
Abstract
The present study is part of a larger research that analyses children’s autonomy in healthcare settings from the perspective of doctors, children and their parents. Based on responses of 52 medical doctors in Estonia, this paper explores doctor’s perspectives on how children’s autonomy is exercised in a child-parent-doctor triangle and how patient’s duality affects this process. The article combines relational theories of agency from childhood studies with the concept of children’s autonomy applied in children’s rights studies.
Introduction
The power to give free and informed consent to medical treatment and intervention is one of the most fundamental rights of a patient. Such right is based on a core principle of medical ethics - autonomy. However, it is also an accepted principle of medical ethics that autonomy does not require the respect of every choice but only choices that are made by competent patients (Goold and Herring, 2018:26). This is why children, as regarded not fully competent, are still treated paternalistically in health-care, although a model based on paternalism (doctors making choices on behalf of patients) has been largely replaced by an autonomy model (patient’s self-determination) over the last 40 years (Goold and Herring, 2018: 11). In children’s rights studies such sentiment towards children has been called “gentle paternalism” (Fortin, 2004: 259) or also “dynamic self-determinism” (Eekelaar, 1994).
Whether children have the right to give an independent consent to medical treatment depends on legal regulations of individual countries. However, regardless of domestic consent regulations, all countries that have ratified the UN Convention on the Rights of the Child (CRC) must allow children to be heard and be involved in decision-making regarding their health (article 12 of CRC). Through the right to be heard the child realises his/her autonomy. As such, participation in decision-making is a wider concept than consent (the conceptual difference between participation and consent is often undeservedly neglected) and is better suited for exploring exercise of child’s autonomy in a triadic relationship that this article focuses on.
It is argued that international and European standards ‘over-emphasise the child’s right to protection, and do not sufficiently recognise the principle of children’s evolving capacities and their right to be heard and participate in decision-making related to their health and care’ (Liefaard et al., 2017: 5).
In addition to limitations deriving from the regulatory framework and low awareness of children’s rights, the attitude of adults hinder children’s participation and realisation of their autonomy. Mårtenson and Fägerskiöld (2008) state that children’s decision-making competence is not so dependent on their own capacity but rather on attitudes of parents and healthcare professionals. Research in Estonia (Praxis, 2018) shows that 40% of adults either are not sure whether a child has the right to be informed about decisions regarding his/her health and the right to participate in making such decisions, or they even believe that a child does not have such rights.
Earlier studies on decision-making by children about their health concentrate mostly on decision-making capacity and competence, and the assessment thereof, thereby focusing on criteria for competence assessment (Grootens-Wiegers et al., 2017; Paron, 2020; Ruhe et al., 2015; Weller et al., 2012). However, there is a gap in knowledge of how a child’s autonomy is supported or restrained where health decisions are made in a child-doctor-parent triadic relationship. The present paper tries to broaden this field of knowledge by analysing the realisation of the child’s autonomy from the perspectives of doctors.
The article starts by introducing a theoretical approach to the theme and continues by describing the methods used and presenting the findings. The paper ends with a discussion and conclusions, in which models of patient autonomy in cases of child-parent disagreement are presented.
Theoretical approach
Agency
In the sociology of childhood there is a consensus that children are autonomous agents (Frønes, 2016; James and James, 2004; James and Prout, 1990; Mayall 2015) who are not passive recipients but rather have influence on their lives and on others. However, there seems to be less agreement about what children’s agency really means and how it serves the progress in childhood studies (Alanen, 2019). In 1998, James, Jenks and Prout (James et al., 1998) stated that childhood agency and the agentic child have been codified in sociology as the ‘new paradigm’. 20 years later, the concept of children’s agency may seem to be an old paradigm in need of reimagination, to use the words of Spyrou et al. (2018). They claim that childhood scholarship has been ‘valorizing children’s agency to the point of fetish’ and that agency ‘in its centrality, dominance, and hegemonic position in childhood studies – may very well stand in the way of reaching for alternative ways of knowing’ (2018: 3-4). They question the notion of a constructed, agentive, knowing child as the only proper approach to childhood, and call for new knowledge that should be more critical towards the ‘old’ paradigm.
One way to change the ‘old’ paradigm is to combine the knowledge of different fields – sociology, law, psychology, pedagogy, etc. For instance, Bonvin and Stoecklin (2014) argue that children’s rights are best studied from an interdisciplinary angle, involving the sociology of childhood, developmental psychology, legal studies, educational sciences, and other relevant disciplines. Greene and Nixon (2020: 190) refer to recent calls among sociologists for more cross-disciplinary or interdisciplinary work, ‘particularly in relation to advancing theoretical understanding of key-concepts such as agency’. Even though childhood studies form an ‘umbrella’ discipline combining various sub-disciplines (Canosa and Graham, 2020), it is also argued that childhood studies are ‘possibly still dominated by the sociology of childhood, the anthropology of childhood and children’s geographies’ (Tisdall and Punch, 2012: 259), while each sub-discipline tends not to move ‘beyond its disciplinary boundaries’ (Punch, 2016: 354).
This article strives for disciplinary ‘beyondness’ by looking for guidance from children’s rights studies for a better conceptualisation of an agentic child. The dialogue between childhood studies and children’s rights studies is a resourceful platform for understanding children’s autonomy in different decision-making situations and contexts.
