
Abstract
In this open-label single-arm study, we tested the preliminary therapeutic effects of a four-week mindfullness-based intervention (MBI) tailored for fibromyalgia, including weekly online group meetings and daily mindfulness practices. Forty-six patients completed the intervention. The primary outcome was pain intensity scored on a numerical rating scale (NRS). Secondary outcomes included verbal fluency and self-reports of affective pain, quality of life, sleep quality, mood, emotion regulation, and psychological impairment. Transcranial magnetic stimulation was used to measure mindfulness-induced cortical excitability changes. Participants reported statistically reduced pain intensity post-training, with only 15.3% of the patients demonstrating clinically meaningful pain relief. A moderate improvement in quality of life, with only 45.6% clinical responders, were noted. Small-to-medium improvements in affective pain level, mindfulness level, and resilience as well as increase in long-interval intracortical inhibition—a measure of GABABergic inhibition—were observed. The study introduces a novel MBI tailored for fibromyalgia. Nonetheless, given the current study design and the lack of clinical significance of the findings despite statistical significance, the results are insufficient to draw firm conclusions regarding its potential therapeutic efficacy. Future sham-controlled randomized clinical trials are necessary to validate and expand upon these results.
Introduction
The management of chronic pain remains a major challenge to the healthcare system (Nicholas et al., 2019). Fibromyalgia (FM) is one of the most debilitating pain conditions, frequently difficult to diagnose and treat (Giorgi et al., 2023; Lledó Boyer et al., 2010; Zhang et al., 2023). It is a complex chronic pain disorder characterized by persistent and widespread musculoskeletal pain and is associated with various symptoms – chronic fatigue, psychological impairment, and sleep fragmentation (Wolfe et al., 2010). Patients often report verbal fluency impairments (Bell et al., 2018; Sallinen & Mengshoel, 2021) and difficulty regulating their emotions (Kim et al., 2023). The impact of FM on patients’ quality of life (QoL), disability, and functionality poses a large burden (Annemans et al., 2009). Unlike the limited benefits of medication in FM (Arnold et al., 2012), the use of non-pharmacological interventions can tackle the multifaceted nature of chronic pain by promoting coping mechanisms, adaptation, and self-management, enabling patients to better control the condition (Kundakci et al., 2022).
Finding its roots in Buddhist meditation (Goleman, 1977), mindfulness is an innate aspect of human consciousness, relating to one's ability to focus on the present moment in a non-attached, non-judgmental, and non-evaluative manner (Kabat-Zinn, 2003; Kirmayer, 2015). Mindfulness, including mindfulness meditation, has emerged as a promising tool to develop non-judgmental awareness of noxious stimuli, boosting coping mechanisms in FM (Adler-Neal & Zeidan, 2017). Mindfulness-based interventions (MBI) have shown efficacy in improving global well-being and symptoms including sleep, fatigue, stress, mood, and depression in FM (Amutio et al., 2015; Cash et al., 2015a; Goldenberg et al., 1994; Perez-Aranda et al., 2019; Sephton et al., 2007). MBIs also improved resilience, pain-coping efficacy, and QoL in FM patients compared to treatment-as-usual groups (Amutio et al., 2015; Cejudo et al., 2019; Davis & Zautra, 2013; Pérez-Fernández et al., 2022). However, pain reductions are limited and inconsistent across studies (Adler-Neal & Zeidan, 2017; Davis & Zautra, 2013).
Despite the therapeutic potential of mindfulness in FM (Adler-Neal & Zeidan, 2017; Gordon et al., 2023; Haugmark et al., 2019; Kundakci et al., 2022; Leça & Tavares, 2022), MBIs demand significant time commitments, typically lasting 6–20 weeks, with weekly 1–2 h sessions and daily home practice (Amutio et al., 2015; Cejudo et al., 2019; Davis & Zautra, 2013; Kabat-Zinn, 2013). MBIs frequently require specialized psychotherapists and pain clinics, limiting their accessibility and feasibility for many patients. In contrast, the implementation of brief MBIs tailored to the conditions can be more effectively administered in primary care (McClintock et al., 2019), with better efficacy than conventional MBIs (Adler-Neal & Zeidan, 2017). Larger improvements in pain, symptoms, and social engagement were previously observed following an FM-tailored MBI than was the case with cognitive-based therapy (Van Gordon et al., 2017). Therefore, we developed an online four-week MBI, comprising weekly group meetings and daily practice, with its modified intensity and duration previously validated in healthy individuals (Demarzo et al., 2017; Jain et al., 2007; Rana et al., 2022) and patients with endometriosis (Moreira et al., 2022, 2023). We also tailored the intervention to FM by including weekly topic education sessions on disease management through mindfulness practice and by designing the whole intervention, while taking into consideration the day-to-day limitations of individuals with FM.
The mechanisms underlying mindfulness-based analgesia are still elusive. The dynamic model of mindfulness-based analgesia postulates that analgesia is achieved via increased cognitive regulation in beginners, while pain reduction in more experienced practitioners is associated with a reduction in the cognitive-affective interference observed in pain processing (Lu et al., 2023). Previous studies have shown that mindfulness-based analgesia is not mediated by endogenous opioid release (May et al., 2018; Wells et al., 2020; Zeidan & Vago, 2016). Rather, its efficacy appears to stem from an interplay of multifaceted mechanisms, including neuronal modulations, emotional regulation, and attentional and cognitive processing (Jinich-Diamant et al., 1916; Zeidan et al., 2011, 2019). Single- and paired-pulse transcranial magnetic stimulation (TMS) paradigms serve as robust tools for exploring cortical excitability, offering valuable insights into mechanisms underlying specific interventions (Burke et al., 2019). FM patients tend to have a global corticospinal hyper-excitability, typified by a higher resting motor threshold (RMT) (Mhalla et al., 2010; Pacheco-Barrios et al., 2022) and a reduced intracortical inhibition, suggesting central disinhibition in FM (Molero-Chamizo et al., 2023; Pacheco-Barrios et al., 2022). Therapeutic interventions including aerobic exercise, transcranial brain stimulation, and pregabalin demonstrated the ability to enhance intracortical inhibition and cortical silent periods in patients compared to placebo groups (Pacheco-Barrios et al., 2022). The only TMS mechanistic investigation into meditation showed increased gamma-aminobutyric acid B (GABAB) receptor-mediated cortical inhibition in meditators compared to non-meditators after a 60-min meditation session (Guglietti et al., 2013). Our study was the first to examine the impact of mindfulness practice in FM patients on brain excitability using TMS.
The primary aim of this single-arm study was to test the preliminary effectiveness and feasibility of the brief and FM-tailored mindfulness intervention in reducing pain intensity in individuals with FM compared to baseline. We also examined whether participants reported improvements in affective pain, QoL, verbal fluency, FM-associated symptoms, and emotional regulation following the intervention. Two further objectives were to explore the mechanistic impact of the MBI on TMS-assessed cortical excitability and whether the intervention was successful in teaching mindfulness to the patients through self-reports of mindfulness level. Furthermore, we explored whether an increase in mindfulness level could predict symptom improvement.
Material and Methods
Study Design
We conducted a monocenter single-arm open-label study at the University Medical Center in Göttingen, Germany. The study had three phases: a two-week baseline period (BA), a four-week Brief Mindfulness Intervention for Fibromyalgia (BMIF), and a post-treatment measure (PM) conducted within a week following the last intervention session. Each measurement visit took place in the clinic, which comprised a German-language battery of questionnaires assessing pain, QoL, mindfulness level, FM-associated symptoms, the Regensburg verbal fluency test (Aschenbrenner et al., 2000), and TMS measurements. The study took place in a hybrid setup, with some meetings taking place in the hospital and others supervised online via Zoom (Zoom Video Communications Inc., California, USA). The licensed version of the videoconferencing platform was used to ensure secure and encrypted online meetings. The study was approved by the local Ethics Committee. Data was collected between May 2022 and July 2023. This study is a subcomponent of a larger clinical trial testing the effects of combining mindfulness meditation and transcranial direct current stimulation in FM patients trained in mindfulness, which was registered at the German Clinical Trials Register (DRKS00029024). In the clinical trial, the BMIF precedes the combined intervention and the findings of the effects of the combined treatment are reported elsewhere.
