
Abstract
Introduction
The normal level of methemoglobin is 1.0–1.5%. 1 Methemoglobinemia is diagnosed when levels rise above 5%; symptoms develop typically at levels >10–20% of total hemoglobin, and levels >30–40% are considered life-threatening. The first neurological signs (headache and dizziness) also appear after 30% MetHb. More pronounced neurological signs, such as epileptic seizures or coma, appear after 50% MetHb. 2
The cases of methemoglobinemia described in the literature are associated with the use of drugs such as rasburicase, 3 local anesthetics such as benzocaine,4,5 lidocaine + prilocaine, 6 with the use of drugs for the treatment of malaria-primaquine and tafenoquine, 7 dapsone, phenazopyridine, amyl nitrite, 1 and many others.
Acquired methemoglobinemia can be caused by exposure to direct oxidants (e.g., benzocaine and prilocaine), indirect oxidation (e.g., nitrates), or metabolic activation (e.g., aniline and dapsone). 8
A single center review of nearly 30,000 transesophageal echocardiograms found the incidence of methemoglobinemia to be 0.067%. 4 A systematic review of cases of local anesthetic-related methemoglobinemia found that benzocaine was an agent in two-thirds of cases. 9
The clinical manifestations of methemoglobinemia depend on the concentration of methemoglobin in the blood.
As the percentage of methemoglobinemia approaches 20%, the patient may experience anxiety, light-headedness, and headaches. At methemoglobin levels of 30–50%, there may be tachypnea, confusion, and loss of consciousness. Approaching 50%, the patient is at risk for seizures, dysrhythmias, metabolic acidosis, and coma. Levels above 70% are often fatal. 10
Clinical cases related to the use of medications in children describing the development of methemoglobinemia are limited to describing the reaction to a single drug. The relevance of the description lies in the fact that in this article we describe the case of methemoglobinemia in a child with polypragmasia, that is, when using five or more drugs at the same time. As far as we know, this is the first documented case of methemoglobinemia in a child with comorbidity and polypragmasia.
Case presentation
A 4-year-old boy from the kidney transplantation department was admitted to the Pediatric Intensive Care Unit (PICU) in serious condition with acute respiratory failure, which developed suddenly. At 11 a.m., the child turned pale and became restless, followed by acrocyanosis, tachypnea of up to 32 respiratory movements per minute, and nausea. The main diagnosis for the patient’s stay in the hospital was the kidney transplant rejection. The condition after allogeneic kidney transplantation (the operation was performed 6 months ago).
It is known from the medical history that on the eve of 2 consecutive days, 2 days before admission to the intensive care unit, the patient used 1 suppository of benzocaine overnight into the rectum for pain associated with external hemorrhoids, and on the day of deterioration due to severe pain in the area of the urinary catheter, lidocaine was used topically + chlorhexidine. The urinary catheter was installed after surgery—ureterocystoneostomy 2 days before admission to the PICU.
On examination, the child is conscious, acrocyanosis is noted, tachypnea up to 32 per minute, and tachycardia. The 4-year-old patient presented in critical condition with severe hypoxemia (SpO2 78%) and metabolic acidosis (lactate 3.3 mmol/L). Breathing through the nose is not difficult, auscultation—vesicular, evenly carried out in all departments, and wheezing is not heard. The heart tones are loud and rhythmic. The pulse in the peripheral vessels is satisfactory. The heart rate is 140 beats/min. Blood pressure is 100/50 mmHg. The abdomen is not swollen, soft, and painless on palpation. The size of the liver and spleen are not enlarged. The patient has no history of allergic reactions to medications.
He received treatment: mycophenolic acid 90 mg 2 times a day, prednisone 2.5 mg 1 time a day, tacrolimus 9.5 mg 1 time a day for the prevention of kidney transplant rejection, co-trimoxazole 120 mg per day 3 times a week for the prevention of pneumocystis pneumonia (for the last 6 months); levothyroxine sodium was given 75 mg per day for hypothyroidism, valganciclovir 450 mg every other day for the prevention of viral infection, folic acid 1 mg once a day, epoetin alfa 1000Ed 3 times a week for secondary anemia, and esomeprazole 10 mg once a day for the prevention of drug ulcers.
The patient was in the hospital in the kidney transplantation department with the main diagnosis: kidney transplant rejection. The condition was found after allogeneic kidney transplantation (6 months ago). Concomitant diseases: obstructive uropathy and reflux uropathy, unspecified urinary stones, anemia, secondary hyperparathyroidism, hypothyroidism, and external hemorrhoids. Background disease: congenital nephrotic syndrome of the Finnish type. He underwent a ureterocystoneostomy 2 days before admission to the PICU.
