
Abstract
This article investigates reproductive work in the Global South which thrives on the commodification of women’s reproductive bodies under local-global reproductive hierarchies, appropriating the process of reproduction for production. Through a qualitative study of commercial surrogacy in north India, it examines the lived experiences of surrogates within the capitalist social relations they are embedded in. Conceptualising surrogacy as reproductive labour which contributes to value generation, the article assesses labour relations at the workplace, for example hostels where surrogates ‘live and work’, and the mechanisms of recruitment, contracting and control which function through dense networks of social and material relations between various stakeholders. The weak bargaining power of surrogates and the immense power of fertility clinics and agents are compounded by the lack of effective regulation and the state’s prohibitionist policy. The article argues for protecting the rights of surrogates as workers rather than the recent ban on surrogacy imposed in India.
Introduction
Surrogacy, and commercial surrogacy in particular, is a morally contentious and politically contested terrain which generates intense discussions. Surrogacy is a stark example of appropriation of social reproduction for production. In surrogacy, the commodification of women’s reproductive bodies and advances in reproductive technologies transform the process of reproduction into production, rendering women’s bodies as sites of work. These developments have not only led to the flow of medical information and technologies from the Global North to South, but also enrolled poor and marginalised women as informal labour into what Cooper and Waldby (2014) call ‘clinical labour’ under neoliberal globalisation. Underpinned by inequalities of class, race, gender and geography, surrogacy is a complex form of reproductive labour that is intimate, emotional and embodied, much like other forms of paid body labour in the increasing commodification of ‘new’ sites and spaces of work (see McDowell, 2014; Wolkowitz, 2002; Wolkowitz et al., 2016). The extensive growth, commercialisation and transnationalisation of the surrogacy industry in recent decades brings longstanding as well as recent debates to the fore. The first concerns the significance of social reproduction in value generation under capitalism (Federici, 2012; Fortunati, 1989; Kofman and Raghuram, 2015; Mies, 1986), posing the question: is surrogacy productive? The second, and more recent, concern is ‘to ban or not to ban’ surrogacy because of the intricate nature of ‘mothering labour’ it involves and the associated ethical dilemma regarding the commodification of motherhood and babies. This article conceptualises surrogacy as a conscious, life-giving, meaningful social activity which creates value (see also Pande, 2014; Rudrappa, 2015; Vora, 2019), resonating with earlier scholarship on the significance of social reproduction. Through the case of commercial surrogacy in north India, it engages with the more recent question of ‘to ban or not to ban surrogacy’; India banned surrogacy in January 2020. By combining the lived experiences of surrogates with the social and material relations they are embedded in, the research captures the complexity of surrogacy labour and industry and assesses the ban against the contextual reality and the totality of experiences in India.
India is an interesting context to study as a key player in the multi-billion-dollar global reproductive industry and as one of the largest suppliers of commercial surrogates. Almost 3000 largely unregulated surrogacy clinics are said to have mushroomed all over the country since commercial surrogacy was legalised in 2002 with thousands of working class, typically married women, in their 20s and 30s bearing babies for commissioning parents from overseas and India. The Indian Council of Medical Research defines surrogacy as an arrangement where a woman agrees to carry and give birth to a child where neither of the gametes belong to her or her husband, with the intention to hand over the child to the commissioning parent or the couple for whom she is acting as a surrogate (Government of India, 2008, 2016). India also has one of the largest and growing informal economies in the Global South where almost 93 percent of workers are informal, that is in insecure and unprotected employment, with women working in the lowest rungs (Hammer, 2019). Surrogate workers join this increasing informal labour. Furthermore, surrogacy remains highly contested in India. The state’s approach has veered from a medico-liberal, contract-based model in the 1990s, to a familial model that prohibited surrogacy for foreign nationals in 2015 and sought to prohibit commercial surrogacy altogether (Government of India, 2016; Kotiswaran, 2018). In the current prohibitionist, carceral model, progressive bans on surrogacy for various groups of people have culminated in a complete ban on all forms of surrogacy in January 2020. The research presented in this article is timely. Conducted in 2016–17, it covers the period between various bans and the total abolition of surrogacy in 2020, which helps interrogate the policy which can have serious and lasting implications for surrogates and the industry.
The article examines the labour relations and structural inequalities in the commercial surrogacy industry in north India. It assesses workplace relations, for example hostels where surrogates ‘live and work’, and the mechanisms of recruitment, contract and control which function through complex social and material relations between fertility clinics, doctors and surrogacy agents. Predominantly migrant women from deprived socio-economic backgrounds with low levels of education work as commercial surrogates. The inequalities in the labour market are reflected in the employment contracts and working conditions which restrict mobility, autonomy, decision-making capacity and bargaining power of informal surrogate workers while according immense power to other stakeholders. The unequal power relations are compounded by lack of effective regulation and the state’s prohibitionist policy. At the same time, the multi-layered experiences of surrogates highlight surrogacy as a survival strategy or a temporary livelihood strategy of the vast majority of informal women workers with limited alternative economic opportunities, where surrogates are active agents who understand and manage their realities albeit within structural constraints. They negotiate their multiple identities as mothers, workers and participants in an unfamiliar and commercialised industry. They manage the complex nature of their labour and the associated stigma and alienation. Importantly, they attempt to exercise some choice at home and at the workplace to counter their weak bargaining position.
This complexity of informal surrogacy labour poses difficult questions regarding banning surrogacy: would abolishing surrogacy stop the exploitation of largely poor and socially disadvantaged women in the South? Would they continue to participate in the industry for the complex and multiple reasons that underpin their choices? Would abolition impact on the structure of the industry and what would it mean for surrogates? Quite evidently, the reproductive labour of informal migrant workers is devalued through secrecy, surveillance and control while creating value for other stakeholders. Nevertheless, the article argues that the answer does not lie in abolishing surrogacy. It would not stop the exploitation of informal surrogacy labour. Surrogates would continue to participate in the industry for the complex and multiple reasons that underpin their choices. Abolition is likely to push the already unregulated commercial surrogacy industry underground or abroad or restructure it, potentially exacerbating exploitation and further weakening the bargaining power of surrogates. Instead, recognising surrogacy as labour and surrogates as productive workers and empowering them through stronger labour laws would be more helpful.
The article is structured as follows: the next section situates commercial surrogacy in the debates in feminist political economy and studies of work and employment. Section three details the research design and methods. Section four presents the findings through the lived experiences of surrogates and mapping the local labour relations and power dynamics in the commercial surrogacy industry. Findings are discussed and conclusions are drawn in section five.