Participants
Mindfulness meditation-naïve FM patients aged from 30 to 75 years and proficient in German were eligible for enrollment if they fulfilled the preliminary American College of Rheumatology Diagnostic Criteria 2010 for FM with a widespread pain index ≥ 7 and a symptom severity ≥ 5 (Wolfe et al., 2010). Included participants had had stable disease for at least six months before participation, and analgesic or psychotropic medication, alternative therapies (psychotherapy and physiotherapy), and/or homeopathic remedies for FM had been stable for more than 4 weeks before baseline and during the study. All participants required access to the Internet and basic skills in how to operate it.
Concerning permitted ongoing treatments during the study, consumption of more than three medications for FM symptom relief and the following therapies—strong opioids, carbamazepine, benzodiazepines, anticholinergics, N-methyl-D-aspartate receptor antagonists, local anesthetic spinal column infiltration, cannabinoids with tetrahydrocannabinol concentrations ≥ 0.2 mg/mL, acupuncture, and chiropractic manipulations––were not allowed. Participants who were taking non-steroidal anti-inflammatory drugs, cyclooxygenase-2 inhibitors, or low-dose cannabidiols (dose < 25 mg/day) were asked to refrain from taking them up to 24 h before study visits. Participants were permitted to continue established and ongoing psychotherapy (maximum once per week) and/or physiotherapy (up to three times per week) throughout the study period. Participants with major medical conditions, chronic migraine, or alcohol/drug addiction were excluded. Pregnant or breastfeeding women were not allowed to participate.
We recruited participants via the pain outpatient clinic of the Department of Anesthesiology at the University Medical Center Göttingen, reports in local newspapers, advertisements in local hospitals, online social media, cooperating local and national pain and rheumatology practices, and collaboration with self-help groups for FM and rheumatological conditions such as the Deutsche Fibromyalgie Vereinigung (www.fibromyalgie-FM.de) and Deutsche Rheuma-Liga (www.rheuma-liga.de). Interested participants were first contacted via email, followed by an elaborate phone pre-screening. When participants met the inclusion criteria, an appointment was made for the clinical assessment and informed consent, confirmed by an experienced pain physician (FP). All participants were required to sign an informed consent form.
Mindfulness Training
Patients participated in a brief mindfulness intervention specifically tailored for patients with FM and spearheaded by the senior author, Olga Lucía Gamboa Arana (OLGA), an adept mindfulness teacher with approximately ten years of experience (www.eqness.com). The four-week intervention aimed to share tools and resources derived from mindfulness practices that would provide participants with the appropriate techniques and adequate experience necessary to follow a 20-min guided breathing meditation. The MBI was structured into four formal mindfulness sessions (once per week, with a duration of two hours led and supervised online via Zoom by a trained mindfulness instructor (SES). That instructor, with five years of experience in teaching meditation, and who additionally received intensive training by OLGA on the teaching of this holistic mindfulness program, delivered the sessions in German. The MBI also involved informal practice conducted individually by the participants at home with the help of audio-guidance (five times per week from Monday to Friday). Participants reported their daily mindfulness routine in a mindfulness diary. Each of the supervised weekly training sessions comprised guided mindfulness meditation practices (including mindful breathing meditation), topic education on different aspects of FM and mindfulness, as well as group discussions. Participants were encouraged to share and reflect on their experiences with the newly acquired mindfulness techniques to enhance their practice, as well as to address any difficulties or problems they encountered while applying the techniques. Through this process of reflection and problem-solving, participants were able to deepen their understanding of mindfulness techniques and improve their ability to incorporate them into their daily lives. The online sessions were conducted in groups consisting of a maximum of 10 participants.
The content of the sessions is summarized in Table 1. During the BMIF, participants had to follow a daily mindfulness routine consisting of a 20-min audio-guided mindful breathing meditation and an informal mindfulness practice of their choice, such as mindful gardening, eating, or walking, among others. For the mindful breathing meditation, the participants were instructed to meditate in a comfortable sitting position with their eyes closed, which they would maintain for 20 min. They were taught the proper sitting posture for meditation, which involved sitting with a straight spine and placing their hands on their thighs if seated on a chair, or using a cushion on the floor to sit on. Participants were encouraged to focus on breathing from the diaphragm or lower abdomen, as opposed to the chest, to aid initial relaxation and encourage a natural breathing rhythm. The audio recording for at-home meditation practice was the mindful breathing meditation taught in the online session that week. Over the course of the weekly sessions, the content of mindful breathing meditation recordings comprised progressively diminished levels of instructional guidance provided and extended duration of silent pauses between narrated segments. The concept of the informal mindful activity involved bringing the awareness of the present moment to the physical, psychological, and emotional sensations, as well as the external surroundings during the activity.
Content of the Supervised Online Sessions of the Brief Mindfulness Intervention for Fibromyalgia (BMIF).
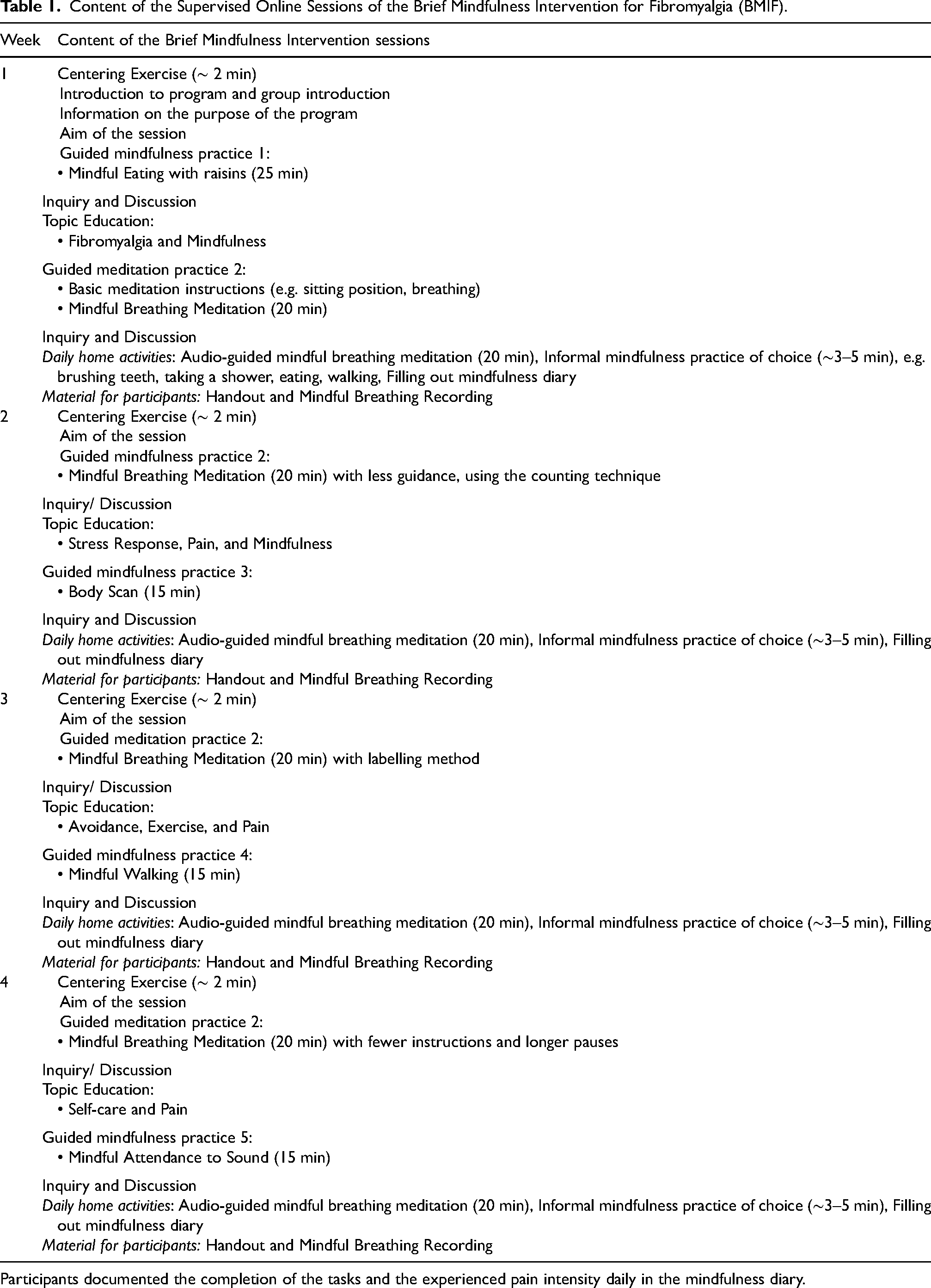
Participants documented the completion of the tasks and the experienced pain intensity daily in the mindfulness diary.
