
Abstract
This article examines the medical front of the anti-narcotics war in post-war Hong Kong. Situating Hong Kong in the American global drug war, this article traces colonial Hong Kong’s development of addiction treatment and cooperation with American medical experts in conducting a controversial experiment, methadone maintenance. It argues that the colonial government constructed a new form of therapeutic governance to medicalize social issues as behavioural problems. Through large-scale rehabilitation and methadone maintenance, the colonial government claimed to transform addicts in the island colony into useful subjects and justified its radical intervention into social life. To American experts, Hong Kong was an ideal laboratory to examine the controversial treatment. Hong Kong’s methadone experiment became an international success and a model reimported into the United States in the 1980s. A medical history of the anti-narcotics war not only offers a new way to reassess the social reform in the 1970s but also helps us understand the contemporary hard-line approach against drugs in Hong Kong and post-colonial Asia.
Keywords
The mid-20th century witnessed a transition from opium monopoly to full prohibition in the British Empire. Under the American influence on policing the global narcotics traffic, the British Empire reluctantly gave up its interest in the opium trade. The colonial legacies of opium monopoly left a daunting task for colonies: a considerable number of people who depended on opium became addicts, the medical infrastructure to provide treatment was insufficient, and an effective cure for opium addiction was lacking. 1 Meanwhile, the opium addicts shifted to heroin as a substitute and ‘chased the dragon’ (追龍), a common method of smoking crude heroin which emerged in Hong Kong and spread to Southeast Asia in the 1960s. 2 Through the case study of Hong Kong, this article focuses on the understudied episode of how the colonial and post-colonial states dealt with the legacies of opium monopoly: an expanding population of addicts that consumed a much stronger drug, that is, heroin. To handle escalating drug-related crime rates, the Hong Kong colonial government launched an anti-narcotics war in 1959, emphasizing not only anti-drug trafficking measures but also treatment to transform the addicts into useful citizens. This study shows why and how Hong Kong addiction treatment programmes played an important role in the colonial history of drugs, as well as in the remaking of state–society relations in colonial Hong Kong.
This article fills a critical gap in the colonial history of drugs. In the past few decades, historians convincingly showed that drugs were central to colonial expansion. 3 The existing literature of the post-World War II period places much emphasis on the American global policing regime in regulating the narcotics trade, 4 but less is known about the emergence of addiction treatment and management of drug addicts in colonial and post-colonial states. 5 Hong Kong was no exception. It came under the close scrutiny of the United States from the late 1950s onwards when Hong Kong became a global manufacturer of drugs. To contain the global narcotics trade, the United States increasingly intervened in Hong Kong’s approach towards drug trafficking and treatment. 6 Hong Kong’s addiction treatment programmes have been widely acclaimed by international experts. 7 This article discusses how the Hong Kong government experimented with large-scale rehabilitative programmes to ‘cure’ its addicts from 1959 onwards. American experts were invited to supervise experiments involving methadone maintenance in the 1970s. The cooperation was mutually beneficial: American supervisors used Hong Kong as a laboratory, gathered data to alleviate domestic concerns, and reimported the ‘Hong Kong model’ back to the United States, while the colonial state sought for an effective treatment to manage the population. Through addiction treatment, the colonial state could redraw the boundaries between legitimate and illegitimate forms of drug consumption. This study contributes to the understudied field of drug addiction and explains the hard-line approach against drugs in post-colonial Asia.
A critical examination of the history of drugs also contributes to the debate on the state–society relationship in post-war Hong Kong. Unlike earlier scholarship that stressed on the stereotype of positive non-intervention in post-war Hong Kong, historians have examined recently declassified archives and revealed the colonial state’s explicit and implicit intervention, such as monitoring public opinion, censoring publications and movies, and combating corruption. These measures were often aligned with the large-scale social reforms on housing, medicine, and social services in the late 1960s and 1970s to add credibility to colonial governance as well as to function as a bargaining chip in negotiations with China about the handover. 8 This study joins the ongoing discussion about social welfare and argues that the colonial government constructed a new form of therapeutic governance by launching the anti-narcotics war and medicalizing addiction as a mental health problem. The colonial state, once an advocate of the opium trade, rebranded itself as a protector of citizens by curing and transforming addicts into useful and productive subjects. Ultimately, rehabilitation and methadone maintenance became useful tools for the colonial state to tame and control addicts in the name of social welfare, giving the government power to aggressively intervene into social life. The blurred boundaries between welfare and control raise important questions about the colonial legacies of social reform in the 1970s, often remembered as the Golden Era of Hong Kong. The case of addiction treatment thus sheds new light on the state–society relationship in which a therapeutic form of governance emerged to medicalize social issues and thus justify the state’s tightening control over undesirable population groups.
The rise of heroin addiction
With the British Occupation in 1841, Hong Kong became a free port for distributing and selling Indian opium to China. To raise revenue and maintain competition between merchants, the colonial government developed an opium monopoly by granting the licence to the highest bidder to sell a small amount of opium in Hong Kong. 9 Opium revenue accounted for around 30 per cent of Hong Kong’s total revenue in the 1910s and 20 per cent in the 1920s, sitting at the heart of the colonial regime. 10 Undoubtedly, commercial interests drew the boundaries between legal and illegal drugs. Before 1948, the Dangerous Drugs Ordinance in Hong Kong only targeted controlling the distribution and sale of morphine, heroin, cocaine, and medical opium. The principle of legislation was to prohibit drugs that threatened government opium revenues and yet establish a moral ground for the colonial government to proclaim protection of the community. 11 In this sense, the meanings of dangerous drugs rested in commercial interests but not the side-effects of the substances. People who purchased opium were consumers, not addicts.
The end of World War II marked a turning point in the global opium trade. From the 1910s onwards, the American government attempted to implement the full prohibition of opium out of domestic concerns and economic interests. 12 European colonial powers insisted that opium monopoly served as an effective mechanism to prevent illicit traffic and that it reduced consumption. At the end of World War II, the United States became a global leading power and made the total prohibition of opium possible. In September 1943, Britain decided to fully prohibit opium in Asia, except for India. To London, opium prohibition was a strategic move. First, it could appease American public opinion and avoid angering the American government. Second, Japanese occupation of colonial territories removed administrative difficulties of prohibition. Eventually, sacrificing opium interests could stop the United States from extending the prohibition to India. Opium banning thus was a diplomatic decision in which British foreign policy goals outweighed fiscal benefits and administrative concerns. 13 In the case of Hong Kong, the post-war power vacuum was a timely opportunity for the Colonial Office to bypass the Hong Kong government for consultation. In 1945, Hong Kong banned opium under Proclamation 13 of the British Military Administration. 14
Since then, the colonial government unwillingly adopted a punitive approach toward drugs, at least in theory. When the British re-established rule in 1948, prepared opium was reclassified as a dangerous drug. Hong Kong implemented a restrictive policy that banned the sale and distribution of all drugs that were dangerous to the public. 15 Nonetheless, in the belief that eradicating opium smoking was impossible, the Colonial Office and Hong Kong government remained pragmatic towards anti-drug measures. In 1945, the Colonial Office already foresaw the problem of drug addiction because there was no cure for long-term opium consumers, who became addicts. The Colonial Office viewed the American approach of forcing addicts into treatment as impractical and decided to supply addicts a prepared form of opium in Malaya, Hong Kong, and Borneo. 16 As a result, the Hong Kong government did not provide any rehabilitative treatment in the early and mid-1950s when Hong Kong suffered from other problems, such as post-war reconstruction, influx of refugees, lack of medical infrastructure, and crisis in the provision of housing, food, and water. 17 Simply put, the colonial government had no incentive to invest in a ‘war on drugs’ before the late 1950s.
