
Abstract
Donating blood (components) is considered a “good deed,” especially in voluntary, nonremunerated contexts where blood is donated for unknown recipients. For donor and recipient safety, blood banks apply deferral criteria. Deferred donors are less likely to return for future donations. Based on theory (e.g., on emotion, habit, and identity) and practice, several methods have been suggested to encourage return after deferral, yet few of these methods have been tested in rigorous study designs, or in the field. In this study, we therefore investigated whether offering an alternative “good deed” or providing additional information about deferral would increase donor return. Results of a randomized controlled field trial at 10 Dutch blood donation centers showed that offering alternative good deeds after deferral did not significantly increase donor return, while providing additional information did increase whole blood donor return. This suggests that additional information contributes to the continuation of pro-social behavior.
Introduction
Blood transfusions or treatments with blood products to help patients can only exist by the grace of donors donating their blood (components). In line with guidelines from the World Health Organization (WHO), donors in many parts of the world donate blood voluntarily, often nonremunerated. Considering that these donors generally do not know who will receive their blood (product) after donating, donating blood is considered a “good deed” to a stranger, that is, a costly behavior and personal sacrifice to contribute to a public good (Ferguson & Masser, 2018).
To ensure both donor and patient safety, blood banks employ deferral guidelines. For instance, donors may not donate if they have traveled to a virus-endemic area because they may have attracted a viral infection which could be transmitted to the transfusion recipient after donation (patient safety). Or their donation may be deferred if their hemoglobin levels are too low, to protect them from anemia (donor safety). Donors who are aware of these deferral guidelines may self-defer their donation and postpone their visit, but many donors will find out only at the donation location that they are not allowed to donate at that time. For example, at Dutch donation centers, around 10% of whole blood (WB) and 4% of plasma donation attempts are deferred (De Groot et al., 2015). The duration of such on-site deferrals varies from one day to a few years.
Even though donors are very welcome to come back after a deferral, many of them never return (Custer et al., 2011; Hillgrove et al., 2011; Spekman et al., 2019). Thus, even though the deferral policies ensure the safety of the blood supply, they might hinder donors in enacting upon their motivation and intention to perform a good deed.
In this study, we specifically focus on blood donor deferrals, but there are other examples of refusing volunteers or donors for pro-social behavior. For instance, during the 2021 floods in Western Europe, many people volunteered to help clean up the affected areas. Yet, the number of would-be volunteers was so high that many were refused because the responsible organizations feared safety risks. Similarly, in Iraq, an earthquake in 2017 mobilized large crowds of volunteers, yet mismatches between supply and demand caused many of them to return home without having been able to help (Sharififar et al., 2021). Several of the volunteers who were unable to help said that they would not volunteer again in case another earthquake would occur.
Because retention of blood donors is often safer and more cost-efficient than recruiting new donors (Bagot et al., 2016; Devine et al., 2007), blood banks are looking for ways to increase the return of deferred donors. While many strategies to mitigate the effect of on-site deferral on return have been suggested, few have actually been tested (Davison et al., 2020; Gemelli et al., 2021a). Furthermore, studies that rigorously test such interventions (using experimental designs such as randomized controlled trials [RCTs]) are currently quite scarce in blood donor research (Godin et al., 2012), especially when conducted through field studies. In this paper, we report on a randomized controlled field trial in which we investigated whether offering alternative “good deeds” and providing additional information about the background and need of deferrals resulted in an increased return rate of on-site deferred donors. This study tests theoretically derived hypotheses on pro-social behavior in a field study, and the information gained from this study contributes to the literature about sustaining pro-social behavior. Blood bank agencies, in particular, may benefit by using these results to target and improve their retention strategies for deferred donors.
Motivations to Donate Blood (Repeatedly)
Several mechanisms have been suggested in the literature that may explain why people donate blood or plasma and do so repeatedly. These mechanisms fit into more general theories about (motivations for) pro-social behavior (e.g., Feigin et al., 2014), such as theories on habit formation in volunteer behavior (Rosen & Sims, 2011), on donor role identity (Piliavin et al., 2002), and on the role of emotions in pro-social behavior (e.g., Van Kleef & Lelieveld, 2022).
One mechanism to explain repeated pro-social behavior is habit formation. In the case of blood donation, donors accumulate experience in donating and their repeat donation behavior leads to the formation of donation habits. After several donations, donating changes from a deliberate, conscious decision to a habitual, automatic behavior that is not given much thought (Bednall et al., 2013; Masser et al., 2008). Especially among plasma donors, such habits may be easily formed (Masser & Bagot, 2015), as they are generally allowed to donate more frequently (up to 26 times per year in Australia; Bove et al., 2011) than WB donors.
Repeated donations can also contribute to formation and strengthening of the blood donor role identity. Role identities are inextricably linked to the behaviors that are associated to that role (Masser et al., 2008), and (the recognition of) successful role performances are essential for legitimizing such role identities (Hillgrove et al., 2012). In the case of blood donation, donors display and strengthen their donor identity by donating blood or plasma and by being recognized for doing so. By repeatedly donating, the donor further internalizes and strengthens this donor identity (Masser et al., 2008).
The emotional experience of donating may also play a role. As it turns out, many blood donors not only donate to help others and contribute to a public good (i.e., pure altruism), but also to experience pride (Ferguson et al., 2019), the joy of giving (Andreoni, 1989), or feel good about themselves, an emotion referred to as warm glow (Ferguson & Lawrence, 2016).
On-site deferral may disrupt these mechanisms. Deferred donors are unable to help others and do not experience the pride, joy, or warm glow they anticipated (Clement et al., 2016; Ferguson et al., 2019), which may result in nonreturn. Being deferred also disrupts the donation habit (Davison et al., 2020), and makes that donors are unable to act upon their donor identity, which may weaken it (Hillgrove et al., 2012; Thorpe et al., 2020). Moreover, strong donor identities lead to more resilience toward negative events such as deferral (Masser et al., 2008), as evidenced by higher return rates among donors deferred for low hemoglobin with a strong donor identity than among those with a less strong donor identity (Hillgrove et al., 2012).
Offering an Alternative to Donating Blood
Because deferral may disrupt donation habits, weaken donor identities, and block the experience of positive emotions after donating, it seems worthwhile to offer on-site deferred donors an alternative instead of letting them leave again empty-handed. Providing such an alternative—especially when related to the transfusion service—may (to a certain extent) prevent weakening of the donor identity, and may in turn increase the chances of return. In addition, offering an alternative good deed may also induce positive emotions such as pride or warm glow, and thus retain donors for future donations.
