
Abstract
The article provides the first comprehensive assessment of age-based triage from the perspective of human rights. Triage, that is the sorting of patients into categories of priority of treatment, has been known for decades. It has however got larger prominence during the Covid-19 crisis. The crisis has exposed healthcare systems in many countries to a critical shortage of resources, forcing them to consider resorting to triage. The absence of legal rules has been compensated by non-binding triage guidelines, adopted by professional medical and ethical associations. This article analyses 11 guidelines, showing that none of them is truly age neutral. Some use allocation criteria that entail disparate treatment of older persons, consisting of their de-prioritization or exclusion from access to life-saving treatment on account of their age. Others rely on allocation criteria whose application has disparate effects on older persons. The article argues that whereas the latter approach could be compatible with human rights standards, the former entails violations of the principle of non-discrimination and of several other human rights (the right to life, the prohibition of inhuman and degrading treatment, the right to private life, and the right to health).
INTRODUCTION
Should age play a role in deciding who will get access to life-saving treatment? Should some persons be denied this access because they are ‘too old’? These questions might seem cynical, misplaced, and unworthy of any serious discussion. And yet, in the past three years, they have been repeatedly raised due to the scarcity of resources that several national health systems have been confronted with during the Covid-19 crisis. Media and non-governmental organisations have reported instances in which these questions have been answered in the affirmative, and when persons over a certain age have been excluded from access to life-saving devices. 1 Moreover, some of the Covid-19 triage guidelines issued by professional medical and ethical associations in various countries since spring 2020 recommend using age as a triage factor. These developments, and the age-based triage as such, have given rise to rich debates among medical researchers, (bio)ethical experts, and moral philosophers. They have stirred less interest among human rights scholars.
This article seeks to fill this gap by providing a human rights analysis of age-based triage. The analysis unfolds in two steps. Section 2 explains the concept of triage and introduces the main allocation criteria used in triage. It also analyses 11 triage guidelines adopted since the outbreak of the Covid-19 crisis in 8 European and 3(4) 2 non-European countries. These guidelines rely on different allocation criteria and, as such, take different approaches to the factor of age. Three main models can be distinguished, none of which is fully age neutral. Section 3 discusses the compatibility of these three models with human rights standards, that is the principle of non-discrimination and several other human rights. The article argues that whereas triage based on criteria whose application has disparate effects on older persons may be compatible with such standards, triage foreseeing disparate treatment of older persons violates them. Age should thus never be one of the factors on which triage decisions are based. Section 4 concludes.
AGE-BASED TRIAGE IN HEALTH CARE
The concept of triage, that is the sorting of patients to determine the priority of their treatment, has been known and applied in the provision of health care for decades. Triage decisions are based on various allocation criteria, which are usually not age neutral (Section 2.1). Since spring 2020, professional medical and ethical associations in many countries have issued special Covid-19 triage guidelines. The analysis of 11 such guidelines adopted in 8 European and 3(4) non-European countries shows that although they rely on different allocation criteria, all three models that can be distinguished foresee age-based triage (Section 2.2).
Triage in Health Care
In the most general sense, triage denotes prioritisation carried out in any area of activities. The European Court of Human Rights (ECtHR), for instance, uses the term when referring to triage of cases in court proceedings, 3 triage of communications to determine their intelligence value, 4 or triage of detained illegal migrants. 5 More commonly, however, the term is reserved for health care contexts, where it refers to the process of sorting individuals in need of medical intervention in order to determine priority of care. The Cambridge Dictionary defines triage as ‘the process of quickly examining patients who are taken to a hospital in order to decide which ones […] must be treated first’. 6 The process distinguishes those who will be treated first from those who will be treated later (de-prioritisation) or who will not be treated at all (exclusion). Triage typically takes place prior to treatment – this is the ex ante triage. Sometimes, the original decision is later reassessed and revised – this is the ex post triage.
The concept of medical triage originated in military medicine.
7
It was introduced to help solve the dilemma of military medical staff who had limited resources but had to take care of many wounded or sick soldiers. The concept was later transferred to civilian medicine and applied mainly in emergency situations such as natural or manmade disasters (plane crashes, earthquakes, fires) or epidemics. The origins of the concept may give rise to the impression that triage only takes place in abnormal times when standard health care services are suspended. This is not the case. Triage is part of the everyday routine at medical institutions. After all, virtually all resources needed in health care, including financial and human resources, are limited. Thus, that ‘each decision taken for one patient may affect the decision-making for other patients’
8
is true at all times. Yet, making triage decisions becomes particularly painful in cases where vital and at the same time scarce resources are at stake, and where treatment delayed often means treatment denied. The shortage of resources may result from the scarce nature of the resource (transplants) or from special circumstances (war, disasters, epidemics). This article focuses on the latter situation. Triage is therefore defined here as A form of rationing or allocation of scarce resources under critical or emergency circumstances where decisions about who should receive treatment must be made immediately because more individuals have life-threatening conditions than can be treated at once.
9
Triage has been extensively discussed by experts in medical ethics. Medical ethics, which has accompanied the development of medicine since the ancient times, centres around four main principles: the principles of beneficence (do the most good possible for the patient), maleficence (do no harm to the patient), autonomy (respect the patient's right to decide about their life), and justice (be fair to patients). 10 It is largely accepted that when confronted with a critical shortage of resources, medical staff may apply these principles in a somewhat different way. The aim then is to use all available resources in the best way to save the biggest number of lives possible (doing the greatest good for the greatest number of people). What, however, the best way is, whether it is linked to efficiency or fairness, and how it shall be determined remains disputed. Different allocation criteria have been proposed to help answer these questions. These criteria determine the order in which individuals get access to scarce resources. They also single out those who are excluded from such access.
The criteria often rely on medical considerations, such as the need of treatment and the likelihood to benefit from treatment. Under these considerations, the health status of patients and their medical prognosis play a crucial role. In the first case (need of treatment), preference is given to those who are, from a medical perspective, worse off – at the expense of those who are better off. In the latter case (likelihood to benefit), preference is given to those who have the highest chance to benefit from treatment – at the expense of those who are better off and can survive without treatment or who are worse off but unlikely to benefit from treatment. The benefit goes beyond a mere capacity not to die during treatment. It tends to be defined in terms of short-term or even long-term survival. 11 Sometimes, the post-treatment quality of life is taken into account as well. 12 The chance of survival and the quality of life are determined through various measurement tools, for example the Clinical Frailty Scale (CFS) which uses a nine-point scale to evaluate the overall fitness or frailty of a person, 13 or the Quality-Adjusted-Life-Years scheme (QALY) which serves to estimate the years of life remaining for a patient, weighting each year with a quality-of-life score. 14 The reliability of these tools continues to be debated. 15
Allocation criteria may be based on other than medical considerations as well. Some rely on economic factors, such as the number of resources needed to treat individual patients, the contribution that the patient has made or is expected to make to the health system, or the number of life-years saved by treatment (life expectancy). Other criteria take into account social factors. This category may favour different persons, including those performing vital functions in society, those having special social merits, or those in a disadvantaged position. Those performing vital functions are typically health care workers, first responders, water suppliers, or fire fighters. 16 Special social merits may consist in any feature that concrete societies consider valuable, for example one's race, gender, age, wealth, or social status. While some of these criteria would not be found acceptable in modern times, others – including age – may still be relevant. Similarly, giving preference to persons in a disadvantaged position may favour different persons in different societies, though some groups (such as poor people or people with disabilities) are among obvious candidates.