The program's development, including the educational aspects, was the result of a joint effort between the University of Göttingen (FP, PR) and the University of Sydney (OLGA). The intervention was designed based on and adapted from the standard mindfulness-based stress reduction program (Kabat-Zinn, 1982, 2013), while its structure bore resemblance to that of Moreira et al. (2022). OLGA, FP, and PR created the content of the topic education parts based on the state of the art surrounding important aspects of FM management and the application of mindfulness in day-to-day life for patients (refer to Topic Education in Table 1).
This intervention's novelty resides in its brief, structured format tailored for FM by incorporating education on FM management alongside mindfulness practices. This aligns with the previous studies showing that tailored approaches may be more effective for specific conditions than conventional MBIs (Adler-Neal & Zeidan, 2017; McClintock et al., 2019). Participants were also instructed to engage in informal mindfulness activities, such as mindful gardening or walking, and to keep a diary, which promotes habitual practice and integration into daily life. Moreover, the intervention emphasizes increasing participants’ independence by gradually diminishing guidance in mindfulness exercises, which is intended to foster self-efficacy and long-term practice beyond formal sessions.
Primary Outcome
Pain intensity was measured using the ordinal 11-point numerical rating scale (NRS) (Bolton & Wilkinson, 1998; Euasobhon et al., 2022; Hawker et al., 2011), expanding from 0 (no pain) to 10 (worst imaginable pain). Participants rated their perceived pain intensity twice per day (reported immediately after waking up in the morning and before going to bed in the evening) in a pain diary. The validated NRS, which is considered the gold standard in studies of chronic pain conditions (Farrar et al., 2001), has a good test-retest reliability (r = 0.79–0.96) (Downie et al., 1978; Hawker et al., 2011; Jensen & McFarland, 1993). The mean NRS was calculated per week. A reduction of ≥ 30% on the NRS ratings is considered a clinically relevant pain relief (Dworkin et al., 2008; Farrar et al., 2001; Smith et al., 2020).
Secondary Outcomes
All Secondary outcomes were assessed at BA and PM.
QoL was assessed by the German version of the Fibromyalgia Impact Questionnaire (FIQ; Cronbach's α = 0.92) (Abd El-Naby et al., 2013; Offenbaecher et al., 2000), which assesses the overall function, symptoms, and overall impact of the disease. The total score is calculated as the sum of all the items (range, 0- no impact of FM to 100- maximal impact of FM), with higher FIQ scores indicating poorer QoL (Gusi et al., 2010). A decrease of ≥ 14% in the FIQ scores is considered a clinically relevant improvement in QoL (Bennett et al., 2009).
Affective pain level was measured using the last four items (affective descriptions of pain: ‘awful’, ‘horrible’, ‘dreadful’, ‘terrible’) of the self-reported Pain Description List (PDL;range:0 to 12) (Korb & Pfingsten, 2003.; Petzke et al., 2020). Higher scores indicate higher levels of affective pain.
The 39-item Five-Facet Mindfulness Questionnaire (FFMQ) (Baer et al., 2006; Michalak et al., 2016) was administered to measure mindfulness levels. It addresses five distinct aspects of mindfulness – observing (observing internal and external experiences; 8 items; α = 0.90), describing (ability to express experiences in words; 8 items; α = 0.88), acting with awareness (maintaining awareness while performing activities; 8 items; α = 0.74), non-judgment (non-evaluative stance towards inner experiences; 8 items; α = 0.80), and non-reactivity (ability to observe inner experiences without reacting to them; 7 items; α = 0.78). Individual scores range from 8 to 40 for the facets, except for non-reactivity (7 to 35), and higher scores reflect higher levels of mindfulness The mean of the five facets was also computed to obtain an overall mindfulness score (range 7.8 to 39). Higher scores reflect higher levels of mindfulness.
The Positive and Negative Affect Schedule (PANAS; Cronbach's α: positive affect: 0.91, negative effect : 0.87) (Breyer & Bluemke, 2014; Díaz-García et al., 2020; Watson et al., 1988) was used to assess positive and negative affect. The 20 items of the questionnaire are adjectives indicating emotional states (“excited“, “nervous“, “afraid“) which are rated according to the extent the respondent has felt these states over the past week. Scores can range from 10 to 50, with higher scores representing higher levels of positive or negative affect, respectively.
Sleep quality was assessed by the Pittsburgh Sleep Quality Index (PSQI; Cronbach's α = 0.83) (Buysse et al., 1989; Tietze et al., 2014). The sum of the 19 self-report items addressing different aspects of sleep quality (e.g. duration, efficiency, latency, disturbance) were summed to calculate the total score (range: 0 to 21), where higher ratings indicate worse sleep. A score from 0–5 points is considered an indicator of healthy sleep.
The Depression, Anxiety, and Stress Scales - 21 Items (DASS) (Lovibond & Lovibond, 1995; Nilges & Essau, 2015) was administered to assess three categories of psychological impairments, namely depressiveness, anxiety, and stress (Cronbach's α: depression: 0.82–0.88, anxiety: 0.72–0.83, stress: 0.82–0.87; Zanon et al., 2021). The final score for each subscale (7 items, range: 0 to 42) is calculated as the summed number in each subscale and multiplied by two. A higher score indicates higher symptom severity.
We evaluated different aspects of competencies for successful emotional regulation by assessing levels of attention, acceptance, understanding, and resilience, which are categories within the 27-item standardized Self-assessment of Emotional Regulation Competencies (SERC-27) (Berking & Znoj, 2011). Given the high internal consistency of the total scale (Cronbach's α = .90), the sum of the scores of three items (range: 3 to 15) was utilized, with higher scores reflecting better emotion regulation competencies.
The four subtests of the Regensburg word fluency test were implemented to test the verbal fluency of patients (Aschenbrenner et al., 2000). Phonemic verbal fluency was evaluated by asking patients to say as many German words as possible in two minutes beginning with the letter P (phonemic naming), and starting with G and R alternately (phonemic switching). Semantic verbal fluency was measured by asking participants to say as many German words as possible in two minutes in the semantic category of animals (semantic naming) and alternately between sports and fruits (semantic switching). The order of the subtests was randomized for each session per subject. The outcome measure was percentile rank values which were calculated from the number of correct responses during two minutes, considering age differences(Aschenbrenner et al., 2000).
Transcranial Magnetic Stimulation (TMS)
Data collection with TMS was conducted following previously published recommendations and safety guidelines (Groppa et al., 2012; Rossi et al., 2021). The reliability and stability of RMT, input-output (I-O) curves, and paired-pulse TMS measures of intracortical excitability have been validated for up to one month (Therrien-Blanchet et al., 2022).
TMS was delivered using two monophasic Magstim 200 stimulators utilizing a Bistim2 module (Magstim Co., Whitland, Dyfed, UK) applied to the M1 ‘hotspot’ representing the right first dorsal interosseous (FDI) muscle through a figure-of-eight standard double 70 mm coil. We recorded motor-evoked potentials (MEPs) via Ag-AgCl surface electrodes (5 mm diameter) arranged in the classical belly-tendon montage (band-pass filter = 2 Hz–3 kHz; electrode impedance = 100 Ω–10 kΩ, sampling frequency = 5 kHz) (Rossi et al., 2009). An isolated patient amplifier system was used for amplification of the raw signal (Digitimer, Ltd., Model D360, Garden City, UK) and then digitized using a CED 3001 analog-to-digital converter (MICRA 1401 mk II; Cambridge Electronic Design Limited, Cambridge, UK). We used the Signal 2.13 software for electromyography recording.
The coil was held tangentially to the scalp and positioned in the posterior-anterior direction with 45o lateral from the midline. To accurately determine the target area and to monitor the optimal coil positioning, we used a frameless stereotactic neuronavigation system (Brainsight TMS Navigation, Rogue Resolutions Ltd) coupled with a ‘Polaris Vicra’ infrared camera (NDI, Waterloo, Canada). During each experiment, we ensured that the distance between the scalp and the coil was within 1 mm, and that the tilt and rotation deviation angles were both within 2o. A similar system was used in previous studies (Chakalov et al., 2022; Zmeykina et al., 2020).
