
Abstract
Exposure to peer incivility and bullying potentially disrupts the respectful, collaborative workplace relationships essential to quality care provision in long-term care homes. This study critically examined the nature of peer incivility and bullying in residential care aides’ workplace relationships. Using critical ethnography, 100 hours of participant observation and 33 semi-structured interviews were conducted with residential care aides, licensed practical nurses, support staff and management in two, non-profit care homes in British Columbia, Canada. While residential care aides’ experiences of bullying were rare, peer incivility was pervasive, occurring on an almost daily basis. Two key themes, ‘gendered work environment’ and ‘seeking informal power and control’, reflect how residential care aides experienced and explained their uncivil encounters. Findings highlight the gendered, relationally aggressive nature of workplace mistreatment within this predominantly female workforce.
Keywords
Introduction
Residential care aides (RCAs), also known as personal support workers and nursing assistants, are unregulated workers who provide 80% of the care for persons in Canadian long-term care (LTC) homes (Berta et al., 2013). Situated on one of the lowest tiers of the workplace hierarchy, RCAs are predominantly middle-aged women, with little formal education, many of whom were born outside Canada (Chamberlain et al., 2019). Despite high levels of unionization within the Canadian LTC sector, RCAs are the lowest paid and afforded little formal power, respect or recognition (Armstrong et al., 2009). In addition to being highly gendered and racialized, RCAs’ workplaces feature high job demands, low job control and low support (Willemse et al., 2012). For example, RCAs routinely experience heavy workloads, working short-staffed, highly regimented routines and have little decision-making autonomy (Daly et al., 2011; Talbot and Brewer, 2016).
Symbolically associated with women and services historically provided to families out of love and obligation (England et al., 2002), care work reflects the gendered, naturalized assumptions of feminized care and self-sacrifice (Daly et al., 2011). RCAs’ work remains perceived as unskilled, domestic work of lesser importance and value (Chamberlain et al., 2019), as opposed to highly skilled work deserving respect, decent wages and working conditions (England et al., 2002). Despite comprising the largest workforce in the LTC sector, RCAs remain an understudied occupational group (Berta et al., 2013).
Of increasing concern is the potential for workplace incivility and bullying (WIB) to disrupt the respectful, collaborative working relationships key to quality care provision (Caspar et al., 2013). While 83% of RCAs in British Columbia, Canada report exposure to aggressive resident acts (WorkSafeBC, 2015), no information exists regarding their experiences of peer WIB. This is a significant knowledge gap as increased WIB is associated with hierarchical and stressful work environments, low job autonomy and specific gender-dominated fields (Roberts, 2015), all of which characterize LTC.
Background
Research on workplace mistreatment is conducted under a variety of constructs, including incivility, bullying, harassment, antisocial behaviour and horizontal hostility (Hershcovis, 2011). Although situated at the lower end of the continuum of behavioural intensity, incivility may serve as a precursor to more serious aggressive behaviour (Pearson and Porath, 2005). Conceptualized as a low-intensity deviant act that violates workplace norms or respectful interactions with an ambiguous intent to harm (Andersson and Pearson, 1999), incivility is one of the most pervasive forms of antisocial workplace behaviour, yet its subtlety makes it difficult to detect (Lim and Lee, 2011). Indeed, uncivil behaviour is notably mundane. While rude, condescending and ostracizing, such behaviour otherwise appears as everyday interaction (Cortina et al., 2017). Over time, experiencing or witnessing incivility can lead others to adopt similar behaviour, creating a downward spiral that results in an organizational climate of incivility (Andersson and Pearson, 1999).
In contrast to workplace bullying, which entails an escalating hostile relationship in which an employee is frequently and persistently subjected to overtly hostile acts from a co-worker or supervisor (Einarsen et al., 2009), uncivil acts are more likely to be passive, indirect and verbal (Pearson and Porath, 2005). Consequently, uncivil actions do not rise to the same level as bullying or harassment, which in many jurisdictions are prohibited in the workplace by law or through organizational policy (Young et al., 2021).
Within the general population of workers, an estimated 98% of workers experience incivility and 50% experience it on a weekly basis (Pearson and Porath, 2005). An accumulating body of literature highlights the prevalence and impact of WIB within the healthcare sector (Roberts, 2015). Globally, 67% of nurses have experienced non-physical violence, including incivility (Spector et al., 2014). The consequences of WIB are far-reaching and include decreased job satisfaction, organizational commitment/engagement, co-worker support/collaboration, as well as increased illness-related absence and intent to leave the organization and sector (Johnson, 2018).
Many of the contextual features associated with WIB, such as excessive workloads, limited resources (Tong et al., 2017), organizational change, low social support, high job demands (Torkelson et al., 2016) and having little control and influence over one’s work (Agervold and Mikkelsen, 2004), describe the current LTC workplace (Chamberlain et al., 2019; Daly et al., 2011). Given such a relationship and the personnel-related challenges facing the LTC sector, including an aging workforce, ongoing shortage of RCAs and retention/turnover issues, there is a clear need to attend to the issue of WIB in LTC.