Allocation may also be based on normative considerations, that is on different conceptions of justice. One of these conceptions stresses the equal value and dignity of all individuals and prohibits discrimination based on personal characteristics, including age. Another conception relies on the life cycle principle, also known as the principle of intergenerational equity. 17 Under this principle, all individuals deserve to be given equal opportunity to live through the various stages of life. Finally, allocation may also be carried out based on random selection. The first-come first-served principle, under which individuals are dealt with in the order they arrive to a medical institution, falls into this category.
In standard situations, individuals get access to health care based on a combination of the first-come first-served principle and the need for treatment. In emergency situations, however, these criteria fail to produce optimal outcomes. The first-come first-served principle unfairly favours those who get sick first, have knowledge and resources to seek early assistance, or live in an area close to hospitals. Giving priority to persons most in need of treatment may result in medical care being provided to those with limited prospects of survival but effectively denied to those with better prospects who will simply not live long enough to wait their turn. In this situation, other allocation criteria need to be opted for.
Most of the allocation criteria are not age neutral. Some take age into account directly, envisaging disparate treatment of older persons. This is typically so with the criteria based on life expectancy and on the life cycle principle, which both prioritise younger persons over older ones. The former does it out of economic considerations – if only one of two persons may get access to treatment, it is seen as rational to save the one who has more years to live. The latter builds on normative considerations – all individuals should have the same opportunity to live through the various phases of life and hence, those who have so far had less opportunity to do so should get priority. 18 The application of those criteria may result in de-prioritisation of older persons so that they get access to scarce resources but only once the needs of younger persons are met. It may also result in the exclusion of older persons from access to such resources when those over a certain age threshold are simply denied treatment. 19
Other allocation criteria do not include age explicitly. Most of them, however, are not age neutral either. They tend to rely on factors that older persons exhibit in a different degree than younger persons and consequently, their application has different effects on persons belonging to different age groups. This is so with criteria based on the likelihood to benefit from treatment (especially if measured through the long-term survival or the post-treatment quality of life), the number of resources needed for treatment, and the expected contribution to the health system. Some criteria, mainly those relying on social and normative factors, may cut both ways depending on the social status that older persons have in a particular society. For instance, the social merit criterion would benefit older persons in societies where they are treated with enhanced respect but disadvantage them where they are treated as the most dispensable. 20
Not all allocation criteria thus work to the disfavour of older persons. Yet, many of them do. Medical and ethical aspects of this approach have been discussed for years. 21 The discussion has become particularly lively since the outbreak of the Covid-19 crisis. 22 The crisis has put medical institutions in many countries under unprecedented strain and has triggered the adoption of a large number of triage guidelines. The next subsection discusses these guidelines, focusing more specifically on the role that they assign to the factor of age.
Covid-19 Triage Guidelines and Age- Based Triage
The first human cases of Covid-19 were reported in China in early November 2019 and the virus quickly spread all across the globe. On 11 March 2020, the World Health Organization (WHO) declared a worldwide pandemic and called upon States to take radical measures to counter the spread of the virus. By January 2023, over 660,000,000 individuals have tested positive for Covid-19 and more than 6,700,000 have died of/with the virus. The rapid spread of Covid-19 together with the severe symptoms that many patients exhibited led to the overloading of the health care systems in the most seriously hit countries, which started to suffer from a critical shortage of places in Intensive Care Units (ICU), ventilators, and other life-saving medical devices. Reports indicating that medical staff resorted to age-based triage and that persons over a certain age were excluded from access to the ICU or to ventilators began to appear in the media and on NGOs’ websites from the early days of the pandemic. 23 To forestall or pre-empt such instances of ‘wild triage’, professional medical and ethical associations in countries all over the world started to issue special Covid-19 triage guidelines.
Such guidelines are usually neither official nor legally binding. 24 Yet, they tend to be considered an authoritative interpretation of the legal rules which require medical institutions and staff to provide health care services at the appropriate professional level (de lege artis) and in compliance with the relevant medical and ethical standards, 25 both in times of normalcy and in emergency situations. The failure to abide by this requirement may result in administrative and criminal sanctions. Since the relevant medical and ethical standards are rarely specified in legislation, non-official guidelines come to aid to help overcome uncertainty.
The relevance of such guidelines can be illustrated by the decisions rendered by the High Court of New Zealand. In 1993, in Auckland Area Health Board v Attorney-General, this Court was asked to consider whether a removal of ventilatory life support from a patient with severe health problems would be lawful. The Court answered this question in the affirmative, relying on the standard of ‘good medical practice’. The standard was to be defined taking into account, inter alia, views of peer-professionals and the medical profession's recognised ethical bodies. 26 In 1998, in Shortland v Northland Health Ltd., the Court expressly confirmed that guidelines adopted by professional associations should be considered in this context, noting that ‘the value of the guidelines […] is that they assist doctors to allocate scarce resources in a principled fashion […] A properly made clinical decision which includes […] considerations of resource allocation constitutes lawful grounds to decline treatment.’ 27 Following their national counterparts, international human rights bodies have also shown readiness to take guidelines issued by professional associations into account when considering whether the State has complied with its obligations under human rights treaties. 28 Thus, while non-binding, the guidelines are not deprived of legal relevance. 29
Triage guidelines started to be adopted years before the Covid-19 crisis. Some responded to a concrete emergency situation, such as the epidemics of SARS (2002–2004), avian flu (2005–2007), or Ebola (2013–2016). Others sought to introduce more general standards within individual medical institutions or at the national or regional level. 30 All these previous initiatives remained limited to certain countries and contexts. The situation changed with the outbreak of the Covid-19 pandemic. Due to its global scale, the pandemic has provoked the adoption of the largest ever set of triage guidelines which come from different countries but apply in the same context. This makes the analysis and comparison of these guidelines very interesting.