Nonetheless, Britain paid close attention to the drug problem in Hong Kong in the 1950s largely due to pressure from the Americans. Harry Anslinger, the first commissioner of the United States Federal Bureau of Narcotics, was empathetic with the Nationalist Government in Taiwan and constantly accused the People’s Republic of China (PRC) of using Hong Kong to smuggle heroin to the United States. Even Anslinger’s colleagues discredited his erroneous claim and suggested that there was little evidence to prove communist China’s involvement in the global narcotics trade. Still, the anti-communist conspiracy theory put Hong Kong under the spotlight. 18 In 1954, when Anslinger learned about Hong Kong’s good anti-narcotics record, he eventually dropped his attack on Hong Kong and diverted his attention to domestic issues. 19 To avoid weakening its political ties with the PRC and not provoke the United States, Britain did not overlook the drug problem in Hong Kong during the 1950s. 20
It was only in 1957 that heroin offences in Hong Kong alarmed the high officials in London. According to government statistics, the cases of heroin offences increased from 400 in 1952 to 12,791 in 1956, and opium offences remained stable at the level of 4906 in 1956. 21 In 1957, Secretary of State for the Colonies Alan Lennox-Boyd, after reading the statistics from Hong Kong, drew attention to the skyrocketing rise in the number of people committed to prison for drug offences. He then recommended that the colonial government learn about the addiction treatment in Singapore and to investigate the drug scene in Hong Kong. 22 Brian C. K. Hawkins, Hong Kong Secretary for Chinese Affairs, initiated a personal investigation of the drug problem and submitted a secret report to the Colonial Secretary in May 1957. He concluded that heroin addiction had become ‘a problem of almost desperate urgency which must be tackled with utmost energy and resource’. 23 However, his focus was heroin, not opium. He admitted that opium was deeply rooted in the colony’s past and would not regard the increase in opium smoking with any great alarm. More importantly, Hong Kong became an international entrepôt and manufacturer of heroin to Japan, Canada, and the United States. Hawkins argued that if the use of heroin continued to grow, the number of addicts, roughly 30,000 estimated by the police would double in two to three years. 24 Heroin posed a grave threat to the local community as well as the international reputation of Hong Kong.
Hawkins’s report should be understood against the broader changes in the 1950s that made Hong Kong an ideal place for the global narcotics traffic. First, many Hong Kong colonial officials associated heroin crime with opium prohibition. They expressed their discontent bluntly, arguing that ‘we made opium-making so difficult and expensive that the lower-class addicts were forced onto heroin’. 25 To both drug dealers and consumers, heroin was smaller in size, odourless when consuming, and easier to transport. 26 Second, members of the Green Gang and the Chiu Chau, the major triad societies in Shanghai, escaped to Hong Kong, turned the colony into Asia’s heroin laboratory, and blended Hong Kong into Southeast Asia’s Golden Triangular Trade in the 1950s and 1960s. They refined opium from Burma, Thailand, and Laos into higher-quality heroin, which would eventually reach North America. 27 Third, despite the outbreak of the Korean War and the American embargo on Hong Kong, the colony remained a free port for the flow of commodities and tourists. The colony developed into a regional air hub, manufacturing centre, and export hub in the late 1950s. 28 These three factors turned Hong Kong into a hub for the global narcotics traffic and led to the surge in heroin offences.
The colonial government followed up the Hawkins report immediately. In 1957, an Ad Hoc Narcotics Committee was formed under the chairmanship of John C. McDouall, the new Secretary for Chinese Affairs. The Committee submitted a new report that substantiated Hawkins’s private investigation with statistical evidence and recommended addressing drug problems on four fronts: (1) trafficking, (2) legislation, (3) treatment of addiction, and (4) publicity. 29 The Hawkins and McDouall reports, approved by the Colonial Office, set up the framework for the anti-narcotics war in the following years. On 11 November 1959, the colonial government tabled a White Paper entitled ‘The Problem of Narcotic Drugs in Hong Kong’ in the Legislative Council. Later, Sir Robert Black, the Governor of Hong Kong, appointed a Narcotics Advisory Committee headed by the Secretary for Chinese Affairs. The committee served as an advisory body to coordinate different departments, such as the Narcotics Bureau under the Hong Kong Police Force on suppressing trafficking, and the Prison Department and Medical and Health Services Department on addiction treatment. 30
Declaring a war on drugs
The colonial government was fully aware of the importance and repercussion of soliciting public support. The Hawkins report eloquently stated that the government should appeal to the Chinese community, learn the communist technique of ‘repeating and repeating facts and exhortations day after day and year after year’, and convey the message in a simple language but never let up. The anti-narcotics war was supposed to make the people realize that the government was trying to protect their homes, lives, and children from the terrible menace of drugs. However, Hawkins was conscious of the possible repercussions of a high-profile campaign. He made it clear that ‘there is one obvious drawback to this scheme . . . it cannot be done quietly. We have got to be prepared to wash our dirty linen in public, to state the unpleasant truth without excuses and to accept any odium which this may bring us.’ 31 Put differently, launching an anti-narcotics war was a double-edged sword: repositioning the role of the state to justify its intervention but at the same time holding the government accountable for its failure and subsequent criticisms.
