
Abstract
Diagnosis of canine periodontal disease relies on clinical and radiographic evaluation including the simplified bisecting angle (SBA) technique. However, difficulty in visualizing the alveolar bone margin and misinterpreting its distance from the cemento-enamel junction (CEJ) diminishes its usefulness. The objective of the study was to compare a new radiographic view, the modified interproximal (MIP) technique, to the SBA technique for the detection of bony defects and furcation involvement in a canine experimental model of periodontal disease of the maxillary fourth premolar tooth (PM4). The authors hypothesized that the MIP technique would detect milder bony defects and furcation exposure compared to the SBA technique. Eleven large breed dog cadavers with mesaticephalic or dolichocephalic skull conformation and without periodontal disease were used. Dental radiography with SBA and MIP techniques was acquired prior to and after creating a horizontal pattern of bony defects, centered on PM4 in 12.5% increments, from 0% to 50% bone loss. The level of the bone margin and furcation exposure was evaluated. Inter- and intraobserver agreement was substantial. Observers systematically underestimated the distance between the CEJ and the bone margin with both radiographic techniques. MIP technique performed better overall than SBA technique (accuracy and sensitivity were significantly improved). These results show that MIP technique is more accurate than SBA in the evaluation of mild bony defects and furcation lesions associated with PM4. Adding a MIP view of PM4 to the canine full-mouth survey may improve detection of bone loss and furcation involvement.
Keywords
Introduction
Periodontal disease (PD) is defined as an inflammatory condition of the supporting tooth structures consisting of the gingiva, periodontal ligament, cementum, and alveolar bone.1,2 It results in variable degrees of attachment loss of the tooth. This condition is frequently encountered in dogs,3,4 the prevalence and severity of disease increasing with age.5,6 Consequences of untreated PD include, but are not limited to tooth loss, abscess formation through combined periodontic-endodontic lesions, oro-nasal fistulas, and chronic pain.3,7,8 In carnivores, the carnassial teeth, (i.e., maxillary fourth premolar [PM4] and mandibular first molar [M1] teeth), represent a distinct functional unit for mastication. These teeth, combined with the four canine teeth, are considered most useful for prehension and mastication. Efforts to maintain these teeth should therefore be made for the benefit of the patient.
Diagnosis of PD relies primarily on periodontal probing and dental radiography.3,7,9–12 Together they allow assignment of a stage of PD to the tooth being evaluated. Four stages of PD are currently recognized in veterinary medicine, ranging from PD0 (absence of PD), PD1 (gingivitis), PD2 (1-24% bone loss, stage 1 furcation), PD3 (25-50% bone loss, stage 2 furcation), and PD4 (bone loss >50%, stage 3 furcation).1,3,7,13 Accurate determination of PD stage, which consists of correctly identifying the amount of bone loss a tooth has suffered from, is essential for subsequent development of an adapted treatment plan. It may include scaling and polishing, closed or open root planing, periodontal surgery or extraction.
Dental radiography has been broadly advocated in veterinary medicine since the late 1980s. It is now considered standard of care for evaluation of a patient's oral health.1,3,5,14,15 Radiographs are useful in staging PD and establishing a prognosis and treatment plan.14,15 Although many studies have shown that the diagnostic yield of computed tomography (CT) and cone-beam CT (CBCT) is superior to dental radiographs,16,17 their use is still limited to a small number of referral practices. Dental radiography remains a widely accessible, pertinent tool for staging oral diseases. Radiography initially designed for human dentistry has been adapted for the dog. As such, a simplified bisecting angle (SBA) technique for evaluating the caudal maxilla was developed. 15 However, the SBA view is associated with superimposition of tooth roots, hard palate, zygomatic arch and nasal cavities often masking the alveolar bone margin,8,18,19 and thus may lead to misdiagnosis. This can result in under- or over-staging the severity of PD and recommendation of suboptimal treatment.2,8,12,17,19 For this reason, in human dentistry, a paralleling technique is considered more accurate for the detection of PD, as it minimizes dimensional distortion.9,20,21
Limitations of the SBA technique lead to discrepancy between the interpretation of radiographs, clinical examination (probing) and degree of actual bone loss. 22 To the authors’ knowledge, only a few veterinary studies have compared radiographic techniques for the diagnosis of PD and no standardized method has been established or proven superior to the SBA technique. 22 In human dentistry, measurement obtained with a probe during periodontal surgery is considered an acceptable assessment of truth.9,10,21,23,24 The objective of this study was to evaluate a novel technique, the modified interproximal (MIP) technique, developed by the authors, by documenting agreement, accuracy, sensitivity, and specificity in the assessment of the degree of simulated bony defects in the area surrounding the maxillary PM4 in dogs and to compare these results to those obtained with the SBA technique. The authors hypothesized that the MIP technique would have superior intra- and interobserver agreement, accuracy, sensitivity and specificity compared to the SBA technique.
Materials and Methods
Eleven dog cadavers were collected from animals euthanized for reasons unrelated to this study. Heads were disarticulated at the atlanto-occipital joint, harvested from the rest of the body and frozen at −21°C. Before experimentation, heads were thawed at 4°C. Skull length, width and index were recorded for all patients as previously described 25 with a ruler between needles inserted at the posthion and inion (the highest point of the external occipital protuberance), and at the widest point of the zygomatic arch, respectively. Subject enrollment was limited to dogs with mesaticephalic or dolichocephalic skull conformation with skull length ranging from 18 to 40 cm. Mesaticephalic and dolichocephalic skull conformations were defined by a skull index of 45.5‒66.5 and less than 45.5 respectively.25,26
(Skull index quantifies head/skull shape by dividing maximum head width by maximum length, then multiplying by 100 to obtain a percentage).