In childhood studies, the terms, ‘agency’, ‘autonomy’ and ‘self-determination’ are entangled and often used to explain one another. Giddens, who is ‘blamed’ for introducing the concept of agency into childhood sociology (James, 2009), calls an agent an ‘acting self’, whereas agency refers above all to people’s capability of doing things (Giddens, 1984). The ability to make a difference, to have an effect on others, is a key-element of Gidden’s agency. In a similar mode, Mayall (2002) differentiates an actor from an agent: an actor is someone who does something, an agent is someone who does something with other people, and in doing so has a wider impact on social reproduction. Frønes (2016) sees agency as development of self-determination and autonomy, being the core of the theorizing of socialization. Kuczynski (2003) conceptualises children’s agency through three dimensions – autonomy (self-determination), construction (capacity to make sense and create new meanings) and action (ability to intervene).
Autonomy
The above is a vivid illustration of the fact that agency is often interpreted as autonomy or self-determination in childhood studies. The Oxford and Cambridge dictionaries define ‘autonomy’ as the ability to act and make decisions without being controlled by anyone else, whereas ‘self-determination’ is defined as the ability or power to make decisions for yourself/the right of a person to control their own fate. In children’s rights studies, as part of a broader human rights discourse, autonomy is a well-established concept. Every human being’s autonomy is the quintessence of a liberal democratic society and a fundamental value recognised in all human rights treaties. Article one of the Universal Declaration of Human Rights stipulates that all human beings are born free and equal in dignity and rights. The freedom to determine one’s own destiny is also called self-determination in human rights discourse. Self-determination and autonomy are often used as synonyms.
Autonomy is also a central principle of the CRC. The practical confirmation of children’s autonomy lies in Article 12 of the CRC which requires that the child who is capable of forming his or her own views must be assured the right to express those views freely in all matters affecting the child, whereby the views of the child must be given due weight in accordance with the age and maturity of the child. The theories surrounding Article 12 have been conceptualised as ‘participation’. According to the CRC Committee’s General Comment No. 12 (2009: 3), the term participation is widely used to describe processes which include information-sharing and dialogue between children and adults that are based on mutual respect.
The above conceptualisation must be analysed, in our view, through a critical lens – a child’s right to self-determination is under constant scrutiny as it is always an adult who decides how much weight is given to the child’s opinion. Even though autonomy as provided for in the CRC is thus limited, the CRC also provides an assisting framework for conceptualising children’s autonomy as a process of gradual shift from limited autonomy towards full autonomy (Paron, 2020). Such process is understood in Article five CRC as ‘evolving capacities’. Article five of the CRC stipulates a right and duty of a parent to provide appropriate direction and guidance to the child in the exercise by the child of his/her rights, in a manner consistent with the evolving capacities of the child. The CRC Committee’s General Comment No. 20 (2016: 6) defines evolving capacities as ‘an enabling principle that addresses the process of maturation and learning through which children progressively acquire competencies, understanding and increasing levels of agency to take responsibility and exercise their rights’. The above means that in realization of child’s autonomy rights articles 12 and 5 must be applied together - the more mature and competent the child is, the more weight must be given to his/her opinion. At some point in his/her development the child acquires maturity equal to that of adults and in such case the child’s view must be determinative when making a decision about child’s life (Tobin, 2019: 403).
The framework of growing autonomy contained in the concept of evolving capacities is a suitable tool for better conceptualisations of agency also in childhood studies. Sutterlüty and Tisdall (2019) argue that ‘given contemporary normative orders, autonomy should arguably become the new core concept of childhood studies rather than agency’. Daly et al. (2019) agree that autonomy is a more suitable term when framing the legal rights of children to make choices for themselves. Autonomy is also a well-established concept in medical ethics. Beauchamp and Childress (2001: 58) define personal autonomy at minimum as ‘self rule that is free from both controlling interference by others and from limitations, such as inadequate understanding, that prevent meaningful choice’. In the context of healthcare, autonomy is therefore better suited than agency for analysing children’s involvement in decision-making.
Relationality
Childhood studies, in turn, can contribute to conceptualisations of autonomy in children’s rights studies with its strong relational theories (Alanen, 2014; Mayall, 2015; Spyrou et al., 2018). Children’s agency does not exist in a vacuum or isolation; it is created and implemented in relationships. Spyrou and colleagues (Spyrou et al., 2018:8) argue that ‘relational ontologizing signals a shift from childhood as an identity category to the practices which enact it as a particular kind of phenomenon’: such shift taking focus from ‘what childhood is’ to ‘how childhood is done’. According to Alanen (2014: 133) ‘children are constituted specifically as children primarily (although not exclusively) within intergenerational relations’. Intergenerationality is also central in Mayall’s works, who states that childhoods are structured through ‘intergenerational relationships’ (Mayall 2000).
The relationality of children’s agency is thoroughly elaborated in Kuczynski’s works. Although his research focuses on bidirectional influence between children and their parents, it gives valuable insight into child-adult mutual agency and its bidirectional nature. Children and parents influence one another’s behaviour and are equally agents with the ability to initiate change and make choices (Kuczynski, 2003). They are, however, unequal in resources or power that supports their effectiveness as agents (Kuczynski et al., 2014). This conclusion of power imbalances is even more valid with regard to other adults, as parents are more receptive to their children’s influence and ‘may offer considerable leeway for children’s expression of agency’ (Kuczynski et al., 2018: 3).