Declaring a drug war imposed a moral responsibility on the colonial government to offer treatment, a decision that appeared to be uncertain and costly at the time. Addiction treatment was not easy due to its practical and financial difficulties. Practically, official hesitation about treatment was evident in planning the anti-narcotics campaign. They debated about postponing treatment programmes with concern about lack of rooms to accommodate large numbers of addicts, patients’ unwillingness to submit themselves to prisons or treatment centres, and bad publicity if the experiment failed. 32 Even in the United States, effective addiction treatment was absent in the early 1960s. 33 Financially, the cost for addiction treatment was considerable. The McDouall report explicitly stated that the minimum costs of the treatment programme was ‘unpredictable’ since rehabilitation involved not only the addicts’ drug withdrawal, but also material support to their family and aftercare for the patients. 34
So, why and how did the colonial government invest in a costly campaign in addiction treatment when results were uncertain? The anti-narcotics war was part of the broader shift of colonial welfare policies from laissez-faire to the integration of refugees. In the early 1950s, the colonial government perceived the refugee crisis as a Chinese problem but not a colonial responsibility. Large-scale relief would only attract more refugees to Hong Kong. Due to inadequate social services and failure in refugee resettlement, the 1956 Riots broke out and escalated into clashes between the Nationalists and Communists. By late 1956, the colonial government recognized the refugee issue as a ‘problem of people’ with serious impact on the colony’s stability. More importantly, Hong Kong shifted from an entrepôt economy to an export-oriented and labour-intensive industrial economy in the late 1950s. For economic purposes, the colonial government was willing and financially able to invest in social welfare. 35 When planning the development of medical services in 1963, the Medical Department noted that ‘a good general standard of health throughout a community is an economic asset . . . particularly in a free enterprise economy’. 36 In this sense, the provision of basic welfare and medical care involved political and economic considerations. As shown in the later sections, the purpose of addiction treatment was to integrate troublemakers into the social fabric of the colony and make them productive and responsible citizens.
The inclusion of addiction treatment in the anti-narcotics war was also a response to the growing public demand, largely from missionaries and political parties. Missionaries who relocated to Hong Kong from mainland China began to offer withdrawal treatment to Chinese refugees in the 1950s. For instance, the Christian Addiction Hospital (仁愛戒煙醫院) in 1956 and Sunshine Island (日光島) operated by British missionaries in 1957 offered voluntary treatment. Emerging political parties campaigned against the government on different social issues. In 1958, the Reform Club of Hong Kong (香港革新會) conducted an investigation about the drug problem in Hong Kong and submitted a report to the government, urging for the provision of addiction treatment and a more comprehensive anti-narcotics campaign. 37 These groups formulated and shaped public opinion regarding addiction treatment in the late 1950s, followed by increasing media coverage of addicts’ stories and numerous public letters about the drug problem in Hong Kong.
Meanwhile, addiction treatment carried considerable propaganda value for the colonial government. In investigating the drug problem in 1958, McDouall was in line with Hawkins and fully aware of the propaganda potential of providing treatment. Contrary to the bureaucratic logic that understood addiction treatment in terms of expense and efficiency, the McDouall report suggested that the cost of the treatment centre should be measured in terms of ‘its usefulness in further swinging the local population behind Government by meeting an already widespread and popular demand in connection with the fight against drugs’. To McDouall, the propaganda value outweighed its effectiveness in reducing the numbers of addicts. ‘Winning the backing of the people of Hong Kong’ was the prime priority of the anti-narcotics war. 38
The White Paper carefully crafted images of addicts to convince the public that the government was protecting them from drug addiction. Unlike the earlier government approach to conceal information related to drugs, the White Paper publicized government data and portrayed drug trafficking and addiction as a problem that gravely threatened social stability. It presented a horrifying drug scene based on statistics from prisons that between 1955 and June 1959, addicts accounted for 50,733 out of 89,338 prisoners, with 67 per cent consuming heroin and the rest taking opium. 39 It then analysed the causes and consequences of addiction. Most often, addicts, largely underprivileged manual workers, sought to take heroin as a replacement for opium to relax and reduce tension from tedious work and boost sexual performance. The White Paper included photos of addicts to depict the terrible consequences of opium and heroin addiction. For example, a middle-aged man, all skin and bones, was said to be going through a ‘living death’ due to heroin addiction (Figure 1). Another photo showed a woman chasing the dragon in search of a world that was free of squalour and worry (Figure 2). Typically, under the colonial gaze, the addicts were victims unaware of and uneducated about the consequences of heroin, lured by gangsters, slaves to drugs that would make them potential criminals, which destroyed their lives and families, and who would eventually die from the craving for drugs. Narcotics meant death. Addiction treatment, as a result, gave the addicts an opportunity of cure to redeem them from their vice. 40 By weaving different stereotypes about addicts, the colonial government repositioned itself to protect citizens from the vice of drugs. The propaganda delivered a clear message: consumption of opium and heroin led to addiction; addiction was an illness that warranted medical intervention. 41
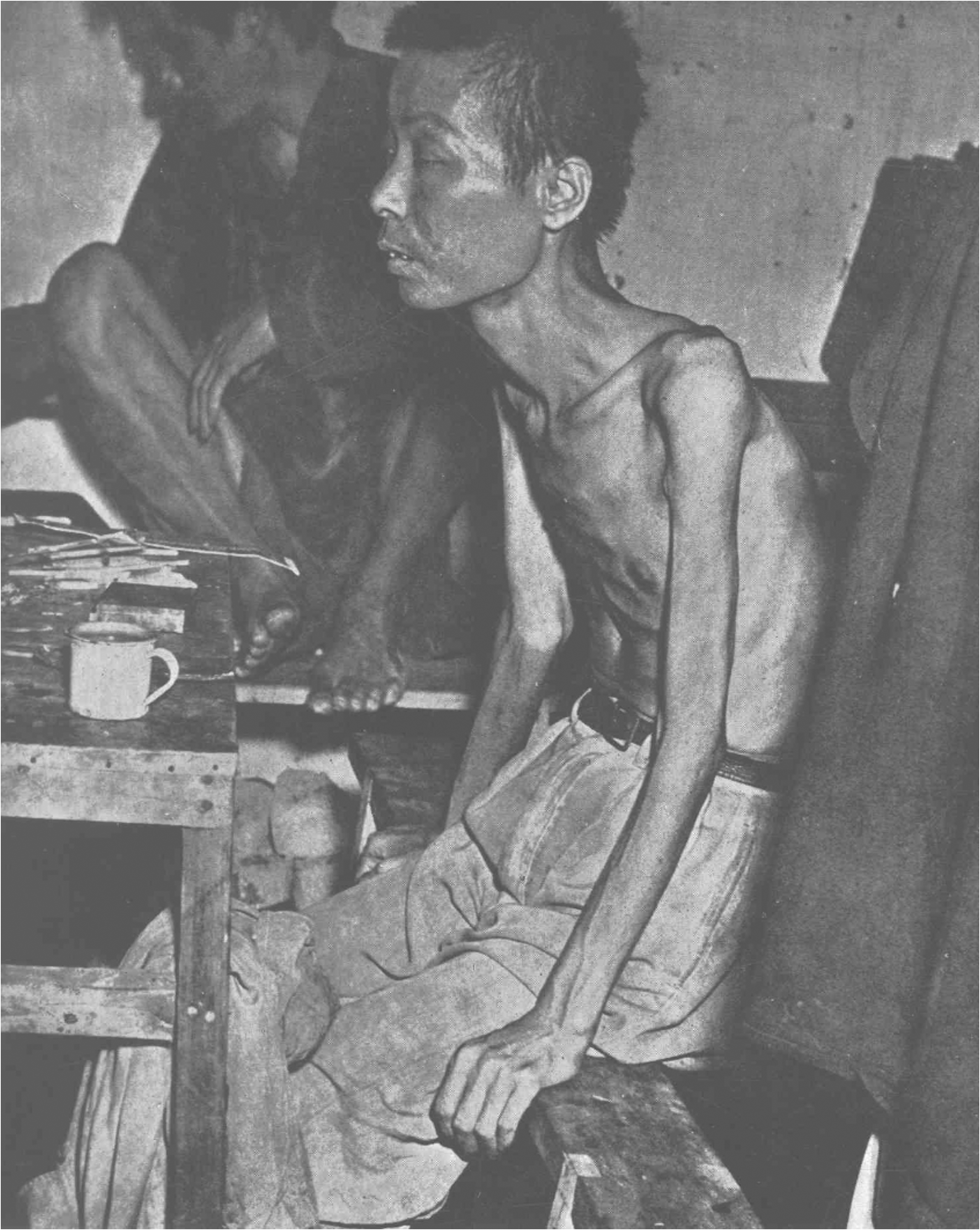
Photo of an addict published in the White Paper.