The maxillary third premolar tooth (PM3), PM4, and M1 were scaled using a combination of ultrasonic and manual methods prior to examination. Any quadrant missing the maxillary PM3, PM4, or M1 was excluded from the study. Each maxilla was examined visually, and periodontal probing was performed.a The furcation was palpated with the same probe. The presence of PD was defined by attachment loss and/or furcation involvement on probing. An alveolar bone margin located more than 2 mm apical to the cemento-enamel junction (CEJ) on radiographs was considered attachment loss. Any quadrant with PD on the above-specified teeth was excluded. Also excluded were quadrants containing teeth with any dental damage preventing identification of the CEJ or apices of the roots. Single bisecting angle radiographs centered on the furcation area of PM4 using the SBA technique were performed to permit assessment of periodontal and endodontic disease as described above. These radiographs later served as a baseline when assessing the SBA technique.
On all specimens, a #15 scalpel blade was used to create a sulcular incision around PM3, PM4, and M1. A releasing incision was created at the furcation on the buccal and palatal aspects of PM3. A triangular mucoperiosteal flap was then elevated.
Fenestration of the buccal bone overlying the apices of the distal and mesiobuccal roots of PM4 with a #2 round carbine bur facilitated precise localization of apices. Because the CEJ is not a straight line, the technique for determination of size of bony defects was adjusted as follows: a straight line was drawn between the most apical point of the CEJ on the distal and mesiobuccal roots. Each of the two roots was measured from that point to the apex using the periodontal probe. The mesiopalatal root was not measured and it was not considered in the ensuing calculations. If the measurement was different between roots, the mean was determined. The percentage of bone removal was calculated according to this value, rounded up to the closest 0.5 mm. Bony defects were created apical to the imaginary CEJ line (Figure 1).
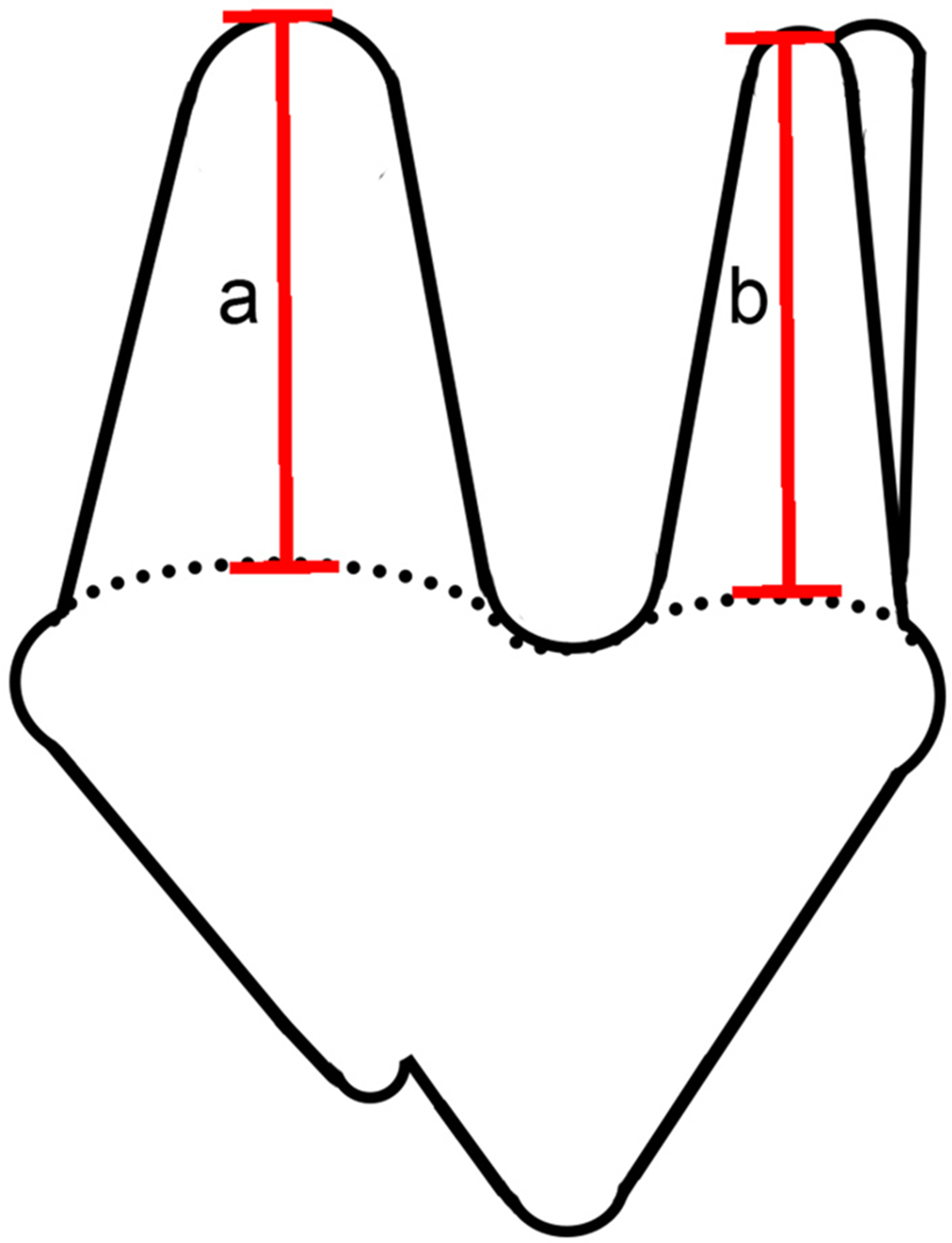
Illustration of maxillary fourth premolar tooth (PM4). The cemento-enamel junction (CEJ) is represented by the dotted line. Measurements were obtained on each root from the most apical portion of the CEJ to the root apex. When both roots were not the same length, the formula « (a + b)/2 » was used to calculate % of bone loss.