Power and power disparities (reflective of an organization’s formal power structure, or differing knowledge, experience or social support among co-workers) are central to workplace mistreatment (Einarsen et al., 2009), whereby individuals engage in incivility as a means of asserting power and maintaining power differentials (Cortina et al., 2017). A commonly cited explanation for WIB in healthcare settings draws on Freire’s (1971) theory of oppressed group behaviour. Members of powerless, oppressed groups develop disdain for their fellow members because they feel devalued in a culture where power resides with another, more dominant group (Roberts, 2015: 37). Unable to express aggression directly towards the dominant group, members use submissive, passive-aggressive behaviours to displace their aggression inwards towards each other. The theory contends nurses are an oppressed group, who lack power and control as a result of their gender and domination within the medical profession (Roberts, 2015), and thus are socialized into structures and unequal power relations resulting in intra-group aggression.
Hutchinson and colleagues (2005) argue oppressed group behaviour theory only partially explains WIB as it obscures the broader organizational context and the role of organizational power relations. They contend behaviour within organizations is governed by rules and norms, with bullying strategically used to reinforce rules and maintain order. For example, casting doubt on a co-worker’s competence by publicly labelling them as stupid or incompetent secures legitimacy for the perpetrator and justifies their actions (Hutchinson et al., 2005). In making an example of the target, the bully draws attention to and reinforces organizational values, such that targets ‘learn their place’.
Much of the literature on WIB within healthcare focuses on acute care and professional staff (i.e. nurses). Far less is known about the experiences of unregulated staff (i.e. RCAs), particularly those in LTC homes. Pickering and colleagues (2017) found RCAs’ WIB experiences began the first week of employment and frequently involved more than one aggressor. Adaptive strategies invoked by RCAs included keeping quiet about safety issues (e.g. work-related injuries, witnessing resident abuse/neglect) as reporting increased the risk of retaliation or blame; forming alliances with co-workers so they had someone to help them with their work; and implementing workarounds (e.g. learning to transfer residents without assistance).
Seeking to add to this small body of literature, we explored the nature of WIB among RCAs working in two LTC homes in British Columbia, Canada. This article addresses two research questions. Firstly, what are the types of WIB to which RCAs are exposed within LTC and, secondly, how do social locations (e.g. gender, race, age) and broader organizational factors (e.g. staffing arrangements, workload, power relations) influence their WIB experiences?
Methods
This study’s method of inquiry was critical ethnography, which specifically seeks to illuminate systems of power and control and sources of inequities (e.g. gender, race, class, organizational factors, healthcare contexts) that contribute to marginalization (Madison, 2012). Adopting this approach offers insight into the domination and exploitation that have become a ‘naturalized’ part of everyday LTC culture. As talk (what people say during an interview) and action (what people do in practice) may differ, the ethnographic practice of utilizing participant observation and in-depth interviews provides a more nuanced and holistic understanding of WIB. Similarly, its emphasis on understanding meaning and providing detailed description offers additional methodological direction. Questioning the taken-for-granted beliefs, discourses and practices of LTC homes while analysing RCAs’ commonplace routines and interactions helped reveal the institutional processes and ideologies that reify accepted norms for WIB within LTC (Thomas, 1993).
Setting and participant recruitment
Two units in two LTC homes that had encountered WIB were selected as study sites. Both homes were situated in suburban areas: one in a small-sized city and the other in a mid-sized city. Each site was purpose-built, had been open less than 15 years and provided 24-hour nursing care to approximately 100 residents. The homes were owned by the same not-for-profit organization and received government funding to operate.
Each unit housed 25–30 residents, most of whom were non-ambulatory, in single-occupancy rooms with en suite bathrooms and ceiling track lifts. Both units’ staffing model followed the traditional LTC hierarchy, whereby RCAs were supervised by a Licensed Practical Nurse (LPN), who reported to the Director of Care, who reported to the General Manager (all supervisors/managers were women). RCAs were permanently assigned to their respective unit but regularly rotated through the residents. The units were staffed with three RCAs and one LPN during the day and two RCAs and one LPN during the evening. While represented by different healthcare unions, RCAs at both sites received similar pay (approximately CAN$20–21 per hour) and medical and employment benefits.
Following university and health authority ethics approval, participants were recruited through a multi-pronged strategy incorporating emailed invitations to all staff, presentations at shift change and posters distributed throughout both facilities. Inclusion criteria entailed full-time, part-time or casual employment and willingness to provide informed consent. Thirty-eight staff provided written informed consent (21 RCAs, six LPNs, seven administrative staff, four support staff). Participants were female, primarily Caucasian and Canadian-born (the latter reflecting the demographics of the surrounding area; see Table 1). RCAs had an average age of 43.9 years, had worked in the field an average of 10.4 years and at their current site for 5.4 years. All RCAs had completed high school and primarily worked at only their current site. The demographics mirror those reported by Chamberlain et al. (2019) for RCAs within the health authority in which the study sites were situated. Each participant received a CAN$15 gift card as a small token of appreciation.
Demographic data – all participants.