Following this, Clement et al. (2016) performed field experiments in which they offered an alternative good deed to deferred donors at donation sites of the German Red Cross. They compared a strategy to increase the return of deferred donors (i.e., an alternative good deed in the form of painting part of a larger painting to be offered to a children’s hospital) against the standard procedure (i.e., a small thank-you gift). Results showed that offering the alternative significantly increased the return rate of deferred donors compared with the standard procedure—from 53% to 73%.
Thus, deferral may disrupt donation habits, weaken donor identities, and block the experience of positive emotions after donating. Blood donors are likely to extend their pro-sociality to related good deeds (Ferguson et al., 2018), and offering an alternative good deed may aid donors in fulfilling their aim for contributing to the transfusion service. In performing an alternative good deed, donors may be enabled to experience some pride or warm glow and their donor identity and donation habit may be harmed less, especially when the alternative offered is related to the transfusion service (i.e., it speaks to their donor identity). This in turn may lead to a lower risk of lapse. Hence, we hypothesize that offering a deferred donor an alternative to donation leads to an increased likelihood of return (Hypothesis 1).
Providing Extra Information About Deferral
Being deferred not only means not being able to experience positive emotions, but it can also evoke negative emotions such as anger, frustration, disappointment, annoyance, and rejection (Hillgrove et al., 2012), particularly when the deferral takes place on-site (Gemelli et al., 2018). Even though effects of such negative emotions are relatively small and those emotions generally fade rather quickly (Gemelli et al., 2018; Hillgrove et al., 2012), high levels of anger and low levels of calmness were still found to negatively affect donor return (Gemelli et al., 2018). In addition, deferred donors may feel as if they are not as healthy as they were before (Bove et al., 2011; Hillgrove et al., 2012; Zeiler et al., 2014). When donors perceive themselves as less healthy and capable donors, this affects their expectations of future donation attempts (Hillgrove et al., 2012) and this may cause them to drop out. To address these effects, better informing donors about deferral may prevent them from experiencing negative emotions and feeling incompetent.
Unfortunately, however, deferred donors are generally provided with relatively little information (Compernolle, 2017). Moreover, they do not always understand the information provided by professional collection staff regarding their deferral (Gemelli et al., 2018), similar to patients in medical situations that do not (correctly) process all of the information they are provided with (Medendorp et al., 2017). This may coincide with the (false) idea of some donors that their deferral is in fact permanent (Mathew et al., 2007). Such misunderstandings and lack of information may lead donors to not returning after having been deferred.
To address the lack of donors’ knowledge about deferral, Gemelli et al. (2021a) performed a trial in which on-site deferred donors were provided with a combination of a brochure about deferral, a guided conversation with a member of the collection staff, and a follow-up e-mail. This combination condition was compared with a condition in which donors received the follow-up e-mail only, and to a “business as usual” control condition (i.e., no additional information provided). Results of this trial showed that providing educational materials increased donors’ knowledge and understanding about their deferral, regardless of whether the donors received the combination of materials or the follow-up e-mail only. However, they also found that donors who received the combination were more likely to rebook a next donation appointment than the donors in the other two conditions.
Thus, on-site deferral can lead to negative emotions in donors and a relatively high information need. Providing accurate information about the importance of deferral policies for the donor’s own health and that of the recipient, and about the temporary nature of the deferral may prevent deferred donors from feeling sad, frustrated, incompetent, or confused. Hence, we hypothesize that providing deferred donors with (additional) information about deferral and emphasizing that their return would be appreciated after the deferral expires leads to a higher likelihood of return (Hypothesis 2).
Offering a Choice
Even though providing additional information or offering an alternative good deed may work for some donors, not all donors may be equally excited about these alternatives. For instance, someone who has already experienced several deferrals may not have the same information need as someone who is deferred for the first time, and some donors may lack the skill or desire to contribute in a creative way (such as the painting in the study by Clement et al. (2016)). Therefore, we want to explore whether providing a choice between alternative good deeds and additional information increases return in deferred donors. In addition, knowing which choices deferred donors make can help in determining what kind of alternatives to offer.
Method
Participants and Design
Sanquin is by law solely responsible for the entire blood supply chain from collection to testing, processing, and distribution of blood products in the Netherlands. This supply chain is fully dependent on voluntary, nonremunerated donations. Registered donors are invited to donate at one of the 50 fixed donation locations, or—for WB donors only—at one of the 85 mobile donation locations. When their blood type is in demand, WB donors receive a card in the mail to invite them to donate within a specified 2-week walk-in period at a fixed location, or for a specific date at the mobile locations. Plasma donors generally make an appointment for their next donation when they present for donation at the location. Upon arrival at the donation center, donors present at the registration desk, after which they fill out the Donor Health Questionnaire. This questionnaire is then discussed with a member of the collection staff to determine eligibility. If all is well, the donor is allowed to donate. If, for some reason, the donor is temporarily not allowed to donate, Sanquin’s procedures prescribe that the donor is informed about the deferral reason and the length of the deferral period.
We performed an RCT—approved by Sanquin’s Ethical Advisory Board—in the field at 10 fixed donation locations throughout the Netherlands. Initially, the eight largest donation locations were included as of January 2019 for their high number of potential participants and spread across the country. After a call in April for additional locations to include in the study, two other, slightly smaller, locations joined as of May 2019. Donors that were deferred on-site during the study period (January–September 2019) at one of these locations were eligible for inclusion. Newly registered donors were excluded because the first visit to Sanquin is not a standard donation but rather consists of an elaborate health check and the drawing of 10 mL of blood for testing purposes.
Employees of the participating donation locations were instructed to invite donors that met the inclusion criteria to participate in the study immediately after the donor was informed about the deferral. In addition to the regular procedure for on-site deferral, donors received an information leaflet about the study and signed an informed consent form if they agreed to participate. Upon participation, the employee opened an envelope to see which condition the participant would be assigned to, the options being either one of two alternative good deeds, additional information about the deferral process, or a choice between the alternative good deeds and additional information. Each envelope contained a short instruction of the assigned condition. The employee then ticked the box of the assigned condition on the informed consent form and provided the donor with the respective materials. For donors in the alternative good deed conditions, a special collection box was placed close by the registration desk where they could return the questionnaire or postcard for a transfusion patient once finished. All finished questionnaires and postcards were collected by the researcher for analysis (in the case of the questionnaires) or distribution (in the case of the postcards). No one-on-one checks were performed to determine whether or not the donor had completed their assigned condition.
A total of 8,396 deferred donors met our inclusion criteria. Because of the additional paperwork and time it would take for employees at the participating locations, it was not registered whether all donors that met the inclusion criteria were actually approached for the study, and how many of them did not want to participate. In the end, 660 (8%) of all donors that met the inclusion criteria actually participated in the trial (Figure 1).
