
Abstract
Taking a longitudinal case study approach, this article examines the process of rule breaking in a newly formed UK domiciliary care provider. In this study, the founder acted in such a manner so as to partially decouple the organization from externally imposed institutional rules and regulations, allowing the emergence of informal rules between carer and client. These informal rules increasingly guided the behaviours of care workers over time, resulting in the breach of formal strictures. Building on the dimensions of hierarchy and contentiousness, rule breaking is conceptualized here as a phenomenon which occurs as a result of the tension between competing formal and informal rules, at multiple levels throughout the organizational hierarchy.
Introduction
In the New Public Management of health and social care provision in the UK, a combination of regulation and market competition have been put forward as the solution to longer-term cost efficiencies and competitiveness. However, these solutions place the state in an ambiguous position (Ferner and Colling, 1995). On the one hand, it has a stake in ensuring privatized services have popular legitimacy. This is particularly the case in social care, given the sector’s growth, and regular public scandals around abuses. On the other hand, too close a monitoring of service quality may undermine the intended appearance of competitive market-based integrity of the privatization process. This balancing act is also played out at many levels, as organizations, managers and frontline workers act to reconcile the often competing demands for competition and regulation. It is within this context that different manifestations of rule breaking can occur.
When studying service providers, exploring the complex interrelationships between organization, employee and service users becomes particularly important (Lopez, 2010), and some have extended this multi-layered approach in the study of rule breaking (Bensman and Gerver, 1963; Gouldner, 1964) in organizations. Recently, Martin et al. (2013: 559) defined rule breaking ‘as an organizational phenomenon captured by two core dimensions: the level of social action (individual, group, or organization) and the intensity of rule enforcement’. First, rule breaking has hierarchical dimensions – individuals or groups at the frontline may break rules on their own accord, or it may be initiated by managers; the latter may range from the pursuit of organizational goals, to outright white collar crime (Martin et al., 2013). Lower-level rule breaking may be abetted by management, allowing them to absolve themselves of responsibility in the event of exposure. Second, as Martin et al. (2013) note, rule breaking may be permitted or opposed by management, and varies in the extent of contentiousness and how intensely rules are enforced. Rule breaking thus exists on a continuum between contested and permitted. Furthermore, rule breaking may be a social phenomenon, coordinated by work groups or an individual act (Martin et al., 2013), the core focus of this article. While Martin et al.’s (2013: 559) account focuses on departure from formal rules, they do not consider violations from informal norms of expected behaviour, nor the creation of new informally constituted rules. Rather, they point towards ‘understanding the interplay between rule breaking and informal norms as a critical next [research] step’ (Martin et al., 2013: 571). Addressing this call, in this study the role played by emerging informal rules on formal rule-breaking behaviours is investigated. Taking a longitudinal case study approach, the growth of a small UK domiciliary care provider was tracked from start-up to its tripling in size in just 12 months. Domiciliary or home care involves the provision of social care services to adults in their homes. As with many organizations operating in this area, the firm was not unionized; hence, workers lacked access to a key channel for voicing any concerns.
This article makes two key contributions to literature in this area. First, drawing on Martin et al. (2013), rule breaking along the dimensions of hierarchy and contention is examined. Rule-breaking behaviours are reinterpreted within the context of a multi-layered system of legitimization, as the founder acted to decouple external and internal processes of legitimization. By adopting institutional rules and regulations at start-up, the founder first sought to achieve external legitimacy within the marketplace. At the same time, she differentiated the company’s service offering from the competition by emphasizing continuity of care and the development of client-focused relationships. Second, the founder sanctioned rule-breaking behaviours among care workers, when it was perceived that such behaviours were (a) in the best interests of clients and (b) when formal rules were seen to hinder the delivery of this client-focused service offering. However, in the absence of formal rules, and as relationships developed between carer and client, informal social rules emerged, which increasingly guided interactions and, with this, formal rule-breaking behaviours. The emergence of these informal rules was driven by values of social care and justice held by the care workers. It is argued here that, given the ambiguous, idiosyncratic and informal nature of care provision, as represented by the carer–client relationship, externally imposed formal prescriptive rules are perceived as inadequate and treated as such. In other words, rule-breaking behaviours sanctioned by the founder allowed the organization to pursue a competitive market position, while maintaining the outward appearance of legitimization. Therefore, this article seeks to add to Martin et al.’s (2013) conceptualization of rule breaking by highlighting the role played by informal rules alongside formal rule breaking. Thus, rule breaking is conceptualized here as a phenomenon which occurs as a result of the tension between competing formal and informal rules, at multiple levels throughout the organizational hierarchy. When competing rules are incompatible, following emergent informal norms may result in formal strictures being broken. This struggle is played out across levels, through the behaviours of individuals, groups and organizations. Contentiousness in this sense refers to differing interpretations of, and power struggles around, competing sets of formal and informal rules.