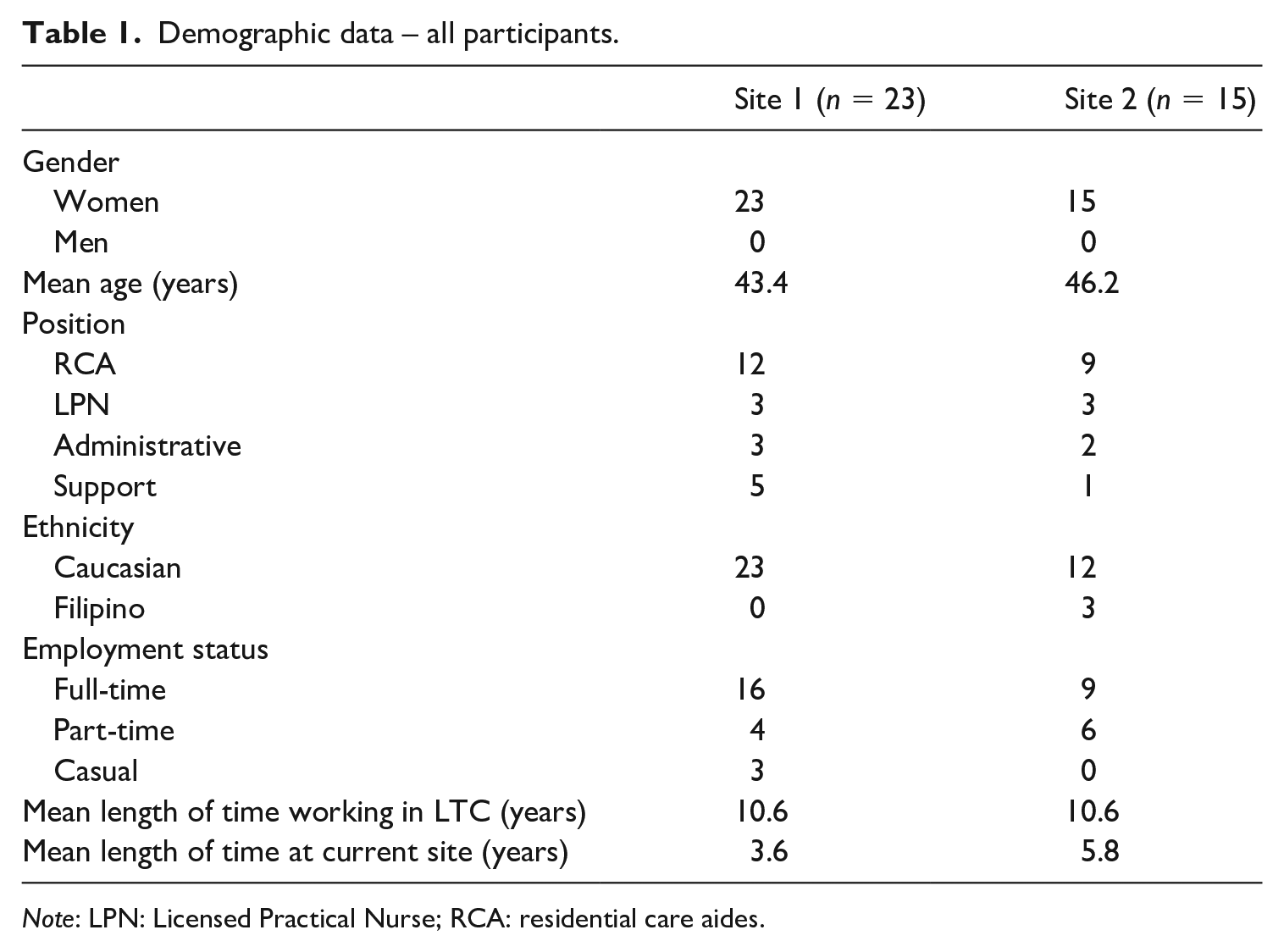
Note: LPN: Licensed Practical Nurse; RCA: residential care aides.
Data gathering
Data collection, which was conducted consecutively at the two sites, occurred between June 2018 and September 2019 and included 33 semi-structured interviews and 100 hours of participant observation. Interviews ranged in length from 43 to 130 minutes (mean length 75 minutes) and were conducted at a location of the participants’ choosing (coffee shop, on-site in private office), audio-recorded and transcribed verbatim. Interviews explored how RCAs worked as a team, their workplace relationships with other RCAs and their experiences of mistreatment (as recipient, instigator or witness).
Participant observation focused on RCAs’ interactions with colleagues and supervisors and included informal conversations with staff. Observations were conducted over a variety of days and times and lasted between 2 and 4 hours. Staff interactions were captured in field jottings and expanded into field notes immediately afterwards.