The above conceptualisations of the relationality of children’s agency may refine the rights-based thinking around children’s autonomy. Recent scholarship on children’s rights is marking such tendency to consider children’s autonomy as a relational phenomenon (Daly, 2020; Varadan, 2020). The present study combines the rights-based concept of child’s autonomy with conceptualisations of relationality of children’s agency.
Legal and social context of the study
Estonia has ratified the CRC in 1991. The general principles of the CRC (including article 12) have been also transposed into the Child Protection Act (2014). The Law of Obligations Act (2002) regulates the contractual relationship between the health service provider and the patient. It provides that in case of patients with restricted legal capacity (including children), the legal guardian (e.g., the parent) has the right to give consent insofar as the patient is unable to consider pros and cons responsibly. Thus, competence of child-patients has to be assessed on case-by-case basis. Still, child-patients’ competence is rarely assessed in medical practice in Estonia (Paron, 2018). Children generally visit doctors with their parents and are on agreement about the child’s health issues. Therefore, the question of who precisely gives consent may not arise. Moreover, doctors and patients may not be (fully) aware about legal rules or do not recognise the child-patient’s right to autonomy (Paron, 2018), and there is no soft law in the form of recommendations or guidelines.
Methods
Sample
The present study is part of a larger research that analyses children’s autonomy in healthcare settings from the perspective of doctors, children and their parents. This paper focuses on doctors’ views on the child-parent-doctor relationship and analyses web-based responses of 52 paediatricians and family doctors (GP) from 2021. The professional experience of the