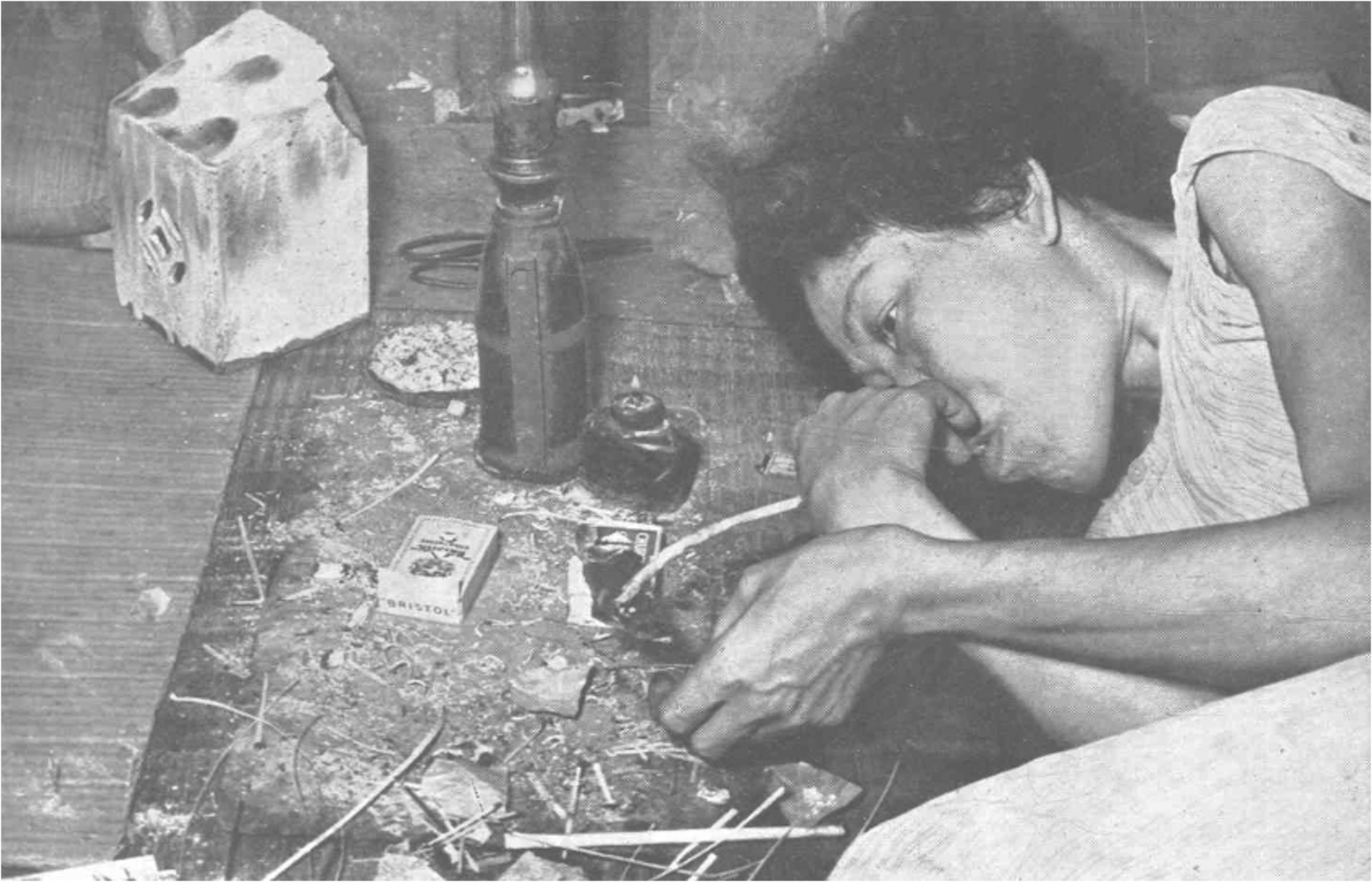
Photo of a heroin addict.
Since 1959, the colonial government has taken a hard-line approach against all drugs. In the official rhetoric, drugs, including opium and heroin, were associated with crime, triad societies, immorality, and illness. Opium addicts would quickly turn to heroin and become heroin addicts. Once afflicted with addiction, addicts were equal to social outcasts and parasites, threatening the stability of Hong Kong. 42 The colonial government also implemented a new Dangerous Drugs Ordinance in 1969 to classify the types of drug offences, from trafficking to manufacturing and possession of dangerous drugs. The ordinance lumped opium and heroin together, along with other stimulants, such as cocaine and marijuana, even though these substances did not produce symptoms associated with heroin addiction. 43 Drug laws in Hong Kong did not distinguish between soft drugs and hard drugs, neither did they take into account the relative dangers of drugs. Unlawful possession of heroin and cannabis might result in a similar penalty with a maximum of three years’ imprisonment and a HK$10,000 fine. 44
However, the government’s hard-line stance, at least in the 1950s and 1960s, was not well received by the public. The government closely cooperated with the various Chinese communities and set up the Narcotics Advisory Committee in 1959, which consisted of seven Chinese tycoons and two members of the Executive and Legislative Councils. The selection of Chinese elites was a deliberate move to solicit public support and mobilize the masses against narcotics by circulating propaganda against heroin, in the form of slogan and essay competitions, leaflets, posters, radio, television, cinema, and lectures. 45 Yet, the propaganda did not enjoy great success. The report by the Advisory Committee in 1965 highlighted how Hong Kong suffered from ‘a large measure of public apathy towards the social, economic, and moral dangers of a creeping tide of drug addiction’. 46 The public’s indifference was not surprising. The colonial government was dealing with a century-long history of opium smoking, coupled with prevalent corruption between drug syndicates and police. For instance, social activist Elsie Elliot described 1960s Hong Kong as a ‘criminal paradise’ where the police were involved in the drug trade. The close relationship between drug trafficking and police corruption was an open secret. 47 The following section examines another problem faced by the colonial government: how to define and cure addiction.