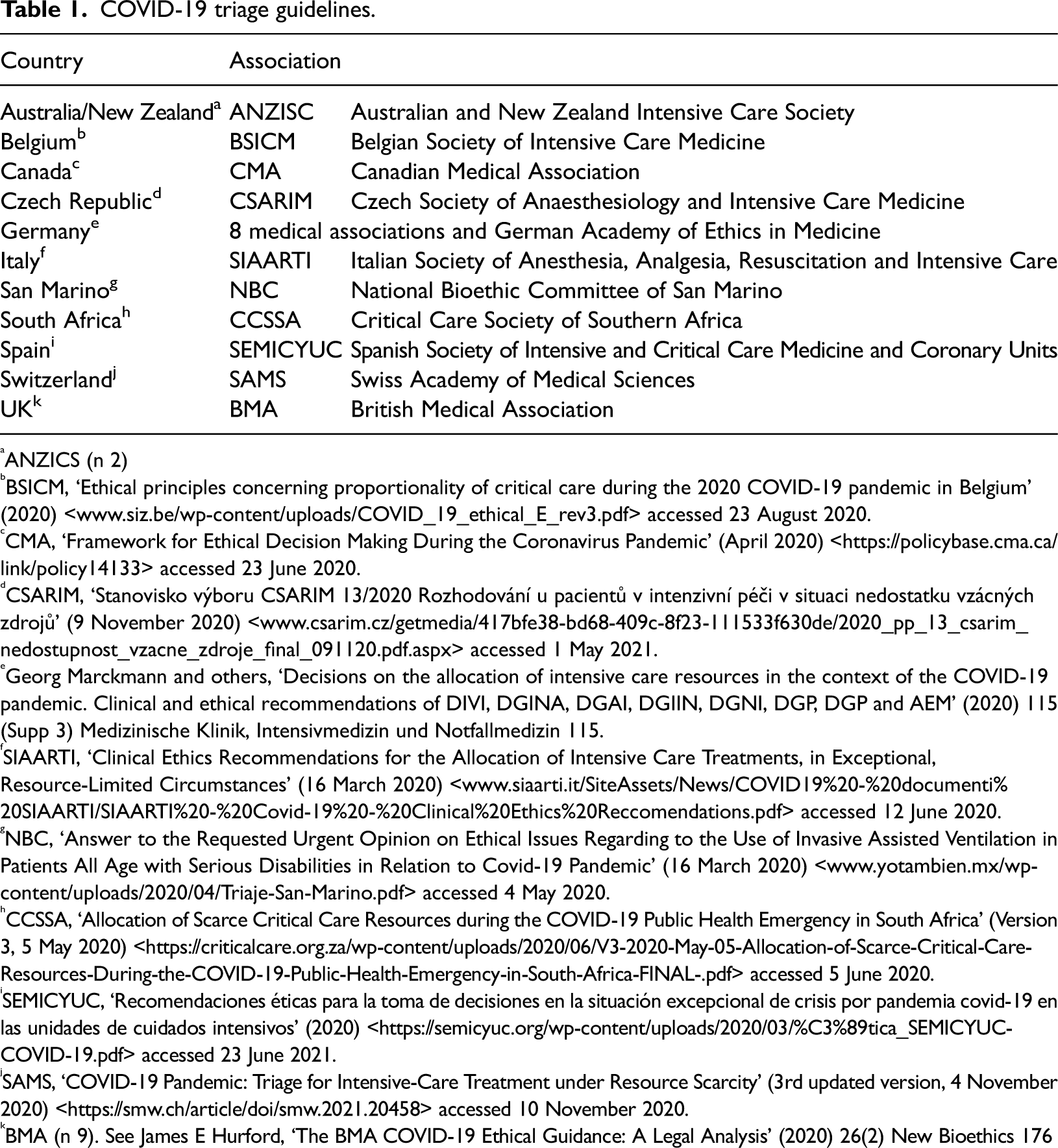
This article focuses on 11 Covid-19 triage guidelines adopted by medical and ethical associations in 8 European and 3(4) non-European countries. All the selected countries are well-established democracies which put emphasis on the protection of human rights and consider these rights justiciable. All the countries moreover are State Parties to the main universal and, in most cases, regional human rights instruments. Due to these similarities, it could be expected that triage guidelines adopted in the selected countries would embrace a largely similar approach towards age-based triage. It could also be expected that such an approach would be in line with the applicable human rights standards. These expectations however are not truly met. There are important differences among triage guidelines, even among those adopted in countries that are bound by the same human rights instruments (for example the European Convention on Human Rights (ECHR)). Such differences confirm that age-based triage is a controversial issue that warrants a more detailed discussion among human rights experts. Table 1 provides a list of the guidelines discussed in this article.
COVID-19 triage guidelines.
COVID-19 triage guidelines.
ANZICS (n 2)
BSICM, ‘Ethical principles concerning proportionality of critical care during the 2020 COVID-19 pandemic in Belgium’ (2020) <www.siz.be/wp-content/uploads/COVID_19_ethical_E_rev3.pdf> accessed 23 August 2020.
CMA, ‘Framework for Ethical Decision Making During the Coronavirus Pandemic’ (April 2020) <https://policybase.cma.ca/link/policy14133> accessed 23 June 2020.
CSARIM, ‘Stanovisko výboru CSARIM 13/2020 Rozhodování u pacientů v intenzivní péči v situaci nedostatku vzácných zdrojů’ (9 November 2020) <www.csarim.cz/getmedia/417bfe38-bd68-409c-8f23-111533f630de/2020_pp_13_csarim_nedostupnost_vzacne_zdroje_final_091120.pdf.aspx> accessed 1 May 2021.
Georg Marckmann and others, ‘Decisions on the allocation of intensive care resources in the context of the COVID-19 pandemic. Clinical and ethical recommendations of DIVI, DGINA, DGAI, DGIIN, DGNI, DGP, DGP and AEM’ (2020) 115 (Supp 3) Medizinische Klinik, Intensivmedizin und Notfallmedizin 115.
SIAARTI, ‘Clinical Ethics Recommendations for the Allocation of Intensive Care Treatments, in Exceptional, Resource-Limited Circumstances’ (16 March 2020) <www.siaarti.it/SiteAssets/News/COVID19%20-%20documenti%20SIAARTI/SIAARTI%20-%20Covid-19%20-%20Clinical%20Ethics%20Reccomendations.pdf> accessed 12 June 2020.
NBC, ‘Answer to the Requested Urgent Opinion on Ethical Issues Regarding to the Use of Invasive Assisted Ventilation in Patients All Age with Serious Disabilities in Relation to Covid-19 Pandemic’ (16 March 2020) <www.yotambien.mx/wp-content/uploads/2020/04/Triaje-San-Marino.pdf> accessed 4 May 2020.
CCSSA, ‘Allocation of Scarce Critical Care Resources during the COVID-19 Public Health Emergency in South Africa’ (Version 3, 5 May 2020) <https://criticalcare.org.za/wp-content/uploads/2020/06/V3-2020-May-05-Allocation-of-Scarce-Critical-Care-Resources-During-the-COVID-19-Public-Health-Emergency-in-South-Africa-FINAL-.pdf> accessed 5 June 2020.
SEMICYUC, ‘Recomendaciones éticas para la toma de decisiones en la situación excepcional de crisis por pandemia covid-19 en las unidades de cuidados intensivos’ (2020) <https://semicyuc.org/wp-content/uploads/2020/03/%C3%89tica_SEMICYUC-COVID-19.pdf> accessed 23 June 2021.