Based on initial screening, all dogs included in the study were free of PD, except for one quadrant that was excluded from the study, and baseline radiographs were assigned a Bone Defect Score of 1 and a Furcation Score of 1.
Increments of bone loss creation and scoring were performed using #2 and #3 round and #7901 flame carbide burs on an air-driven high speed handpiece by the same author (JM) to create horizontal bone defects around maxillary PM4 in 12.5% increments, until 50% bone loss was achieved for a total of four scores (12.5%, 25%, 37.5%, and 50%) in addition to baseline. Alveolar bony defects were created paralleling the most apical aspect of the CEJ on the buccal aspect of PM4, extending, on a frontal plane, to the palatal aspect of the tooth and, on a parasagittal plane, to the distal and mesial aspects of PM3 and M1, respectively (Figure 2). Measurements were made from the CEJ for each increment, using the periodontal probe, measuring at every line angle, and in two areas on the buccal and palatal aspect of each tooth. Interproximal bone was removed on the distal and mesial aspects until the root of the adjacent tooth was met, where bone was tapered to the furcation of that tooth. A #6 round bur was used to bevel the edge of the alveolar margin on the buccal and palatal aspects of teeth. The alveolar ridge was removed medially until it reached the palatal aspect of the tooth, then was quickly tapered to meet the palatine process of the maxilla (Figure 3). The furcation was probed with the periodontal probe, measured and recorded at each increment. Soft tissues were manually replaced into their original position before obtaining radiographs.
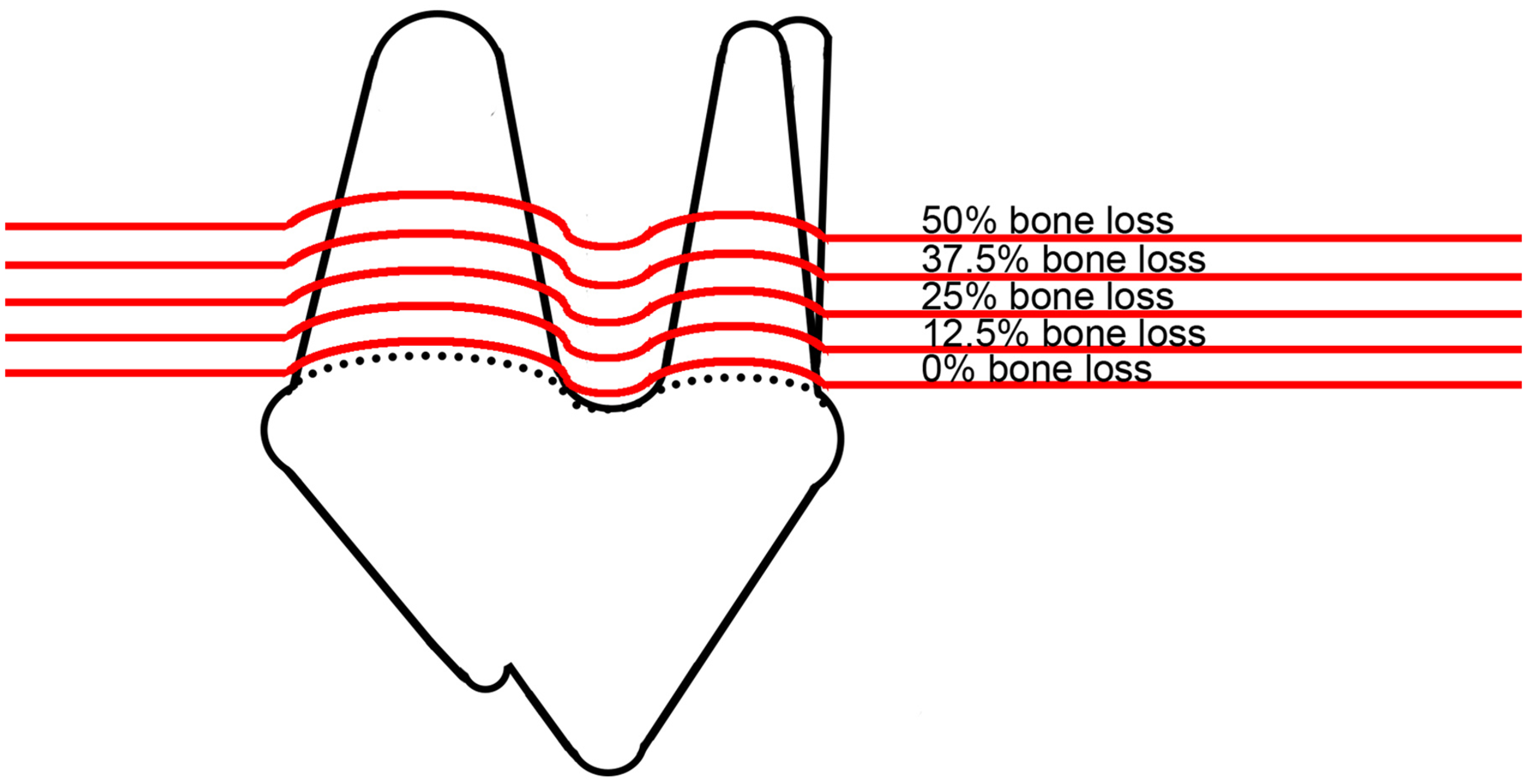
Illustration of maxillary fourth premolar tooth (PM4). The cemento-enamel junction is represented by the dotted line. Horizontal bony defects were created in 12.5% increments up to 50%, based on measurements of tooth roots shown in Figure 1.