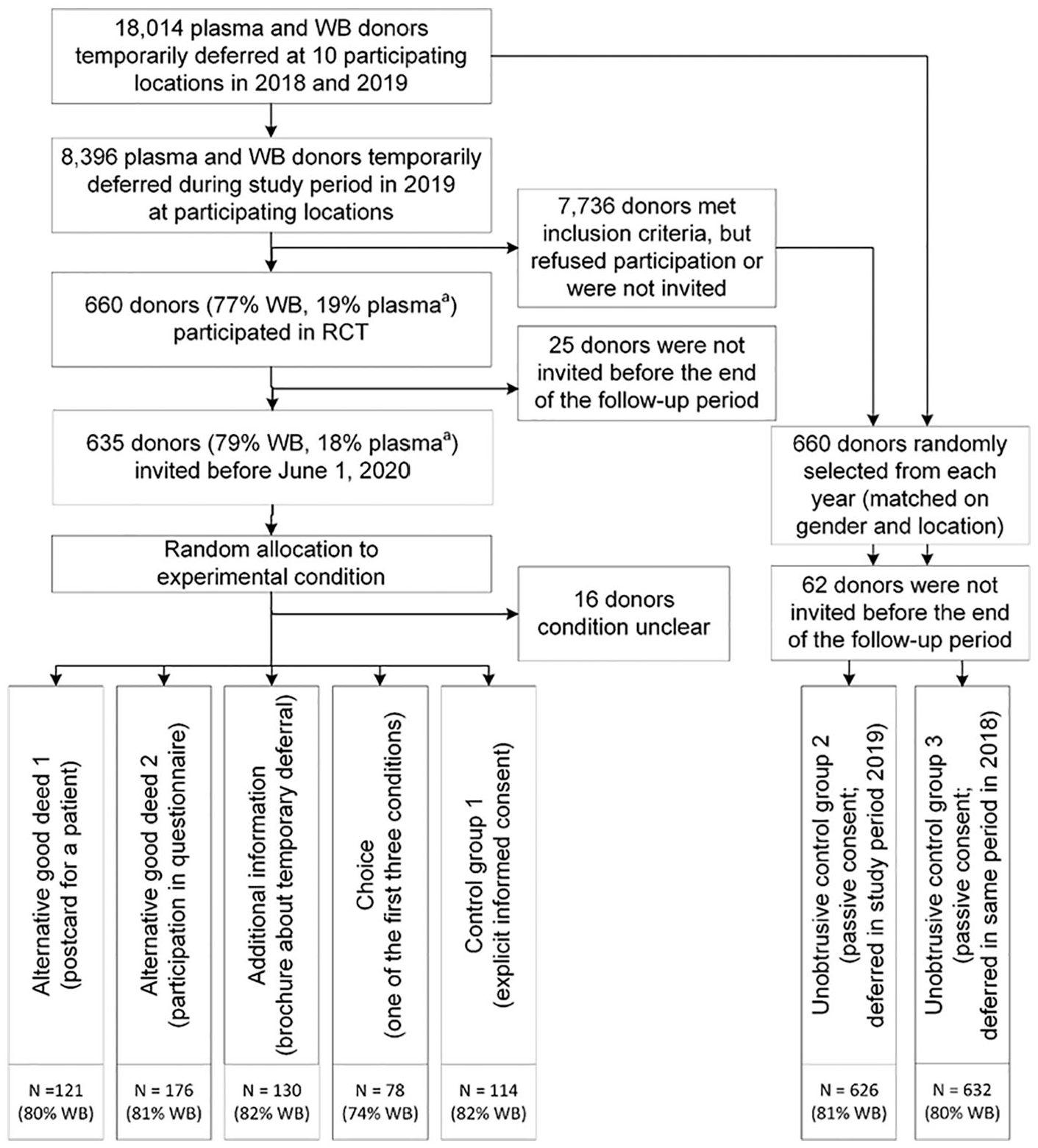
Flowchart for inclusion in experimental and control groups.
For all donors in the study, we tracked their return behavior up until 4 weeks after they had received the first invitation after their deferral expired, or until the end of the follow-up period (June 1 of the next year, i.e., 2020 for RCT participants); whatever came first. Donors that returned on their own initiative before receiving an invitation (2% of RCT participants) were retained for analyses. Donors that did not receive an invitation and also did not return before the last day of the follow-up period (4% of RCT participants) were not included in the analyses. Among the remaining donors, 81% were WB and 19% were plasma donors. Their average age was 35.8 (SD = 15.1) and 72% was female. The majority was deferred for low Hb (63%), followed by short-term medical deferral (18%), and travel to virus-endemic areas (12%).
Conditions
The RCT included four experimental conditions and a control condition. We added two external control conditions for comparison purposes. Figure 1 presents an overview of the study design and the number of participants included.
In consultation with the collection staff managers, we decided on two alternative good deeds that could be performed individually by donors and that required minimal support from the collection staff. Both these alternatives were framed as “helping out the transfusion service in a different way.” The conditions are described in detail below, and all materials used can be found on the paper’s OSF project page (https://osf.io/e8q2d).
In the first condition, participants were offered the opportunity to perform an alternative good deed by writing or drawing a postcard to hearten a patient receiving a transfusion. Participants in this condition were informed by the collection site staff as follows: Unfortunately, you cannot donate blood/plasma today, but you can “give” in a different way. If you want, you can write or draw a postcard for someone in the hospital that needs a transfusion. Cards, pens, pencils, and a number of examples are available at the refreshment area. When you are finished, you may return the card in the designated mailbox at the reception.
Participants could choose from a variety of cards with or without preprinted text and images, so they could draw and write as much or as little as they wanted on the card. The preprinted cards included images of pelicans (cf. Sanquin’s logo) or facts about blood donation (e.g., “One in every seven people needs blood during their life”). Thus, by writing a card, donors could still “do something” for a patient and contribute to the transfusion service.
In the second condition, participants were also offered an alternative good deed. This time, however, the alternative was presented as helping out the blood bank instead of a patient. Donors were informed as follows: Unfortunately, you cannot donate blood/plasma today, but you can “give” in a different way. If you want, you can fill out a questionnaire to help Sanquin get more insight into the experiences of her donors. When you are finished, you may return the completed questionnaire in the designated mailbox at the reception.
This paper-and-pencil questionnaire contained items to assess the emotional experience of the deferral, intention to return for a future donation, donor self-efficacy, satisfaction with the blood bank, experienced pressure to donate, personality, and blood donor role identity.
In the third condition, participants were offered additional information about deferral in the form of an information brochure. Sanquin’s current procedures require deferred donors to be informed of the reason and duration of the deferral, but no specification exists about how exactly donors should be informed. The information brochure was offered to the donors as follows: You will receive the information brochure “Deferral.” In this brochure, you will find extra information about the purpose and importance of deferral. In addition, it also contains information about the most common reasons for deferral and what you could possibly do yourself to prevent this from happening in the future. You can take this brochure home with you so you can read it or refer back to it at your own convenience.