The article thus explores the process through which the rule-breaking process is engendered and persists through interactions between employees, owner and client and through overlapping agendas: effective client-centred service delivery, organizational performance and duties of care. The study unpacks the multi-layered nature of rule-breaking behaviours, including the manner in which such transgressions on the part of care workers are justified – and, at times, even imparted with a degree of moral purpose – and the ambivalent role of management as agents of both formality and misconduct.
Rule breaking and the care sector
The relevance of rule-breaking behaviours is particularly salient in the care sector, with public sector reforms resulting in the promotion of predetermined standards and associated rules (Dibben and James, 2007; Le Gales and Scott, 2010). In the case of care provision there are two strands of externally imposed regulation. The first, more ideologically motivated, seeks to promote and manage the market for social care. In the UK, the Community Care Act (1996) was put in place to give power of choice to clients, by putting finances in their hands and giving them the choice to directly employ carers (Morris, 1997; Ungerson, 1999). While the rhetoric of ‘consumer choice’ has attained dominance within New Public Management (Dibben and James, 2007), this has often been coupled with increasing regulations aimed at micro-managing such a process, either to promote an ideological agenda and/or to favour certain commercial players within a sector. The second strand of regulation, more directly orientated towards immediate patient well-being, seeks to uphold the quality of care provision, although, in reality, these two agendas may overlap. The Care Quality Commission (CQC) is an independent regulator of all health and social care services in England with legal powers. All care providers must register with the CQC, which sets rules and operating procedures and inspects all domiciliary care providers at least once per year, including interviews with clients and staff, checks on formal systems and procedures, and assessments of standards of quality and safety. Guidelines set out by the CQC, however, allow some room for manoeuvre for organizations, with regards to the specific practices adopted in, say, recording medication, providing these practices address key quality measures. In addition to such regulatory and institutionally linked rules, many companies also adopt organization-specific rules (e.g. wearing uniforms).
What sets these regulated sectors apart is that many of the standards and rules are imposed from outside the organization (often ultimately devised by external consultants; Le Gales and Scott, 2010), which means that aspects of them may lack legitimacy in the eyes of managers and workers alike and be poorly aligned to the realities of day-to-day practice (Mascini, 2005). Given the complexity of care, and the unpredictability of some older adults, the rigid adherence to standardized guidelines is at times not in the interests of the latter, and can conflict with the personal values of the care worker (Carlsson-Wall et al., 2011). As a result, the breaking of generalized hard and fast rules is a key element in the provision of care (Bolton and Wibberley, 2014; Burns et al., 2013; Carlsson-Wall et al., 2011), with care companies and clients regularly relying on the discretionary effort of carers who do things beyond the care plan (Bolton and Wibberley, 2014). Changing economic pressures in the care industry have further resulted in an increasing focus on cost efficiencies, and pressures to standardization (Carlsson-Wall et al., 2011). Yet, to cope with the complexities of the job, care workers often have to decide what care to deliver, resulting in tasks being completed outside the care plan, or not following guidelines when they conflict with the carer’s understanding of the client’s needs (Bolton and Wibberley, 2014). As the industrial relations literature alerts us (Hyman, 1975), smooth production may depend on everyday low-key rule breaking of unnecessary or minor strictures, making ‘work to rule’ such an effective union tactic (Kleiner et al., 2002).
A central concern of the literature on the moral economy of the workplace is the intertwined nature of the economy and society; ultimately, the latter is reliant on the persistence of a social and moral sphere. It further highlights the extent to which the employment relationship is not simply a transactional one, but encompasses a range of moral and social relations (Bolton and Laaser, 2013: 517), including the empathy and moral agency components of work and employment. It is within this context that rule breaking needs to be viewed. Individuals engage in particular types of behaviour in response to the different ties and pressures that may pull them in different directions: towards the organizational agenda, their ties with peers and their perceived duties to clients and other stakeholders. Organizations might further adopt rules ceremonially, by decoupling external strictures and internal operations (Meyer and Rowan, 1977). Seeking internal flexibility to dilute external systemically imposed rigidity thus rests at the heart of rule-breaking activity (Hodson et al., 2012; Meyer and Rowan, 1977).
In this sense the emergence of informal rules, which act to challenge externally imposed strictures, give individuals the opportunity to innovate and manage this flexibility (Ackroyd and Thompson, 1999; Burawoy, 1979). What Burawoy (1979) calls ‘making out’ is a game played at the group level, with its own set of informal norms and rules, which compete and at times triumph over formal organizational rules. By adhering to formal rules, ‘management is being accused of “cheating”, of not playing according to the rules of the game; and these accusations serve to reassert the legitimacy of the rules and the values of making out’ (Burawoy, 1979: 83).