Surrogacy labour in globalising capitalism
Commercial surrogacy animates intense feminist, ethical, legal and social debates. While liberal feminists defend the right of a woman to use her body the way she chooses, for others the commodification of women, motherhood and babies as labour is troubling and poses a moral dilemma. Here, the bond between a mother and her child is assumed to be fundamentally different from the bond between a worker and his/her product. As motherhood becomes work, and children the product of the labour of mothering, there is ‘commodification of children and the proletarianization of motherhood’ (Rothman, 1989: 66). Yet, others take a more nuanced view. Such moral dilemmas notwithstanding, the commodification of reproductive labour (and surrogacy) is an empirical reality and its theorisation by feminists has historical antecedents and recent interventions (e.g. Cooper and Waldby, 2014; Kofman and Raghuram, 2015; Mies, 1986; Pande, 2014; Parry, 2015; Vora, 2015). Whether a moral issue or as reproductive labour, surrogacy also generates strong views regarding its abolition or regulation by the state (Dickenson, 2017; Kotiswaran and Banerjee, 2021; Pande, 2017).
This section builds on the scholarship that conceptualises surrogacy as reproductive labour which contributes to capital accumulation, while emphasising the contextual factors and lived experiences of surrogate workers. The next two subsections engage with the theorisation of surrogacy as labour, followed by a discussion on the relevance of lived experiences and contextual factors to understand the complexity of surrogacy.
The ‘value’ of surrogacy labour: Clinical labour and social reproduction
Cooper and Waldby (2014) theorise how reproductive work – gestational surrogacy among others such as clinical trials, invasive biomedical procedures, tissue extraction – has become constituted as a form of economically productive ‘clinical labour’ under neoliberal globalisation. They define clinical labour as ‘the process of material abstraction by which the abstract, temporal imperatives of accumulation are put to work at the level of the body’ (Cooper and Waldby, 2014: 12). The reproduction process is made alienable and each segment of reproductive biology is hyper-medicalised, with workers/bodies of the workers treated as disposable commodities (elaborately captured in the literature on body work e.g. Wright, 2006). Rising informalisation and precarisation of employment sees reproductive labour increasingly contractualised and transnationalised; brought out of the home into the clinics and into capital accumulation processes echoing the earlier historical gendered and racialised division of labour in the commercialisation of other intimate relations such as care work and sex work. This insecure and unprotected clinical labour bears all the risks under the guise of contracts and the rhetoric of choice. The structural inequalities inherent to the reproductive industry are sharply evident in the Global South where it has gained both its resource base and markets. India and China have emerged in the international market as developers of biotechnologies and suppliers of reproductive materials, intensifying the forms of its feminised labour, mainly minority and migrant women (Cooper and Waldby, 2014). The phrase ‘market in life’ aptly describes the ways in which reproductive markets are assembled by people from the margins of society, as well as scientists, doctors, pharmaceutical products, and customers from more privileged sections of society (Rudrappa, 2015).
Clinical labour, however, is underpinned by binary assumptions (Fordism/post Fordism, social production/reproduction, male manufacturing/post-industrial visceral processes), and neglects the link with other longstanding forms of paid body work (Wolkowitz et al., 2016: 1040). Here, early Marxist feminist debates are relevant, which emphasise the significance of the reproductive realm and its interlinkages with production in value creation under capitalism (Federici, 2012). Questioning the distinctions between private/public, nature/social, reproduction/production and non-market/market, early theorists identified such distinctions as the basis of the asymmetrical and patriarchal division of labour where the concept of labour is reserved for men’s productive work while women’s share in production and reproduction becomes a function of their biology and nature. The act of giving birth or ‘labour’ is assumed to be not labour or work but rather an activity of nature. Fortunati (1989) details how reproductive labour has a dual function in capitalism: while work performed in the private sphere is devalued, the value created is channelled into the capitalist system through the visibly productive workers who consume it. In order to challenge the asymmetrical division of labour, Mies (1986) argues that it is critical that women’s activity in bearing and rearing children be understood as a conscious social activity: and as ‘work’. Following from this, although gestation is not recognised as labour per se because the surrogate mothers do not perform codified, quantifiable tasks, ‘they offer them-selves up as subjects, giving clinics access to the productivity of their in-vivo biology, the biological labour of living tissues and reproductive processes’ (Waldby and Cooper, 2008: 59), surrogate mothers are workers in a Marxian sense because in-vivo processes of oogenesis and gestation create surplus value. Surrogacy is labour, a form of reproductive labour, that is a conscious, life-giving, meaningful social activity (Rudrappa, 2017).
Surrogacy as intimate, embodied and emotional labour
The integration of paid body labour in the capitalist economy and the recognition of bodies, emotions, and sexualities as sites of commodification is gaining increasing attention in studies of work and labour process (e.g. Hochschild, 2011; Wolkowitz et al., 2013). In surrogacy, production and reproduction are integrated and women’s bodies are used as sites of economic production. Yet, surrogacy labour is more than just labour as Marx may have described. Not surprisingly, surrogacy is a troubling form of reproductive work and labour.
As Pateman (1988: 207) suggests, a woman’s reproductive labour is ‘more integral’ to her identity than her other productive capacities and hence should be treated differently. The way ‘gestation and childbirth are imbricated with the body and subject of surrogate makes it difficult to distinguish between what is labour and what is not’ (Vora, 2019: 42). There is also the social location of surrogacy as ‘mothering labour’ with associated cultural and economic weight. The nature of surrogacy labour alienates the woman from her body and from her ‘normal’ emotions. Commercial surrogacy, similar to sex work, represents a form of labour practice that demands only the biological structure of the body for production. The surrogate as a mere carrier or a means of production becomes invisible in the process. However, the idea of a mindless body in the social relations of work has been challenged by corporeal feminists (e.g. Rudrappa, 2015; Wolkowitz, 2002).
Considering the complex nature of labour it involves, commercial surrogacy in this article is associated with forms of intimate, embodied and emotional labour. It is where bodies and emotions are both the subject and object of labour. It is an intimate and gendered form of labour which extends into the private and intimate sphere of sexuality and reproduction, and involves ‘embodied and affective interactions in the service of social reproduction’ (Boris and Parreñas, 2010: 7). It is intimate in nature, similar to sex /domestic/body work, since it involves maintaining and managing interpersonal ties by tending to the bodily needs of the recipients. The surrogacy industry is an intimate industry, with its institutionalisation of intimate labour and the unequal relationships between various actors engaged in intimate exchanges (Rudrappa, 2017).