The brochure was formatted in Sanquin’s corporate design and developed together with donor physicians. It included general information about deferral (i.e., to protect both donors and recipients), about the most common reasons for deferral (low Hb and travel), advice to prevent future deferrals (to the extent possible), and ended with explicitly mentioning that the donor’s return after the expiration of the deferral period would be greatly appreciated.
The fourth condition offered participants a choice between the first three conditions. Instructions were the same as for these conditions, except that donors were first informed that they could choose one of the three options.
Finally, we included three control groups to compare the effects of the experimental conditions with. The first control group was part of the RCT and consisted of donors that were explicitly asked to participate in the study and sign the informed consent form, yet they were not offered an alternative (due to their random allocation to the control condition) and sent on their way. Donors in this condition received a little bit of extra attention compared with the regular procedure followed with on-site deferred donors: You are in the control group. This means that you will not be offered an alternative to donating and you are free to leave. Your participation is very valuable to us, as it enables us to compare the data from all participants in the control group (including yours) to the data of donors in the other groups.
To rule out potential observer (or Hawthorne) effects that such an explicit, active request for participation could elicit even in the control group (McCarney et al., 2007), we included a control group existing of donors that met our inclusion criteria (i.e., deferred on-site at a participating location in 2019), but did not participate in the RCT. This group was unobtrusively followed, which they passively consented to via a question on the Donor Health Questionnaire (asking whether their data could be used for research purposes). Because this group may be different from the participants in the experimental conditions (for instance, due to self-selection bias of RCT participants), we added another, unobtrusively followed control group consisting of donors that met the inclusion criteria in the same time period in the year before the study (i.e., January–September 2018). These two control groups are referred to as the two unobtrusive control groups from hereon.
Because the number of donors that met our inclusion criteria for the two unobtrusive control groups was large (N = 7,736 and N = 9,618 for 2019 and 2018, respectively), we matched these control groups to the 660 participants in the RCT in terms of gender and donation location and then randomly selected participants to include (see supplemental materials on the OSF project page for a detailed description of the matching procedure). After excluding participants who were still deferred or not invited before the end of the follow-up period, we ended up with two unobtrusive control groups that were similar in size to the RCT participants (see Figure 1). The two control groups were perfectly matched in terms of gender and location, but were somewhat different in terms of age, reason for deferral, and deferral duration (see Table 1, and Table S1 in the supplemental materials for pre- and post-matching comparisons). RCT participants were somewhat younger on average than the donors in both matched control groups, F(2, 1,874) = 4.2, p = .02, ƞp2 = .004, and were more often deferred for low Hb, χ2(8) = 37.8, p < .001. With regard to the duration of the deferral, donors in the unobtrusive control group in 2019 were deferred for a shorter amount of time than donors from the other unobtrusive control group and RCT participants, F(2, 1,874) = 7.3, p = .001, ƞp2 = .008.
Composition of RCT Participants in Comparison to Matched Unobtrusive Control Groups.
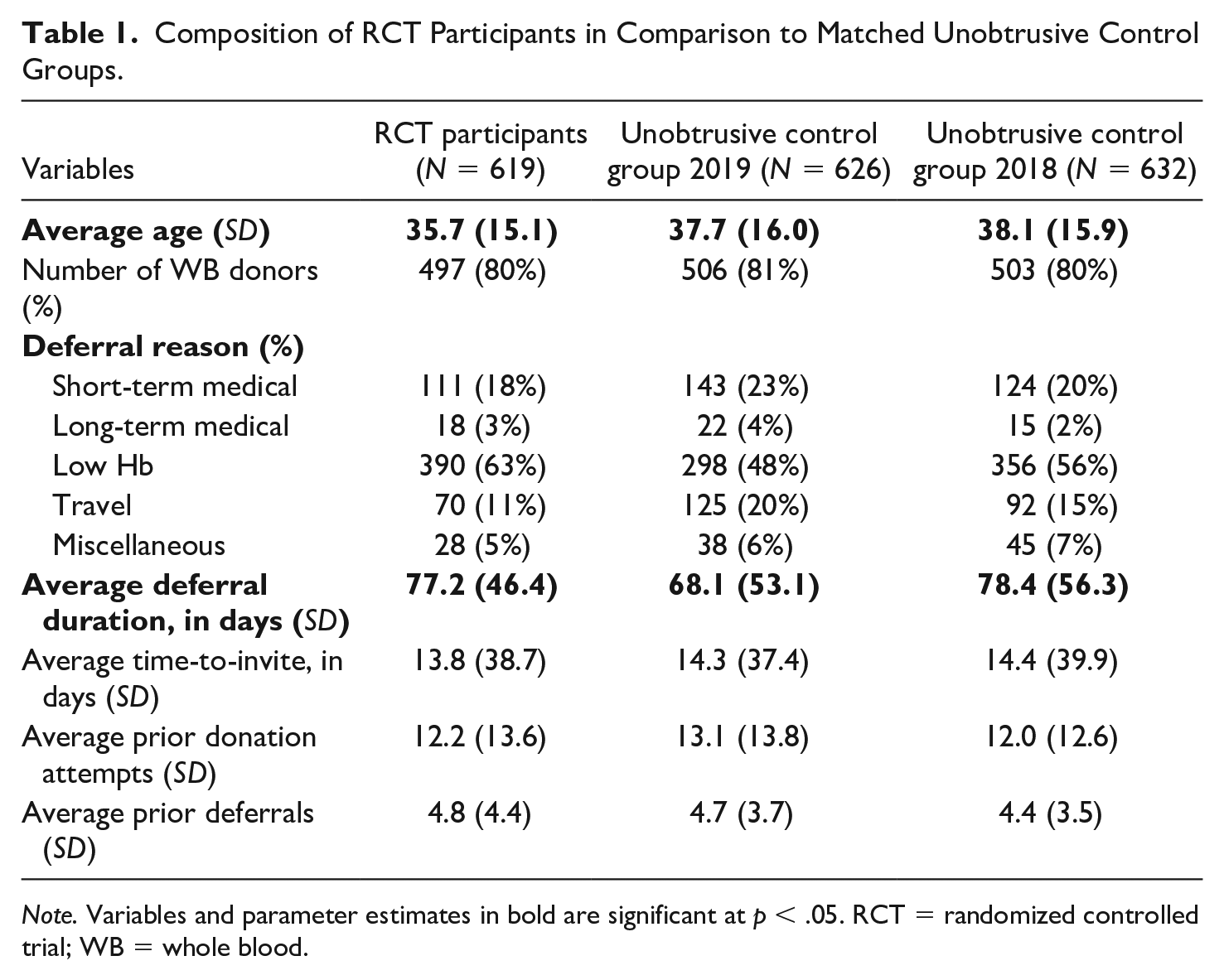
Note. Variables and parameter estimates in bold are significant at p < .05. RCT = randomized controlled trial; WB = whole blood.