Medicalizing addiction: Rehabilitation and personality change
Medicalization of addiction, a key element in the anti-narcotics war, was deeply associated with psychiatry dating from the 1950s. The White Paper defined addiction as ‘a medical question in the first place; at a later stage, it becomes a matter of psychological readjustment and social rehabilitation’. 48 David J. M. Mackenzie, Director of Medical and Health Services in 1959, commented that addiction was essentially ‘a problem of mental health . . . an indication that the individual concerned has broken down mentally under conditions of environmental stress including physical ill health’. 49 Such emphasis on mental health reflects the Anglo-American trend in medicine where psychiatrists have played a key role in policymaking and research of drug addiction since the 1960s. At the same time, psychiatrists were more closely associated with social control and confined patients suffering from alcoholism for a short period in an institutional setting. 50 Viewing addiction as a mental health problem, the Hong Kong colonial government assigned psychiatrists as the chief advisors in the early anti-narcotics campaign. Medicalizing addiction as a mental health problem laid the theoretical ground for the government to cure and ‘transform’ the addicts into useful citizens.
The colonial government proposed two rehabilitative schemes. The first scheme was a special prison to provide compulsory treatment for prisoners (with sentences between 6 and 12 months) in Tai Lam. Located next to the Castle Peak Mental Hospital, Tai Lam Prison began to experiment with addiction treatment for prisoners from 1958 onwards. The second scheme was a Treatment Centre in the Castle Peak Mental Hospital that offered occupational therapy and treatment regime, targeting voluntary patients with no criminal records. 51 Voluntary organizations also played a crucial role in providing treatment. The key rehabilitation programme was run by the Society for the Aid and Rehabilitation of Drug Addicts (hereafter the Society for Aid and Rehabilitation), founded in 1961 by Brook Antony Bernacchi, a lawyer, social activist, and politician from the Hong Kong Reform Club. With grants from the Jockey Club, they built a Rehabilitation Centre in the Shek Kwu Chau (石鼓洲), covering an area of 300 acres and located south of Lantau Island. It replaced the Castle Peak Centre in 1965 which suffered from a shortage of accommodation and staff. 52
All these programmes, despite slight differences in approaches and targets, centred on personality change by ‘correcting’ the addicts and treating them as patients. Normally, patients would receive treatment in three steps: withdrawal, rehabilitation, and aftercare. For instance, after admission into the Castle Peak Centre, addicts would undergo one to two weeks of withdrawal, followed by three weeks of recreational activities, such as table tennis, cards, and music, and occupational therapy such as tailoring and gardening. After discharge, social workers would offer material support, conduct group therapy, and follow up on their recovery. 53 Even the treatment centre in Tai Lam Prison shared a similar programme structure and distinguished itself from the harsh prison setting, stressing on an open environment, an acceptable level of discipline, and manual work to build up physical and mental strength in the addicts. 54
The Society for Aid and Rehabilitation’s programme for voluntary patients exemplified the therapeutic ideal of transforming drug addicts. Incorporating the theory of group dynamics created by Kert Lewin, a German-American social psychologist, the society developed a scheme of rehabilitation to experiment with changes in personality and behaviour. In addition to occupational and recreational therapy, the core of the scheme was promoting addicts to different ranks of ‘Hong Fook Yuen’ (inmate being rehabilitated, 康復員) to symbolize their level of rehabilitation. Higher ranks meant higher incentive pay and sometimes a supervisory position in occupational therapy. It divided all addicts into five houses and organized 20 people in a group to live and work together as a way to establish solidarity. 55
Among all therapeutic techniques, psycho-social assessment was the evaluation tool used to determine whether the patients were cured. Dr S. H. Moore, the medical superintendent of the Society for Aid and Rehabilitation’s programme, believed that addicts were social outcasts, lazy, sensitive to criticism, and mentally unstable and that they should be rehabilitated and equipped with moral strength, confidence, and self-respect. Successful rehabilitation, in this sense, meant forging trust between addicts and staff, promoting self-respect and pride in their work, and establishing moral strength to resist temptation after discharge. To evaluate their progress, the staff and group leaders regularly submitted observational reports of addicts’ behaviour, personality, and response to occupational therapy. The assessment criteria based on behavioural change explained the ultimate goal of the Shek Kwu Chau Centre: to get rid of the dependent attitude of a ‘sick man’, be a good citizen, stabilize the growth of the patient’s personality, and prepare for a new life following discharge. 56
Nonetheless, the therapeutic ideal of rehabilitation was replete with tensions in everyday operation. While the colonial government preached the therapeutic ideal, psychiatrists, medical officers, and social workers on the frontline struggled to manage the addicts. Pow Meng Yap, the psychiatrist in charge of the experiment in Castle Peak Hospital, admitted that its treatment centre developed into a disciplinary institution associated with punishment instead of therapy. Without legislative power to apply formal punishment, the Castle Peak Centre had to standardize the punishment in a mild form, such as deprivation of dietary extras or cigarettes, and confinement in a single room. 57 Meanwhile, once discharged from rehabilitation centres, the ex-addicts immediately faced several problems that could potentially bring them back to their drug habit: free drugs offered by other addicts and drug dealers as a welcome gift, pain inflicted by long-term sickness, unemployment, and family crisis. Later governmental surveys also showed that the Society for Aid and Rehabilitation suffered from a lack of discipline among the addicts, who often had been incarcerated and were involved in triad activities, gang fighting, abuse of staff, assaults, escape, and caused disturbances. 58 Despite the therapeutic ideal of rehabilitation, the elusive meanings of cure invited criticism and thus led to another experiment, methadone, in the following years.