The association of surrogacy with embodied and emotional theories of labour is also based on the idea that the labour it produces is immaterial in nature, i.e., the commodity is not simply a material entity, that can be bought, consumed and discarded, but has lasting and deep social and cultural implications (Lazzarato, 2006). Crucially, commercial surrogacy as emotional labour highlights the emotional conflict of surrogates: emotional detachment is a key part of the contract, at the same time as the women are expected to act as a caring mother. This mother-worker and producer-reproducer dualism lays the framework of exploitation in the commercial surrogacy industry (Pande, 2014).
To sum up, surrogacy is ‘exemplary of the ways in which the extension of capitalist relations deepens the social hierarchies and the colonial structuring of the global economy, with the further racialisation of the activities considered to be of least value, beginning with the process of procreation itself’ (Federici, 2019: 57). Recognising surrogacy as work and labour, along with other forms of reproductive labour, brings to attention surrogate workers who are joining the ranks of informal labour in the South with limited alternative economic opportunities and susceptible to exploitation under unequal power relations, as also the multiple bases of inequality in this form of labour (Vora, 2019). Importantly, this recognition allows a move beyond moral discussions to the dynamics of surrogacy outside the sphere of reproduction (Pande, 2014) – to an analysis of how a surrogacy labour regime is instituted, how recruitment and control function, and how surrogate workers negotiate and resist these mechanisms.
Lived experiences of surrogate workers embedded in wider capitalist social relations
The wider theorisation of surrogacy as ‘clinical labour’ and ‘reproductive labour’ and the intricate nature of labour it involves is accompanied by calls for an examination of the ‘complex lived experience of clinical labour in situ’ so as not to miss key contextual factors (Parry, 2015: 37). It examines surrogacy work as embedded in an intertwined network of social relations between surrogates, agents, medical personnel, family, community and the state; capturing the nuanced experiences and agency of surrogates along with the power relations in the surrogacy labour process and the wider social relations.
There is rich ethnographic scholarship on India which is empirically grounded in the lived experiences of surrogacy (Pande, 2014; Rudrappa, 2015; Vora, 2015). The intricacies of surrogacy reveal how surrogate mothers find themselves in an unfamiliar relationship with a hyper-medicalised system of reproduction, a medical system that has previously been inaccessible to them as socially and economically underprivileged women. The women navigate multiple identities as mothers, workers and as participants in an industry that is fast-growing and morally contentious. As women hired by commissioning parents and clients from within and across borders, they also navigate relationships that often cross boundaries of race, class and nationality.
A focus on lived experiences of surrogates allows a move beyond surrogates as mere victims to active agents who understand, manage and negotiate their realities albeit within the structural constraints of the global-local reproductive industry. It brings to light the choices surrogates make and the meaning they derive from or ascribe to these choices. For many, surrogacy is a survival or temporary livelihood strategy in the face of their structural constraints; often coerced, some negotiate with their families to gain control over their own bodies and their fertility in order to participate in the industry (Pande, 2014; Parry, 2018). Though highly stigmatised in India, surrogates counterbalance it by seeing the activity of bearing a child for someone else as philanthropic, even divine, and expect ongoing social relations and support by the commissioning parents. While the need for income is key in the decision to become a surrogate, surrogates often refute the alienation of the commercialisation of their surrogacy through the contract, as paid service of gestation, by insisting on its meaningfulness beyond the labour contract. This suggests the possibility of surrogacy as a site of contestation, or even resistance (Vora, 2019: 45).
This article contends that the understanding resulting from the multi-layered experiences of surrogates and the wider social relations can help better interrogate policy approaches, such as a ban on surrogacy, which can have serious and lasting implications for surrogates and the industry. India has traversed from a medico-liberal, contract-based model in the 1990s, to a familial model that prohibited surrogacy for foreign nationals in 2015 and sought to prohibit commercial surrogacy in the Surrogacy (Regulation) Bill, 2016, to the current prohibitionist, carceral model culminating in a ban on all forms of surrogacy in January 2020 (Kotiswaran and Banerjee, 2021). However, the reality of informalised reproductive labour in India, and the South, raises difficult questions: would abolishing surrogacy stop the exploitation of largely poor and socially disadvantaged women in the South? Or would they continue to participate in the industry for the complex and multiple reasons that underpin their choices? Would abolition restructure the industry and what would it mean for surrogates? The article investigates these pertinent issues within the framework of commercial surrogacy as reproductive labour with greater attention to contextual factors and the embodied and lived experiences of surrogate workers. The methodological implications are discussed next.
Research design and respondents
This research is a qualitative study of commercial surrogacy in the National Capital Regions of Delhi (NCR) in north India. The research was conducted between October 2016 and April 2017. Commercial surrogacy for foreign nationals was banned at the time of the research, and all forms of surrogacy has been outlawed in 2020. This research, conducted in between the two bans, is revelatory and pertinent to debates around regulating or banning surrogacy in India, and more broadly.
The research design was guided by a focus on the lived experiences of commercial surrogates embedded within the social and material relations of the industry to identify the unequal power relations and the background within which these inequalities emerge (Pande, 2014; Parry, 2018; Rudrappa, 2015; Vora, 2015). A snowballing technique was used owing to the nature of the research where potential informants were hard to identify or locate. In the absence of any estimate of infertility clinics and hospitals in India that offer surrogacy services, it was difficult to follow a systematic approach in selecting the fertility clinics or respondents. Instead, the clinics were selected with the help of the All India Fertility and IVF ranking survey. Out of the seven clinics selected, the research covered four fertility clinics. The remaining three were e-mailed but only one clinic responded. In this clinic, an informal conversation took place with the media relations officer, and an appointment was scheduled with the doctor and the founder of that clinic but the doctor cancelled the interview later. Multiple visits to these clinics and in-depth conversations with doctors and fertility experts contributed to a clear understanding of the ways in which the production process takes place. The interaction with the doctors was often fraught with many refusing to cooperate.
The surrogates were identified through referrals from doctors, agents, and friends of respondents. One doctor introduced the researchers to an agent working at a surrogacy agency, who also recruited women for egg donation. The agent informed the researchers about a surrogacy agency running a surrogacy hostel and helped in scheduling a meeting with the owner of that agency. The owner agreed to let the researcher interview the surrogates only if the name and the location of the hostel were not disclosed.