Measures
Donor return
Donor return was assessed by establishing whether or not the donor returned within a period of 4 weeks after the donor was invited again for a donation attempt (after their deferral had expired). This information was retrieved from Sanquin’s donor registry.
Deferral reason
For each participant, the reason for deferral was retrieved from the donor registry and categorized into one of five categories: Hb, travel, medical short-term, medical long-term, and miscellaneous (cf. Spekman et al., 2019).
Demographic information
Information was retrieved from the donor registry about donors’ gender, age at the time of the deferred donation attempt, donation type (plasma = 0; WB = 1), number of prior donation attempts (since 2012, regardless of donation type and whether attempts were successful or not), and prior deferrals (since 2012, including both on-site and self-deferrals).
Deferral duration
The duration of the deferral is the difference between the date of the deferred donation attempt and the date the deferral expired, in days.
Time-to-invite
Time-to-invite is the number of days between the end of the deferral and the date of the first invitation to donate again. Time-to-invite was set to 0 for donors who were invited or who returned before their deferral had expired (or both; n = 10), and for donors who returned after deferral expiration but before they received an invitation (n = 62).
Analyses
We first conduct descriptive statistics related to the choice condition. Next, we test for differences in return between the RCT participants and the two unobtrusive control groups using a chi-square test. To test our hypotheses, we use hierarchical logistic regression of return within 4 weeks, in which we add covariates related to deferral and return in model 1 (i.e., deferral duration, time-to-invite, deferral reason, number of prior donation attempts, and number of prior deferrals), followed by the experimental conditions in model 2 (i.e., dummies for our conditions and unobtrusive control groups, with the RCT’s control group as the reference group), and demographic covariates in model 3 (i.e., age and gender). Because plasma donors and WB donors are treated differently at the blood bank (i.e., the invitation process is different and not all deferral guidelines apply to plasma donors and WB donors alike), we stratify our analyses for these two groups of donors. Next, we reassign participants in the choice condition to their chosen condition and repeat the analyses for further insight into the effects of giving donors a choice between the alternatives.
Results
Before testing our hypotheses, we first looked at donors in the choice condition (n = 78). Filling out a questionnaire was chosen by 39 donors. Others chose the postcard (19 donors) or receiving additional information (16 donors). Two donors chose to be part of the control group, and for two donors no information on their choice was available.
Out of the 619 participants of the RCT that had the opportunity to return and of whom the treatment condition was known, 365 (59%) had returned within 4 weeks after receiving a new invitation when the deferral period had ended or even before receiving an invitation. This was similar to the return percentages among the unobtrusive control groups (i.e., 58% and 57% for the 2019 and 2018 control groups, respectively), χ2(2) = .54, p = .76. Among the RCT conditions, return was highest for donors that had received additional information (65%), followed by the alternative good deeds (60% for the questionnaire and 57% for the card), the choice condition (55%), and the control group (54%); these percentages were not significantly different, χ2(4) = 4.0, p = .41. When we stratified results for whole blood and plasma donation, we found a lower percentage of return overall among whole blood donors (50%; N = 1,506) than among plasma donors (91%; N = 371). For whole blood donors, we found that donors that received additional information had the highest return (60%; confidence interval [CI] = [50%, 69%]), followed by the questionnaire (53%; CI = [45%, 61%]), the card and the control group (both 46%; CIs = [37%, 56%] and [36%, 56%], respectively), and, finally, the choice condition (45%; CI = [33%, 58%]), χ2(4) = 6.1, p = .19. Although the return rates in the five conditions do not differ significantly overall, based on the CIs, it appears that the return rate in the additional information condition (60%; CI = [50%, 69%]) is higher than that in the control condition (46%; CI = [36%, 56%]). Among plasma donors, the return percentages in the experimental conditions ranged from 85% to 100%, although the relatively low number of plasma donors that participated in the RCT may have skewed results, χ2(4) = 3.4, p = .49.
Results of the logistic regression of return for both WB and plasma donors are presented in Table 2. For whole blood donors, all three regression models were significant. Number of prior donation attempts and age were found to be significant predictors of return, in that higher numbers of prior donation attempts and higher age led to higher odds of return within 4 weeks after being invited. We found in Models 2 and 3 that the participants in the information condition had a higher likelihood to return compared with the control group in the RCT (cf. estimated marginal means indicate 62%, CI = [52%, 70%] return after receiving additional information vs. 47%, CI = [37%, 57%] return in the control group; see Figure 2). Due to the low number of plasma donors among the participants, we had to adjust the model for plasma donors. We collapsed the RCT conditions and compared the total pool of RCT participants to the plasma donors in the unobtrusive control groups, and we also collapsed long- and short-term medical reasons for deferral. None of the three regression models for plasma donors was significant.
Logistic Regression of Return Within 4 Weeks After Being Invited, for Whole Blood and Plasma Donors.
