
Abstract
Despite evidence supporting the application of health and well-being policies and practices in the workplace, small and medium-sized enterprises (SMEs) still struggle to manage health at work. To address this gap, this research explores the role of a new occupational health (OH) adviceline assisting and managing health at work within SMEs. From our qualitative data we develop a typology of managerial response patterns, which can be summarised into four behavioural types: business case behaviour, social model behaviour, protective behaviour, and avoidant behaviour. The study posits that both the business case and the social justice arguments need to be acknowledged while implementing and managing health and well-being initiatives in SMEs. However, the combination of these two models is very difficult to achieve, and in addition to an OH adviceline, other interventions need to be implemented to support SMEs.
Keywords
Introduction
Employment and working conditions in advanced societies have changed extensively over recent decades, with several implications for workers’ health and well-being (Carter et al., 2013; Kowlaski and Loretto, 2017; McGann et al., 2016; Quinlan, 1999). The growing number of SMEs embodies one of these changes; SMEs clearly represent an under-researched context in which OH services are underutilised (Black, 2008; Harrison et al., 2013; Hasle et al., 2012).
However, ‘the relationship between work and well-being is not straightforward’ (Kowalski and Loretto, 2017: 2230). While some employers see the value of health and well-being policies and practices, others introduce them with the objective of increasing employee performance (Guest, 2017).
Although research emphasises the business case of OH and well-being at work, in practice, it is very difficult to measure the effectiveness of these health and well-being initiatives. For these and other reasons, the business case argument should be coupled with the argument of social justice, which, as the authors have highlighted, embodies the social model of health and well-being (Bleijenbergh et al., 2010; Foster, 2018; Noon, 2007; Oliver, 1983, 1996). Still, there is limited if any research that challenges the argument of a business case for managing health at work and that links it to the social model of health and well-being.
To address this gap, this article explores the role of a free OH adviceline (or the Occupational Health Adviceline – OHA 1 ) in supporting managerial decisions regarding implementing and managing health at work within SMEs. The main reason for implementing this government-funded service is the belief that small business owners hold only limited knowledge of Occupational Health and Safety (OHS). Hence, they need to see the business case in OH and well-being initiative to invest in them (Black, 2008; Harrison et al., 2013; Health and Safety Executive (HSE), 2016).
The authors thus aim to address the following questions: (1) How do SME managers deal with health and well-being in the workplace? (2) Has the OHA prompted new managerial behaviours, policies and practices? (3) Are these behaviours, policies and practices used by managers mainly to increase employee work performance (business case)? (4) Are these behaviours, policies and practices introduced by managers to support the health and well-being of their employees (social justice)? (5) Does the specific context of SMEs affect managerial actions and behaviour towards health at work?
This study offers a series of contributions. First, the authors shed light on the theoretical concepts of the business case and the social model of health and well-being (Bleijenbergh et al., 2010; Foster, 2018; Noon, 2007), which are both relevant for facilitating the implementation and management of health and well-being initiatives in the context of SMEs. Second, by exploring the impact of a free OHA on managerial actions, the authors develop a theoretically grounded typology of managerial behaviours, which leads to a reflection on the under-researched context of SMEs (Kowlaski and Loretto, 2017) and the effects of the digitalisation on OH. Third, the exploration of the OHA – a government-funded service – represents a unique opportunity to evaluate whether policy-making interventions have succeeded in educating managers of SMEs in managing health at work and highlighting recommendations for further research.
The management of health and well-being in SMEs
SMEs represent a large element of the overall UK economy. They consist of approximately 99.9% of all UK businesses, precisely 5.9 million businesses (The Federation of Small Businesses, n.d.). Despite the prominence of SMEs in the UK labour market, the literature points out that OH services are more common in larger organisations than in small businesses (Arcocena and Núňez, 2010; Black, 2008; Harrison et al., 2013), and SMEs tend to have a poor rate of compliance with OHS laws (Kheni et al., 2010).
Some traits of SMEs allow for smooth OHS management. For instance, the management of OHS is less formalised, and this helps to instil loyalty and commitment among managers and employees (Carsrud and Brannback, 2011; Marlow and Patton, 2002; Masi et al., 2014; Tsai et al., 2007; Zachary and Mishra, 2010). Moreover, the lean and flexible organisational structure of SMEs tends to rely less on OHS infrastructure and keeps administrative costs down (Clifton, 2005; Rikhardsson and Impgaard, 2004).