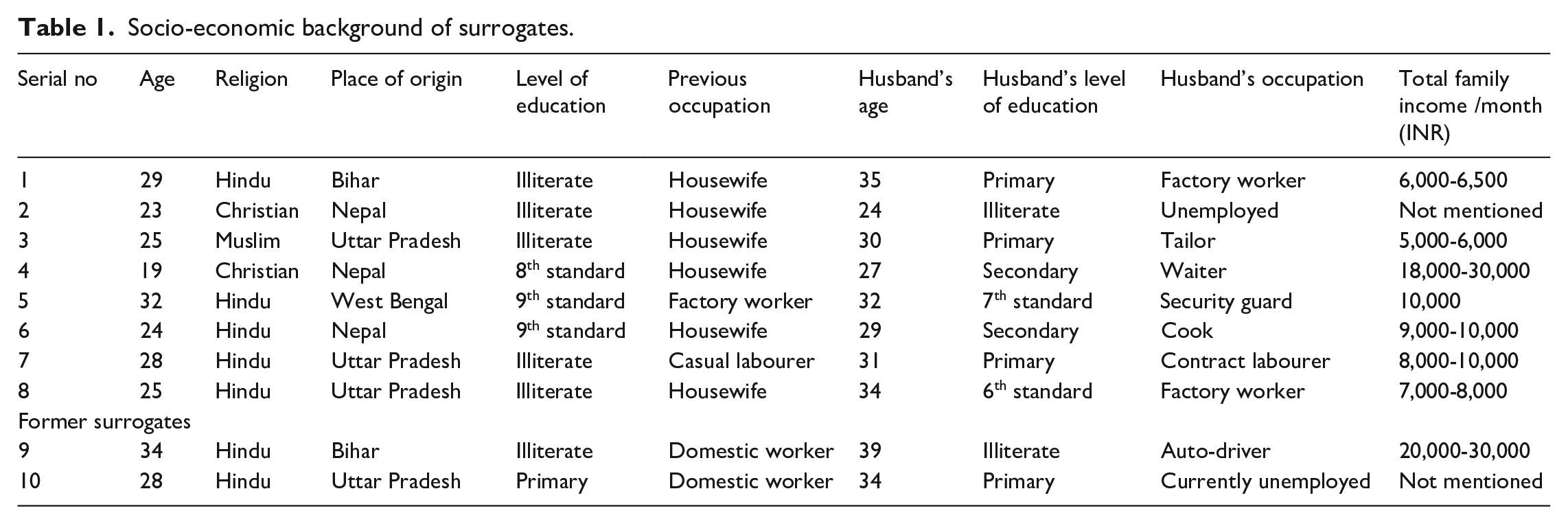
The case study design involved eight surrogate mothers in a surrogacy home for a period of two months. Two former surrogates were also interviewed at their homes on the outskirts of Delhi. All ten surrogates were married, with at least one child. Their ages ranged between 19 and 34 years. All surrogates were either internal rural migrants (other states in India) or external migrants (Nepal) who came from impoverished backgrounds with limited education and occupational opportunities. Their education ranged from illiterate to secondary school level and they laboured in the lowest rungs as domestic workers or hired labour. Their average family income was around Indian Rupees (INR) 10,000, insufficient to maintain a family in Delhi and was often the prime motivator for their decision to become a surrogate. Tables 1 and 2 provide details of the surrogates interviewed.
Socio-economic background of surrogates.
Women’s experiences as reproductive labourers.
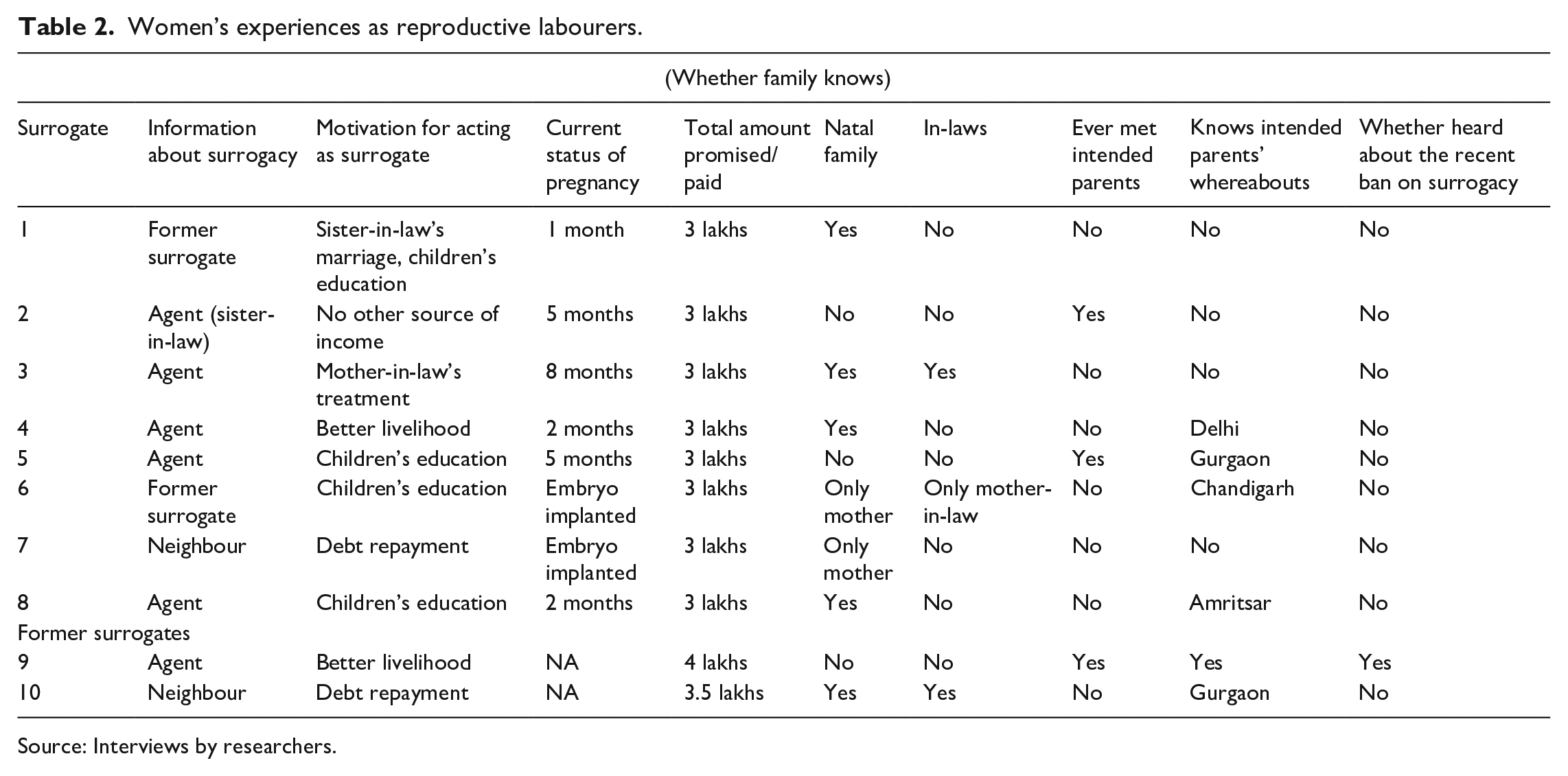
Source: Interviews by researchers.