doctors varied from 10 to 30 years, 14 doctors had practiced medicine for more than 30 years, and eight less than 10 years. The doctors received invitations to participate in the study via the mailing lists of the Estonian Family Doctors Association and the Estonian Paediatricians Association.
Data
Doctors were asked in a web-based questionnaire to tell in their own words how they establish contact with a child and how they communicate with children and their parent(s). They explained whether they communicate either mostly with the child, mostly with the parent, or equally with both the child and parent. Doctors also gave assessments to the factors that influence children’s participation in decision-making (Figure 1) and explained how they act in cases of child-parent disagreement. Agreement of doctors with the statement “A child’s involvement in decision-making depends on …”, N.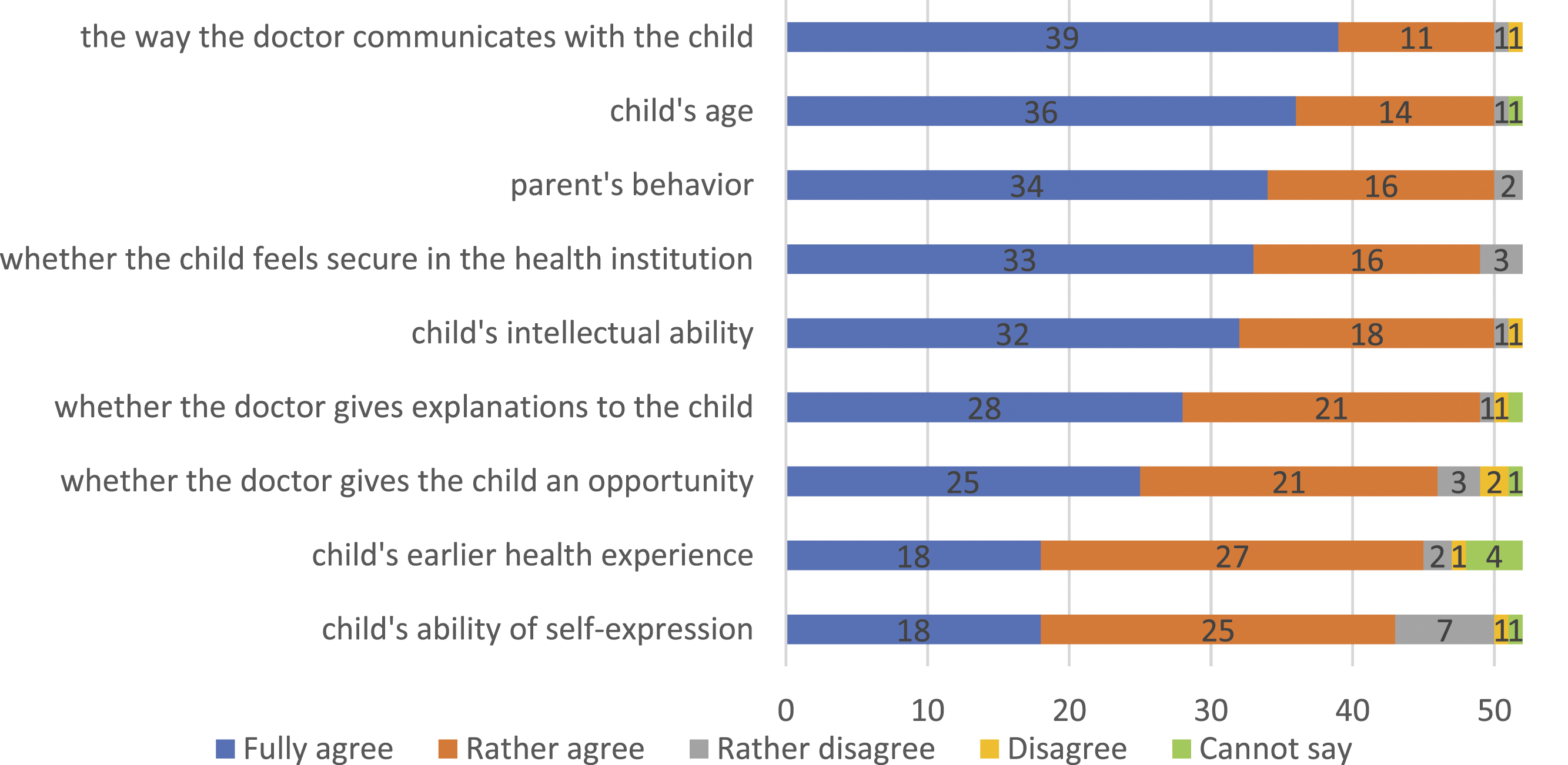
Under Estonian law, in order to consider that a child is able to give consent autonomously, he/she must be capable of weighing all the pros and cons responsibly. The research intended to analyse how doctors assess such capacity (Figure 2). An agreement type scale was applied to all questions, ranging from 1 (‘fully agree’) to 4 (‘do not agree’) or 5 (‘cannot say’). Aspects considered by doctors when assessing children’s decision-making capacity, N.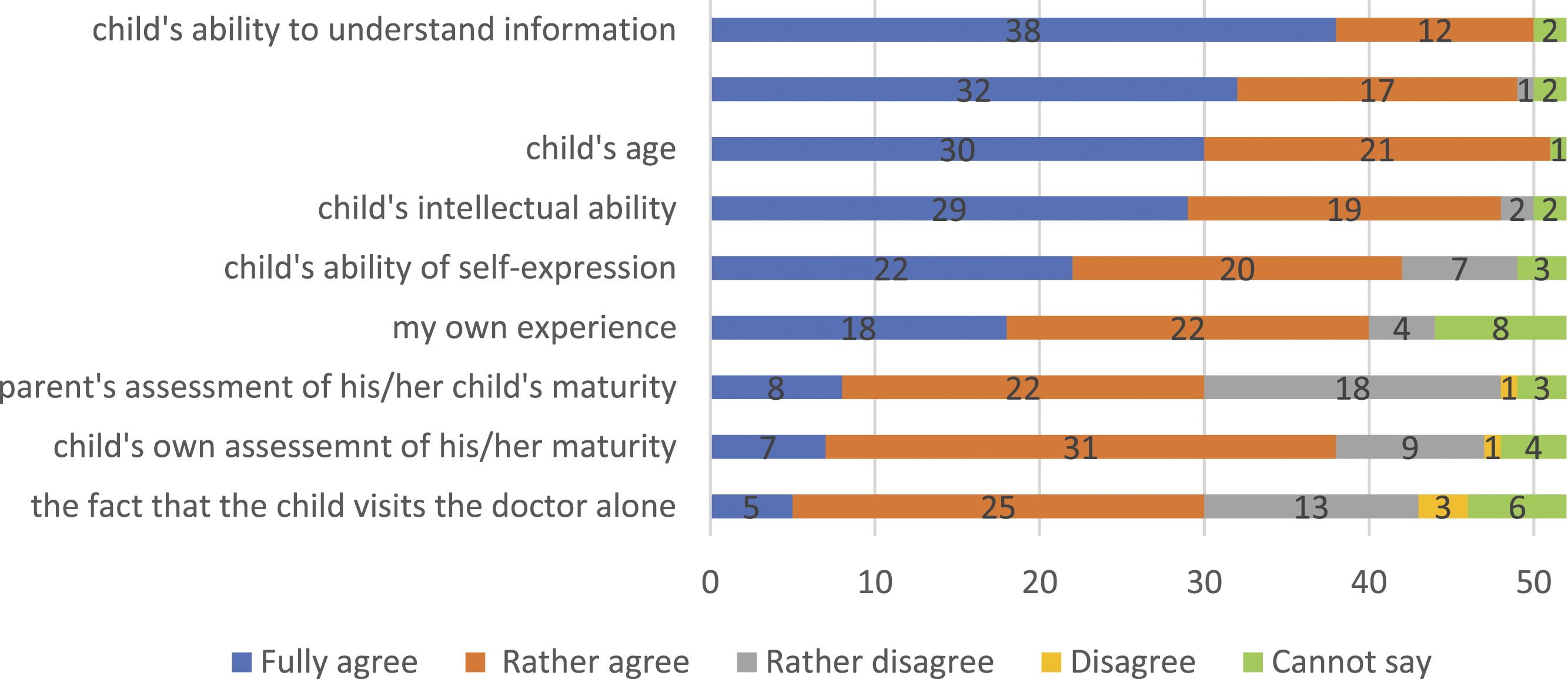
Analysis
This study combines quantitative and qualitative approaches. Univariate analysis demonstrates the distribution of responses to the agreement scales. Answers to the open-ended questions were analysed thematically, by combining the deductive and inductive approaches for identifying themes and subthemes (Braun and Clarke, 2006). The latter included repeated readings of the responses, identification of codes, double-checking the codes and additional analysis of the themes with the second author.