However, the scarcity of resources of SMEs has a negative impact on the health and well-being of their employees. Evidence from previous research shows that employees of SMEs struggle to maintain a good work–life balance because they need to assume multiple roles due to the organisational labour shortage (Guest, 2002; Malik et al., 2010). Moreover, these employees tend to experience high levels of stress due to heavy workloads, tight deadlines and poor promotion opportunities (Galabova and McKie, 2013; Lewis et al., 2017), thus leading to a high sickness rate. Furthermore, SMEs’ work environment indirectly encourages presenteeism, due to financial resources, high workloads and an organisational structure that is too informal (Holt and Powell, 2014; Legg et al., 2015; Masi and Cagno, 2015).
This scarcity of resources among SMEs prevents them from building up relevant OH knowledge and limits the potential development of an appropriate OHS policy. This explains why policies adopted by larger firms fail to be implemented by SMEs (Cocker et al., 2013; Harrison et al., 2013). Furthermore, SMEs might not have sufficient data (e.g. absence days or costs related to OHS) to evaluate the effectiveness of OHS interventions (Griffin et al., 2005). For these reasons, SMEs do not see the business case in investing in OH and well-being programmes.
The implementation of OHS within SMEs is not without problems. For instance, managers and workers can harbour negative feelings towards health and well-being, excessive or ineffective regulation, limited time to complete OHS activities, lack of training and economic resources/human capital, and delocalisation of company activities preventing affective communication and training (Masi et al., 2014). SMEs tend to have a reactive approach to OHS (Clifton, 2005). Many SME owners also wrongly believe that, because of their small size, the OHS risks are insignificant, but the opposite is true, as the incident rates for SMEs are higher than those of large enterprises. Similarly, some SME owners tend to minimise their spending on prevention strategies associated with OH risks because they view investment in health and safety as a cost with little immediate return to the business (Nowrouzi et al., 2016).
Even when OHS is taken up by SMEs, its management can be challenging. SMEs lack clarity about whom to report to regarding OHS issues (Kheni et al., 2010). Nowrouzi et al. (2016) suggest that challenges with communication present a major barrier preventing the effective adoption of OH policy, which can be explained by the transitory nature of SMEs.
The happy-family image of SMEs can conceal forms of authoritarian management, in which a family or forms of kinship ties govern employees with very little external control or fairness (Marchington and Suter, 2013; Ram et al., 2011; Saridakis et al., 2013; Sheehan, 2014). Furthermore, the management of health and well-being in SMEs is also influenced by other external forces, such as the overall changing nature of work in our society, the political and economic climate, and national legislation, which govern health and well-being at work.
Why the business case is insufficient for the management of health and well-being at work in SMEs
This article posits that the sole business case is not comprehensive enough to implement and manage health at work; it also outlines the need to link it with the social model of health and well-being. The usefulness of the business case for the implementation of new HR practices, policies and expenditures has been previously debated in relation to the diversity management policy (Bleijenbergh et al., 2010; Noon, 2007). Managers and policy makers have often used the business case argument to retain and attract human capital and increase employee performance (Bleijenbergh et al., 2010). Furthermore, the business case approach has been highly supported by neoliberals who emphasise that this argument ensures fairness among workers through more inclusive human resource policies (Noon, 2007). However, scholars point out the high risk of focusing solely on the business case argument to favour the implementation of diversity management policy, and thus the argument of social justice needs to be explored. Drawing on these existing scholarly discussions, we share this perspective and apply it to our study about implementing and managing health at work within SMEs.
Similarly to diversity management, employers fail to recognise the business case for the implementation of health and well-being policies and practices because they take a short-term focus. This behaviour is very common among SMEs, mainly because they have limited financial resources (Cocker et al., 2013). Furthermore, employers struggle to see the business case related to the investment in OHS and well-being practices and policies, because it is difficult to measure the benefits, especially in the context of SMEs. The business case argument relies on a cost-benefit analysis, which is very difficult to be measured in a short period of time, and SMEs often do not record the relevant data (Griffin et al., 2005).
Moreover, by considering the institutional changes of the management of health at work, the article illustrates why an over-reliance on productivity does not result in helpful strategies to manage health at work. The introduction of the Statutory Sick Pay (SSP) Act in 1994 emphasised the productivity principle in relation to the management of health at work. This act represents the neoliberal deregulation philosophy, which shifted the responsibility for managing absences due to sickness from the state to organisations, particularly to line managers (Taylor et al., 2010). Under this perspective, sickness absence is considered an undesirable cost to minimise, and thus a series of policies were introduced to reduce such absences. These new policies and procedures mainly aimed at reducing the number of sickness absences without considering how to prevent the occurrence of this phenomenon (e.g. the ‘Bradford factor’ in Gryner and Singleton, 2001; Taylor et al., 2010).