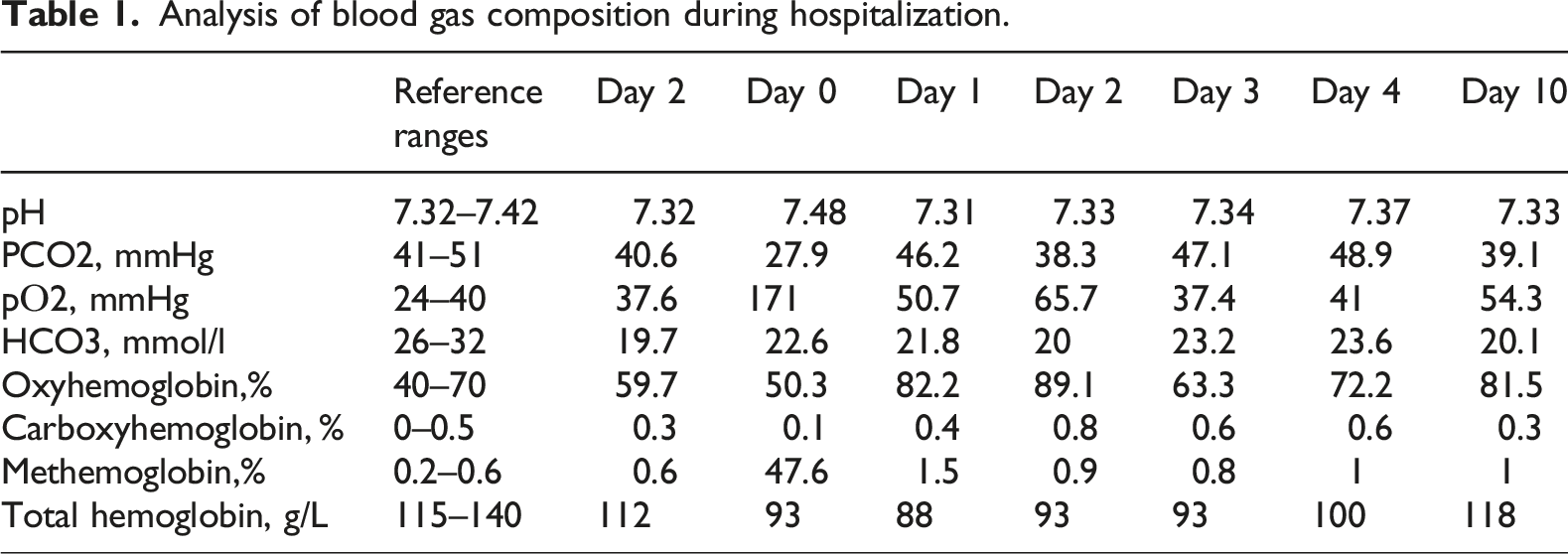
Analysis of blood gas composition during hospitalization.
On the 5th day, the results of chemical and toxicological examination of urine, conducted by methods of immune chemical analysis, enzyme immunoassay, high-performance liquid chromatography tandem with mass spectrometry, and gas chromatography with mass spectrometry, became known. The following substances/agents were detected: tramadol, drotaverine, etaverine (also known as ethaverine), lidocaine, benzocaine, trimethoprim, and ondansetron. In the analysis, three drugs used by the patient had a potential threat in the development of methemoglobinemia: lidocaine, benzocaine, and co-trimoxazole (sulfamethoxazole with trimethoprim).
An adverse drugs reaction to the benzocaine, lidocaine combined with chlorhexidine, and co-trimoxazole (sulfamethoxazole plus trimethoprim) was documented and electronically reported to the Pharmacovigilance service. The association between methemoglobinemia and drug administration was evaluated using the Naranjo Scale and amounted to 5 points for benzocaine (probable association), 4 points for lidocaine with chlorhexidine (possible association), and 2 points for co-trimoxazole (possible association).
Discussion
Benzocaine is relatively safe and has a low risk when applied topically. However, one of the more life-threatening side effects is methemoglobinemia, which occurs due to the ability of benzocaine to be metabolized into nitrobenzene, which reduces the oxygen-binding ability of hemoglobin by oxidizing iron (Fe2 + to Fe3+). Benzocaine is characterized by minimal systemic absorption when administered subcutaneously and orally. It is metabolized in the liver and blood plasma by esterases to paraaminobenzoic acid (PABA) and ethyl alcohol, which are excreted by the kidneys. In renal failure, the excretion of PABA slows down, which potentially increases the risk of accumulation of metabolites and toxic effects, including methemoglobinemia. The combined use of benzocaine with other oxidizing agents (lidocaine, co-trimoxazole) increases the risk of methemoglobinemia. Benzocaine and lidocaine are aniline derivatives that mediate the oxidation of hemoglobin.