The standard Montreal Neurological Institute 152, 2 mm T1-weighted MRI image was used as the template for the neuro-navigated anatomical hotspot hunt. The hotspot search started by manually administering single pulses with 4 s inter-stimulus interval (ISI) at 45% of maximum stimulator output (MSO) intensity while moving the coil with approximately 10 mm distances within the area between Fz, Cz, C1, and C3. In the absence of MEPs, intensity was gradually increased in steps of 5% MSO. When consistent MEPs were observed at a specific position, the position of the coil was noted in the neuronavigation. The area around this first site was then scanned carefully by gradually lowering the intensity in steps of 1–3% MSO and moving in 1 to 5 mm distances until only one site with consistently positive MEP responses remained. The hotspot was defined as the target area at which single pulse TMS consistently evoked MEPs.
First, we measured the RMT, which is the stimulator intensity to constantly produce MEPs ≥ 0.05 µV (positive MEPs) in the FDI muscle, estimated using the maximum likelihood parameter estimation by sequential testing (Awiszus, 2003; Awiszus et al., 1999; Groppa et al., 2012) based on adaptive threshold-hunting in the TMS Motor Threshold Assessment Tool (MTAT 2.1) software. To determine the state of the corticospinal activity, we increased the stimulation intensity in 10% increments from 90% to 140% RMT and measured the electromyography responses. At each intensity, 10 single pulses were delivered at 0.25 Hz and the mean was determined. The data was fitted to produce a recruitment curve with the Boltzmann sigmoid equation (Devanne et al., 1997). In case of poor curve fitting, the Gompertz sigmoidal function was implemented. The outcome parameter was the slope of the curve (Kukke et al., 2014). We also measured the TMS stimulation intensity that elicits an MEP with a mean peak-to-peak amplitude of approximately 1 mV in the FDI muscle, SI1 mV. Then, we measured intracortical activity by short-interval intracortical inhibition (SICI), intracortical facilitation (ICF), and long-interval intracortical inhibition (LICI) measures using the paired-pulse TMS mode. The SICI/ICF protocol (Kujirai et al., 1993) consisted of a subthreshold conditioning stimulus (CS) delivered at 80% of RMT, followed by a suprathreshold test stimulus (TS) at 120% of RMT. The ISIs were 3 ms and 10 ms for SICI and ICF respectively. For the LICI protocol (Burke et al., 2019; Hallett, 2007), both the CS and the TS were set at 120% RMT, which were delivered with ISIs of 100 ms and 150 ms (Redondo-Camós et al., 2022; Sanger et al., 2001; Valls-Solé et al., 1992).
TMS measures were conducted at BA and PM. The appointments of the participants were kept at the same time of day to limit circadian effects (Lang et al., 2011) and they were asked to maintain the same dose of caffeine intake before each measurement (Kalmar & Cafarelli, 2004; Zulkifly et al., 2021). We preprocessed the raw MEP data using an internally developed software, the tmsExplorer (https://github.com/omeganow/tms-explorer), to remove noisy baselines, characterized by a pre-activation of peak-to-peak amplitude ≥ 50 µV before the TMS pulse delivery, and stimulation artifacts.
Feasibility
Following successful completion of the BMIF, patients rated six statements on a 5-point Likert scale (1: strongly disagree, 2: disagree, 3: neutral, 4: agree, 5: strongly agree): 1) The contents of the group meetings were well structured, 2) The order in which the content was presented was coherent, 3) I found the psychoeducation part helpful, 4) The mindfulness teacher conveyed the concepts of mindfulness competently, 5) I found it easy to apply what I learned in the group meetings to my mindfulness practice at home, and 6) I am overall satisfied with the mindfulness intervention. A total feasibility score (range: 6 to 30) was calculated by summing up the scores of the individual statements for each participant. The feasibility outcome was assessed based on descriptive statistics with a priori criteria. The BMIF was considered feasible if the majority (≥ 50%) of the patients who completed the intervention had an overall feasible score ≥ 27 (a conservative score to ensure that the participants agree on all the statements, i.e. a minimum of 4 on each statement without the possibility to score lower than 4).
Statistical Analysis
Since our study was the first to test a brief tailored MBI in FM, we computed the sample size for a moderate effect (d = 0.5) of reduced pain intensity at PM compared to BA using a Student's paired t-test. The statistical power was set at 0.80 and α error rate of 0.05 using the G*Power software (G*Power 3.1, Düsseldorf University, Germany). A minimum of 34 participants was required to achieve a powered sample.
Baseline demographics were presented descriptively as means ± standard deviation for age, body mass index, symptom severity, widespread pain index and subgroup size/percentage for sex, handedness, and severity level of each psychological impairment. At baseline, the DASS subscores for each participant were categorized to their respective severity level (normal, mild, moderate, severe, and extremely severe) (Nilges & Essau, 2015). To address our main aim, a two-tailed Student's paired t-test was conducted to compare the QoL, pain measures, mindfulness level, FM-associated symptoms (sleep quality, mood, and psychological impairment), verbal fluency, emotional regulation competencies, and TMS outcomes. The effect size was computed as Cohen's d for parametric tests and as Wilcoxon's r for non-parametric tests. Effect size was interpreted based on Cohen's benchmark categorization (small, 0.2 ≤ d < 0.5; medium, 0.5 ≤ d < 0.8 and large, d ≥ 0.8) (Cohen, 1988). The normality of raw data was verified using the Shapiro-Wilk's test and visually with normality plots. Owing to violations of parametric assumptions or inability to transform data, Wilcoxon signed-rank tests were conducted for the following measures: FFMQ non-judgement, DASS anxiety, SEC-27 acceptance, SEC-27 attention, SEC-27 resilience, semantic switching, RMT, and SI1mV. While recognizing the challenges associated with analyzing multiple secondary outcomes, we implemented the precision interpretation method described by Parker and Weir (2022), which highlights that the risk of a false positive result increases only if general treatment efficacy is claimed based on a single secondary outcome. In our study, we do not infer any overall improvement but clearly specify which secondary outcomes showed statistically significant changes.
As part of exploratory analyses, we conducted a simple linear regression to test whether the increase in overall mindfulness level can be used to predict symptom betterment, increase in QoL, or emotional regulation. Linear regressions were only conducted for outcomes, which showed statistically significant changes from BA to PM, as shown by the paired t-tests. The normality of residuals was tested visually using histograms. Linear relationships between independent and dependent variables were checked using a scatterplot of raw data, while homoscedasticity of data was checked visually using a scatterplot of standardized residuals and standardized predicted variables. The data was transformed in case of deviations from parametric assumptions for linear regression.
The statistical analysis plan was approved by the Department of Medical Statistics at the University Medical Center Göttingen. The statistical analyses were conducted in IBM SPSS 28.0. Statistical significance was set at P ≤ .05.
Results
Sample Description and Baseline Demographics
Out of 106 individuals screened and assessed for eligibility, forty-eight (45.3%) were included in the study. Two participants did not receive the intervention due to changes in medication and health reasons respectively. Forty-six participants completed the mindfulness intervention (weekly meetings and daily assignments) and were included in the analysis. The participant flow diagram is illustrated in Figure 1. Baseline characteristics are summarized in Table 2.