Since the introduction of the SSP Act, line managers have been considered responsible for the health and well-being of their workers. However, these actors have proven to be poorly equipped for the management of ill health and absenteeism. In some cases, the goodwill of individual managers has supported employees (Cunningham et al., 2004; Foster, 2007; Foster and Scott, 2015). In the opposite case, managers abuse their personal power (Fevre et al., 2013; Werth, 2015) or delegate their responsibility to the employees, who are empowered to build up resilience at work (Cedeström and Spicer, 2015; Ferguson, 2007; Foster, 2018). The business case argument does not acknowledge that managers are responsible for addressing bad health at work. Consequently, the business case alone cannot constitute a foundation to justify the implementation and costs related to OHS and well-being policies and practices.
In order to solve this dilemma, this article introduces the concept of social justice, embodied by the social model of health and well-being (Foster, 2018). This theoretical model relies on the assumption that society is the main contributory factor in creating poor health at work. Thus, it is the duty of employers and policy makers to remove these obstacles (e.g. bad management, work intensification, unfit workplaces) to create healthier workplaces.
The social model of health and well-being (Foster, 2018) is a re-elaboration and extension of the social model of disability, which posits that disability exists according to the way society is organised, rather than through a person’s impairment (Oliver, 1983, 1996). It focuses on removing barriers that limit the activities of disabled people. Recent research adopts this model to explore why workers with impairments have limited work opportunities in the film and television industry (Randle and Hardy, 2017). These authors pointed out that the labour process of this specific industry depends on ideal, resilient workers and thus impedes equal participation for workers with impairments. Similarly, Foster (2018) asserts that recent neoliberal initiatives, such as wellness training, only attempt to improve the individual resilience of the workers at the expense of initiating more constructive managerial actions. According to the neoliberal point of view, it is the workers’ responsibility to adapt to a tough work environment, not the managers’ responsibility to improve workers’ conditions.
The authors assert that the business case for health and well-being at work should be coupled with the tenets of the social model of health and well-being. Only in this way can employers fully understand their duty of care towards their employees. Through this theoretical lens, the authors explore the way in which the OHA has helped SME employers to implement and better manage the health and well-being of their employees.
Background to the study
The OHA is an occupational health service that provides support to SMEs through a telephone adviceline and an interactive online service. It was launched by a governmental body in 2009 as part of a series of initiatives to address some of the recommendations brought up by Dame Carol Black in her review, ‘Working for a Healthier Tomorrow’ (Black, 2008).
This service was created by a group of professionals in the field of OH in response to Dame Carol Black’s review (2008), which highlighted the lack of OH support among SMEs (Valsecchi et al., 2019). Initially, this OH service was delivered through the National Health Service (NHS). In 2012, this service became part of a Community of Interest Company. The aims of this service are to provide SMEs with free, early and easy access to high-quality advice regarding employees’ health issues. During the initial period, the OHA only provided advice over the phone to SMEs. Since 2012, the OHA has become a multi-channel service; employers and employees can seek advice over the phone, through online chat, or by accessing detailed material provided on the OHA website (Department for Work Pension (DWP), 2012). The authors conducted an evaluation of the adviceline between 2013 and 2015, during which period they collected the data for this article.
Methodology
The research draws on 43 semi-structured interviews with managerial staff members and nurses working for the OHA (17 semi-structured interviews) as well as managers and employees of SMEs who have used the OHA (26 semi-structured interviews from 23 case studies).
During the first stage of the research process, interviews were carried out with the managerial staff of the OHA (4 interviews), asking how the adviceline was created and its latest transformations. Additional interviews were carried out with OH nurses, contact centre managers and contact centre operators (12 interviews). The interviews were carried out as we wanted to get an in-depth understanding of how the service works so we could create two online surveys. These were sent to a list of managers and employees who have used the service.
An online survey was sent to 1295 managers who have used the service, which generated a response of 218 employers. In the first survey, we asked employers of SMEs why they contacted the OHA, which services they have used (telephone support, online guidelines, chat line), the impact of the OHA on their organisations in terms of job adjustments, contact with other services and the development of new policies and procedures. Moreover, in the final part of the survey, we asked employers to leave their email address or phone number and specify whether they were willing to be contacted for further interviews.