A key aspect of the research was to present a description of the surrogacy hostel as the workplace of surrogates, where the labourers (or their bodies) are put to work for nurturing, crafting and developing the commodity. Surrogates stay in the hostels for the entire duration of their pregnancies, including occasional visits to hospitals and clinics. It was convenient to interact with the surrogates and observe their daily schedule in the hostel. The hospitals and clinics are also crucial in this scenario, but the doctors did not grant permission to conduct interviews in clinical settings. The conversations with the surrogates explored themes around their socio-economic background, reproductive history, reasons/motivations behind their decision to work as a surrogate, their perceptions about surrogacy, and their experiences in the hostel during pregnancy. Spending hours in the surrogacy home over 11 visits, constant interaction with the surrogates and observing their daily activities added to the depth and quality of research. The majority of surrogates were not aware of the intended parents or their whereabouts, or of the proposed ban on commercial surrogacy in 2016.
Particular attention was paid to identifying and interviewing all stakeholders in order to create a holistic picture, for ensuring reliability and to understand the complex web of networks in which surrogacy was embedded. These included doctors, owners and staff at the surrogacy agency. Interviews with the staff of the surrogacy hostel were conducted mainly through informal interactions during their working hours. Other interviews included an owner of the surrogacy agency and two surrogacy agents associated with two different surrogacy homes. Two doctors specialising in infertility treatments were interviewed in a fertility clinic.
The research process was reflexive and iterative. The Jawaharlal Nehru University and British Sociological Association’s ethical norms were adhered to regarding informed consent, voluntary participation, anonymity and data security. Written consent forms (translated in Hindi) were obtained from each participant. Data were collected through a combination of workplace observations and interviews. In-depth, semi-structured interviews were conducted in different settings, ranging from private fertility clinics, public hospitals and research institutes, surrogacy hostels, and private households. The interviews with surrogates took place in Hindi as per the preference of the surrogates. The rest of the interviews (with doctors, agents, agency owners) were conducted either in Hindi or English depending on the participant’s preference. Both researchers are fluent in Hindi and English. Interviews with surrogates lasted over several visits and hours, while other interviews ranged from 30 minutes to one hour. Although agents and doctors assisted with the identification of surrogates, the interviews were conducted in the absence of the medical personnel, facilitating a manipulation-free environment for the interview. Each recorded interview was transcribed and translated verbatim. In addition, field notes, general observations and workplace observations were documented as accurately as possible, ensuring minimum bias. The findings are presented in the next section.
Lived experiences of surrogates and social relations of commercial surrogacy in India
This section details the lived experiences of surrogates to capture the complexity of surrogacy labour and how this devalued labour creates value for fertility clinics, doctors and surrogacy agents in the Delhi NCR region. After providing an insight into the background of surrogates, it proceeds to examine recruitment, employment contracts, wages, working conditions, risks and bargaining power of surrogate workers and how they negotiate the multiple dilemmas facing them.
Background, motives and recruitment of surrogates
All surrogates came from socially disadvantaged backgrounds. They were either internal rural migrants or external migrants with associated disadvantages of poverty, lack of networks of support and for access to employment.
Sabita, a mother of two, came to Delhi from Nepal. Her husband was unemployed and suffered from alcohol use disorder, leaving her in desperate need for money to raise her two children. Rubina’s parents died when she was three years old, and she was raised by her paternal uncle in a village in Uttar Pradesh. She was never allowed to attend school. She had to work all day while her cousins went to school. When she got married at 18, her uncle refused to pay for the expenses of her marriage. Her life after marriage was better, but not without extreme financial difficulties. Her husband was a tailor but his income did not suffice for the family. Pratima came from a town in northern West Bengal and was educated till the ninth grade before getting married at the age of 14. Her husband did not study after seventh grade and could not find a job with reasonable pay to support his children and parents. Their financial condition worsened after Pratima had three children. They moved to Delhi but did not earn enough to survive in Delhi and send money back to the parents.
The education of surrogates varied from illiteracy to secondary school level, providing them with limited occupational opportunities. Of the ten, six were ‘housewives’ and the remaining four laboured in the lowest rungs as domestic workers or hired labour. Their average family income was around INR 10,000, insufficient to maintain a family in Delhi. Their husbands were unemployed or employed in informal or contract work. In contrast, the women as surrogates could earn between INR 300,000 and 400,000 (£ 3000–4000). Their reasons for surrogacy ranged from being able to pay for children’s education, family member’s marriage or medical treatment, to debt repayment, emphasising surrogacy as a survival strategy of many women in India.
The surrogates were recruited through former surrogates, midwives or dais, neighbours or agents. Rubina came to know about surrogacy from a woman in her neighbourhood, who had been a surrogate and now worked as a recruiting agent, and often came to her husband’s tailoring shop. Pratima was looking for work as a domestic help and the woman helping her suggested surrogacy as an option. Sabita was recruited through her sister-in-law, who worked as a recruiting agent in Delhi. The recruiting women have intimate reproductive knowledge, economic information of neighbouring households, or experience of surrogacy; therefore, finding and recruiting potential surrogates is easy for them. Most agents are recruited by the surrogacy agencies or fertility clinics, and they go from door to door in the villages, or in slums in urban areas, places where people live in poverty and are easier to convince.
Workplace dynamics: Labour contract, control and risk
This section details how the working-class background of surrogates as well as the secrecy and control by the middlemen ensured that surrogates had inadequate understanding of the contracts they signed and the risks they bore. This was accompanied by their confinement and control in surrogacy hostels, where they ‘live and work’.
