-related stressors invite further examination of workplace contexts and their effects on wellbeing. As our research with communicators suggests, it is the rigidity of the gender structure – including sanctioned and unsanctioned conformity to gendered emotional norms – that influences health through the organisation of work, rather than being a man or woman, a male or female, per se. For high dual-gender norm conformers, EL is an embodied struggle; a process whereby EL leaves traces of the gender structure in the flesh in the context of repeated exposure to potentially traumatic incidents in a highly emotional yet masculinised environment.
By listening to the stories bodies tell about the lives we experience, it is therefore possible to both contextualise and move beyond the limits of what people are willing or able to recount (Einstein, 2012; Krieger, 2005). An embodied study of emotional experiences recognises that physical bodies – in conjunction with recounted experiences – are also a manifestation of experiential knowledge. Thus, the experience of stress and associated hormonal responses is one mechanism through which we can examine how the social penetrates the body and gets under the skin to differentially construct material realities, including health inequalities (Freund, 2006). This research begins to demonstrate how gender, as a social structure, might simultaneously influence the organisation of work, the interactional expectations of others, and patterns of internalised norms. In turn, each produces differentiated emotional experiences that enter the body through neurohormonal pathways, thereby shaping the body’s physiological, material reality (Pearlin, 1989). In order to see this, however, we must eschew common dichotomous conceptions that mask the reach of gender structures and obscure the fleshy depths of the body/work/gender nexus.
Supplemental Material
sj-pdf-1-wes-10.1177_09500170221080388 – Supplemental material for Gender in the Flesh: Allostatic Load as the Embodiment of Stressful, Gendered Work in Canadian Police Communicators
Supplemental material, sj-pdf-1-wes-10.1177_09500170221080388 for Gender in the Flesh: Allostatic Load as the Embodiment of Stressful, Gendered Work in Canadian Police Communicators by Arija Birze, Elise Paradis, Cheryl Regehr, Vicki LeBlanc and Gillian Einstein in Work, Employment and Society
Footnotes
Acknowledgements
The authors thank Jessica Scott for her help with the study, Nicole Gervais for her assistance and statistical support, and Walter Tavares and Annie Duchesne for their comments on earlier versions of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: This research was supported in part by funding from the Wilson Centre Currie Fellowship (AB), research start-up funds provided by the Faculty of Medicine, University of Ottawa (VL), Social Sciences and Humanities Research Counsel (CR), Wilfred and Joyce Posluns Chair in Women’s Brain Health and Aging (GE), and The Jacqueline Ford Gender and Health Fund (GE).
Supplemental material
Supplemental material for this article is available online.
![]()
![]()
![]()
![]()
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.