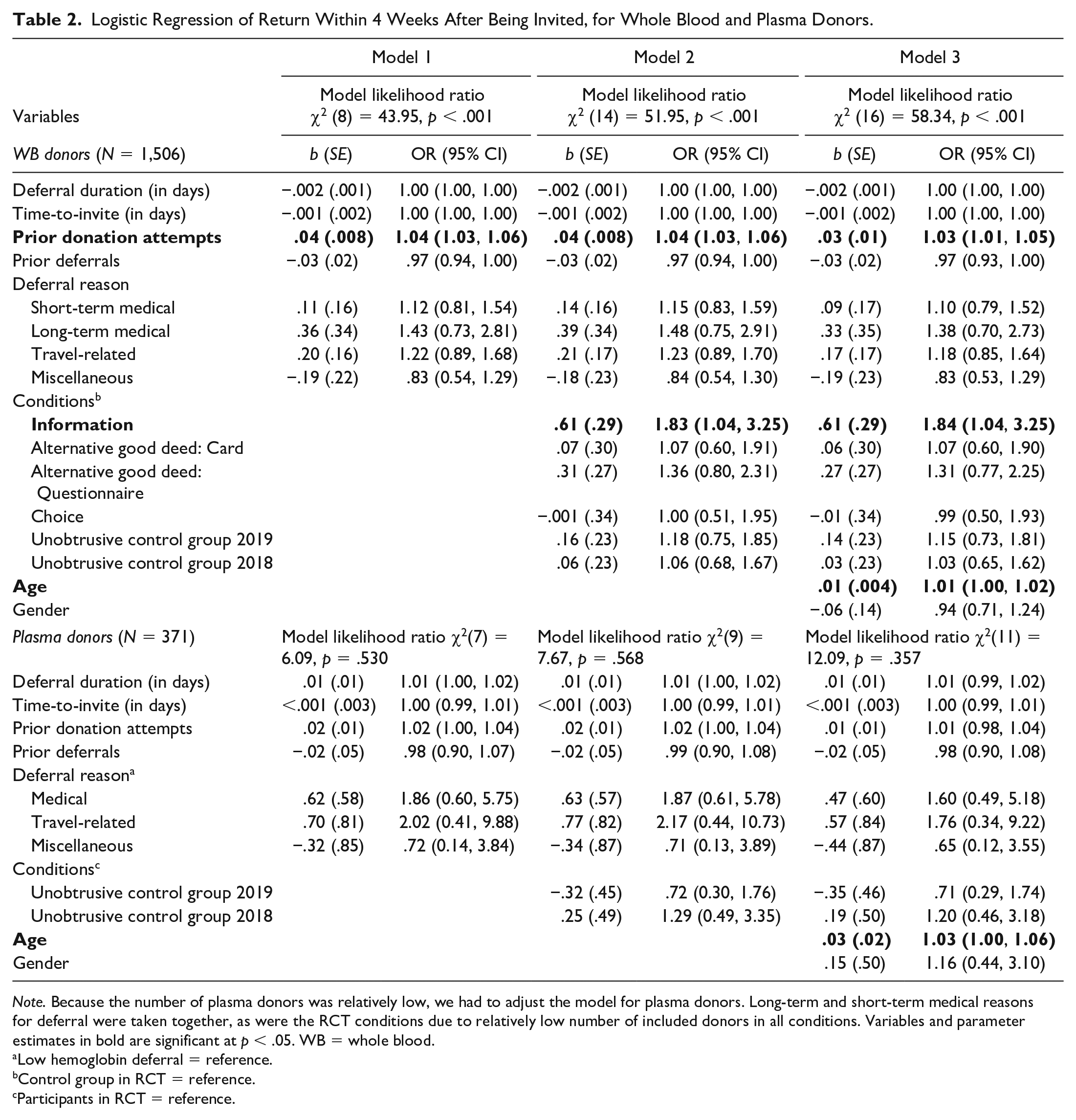
Note. Because the number of plasma donors was relatively low, we had to adjust the model for plasma donors. Long-term and short-term medical reasons for deferral were taken together, as were the RCT conditions due to relatively low number of included donors in all conditions. Variables and parameter estimates in bold are significant at p < .05. WB = whole blood.
Low hemoglobin deferral = reference.
Control group in RCT = reference.
Participants in RCT = reference.
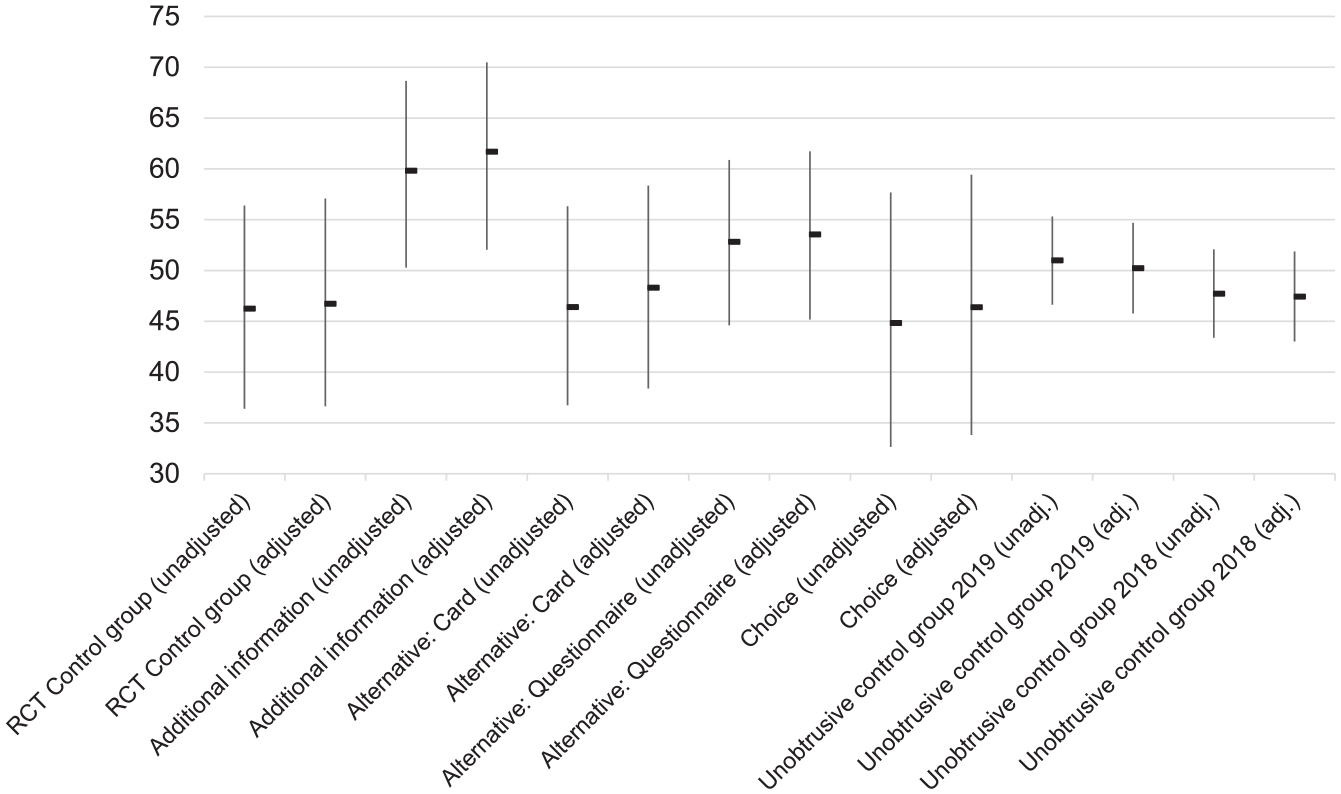
Return rates per condition, unadjusted and adjusted for control variables (based on estimated marginal means).