Thus, upon considering the employees who were willing to participate further in our study, the researchers selected 15 case studies by taking into consideration the participants’ industry, their motivation for using the OHA, and the type of adjustments implemented. The Principal Investigator (PI) interviewed 15 managers and 3 employees who were back at work after a period of sickness leave whose managers utilised this service. Afterwards, another survey was sent to the employees who had utilised this service (550 in number – 103 responses). From this second survey, 8 case studies were selected by taking into account the participants’ willingness to participate, participants’ industry and their motivation for using the OHA. The PI conducted 8 semi-structured interviews with these employees.
The overall sample includes 23 SMEs, our case studies, which included a mix of sectors and industries (public, private and third sectors, finance, education, advertising and manufacturing). The range of workforce size across the SMEs considered in the sample varies from four up to 90 employees. Semi-structured interviews with managers and employees of SMEs were conducted. These questions expounded further our previous surveys, which enabled the authors to collect more in-depth qualitative data about the usefulness and impact of these services and to better analyse the immediate actions that managers took after the use of the OHA. Because of the variety of our sample, the interview schedule was adapted for each of the cases, and new questions emerged during the interview process.
The interviews lasted between 30 and 75 minutes on average and were tape-recorded. The researchers analysed the data by first transcribing the interviews and then coding the data into themes. All of the themes emerged intuitively from the data collection and afterwards through the coding process. Following the methodological approach of Gioia et al. (2012), the authors built up first-order categories/themes by trying to adhere to the informants’ experience of using the service. During this initial coding, the authors explored why managers/employees had utilised the OHA, the work adjustments implemented and the main impact of this service.
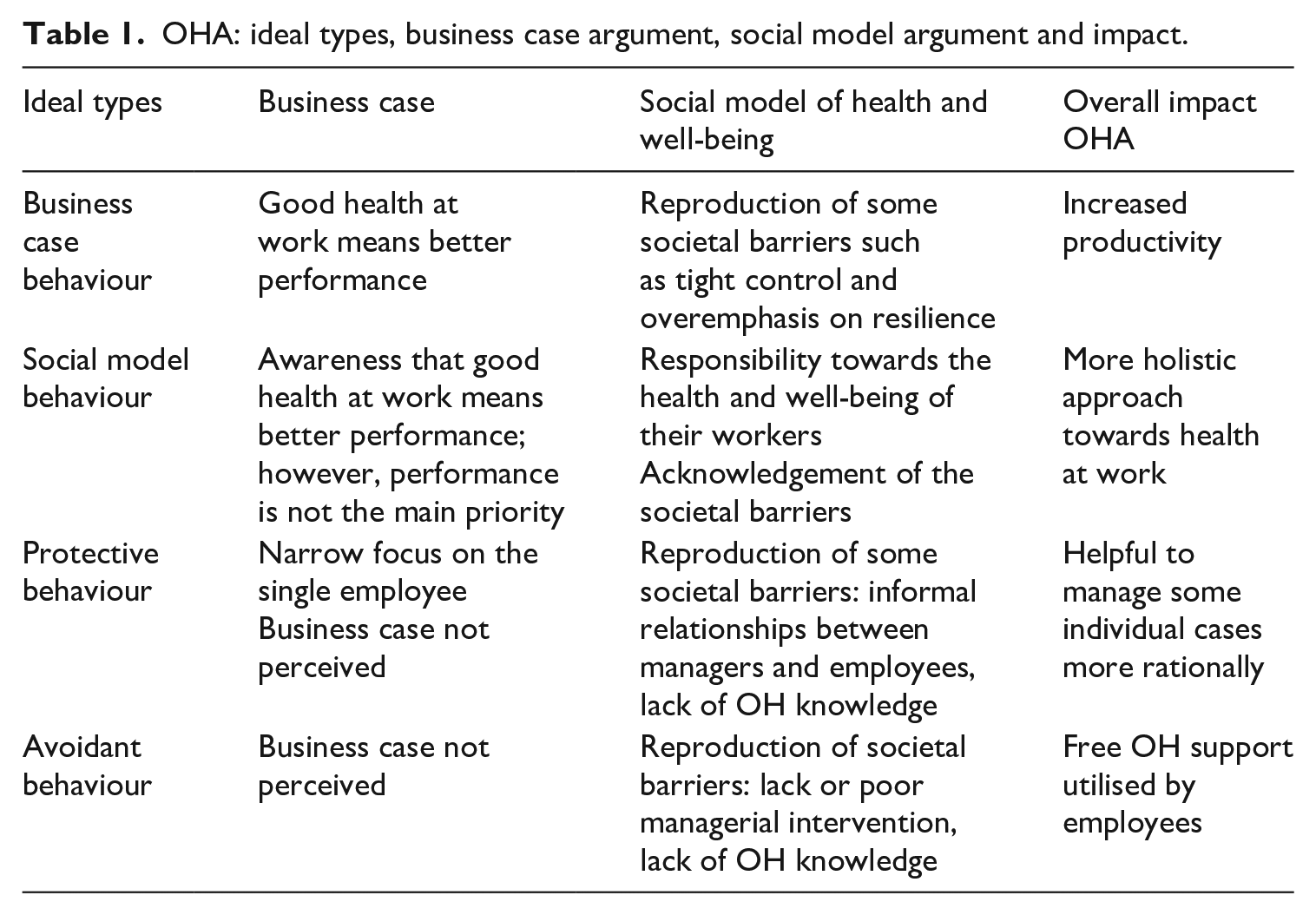
Subsequently, the authors took into account these intuitive categories and, upon reflecting on the societal barriers and the business case argument explored in the literature review, generated second-order categories. These categories are summarised as follows: ‘focus on targets and/or control versus focus on employees’ health and well-being’, ‘collective actions versus individual responsibility/resilience’, ‘acknowledgement of the importance/responsibility of health and well-being at work versus ignorance/avoidance of health and well-being at work’ and ‘rational managerial actions versus personal ties’. Finally, by combining these managerial orientations towards health and well-being (second-order categories), the authors developed a typology of line manager behaviours, which is discussed in the Results/analysis section below and in Table 1. Table 1 summarises the impact of the adviceline in relation to each ideal type, with reference to the business case and social model arguments and their overall impact on SME users.
OHA: ideal types, business case argument, social model argument and impact.
The research has been conducted by following the main ethical research guidelines, and the research team obtained ethical approval from the research ethics committee of their academic institutions.
Results: A typology of line manager behaviours in SMEs