Findings
Doctor-patient communication
The analysis revealed that active participation of both parents and children in communication is important for doctors: 43 of 51 doctors said that they communicate with both, whereas eight doctors reported that they communicate mostly with the child. This is in line with results of other studies (Boland et al., 2016; Carlsson et al., 2018; Schalkers et al., 2016). None of the doctors admitted that they communicate mostly with the parent. The vast majority (51 of 53) agreed that it is important that both the child and the parent understand the information shared by the doctor.
In general, doctors wish to hear about the health issue that is the reason for the appointment directly from the child. The doctors’ responses indicated that the child is regarded as a source of information but not necessarily as a fully-fledged patient: “When I talk to the child and ask his/her opinion, then I communicate only with the child. The treatment decisions will be discussed with the parent”.
Communication patterns
There are several factors that may lead a doctor to behave in one way or another when communicating with a child or parent, such as an understanding that children may be afraid of doctors or that discussing treatment options with a child is not proper. Three main communication patterns of the doctors emerged from the data: (1) age-based; (2) capacity-based and (3) child-centred. An age-based pattern of communication was most often reported by the doctors, e.g.: “In the case of younger children, I communicate more with the parent, in the case of school-aged children 1 I communicate more with the child”; “With adolescents, I try to communicate more with the child”. A capacity-based communication pattern emerges where doctors adjust their communication according to the child’s social skills and openness, e.g.: “Communication depends on the child’s readiness to communicate (whether the child is afraid, talkative; wants to answer my questions or looks for the parent’s assistance)”; “If the child is talkative, I communicate with the child. If not, the parent will help”; “If the child avoids contact and looks for contact with the parent, I will keep a low profile with them”. The third and the rarest was the child-centred pattern, where the doctor’s attitude is a priori child-centred and supportive of the child’s autonomy. Doctors explained: “I always try to concentrate on the child and their feelings, not on what the parent wishes or thinks”; “If the parent tries to dominate over the child and constantly interferes when the child is speaking, I get cautious. If needed, I educate the parent in this respect.”
Factors influencing children’s involvement in decision-making
We were interested in the factors influencing child’s involvement in decision-making related to the doctor’s behaviour, parent’s behaviour, and to the child’s capacities and age (Figure 1). The results reveal that involvement of a child in decision-making depends primarily on the way the doctor communicates with the child. A slightly smaller number of doctors agreed with the significance of instrumental criteria, such as giving explanations to the child and creating opportunities for them to participate in the decision-making process. Interestingly, doctors assigned less significance to their own behaviour compared to the parent’s behaviour. While 25 doctors fully agreed with the statement that a child’s involvement in decision-making depends on whether the doctor provides such an opportunity, 34 doctors fully agreed that a child’s involvement in decision-making depends on the parent’s behaviour.
The vast majority of the doctors agreed that a child’s participation in decision-making depends on the child’s age and intellectual abilities. In the doctors’ views, a child’s ability of self-expression and previous experience with their health have less influence on their effective participation.
Doctors’ approaches to child-parent disagreement
Children and parents do not always agree on the question of medical intervention. The analysis revealed three approaches that doctors take in such situations.
According to doctors, the child-parent common or shared autonomy is most spread: the doctor asks the child and the parent to discuss the matter among themselves and to try to come to an agreement. Two sub-patterns emerged within this approach. Within the first sub-pattern, the doctor leaves the process of finding an agreement clearly in the hands of the parent and the child, e.g.: “I leave them to clarify the matter among themselves”; “I ask them to clarify the matter at home and to come back once they have reached an agreement”. The above shows that doctors are reluctant to interfere in family relations and they do not want to override parental authority. Within the second sub-pattern, the doctors see themselves as being part of the process of coming to an agreement, e.g.: “I try to find a compromise”; “I communicate and explain, as long as it takes to reach an agreement”; “I have to convince the party that does not agree with my medical opinion on this issue”.
The second approach practiced by doctors in cases of child-parent disagreement is parent-centred. The doctors are of the opinion that they cannot overrule the parent’s decision, e.g.: “I have to accept the decision of a parent who is the legal guardian of the child”; “Until the age of 18, it’s the parent’s decision”.
The third approach of the doctors where the doctor is child-centred and supportive of the child’s autonomy is rare, e.g.: “I explain to the parent that the child has the right to decide on his/her health”; “I tend to be on the child’s side”.
The analysis showed that doctors used explaining, persuading, giving additional time for thinking or a new time for another appointment most often when there were disagreements between the parent and the child.