The autonomy achieved through this process of self-organization reflects a need for local rules to meet the interests of those concerned, including values of social justice (Baines, 2011; Bolton and Laaser, 2013). For example, Blau (1964) found that frontline receptionists at an unemployment agency broke rules when they saw such actions as helpful to jobseekers. Similarly, Hutchinson (1990: 4) found that nurses broke ‘illegitimate’ rules, arguing that ‘a principled level nurse … questions rules that do not serve human values’. Again, as Bensman and Rosenberg (1963) argue, employees break rules in order to accommodate client or subordinate needs, and as a result either empower themselves or better identify themselves with the client. Although often depicted in negative terms, such rule breaking may fulfil a social function and contribute to organizational and/or stakeholder well-being (Morrison, 2006).
However, management themselves also have a role to play in such rule-breaking behaviours, as they attempt to balance conflicting goals at different levels. Indeed, ‘forbidden’ behaviour may be sanctioned and supported by frontline managers (Bensman and Gerver, 1963). Hence, a key distinction is between managerially encouraged rule breaking to get the job done and employee motivated rule breaking to impart work with meaning, challenge managerial authority and/or uphold notions of duty or professionalism; as noted above, rule breaking varies according to contentiousness and underlying rationale (Martin et al., 2013). It also makes it harder for employers to crack down on rule breaking that goes beyond what is managerially sanctioned: workers may respond by keeping to all rules, undermining the capability to get the job done. As with the precise amount of labour power provided, the commitment to adhere to managerial rules that form an inherent part of the employment contract is never something that can be fully enforced or even clearly delineated (cf. Hyman, 1975).
Ackroyd and Thompson define misbehaviour, in encompassing a wide range of activities from pilfering to adjusting production rates, as ‘deviation from expected standards of conduct’ (1999: 3). As Taska (2012) notes, rule breaking also may involve the making of new informally constituted rules. This is importantly different from ‘misbehaviour’ in that it is not just about engaging in conduct that contests ‘matters related to work, product and identity’ (Ackroyd and Thompson, 1999: 25), but also delineating, albeit informal strictures, as to what constitutes acceptable behaviour. Rule breaking may not only encompass the type of creativity and informality that characterizes misbehaviour, but also attempts at legitimization (Martin et al., 2013). Finally, unlike a significant component of rule breaking, outright misbehaviour is generally not something encouraged by management.
Research method
This study seeks to explore the process through which rules are broken over time, and indeed in the first instance. By examining these behaviours at multiple levels of analysis (Carlsson-Wall et al., 2011), light is shed on the process through which individuals and groups deviate from rules imposed at an institutional and organizational level. To address this objective, a longitudinal case study approach (Eisenhardt, 1989) was taken, in which the growth of a firm operating in the UK domiciliary care sector was tracked from start-up to tripling in size in just 12 months. While studies of the care sector have been carried out before (Essen, 2008; Eustis and Fischer, 1991; Ungerson, 1999), this study focuses on the emergence and development of practices over a period of time following the business start-up. In addition, past studies have largely focused on the views of clients, with little research examining care from the perspective of the care worker, or the management of those care workers within a growing small business context (Eustis and Fischer, 1991; Ungerson, 1999). It is argued that this perspective is needed given the nature of rule-breaking behaviours. As a result, the case chosen captures the emerging practices through interaction between carers, client and owner-manager. The study was therefore carried out in two stages:
Stage I: In this stage the behaviour of the start-up group of employees working at the organization between August and December 2010 was studied. In-depth interviews (between 1 and 1.5 hours) were carried out with the founder, senior carer A, and carers A–D (a total of 10 employees worked at the organization at that time). Interviewees were asked to describe their daily care activities, and how these changed over time. Both observations and recorded daily log entries were used to confirm descriptions of behaviour given (Eisenhardt, 1989). The researcher spent a period of 1 month during August/September 2010 observing the behaviours of senior carer A, and carers A–D at the home of client X. The client in question had been with the organization since its founding and employed all carers mentioned. Copies of all daily logs were also taken during this period. In this manner a typical care arrangement was tracked over a period of time, during which the researcher spent between 1 and 2 hours, typically 4 days per week, at the client’s home. As shown below, these observations were used to verify interview responses, observe behaviours and include the client’s perspective in the research.
Stage II: In this stage the researcher spent a total of 15 days at the offices of the company, and a further period of 1 month in May/June 2011 observing the changing behaviours of carers A–D in the home of client X. Copies of accompanying daily log sheets were taken. Client X was also interviewed to explore changes in behaviours of the care group over the previous year. During this period a total of 30 employees were working for the organization, of which 17 were interviewed, including the founder, all four senior carers (senior carers A–D), the training manager and 11 carers (carers A–K). As in Stage I, interviewees where invited to describe in detail their daily practices, including the key tasks completed, interaction with clients, other carers and the owner-manager. In addition, they were asked about key changes which had occurred over their period of employment with the organization. Given the sensitive nature of the research carried out, agreement and consent was sought in advance with the founder, all participating care workers and client X (the latter being known to the researcher before the study). In order not to compromise the client or any of the care workers, observations did not include any tasks which might be considered personal or sensitive in nature (e.g. showering, washing).