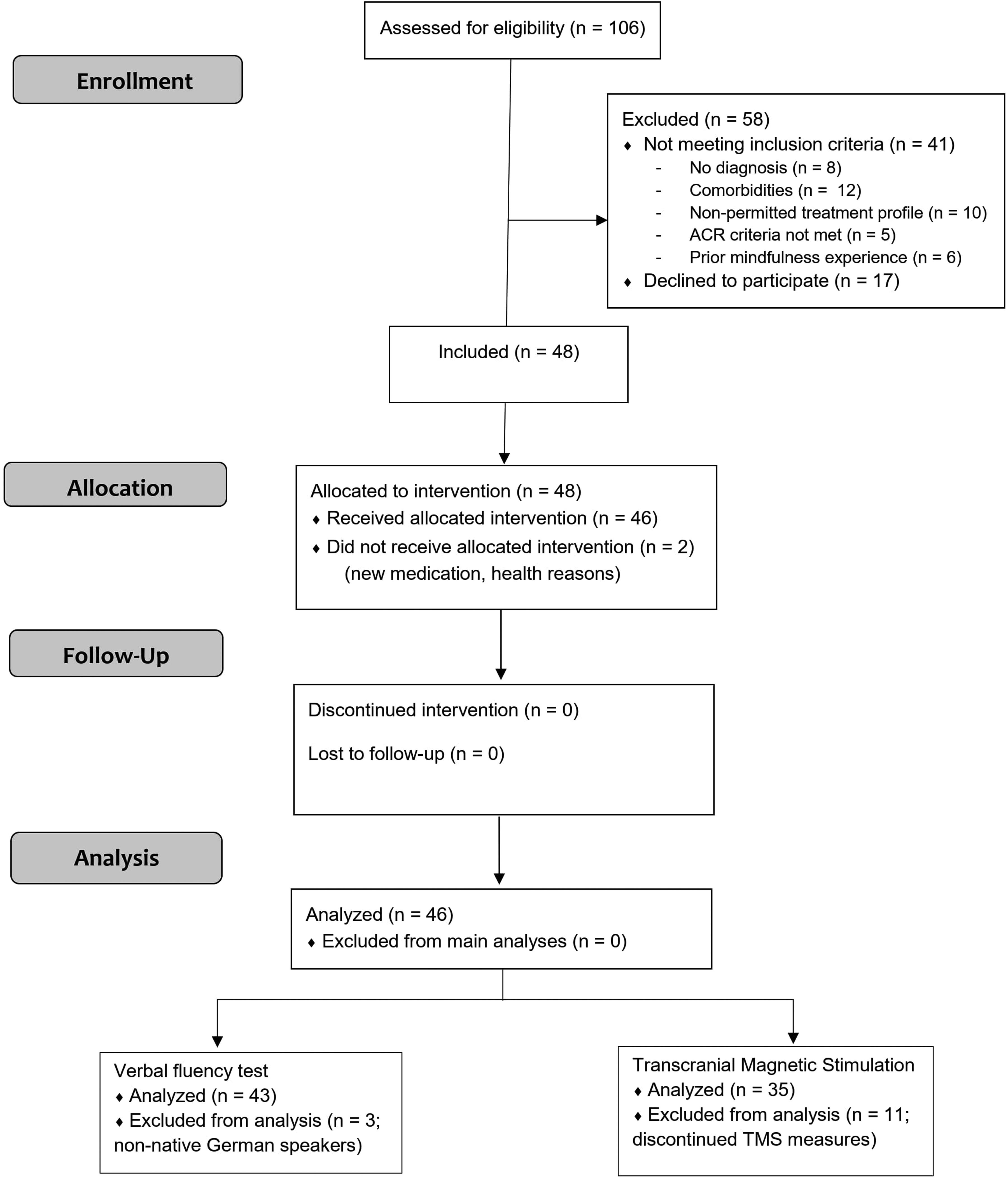
Flow diagram of the participants with fibromyalgia throughout the clinical trial.
Baseline Demographics.
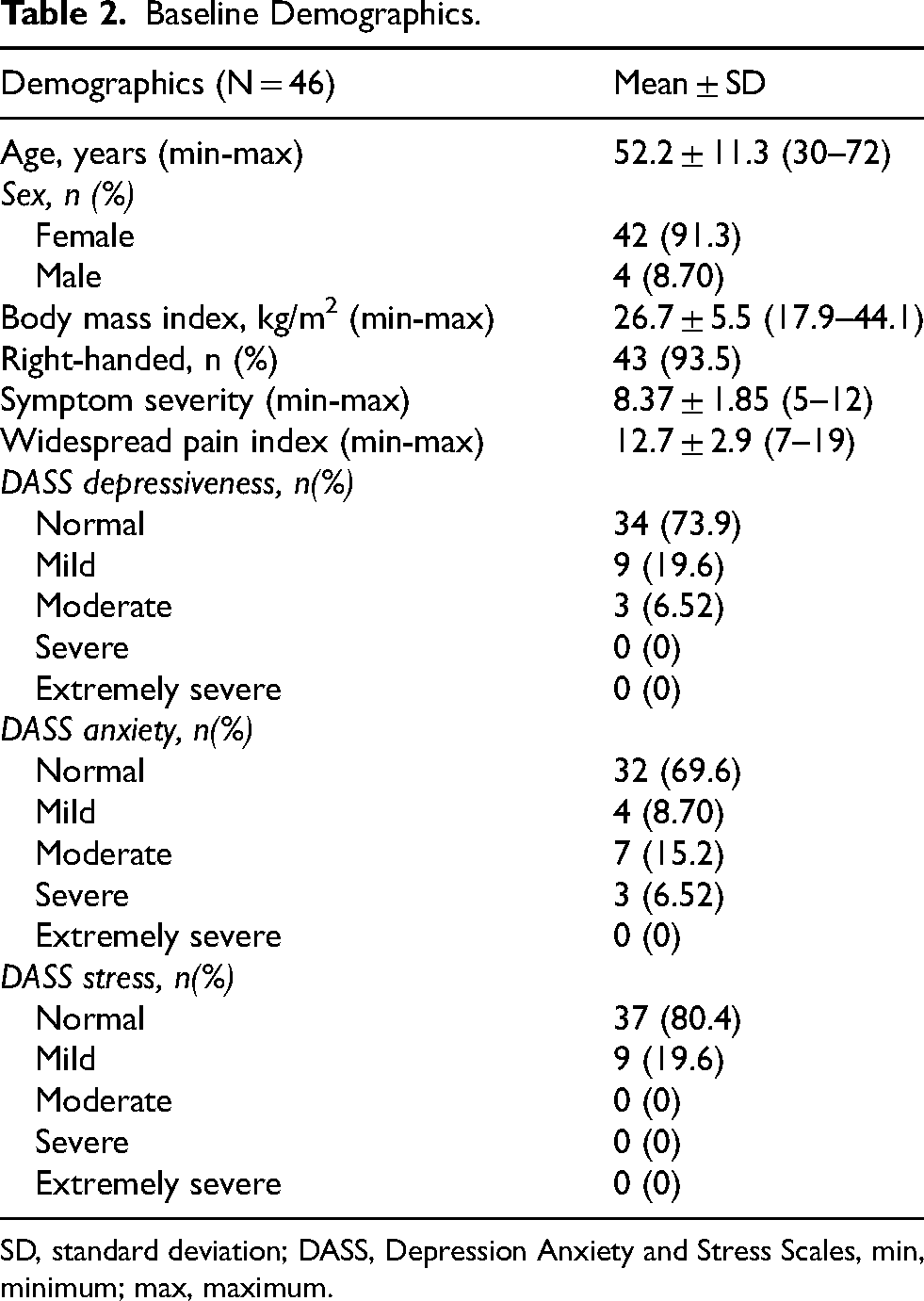
SD, standard deviation; DASS, Depression Anxiety and Stress Scales, min, minimum; max, maximum.
Primary Outcome
All participants completed the pain diary every day, and no data were missing. Participants reported a reduced NRS pain intensity at PM (x̄ ± σM = 4.87 ± 0.27) compared to BA (x̄ ± σM = 5.17 ± 0.23), with a small effect size (t(45) = −1.86, P = .035, d = 0.274). Seven out of 46 (15.3%) patients exhibited clinically meaningful pain relief.
Secondary Outcomes
We found a medium increase in QoL and a medium reduction in affective pain post-BMIF compared to BA, as summarized in Table 3. Out of the 46 patients who completed the intervention, 21 (45.6%) demonstrated a clinically relevant improvement in QoL. The overall mindfulness level and the level of each mindfulness facet also improved over time, with small to medium effect sizes. Participants showed a statistically significant improvement in resilience over time. No changes were observed in mood, psychological impairment, sleep quality, understanding, acceptance, and attention levels (Table 3). It is important to highlight that given the high number of secondary outcomes and lack of a control group, the findings can only be interpreted as exploratory at this stage.
The Effects of the Brief Mindfulness Intervention for Fibromyalgia on Secondary Outcomes.