From mental health to public health: The methadone maintenance pilot scheme
The mid-1960s marked an acceleration of the anti-narcotics campaign when Hong Kong came under pressure from London. In 1965, a series of three articles by Frederick Joss writing for Eastern World, a left-wing magazine published in Britain, touched a nerve of high officials in London. These articles criticized Hong Kong’s ‘drug cancer’ and its supremacy as ‘the strategic centre of the world’s filthiest organised business (of drugs)’, which facilitated the global trade of narcotics through refining heroin and exporting it to Japan, Canada, and the United States. Anthony Greenwood, the Secretary of State for the Colonies, expressed great concern, directly corresponded with Joss, and urged Sir David Trench, the Governor of Hong Kong, to take possible measures to ‘increase the effectiveness of Hong Kong’s campaign against trafficking and addiction’. 59
The publication of the three articles coincided with the restructuring of the Narcotics Advisory Committee. In 1965, to centralize coordination and communication, the Narcotics Advisory Committee set up the Action Committee Against Narcotics to exchange information related to narcotics between 11 governmental departments and 9 voluntary organizations. Divided into five sub-committees, including education and publicity, illicit traffic, deterrents, research, and treatment and rehabilitation, the Action Committee held periodic meetings to facilitate immediate cooperation and coordination. A full-time Assistant Secretary for Chinese Affairs (Narcotics) was appointed to serve as the principal co-ordinating officer for the entire anti-narcotics campaign. 60 More importantly, the broad membership included Chinese tycoons to government departmental representatives, medical professionals, community leaders, and voluntary and religious organizations. 61 Although the Action Committee was not an executive body, the regular meeting of sub-committees brought different department organizations in charge of rehabilitation together. The restructuring of anti-narcotics agencies paved the way for evaluating the efficiency of the rehabilitation programme.
Criticisms of treatment programmes quickly emerged in the Treatment and Rehabilitation sub-committee. First, statistics gathered in the 1950s and 1960s were confined to a small sample that was hardly representative. 62 Different institutional practices also made data gathering difficult. For instance, the Prison Department and the Society for Aid and Rehabilitation followed up on addicts for one year and three years respectively. 63 In other words, addicts could have been through all treatment programmes without a working system. Second, and most importantly, the Treatment and Rehabilitation Sub-committee confirmed patients’ high relapse rate. Data from the Society for Aid and Rehabilitation showed that between 1963 and 1972, it discharged 4331 ex-addicts and 1993 relapsed. 64 The high relapse rate, almost 50 per cent, was shocking to many committee members and explained why the Action Committee introduced new experimental treatments in the late 1960s.
The discussion of methadone was first brought up in 1968 by Dr Lik-Kiu Ding, who obtained a medical degree from Johns Hopkins University. His close association with the American medical profession naturally led him to the American approach against drugs. After visiting New York Hospital for addiction treatment, he advocated methadone as a narcotic substitute and vigorously defended the plan in the Action Committee. 65 He also convinced the members of the Discharged Prisoners’ Aid Society, a voluntary organization that operated a withdrawal hostel that used methadone, to conduct experiments on methadone maintenance under his guidance. 66
However, methadone maintenance faced strong opposition from colonial government officials who were involved in existing rehabilitation programmes. K. F. Chan, the representative of the Director of the Medical Department, was firmly against methadone on medical grounds. First, he questioned the experimental nature of methadone in the United States. Citing a study conducted by the Narcotics Advisory Committee in 1964, Chan argued that methadone could not serve as a substitute for heroin if the latter was available to addicts at the same time. Methadone would pander to the addiction and was not a treatment. To him, ‘there is practically no difference whatsoever from the system of supplying stabilising doses of narcotics to addicts through legitimate medical channels, to enable them to lead relatively normal lives’. 67 Fundamentally, methadone maintenance, which controlled addicts with another drug, contradicted with the rationale of rehabilitation, which stressed on helping addicts withdraw from drugs. Other officials opposed the Pilot Scheme from an administrative perspective, including arguments about the diversion of methadone into the black market, difficulties in distributing methadone to addicts, and keeping the addicts permanently on drugs if the programme failed. 68
To other committee members, methadone maintenance was a risk worth taking. They believed that users, under supervision, would resume ordinary life with the help of methadone. Methadone treatment was economical because patients would not be treated with excessive hospitalization and detention. The cost of daily methadone treatment was only one-tenth the cost of maintaining an addict in prison or an addiction treatment centre. 69 Also, the treatment facilities had an annual capacity of 2500 patients, which could not meet the growing numbers of addicts. Male addicts were estimated between 30,000 and 65,000 in 1966, excluding the high relapse rate. Brook Bernacchi, Chairman of the Treatment and Rehabilitation Sub-committee, supported Ding’s proposal from the standpoint of efficiency and argued that ‘the drug problem in Hong Kong could never be effectively dealt with if we did not explore and experiment with new methods of treatment’. 70
A majority vote passed the proposal for a Methadone Maintenance Pilot Scheme in the Action Committee in 1971. The plan would be implemented by the Discharged Prisoners’ Aid Society, which had experience operating a withdrawal hostel that involved the use of methadone and provision of aftercare. The Pilot Scheme, lasting three years, was meant to ascertain what methadone maintenance could achieve in terms of withdrawal from heroin addiction. The Pilot Scheme was carried out in a centre located in the Tung Tau Tsuen area. The centre would first admit 100 cases of hardcore heroin addicts for inclusion in the project, and it was open to males between 25 and 50 years old, who were residents in the Kowloon City area with at least one unsuccessful attempt to withdraw from heroin in recognized programmes, on a voluntary basis. After an interview with the selection committee, patients would be sent to Maryknoll Hospital for two weeks for induction to methadone. Once discharged, they would attend the centre in Tung Tau Tsuen for their daily dose of methadone, submit a urine specimen, and meet counsellors to discuss their real-life problems. 71
The Pilot Scheme was conducted in the form of a double-anonymous study, a type of clinical trial where participants and researchers were unaware of which group of participants actually received treatment. At the time, there was no anonymous experiment to validate methadone maintenance, which made Hong Kong’s experiment irreplaceable. The patients were divided into two groups: (1) a treatment group that received methadone in an orange juice mixture, and (2) a control group that received a placebo (not methadone) mixed with orange juice. 72 Simply put, the control group did not receive any methadone after withdrawal treatment in hospital. The experiment took place between 1972 and 1975, and the results of the methadone experiment were encouraging. The measurements of success or failure of the Pilot Scheme included the use of heroin determined by urine tests and family reports, return to permanent addiction, criminal activities, income and employment status, and family life. In simpler terms, most participants in the control group quitted the scheme largely due to reuse of heroin, while those in the treatment group stayed and continued to consume methadone to reduce their dependence on heroin. In terms of criminal activity, the average conviction rate of the control group was double that of the other group. 73 Put differently, the Pilot Scheme proved that methadone could keep the addicts away from heroin, restore them to a normal life, and reduce the crime rate.