SAMS, ‘COVID-19 Pandemic: Triage for Intensive-Care Treatment under Resource Scarcity’ (3rd updated version, 4 November 2020) <https://smw.ch/article/doi/smw.2021.20458> accessed 10 November 2020.
BMA (n 9). See James E Hurford, ‘The BMA COVID-19 Ethical Guidance: A Legal Analysis’ (2020) 26(2) New Bioethics 176
Covid-19 triage guidelines usually combine substantive rules, which stem from one or more allocation criteria identified above, and procedural rules dealing with the authority competent to make individual triage decisions and with the procedure to be followed in this context. The latter rules typically place emphasis on the transparent and inclusive nature of the decision-making process, the involvement of an interprofessional team, and the possibility to review triage decisions ex post based on detailed reports. Virtually all the guidelines stress the exceptional nature of triage, which should only be resorted to in extreme situations, when there is ‘an imbalance between the real clinical needs of the population and the effective availability of intensive resources’ 31 and when alternative means (additional funding, relocation of patients, and so on) have been exhausted or are unavailable. The guidelines also concur that those who are denied access to life-sustaining treatment must be provided with palliative care. 32
Concerning the substantive rules, most guidelines recommend using the likelihood to benefit from treatment as the main allocation criterion. For instance, SAMS indicates that ‘if ICU capacity is exhausted and not all patients who require intensive care can be admitted, the short-term prognosis is decisive for purposes of triage’. 33 BMA notes that ‘ethically, triage requires identification of clinically relevant facts about individual patients and their likelihood of benefiting from available resources’. 34 CSARIM also suggests that ‘the allocation of scarce resources […] can only be based on the criterion of medical needs, resp. expected clinical outcome’. 35 A similar approach is embraced by virtually all the other guidelines. The allocation criteria based on medical considerations are thus the preferred ones. As we saw above, however, the likelihood to benefit may be defined by various factors.
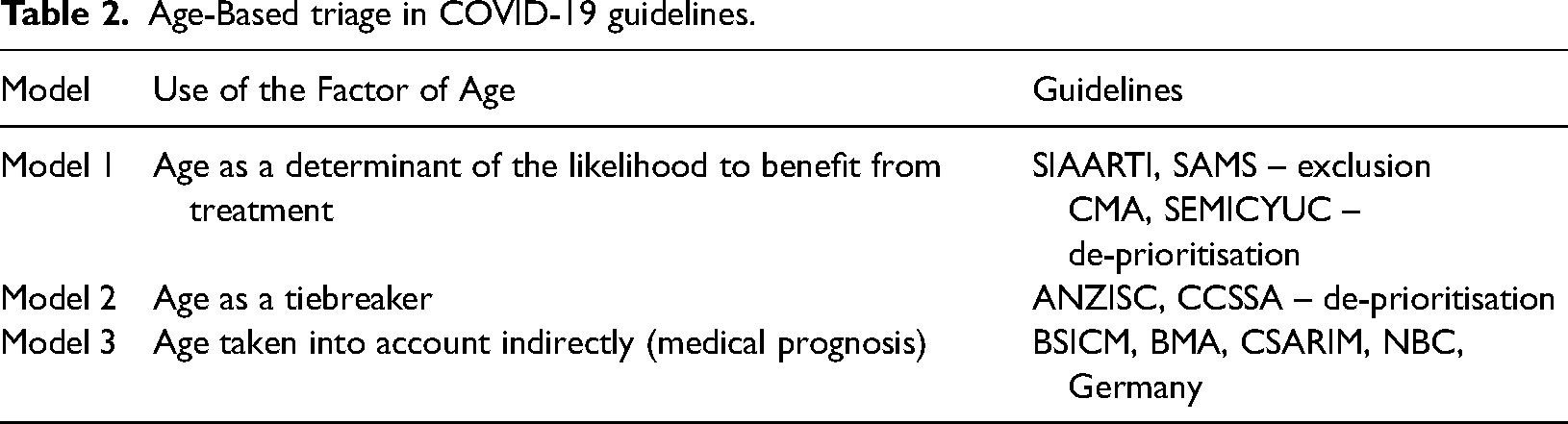
Some of the guidelines consider that such factors shall include older age (Model 1). This is so in the SIAARTI guidelines, which note that ‘an age limit for the admission to the ICU may ultimately need to be set’. 36 The exclusion of persons over this age limit shall make it possible to save scarce resources for ‘those who have a much greater probability of survival and life expectancy’. 37 Age is thus considered an independent variable that in itself determines the likelihood to benefit from treatment and life expectancy. Although no age limit has been set officially, ‘empirical reports from clinicians on the Italian front line suggest that in practice this age limit is currently being set somewhere between 60 and 65’. 38
A similar model is used in the guidelines issued in Canada, Spain, and Switzerland. The first two guidelines consider age as an independent factor determining the likelihood to benefit and the post-treatment life expectancy. 39 However, since they recommend using age for de-prioritisation, not exclusion, no age limits are set, and younger patients always get prioritised. The SAMS guidelines, conversely, include age among the exclusion criteria and introduce specific age limits (85, 75, and 65 years). Yet, age does not operate as an independent variable here but must be combined with certain medical factors. 40 Two other guidelines, those issued in Belgium and the UK, note that age can be used for triage decisions when ‘integrated with other clinical parameters’ 41 or when ‘clinically relevant’. 42 No further details are provided.
The other guidelines recommend determining the likelihood to benefit from treatment by medical factors. They, however, often combine this criterion with additional factors. These come in as tiebreakers when the main criterion fails to produce adequate results, that is when after its application there are still too many persons left in need of life-sustaining treatment. In addition to priority accorded to those performing vital functions, age-related factors feature among these tiebreakers (Model 2). This is so in the guidelines issued by ANZISC and CCSSA, which both envisage de-prioritisation of older persons. The former guidelines suggest that ‘if a situation arises where patients are similarly ranked in terms of clinical priority’, it might be legitimate ‘advocating that younger patients who have lived through fewer life stages are prioritised over older patients’. 43 The latter guidelines distinguish three groups depending on medical factors but note that if there are ties within the same group, other factors may be considered, such as ‘life-cycle considerations with priority going to younger patients, who have had less opportunity to live through life's stages’. 44 Four age groups are distinguished: age 12–40, age 41–60, age 61–75, and older than 75; priority should be given in this order. The two guidelines both promote de-prioritisation of older persons based on the life cycle principle.