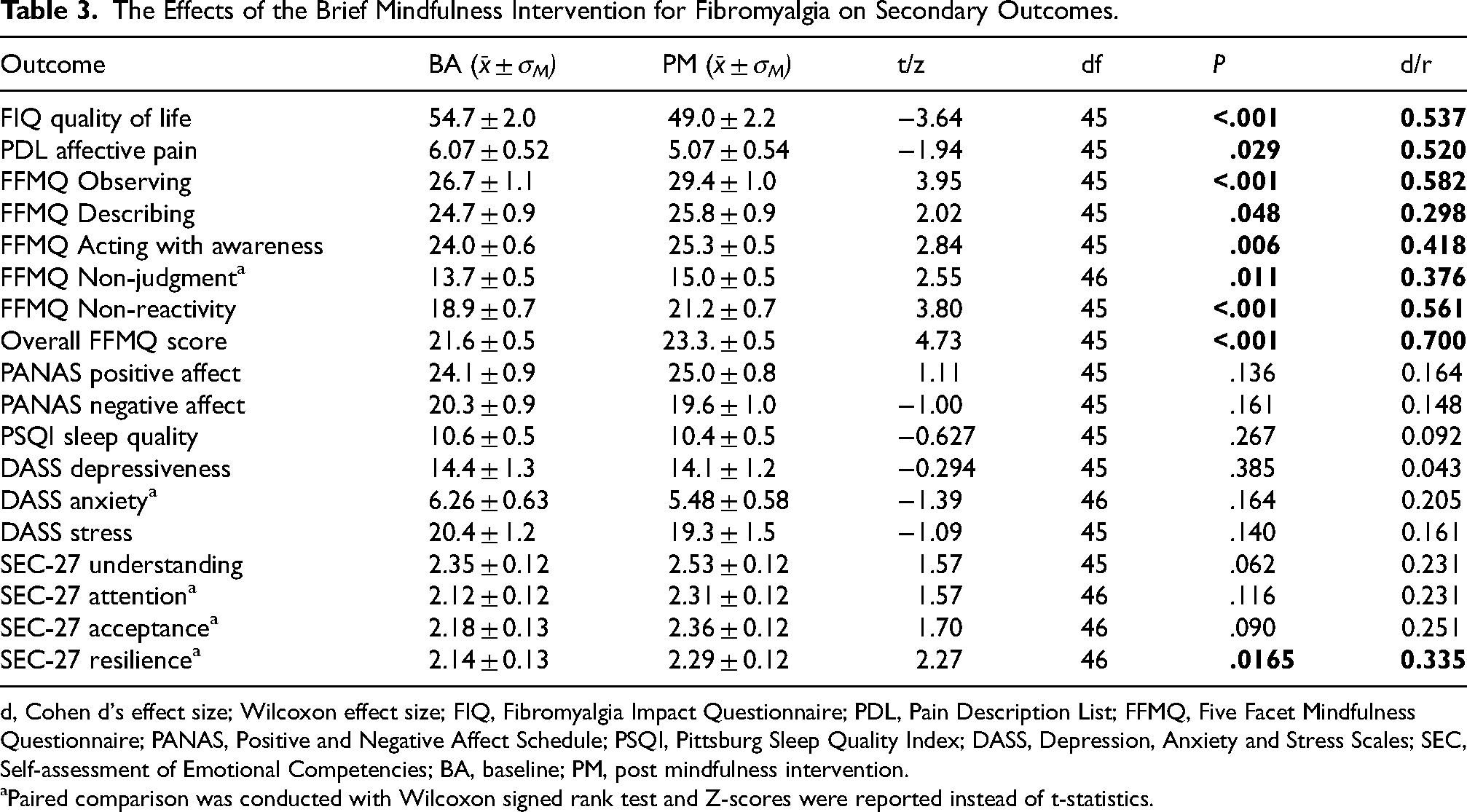
d, Cohen d's effect size; Wilcoxon effect size; FIQ, Fibromyalgia Impact Questionnaire; PDL, Pain Description List; FFMQ, Five Facet Mindfulness Questionnaire; PANAS, Positive and Negative Affect Schedule; PSQI, Pittsburg Sleep Quality Index; DASS, Depression, Anxiety and Stress Scales; SEC, Self-assessment of Emotional Competencies; BA, baseline; PM, post mindfulness intervention.
Paired comparison was conducted with Wilcoxon signed rank test and Z-scores were reported instead of t-statistics.
Verbal Fluency
Two patients, who were fluent but non-native German speakers, were excluded from the analysis of the verbal fluency test (Figure 1).
When investigating the impact of the BMIF on verbal fluency, we noted a small improvement in phonemic switching, semantic naming, and semantic switching, but not in phonemic naming (Table 4).
The Effects of the Brief Mindfulness Intervention for Fibromyalgia on Verbal Fluency.
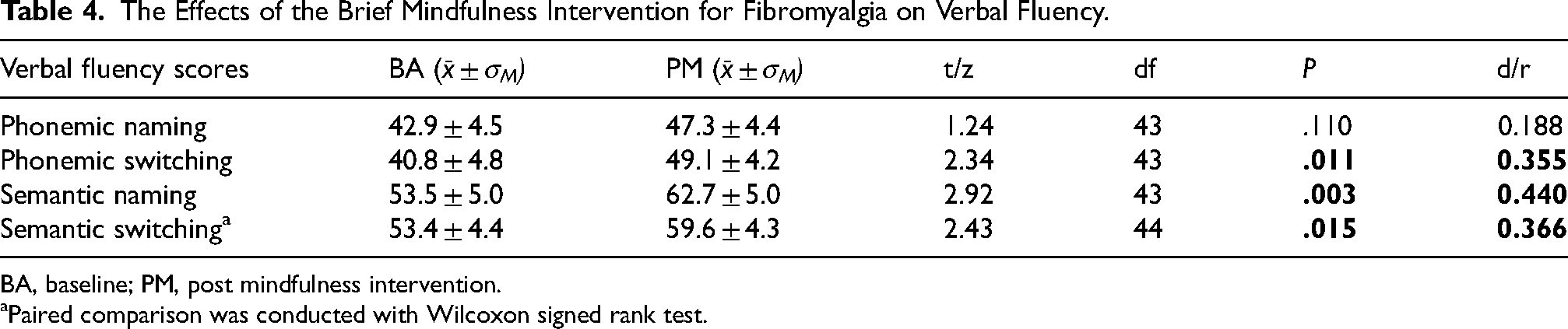
BA, baseline; PM, post mindfulness intervention.
Paired comparison was conducted with Wilcoxon signed rank test.
TMS Outcomes
Out of the 46 patients who completed the mindfulness intervention, 35 participated in the TMS experiments. Eleven patients discontinued the TMS measures after BA and were excluded from the TMS analysis (Figure 1). The reasons for the dropouts were strong headache (n = 3), dizziness (n = 1), overall discomfort (n = 3), unwillingness to receive TMS after demonstration (n = 1), whole body twitching at higher intensities (n = 1), and no MEP being observed despite hotspot being determined properly (n = 2). The SI1mV for two patients at baseline could not be determined, thus excluding them from the analysis. When analyzing the paired-pulse data, some participants showed inhibition instead of facilitation for ICF and facilitation instead of inhibition for SICI. Moreover, some participants decided to discontinue the paired-pulse session due to discomfort from stimulation at higher intensities (n = 2). These participants were excluded from the analysis, hence contributing to the inconsistency in the number of participants who completed SICI (n = 27) and ICF (n = 30). There were no serious adverse effects due to TMS.
Exploring the potential mechanistic effects of the BMIF, LICI increased significantly from BA to PM, with a small effect size (t(32) = 2.33, P = .026, d = 0.406). No significant changes were noted in the other TMS outcomes (Table 5). Given the significant attrition in the sample (between 24% to 30% dropout) and lack of statistical power for the TMS measures, the findings are only exploratory and should be interpreted with caution.
The Effects of the Brief Mindfulness Intervention for Fibromyalgia on Transcranial Magnetic Stimulation (TMS) Outcomes.