The case study data offered in-depth insights into how the OHA has helped managers and owners of small businesses to deal with OH and well-being at work. Its interventions have been summarised into four ideal types of managerial behaviours: business case behaviour, social model behaviour, protective behaviour, and avoidant behaviour. These ideal types need to be understood as artificial constructs that help us to better understand managers’ actions and attitudes towards the management of OHS and well-being at work in SMEs but, in reality, the managerial actions taken by these managers are more complex and varied.
Business case behaviour
This category embeds the behaviour of managers who are more concerned with the overall organisational performance rather than the health of their employees. Managerial actions and OH practices and policies that fit in this category mainly aim to decrease sickness absence without considering how to prevent the occurrence of such events. Bad health at work was thus perceived as an individual problem.
For instance, the director of a charity domiciliary care agency (manager 2 – case study 2) contacted the OHA because the organisation was experiencing a high level of sickness absence and did not have a specific system to monitor sickness absence. The OH specialist explained how to implement a sickness absence policy, which, according to the manager, helped her to reduce the level of absenteeism among her employees: I’m now meeting with them [the employees who are off sick] and saying, ‘Look, this is the process’, so we’re stopping it now before it gets to that point, whereas before, we’ve just, it’s just carried on, carried on, and carried on, we’re now actually stopping it. (Manager 2, female)
This manager found that, since the introduction of sickness absence policies and the return to work interview, the cost of sickness absence dropped: So, we can see by looking at it and obviously by the monthly figures that’s generated on how much was paid out each month on sick pay, we can see that that’s dropping down cost-wise. (Manager 2, female)
This manager also observed that these practices not only helped her to stop long-term sickness but also that short-term sickness decreased: They know that we monitor their absence so that now they think twice before taking a day of leave just because they have a headache. (Manager 2, female)
Although sickness health policies are necessary in workplaces, they cannot solve the roots of the problem alone. In many cases, these measures merely increase the incidence and preponderance of presenteeism in the workplace. Ideally, sickness absence policies should be introduced in conjunction with other HR practices and training, including appropriate support for employees working under stressful conditions or experiencing other negative demand factors.
Moreover, other cases suggested that the OHA can also encourage individualistic behaviours in an unintentional way. As discussed, the OHA became a multi-channel service and, in addition to the telephone advice offered by OH nurses, users can also access information on OHS and well-being online. While this OH knowledge base website enabled both managers and employees to increase their knowledge regarding health and well-being, it also created in an unintended way some individualistic behaviours that were not foreseen by the creators of this service. For instance, many employees attempted to find a solution to their problems by learning how to deal with stress by themselves without consulting their manager. Employee 4 revealed that he was ‘terrified’ of the thought of approaching his managers, so he tried to cope with his stress condition by himself through the knowledge base information, which he found very helpful.