Assessment of children’s decision-making capacity
In order to analyse the process of realisation of autonomy, we aimed to understand how doctors judge the ability of children to make autonomous decisions (decision-making capacity). The analysis shows (Figure 2) that child-based aspects are the most important: with one or two exceptions, the doctors agreed that they consider the child’s ability to understand the shared information; to form a view based on that information; the child’s age, and the child’s intellectual abilities. A child’s ability of self-expression is less important for doctors, yet they consider this essential in doctor-patient communication. The fact that a child has visited the doctor alone is the least considered factor when assessing the child’s decision-making capacity. The assessment of parents of their child’s decision-making capacity and the child’s own evaluation have less relevance for doctors compared to other aspects. Moreover, the study reveals that a child’s own evaluation of his/her decision-making capacity may be more relevant for the doctor than the estimation of the child’s parent of the same.
Other factors noted by doctors included chronic illness, and the seriousness of the decision in question when assessing a child’s ability to make autonomous decisions. “If it’s about an issue that puts the child’s life in danger or has high risks, then the issue definitely needs to be discussed more and with more involvement of the parents compared to treating a simple cold’.
Discussion
Children’s autonomy is relational
The results of this study confirm that children’s autonomy is a relational phenomenon. The child and the adults form a healthcare relationship where they have effect on each other and each other’s behaviour (Alanen, 2014; Alderson, 2007; Kuczynski, 2003), and their relationship is in constant change. The experiences of doctors revealed in this study confirm that ‘children are able to intervene in the world or to refrain from such intervention’ (Kuczynski, 2003), thereby influencing the processes in which they participate. In this process, doctors change their patterns of behaviour according to the child’s age, initiative, involvement and communicative capacities, which proves that children’s autonomy is relationally negotiated (Greene and Nixon, 2020; Mayall 2015). However, the child and the adult parties of the relationship are unequal in resources of power in the process of negotiations of autonomy (Kuczynski et al., 2014). In child healthcare, the relational autonomy functions in a unique triangle – three individuals meet in a healthcare setting: a child who has a health issue, his/her parent who exercises parental authority and a doctor who exercises professional authority. The patient is represented by two individuals (patient’s duality), and therefore relationality functions on three axes: child-doctor, child-parent, and parent-doctor. Power alliances may be formed between any two of the parties depending on the situation and conformity of their views. Most contemporary scholarship on child-parent relations accepts the bidirectional model of causality (Kuczinsky, 2003), acknowledging that both the parent and the child influence each other’s behaviour and actions. This study allows us to assume that interdependency functions in a similar way in the child-doctor relationship as discussed herein.
Models of patient autonomy in cases of child-parent disagreement
The central interest of this study was the question of how autonomy is exercised in the child-doctor-parent relationship. The patient’s duality renders this a complex process – the child and the parent may disagree on the question of medical intervention. We asked doctors to reflect on their practice in cases of child-parent disagreement. Three models emerged from the analysis: a child-parent shared autonomy model, parent-centred model and child-centred model (Figure 3). Models of patient autonomy in cases of child-parent disagreement. Note: As neither the parent-centred, nor the child-centred model fully excludes the third party, the relationship of the third party with the others is marked with a dotted line.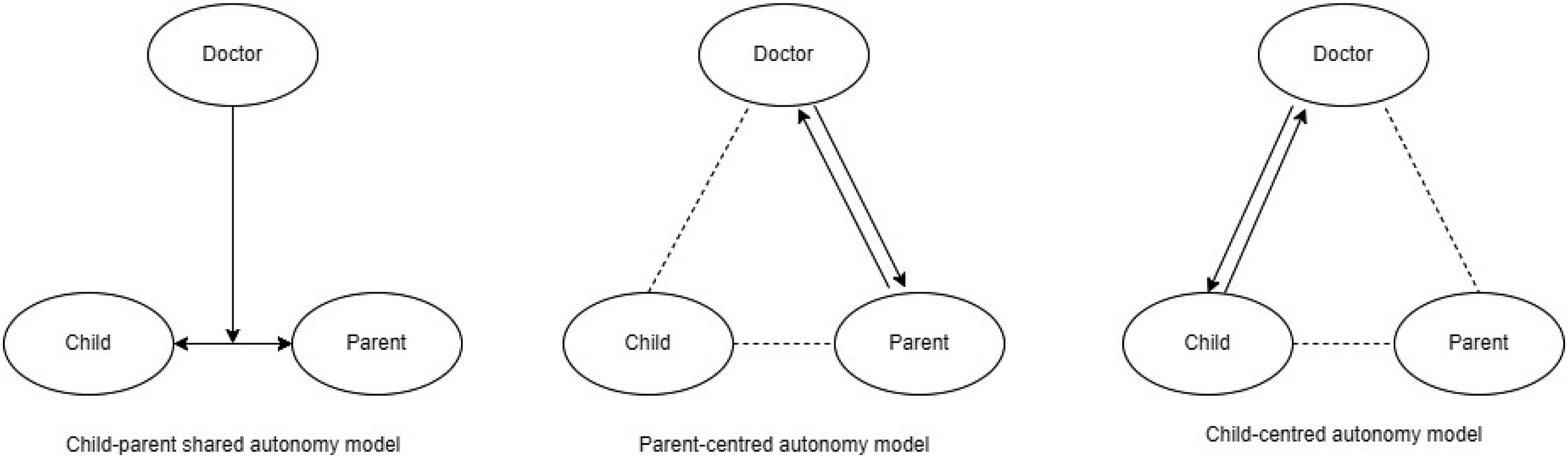
Child-parent shared autonomy model
The child-parent shared autonomy model is applied most often by the doctors in cases of child-parent disagreement, i.e. the doctor asks the child and the parent to discuss the matter among themselves until they come to an agreement. Such approach acknowledges the interdependence between the child and the parent, and the parent’s effectiveness as an agent that is supported by their knowledge of the child (Kuczynski et al., 2014). Parents have relational resources vis-à-vis their children (and vice versa) deriving from their long-term close relationship (Kuczynski, 2003). A doctor’s choice to encourage the child and the parent to find an agreement capitalises on such resources.