Data analysis
To facilitate data management and analysis, all transcribed interviews and field notes were entered into NVivo 12 (QSR International Pty Ltd). Thematic analysis was an iterative, multi-step process that occurred concurrently with data collection (Braun and Clarke, 2006). Guided by the research questions, multiple, line-by-line readings of the data were conducted (Lofland et al., 2006), resulting in the generation of codes derived from recurring patterns in participants’ narratives and behaviours at both sites. Initial codes included key descriptive terms/phrases; for example, ‘silent treatment’, ‘gossiping’, ‘pervasiveness’, ‘gender’ and ‘personality’. These were then categorized, compared and contrasted within and across sites and data sources, and further refined into themes (Huberman et al., 2014). For example, the codes, ‘gossip’, ‘criticism’ and ‘cattiness’ were brought together under ‘intra-gender relations’. Site 2 themes confirmed those from Site 1. Memoing and regular research team meetings captured insights about emerging codes/themes and their relationships to larger structural issues; for example, ‘intra-gender relations’ and ‘it’s just like high school’ were collapsed into ‘gendered work environment’.
Rigour
Trustworthiness was facilitated by prolonged engagement, the creation of an audit trail (i.e. a research log documenting key decisions, activities and process memos; Onwuegbuzie and Leech, 2007), peer debriefing and the analysis of reflexive field notes (Creswell, 2013). Triangulation of multiple data-collection methods (e.g. interviews, observations) and sources (e.g. RCAs, LPNs, support staff, administrators) (Patton, 1999) reinforced what we saw and heard. Often, the same incident was relayed by the recipient, witness and management. Throughout the research, close attention was paid to the authors’ own social positioning, biases and assumptions, documenting as such in reflexive field notes. The rich description of context, participants and methods offers readers the opportunity to determine the transferability of findings to other LTC settings (Lincoln and Guba, 1985).
Findings
Study findings highlight how, in contrast to more egregious, overt acts of bullying, RCAs primarily encountered peer incivility – subtle, insidious, passive-aggressive behaviours with an ambiguous intent to harm – in their workplace relationships. Such peer incivility was pervasive, occurring on an almost daily basis. Audrey commented: ‘In healthcare, I’ve experienced passive-aggressive behaviours in a way I never have in any other job and I’ve had a pretty full spectrum of jobs . . . It’s almost daily from someone, somewhere.’ Her colleague Brooke acknowledged: ‘I don’t think there’s anybody that can say they haven’t experienced it in care . . . You’ve really got to be the person who lets things slide if you’re in our job or you’re miserable.’ During the interviews, participants were asked to provide examples of WIB, yet at times had difficulty coming up with a single example. ‘I’ve seen it happen everywhere, at any of the homes’ noted Olivia, an LPN who worked at multiple sites, ‘. . . it’s almost like it happens so frequently that I kind of just brush it off . . . .’ References to ‘letting it slide’ or ‘brushing it off’ suggest over time the ubiquitous nature of incivility becomes an entrenched part of the workplace culture.
Two key themes reflect how staff experienced and explained peer incivility within the LTC workplace: firstly, a gendered work environment and, secondly, seeking informal power and control.
Gendered work environment
Intra-gender relations
The gendered nature of the LTC workplace featured strongly in participants’ experiences. Staff drew on gendered attributes as a means of explaining and thereby normalizing the uncivil behaviours they encountered. For example, criticism, gossip and cliques were considered part and parcel of working in an environment with ‘too many women’. Women faced criticism and judgement from both men and women for their intra-group behaviour. Emily relayed an encounter she had with a male co-worker at a previous worksite:
. . . he came in and plunked this plate of bird seed down on the table. And he was like, ‘Here you go. Help yourself.’ Because he said, ‘You’re all a bunch of hens. You all just sit there and [makes chirping noise], right?’ It’s what happens. I don’t know, it’s part of the genetic makeup of women or something, that need to sit and talk about whatever? You see it and hear it all the time . . .
This sentiment was echoed by Stacey: ‘women like to gossip . . . it’s like when you have so many in one place, it’s like everyone knows your shit’. Hen-like behaviour, gossiping or nit-picking were seen as inherently feminine traits:
But in general, women get really catty. I don’t know how else to describe that. And we try and pull each other apart . . . I’ve not worked with a large amount of men, so I don’t know if that’s the same with them or not . . . But with women, there’s definitely . . . that competition. And it’s like it’s just too many women in one place? I don’t know. Because sometimes it can just get to that with so many women in one place. They nit-pick each other, you know. (Brooke)
However, this suggests such behaviour may also be a reaction to the setting in which women find themselves. In a workplace where formal status, power and recognition are difficult to achieve, women compete for power and status in other ways, through the use of petty squabbles, blame and criticism. Indeed, cattiness has been described as an unhealthy reaction to otherwise healthy feelings of blame or criticism (Firestone, 2012). The challenge with this discourse and attributing traits to simply being women is that it sanctions the incivility, allowing bad behaviour to continue unabated. While having men as part of the care team was seen to change up the dynamic, participants acknowledged their intra-group behaviour resulted in higher turnover among their co-workers who were men:
Sometimes it can get very catty. But I think that’s anywhere where you have a lot of women together. I find when we do get men on the floor, it breaks up that oestrogen a little bit . . . It’s really nice to have male care aides around . . . [but] they don’t stay around for very long if they do because it’s catty. (Miranda)
It’s just like high school
The gendered nature of LTC contextualizes references made by almost all participants as to how their workplace relationships made them feel like they were still in high school – the gossiping and rumours, the cliques, the social exclusion and tit-for-tat behaviour when someone did something that ‘pissed them off’. RCAs’ experiences invoke the meme of the ‘mean girls’ of high school and yet many of these women were well beyond their high school years:
It’s really hard when you work there to have friends that aren’t going to throw you under the bus two seconds after you walk away . . . You think you have friends, but you don’t really . . . It’s not like any other workplace I’ve had before . . . It’s like being in junior high . . . some of them will be really happy to see you but deep down it’s because they want something. Not because they really want to help you and want to be nice to you. It’s because they know something else is coming up and they’re going to need your help to do it or they want you to do it for them. (Carolyn)
Here, Carolyn suggests her colleagues manipulate their social relationships for assistance with their workload. For RCAs, throwing someone ‘under the bus’ typically meant bad-mouthing a co-worker in front of families. If something was amiss with a resident (e.g. missing their dentures or unshaven) or in their room (e.g. soiled towels left behind), staff were quick to blame it on another RCA, ‘Oh, [insert name]’s on that wing today’, implying the RCA in question was neglectful in her work. While these behaviours likely reflect the culture of blame and criticism prevalent in many LTC homes, they also left staff questioning the sincerity of colleagues’ motives, potentially undermining the development of trust. When asked why RCAs might throw their colleague ‘under the bus’, one RCA speculated it was because it allowed them (by default) to look better and by doing so potentially elevated their own status in the eyes of residents’ families.