However, this employee did not mention to his manager either that he had contacted the OHA or that he was experiencing stress-related problems. He pointed out that his company used a private adviceline, which unfortunately does not effectively support employees: . . . they will take it against you for doing that (saying that he has used the OHA), because they’re spiteful and that there is no way around this, well there is a way around this, the only way around this is that they actually suggest that their employees use a line similar to yours which is actually privately funded, and if you call that line, that line didn’t give as good information as yours. (Employee 4, male)
According to this employee as well as others, the main solution to fight stress is to become more resilient, without seeking any support in the workplace. In an unintended way, the knowledge base website of the OHA reinforced some neoliberal ideologies that workers must develop resilience instead of seeking help from their line managers or trade unions.
Social model behaviour
Social model behaviour is displayed by managers who recognise that there are some structural barriers that can interfere with good health at work and thus acknowledge that the management of health and well-being of employees is a manager’s responsibility. These managers appreciate the business case of health at work; however, this is not a priority for them.
In order to deal with OH problems, some managers make adjustments to work tasks, and others improved the overall organisational support available by arranging new trainings and improving communication channels to prevent bad health at work.
Managerial actions that fit into this category have also aimed to prevent bad health at work. As our interviews revealed, bad health at work is not an individual matter, but at times can be prompted by the work environment or an unsupportive organisational culture. One manager (manager 4 – case study 4) initially contacted the adviceline because one employee was off sick due to stress. Manager 4, by reflecting on the case of her ill employee, utilised in a creative way the advice provided by the OHA and initiated some activities aimed to prevent stress at work. She recognised that this specific employee probably did not feel comfortable in the office because he was the only male employee of the company. She came to the conclusion that good communication is crucial to prevent stress at work. Consequently, she decided to organise some informal staff gatherings during which staff members could discuss the problems they experience at work: Well, it’s not really a policy as such, we have a system in which Friday afternoons we sit down in a less formal place and the Managing Director will go out with people, one or maybe two, and sit down and cover any issues that might have happened . . .. So, it’s not a formal meeting, but it’s a chance to catch up regularly with people to make sure that they’re happy and make sure that everything’s going okay, make sure that they understand what they’re supposed to be doing so that we can kind of avoid any situations like we had earlier. (Manager 4, female)
Similar to the way this manager did, others utilised the OHA in a reflective way and, although they contacted this service for an individual health problem, after the phone consultation, they introduced additional policies, practices and training aimed at preventing ill health and maintaining a healthy work environment.
Protective behaviour
As discussed in the context of SMEs, the personal ties between the managers and the employees can interfere with the management of OHS. Our data revealed that some managers treat their loyal employees as family members and display protective behaviours while managing their ill health at work. These employers decided to utilise the OHA to deal with a problem related to a specific employee. Overall, the use of this service helped them to deal with the bad health of their employee; however, in contrast to the previous ideal type, these managers are more narrow-minded and do not reflect on this specific experience to offer more structured health and well-being policies and practices within the whole organisation.
For instance, manager 7 (case study 7) contacted the OHA because one manual worker developed rheumatoid arthritis, a health condition that forced him to stop working. This employee has been working for many years with that company; his relatives were even working there, as the manager pointed out: I mean he has relatives, his son works for us . . .. His brother was working here when he was working here. (Manager 7, male)
This manager wanted to support his employee and contacted the OHA for some advice. Unfortunately, the only solution was to help the employee to get some disability benefits: We were trying to help him; we didn’t want to see him go without all the benefits he could claim, and we wrote to his doctor a letter explaining in detail that he was a man that, you know, was genuinely disabled, couldn’t do his work and he did, despite the culture at the moment, as you know probably of cutting back on disability benefits . . .. We kept in contact with him to make sure that he did the claim successfully. (Manager 7, male)
The same manager also pointed out that, because the company was very small (15 employees/manual workers), he could not ask the employee to carry out a different job that was not manual and, for him, the disability benefits presented the only option. Although this protective approach highlights the supportive intentions of the manager, it also limits the opportunities for intervention. For instance, with additional training, this worker could have performed a different job in another company.