Even before the experiment was completed, the Medical Department already expanded the scale of treatment. In 1974, the Hong Kong Police arrested several syndicates smuggling opium and crude morphine into Hong Kong. Ironically, it resulted in a heroin famine that sent an alarming signal to the Medical Department: thousands of addicts could not obtain their drugs from normal supply channels and thereby turned to crime for more money to buy highly priced heroin. Fully aware of the limited capacity of existing rehabilitation programmes, the Medical Department viewed methadone maintenance as a solution to the heroin famine and opened three more Methadone Clinics in addition to the existing two centres. For the first time, methadone treatment became attractive to the addicts because it offered alleviation from the severe pain and stress experienced during drug withdrawal. 74 Flooded with addicts rushing for drugs, the Methadone Centres had a three-month waiting list during the heroin famine in December 1974. 75 Table 1 indicates the surge of addicts into methadone clinics from 1480 in 1974 to 10,400 in 1976. Yet, the attendance dropped slightly in 1977, possibly because more addicts attended the clinic during the heroine famine in 1976 and dropped out in 1977 when heroin became available again. 76 By 1981, 69 per cent of the dependents were admitted to the methadone treatment programme. 77 This major shift from rehabilitation to methadone maintenance became the key to the anti-narcotics campaign in the following years.
Yearly admission into treatment institutions, 1969–1979.
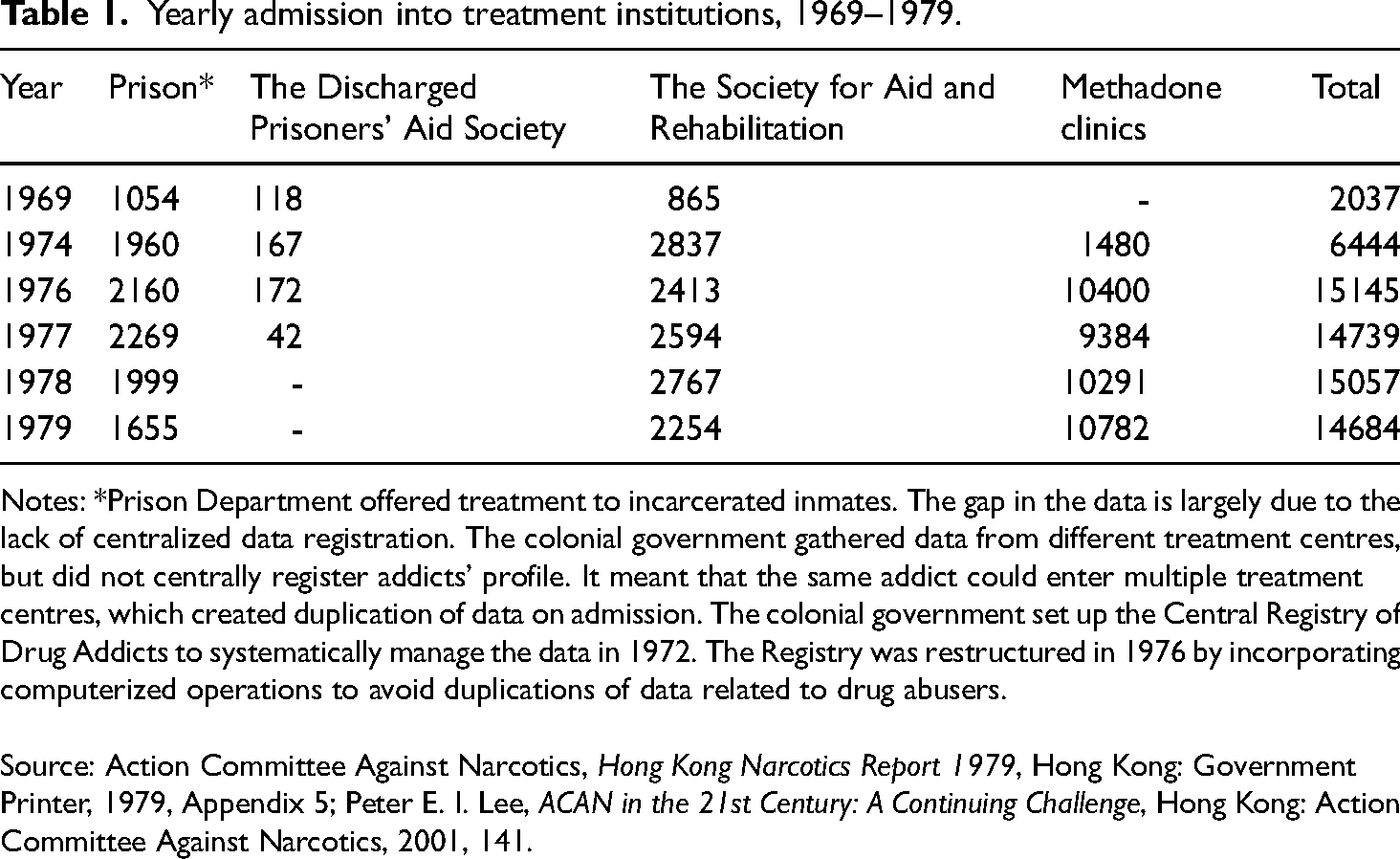
Notes: *Prison Department offered treatment to incarcerated inmates. The gap in the data is largely due to the lack of centralized data registration. The colonial government gathered data from different treatment centres, but did not centrally register addicts’ profile. It meant that the same addict could enter multiple treatment centres, which created duplication of data on admission. The colonial government set up the Central Registry of Drug Addicts to systematically manage the data in 1972. The Registry was restructured in 1976 by incorporating computerized operations to avoid duplications of data related to drug abusers.
Source: Action Committee Against Narcotics, Hong Kong Narcotics Report 1979, Hong Kong: Government Printer, 1979, Appendix 5; Peter E. I. Lee, ACAN in the 21st Century: A Continuing Challenge, Hong Kong: Action Committee Against Narcotics, 2001, 141.
The ‘Hong Kong’ model: Local and international responses
Throughout the 1970s, supporters of rehabilitation constantly questioned the methadone programme in newspapers. Some challenged its efficiency and described methadone as ‘a lesser evil’. 78 For instance, Reverend Karl Stumpf, a member of the Action Committee, criticized methadone as a ‘temporary holding operation’ and contended that addicts must be helped through counselling to start a new life, including basic schooling, skills training, housing, and a job. 79 In 1982, a report from The Star revealed that only 420 drugs addicts from the 26,200 treated kicked the habit, a success rate of around 2 per cent. The newspaper interviewed a social worker who commented that methadone ‘was only a cheap legal drug for addicts . . . addicts label heroin as steak and methadone as rice. When they can’t afford steak, they’ll take the rice.’ The report quoted the response from the Action Committee, which defended methadone and argued that it ‘has achieved its prime purpose – to cut down on crime’. 80
Was methadone maintenance successful in Hong Kong? Yes, to colonial officials, methadone was a great success. In a different context, historian Claire Clark aptly captures why methadone appealed to American officials: while the approach of rehabilitation emphasized personality changes and familial transformation through a labour-intensive form of counselling, methadone maintenance was cheap, effective, and convincing by blending methadone clinics with existing medical infrastructure and gathering crime data. 81 In a similar vein, methadone maintenance appealed to Hong Kong colonial officials because of its function as an effective crime-fighting tool. By grounding successful treatment on lowering the crime rate, the final report of the pilot scheme set aside earlier definitions of cure based on personality changes and offered convincing and visible results. 82
However, a more important question remains: was methadone a cure? To Dr Gerald Choa, the Director of the Medical Department in 1976, methadone – whether long-term maintenance or short-term detoxification – was neither a panacea nor a cure for drug addicts. He admitted that the multiple approaches to rehabilitation and methadone made cure hard to define and that treatments could not be assessed by retention rate in rehabilitation programmes nor attendance in methadone clinics. 83 The primary purpose of methadone maintenance was to keep the addicts on the programme, and the addicts would get counselling and aftercare. Eventually, they would be rehabilitated as ‘working and contributing members of society’. 84 Through the combination of methadone maintenance and rehabilitation programmes, the colonial government departed from the past of opium monopoly and now centred governance on therapeutic transformation of addicts into useful subjects.