The surrogates had little or no understanding of the surrogacy contracts, nor any idea of its legal enforceability in case of breach of contract. They were also unaware of the ART Bill (Government of India, 2008) which defines the rights of both parties (the surrogates and the intended parents), or the proposed ban on commercial surrogacy. They received inadequate counselling by the clinics and were told to simply follow instructions. When asked how well she understood the contract, Rupa, a surrogate in her mid-twenties replied: They gave us forms after forms; it took hours to sign them. But everything was written in English, so I could not understand a single thing. Only one page was written in Hindi, giving a short description of the processes and the rules.
In the fertility clinic all transactions from the clients and hospitals were strictly mediated by Mr Sharma, the owner of the agency and the hostel. None of the surrogates had any interaction with the commissioning couples regarding their payments. Mr Sharma offered INR 300,000 (£3000/US$4000) to every surrogate hired through his agency, and any kind of bargaining was not allowed. The amount paid to Indian surrogates is considerably lower than other countries. For instance, commercial surrogates in the United States are paid (all figures in US$) $20–30,000 (Finkelstein et al., 2016); $24–29,000 in Russia (www.surrogacy.ru, 2017) and $10–25,000 in Israel and Canada (www.surrogacy.ca, 2015). Leela, who was offered the same amount as everyone, tried to bargain for a higher amount but did not have the choice to walk away: They told me, this is the last amount we can offer, stay if you are okay with it, otherwise you are free to go.
Along with the monetary transactions and contracts, the communications between the surrogates and intended parents were also strictly monitored. Of the ten surrogates, five knew of the whereabouts of the commissioning parents, and only three had met them. The surrogates were not allowed to contact the intended parties and were not provided with their names or contact information. Rubina had never met the commissioning parents. They never visited her in the hostel, nor did she ever see them in the fertility clinic. Despite her requests, the hostel matron did not reveal anything about the parents except the fact that they live somewhere far away.
All I know that they are not from here (Delhi), but I do not know their names, I don’t have their phone numbers either. We are strictly forbidden to contact the parties (commissioning parents) directly.
The secrecy and the monitoring make it easier for the mediators to put the women in a vulnerable position as labourers.
Informed consent was absent. The agents provided the surrogates with a rough idea about the clinical tests, but no information regarding risks, the kinds of medical interventions they would eventually undergo, and long-term health consequences was provided. The women had limited understanding of the risks associated with in-vitro procedures, gestation, or postnatal complications. Nor was there any discussion about post-natal care. Asha underwent multiple rounds of embryo transfer (ET) process. However, the first attempt was a failure. Asha was desperate so she refused to give up and underwent the second cycle of ET, this time too without success.
In the beginning, the reports would show promising results, I would take the medicines religiously, but for some reason, I was not able to conceive.
Asha lived in the hostel for the first three months undergoing four failed cycles of ET without a contract and without any payment. The surrogates got a contract only after conceiving. Though legally entitled to some compensation if implantation fails, agencies often do not pay them in order to maximise their own earnings or accrue savings for clients. Asha was planning to donate her eggs and go back to Nepal with whatever money she could make. Other surrogates in the hostel encouraged her to try one more time, and after the fifth cycle of ET Asha was able to conceive.
Even though almost all surrogates had delivered their own children vaginally, delivery through caesarean surgery at weeks 36 to 38 of gestation appeared to be the norm. Rubina, a surrogate in her last trimester, speculated about it. She had her daughter through normal delivery assisted by a midwife. When asked if the doctors have informed her about the forthcoming delivery, she replied, We are not told that much. There were two women before me (surrogates who left the hostel after delivery) who had caesarean deliveries.
While the risks were passed on to the surrogates under the guise of ‘choice’ and contracts, once pregnant they were controlled through multiple mechanisms, most strikingly at the hostels. Surrogacy hostels were the workplaces, along with the clinics and hospitals, where the workers (or their bodies) were put to work in a highly controlled environment which restricted surrogates’ lives and mobility. The women lived under constant surveillance. CCTV cameras were installed all around the house. The hostel had a total of five staff, a cook who came twice a day to cook meals for the surrogates, a nurse who took care of the surrogates, a helper who ran errands, and two employees who took the surrogates to the hospitals for their medical check-ups and tests.
The surrogates followed a strict, mundane and fixed routine during their entire stay in the hostel. They woke up around nine in the morning and had their tea and breakfast. Lunch was served at one, after which the surrogates usually took an afternoon nap or took a stroll in the small garden or watched television. They had their evening tea at 5.30 pm, and dinner was served at 8.30 pm. The menu remained almost the same, and the surrogates who had undergone embryo transfers were not allowed to eat non-vegetarian food. Only after the first trimester could they eat egg, fish or meat. The nurse explained: Non-vegetarian food heats the body up, which might result in failure right after the embryo has been transferred into the surrogate’s uterus. That is why we keep them (surrogates) under strict restriction. After pregnancy successfully takes place, they are free to eat anything. It’s for their own good, you know.
Along with the strict control over their diet, the surrogates’ physical mobility was restricted. They were not allowed to do any household work. Their food was served in their bed, ensuring minimum physical movement. They were not allowed to leave the hostel to visit family and their children could not stay with them, except toddlers.
The surrogates invested considerable effort in convincing their husbands for surrogacy, in travelling from Nepal to Delhi like Asha and Sabita, and in getting ready for surrogacy through hospital visits for hormonal injections, check-ups and embryo transfer. It also cost them substantially if implantation failed. Surrogates bore many pre- and all post-natal costs and risks; dispensable if implantation failed and after giving birth; at the same time necessary for production (Rothman, 2014; Wright, 2006). Their disadvantaged backgrounds, lack of autonomy and their surveillance not only infringed their rights to privacy but also manifest the acute power imbalance that diminished their status as workers and limited their bargaining power at work (Rudrappa, 2015, 2017).
Surrogacy labour creating value for fertility clinics, hostels and agents
While the labour of surrogates was devalued, an examination of the wider social relations in commercial surrogacy reveals the profits generated by their labour; profits that are appropriated by the fertility clinics, agents and hostel owners in a dense and highly commercialised network. The surrogates were paid INR 300,000, while the agents earned INR 35,000 per surrogate and the clinics earned exponentially, nearly seven times more than the surrogates.