Photograph of a defect showing 50% bone removal. Note the horizontal defect affecting both mesiobuccal and distal roots of the fourth premolar tooth (PM4), then tapering to the furcation of the adjacent tooth.
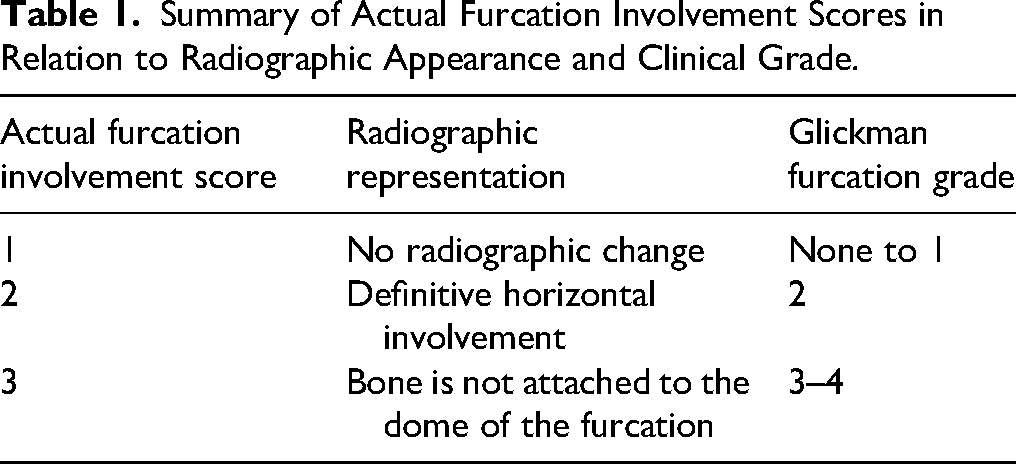
Furcation Involvement Scores were established based on a modification of the Glickman classification 27 (Table 1). A Furcation Involvement Score of 1 was assigned to a healthy furcation. A Score of 2 was assigned to teeth showing a subjective thinning of bone, visible on radiographs and clinically detectable by penetration of a probe into the defect with no communication to the other side of the furcation. Finally, a Furcation Involvement Score of 3 corresponded to the alveolar margin being clearly apical to the dome of the furcation on radiographs and being able to pass a periodontal probe through the furcation until visible on the other side.
Summary of Actual Furcation Involvement Scores in Relation to Radiographic Appearance and Clinical Grade.
Bilateral SBA and MIP radiographs were obtained prior to and following the induction of bony defects for each increment starting with the right side.
SBA
Radiographs of the right and left caudal maxillae were successively performed for each head positioned in lateral recumbency. Care was taken to position the palate perpendicular to the table; sandbags were used when necessary. A size 4 storage phosphor plateb was placed parallel to the palate, and the x-ray beam was angled at 45° according to a simplified technique. 15 For each projection, the x-ray beam was centered on the furcation area of PM4.
MIP
With the head in lateral recumbency, a size 4 plate was first positioned perpendicular to the palate, with one side resting on the palatal midline. The x-ray tube head was placed at a 70° vertical angle, and the angle of the plate was aligned perpendicular to the x-ray tubec (Figure 4). The plate was stabilized with a paper ball to ensure proper positioning, if required. The radiographic view was obtained with the x-ray beam centered on the furcation area of PM4. All radiographic projections were acquired by a single operator (JM). Radiation exposure times ranged from 0.14 to 0.18 s according to the size of the head, with a tube voltage of 60 kV and tube current of 6 mA.