For Tina, the parallel between her workplace and high school was because ‘people are all in [other] people’s business’. The gossip, rumours and half-truths that ran rampant at her site led her to conclude ‘there’s no other way to describe it – it’s almost worse [than high school]’. Supervisors and managers also spoke of the gossip and rumour-mongering that occurred:
. . . there’s a multitude of staff I’ve never worked with directly . . . But I can tell you, it’s amazing what I know about those people. Amazing. Or what people want me to know about these people. I don’t know whether it’s true or not . . . I could tell you probably 10 things about every person I’ve not worked with and yet I’ve never actually directly worked with these people. (Sabrina) Staff love to tell tales . . . I guess the word is they love to rat each other out. Because you’d be amazed, you know, ‘Oh, so and so called in sick but I know she’s going to the [concert] . . .’. They just cannot help but tell us. (Monique)
Sabrina’s comment that it is what people ‘want her to know’ suggests there is an element of relational manipulation occurring, that staff are purposeful in the gossip they spread to portray a colleague in a particular light. Indeed, while Monique indicates staff cannot help themselves in ‘ratting out’ their colleagues, doing so potentially places them in a better light with the underlying subtext being, ‘I would never call in sick because I had tickets to a concert’. Such experiences reflect the larger organizational context. Staff shortages plaguing the industry meant staff were often not replaced when a colleague phoned in sick. Making sure management was aware of why someone was off sick was one way of punishing the individual for their apparent transgression.
RCAs also talked about other RCAs behind their backs – often such chatter focused on characteristics related to work ethic or job performance. Common terms included being too lazy, too fat, too short, or not strong enough to carry out their work, or not following protocol. Given RCAs’ perception that they only heard from management when mistakes were made, or when blame or criticism was to be levelled, it is of little surprise they took up such blame and criticism in their own conversations. The primacy of one’s status and reputation as a hard worker is illustrated in the experience of one RCA falsely accused of starting an unfounded rumour about an interaction between another RCA and a resident. ‘I don’t want my name to be ruined because of the gossip thing . . . I’m embarrassed of going to work because of what they [other staff] have heard . . . I’m a hard worker, don’t ruin my reputation’ (Bettina). For RCAs, who are accorded little formal power and status in the workplace hierarchy, their work ethic is the currency by which they perceive they are judged, on which reputations are staked and claimed. Gossip, rumours and back chatter not only sabotage such reputations but also collegial relationships. In an era of increasingly complex resident needs and workloads, RCAs do not want to work with someone perceived as not pulling his or her weight.
While friendship groups are not uncommon in a workplace, those at the study sites were particularly ‘clique’-like, a term used to describe groups that are by nature exclusionary (Barton et al., 2011):
You know [in high school] you’ve got your jocks, you’ve got your geeks . . . and I think it’s the same thing there, right? You’ve got your ones that are all into their beauty and there just to make a pay cheque. (Stacey) People have their own little groups they hang out with. So, you know who you talk to and who you don’t. You know I have my own clique I hang out with that I talk to about my stuff, they talk about their stuff with me. (Courtney)
Participants at both sites were consistent in their use of the term cliques. Courtney acknowledges the exclusionary aspect of the groups, when she notes: ‘you know who to talk to and who you don’t’. RCAs gravitated towards individuals with whom they were friendly outside of work, which meant at times other RCAs on shift were excluded from the laughter and inside jokes. This was particularly noticeable when a casual was working or a new RCA orientating. Certain RCAs would not talk to the casual/orientating RCA and, when break-time arrived, would head off together, leaving the third RCA to remain with the casual (typically breaks were taken one at a time to ensure adequate coverage).