Fertility clinics, nursing homes, and hospitals that offer surrogacy services act as a crucial segment within the network. The fertility clinics represent the capitalist institution within which fertility specialists, embryologists, surgeons, and other medical personnel operate to create the end product. They act as the prime facilitator of the service; starting from attracting the childless couples through advertisements and lucrative ‘deals’, supplying surrogates by maintaining an extensive network of ‘field agents’ who find and recruit potential women for surrogacy, creating embryos in laboratories in-vitro, preparing the surrogate’s body for pregnancy and gestation by injecting artificial hormones, to delivering the baby to the commissioning couples. It is estimated that clinics earn around INR 2 million per surrogacy (£21,000). Not surprisingly, the doctors at the fertility clinics often expressed discontent with the proposed ban on surrogacy. A renowned fertility expert refused to interact after several visits stating: You researchers and academics are responsible for the negative portrayal of Indian surrogacy industry. You cannot blame us for being non-cooperative. This ban will have serious consequences for the entire industry.
The middlemen, surrogacy agents and surrogacy agencies play a vital role in the surrogacy industry. With the mushrooming growth of surrogacy clinics around the city, the number of surrogacy agencies had also increased significantly over the past few years. Mr Sharma, the owner of a surrogacy agency, reported working in the sector for the past nine years. A software engineer by profession with a Master’s degree, he first heard about surrogacy from his doctor friends.
In that moment, I recognised the immense business potential commercial surrogacy had in the Indian market.
With the continued growth of the industry, in 2008 he rented a house for keeping surrogate mothers. Most surrogacy agencies supply surrogates to more than one fertility clinic, ‘to keep up with the increasing competition with other agencies’.
The agencies work directly with the fertility clinics; their primary task involves supplying potential surrogates as per the demands of the doctors and the parties (commissioning parents). They are also tasked with keeping the surrogates in surrogacy hostels during their pregnancy, starting from embryo transfer to the post-caesarean recovery period. The power of the clinics is evident in the control they exercise over hostel owners and surrogates: At first, the families were allowed to stay in the house with the surrogates, but later the doctors objected and directed the agencies to keep the surrogates separate from their families. So, I started this hostel for surrogates. Their families are allowed to visit them, of course, but they are not allowed to stay at night. Only the toddlers are allowed to stay with their mothers at the hostel.
Surrogacy agents are a key link between surrogates, hostels and the clinic. Vinod, a surrogacy agent, apart from locating and recruiting surrogates was also tasked with taking the surrogates to clinics and hospitals for tests and medical appointments. After working in the ‘field’ for more than seven years, he now had other agents working for him. For every recruitment, Vinod earned from INR 30,000 to INR 35,000 (£400 per surrogate). He boasted proudly: I do not even need to go to the field. I now have contacts with so many people. I inform them, and they find me the women who are willing to work as surrogates. I have extended my network over almost half of Delhi by now.
The considerable disparity between the profits made by doctors and middlemen and the surrogates’ earnings is exacerbated by the surrogates’ impoverished background, lack of knowledge regarding the intended parents, and their unfamiliarity with modern medical technologies. Through secrecy, surveillance and workplace control, the middlemen weaken the bargaining power of informal women workers even further.
Multiple dilemmas and negotiations of surrogates: Emotions, stigma and meaning
Quite evidently, the surrogates were from disadvantaged backgrounds, economically motivated and compelled to surrogacy because of their circumstances. Yet, they were not mere victims (see also Pande, 2014; Parry, 2018; Vora, 2015). They negotiated with their multiple identities as mothers, workers and participants in an unfamiliar and commercialised industry. They managed the complex nature of their labour and the associated stigma and alienation. Importantly, they tried to exercise some choice at home and at the workplace in an attempt to counter their weak bargaining position.
Almost all surrogates tried to negotiate with their husbands as well as the agents. They decided to go for surrogacy themselves and convinced their husbands. For Pratima, it involved gaining some control over her fertility. Despite her three children, Pratima’s husband and parents-in-law did not allow her to undergo sterilisation. Through surrogacy she assumed control over her reproductive capacity in order to address the material deprivation of her family. Others, like Leela, tried to negotiate a better payment package despite their lack of knowledge and the insufficient information provided by the agents and the clinics.
The surrogates managed intricate dilemmas associated with the societal stigma of carrying someone (other than your husband) else’s child, the emotional cost of separation from their own children, and the alienation instigated by the surrogacy process. None of the surrogates had informed their families of their surrogacy because of the stigmatisation. Pratima and her husband decided to keep it a secret. Sabita did not reveal her plans to anybody in her village. Her parents and in-laws knew that she worked as a domestic help in Delhi.
I could not tell them the truth. If they knew, I would be misunderstood. Nobody knows about these things (referring to surrogacy) in my village. It’s better this way.
Almost all the surrogates, with the exception of Asha, had left their children in their villages of origin and found it very difficult. Rubina left her daughter with her in-laws: Although I talk to my daughter over phone, I still miss her. But what option do I have? I need the money for my mother-in-law. She needs to operate her eyes immediately, and if I am left with some money after her operation, I will save it for my daughter’s education.
Pratima left her two sons in the village, while her daughter stayed with her husband in Delhi. They would come and visit her at the weekends, but Pratima worried about them: My daughter is only eight; there is nobody to take care of her. I have no idea how my husband has been managing all that cooking, cleaning, by himself.
To manage the psychological and emotional aspects of work which involves becoming a mother and a worker at the same time the women developed different coping mechanisms, both to negotiate an unfamiliar hyper-medicalised system and to alienate themselves from their pregnancy. They described the emotional labour they performed in disengaging their feelings from the foetus so that they could fulfil the terms of the contract and give up the baby. They differentiated the pregnancy from their earlier ones attributing it to the medicines and the procedures involved, and the unnaturalness of it. Recalling her pregnancy with her daughter, Rubina claimed it was different: This baby moves a lot, especially during the night; I am having a tough time sleeping recently. It was not like this at all when I was pregnant with my daughter. I could eat anything I wanted. I could even run if I wanted to. I did not take any medicine before childbirth. However, with this child, everything is different. I was injected with multiple medicines for the first three months, and after that, had to continue taking iron and vitamin pills. Yeh to dawai ka baccha hai (this is not a natural baby), and it needs special care. I am very careful when I go to the washroom. I am not allowed to lift heavy things, and I am not allowed to eat anything from outside. I did not have any issues with my own pregnancy, but this time I have developed certain complications. I have developed certain food cravings as well which I never had during my earlier pregnancies.
Her encounters with modern medicine and technology left Rubina astonished, terrified and humiliated at the same time: I was scared of the transvaginal ultrasound at first; it was quite painful. Thankfully I did not have to go through that again.
Sabita described the difference as arising from: Maybe it’s because of the procedures we undergo, the medicines we take. I don’t remember taking any medication in my times. I ate whatever I wanted and went wherever I wanted to. But the doctors say this child needs special care, so I can’t act irresponsibly. Even my body feels different. I am hardly allowed to leave my bed, and I spend most of the day sleeping, or simply lying on the bed.