According to the general characteristics of the drug, benzocaine is indicated for use in children over the age of 12 and adults. The dose of benzocaine contained in 1 suppository is 206 mg. The child’s weight is 14.9 kg. The drug was used without the consent of the child’s legal representative with the attending physician. Thus, the daily dose of benzocaine was 13.8 mg/kg. In a retrospective analysis of cases of benzocaine poisoning in children, the oral dose of benzocaine was 86.8 (+/− 89.5) mg/kg and 50 mg/kg, the average and median, respectively, 11 which is much higher than the dose that was used in the described case. Co-trimoxazole (sulfamethoxazole + trimethoprim) enhances the effect of benzocaine, as sulfonamides compete with PABA for metabolism, increasing the concentration of oxidizing agents.
The dose of lidocaine applied topically to the urethra did not exceed 2 g (the dose contained in 1 syringe). The recommended maximum total dose of lidocaine for applicative anesthesia for a 4-year-old child weighing 14.9 kg is 20 g. 12
In the described clinical case, in a child with kidney transplant death and rejection, the level of methemoglobin reached 47.6% against the background of a combination of three drugs with a potential threat of developing methemoglobinemia, demonstrating the development of synergy.
However, the difficulty in identifying the etiological factor in the case of methemoglobinemia arose because rectal suppositories containing benzocaine had a trade name very similar to that of rectal suppositories containing phenylephrine.
Alternative methods of pain relief in patients with renal insufficiency include the use of non-safe analgesics: paracetamol (in reduced doses), gabapentin (with dose adjustment), 13 the use of local anesthetics without oxidative potential (ropivacaine and bupivacaine), and non-medicinal methods (physiotherapy and cognitive behavioral therapy).
Clinical case reports of methemoglobinemia in children associated with lidocaine use, based on PubMed data from 2020 to 2025, are limited. One reported case involved a 15-month-old female who experienced generalized seizures and respiratory failure. 14 This case resulted from the unintentional use of a lidocaine-prilocaine cream, although the exact method of drug administration was not specified. Treatment included intravenous administration of 20 mg methylene blue. While uncommon, severe toxicity resulting in CNS depression or seizures may require endotracheal intubation. In the described case, the child required intubation, but after 8 h, she was extubated. 14
Description of our clinical case has several limitations.
The patient did not undergo tests to exclude hereditary methemoglobinemia, including assessments for glucose-6-phosphate dehydrogenase deficiency, NADH-cytochrome b5 reductase deficiency, and genetic analysis of mutations in the CYB5R3 gene.
The use of benzocaine in a 4-year-old child was off-label (the drug has been approved for use since the age of 12).
Another limitation of this case is that the chemical and toxicological examination of the urine was conducted only after the child received emergency care in the intensive care unit. Consequently, drugs used in symptomatic therapy—tramadol, drotaverine, and ondansetron—were detected in the urine.
The progression of diagnosed drug-induced methemoglobinemia is usually benign. However, an unfavorable outcome is possible in severe cases of toxic methemoglobinemia characterized by a high concentration of methemoglobin in red blood cells.
The diagnosis of drug-induced methemoglobinemia depends on a thorough and accurately collected medical history. Therefore, the patient or their representative should report all medications used, specifying the international nonproprietary name rather than just the trade name. This information should be documented in the local hospital records where the case occurred.
Conclusion
Polypragmasia in patients with comorbidity increases the risk of methemoglobinemia, even when using drugs with moderate oxidative potential.
The use of benzocaine in rectal form, particularly in patients with impaired renal function and anemia, requires caution and close monitoring. If cyanosis or hypoxia develops in patients receiving multiple drugs from the oxidant group (such as local anesthetics and sulfonamides), it is essential to monitor methemoglobin levels.
Registration of undesirable side effects is critically important for the detection of rare complications of polypragmasia.
Footnotes
Acknowledgments
We sincerely thank all healthcare workers who contributed to this patient’s management and helped us publish the case report.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
The patient’s legal representative wrote consent for permission to publish this case.
Author contributions
Alina B. Strok and Maria N. Kostyleva: concept and methodology development, manuscript writing, and visualization. Maria N. Kostyleva: management, manuscript review and editing, and participated in the management of patients. Anna V. Kostina: manuscript writing and editing and participated in the management of patients.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.