The study focused on analysing and interpreting the anonymized narratives given by individuals as they described the emergence and development of care relationships over time. To avoid precedence being given to prior theoretical views, an attempt was made to represent the experience and interpretations of informants, and as such the approach adopted for this study can best be described as interpretivist. In order to allow key themes to emerge from the data, analysis was carried out concurrently at both stages of data collection. In Stage I, all interviews were fully transcribed and, together with detailed field notes, were manually analysed and coded to identify key emergent themes. In Stage II, the interview format was altered slightly, with individuals being asked to elaborate on these themes. Again, coding and analysis was completed in parallel (using NVivo 9). This analysis consisted first in identifying key themes drawn directly from interview responses given by participants, observation field notes and daily log records (Eisenhardt, 1989; Yin, 1994). From these concepts in use, second-order relationships were identified between and among these emerging themes. This involved a process of constant comparison in which comparisons were made between participants and observations, and over time in both stages of the research. In this way, a convergence in theoretical relationships was identified. These themes and relationships were further analysed and compared with key concepts in the extant and enfolding literature as discussed below. A limitation of the research is that it did not encompass the stories of the subjects of the care (with the exception of client X), who, it is recognized, may have alternative understandings as to the operation of the rules governing the carers and the extent to which rule breaking really serves their interests or not.
Findings
Formal rules at start-up
At start-up the small business owner put in place a number of formal policies and procedures specifically in relation to the delivery of care, many of which were required as part of the registration process with CQC. Table 1 summarizes these key organizational policies, regulations and rules, which include a mix of abstractly defined, managerialist rhetoric, more specific company rules (e.g. uniform requirements) and regulatory requirements (e.g. review and monitoring procedures).
Company procedures and documentation introduced following start-up.
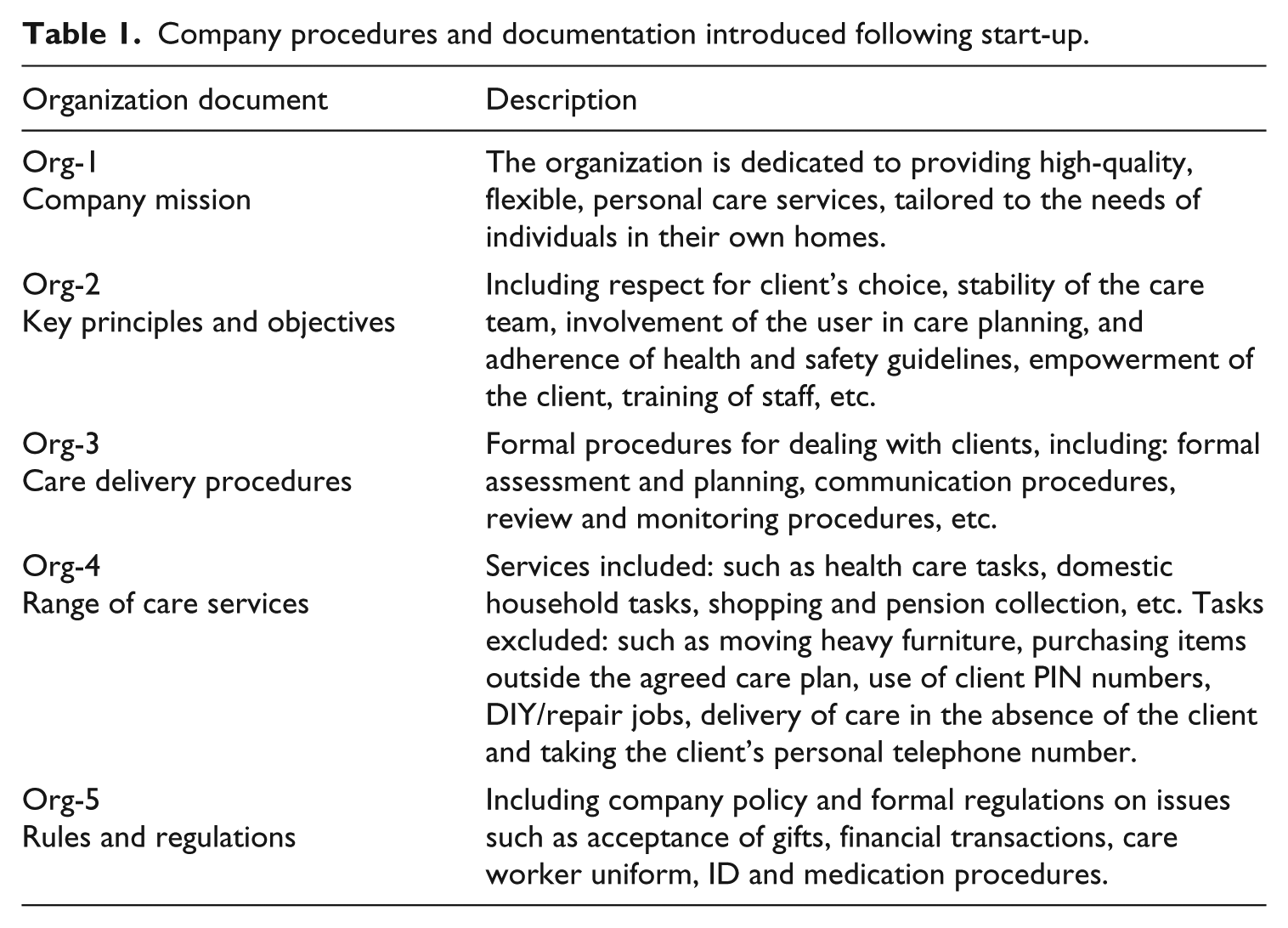
Most of these formal practices, such as client assessment, planning, review and monitoring procedures were dealt with directly by the owner-manager, who had previously worked as a care manager with a large competitor. Other policies related to the delivery of care and were discussed in detail with all care workers and clients during induction and initial client visits, respectively. Printed copies were also retained at every client’s home. Rules and procedures relating to the delivery of care (e.g. how the care worker developed his/her working relationship with the client) were unclear, and focused instead on key ‘dos and don’ts’ (e.g. do not use the client’s bank cards to withdraw cash, do not take the client’s telephone number, etc.) (see Table 1). This reflects the trend noted by Bolton and Wibberley (2014) towards documenting only the explicit aspects of care, as opposed to the more ambiguous nature of emerging relationships and behaviour. Equally, while the founder ‘trained’ carers in how to carry out key formal practices such as completing daily log sheets, or medication sheets, she had little direct involvement in how the care workers delivered care to clients. Though formal control procedures were in place, as shown in Table 1, to monitor the quality of care provision, the founder also ‘kept an eye on things’ through informal communication directly with both clients and carers. In this way, both carers and clients could directly contact the founder whenever anything ‘out of the ordinary’ occurred (as noted below, these ‘extraordinary’ occurrences became much less frequent over a period of time): … If there [are] any issues then she’d ring the carers and ask us if there [are] any issues as well … (Senior Carer A) … If there’s a problem I’ll phone them straight away and say ‘why has this happened?’… (The founder)