Similarly, in case study 13, the director of a charity organisation (manager 13) noticed that the behaviour of one of her employees was unusual; however, because of their close relationship, she did not know how to approach him. The consultation with an OH specialist was very helpful in disclosing latent health conditions and initiating rational interventions. After a referral to an OH specialist, she realised that this employee had early symptoms of Alzheimer’s disease, and this explained his confusing behaviour. As she pointed out, the process was very painful and stressful because she had known the employee for many years: It’s very emotional to have somebody you’ve known for a long time and you’ve thought, ‘Oh my God, he lost his memory. This is a nightmare!’ In lots of situations, it wouldn’t be quite as extreme as that . . .. You know, I mean, I don’t want to put somebody out of a job. (Manager 13, female)
The OHA helped this director to act more rationally so that the employee was treated and work adjustments were implemented. Yet, based on this specific case, no policies or interventions (e.g. managers’ training to deal with health at work) have been spread more generally across the organisation.
Avoidant behaviour
This category embeds the behaviours of those managers who tried to side-step, deny, or ignore any duty of care towards their employees and are uninformed about OHS. Because these managers overlook their OHS commitment, we could only grasp their behaviours and orientations towards OHS through the interviews of employees. For instance, a teacher (case study 18) contacted the OHA to ask about possible work adjustments. She immediately realised that her line manager was unaware of the OHS issues: I contacted the OHA, and they told me things like look at occupational health and maybe they can come and see me, see my working environment. When I actually suggested that to my school, they told me that occupational health was really only for those people who are off sick for many months, and I’ve kind of got some kind of suspicion . . .. (Employee 18, female)
Owing to the lack of work adjustments, the employee finally decided to cut her work hours, which was not the best option for her personal finances: So, once I got the GP to write the letter, they started to change, but I’ve constantly got to keep reminding them, and that’s one of the things that I feel I shouldn’t have to do . . .. I feel pain, and you know, it just isn’t, it’s not a pleasant experience, so I decided to cut my working hours . . .. I am feeling some benefits from it . . .. (Employee 18, female)
The narratives of many employees who have used the OHA gave similar messages: the managers either lack OHS knowledge or even believe that it is not their responsibility to provide adjustments for workers with OH problems. Many of these managers delegate their responsibilities to their employees, making them accountable for their illness. The implications of this finding are discussed in the following sections.
Discussion: The role of the OHA
Following our research questions: (1) How do SME managers deal with health and well-being in the workplace? Our qualitative data reveal that most of the case studies – before the use of the OHA – show some of the characteristics and problems related to the management of health and well-being of SMEs, discussed in the literature review. Some examples of these are a lack of, or ineffective, regulation (Clifton, 2005; Masi et al., 2014), informal structure (Saridakis et al., 2013; Sheehan, 2014), poor communication (Nowrouzi et al., 2016), a reactive approach towards OHS (Clifton, 2005), a lack of OH knowledge, and consequent unawareness of the business case for OH investment (Black, 2008; Harrison et al., 2013). Moreover, our interviews with employees who used the OHA services to support their health at work confirmed the argument that many SME managers are still unaware of their duties of care towards their employees and, through poor or inexistent OH knowledge, ignore their responsibilities (avoidant behaviour).
(2) Has the OHA prompted new managerial behaviours, policies and practices? Our data also highlighted that the majority of SME managers who have used the OHA developed OH knowledge and became more aware of the importance of health at work. They introduced a series of policies and practices, such as sickness absence policies, health and well-being training, and improvement in communication among their employees. Nevertheless, the flexible use of OHA enhanced by digital technologies, the informal structure of SMEs and their peculiar culture allow the development of a variety of managerial behaviours in relation to OH, with often contradictory and unintended actions.
(3) Are these behaviours, policies, and practices used by managers mainly to increase employee work performance (business case)? Some managers, through the use of the OHA, became aware of the business case of health at work (case study 2) and introduced OH policies and practices with the main goal of increasing employees’ performance (Guest, 2017). Some of them replicated previous common mistakes that occur in large companies by focusing on quantitative productivity measures through a more thorough monitoring of sickness absence (Gryner and Singleton, 2001; Taylor et al., 2010). The online knowledge base website enabled both managers and employees to increase their OH knowledge and to act independently. However, this empowerment indirectly triggered some individualistic coping mechanisms of employees who attempted to solve stress-related problems by themselves by enhancing their resilience without contacting their line managers (Foster, 2018). The OHA has good intentions towards OH at work; however, particularly through the knowledge base website, managers can choose their preferred dispositions and, unless the OH query is passed to OH professionals, managers are free to take actions without any particular external control.