This approach, despite its respect for child-parent mutual interdependence, involves several problematic aspects. First, the child and the parent are not equal in their power (Kuczynski, 2003), and leaving them to solve their disagreement may leave the child vulnerable and restrain his/her autonomy. The doctor, having professional authority and expertise, can encourage the parent to consider the child’s position. However, a doctor’s distancing from the child-parent disagreement raises both an ethical and legal dilemma. If the doctor considers the child capable to decide autonomously and the child’s choice is rational from a medical point of view, it may be unethical or even illegal (under Estonian law) to leave resolution of the issue to the sole discretion of the child and parent. The doctor has the legal power to intervene and avoid overuse of parental power. The doctor is a professional who should be aware of the law governing a child-patient’s autonomy. Thus, the child’s autonomy will depend on how the doctor and parent resolve their power relations and how the doctor’s professional authority and medical expertise balance against parental authority and knowledge of the child. The study revealed that it is a common practice among doctors not to intervene in the child-parent relationship. This may be an appropriate solution in some cases but not in others. Leaving the issue in the hands of the ‘dual patient’ may mean that the child will not get adequate treatment.
Parent-centred autonomy model
The parent-centred autonomy model uncovers recognition of parental power by doctors. Parents are the legal guardians of their children, and doctors may not wish to override parental authority. The study showed that one reason for such approach might be the fact that not all doctors are aware of the special legal rules regulating child-patient consent or they may be aware of them but are reluctant to apply them in practice. Finding the proper balance between respect for a parent’s authority and respect for a child’s autonomy is a complex relational process, which may be influenced by a doctor’s lack of time and/or insufficient knowledge of children’s rights.
In the parent-centred model, the child’s right to autonomy is disrespected because he/she is kept away from the decision-making process. Similarly to the shared autonomy model, the doctor has an ethical and/or legal obligation to respect the child’s autonomy and thus may be the only person who could influence the parent’s behaviour. Ultimately, acceptance of the sole power of the parent may leave the child without adequate medical treatment.
Child-centred autonomy model
The child-centred autonomy model regards the child as a primary agent executing patient’s rights. According to this study, such practice among doctors is rare. Although the child-centred model may seem ideal based on the CRC, it also involves certain risks. According to a common understanding, a parent is the best expert on his/her child and will act in the best interests of the child. Doctors usually do not have relational resources similar to those of parents and therefore may need the assistance of parents. If doctors avoid involving parents, they may lose valuable information and expertise, and this may influence the quality of medical judgement. It is often the case that the doctor and the child have contact only for a short time during an appointment, and the doctor may therefore lack time to make a proper and thorough assessment of the child’s capacities. In the present study, more than one-half of doctors found that a lack of time hinders assessment of children’s decision-making capacity. This may be one of the reasons why child-centredness in healthcare relationships is rare.
A synthesis of models
To overcome the challenges of the above models, we present a synthesis of them (Figure 4). The new model is child-centred, considers the relational nature of autonomy, accepts the rights of the child under the CRC – above all the right to self-determination – and is non-hierarchical (Figure 4). Child-centred relational autonomy model.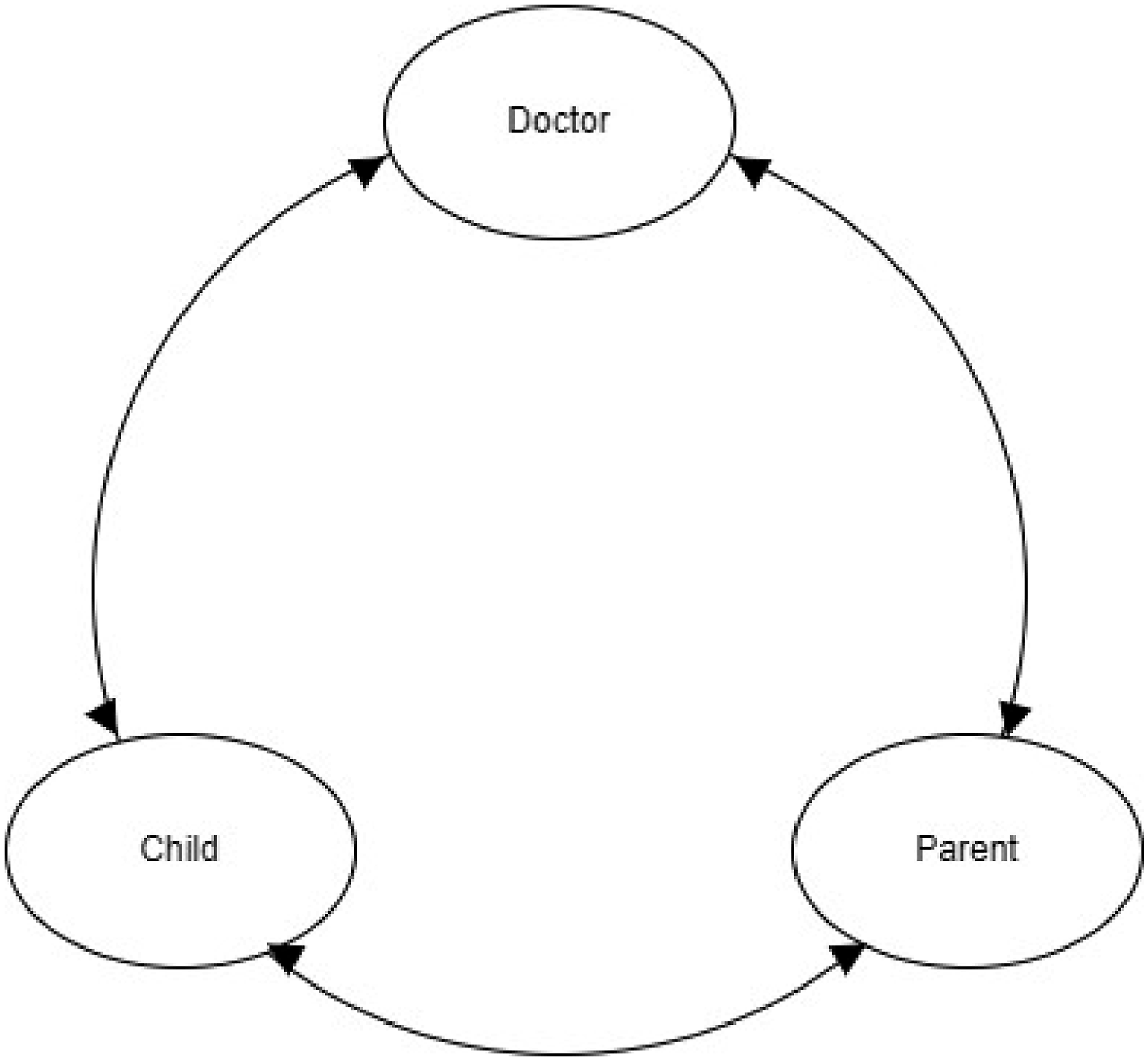