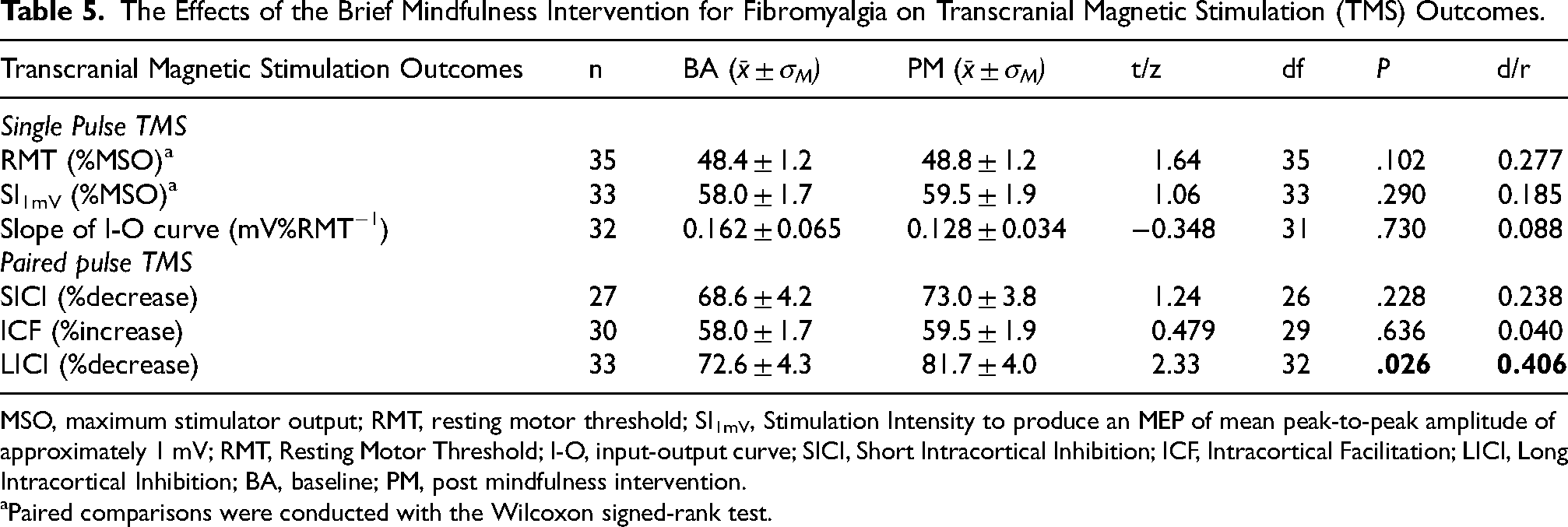
MSO, maximum stimulator output; RMT, resting motor threshold; SI1mV, Stimulation Intensity to produce an MEP of mean peak-to-peak amplitude of approximately 1 mV; RMT, Resting Motor Threshold; I-O, input-output curve; SICI, Short Intracortical Inhibition; ICF, Intracortical Facilitation; LICI, Long Intracortical Inhibition; BA, baseline; PM, post mindfulness intervention.
Paired comparisons were conducted with the Wilcoxon signed-rank test.
Feasibility
Thirty-four of the 46 participants (73.9) reported an overall feasibility score ≥ 27. Most participants agreed that the meeting contents were well-structured (x̄ = 4.82, minimum (min) = 4, maximum (max) = 5) and noted the coherence in the order of content presentation (x̄ = 4.89, min = 4, max = 5). The majority agreed that the psychoeducation part of the online sessions was helpful (x̄ = 4.62, min = 3, max = 5) and that the mindfulness facilitator was able to teach mindfulness concepts competently (x̄ = 4.96, min = 4, max = 5). Participants mostly agreed on the easiness of transfer of learned skills to their mindfulness practice (x̄ = 4.16, min = 3, max = 5) and that they were satisfied with the intervention overall (x̄ = 4.47, min = 3, max = 5). Therefore, the BMIF intervention was evaluated as a feasible MBI for FM patients.
Mindfulness Level as a Predictor of Symptom Improvement: Exploratory Subanalysis
The simple linear regressions testing whether the overall mindfulness level explained changes in outcomes indicated that the increase in mindfulness level explained 8.9% of the variation in FIQ reduction (F(1,44) = 4.32, P = .044) and 12.2% of the reduction in affective pain level (F(1,44) = 6.10, P = .017). We did not find any significant results for other outcomes— NRS pain intensity (F(1,44) = 0.554, P = .460), phonemic switching (F(1,42) = 0.292, P = .592), semantic naming (F(1,42) = 0.659, P = .422), semantic switching (F(1,42) = 0.657, P = .422), and resilience (F(1,44) = 1.15, P = .290).
Discussion
This is the first study to assess whether adding a BMIF to standard medical care and self-management benefits mindfulness-naïve patients with FM in terms of pain relief, QoL enhancement, and symptom improvement. Our results demonstrate that BMIF resulted in small- to medium-sized, yet significant reductions in pain intensity and affective pain level as well as improvements in QoL, mindfulness level, and resilience. Contrary to our expectations, no changes in sleep quality, mood, psychological well-being, and other aspects of emotional regulation were observed. Despite the statistical significance in pain intensity and QOL improvements, the minor proportion of clinical responders (15.3% for pain and 45.6% for QoL) limits the overall therapeutic impact of the BMIF in this study. Moreover, the exploratory linear regression analyses assessing the ability of mindfulness level improvement to predict better QoL and reduced pain intensity account for only a small portion of the variance (variance (R2 = 8.9–12.2%). Given the lack of a control group in the study, all the findings were only preliminary. The online implementation of the BMIF in this study was judged by the patients to be feasible, with no dropouts. Moreover, given the exclusion of patients taking more than 3 medications and some potent medication like strong opioids as well as the lower than usual rates of depression and anxiety in this sample, the study warrants that the significant findings observed in this study can only be generalized to FM patients with low to moderate severity.
Our results are partly in line with previous studies regarding the positive impact of MBIs on QoL, pain, and resilience in both healthy (Khoury et al., 2015; Marciniak et al., 2014; Sharma & Rush, 2014) and diseased populations, including chronic pain and FM (Brandel et al., 2022; Cardle et al., 2023; Dubey & Muley, 2023). Our findings are in contrast to previous studies with a limited impact of mindfulness on QoL and pain in FM (Adler-Neal & Zeidan, 2017; Davis & Zautra, 2013). While small and moderate statistically significant decreases in NRS pain intensity and FIQ scores respectively were noted, only a minority of participants reported a clinically meaningful improvement in pain (15.3% of patients) and QoL (45.6%). Therefore, the impact of the BMIF on QoL improvement and pain reduction cannot be considered clinically relevant. One inconsistency of our findings compared to previous overall positive studies is the lack of improvement in sleep, mood, and psychological impairment (Amutio et al., 2015; Cash et al., 2015b; Davis & Zautra, 2013; Goldenberg et al., 1994; Gordon et al., 2023; Pérez-Fernández et al., 2022; Sephton et al., 2007). Mindfulness practice has been shown to strongly predict stress reduction (Bartlett et al., 2021; Cardle et al., 2023; Dubey & Muley, 2023; Sousa et al., 2021; Wielgosz et al., 2019), with the relationship between mindfulness training and stress mediated by increased trait mindfulness (Baer et al., 2012). In our study, all participants had either normal (80.4%) or mild (19.6%) stress severity. It is important to note that the low levels of stress, anxiety, and depression reported at baseline in our sample are uncharacteristic of many individuals with FM and contrast with previous research (Uçar et al., 2015). The relatively low baseline of these psychological impairments in this cohort might explain the lack of changes in the level of stress, anxiety, and depression. Future studies should explore whether a patient subgroup reporting higher levels of higher emotional distress might benefit more significantly from the BMIF. Moreover, the significant increases in overall mindfulness levels and subscores as well as a majority of participants with high ratings of feasibility postulate a successful implementation of the mindfulness practice in their day-to-day life and the acquisition of meditation skills (Goldberg et al., 2016). The high variability in the outcomes across MBIs in terms of specific symptom improvement could be due to differences in the duration and intensity of mindful practice and the aspects of mindfulness, which are the focus of the intervention (Gordon et al., 2023; Leça & Tavares, 2022).
Pain perception is conceptualized in two dimensions: a sensory-discriminative dimension, relating to pain intensity, duration, and location, and an affective-motivational dimension, referring to the emotional aspects of pain such as unpleasantness, secondary pain affect, and motivating behaviors (Mory et al., 2022; Price, 2000). The affective component of pain has been shown to play a key role in the interaction between pain, sleep impairment, and mood dysfunction, hence demonstrating a stronger association than the sensory-discriminative aspect of pain (Mory et al., 2022). Previous studies have shown that MBIs, including meditation, reduced affective pain without any change in pain intensity in FM (Adler-Neal & Zeidan, 2017; Gard et al., 2012; Hilton et al., 2017; Lutz et al., 2013; Perlman et al., 2010; Zorn et al., 2020), pointing to a stronger impact of mindfulness practice on the affective rather than sensory components of pain. This is in line with our study, showing a statistically significant larger reduction in the affective pain level (medium effect) compared to NRS pain intensity (small effect). Nevertheless, given the small proportion of clinical responders to the intervention in terms of pain intensity reduction, our findings cannot confirm the definite analgesic potential of the MBI despite the statistical significance.