Observations during Stage I of the research revealed all carers closely following these key formal procedures, with the exception of senior carer A. Senior carer A on the other hand regularly did not wear a uniform, changed the care rota without informing the office, bought medication for the client and frequently failed to complete daily log and medication sheets, effectively breaking organizational rules 3–5 (see Table 1). By contrast, other care workers recorded notes in the daily log sheet, completed medication and financial transaction sheets and adhered to the guidelines set out in the care plan (e.g. wearing the uniform). Any instances which involved tasks not specified in the care plan were referred back directly to the founder, either by telephone or face-to-face. In this way, carers tended to abrogate the responsibility for difficult decisions, including those which resulted in departure from the rules.
Formal rule breaking one year later
One year later, the founder was no longer involved in all new client assessments, or shadowing new care workers, with these tasks being increasingly completed by senior carers (who were now based at the company’s offices). Senior carers had also begun to complete biannual care reviews with clients. As noted above, following start-up the founder maintained informal lines of communication with all carers and clients, but this proved harder over time: … Initially when I was small I probably spoke to all the service users each week. I had time to call them and say, ‘everything ok, fine?’… But that’s not going to work as I’m getting larger, I’m realizing that I need to have somebody that I trust to do it how I do it … (The founder)
Over the first year, the operation also became increasingly spread out over wide geographic distances. This resulted in care workers travelling further between client visits, and so spending less time with clients. One year later, incidents of rule breaking had also increased. For instance, in Stage II, both senior carer A and carer B failed to wear uniforms, as the founder herself noted: … I presume that all my carers wear uniforms [but] one service user said, not always … (The founder)
Some of this rule breaking, such as choosing not to wear uniforms, may simply have constituted a departure from company procedures. The founder argued that the uniform was key to presenting the organization in a professional manner. Carers broke this rule for a number of reasons, ranging from convenience or personal finances (e.g. not having a clean, spare uniform), to keeping the client happy (e.g. for clients who preferred that the carer did not wear a uniform on social excursions). Other rule breaking, such as a failure to take adequate notes, or not following guidelines in the administration of medicines, were clearly at odds with external CQC requirements. In Stage II, for example, carers B and D were less thorough in completing daily logs and finance sheets, while carers A–D withdrew money for client X and regularly bought additional medication: … I think as a whole some carers don’t document as much as they should with medication … I think sometimes people are too lax with medication … (Carer C)
In Stage II, all carers also changed care rotas without informing the office by contacting the client directly: … I would ring [the client] straight away rather than bother the person who is on-call in the office … (Carer I)
Carers also completed tasks outside the care plan, delivered services when the client was not at home and regularly accepted gifts from clients. This is reflected in the following daily log entries: ‘… collected parcel for X …’ (Carer A) ‘… popped to Boots for codeine …’ (Carer D) ‘… posted a letter …’ (Carer A) ‘X out, instructions to let myself in …’ (Carer B) ‘Let myself in, X not at home …’ (Carer A)
So what became evident is that with growth also came more rule breaking, and that increasingly it was not formally managerially sanctioned. At the same time, the founder made it clear that flexibility, being caring and able to respond to client needs on a personal basis had enabled the organization to gain advantages over its competitors: rule breaking may have helped carers at times provide a better quality of care, and fulfil social needs, but it also served commercial ends – different objectives that became blurred.