The cliquey-ness and social exclusion was also evident during report or shift change, when staff gathered at the nursing station. Subtle body positioning and language conveyed which RCAs were in or out of the group:
Katherine and Courtney are already at the nursing station when Crystal approaches. Katherine stands near the filing cabinet towards the back of the nursing station, Courtney sits in front of her beside the RCA computer. Crystal extends a cheery greeting to Courtney, but blatantly ignores Katherine. She sits so she is positioned slightly behind and to the left of Katherine . . . The door to the med room opens and Katherine walks quickly into the room; the door closes and the other two continue to chat. A moment later, the door re-opens and Courtney and Crystal enter. Crystal positions herself beside the nurse; as report begins, she leans on the counter, her back towards Courtney and Katherine, and jots down notes . . . The nurse later comments no one ever stands next to her at report; given it was Katherine’s first day back after several weeks off, she feels Crystal was asserting herself and Crystal’s relationship with her to Katherine. Katherine later tells me she could’ve spoken to Crystal, as communication goes both ways, but she wanted to see what she would do [which in this instance, was to ignore and exclude Katherine; 3 hours into the shift, I have yet to see Crystal say one word to Katherine]. [FN01-38; 01/18/19]
The refusal to respond to a co-worker’s greeting was particularly egregious for Tina who interpreted it as a ‘slap in the face’. Believing such acknowledgement to set the collegial tone for the shift, she felt such behaviour could be interpreted as a blatant ‘screw you’.
At times, social exclusion was also employed as a means of punishment:
I’ve done it to people, I’m sorry to say . . . I think it was after the fourth time I worked with Jenna that she didn’t call or show up. The next day I was just like, I don’t want to talk to you right now. Like she kind of gets the cold treatment from us for a while. I’m like, there’s no reason not to phone or show up . . . She knows we’re mad and she doesn’t interact with us either. There’s this whole silent thing going on. And then towards the afternoon – it’s always in the afternoon – she’ll start, ‘Oh . . .’, like she’ll just try to sweet talk you a little bit. (Stacey)
In this instance, staff had complained to management about their co-worker’s behaviour. Frustrated with what they perceived as management inaction, their solution was to mete out their own version of justice. Such silent treatment is particularly damaging given the centrality of communication to RCAs’ ability to conduct their work efficiently and effectively. Staff also engaged in exclusionary behaviour as a means of revenge:
Me and Courtney, we literally just teamed up and left Katherine to her own. Because Katherine would never help us. So, we were just like, ‘Well, if she’s not helping us, we’re not going to help her’. We did that for probably 3 to 4 weeks. (Crystal)
Excluding co-workers as such meant the ostracized RCA had only the LPN to call for assistance when transferring or lifting a resident who required a two-person assist. Yet, typically, the excluded RCAs would simply proceed without help, placing the resident and themselves at risk of injury.
Seeking informal power and control
Staff also invoked the notion of strong personalities as a means of explaining their encounters with peer incivility, that it’s ‘just the way some people are’ in terms of their interpersonal skills and interactions with others. Yet, such references appeared less about immutable personality characteristics and more about informal power, control and status and how RCAs leveraged such power through overt and covert acts:
When I worked as a care aide, you always had that one person that, there was nothing you could do to get along with them . . . they were going to do it exactly how they wanted and if you didn’t follow suit, they were going to beak on you . . . you’re always going to have [those people], regardless of where you are. (Bridget)
For Bridget, there was a sense of resignation, that such individuals exist in all LTC homes and when co-workers do not acquiesce to that individual, they run the risk of becoming the target for blame and criticism. While RCAs go along with the status quo to prevent further discord, it further entrenches their co-worker’s quest for power and control.
Participants drew attention to RCAs for whom there was only one way, their way, to provide care and refused to adopt a different approach. While management might attempt to intervene, there was a sense of futility as the controlling individual simply directed their attention towards a new target:
. . . it’s almost like it’s a power struggle with them. It’s a game. It’s this ‘I need to be in control’ personality, right? And if they’re not getting along with one person and you shut them down in that avenue, then the next thing that employee . . . is now onto another employee. (Kari) . . . you have those that instead of using it [informal power] to the benefit of advocating on behalf of everyone, use it to manipulate their own agendas into always getting their own way and never apologizing. I’m just going to strong-arm my way in there because I can . . . This is how it’s done and how we’ve always done it. (Meredith)
These individuals could create considerable dissension on a unit; who their co-workers were and the extent to which they were willing to relinquish control set the mood for the entire team. Issues arose when more than one individual wanted to be the one to say: ‘This is how you do it and you’re doing it wrong’.