Next, we repeated the logistic regression procedure with the participants in the choice condition reassigned to the condition of their choice (thereby losing two participants whose choice was unclear). We repeated this analysis for whole blood donors only, as the models for plasma donors would not change. Similar to the previous analysis, we found that all three regression models were significant (Table 3). However, even though we again found significant positive effects of the number of prior donation attempts and age on the likelihood of return, we did not find the effect of providing additional information compared with the control group when we reassigned the participants from the choice condition to the condition of their choice. This is also reflected by the return rates in the different conditions, which are closer together when participants in the choice condition were reassigned to their chosen condition (i.e., estimated marginal means indicate 52%, CI = [44%, 60%] return for the questionnaire condition; 48%, CI = [39%, 57%] for the card; 60%, CI = [51%, 69%] for additional information; and 48%, CI = [38%, 58%] for the control group).
Logistic Regression of Return Within 4 Weeks After Being Invited, for Whole Blood Donors.
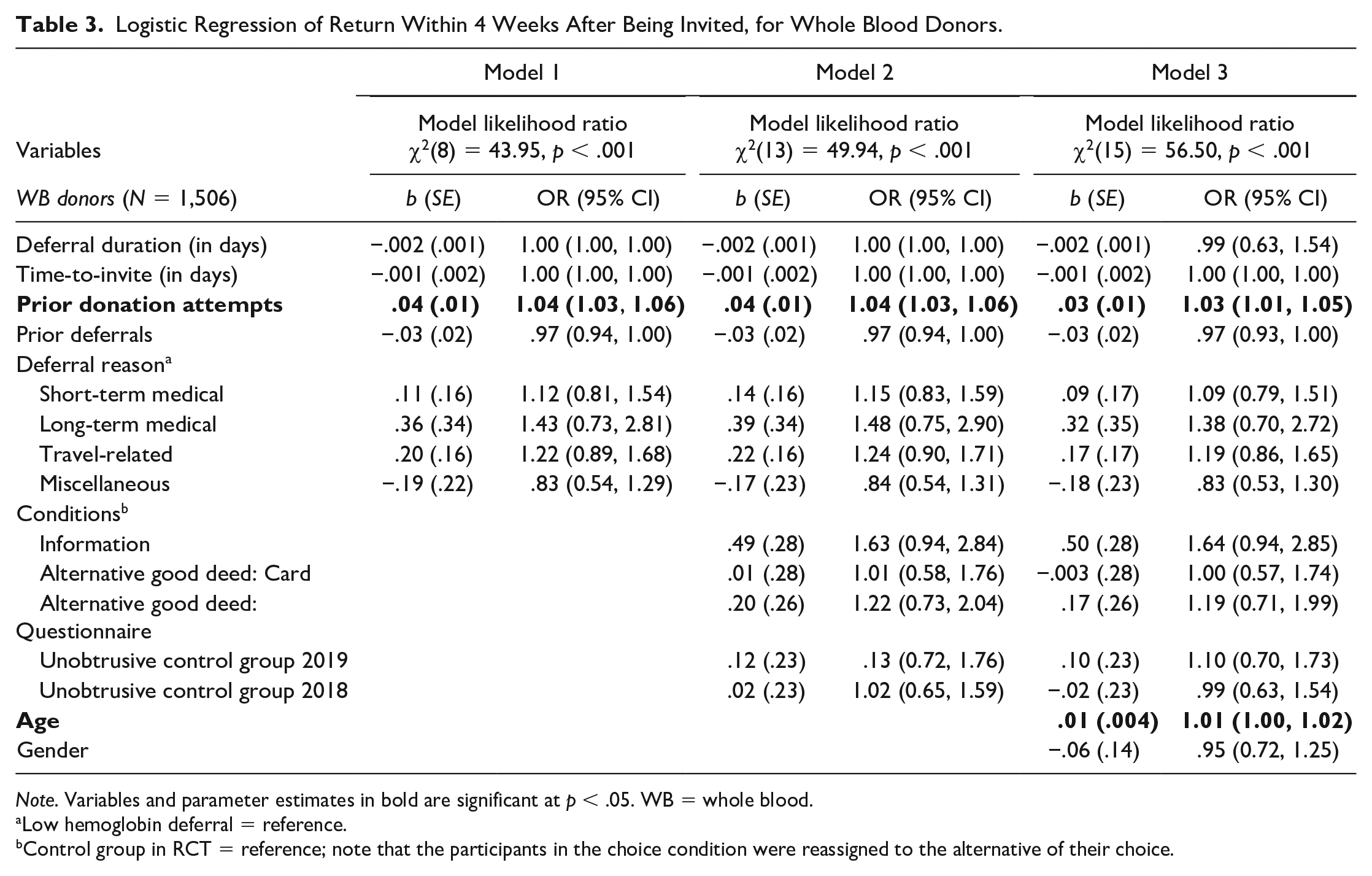
Note. Variables and parameter estimates in bold are significant at p < .05. WB = whole blood.
Low hemoglobin deferral = reference.
Control group in RCT = reference; note that the participants in the choice condition were reassigned to the alternative of their choice.
Discussion
As on-site deferral of blood donors may lead to donor lapse (Custer et al., 2011; Hillgrove et al., 2011; Spekman et al., 2019), blood banks are looking for ways to encourage deferred donors to return once they are eligible to donate again. In this study, we tested several ways of offering those donors an on-site alternative when they were deferred from donating blood or plasma. In an RCT in the field, we tested whether proposing an alternative good deed to aid the blood service, providing additional information, or giving donors a choice between these options affected whether or not they returned after their deferral had expired and they were invited for a next donation. In contrast to Hypothesis 1, findings showed that offering an alternative good deed in the form of writing a card for a patient or helping the blood service by filling out a questionnaire did not affect the return rate of on-site deferred donors. Offering these donors a choice between the two alternative good deeds or receiving additional information also did not affect their return rate. Supporting Hypothesis 2, providing on-site deferred donors with additional information about deferral did appear to have a positive effect on return, yet only for whole blood donors.
The effect of providing additional information on the return of deferred whole blood donors is in line with the findings from Gemelli et al. (2021a). While they did not measure actual return behavior, they did find that providing on-site deferred donors with a brochure increased their knowledge about the deferral as well as their chances of rebooking a next appointment. Although the intervention in the Gemelli et al. (2021a) study was more elaborate—consisting of a brochure, plus a guided conversation with a member of the collection staff and a follow-up e-mail—our results also suggest that providing extra information to deferred donors may help to retain these donors. This shows that deferred donors have a relatively high informational need (Compernolle, 2017) and that providing clear information about the nature and duration of the deferral may help to encourage return (Davison et al., 2020). Multiple explanations are possible in trying to understand why the information brochure was more effective than the alternative good deeds. For instance, the fact that donors could refer back to the brochure after leaving the donation center may have helped in coping with the deferral and the emotions it caused. In addition, the brochure explicitly mentioned that the deferral was temporary and that return would be appreciated, so this may have increased the feelings of self-worth among these donors. However, further research is needed to understand which mechanisms have played a role.