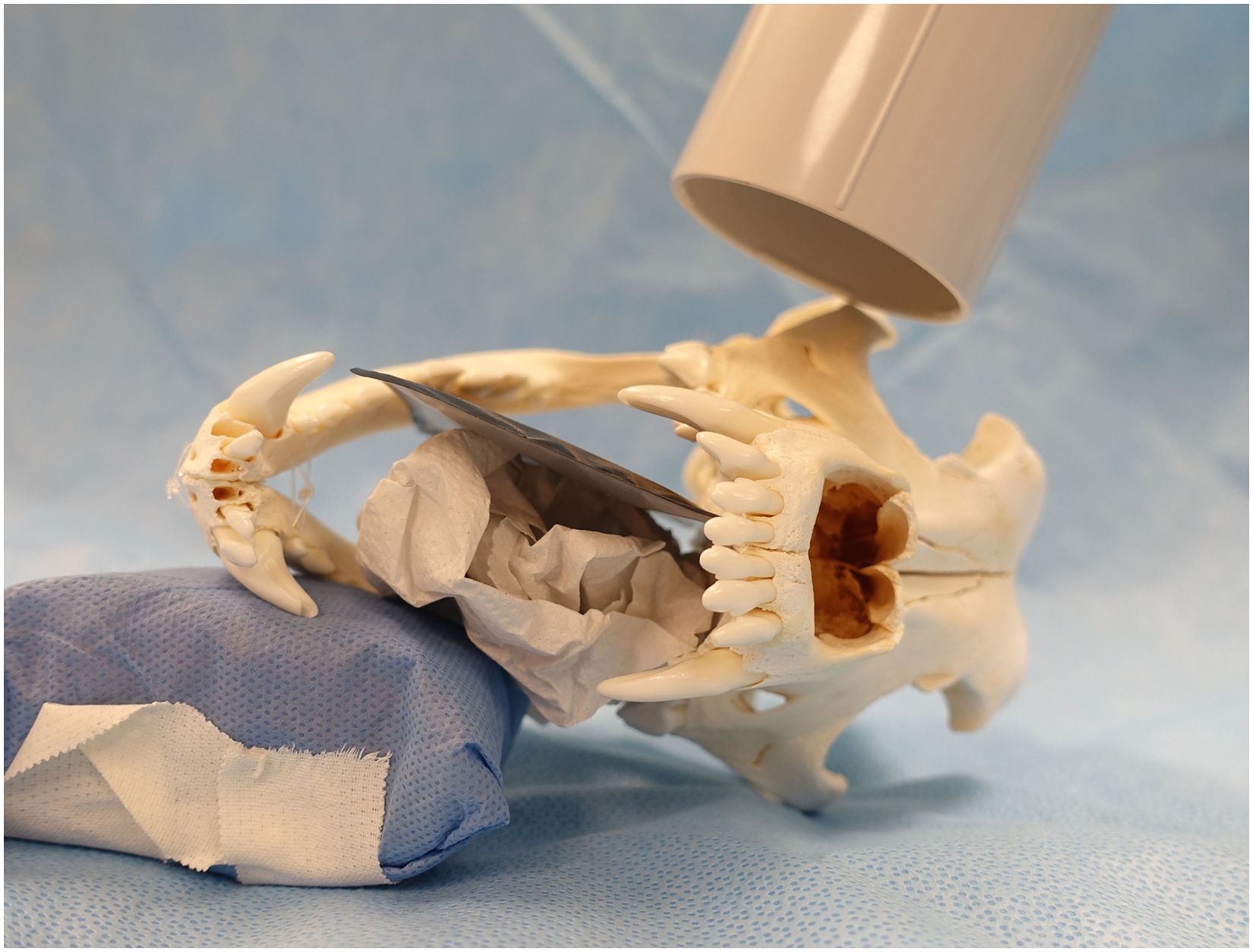
Placement of plate and x-ray beam for modified interproximal view. The canine skull was positioned in lateral recumbency so that the palate is aligned perpendicular to the table. The x-ray tube head is directed toward the maxilla at a 70° vertical angle, centered on the furcation area of the maxillary fourth premolar tooth (PM4). The plate is held perpendicular to the x-ray tube head with a paper ball.
A six-digit number was attributed to each radiographic view using a series random number generatord based on atmospheric noise. All images were transferred to a commercially available picture archiving communications system (PACS)e. Data collected for each radiograph included: dog identification number, right or left maxilla, Bone Defect Score (from 1 to 5 as previously described), Furcation Score and type of radiographic projection (SBA or MIP) performed. Each radiographic projection constituted a separate folder on a DICOM viewerf. Studies were then sorted according to the six-digit generated random number ensuring blind evaluation of imaging studies.
All imaging review sessions to evaluate bony defects took place in a dedicated room under uniform ambient lighting using a factory calibrated flicker-free 3840 × 2160 4 K commercial screen monitorg with a brightness of 250 cd/m2, native contrast of 1000:1 and a refresh rate of 60 Hz. The monitor was connected to a personal computerh and the same softwarei was used for all sessions. Two blinded observers consisting of a third-year dentistry resident (Observer 1) and an American Veterinary Dental College (AVDC) Board-certified veterinary dentist (Observer 2) reviewed the radiographs independently. Each observer was asked to estimate the bone defect score based on the most apical alveolar margin height as defined by the following: 1 (no bony defect as shown by an alveolar margin positioned within 2 mm from the CEJ); 2 (12.5% bony defect represented by an alveolar margin positioned at 12.5% of the distance between the CEJ and location of the tooth apex); 3, 4 and 5 were assigned to 25%, 37.5% and 50% of bone loss, respectively, as determined by an equivalent percent distance between the CEJ and location of tooth apex, without using enhancement or measurement tools on the software. Observers were not trained further or calibrated prior to viewing radiographs, as it was the authors’ intention to assess interexaminer variability and usefulness of the MIP view in a larger population of veterinary practitioners. Furcation involvement was also scored on radiographs according to criteria specified in Table 1.
Statistical Analysis
Each observer scored % bone defect (1‒5) and furcation involvement (1‒3) on all anonymized radiographs during two sittings 1-week apart. These scores were identified as interpreted scores (IS). Agreement between scores recorded for each sitting was calculated for each observer (intraobserver agreement) and scores of each observer compared with each other (interobserver agreement) using a weighted kappa method. 28 The scale for weighted kappa was interpreted as follows: κ ≤ 0 was determined as agreement or worse than random agreement; 0.01–0.20 was considered slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement and 0.81–1.00 was considered almost perfect agreement.