Often, those identified as controlling were long-tenured RCAs who had been at their site for five or more years:
. . . a lot of people think that this is just their personality, but I say it’s not. Like they didn’t start at this job with this personality, you can bet. And if they went to a new job, they wouldn’t be acting like that to tenured staff . . . (Brooke)
These RCAs had learned to use their considerable on-the-job experience and ensuing sense of entitlement to manipulate their informal power and maintain the status quo that made work comfortable for them, but difficult for others. In the field note excerpt below, two RCAs are working to transfer a resident; Brooke has been at the site less than a year and Courtney for more than 5 years:
Courtney and Brooke start to position the sling and lift. Courtney pipes up, ‘Before we go any further, this is what I do. I bring this [sling] down’, and she demonstrates for Brooke . . . Brooke is not new to this resident [Phyllis] or the unit. Although currently assigned to this wing, when she starts in with the sling, she is stopped by Courtney. I’m not sure if Brooke’s approach is ‘worse’ than what Courtney is proposing, but it’s clear from the exchange Courtney feels her way is the ‘right’ way. Her ‘before we go any further’ comment feels like an attempt to assert herself as the one in the room with more experience. She clearly assumes the lead in the interaction, even though it is currently Brooke’s wing. Brooke defers to Courtney but attempts to translate Phyllis’ wishes about where to position the incontinence pad: ‘She just wants the pad between her legs hidden’, says Brooke. ‘Why Phyllis?’, says Courtney, ‘you can’t see it. Why create extra work if no one can see it?’. Her voice becomes louder, her tone edgier. [FN01-43 01/29/19]
When the supervising LPN was a recent graduate, this entrenched sense of informal power created additional friction. Reflective of the potential practice–theory knowledge gap between RCAs and LPNs, longer-tenured RCAs would bristle at being told by the newer/younger LPN how to do something. While the LPN, as the team lead, held the formal power and status, the longer-tenured RCA possessed the social power, which they could use to usurp the LPN. However, as Brooke astutely pointed out: ‘You have to have the leader be in charge, not everyone under the leader thinking they’re in charge. It doesn’t work very well when it looks like that.’
Discussion
This study critically examined RCAs’ experiences of WIB in two LTC homes in British Columbia, Canada. Findings add to the very small body of literature regarding RCAs’ encounters with workplace mistreatment, highlighting the primarily covert incivility rather than the more overt bullying, to which they are exposed. This is an important finding given that the primary focus on workplace mistreatment among healthcare staff has centred on bullying; that is, overt, direct behaviours intended to undermine, humiliate, denigrate or injure that occur on a regular basis for an extended period of time (Einarsen et al., 2009).
With regards to the first research question (i.e. what are the types of WIB to which RCAs are exposed), the nature of the behaviours discussed and exhibited by participants appear illustrative of relational aggression, a construct used extensively in researching bullying among (pre)adolescent girls (e.g. Björkqvist et al., 1992), but rarely examined within workplaces or among healthcare workers (Dellasega et al., 2014). Relational aggression refers to non-physical, manipulative and exclusionary forms of social aggression that threaten friendships and relationships (Archer and Coyne, 2005) and encapsulate RCAs’ behaviours, such as gossiping, spreading rumours and social isolation/exclusion. It is thereby of little surprise RCAs referred to their workplaces as ‘just like high school’, a setting in which such behaviours predominate. McAndrew (2014) refers to relational aggression as ‘covert strategies of social competition’ (p.197). Indeed, this is reflected in the RCAs’ ratting out of their colleagues to supervisors or throwing their co-worker ‘under the bus’ in front of a family. Doing so potentially elevates their status in the eyes of those who judge them (e.g. supervisors and families).
Expressed in a socially skilled manner, relationally aggressive behaviours remain under the radar, making it appear as if there was ‘no intention to hurt at all’ (Björkqvist et al., 1992: 125). Consequently, they are an ideal way for perpetrators of workplace incivility to evade repercussion. As relational aggression is not readily observable to those not enmeshed within it (Gomes, 2007), managers who spend little time on the unit may not readily pick up on the nuanced interactions occurring among RCAs. By the time behaviours come to their attention, the downward incivility spiral is well underway, creating an environment in which anxiety and mistrust flourish (Dellasega et al., 2014).
The second research question focused on how social locations and broader organizational factors influence RCAs’ WIB experiences. RCAs’ encounters can be situated within oppressed group behaviour; that is, how intra-group conflict is expressed in the context of being excluded from the power structure (Roberts, 2015). As Freshwater (2000) observes, the greater the visible order (i.e. hierarchy) within the healthcare workplace, the greater the invisible disorder. In a system in which RCAs possess little structural power, their intra-group relations are tied to tensions and struggles around the informal power they hold. Situated far down the power hierarchy, RCAs resort to intra-group aggression as a means of achieving social status and dominance. Superiority, control and power are thus sought and expressed through relationally aggressive behaviours.
Women’s gender stereotypes convey that the ‘ideal woman has concern for the welfare of others and displays behaviours aimed at being kind, cooperative, helpful, sympathetic, gentle and nurturing’ (Sheppard and Aquino, 2017: 695). Such stereotypes also describe the ‘ideal’ RCA. Utilizing overt physical confrontation as a means of resolving conflict and establishing dominance at work is inconsistent with such stereotypes, leading RCAs to utilize more subtle, socially manipulative means that impact communication, social relationships and reputation (Salin and Hoel, 2013). George (2008) notes many female carers internalize stereotypical roles defined by self-sacrifice, silent suffering, altruism and piety. Such self-sacrifice and silent suffering can be seen in participants’ references to the importance of ‘letting things [i.e. incivility] slide’ or ‘brushing it off’ as a means of surviving in the job. Given such gender stereotypes, it is not surprising that participants attributed workplace conflict to the presence of ‘too many women’. However, such perceptions are problematic as they not only normalize incivility as an intrinsic part of care work, but also attribute the source of uncivil behaviours to women’s own behaviour rather than to the broader organizational context (e.g. the unequal positions held by RCAs in the LTC hierarchy) that (re)produces structural disadvantages (Sheppard and Aquino, 2017).