The remaining guidelines explicitly reject age as a determining factor at any stage of triage (Model 3). The German guidelines indicate that ‘according to the principle of equality, prioritisations […] are not permitted on the basis of calendar age’. 45 CSARIM notes that ‘any discrimination based on criteria not directly related with the expected clinical outcome of care (especially […] age only) is inadmissible’. 46 NBC adds that triage based on criteria such as age is ‘ethically unacceptable, as it would implement a ranking of lives only apparently more or less worthy of being lived, constituting an unacceptable violation of human rights’. 47 Even the guidelines issued in Belgium and the UK, although they make it possible to use age when clinically relevant, stress that ‘age in isolation cannot be used for triage decision’ 48 and ‘a simple “cut-off” policy with regard to age […] would be unlawful’. 49 These guidelines all recommend using the likelihood to benefit as the main criterion. Concerning tie situations, some guidelines remain silent on them (Germany, NBC, BMA), while others recommend using the first-come first-served principle or randomness (BSICM, CSARIM). The rejection of age as a triage criterion mostly relies on the equal value principle as an ethical imperative and its legal counterpart, the principle of non-discrimination.
Some of the guidelines admit that even when age is not included among the triage factors directly, that is when no disparate treatment of older persons is foreseen, it plays a role in triage indirectly since the application of the main allocation criterion (the likelihood to benefit) has disparate effects on older persons. SAMS notes that ‘age is […] indirectly taken into account under the main criterion “short-term prognosis”, since older people more frequently suffer from comorbidity’. 50 BMA, in a similar way, indicates that ‘some of the most unwell patients may be denied access to treatment […] This will inevitably be indirectly discriminatory against […] the elderly’. 51 Thus, although triage based on the medical prognosis seems age neutral, older persons have a higher chance to score worse under it.
The overview of the Covid-19 triage guidelines shows that none of the guidelines are truly age neutral. Some use the factor of age directly, treating it either as part of the primary allocation criterion (Model 1), or as a tiebreaker (Model 2). These two models foresee disparate treatment of older persons, that is their de-prioritisation or exclusion from access to life-saving treatment. The other guidelines rely on criteria that seem age neutral but whose application has disparate effects on older persons (Model 3). Before we turn to the analysis of the guidelines from the human rights perspective, it may be useful to sum up the three models under which the triage guidelines examined in this article can be subsumed, as is done in Table 2
Age-Based triage in COVID-19 guidelines.
The triage guidelines adopted in the Covid-19 context and age-based triage in general have so far stirred limited debate among legal scholars. The few texts that seek to deal with triage from the human rights perspective either focus on a specific national legal framework or fall back on ethical arguments. 52 In recent months, several papers discussing the impact of Covid-19 triage guidelines on human rights of disabled persons have been published. 53 The effect on human rights of older persons has, conversely, remained largely ignored. 54 And yet, as we saw above, some guidelines expressly draw attention to the potential incompatibility of age-based triage with human rights standards. It is thus important to consider whether, and under what conditions, age-based triage is in line with these human rights standards, that is with the principle of non-discrimination (Section 3.1) and several other human rights (Section 3.2).
Age- Based Triage and the Principle of Non- Discrimination
Of all the human rights standards, the principle of non-discrimination is the most relevant to triage. Several guidelines expressly note that denial of access to life-saving treatment based on age would amount to discrimination (BMA, CSARIM). Some of them, moreover, stress that whereas triage involving disparate treatment of older persons is undoubtedly unlawful, the same is not necessarily true of triage which has disparate effects on those persons. BMA considers that: Where patients are refused access to life-saving treatment as a result of triage […] it is likely that questions about possible discrimination may be raised […] A simple “cut-off” policy with regard to age […] would be unlawful as it would constitute direct discrimination […] Although a “capacity to benefit quickly” test would be indirect discrimination […] it would be lawful in the circumstances of a serious pandemic because it would amount to “a proportionate means of achieving a legitimate aim” […] – namely fulfilling the requirement to use limited […] resources to their best effect.
55
This view is implicitly shared by the guidelines that reject age as a triage factor but recommend the use of one of the allocation criteria with a disparate effect on older persons (Model 3). Other guidelines, however, consider the use of age for triage purposes acceptable. Since the guidelines have virtually all been drafted by medical or ethical rather than legal experts, they fail to provide a deeper analysis of the compatibility of age-based triage with the principle of non-discrimination. This subsection seeks to engage in such an analysis.
The principle of non-discrimination is one of the most fundamental principles of the human rights system. It is enshrined in all major human rights instruments. 56 The principle prohibits unfair differential treatment 57 based on certain prohibited grounds. It targets rules, policies, and measures that entail disparate treatment, that is when persons belonging to certain groups are treated differently than other persons without reasonable justification (direct discrimination). It also targets rules, policies, and measures that have disparate effects, that is when despite their apparent neutrality, they affect persons belonging to certain groups more severely than other persons (indirect discrimination). 58 Having regard to these definitions, it appears that all of the three above-mentioned models of triage involve discrimination. In Models 1-2, older persons are de-prioritised or excluded from access to life-saving treatment because of their age; they are thus prima facie directly discriminated against. In Model 3, older persons are disproportionally affected by the application of apparently neutral criteria; they are thus prima facie indirectly discriminated again. Yet, whether unlawful discrimination really takes place in these cases depends on actors, grounds for distinction, and justification.
Triage guidelines are adopted by professional medical or ethical associations. Triage decisions are made by medical staff or special bodies established within medical institutions. Since professional associations and medical institutions may be private entities, the question arises as to whether they are in the position to interfere with the principle of non-discrimination. After all, this principle, and human rights standards more generally, apply primarily between individuals and States, not between individuals and private actors. This is reflected in the texts of human rights instruments where the obligation to ‘secure to everyone’ (Article 1 of the ECHR) or to ‘respect and ensure to all individuals’ (Article 2(1) of the International Covenant on Civil and Political Rights) human rights is addressed solely to States. That might suggest that triage is only subject to human rights standards when carried out by public (State) bodies. This, however, is not the case.
Over the years, the so-called doctrine of horizontal effect of human rights has found its way to international law. 59 Under this doctrine, States may be held accountable for violations of human rights stemming from the conduct of private actors if they fail to take adequate actions to protect individuals against this conduct. At the UN level, the doctrine has been translated into the obligation to protect, which requires that States ‘prevent third parties from interfering in any way with the enjoyment of the right’. 60 At the Council of Europe level, it has been subsumed under positive obligations by means of which ‘fulfilment of a duty […] on occasion necessitates some positive action on the part of the State; in such circumstances, the State cannot simply remain passive’. 61
The applicability of the doctrine of horizontal effects in the area of health care has been repeatedly confirmed by international human rights bodies. In General Comment No. 14 (2000), the UN Committee on Economic, Social and Cultural Rights (CESCR) noted that obligations to protect include, inter alia, the duties of States […] to ensure that medical practitioners and other health professionals meet appropriate standards of education, skill and ethical codes of conduct. States are also obliged to […] take measures to protect all vulnerable or marginalized groups of society, in particular […] older persons.