The carer–client relationship and rule breaking
Despite the absence of formal rules and guidelines concerning the delivery of care, a strong degree of thematic similarity emerged in discussions with employees with regards to how they delivered care. The founder had attempted to differentiate the company’s service with the promise of consistency, and this allowed carers to develop trusting relationships with clients over time. This in turn facilitated communication, as the carers tailored behaviours to the specific needs of the client. Working at clients’ homes, of course, means that work is spatially highly fragmented, making continuous managerial monitoring and the uniform enforcement of rules impossible. This gives carers a great deal of flexibility in their interactions with clients (albeit subject to time constraints), allowing for the evolution of relationships that transcend the depersonalized exchanges characteristic of modern economic life (see Simmel, 1980), and with this the emergence of informal social rules guiding and shaping behaviours and interactions: … You build that trust with them for them to be able to tell you things they wouldn’t normally tell anybody else … (Carer G) … Once you get to know them then you will know … they don’t want that or they don’t want this … (Carer J) … It is sort of a relationship but a working relationship. It is just talking to them and getting to know them … finding out things that they like … (Carer H)
In effect, alongside these developing relationships, norms and social rules emerged between carer and client that had greater legitimacy for both (Bensman and Gerver, 1963; Taska, 2012). Given the degree of legitimacy of such local social rules to both parties, at times these took precedence over what might be perceived as broad, rigid and ill-suited formal regulations. These informal norms reflect the clients’ own conceptualization as to what constitutes acceptable behaviour which, in turn, gradually evolves as it is largely removed from the sight of managers. Many of the breaches observed stemmed on the one hand from the fundamental tension between emerging client-specific norms and ‘social rules’, which were created through developing trusting caring relationships with clients, and on the other hand adhering to prescriptive care plans and rules concerning the delivery of care (Bolton and Wibberley, 2014; Carlsson-Wall et al., 2011). Moreover, the emergence of these informal rules allowed care workers to redress perceived imbalances in the moral economy, becoming more aligned with their own values of social justice. As the company grew, lines of communication between carer and founder became less frequent, with care workers increasingly using their own judgement in deciding whether to complete additional tasks consistent with these informal rules: … sometimes you end up doing extra than the care plan anyway because there is always little, other little things that they can’t do and you might do it for them … (Carer H) … I always say that I treat my clients as I would expect a carer to treat any of my family … to want to do this job you have got to have a caring nature otherwise you won’t last doing it … (Carer G)
In this manner, formal rule breaking was justified on the grounds that it might be in the client’s best interest (such as withdrawing money when the client was unable to), as care workers used their judgement and initiative in assessing whether or not they should do additional tasks (not included on the care plan).