While we expected the alternative good deeds to increase the return of deferred donors, we found that this was not the case. This is especially surprising given that the alternative good deeds were preferred by the majority of donors in the choice condition. These choice data should, however, be considered with caution. The number of donors in this condition was considerably smaller than in the other conditions. The fact that offering an alternative good deed to deferred donors did not affect their return behavior in our study does not align with the finding from Clement et al. (2016) that offering an alternative good deed did increase donor return in Germany. Several factors may explain why the findings of this study are different.
In the Netherlands, the current policy states that donors need to be informed about the reason and duration of their deferral, but does not provide guidance on how to do this. Also, deferred donors receive no additional information or thank-you gifts. After the deferral has expired, donors receive an invitation to donate (via postal mail) when their blood type is in demand. Thus, Dutch donors are actively encouraged to return for a new donation attempt, even if they had been deferred previously. German donors, however, receive a standard thank-you gift (regardless of whether they donated successfully or not) and have to return on their own initiative (Clement et al., 2016). The active invitation strategy in the Netherlands may result in a return rate that does not differ much between deferred donors who are offered an alternative on-site and those who are not offered such an alternative, as all of them receive an invitation to donate as soon as they are eligible to donate again. This aligns with findings from Gemelli et al. (2021b), who showed that notifying donors at the end of their deferral is an effective means to retain them.
In terms of the content of the alternative good deeds, this study offered alternatives that were explicitly connected to the transfusion service. This is a substantial difference from to the alternative good deed used in the Clement et al. (2016) study—painting part of a larger picture for a children’s hospital—which was not directly related to the transfusion service. Also, the alternative good deeds offered in this study were individual activities compared with the collaborative effort of the painting. Finally, the fact that the painting was to be offered to a children’s hospital may have evoked empathy, whereas drawing or writing a card for a transfusion recipient might not evoke similar levels of empathy. In fact, asking donors to write or draw a card to a recipient when they could not donate blood or plasma may have even emphasized the feeling of having failed to deliver what they came for, although we have no evidence that this was an issue for the donors in this condition. Because we did not assess perceptions of donors about the alternatives we offered, we do not know if the alternatives actually induced feelings of warm glow similar to an actual donation. It is possible that the failure of our chosen alternatives to induce such feelings may have resulted in a less effective intervention. This goes to show that designing an effective intervention that is usable in the field is a delicate balancing act between doing what is theoretically relevant and interesting and what is practically feasible in terms of costs, materials, and long-term maintenance.
In this study, we used a 4-week time period for return after donors received the first invitation after the deferred index donation attempt. This may have had consequences for our results, as a significant proportion of donors normally return after this period, especially after a deferral (Spekman et al., 2019). For instance, in their paper, Spekman et al. (2019) find that 76% of deferred whole blood donors returns within 2 years after expiry of the deferral. Thus, the 45% to 60% found among whole blood donors in this study appears to be rather low but may be a better indication of quick return than of return in general. However, we decided to limit the follow-up to a 4-week period because donors may also receive a second invitation after these 4 weeks, which would complicate return dynamics considerably. Yet, offering an alternative or additional information about deferral may be of particular importance to donors that are generally late to return, so longer-term effects of such alternatives are worth further study.
Due to several factors, not all donors who met our inclusion criteria were actually included in the RCT, which may have affected our results. In consultation with donation center personnel, we decided not to bring additional burden upon the staff by asking them to monitor reasons for nonparticipation. Moreover, when the donation centers were overcrowded with donors during busy hours, not all on-site deferred donors were invited because of the extra time it took. The consequence of this is that we cannot distinguish between donors who were not invited and donors who were invited but declined to participate. In the worst case scenario, this may have led to a self-selection bias of including only those donors who were already planning to return, while donors who would have benefited (more) from the offered alternative or additional information may not have been reached. However, this scenario is implausible given the lack of difference in return rates between the RCT control group and the unobtrusive control group from the same period. Moreover, the process of randomizing participants across conditions ensured that our results are valid for the group of donors that participated in the trial.
Originally, we had planned for a more complex study design, for which we calculated that we needed 99 participants per condition (see the supplemental materials on the OSF page for more information about the original design and the power calculation). Based on discussions with the blood bank staff about study implementation in their locations and staff burden, we decided on the current, simpler design while retaining the estimated 99 donors per condition. More than 99 donors were included in all conditions, with the exception of the choice condition (78 donors). There are indications that this low number may have been caused by errors at registration. For instance, some informed consent forms were returned that mentioned two alternatives (instead of one). Furthermore, it is possible that donors assigned to the choice condition were registered with the condition they chose, instead of the choice condition.
This study tested effects of offering an alternative to on-site deferred donors on their return, yet we did not look at the potential mechanisms that explain why donors do or do not return. As suggested in the Introduction, deferral may disrupt donation habits and donor identities that have formed over time. Perhaps Sanquin’s strategy to actively and personally invite donors again (regardless of prior deferrals) plays an important role in re-establishing this habit and donor identity. Further research is needed to understand the exact role that donation habits and donor identities play in the (negative) relationship between deferral and donor return, and how interventions may affect that relationship.
Similar alternative hypotheses can be suggested for the role emotions play in the relationship between deferral and donor return. As suggested by previous research, the negative emotions that donors experience after on-site deferral may be short-lived (Gemelli et al., 2018; Hillgrove et al., 2012) and thus their effects on donor return may be minimal. Another potential pathway may be that deferral may cause donors to not experience pride or warm glow at the current visit, which may make them even more motivated to return (especially when they have experienced that feeling at previous donations), regardless of whether they are offered an alternative or not. In addition, Sanquin’s strategy to personally invite donors may also play an important role in moderating the effect of emotions on donor return after deferral. To understand the effects of both positive and negative emotions on donor return, more research is needed.
Overall, this study showed that offering the possibility to do an alternative good deed to deferred blood and plasma donors did not impact their return behavior. The results further suggest that offering deferred whole blood donors additional information about deferral did impact their return positively, that is, that additional information contributes to the continuation of pro-social behavior. These results may also apply to other (nonprofit) organizations that rely on volunteers or donors. For instance, nonprofit organizations offering emergency relief or disaster assistance may be able to retain more volunteers for future events by providing them with more information about the reasons for not accepting all help at that time (e.g., to avoid overcrowding). Our findings are strengthened by the fact that we tested this in an RCT in the field. Thus, we showed that providing donors with more information about reasons for turning them away and showing appreciation for their willingness to help at the current time may help to retain more of them for future donations.
Footnotes
Acknowledgements
The authors would like to thank all team leaders and collection staff of the participating donation locations for their cooperation, as well as all donors that participated in the RCT.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Sanquin Blood Supply (PPOC 17-13). Eva-Maria Merz’ contribution has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme (grant agreement No 802227).