Nonetheless, the success of methadone in the late 1970s symbolized the broader victory of the anti-narcotics war. From the late 1970s, newspapers began to declare that the war on drugs was ‘being won’ and complimented the Hong Kong government’s realistic approach to contain addicts’ habit and work to earn a living wage through methadone maintenance. 85 The surging numbers of attendants in methadone clinics, often quoted in the newspapers reports, conveyed a different logic: the higher the numbers, the lower the crime rate. To the colonial government, the data gathered by methadone clinics visualized their efforts to the public in clear and simplified terms. Methadone maintenance as such allowed the Hong Kong colonial government to present itself as having narcotics under control. 86
With the initial purpose of restoring social security in the 1950s, the anti-narcotics war became part of the colonial effort to construct ‘good governance’ in the 1970s. Examining Anglo-American cooperation in combating drug trafficking, historian Philip Thai rightly observes how the anti-narcotics campaign met Chinese communities’ increasingly vocal demand for law and order by the 1970s when fears of public disorder, such as violent crimes and drugs, became widespread. 87 In this light, the anti-narcotics campaign dovetailed with the London officials’ diplomatic agenda. By bringing stability and prosperity to the colony, the anti-narcotics war, along with other social welfare projects, added credibility to colonial governance and turned good governance into a bargaining chip in negotiations on the handover of Hong Kong with the PRC. 88
Meanwhile, Hong Kong’s experiment with methadone was well received by American methadone experts. Vincent P. Dole, the pioneer of methadone maintenance, commented on the Hong Kong Scheme as ‘the only study that meets the rigorous requirements of randomisation of subjects and double-blind administration of treatment. For the first time in this field, statistically compelling evidence is available to demonstrate the efficacy of this treatment.’ 89 Robert L. DuPont, the Director of the National Institute on Drug Abuse, described Hong Kong’s Pilot Scheme as ‘one of the most important studies on the efficacy of methadone maintenance treatment conducted to date’. 90 In 1985, Robert Newman, the American advisor of the methadone maintenance programme in Hong Kong, submitted a proposal for methadone clinics based on the Hong Kong model to the Food and Drug Administration in the United States. According to him, Hong Kong’s model involved interim clinics that distributed methadone to addicts without counselling, rehabilitation, and other social services that are required by federal regulations. 91 As a temporary measure, interim clinics would free addicts from the overly long waiting lists and prevent them from returning to the street for drugs. Later research validated the efficiency of interim clinics, and the FDA legitimized their operation in 1993. 92 As Newman put it, Hong Kong provided ‘lessons for the United States’ in addiction treatment. 93
To Newman, Hong Kong was the ideal laboratory for methadone maintenance. Newman’s support for the Hong Kong model should be understood in the light of methadone’s immediate rise in the early 1970s and decline in the late 1970s in the United States. A number of factors contributed to its decline: controversy about feeding addicts with drugs, 94 the ascendence of cocaine in the late 1970s (methadone was of no use for treating these addictions), 95 community resentment toward methadone clinics, 96 and diversion of methadone from clinics to the street. 97 In this sense, Hong Kong carried a unique appeal to the American advisors and was a free space for experiments. In an 80-page detailed report submitted to the colonial government, Newman noted that Hong Kong was ‘in an excellent position to avoid the counter-productive fragmentation which has plagued the addiction treatment efforts elsewhere (the United States)’. 98 Hong Kong’s highly centralized and government-funded programmes proved the feasibility of extensive methadone maintenance. To Newman, Hong Kong was the key evidence to alleviate and dispel domestic concerns about methadone.
Conclusion
By examining the anti-narcotics campaign from 1959, this article uncovered the uneasy process whereby the colonial government constructed a new form of therapeutic governance. To cope with the colonial legacies of opium monopolies, the colonial government launched the anti-narcotics campaign to medicalize addiction and thereby cure drug addicts. These efforts successfully transformed Hong Kong from a distribution port of opium into a leading Asian city in drug treatment. The implication of such transformation is crucial for understanding the post-war history of Hong Kong and other colonial states: the colonial government was no longer involved in the opium trade and it proclaimed the protection of its citizens as a rationale to justify its governance. By redrawing the boundaries between legal and illegal drug consumption, the new form of therapeutic governance justified the state’s constant intervention into everyday life. Yet, this process of medicalization was replete with tensions between the state and medical profession, between therapeutic ideal and clinical reality. While medical experts struggled with the elusive meanings of cure, the colonial state viewed methadone and rehabilitation as serving the same purpose: to control, tame, and transform addicts into useful subjects. Chemical intervention and personality change were part of the colonial governing machine. In this sense, a focus on addiction treatment blurred the boundaries between social welfare and control.
Hong Kong anti-narcotics campaign was also part of the global struggle against drug addiction. Hong Kong’s response to narcotics was profoundly shaped by the American approach toward drug addiction. In testing out possible approaches to cure addicts in the colony, medical officers in Hong Kong naturally drew references to treatment programmes in the United States and introduced methadone maintenance. To American experts who supervised the Pilot Scheme, Hong Kong’s experiment was an ideal laboratory to gather evidence to alleviate domestic concerns. The Pilot Scheme turned out to be an international success and convinced the American experts to reimport the Hong Kong’s model, creating a lasting impact over global methadone programmes. Similar methadone programmes received momentum in the Netherlands (1980s), Germany (1990s), France (1990s), Vietnam (1997), and China (2000s). 99 These contexts help explain why, since the mid-1970s, the colonial government has hailed Hong Kong as an anti-narcotics training ground for Southeast Asian and Asian countries. By the late 1970s, over 400 international trainees and visitors went to Hong Kong to learn about the anti-narcotics campaign. 100 The case of Hong Kong’s treatment programmes, thus, opens up new inquiries into the far-reaching consequences of the global drug war in colonial and post-colonial Asia.