Interpreted scores for bony defects and furcation involvement were compared to the actual bony defect scores (AS) and actual furcation involvement scores, respectively. Discordance between IS and AS yielded a ‘delta’ value for each radiograph. For example, if Observer 1 interpreted radiograph number 123456 as having an IS score of 3 when the AS for this view was 5, the resulting delta value was −2. A negative value therefore represented an underestimation of the distance between the CEJ and alveolar margin. Inversely, a positive delta value would show overestimation. A delta value of zero would indicate an identical interpreted and actual score and therefore a reliable estimation of the level of the alveolar margin. Accuracy was calculated as the number of instances a delta value of zero was found.
To determine the extent of bias (i.e., discrepancy) between techniques, a linear mixed model was used. To avoid pseudo replication bias, dog identification was considered a random effect. Observer and technique were considered fixed effects. The significance level of p = .05 was used to determine statistical significance. The same method was used to analyze Furcation Scores. In addition, data were examined as to whether bias varied as a function of AS. A linear mixed model was used with dog identification as a random effect and the following fixed effects: technique, AS and the interaction between the two factors. Furcation Scores were treated similarly.
For both bone defect scores and furcation scores, the scores for each tooth were reduced to a binary scale of disease versus no disease, using scores of 1 as no disease and scores >1 as disease.9,29 Data from both observers were pooled. For assessment of accuracy, sensitivity and specificity, data from the first assessment were used, as kappa values for agreement were high. To examine differences between techniques for accuracy, the exact chi-square test was used. Data analysis were performed using a software programj.
Results
Radiographic identification errors resulted in the exclusion of eight radiographs; therefore, 202 radiographs were interpreted. Intra- and interobserver agreement for interpreted Bone Defect and Furcation Involvement Scores are summarized in Tables 2 and 3, respectively. Agreement between sittings was substantial to almost perfect, and agreement between observers 1 and 2 was substantial for Bone Defect Scores and moderate to substantial for Furcation Involvement Scores. The mean delta value between IS and AS for scoring bone defects using SBA was −0.95 for Observer 1 (range: 0 to −3) and −1.04 for Observer 2 (range: 1 to −4). For MIP, the mean delta value in scores was −0.37 for Observer 1 (range: 1 to −2) and −0.29 for Observer 2 (range: 1 to −1). The majority of delta values between IS and AS were negative, with the MIP technique showing a narrow range of delta values, and a mean approaching 0 in comparison to SBA technique (Figure 5).
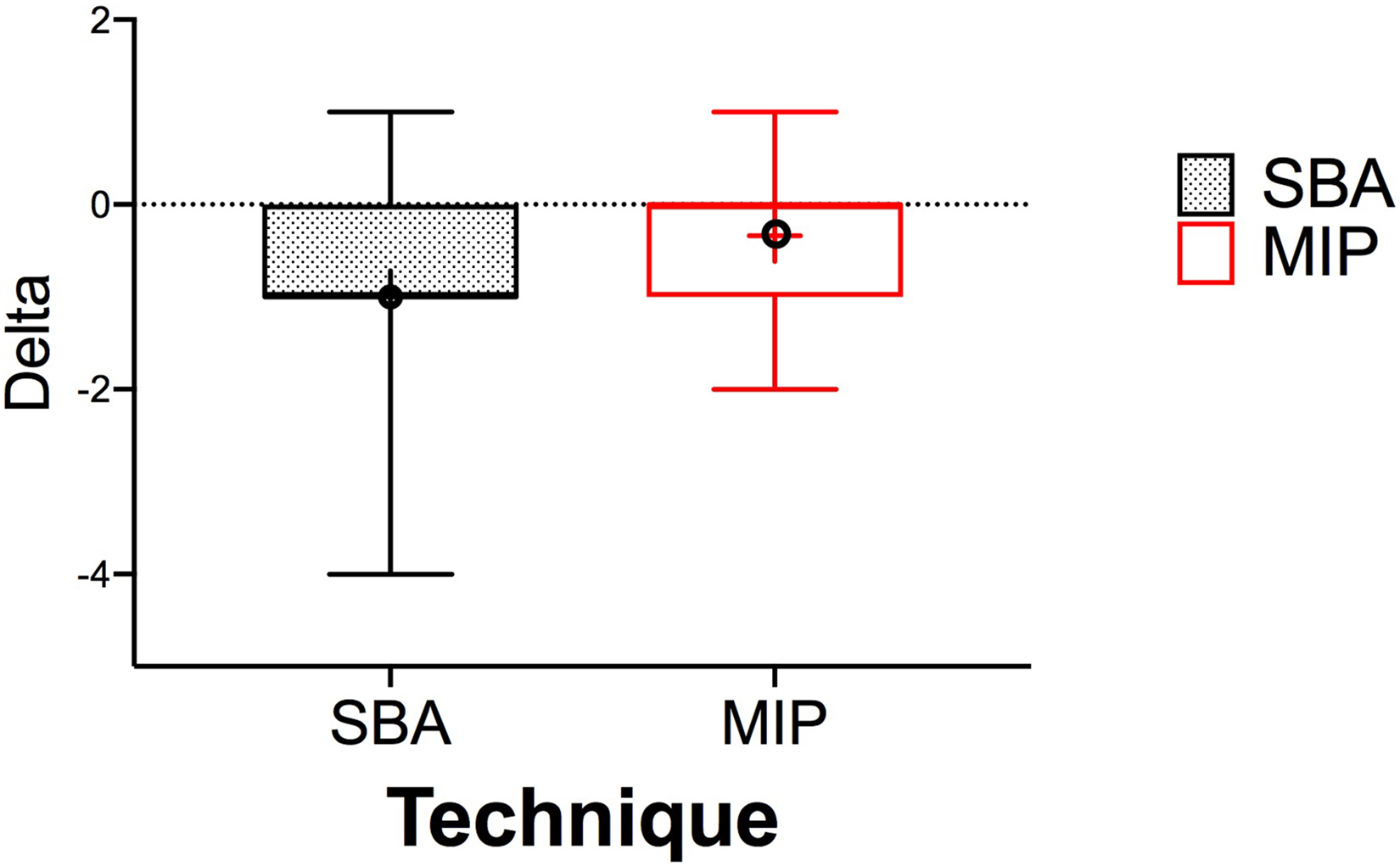
Distribution of delta values from scores for simplified bisecting angle (SBA) and modified interproximal (MIP) techniques. Data from the first assessment was pooled between both observers. Horizontal lines define, from top to bottom, the maximum, first quartile, median, third quartile and minimum. The mean is represented by a black circle.