62
The CESCR has furthermore stressed that the principle of non-discrimination entails ‘the right of access to health facilities, goods and services on a non-discriminatory basis’. 63 In a similar vein, the ECtHR has held that in the public-health sphere, the positive obligations ‘require States to make regulations compelling hospitals, whether public or private, to adopt appropriate measures for the protection of their patients’ lives’. 64 The ECtHR has also confirmed that ‘the responsibility of the State may be engaged in respect of the acts and omissions of health-care providers […] where an individual patient's life is knowingly put in danger by denial of access to life-saving emergency treatment’. 65 Triage guidelines and decisions that involve disparate treatment or have disparate effects on older persons may thus give rise to a violation of human rights attributable to a State even when they are issued or taken by private professional associations or private health care providers.
The principle of non-discrimination prohibits differentiated treatment which is based on one of the prohibited grounds listed in the non-discrimination clauses. 66 Age rarely features in the clauses. Yet, the lists of the prohibited grounds are virtually all open-ended, prohibiting discrimination based not only on the explicitly mentioned grounds but also on ‘other status’. 67 This expression has constantly been interpreted as encompassing age. In Love v Australia, the UN Human Rights Committee (HRC) noted that ‘a distinction related to age […] may amount to discrimination on the ground of “other status”‘. 68 Similarly, the ECtHR has confirmed that ‘the list set out in Article 14 is illustrative and not exhaustive […] “age” is also a concept covered by this provision’. 69 The same view has been expressed with respect to Article 2(2) of the International Covenant on Economic, Social and Cultural Rights (ICESCR), 70 Article E of the Revised European Social Charter (ESC), 71 and Article 1 of the American Convention on Human Rights. 72 The unacceptability of discrimination on grounds of age is also stressed in instruments related specifically to human rights of older persons. 73 Thus, (older) age is one of the prohibited grounds, regardless of whether it is expressly mentioned in a non-discrimination clause. Age-based triage therefore falls under the scope of application of these clauses.
Unlawful discrimination occurs when the differentiated treatment based on one of the prohibited grounds has no objective and reasonable justification, that is it does not pursue a legitimate aim and there is no ‘reasonable relationship of proportionality between the means employed and the aim sought to be realised’. 74 International human rights bodies have repeatedly found that certain instances of prima facie discrimination based on age were compatible with human rights standards. In Love v Australia, the HRC held that imposing a mandatory retirement age (60) on a pilot pursued the legitimate aim of maximising flight safety and was proportionate, since the selected age threshold reflected widespread national and international practice. 75 In Schwizgebel v Swizerland, the ECtHR concluded that debarring a woman from adopting a second child due to her age did not amount to discrimination because the measure pursued the legitimate aim of protecting the well-being of the child and was not clearly disproportionate. 76
There is very limited international case-law related to triage. Claims of discrimination, albeit based on the place of residence, were made in Pentiacova and Others v Moldova. The applicants were individuals suffering from chronic kidney failure, who wished to have access to a higher quality treatment purportedly provided in a specific hospital in the capital. 77 The ECtHR rejected the application on account of the lack of evidence attesting to the differences between hospitals, without engaging in any detailed analysis of the principle of non-discrimination. A more relevant case, considered by the Inter-American Court of Human Rights (IACtHR), is Poblete Vilches et al. v Chile. 78 The petitioners argued that the death of their relative, a 76-year-old man, was caused by medical malpractice and the refusal to provide him with access to the ICU and to an artificial respirator. The Court concluded that ‘[t]he patient required urgent, good quality medical care, which the public health system failed to provide, so that the situation resulted in discrimination owing to his condition as an older person’. 79 It stressed that States had the obligation to ensure access to emergency medical services on an equal basis and that ‘in the case of older persons, as a vulnerable group, there is an increased obligation to respect and to ensure their right to health’. 80 Although the Court did not go into detail as to whether critical shortage of resources has an impact on the scope of this obligation, its reasoning and the emphasis placed on special obligations towards older persons do not seem to leave space for any de-prioritisation or exclusion of older persons from access to life-saving treatment.
The scarcity of case-law makes it difficult to predict whether other human rights bodies would embrace the same approach as the IACtHR. What is clear is that they would need to assess whether triage, in any of its three models, has objective and reasonable justification, that is whether it pursues a legitimate aim and is proportionate to this aim. The overall aim of triage is to save as many lives as possible in an emergency situation. Although non-discrimination clauses do not contain any lists of legitimate aims, it is highly unlikely that the aim of saving as many lives as possible would be found illegitimate. After all, human life is the supreme value protected by all human rights instruments. The aim however does not justify all the means. The means – the three models of triage – must be assessed to see whether there is a ‘reasonable relationship of proportionality between [them] and the aim sought to be realised’ 81 and whether they are able to reach this aim in the first place.
Model 1 suggests that older persons should be treated less favourably because older age determines the likelihood to benefit from treatment. It is thus argued that de-prioritisation or exclusion of older persons is a means to achieve the aim of saving as many lives as possible. This argument, however, is problematic. The prevalent view is that while older persons might, as a group, have a lower likelihood to benefit, it is not due to older age itself. As noted in the BSICM guidelines, ‘frailty and reduced cognition, more than age, are independent predictors of outcome when elderly patients are admitted to the ICU’. 82 That older persons might be on average less likely to benefit from treatment does not mean that it is lawful to de-prioritise or even exclude all older persons from access to life-saving treatment. Patients need to be assessed based on their individual health condition, not on personal characteristics. Doing the latter would amount to an act of ageism: 83 older persons would be treated worse merely because of their birth date, on the assumption that this date mechanically determines their medical prognosis. It is hard to imagine how this model could be compatible with the principle of non-discrimination.
Model 2 uses age as a tiebreaker. Here, taking account of age is not meant to contribute to saving as many lives as possible but, rather, to help decide which lives shall be saved. Using older age in this context tends to be justified by the life cycle principle which suggests that younger persons should be accorded priority in treatment because they ‘have had less opportunity to live through life's stages’.
84
The principle of non-discrimination indeed makes it possible to take positive measures with respect of certain groups. In D.H. v the Czech Republic, the ECtHR held that this principle does not prohibit a […] State from treating groups differently in order to correct “factual inequalities” between them; indeed in certain circumstances a failure to attempt to correct inequality through different treatment may in itself give rise to a breach […]
85
It is uncertain, however, whether difference in age can be treated as a factual inequality. And even if it could, it might be argued, as the IACtHR did in Poblete Vilches, that ‘older persons are particularly vulnerable as regards access to health’ 86 due to both natural and social factors. Hence, positive measures should be adopted in their favour rather than to their detriment. Model 2 does the latter and, as such, it seems to be, again, largely based on ageist attitudes, carrying a risk of further strengthening and even institutionalising these attitudes. This model, thus, has a negative effect not only on the individual level, depriving older persons of ‘a meaningful opportunity to benefit from life-saving care’ 87 because of their age, but also on the societal level, making the view that older lives are inherently less valuable than younger lives part of the official policy. 88 It is again hard to imagine how this model could be compatible with the principle of non-discrimination.