The carer–founder relationship and rule breaking
One might argue that given the small size of the organization, the founder might have acted to influence these rule-breaking behaviours and, as a result, the development of these emerging and potentially deviant ‘social rules’. As the company grew, informal communication with the founder (or ‘the office’) had become less frequent (as noted above). For instance, following start-up, carer A noted that she contacted the founder to gain approval for any request which was ‘out of the ordinary’ (including filling a hot water bottle) and refused to complete tasks without formal approval. One year on, she completed a number of tasks which were outside the formal care plan, including withdrawing money for a client and answering personal phone calls during care visits. However, it would be mistaken to assume that such rule breaking was an indication of increased ‘lawlessness’. From conversations with the carers, it was noted that initially transgressions beyond the company rules were first checked with the founder, or the senior carers, which would seem to imply that the owner-manager herself allowed rules to be altered or departed from when she felt it was in the best interests of the client. For example, carers A–D withdrew money for client X following an initial informal approval being given by the founder. This exception to the rule was seen to be in the best interests of the client, who was unable to access the bank due to severe mobility issues and a lack of informal care support. In other cases, ‘trusted seniors’ similarly acted on behalf of the founder to either condone activities, or in some cases lead by example. For example, from observations it was seen that senior carer A frequently broke rules concerning uniform wearing and completing log sheets immediately following start-up. This individual had known the founder for several years, and the latter believed that she would only break rules if this was in the best interests of the client: … I’m very much like [the founder], in the respect that I care … Me and [the founder] have worked together for about 6 years in these bigger companies. She thought the same as me … (Senior Carer A)
Following her example, in Stage II of the study, all care workers within the same group were breaking rules to some extent: … if they’re asking you to do something reasonable and you have got time to do it there is no reason why you shouldn’t … walk up to the shops or something like that, it is acceptable to do that … (Training Manager)
Hence, the founder tolerated or sanctioned rule breaking when she believed it led to better quality care being delivered, improving client wellbeing and satisfaction with the care service and so increasing the competitive advantage of the organization. Care workers therefore interpreted the founder’s approval more broadly, and later used their own judgement when being asked to perform tasks beyond formal guidelines. If management were prepared to sanction – and, indeed, at times authorize – formal rule breaking, then it was alright for them to similarly do so. Some rule breaking (e.g. uniform wearing) would be simply a departure from company rules. Other rule breaking, such as failure to keep logs or purchasing over-the-counter medicines for clients, would depart from sectoral regulatory guidelines. What is evident is that these two types of ‘rule breaking’ went hand in hand, and that one may have paved the way for the other because carers at the frontline do not always readily distinguish between institutional and organizational rules, and owner-sanctioned departures from the latter might make breaches of the former seem more acceptable. Carers constantly had to make judgements as to when and to what extent rules could be broken; both types of rule breaking may, if pushed too far, result in managerial disciplinary action.
Discussion
Drawing on Martin et al. (2013), the process of rule breaking in this study can be further unpacked when one considers the dimensions of hierarchy and contentiousness.
Rule breaking at the level of the organization
At start-up the founder registered the organization with the CQC, and, as a consequence, set in place formal rules and regulations, including both broad principles and formal task-specific procedures and rules. This registration gave the organization the appearance of adhering to institutional rules and regulations, and as a result achieving external legitimacy within the care sector. At the same time, the founder decoupled local behaviours from these externally imposed standardized regulations (Meyer and Rowan, 1977) by allowing frontline staff to adapt behaviours and break rules in order to make operations more effective and efficient. Therefore, right from the start, the owner personally saw departing from a number of external and internal rules as uncontentious, and in some cases, authorized them. In other words, initiating rule breaking was not simply something that came from below. First, by suggesting the transgression of specific company rules, the founder confirmed to carers that the needs of clients, and with this emerging informal ‘social rules’, might take precedence over broader and more prescriptive organization rules and regulations. Second, the founder had a key role in managing the official CQC inspection process (see Meyer and Rowan, 1977), making available selected clients and care workers for interview who would advocate and demonstrate a more formal adherence to institutional rules. This decoupling action allowed the organization to differentiate its service offering and secure an advantage over competitors. As noted above, the founder developed a service which, in her view, addressed many of the shortcomings of other care companies, including continuity of care, time to develop relationships and putting the client’s needs first (see Table 1). Decoupling was thus seen as uncontentious as it allowed the organization to achieve key strategic goals.
Rule breaking at the level of the individual
When considering the care workers, three key processes underpin the increased prevalence of rule-breaking behaviours. First, decoupled from the constraints of more formal institutional rules, care workers acted to find solutions to the often complex daily problems of the clients they served (Burns et al., 2013; Carlsson-Wall et al., 2011; Heaphy, 2013). Faced with these problems, carers interpreted the appropriateness of externally imposed standardized rules and adapted behaviours to suit local conditions through everyday low-key rule breaking. Second, increasing workloads might have further resulted in administrative shortcuts being taken, such as a failure to complete recording tasks (Baines, 2011). The failure to complete medication records might be seen to compromise client wellbeing. However, when visits became increasingly time-constrained, carers choose to focus on the more personal aspects of care. Third, care workers broke rules in order to continue to deliver on the values for care and social justice that they had signed up for when they joined the organization (cf. Barnes, 2012), ‘gifting’ extra services to clients despite formal rules (Baines, 2011; Bolton and Laaser, 2013). After all, many carers left previous employers attracted by the value positioning of the organization in question, as one in which carers had the time to develop relationships with the client. Through a process of self-organization, carers and clients thus worked together to develop locally adapted informal rules to reflect the interests of those concerned (Ackroyd and Thompson, 1999; Burawoy, 1979), which had legitimacy within client–carer relationships that outweighed those of externally imposed regulations.