Weighted Kappa Values for Interpreted Bone Defect Scores.
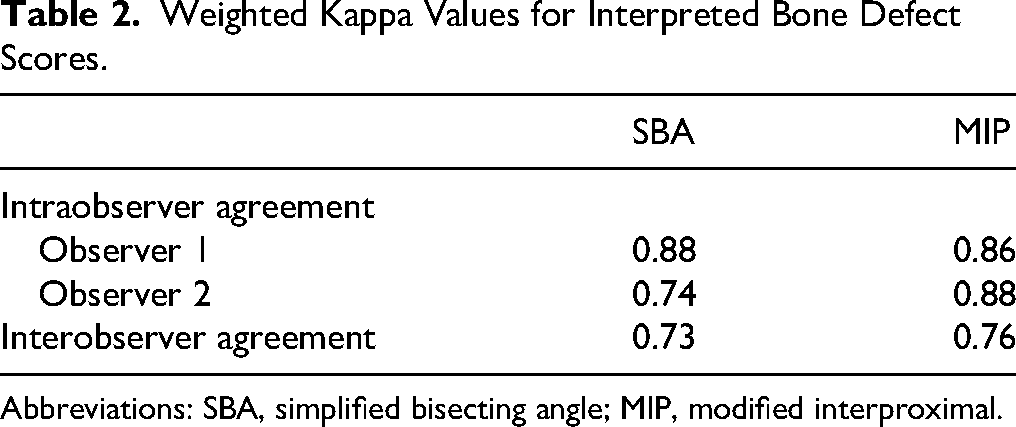
Abbreviations: SBA, simplified bisecting angle; MIP, modified interproximal.
Weighted kappa Values for Interpreted Furcation Involvement Scores.
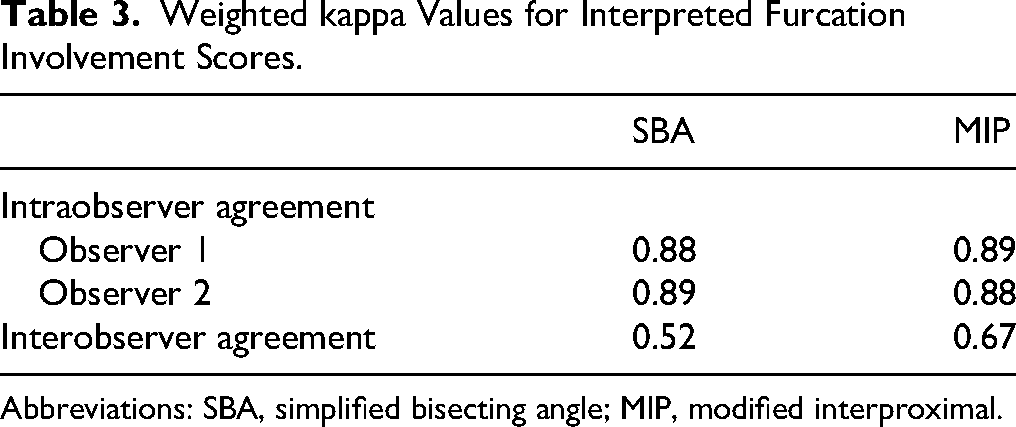
Abbreviations: SBA, simplified bisecting angle; MIP, modified interproximal.
Mean delta values in scores for Furcation Involvement using SBA technique were as follows: −0.62 for Observer 1 (range: 0 to −2) and −1.07 for Observer 2 (range: 0 to −1). For MIP, mean delta values were −0.09 for Observer 1 (range: 1 to −2) and 0.38 for Observer 2 (range: 0 to −2). Similar to bone defect scores, the MIP technique, in comparison to SBA technique, shows a narrower range of delta values and a mean closer to 0.
Overall, Bone Defect IS was significantly lower than AS for both observers (p < .0001). The magnitude of the bias (i.e., discrepancy between scores) did not differ between the two observers (p = .94). The bias was significantly more pronounced with the SBA technique than with MIP technique (p < .0001). In contrast to SBA, delta values between IS and AS did not reach statistical significance for MIP technique.