The attempts at disengaging from the pregnancy highlights the emotional conflict of surrogates: emotional detachment is a key part of the contract, at the same time as the women are expected to act as a caring mother. This mother-worker and producer-reproducer dualism lays the framework of exploitation in the commercial surrogacy industry (Pande, 2014; Rudrappa, 2015). Almost all the surrogates sought to counter the stigma, the strangeness and the unfamiliarity, and the emotional costs involved in surrogacy by emphasising that their motivation and purpose was driven by a desire to provide for their family and children. By ascribing a ‘societally acceptable’ meaning to their choice, the surrogates were consciously arrogating a dignity to their labour which was stigmatised in society and devalued at the workplace.
Discussion and conclusions: To ban or not to ban?
The details of the labour relations and structural inequalities in an unregulated and highly commercialised surrogacy industry in the region reveal the weak bargaining power of informal surrogate workers in determining their earnings, working conditions and decision-making capacity, and the immense power of fertility clinics, doctors and surrogacy agents exercised through secrecy, surveillance and control. The women’s access to information, mobility and safety is severely constrained and their mental, emotional and physical well-being undermined; emphasising the disposable nature of reproductive labour (Colen, 2006; Wright, 2006). The power imbalances are amplified by the disadvantaged background of predominantly migrant women at the bottom of the reproductive hierarchy: the payments to them are meagre as compared to the profits reaped by middlemen and doctors. The already huge profit gap widens when payments to surrogates are compared across countries of the North and South: the surrogate workers in the South are paid considerably less than in the North (Cooper and Waldby, 2014). While the reproductive labour of informal surrogate workers continues to be devalued, for whom surrogacy is often a survival strategy or a temporary livelihood strategy, the surrogacy industry flourishes embedded as it is in wider social relations.
It is against this contextual reality of the availability of a compelled and compliant informal surrogacy labour and a surrogacy industry interlocked with processes of capital accumulation in India that the question posed at the start of this article – ‘to ban or not to ban’ – needs to be assessed. Surrogacy draws polarised positions. Advocates of the ban, on account of surrogacy being immoral, unnatural and unethical, overlook the economic means surrogacy provides to informal women workers, however exploitative, as well as the wider social relations of surrogacy. Opponents of the ban, often liberal feminists, consider it as an assault on women’s reproductive rights. Some scholars, such as Dickenson (2017), provide a nuanced explanation for a shift in their position from surrogacy as a valorisation of women’s agency in their reproductive labour to argue for its abolition in view of its exploitative nature and re-establishing existing forms of subjection, including neo-colonialism, poverty and caste. As she concludes, surrogacy is neither revolutionary nor emancipatory. While a focus on women’s autonomy and reproductive rights may empower women and further working-class women’s rights, it is insufficient to capture the dilemmas of surrogacy given social and economic realities in India. This article concurs with scholarship that opposes the ban on grounds that one needs to consider the ‘totality of women’s experiences . . . and alter power relations in their favour’ (Rudrappa, 2015: 173; also Pande, 2017; Parry, 2018; Vora, 2019).
In light of the above, the ban on surrogacy in India in January 2020 poses a number of concerns. Earlier developments, for example the ban on surrogacy for single individuals, gay and unmarried couples in 2012, and the reality of social relations of the surrogacy industry as detailed in this research suggest three potential outcomes. The first possibility is that the surrogacy industry will die out, taking away the survival or livelihood strategy of already disadvantaged working-class women. The dying out option, however, is uncertain in the face of both national and international demand for surrogacy, supply of surrogate workers, and the dense networks that underpin a thriving surrogacy industry.
A more viable, and second, possibility is that the surrogacy industry would go underground, pushing what is already a predominantly unregulated industry into the realm of ‘illegality’. For example, in China the 2001 ban on any trade in fertilised eggs and embryos, which in turn forbids hospitals from performing any gestational surrogacy procedures, is regularly flouted by clinics and clients and has effectively driven the industry underground (cited in Pande, 2017: 276). The ban, and associated illegality, would not stop the exploitation of poor and socially disadvantaged women who would continue to participate in the industry for the complex and multiple reasons that underpin their choices. Instead, it would make already unprotected and insecure informal surrogates even more vulnerable and stigmatised and undermine their rights as workers, further weakening their bargaining power vis-a-vis the middlemen.
The third, and very probable, possibility is the reorganisation and/or relocation of the industry. When surrogacy was banned for single individuals, gay and unmarried couples in 2012 and the clients could not come to India, Indian surrogate mothers were moved across international borders into Nepal to facilitate the trade. They would give birth in Kathmandu, from where clients could pick up their children. In another example, Kenyan surrogate workers were flown in to India, implanted with embryos and then flown back to Nairobi to give birth (cited in Rudrappa, 2017: 5–6). Simultaneously, a surrogacy industry specifically catering to gay couples grew in Thailand. The point is that exploitation is likely to deepen when women are flown to unfamiliar destinations without support, leading to situations where they can be held in hostels with their passports confiscated, for example in the case of Vietnamese women in Taiwan (cited in Pande, 2017: 276). Exploitation is also likely to shift from vulnerable women in one geographical setting to another, often in the South.
To conclude, the answer to stop the exploitation of poor surrogate workers, as professed by the proponents of the ban in India, does not lie in banning surrogacy but in social, political and legal recognition of surrogacy as reproductive labour. Recognising surrogacy as a legitimate form of work would keep the focus on exploitation and weak bargaining power of informal surrogate workers within the capitalist accumulation process and the need to address it. It would lead to the formulation of effective regulation which protects the rights of surrogates as workers. Through providing for collective bargaining rights on wages, work conditions, health and safety, the right to unionise and possibilities/opportunities for self-organisation, the recognition would thereby empower surrogates (see also Kotiswaran and Banerjee, 2021; Pande, 2017; Rudrappa, 2017).
Finally, this research focused on the lived experiences and wider social relations of commercial surrogacy. An analysis of social relations of production and exchange along the global reproductive chain would likely support the research but would have been beyond the remit of this research. The grey area in which the industry functions, for example the secrecy surrounding financial transactions and commissioning parents, who could have been local or international, was often restrictive. An examination of the chain, which includes commissioning parents and corporate medical companies, would deepen the understanding of how exploitation and oppression function in the global reproductive industry.
Footnotes
Acknowledgements
We would like to thank Professor Eleonore Kofman and the three peer reviewers for their constructive suggestions and support.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.