According to this child-centred relational autonomy model, each party understands his/her role and is aware of the rights framework of a healthcare relationship. It is guided by newer concepts of interdependent power asymmetry and acknowledges that both children and adults have relational resources to influence one another (Kuczynski, 2003). Inspired by Kuczynski’s framework analysis of child-parent interaction (2003), this model is neither vertical nor static, but is visualised through circular causality. All three parties of the relationship are involved in communication and negotiations, and their interaction produces the child’s autonomy in a constant circulation. Child-centredness means that the adult parties understand and acknowledge that the child is the patient, and both the doctor and the parent support the child’s autonomous decision-making by offering advice and explaining alternatives. The child’s autonomy is growing gradually according to his/her actual knowledge, experience and understanding, i.e. evolving capacities, whereas the adult parties gradually reduce their intervention and directions (Arts. 5 and 12 CRC). Such fluid autonomy model serves the concept of evolving capacities better than models that determine specific stages of a child’s consent according to intervals of age limits, as it is regulated in some countries, since it is not possible to draw age-based lines between the stages of independence. Open and trustworthy communication between all parties is a central value of a child-centred relational autonomy model. In terms of the principle of informed consent, this model assumes that both the child and the parent give their informed consent to treatment. It could be conceptualised as shared consent, similarly to shared autonomy.
The proposed model is applicable in situations that involve all three parties – the child, the doctor and the parent. Domestic laws in many countries stipulate an age limit from which a child acquires full patient’s rights, or enable doctors to consider a child to be an autonomous patient. Such cases remain outside of this model. It is also evident that using such a child-centred model in emergency situations or with very young children or children with disabilities is demanding for doctors, and requires special training. The challenge remains for all health practitioners to assess the necessary level of participation of children on a case-by-case basis.
Conclusion
A child-patient’s autonomy is produced in an interdependent relationship. Being fluid by its nature child-patient’s autonomy is in constant change. From a generational perspective, the child is dependent on the decision of the adults, while the adults take responsibility for the child’s welfare, including health issues. From the perspective of power, doctors have medical expertise and professional authority, while parents hold parental authority and know their children best. According to this study, the amount of involvement shared between a parent and a child depends mainly on the child’s age and decision-making capacity, the exercise of parental power and the doctor’s willingness to intervene in this by exercising their professional authority.
This research contributes to the field of childhood and children’s rights studies with a transdisciplinary approach to child-patient autonomy that builds on relationality and interdependence.
Limitations
This study is pioneering in Estonia as exploratory research on child-patient autonomy in healthcare. It involved a limited number of participants and their reflections, and does not therefore allow for generalised conclusions. Moreover, it focuses on the views of doctors only; examination of the entire child-doctor-parent relationship will follow in further publications.
Footnotes
Acknowledgements
The authors are grateful to Kadri Soo and Mai Beilmann for their kind help in the data preparation process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eesti Teadusagentuur, Grant PRG700.