One of the disabilities typically reported by FM patients (75–85%) is impaired word retrieval, also known as word finding (Cherry et al., 2009; Glass, 2009; Leavitt et al., 2002). Zeidan et al. (2010) demonstrated an increase in verbal fluency ability in young healthy participants following a four-day mindfulness training compared to a placebo. Mindfulness training also improved word recall in semantic and lexical fluency ability compared to the control group in healthy individuals (Heeren et al., 2009). Similar improvements were observed in the elderly and patients suffering from neurodegenerative diseases (Marciniak et al., 2014). Our study was the first investigation on the effects of mindfulness on verbal fluency in FM. Despite the observed improvements in phonemic switching, semantic naming, and semantic switching performances supporting prior studies, the potential for practice/learning effects is acknowledged, particularly given the same test was used at BA and PM. In healthy individuals, the practice effects of verbal fluency have been shown to range from small to strong effects, lasting from one week to three months (Bartels et al., 2010; Basso et al., 1999; Zgaljardic & Benedict, 2001). The practice effects of the Regensburg verbal fluency test have not been yet investigated in FM patients. However, practice effects have been previously reported to be smaller in cognitively impaired individuals than in healthy ones (Jutten et al., 2020; Weingartner et al., 1993; Wilson et al., 2000). Future studies could consider incorporating a ‘dual-baseline’ approach could be implemented to reduce early practice effects, which implies that the test is repeated twice before starting intervention and the second time point is taken as baseline (Bartels et al., 2010; McCaffrey & Westervelt, 1995; McCaffrey et al., 2000).
During our exploration of the neurophysiological impacts of the BMIF on participants using TMS, we observed a notable increase in long-interval intracortical inhibition (LICI). However, its clinical relevance should be cautiously interpreted. Moreover, the significant sample attrition and small sample size for TMS outcomes limits the power and reliability of these mechanistic interpretations. Previous studies implied that the reduced intracortical inhibition in FM has been mainly attributed to changes in SICI, a marker for GABAAergic inhibition (Cardinal et al., 2019; Mhalla et al., 2010; Molero-Chamizo et al., 2023; Pacheco-Barrios et al., 2022). There are discrepancies in the alterations in the glutamatergic excitatory pathways, as measured by ICF (Cardinal et al., 2019; Mhalla et al., 2010). The restored intracortical inhibition following therapeutic interventions in FM could be mediated by a restoration of the dysfunctional descending pain modulatory system (Molero-Chamizo et al., 2023). The increase in LICI observed in our study following the MBI, if replicated in larger sample with a control group, might suggest enhanced GABAB-mediated cortical inhibition among participants (McDonnell et al., 2006). Guglietti et al. (2013) previously noted an increase in cortical silent periods post-meditation, which is also a measure of GABAB-modulated cortical inhibition. Moreover, Guglietti et al. (2013) have specifically demonstrated that meditation can lead to improvements in cognitive functions and emotional regulation. The observed improvements in mindfulness, resilience, and aspects of verbal fluency in our study suggest potential cognitive benefits. However, given the complexity of these neurocognitive processes and the absence of significant changes in mood, psychological impairment, and other measured factors, the direct impact on cognitive performance and emotional regulation remains speculative. Thus, we cautiously interpret these results as preliminary evidence.
Our preliminary findings must be considered in light of the study's limitations. Despite a powered sample, we used a single-arm design without follow-ups, inherently limiting causal inference. The observed variability in the baseline characteristics among the participants could have also influenced the outcomes. While the included sample size was powered for the primary outcome, another limitation of the study was the inadequate statistical power for many secondary and TMS outcomes. FM is known to have a high intra-variability in flare-up symptoms, both in intensity and temporally, with the degree of symptom impact fluctuating over time (Fitzmaurice et al., 2024). Therefore, a control group for the BMIF, such as a group receiving treatment-as-usual, would be necessary to allow us to attribute the observed changes solely to the intervention. This would also reduce the vulnerability of the finding to placebo effects, regression to the mean as well as nonspecific therapeutic factors, such as social support from weekly group sessions. Furthermore, the sample comprised mostly of women (91.3%), limiting the external validity of the findings to the general FM population. Nevertheless, it is important to highlight that FM has been shown to be three times for prevalent in women than in men (Sarzi-Puttini et al., 2020). Another limitation was the short follow-up post-intervention. However, already after four weeks, relevant changes were seen, making it feasible for relative comparisons of combination therapies. In this study, a significant dropout rate of 25% to 30% was observed during the TMS procedures, primarily due to adverse effects such as headache, dizziness, and general discomfort. This higher-than-expected dropout rate due to adverse effects is higher than those typically reported in patients with depression (3.2%) and other psychotic conditions (2.3%) receiving TMS treatment (Zis et al., 2020). The elevated dropout rate in our study may be attributed to the specific characteristics of our sample, comprising FM patients. These individuals may exhibit heightened sensitivity to discomfort due to underlying factors such as central sensitization, which can amplify pain perceptions and discomfort. Future research that aims to use this cohort could benefit from modified TMS protocols better suited to the sensitivities of fibromyalgia patients, along with the incorporation of desensitization sessions to improve tolerability for FM patients. These sessions could help minimize reactivity to the sensations of TMS by alleviating initial discomfort and anxiety associated with the procedure. Also, the treatment profile of each participant was different from the other, owing to the heterogeneity of FM symptoms. Participants were permitted to continue their medication as withdrawal in FM studies poses challenges and would lead to bias in including participants. Recently, it was found that the expectations, motivations, and beliefs of participants have been shown to play a greater role in reducing acute pain in naïve meditators after brief MBIs than the actual mindfulness process itself (Davies et al., 2022; Perez-Aranda et al., 2019). Future studies must also include these measures to better understand the therapeutic effects of MBIs in chronic pain patients.
Despite the statistical significance for pain reduction, quality of life improvement, as well as improvements in secondary outcomes, the lack of clinical relevance and the current single-arm open-label investigation render the therapeutic potential of a four-week brief MBI inconclusive. Future sham-controlled blinded randomized clinical trials with a larger sample size and longer follow-up time points are required to validate the therapeutic efficacy of the BMIF in patients with FM as well as to better understand the underlying mechanisms.
Footnotes
Acknowledgments
The authors acknowledge all the patients who took part in this clinical trial. We are thankful to the patient self-help groups: the Deutsche Fibromyalgie Vereinigung and Deutsche Rheuma-Liga for supporting our study and promoting it within their groups. We further acknowledge the support by the Open Access Publication Funds of the Göttingen University. We also express our gratitude to David Johannes Conrad for conducting the language proofreading of the manuscript. In addition, PR was funded by the International Max Planck Research School for Neurosciences at the Georg August University, Göttingen, and the Studienstiftung des deutschen Volkes.
Ethical Considerations
Not applicable.
Consent to Participate
All participants were required to sign an informed consent form.
Consent for Publication
Not applicable.
Author Contributions
Design of study: PR, OLGA, FP, AA; Design and development of Brief Mindfulness Intervention for Fibromyalgia: OLGA, PR, FP; Translation of mindfulness instructions from English to German: SES; LCH; Data collection: PR, TTM, LCH, EF, SES, AL, YG, and XG. Conducting mindfulness classes in German: SES, LCH; Medical assistance to participants during the study: FP; Development of the TMS data processor: OM, TTM, PR; Data analysis: PR; Writing the manuscript: PR; Data interpretation: PR, OLGA; Reviewed the manuscript: OLGA, XG, YJ, AL, FP, AA; Supervision of study: AA, OLGA.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PR has received fees for teaching by Neurocare (Germany) and non-financial support from Sooma (Helsinki). AA is a vice president of the European Society for Brain Stimulation, Member-at-Large at the EMEAC – IFCN; Member of the safety or advisory boards: Boss-Stroke, Brady, Brainn, MemoSlap, GifteD, DisCoVer, PlatoScience; Paid consultant at NeuroConn, Ilmenau, and she is a paid advisor at Electromedical Products International (Pulvinar), USA. Member of the advisory board at PlatoScience; Paid Editor by Elsevier, AA is supported by the DFG (AN 687/9-1), EU-Horizon 2020 (PAINLESS, No. 101057367), BMBF (NEURO VR-Plus 16SV9248), DAAD-PPP (57702891). The other authors do not have any conflicts of interest to declare.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
{kind=link}
{kind=link}