(4) Are these behaviours, policies and practices introduced by managers to support the health and well-being of their employees (social justice)? Yet, as the research suggested, some managers took into account both the business case argument and the argument of social justice in the management of health at work after the use of the adviceline (social model behaviour – case study 4). These managers learnt of some structural barriers that can interfere with good health at work; for example, long-term health conditions, poor communication style and unsuitable management style. They understood that it is their duty to manage health at work more holistically, without just considering short-term profits. So, after their use of this adviceline, they also implemented practices and policies aimed to prevent bad health at work, such as flexible working practices, improved communication, and health and well-being training.
(5) Does the specific context of SMEs affect managerial actions and behaviour towards health at work? The authors also found that the peculiar culture of SMEs prompted protective managerial behaviour towards employees. This behaviour is embedded in the cultural context of SMEs, in which loyalty and personal ties play a very relevant role in the management of health at work. Indeed, some managers contacted the OHA because they wanted to solve a health-related problem, mainly because they developed informal relationships and close ties with their employees and at times replicated individualistic and narrow-minded actions, as discussed in previous studies (Fevre et al., 2013; Marlow and Patton, 2002; Tsai et al., 2007; Werth, 2015). While the adviceline helped some managers to manage ill health at work more rationally (case study 13), it did not help these managers to exercise such care beyond the single case (case studies 7 and 13).
Conclusions
Through this research, the authors explore the impact of an OHA on managerial actions in the context of SMEs using a theoretically grounded typology of managerial behaviours. The main contribution of this article is to show that both the theoretical concepts of business case and the social model of health and well-being (Bleijenbergh et al., 2010; Foster, 2018; Noon, 2007) are relevant within the management of health at work. However, in practice, this study shows that it is very difficult to embed these two concepts in the management of health at work, specifically in the context of SMEs. Only managers who have adopted social model behaviour fulfil the ambition of bonding together the argument for a business case with the tenets of the social model of health and well-being to manage health at work in SMEs. As the extant research suggests, a variety of managerial behaviours is displayed because of the loose structure of SMEs (Saridakis et al., 2013; Sheehan, 2014) and the flexibility enabled by the digital technology of the OHA.
The context of the research – SMEs – represents the second important contribution of this article, as the management of health at work in SMEs is indeed an under-researched area in the field of the sociology of work (Kowlaski and Loretto, 2017). This area is under-researched due to the complexities of the SME context and the underutilisations of OH services. Yet, data demonstrate that the lack of use of OH services because of costs represents just one problem, because even when OH support is offered for free, some managers struggle to implement appropriate adjustments without going beyond the case of a single employee. Moreover, other managers focus only on employees’ performance, and others do not even acknowledge OH-related problems.
The results show that this new OH service did not fail its intentions; however, it should be regarded as an important piece of a big puzzle of health at work. For this reason, the authors posit that, in addition to providing the OH service free of charge, a cultural change needs to be promoted through different networks and associations to help SME managers understand the complexity of health at work. Moreover, the argument of social justice should be more widely promoted by policy makers, who conventionally tend to emphasise business case arguments over other topics.
A third contribution of this article is embedded in the case study itself – the OHA. This innovative OH service shows both the intended and unintended consequences of digital technologies. The OHA has good intentions towards OH at work; however, managers, particularly through the knowledge base website, can pick and choose their preferred dispositions in most of the cases, without any particular external control. The authors encourage further study to explore the role of digitalisation in terms of the empowerment of stakeholders in the context of OH.
Another interesting finding related to the use of technology is that many employees started using the OHA even though this service was initially created for managers of SMEs. This example makes us consider the sociomaterial aspect of technology that leads to the performativity of specific behaviours from users, even if these behaviours were not foreseen by the funders of the adviceline (Orlikowski and Scott, 2008). We encourage further research in this specific area.
This research has some limitations. Although qualitative case studies allow researchers to gather in-depth information on a series of SMEs, it is difficult to generalise our findings. Moreover, we are aware that our sampling strategy enabled us to research only SMEs that have used the OHA.
Footnotes
Acknowledgements
We would like to thank the British Academy / Leverhulme Trust (grant no. SG122331) and the Knowledge Transfer Scheme (Brunel University London) for having funded our research. Moreover, we would like to express our gratitude to the OHA (we have anonymised the organisation) and all our participants for helping us to conduct our study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: British Academy / Leverhulme Trust (grant no. SG122331); Knowledge Transfer Scheme (Brunel University London).
Notes
Maria