As in other studies examining RCAs’ work life (Chamberlain et al., 2019; Willemse et al., 2012), participating RCAs experienced high job demands (i.e. increased resident complexity, heavy workloads) and low job control (little decision-making autonomy). Human resource shortages within the industry meant absent RCAs were frequently not replaced, further increasing workload challenges. Not surprisingly, when workplace resources are scarce, competitive behaviour and interpersonal hostility increase, while relationship-maintaining behaviour decreases (Sheppard and Aquino, 2017). Such a pattern is reflected in RCAs drawing attention to workers who called in sick yet posted on social media their presence at a social event, the social exclusion used to punish co-workers who failed to show up for a previous shift, and the blame and criticism levelled at co-workers when beds were not made, rooms were not tidied and residents went unshaven. Indeed, a culture of blame is common to many LTC homes due in part to limited resources, high workload and overwhelmed leadership (Scott-Cawiezell et al., 2006).
RCAs’ encounters with workplace incivility suggest a certain level of dysfunctional teamwork. The presence of cliques, and the associated behaviours of blame, criticism and exclusion, are divisive, setting up an us versus them dynamic detrimental to the social cohesion and trust essential for team functioning, destroying unit morale and increasing turnover (Barton et al., 2011). The social exclusion displayed towards new or casual RCAs may also preclude the new/casual RCA from asking questions of others, potentially adversely impacting resident care should they subsequently do something wrong. Intra-team conflict stems from both task and relationship conflict. The former pertains to disagreements around tasks, objectives and procedures and can be viewed as a strategy to enhance one’s own power and influence at others’ expense (Gamero et al., 2008). Task conflict is evident in RCAs’ experiences in dealing with staff for whom there was only one way (i.e. their way) to provide care and who, according to their co-workers, manipulated their own agendas into getting their own way. Teams engaged in task conflict may inadvertently prompt relationship conflict, in which disagreement over task-related issues is perceived as personal criticism and incompatibility (Gamero et al., 2008), as illustrated by RCAs’ perceptions that incivility results from strong personalities (i.e. just the way some people are). The danger is that offended team members respond with personal attacks of their own (e.g. refusing to help a colleague because the colleague never helps them), perpetuating the incivility spiral.
Supervisors and unit managers play a key role in fostering civility, cohesion and trust among RCAs. However, the interpersonal communication skills required to do so are not necessarily innate and thus additional training is required of LPNs and managers to improve their skill set and confidence. Given the subtlety of relational aggression, managers are encouraged to be actively engaged and visible on the unit. In addition, managers may want to seek ways to flatten the LTC hierarchy, thereby increasing the sense of autonomy and control among RCAs.
Study limitations
Participating RCAs were primarily Caucasian, Canadian-born and enjoyed relatively stable tenure as an RCA and at their workplace. While representative of the regional demography of English-speaking Caucasians and RCAs within the area (Chamberlain et al., 2019), their experiences of WIB may not reflect those of other ethnic groups more commonly involved in care work in larger urban centres (e.g. South Asian, East Indian). Similarly, RCAs were unionized and employed at not-for-profit sites. The experiences of those working in owner-operated or private for-profit sites may be different. There was limited involvement from differing levels of senior management. Future research will want to explore the role of management within RCAs’ experiences of incivility.
Conclusion
The work of RCAs is mentally and physically demanding. Exposure to peer incivility further exacerbates the difficult nature of the work and disrupts the respectful, collaborative relationships essential to quality care provision. This study makes several meaningful contributions to the extant literature. Primarily, it is one of the few studies to examine workplace incivility among the understudied workforce of RCAs in LTC. Secondly, it offers a nuanced understanding of the types of behaviours to which RCAs are exposed. Finally, it highlights the problematic, subtle and insidious workplace interactions that do not rise to the level of overt, explicit bullying commonly prohibited in workplace law or organizational policy. The gendered nature of RCAs’ experiences of incivility and the ways in which power is experienced and channelled highlight the importance of developing gender-informed workplace policies and procedures. Attending to issues of gender, power and inequality appears key to ensuring RCAs’ workplace relationships mirror the care and compassion underlying their daily care practice.
Footnotes
Acknowledgements
We wish to thank the study participants, who so willingly welcomed us into their world and candidly shared their experiences with us, our research assistant, Kaitlyn Murray, for her assistance with data coding and management, and our Community Advisory Committee for their valuable insights into the study findings.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: support for this research was provided by the Alzheimer Society of Canada (Post-Doctoral Award), the Michael Smith Foundation for Health Research (Research Trainee Award) and with funds from the WorkSafeBC Research Program.