Rule breaking and informal rules
While the discussion so far has highlighted the dimensions of hierarchy and contentiousness in rule-breaking behaviours (Martin et al., 2013), the emergence of informal rules has a key role to play in this study. Extending Martin et al.’s conceptualization, rule breaking is seen here as a phenomenon which occurs as a result of the tension between competing formal and informal rules, at multiple levels throughout the organizational hierarchy. As Taska (2012) notes, informal rules arise alongside formal rules, and ‘the pressure to break rules is never formal. Rather, it occurs through social norms, group pressures and institutional logics’ (Martin et al., 2013: 569). The breaking of formal rules occurs here when individuals adopt behaviours which are governed by local informal rules, as ‘such norms often demand the violation of formal organizational rules’ (Martin et al., 2013: 571). Conceptualizing rule breaking in terms of both formal and informal rules has implications for Martin et al.’s (2013) dimensions of hierarchy and contentiousness. First, the behaviours of individuals are influenced by competing rules which exist at different hierarchical levels, including both formal institutional/organizational rules and informal group/individual-level ones (Breslin, 2011). For example, when choosing whether to withdraw cash for a client, care workers are faced with two competing sets of rules to follow. On the one hand, they could adhere to the relevant company rule (Org-4 in Table 1), which relates to the CQC guideline for client safety and wellbeing. On the other hand, they could follow an informal rule developed with the client concerned, who believes that the carer will not abuse their trust. The choice of which set of rules to follow depends on the contentiousness of each for the different parties concerned, and the relative power they exert on local behaviours.
Therefore, contentiousness now refers to differing interpretations of, and power struggles around, these competing sets of formal and informal rules. The informal rule of withdrawing cash is not contested by the client as it serves his/her immediate needs. It is also not contested by the carer, who is acting in the client’s best interests, and fulfils personal goals for social justice and fairness (Bolton and Laaser, 2013). As noted above, these behaviours helped differentiate the service offering of the organization, and so were not contested by the founder. It is seen that the changing balance of power also acted to ensure the dominance of local informal rules over time. First, by decoupling local actions from formal rules, the founder acted to increase the importance of the carer–client interaction relative to the external regulatory body. Second, positioning the organization as one which puts the client’s needs first increased the power of the client in the trilateral relationship between employer, worker and customer (Bélanger and Edwards, 2013; Lopez, 2010). Third, by recruiting care workers she believed would prioritize the interests of the client, the founder empowered staff to adapt to the latter’s needs. In summary, the shifting balance of power within the organizational hierarchy allowed informal rules to emerge as dominant, resulting in the breach of competing formal strictures.
More generally, where adopting an informal group-level rule also serves the interests of the wider organization, then breaking the formal organizational rule will not be contested. Thus, different sets of rules can co-exist and be uncontested. However, when the enactment of both is seen to be incompatible, then conflict may occur as informal and formal rules compete in the guidance of behaviours. This results in a struggle for survival at multiple levels, as the advocates of each set of rules use their power to ensure the dominance of one over the other. As Ackroyd and Thompson (1999: 29) note: ‘for at the same time they are adapting, interpreting and challenging those rules, in part because they are orienting their conduct to a conception of informal norms’.
Conclusion
This study not only highlights the extent to which different dimensions of rule breaking may both span and challenge existing hierarchies of authority and regulation both within and beyond the organization, but also the extent to which the boundaries of what is contentious behaviour is fluid, and, at times, difficult to define (cf. Martin et al., 2013). The rule breaking seen in this case did not constitute irresponsible autonomy (Ackroyd and Thompson, 1999), but instead efforts to define autonomy on social and professional grounds, rather than in terms of formal organizational demarcations. At the same time, operators of outsourced public services are often reliant on a low wage, highly precarious (and, in many instances, including the firm under review, non-unionized) workforce and an intensification of labour time to make money (Baines, 2011: 143). Workers may engage in such rule-breaking activities to claw back an ethos of professionalism and a sense of worth in the jobs they perform; as the literature on moral economy alerts us, work and employment encompasses a dense range of ties and moral relations (Bolton and Laaser, 2013).
The role of the founder in this process should not be viewed uncritically, surviving and making a success of the business in a highly competitive market, but, through countenan-cing rule breaking as a way to achieve this, running the risk of an existential crisis should there be a serious complaint or breach of duty of care. Driven by growth and profit, she increased workloads, making it more difficult for carers to deliver the required level of service. However, having developed the space and community which fit their notions of fairness and justice, informal rules increasingly guided behaviours. The study thus adds to the view of rule breaking along the dimensions of hierarchy and contentiousness (Martin et al., 2013), by highlighting the key role played by these emerging informal norms.
Footnotes
Acknowledgements
The authors are indebted to the invaluable comments of Dr Diane Burns, Dr Rob Wapshott, three anonymous referees and the editors, Prof Ian Kirkpatrick and Prof Melanie Simms.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.