Model 3, building solely on medical considerations, does not foresee disparate treatment of older persons. Yet, although apparently neutral, it affects those persons more severely as well due to their statistically higher likelihood to have worse medical prognosis. This model may, therefore, involve indirect discrimination. 89 The BMA guidelines pay attention to this aspect noting that indirect discrimination might be justified in extreme situations ‘because it would amount to “a proportionate means of achieving a legitimate aim” […] – namely fulfilling the requirement to use limited […] resources to their best effect’. 90 This argument has merits. Model 3 relies on a criterion, which, although not age neutral, directly contributes to saving as many lives as possible. It does not target older persons specifically, nor does it intend to have any direct impact on them. All individuals, whatever their age, have ‘a meaningful opportunity to benefit from life-saving care’. 91 The only factor which matters is the individual health condition, not membership in any age group. While triage decisions made within Model 3 may still take a heavier toll among older persons, the model does not deny these persons the chances open to others. Unlike Models 1 and 2, which explicitly envisage disparate treatment of older persons, Model 3 does not envisage such treatment and, as such, it is compatible with the principle of non-discrimination. 92
Age- Based Triage and Other Human Rights
In addition to the principle of non-discrimination, age-based triage may conflict with certain other human rights, especially the right to life, the prohibition of inhuman and degrading treatment, the right to private life, and the right to health. All these rights are enshrined in international human rights instruments. 93 The right to life and the prohibition of inhuman and degrading treatment are absolute rights. Yet, triage typically involves positive obligations and judicial bodies have shown readiness to treat these rights as somehow ‘negotiable’ and to grant States a rather wide discretion (margin of appreciation) in this area, similarly to cases involving relative rights. 94 In a rare, albeit very short piece of scholarship looking on triage from a human rights perspective, Arosemena Solorzano rightly notes that since triage constitutes an interference with human rights it needs to be assessed under the classical limitation test. 95 This test includes three conditions – legality (the measure is prescribed by law), legitimacy (the measure pursues a legitimate aim), and necessity (the measure corresponds to a pressing social need and is proportionate to the aim). 96 While the test has been elaborated upon in most detail by the ECtHR, it is applied by other human rights bodies as well. 97
The Pentiacova case confirms that triage should be subject to this test. In this case, the applicants, who had allegedly been denied access to higher quality treatment, invoked the right to life, the prohibition of inhuman and degrading treatment, and the right to private and family life.
98
The ECtHR started the analysis with the right to private and family life. It first stressed that ‘private life includes a person's physical and psychological integrity’
99
and that complaints related to funding of health care could fall under Article 8 of the ECHR. It also noted that when ‘the issues involve an assessment of the priorities in the context of the allocation of limited State resources’,
100
States enjoy a wider margin of appreciation. In a passage which merits particular consideration, it held that while it is clearly desirable that everyone should have access to a full range of medical treatment, including life-saving medical procedures and drugs, the lack of resources means that there are, unfortunately, […] many individuals who do not enjoy them, especially in cases of permanent and expensive treatment.
101
The ECtHR thus accepted that triage may in some cases be necessary and compatible with the right to private and family life. When faced with scarce resources, States may limit access to these resources as long as they ‘strike a fair balance between the competing interests of the applicants and the community as a whole’. 102 Moldova, according to the ECtHR, struck such a balance in the case at hand and the complaint was declared manifestly unfounded under Article 8 ECHR. Due to this conclusion, the ECtHR did not find it necessary to discuss the complaints under Articles 2 (the right to life) and 3 (prohibition of inhuman and degrading treatment) of the ECHR in any detail, suggesting nonetheless that the same test would apply here with respect to the positive obligations of States. It expressly noted that ‘an issue may arise […] where it is shown that the authorities […] put an individual's life at risk through the denial of health care which they have undertaken to make available to the population generally’. 103 In Pentiacova, this issue did not arise, because a death from a disease was not in itself proof of the shortcomings in the health care system. The statement however confirms that triage falls under the scope of the right to life.
The same conclusion has been reached by other human rights bodies. In Toussaint v Canada, the HRC held that States parties have the obligation to provide access to existing health-care services that are reasonably available and accessible when lack of access to the health care would expose a person to a reasonably foreseeable risk that can result in loss of life.
104
In Poblete Vilches, the IACtHR went one step further, concluding that ‘the omission to provide basic health care services’ 105 to an old man due to his age amounted to a violation of his right to life. Other human rights, including the rights to personal integrity and to health were also violated in the case. That triage raises an issue under the right to health was, moreover, acknowledged by the European Committee on Social Rights (ECSR) in its 2017 Conclusions on France. 106 The UN CESCR did not invoke triage explicitly but recalled that even when the State is unable to comply fully with its obligations under the ICESCR due to limited resources, it must ensure equitable distribution of health care facilities, goods, and services. 107
Despite the relative scarcity of case-law, international human rights bodies clearly accept that triage constitutes a prima facie interference with several human rights and, as such, it must be scrutinised under the three-part limitation test. First, triage must be prescribed by law, that is ‘there must be some rule framework through which the decisions on triage are taken’. 108 This framework must contain substantive rules commanding the outcome of triage as well as procedural rules indicating how this outcome should be reached. Whether the combination of a general legal act – setting the requirement of ‘appropriate professional level’ of health care – and guidelines issued by professional associations providing details on how this term is to be interpreted in times of emergency meets the condition of legality remains uncertain. Human rights bodies have, however, shown willingness to accept that certain matters within health care may be ‘left to medical practice and guidelines’. 109 Second, triage must have a legitimate aim. That this is generally the case was established in the previous subsection, though the aim identified there (to save as many lives as possible) would need to be subsumed under the legitimate aims listed in human rights treaties (the protection of health, the protection of rights and freedoms of others, and certain others).
The third condition, that of necessity and proportionality, indicates that triage must correspond to a pressing social need and be proportionate to the legitimate aim. The requirement of a pressing social need suggests that human rights must not be restricted without cogent reasons. When assessing this requirement, the ECtHR considers ‘whether the reasons adduced by the national authorities […] were “relevant and sufficient”‘. 110 In areas where no international consensus exists, wider discretion tends to be granted to States to select from various measures at their disposal. Triage belongs among such areas because, as the WHO has acknowledged, ‘there is no single correct way to resolve potential tension between utility and equity’ 111 when triage is resorted to in emergency situations. States thus have space to choose from the different allocation models available and as long as their choice is not obviously irrelevant or insufficient, it could be found acceptable.
Model 3, based on medical considerations, would very likely meet this condition. In fact, this model has been advocated for by several national and international human rights bodies, which have commented upon triage in the Covid-19 context. The UN Independent Expert on the enjoyment of all human rights by older persons Rosa Kornfeld-Matte stressed that ‘triage protocols must be developed and followed to ensure such decisions are made on the basis of medical needs, [and] the best scientific evidence available’. 112 The US Department of Health and Human Services Office for Civil Rights (OCR) noted that ‘decisions […] whether an individual is a candidate for treatment should be based on an individualized assessment of the patient based on the best available objective medical evidence’. 113 That ‘decisions related to access to or withdrawal of intensive care services […] should be based on an evaluation of a patient's individual prognosis’ was also highlighted by Alzheimer Europe. 114 These same bodies, conversely, have taken a critical stance toward models that foresee disparate treatment of older persons (Models 1 and 2). The Independent Expert opined that ‘withholding or refusing the provision of medical treatment on the basis of an age […] is implicitly prohibited under international human rights law’. 115 OCR rejected the possibility to deny medical care ‘on the basis of stereotypes, assessments of quality of life, or judgments about a person's relative “worth” based on […] age’. 116 Alzheimer Europe added that ‘the ranking of lives on the basis of value judgements or of assumptions about quality of life are unacceptable’. 117
The three models score differently not only under the pressing social need requirement but also under the principle of proportionality. As we saw above, this principle requires that a fair balance be struck between the interests of certain persons or groups and those of the broader society. We also saw that Models 1 and 2, foreseeing disparate treatment of older persons, are not better suited to reach the legitimate aim of saving as many lives as possible than the model relying solely on medical considerations. Unlike the latter, however, these two models de-prioritise or exclude all persons belonging to certain age groups from access to life-saving treatment, without taking into account their individual health condition. By marking older persons as dispensable, Models 1 and 2 can hardly be considered as striking a fair balance between the interests of older persons and those of the broader society. Model 3, based on the likelihood to benefit, distributes the burden of an emergency situation more evenly across the society. While older persons have a higher probability that this burden will befall them, they are not doomed to be ‘sacrificed’ merely because of their age. The balance is thus struck more fairly and without a disproportionate interference with rights of any specific group of persons.
Triage is therefore not necessarily incompatible with such human rights as the right to life, the prohibition of inhuman and degrading treatment, the right to private life, or the right to health. Yet, it must be prescribed by law, pursue a legitimate aim, and refrain from imposing an unnecessary and disproportionate burden on certain groups. Whereas Model 3, based on the likelihood to benefit, meets this test despite the disparate effects of its application on older persons, Models 1 and 2, which envisage disparate treatment of such persons, singling them out merely because of their age, fail to do so.
CONCLUSION
In their common statement issued on 26 March 2020, UN experts on human rights noted that Covid-19 is a serious global challenge which, however, could be ‘a wake-up call for the revitalization of universal human rights principles’. 118 Such a wake-up call is also warranted with respect to triage. Although known and practised for decades, triage has so far attracted limited attention of legal scholars. The recent Covid-19 crisis has shown that there are cogent reasons to change this approach and to subject triage to thorough human rights scrutiny.
Since spring 2020, professional medical and ethical associations in many countries of the world have adopted Covid-19 triage guidelines which should help medical institutions and medical staff solve ethical and legal dilemmas that arise in the situation of critical resource shortage. These guidelines compensate for the lack of formal legal rules on triage, providing an authoritative interpretation of what an appropriate professional level of health care means in a critical situation. The guidelines rely on different allocation criteria and, as such, take different approaches to the factor of age. The analysis of 11 triage guidelines adopted in 8 European and 3(4) non-European countries has shown that there are three main models used in these guidelines. None of them is truly age neutral. The first two models use older age as a part of the primary allocation criterion, helping determine the likelihood to benefit from treatment in Model 1, or as a tiebreaker in Model 2. Under these models, older persons are de-prioritised or excluded from access to life-saving treatment merely on account of their age (disparate treatment). Model 3 rejects using age as a relevant consideration, relying solely on the medical prognosis. The application of this model, however, also has greater effects on older persons due to their higher chance of having a worse medical prognosis (disparate effects).
By singling out, directly or indirectly, older persons, the Covid-19 triage guidelines give rise to challenges with respect to the principle of non-discrimination and several other human rights (the right to life, the prohibition of inhuman and degrading treatment, the right to private life, and the right to health). Age-based triage under any of the three models constitutes a prima facie interference with these human rights standards. The potential conflict with the principle of non-discrimination must be assessed through the non-discrimination test. This test limits unlawful discrimination to differentiated treatment that is based on one of the prohibited grounds and has no objective and reasonable justification (that is, there is no legitimate aim or the means are not proportionate to the aim). The potential conflict with human rights must be assessed though the limitation test. This test considers unlawful those interferences with human rights which are not prescribed by law, do not pursue a legitimate aim, or are not necessary (that is, they fail to correspond to a pressing social need or are disproportionate).
This article has shown that the three models of age-based triage are subject to the non-discrimination test and that they score differently under it. They are subject to this test regardless of whether triage guidelines are adopted and triage decisions are made by public or private actors. While human rights standards primarily apply in the relation between individuals and States, States have, under the doctrine of horizontal effect of human rights, the positive obligation to protect individuals from interferences with their human rights by other non-State entities. Moreover, although age is rarely expressly included in non-discrimination clauses contained in human rights treaties, it has been consistently read into them by human rights bodies. All the three models of age-based triage entail prima facie discrimination based on age. In Models 1 and 2, which foresee disparate treatment of older persons, direct discrimination is at stake. In Model 3, whose application has disparate effects on older persons, indirect discrimination is at stake.
Triage in general pursues a legitimate aim of saving as many lives as possible in times of critical resource shortage. Models 1 and 2 recommend reaching this aim by denying access to life-saving treatment to individuals identified by their age, on account of the views that older age automatically determines the medical prognosis or that it should play a role in the ranking of lives more or less worthy of being lived. These views are prejudicial to older persons, depriving them of a meaningful opportunity to survive solely because of their birth date. They are also harmful to society at large, as they are built on, and further strengthen, ageist attitudes. Models 1 and 2 thus place a disproportionate burden on older persons and, as such, are incompatible with the principle of non-discrimination. Model 3 also affects older persons more severely due to their higher likelihood to have worse medical prognosis. It, however, does not target older persons specifically, nor does it deprive them of a meaningful opportunity to survive. The only factor which matters is individual health condition, not membership in any age group. By not placing a disproportionate burden on older persons, Model 3 is compatible with the principle of non-discrimination.
The three models also score differently under the limitation test applied in case of prima facie interference with certain other human rights. Similarly to the non-discrimination test, Models 1 and 2 fail in the part of the test which focuses on the proportionality of the measures and the overall necessity to resort to them. Model 3, which is based on an individual assessment of the health state of each individual and which treats all personal characteristics, including age, as irrelevant, constitutes a more balanced, proportionate, and fairer means to reach the aim of saving as many lives as possible in situations involving scarcity of resources. Triage guidelines should therefore opt for this third model and should never include older age among factors determining access to life-saving treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This article is the outcome of the Research Project on Human Rights of Older Persons, funded by the Research Academy of the Czech Republic (GAČR project No.18-08130).