Results for furcation involvement showed IS being significantly smaller than AS for both observers (p < .0001). The magnitude of the bias did differ between the two observers (p = .0005) and was statistically higher with SBA than MIP technique (p < .0001).
Bias as a function of distance from CEJ to alveolar margin increased with severity (p < .0001) (Figure 6). This was true for both bony defect and furcation involvement scores. The bias was larger with the SBA technique than with the MIP technique (p < .0001).
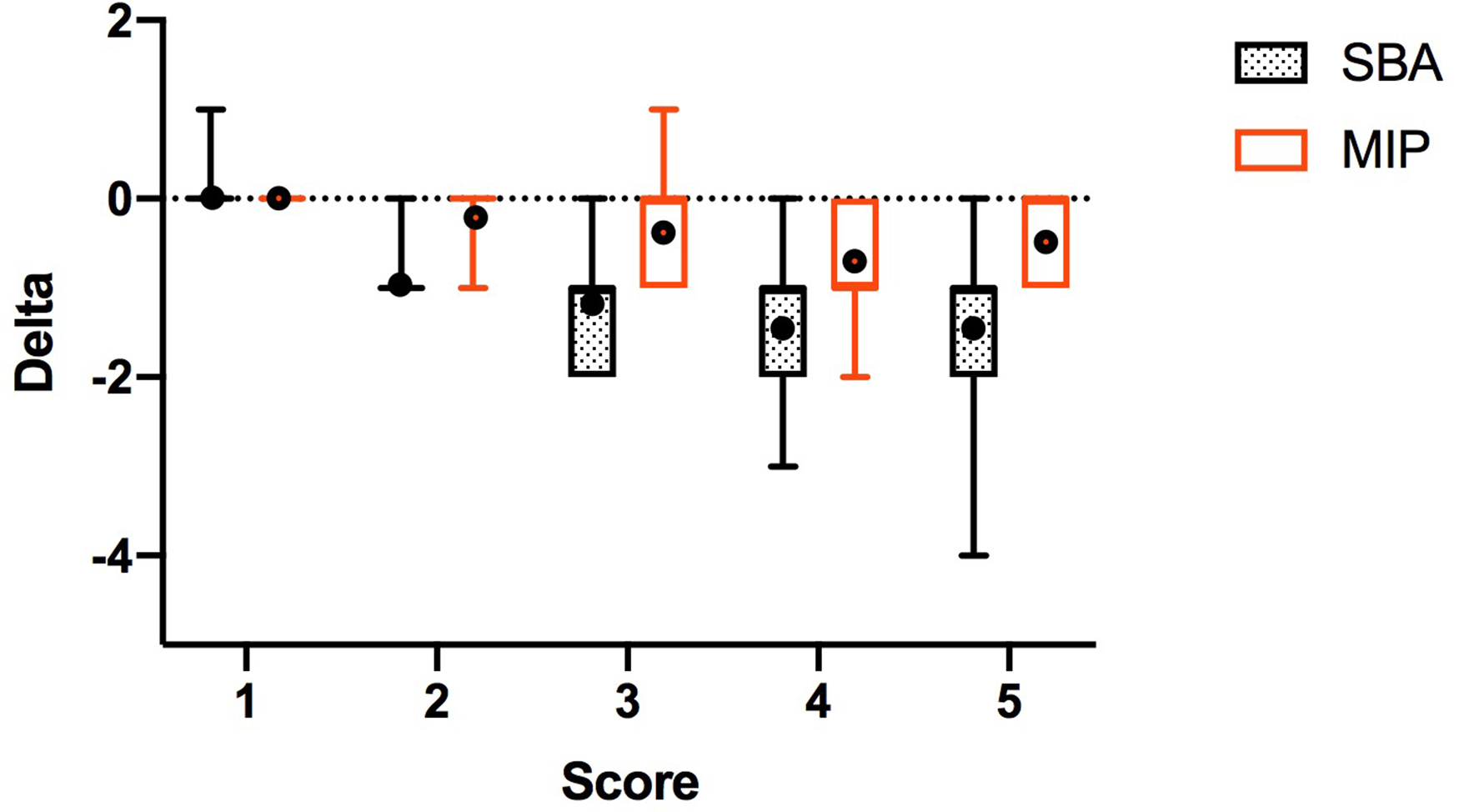
Distribution of delta values from scores for simplified bisecting angle (SBA) and modified interproximal (MIP) techniques, according to bone defect score. Horizontal lines define, from top to bottom the maximum, first quartile, median, third quartile and minimum. The mean is represented by a black circle.
A detailed summary of accuracy for each observer to correctly identify the actual bone defect score and furcation involvement with each technique is presented in Tables 4 and 5. Accuracy was significantly improved by the MIP techniques for scores 2 and 5 for Observer 1, and for scores between 2 and 5 for Observer 2 (p < .05). The same is true for a score of 3 for furcation involvement, for both observers. Both techniques correctly identified normal radiographs. Accuracy was significantly improved with MIP technique for mild (bone defect score of 2) and severe (bone defect scores of 5). A side-by-side comparison of radiographic images is available in Figure 7. Sensitivity and specificity for detection of Bone Defect Score and Furcation Involvement Scores are described in Tables 6 and 7, respectively. Both techniques showed high specificity (>88%) for normal radiographs.
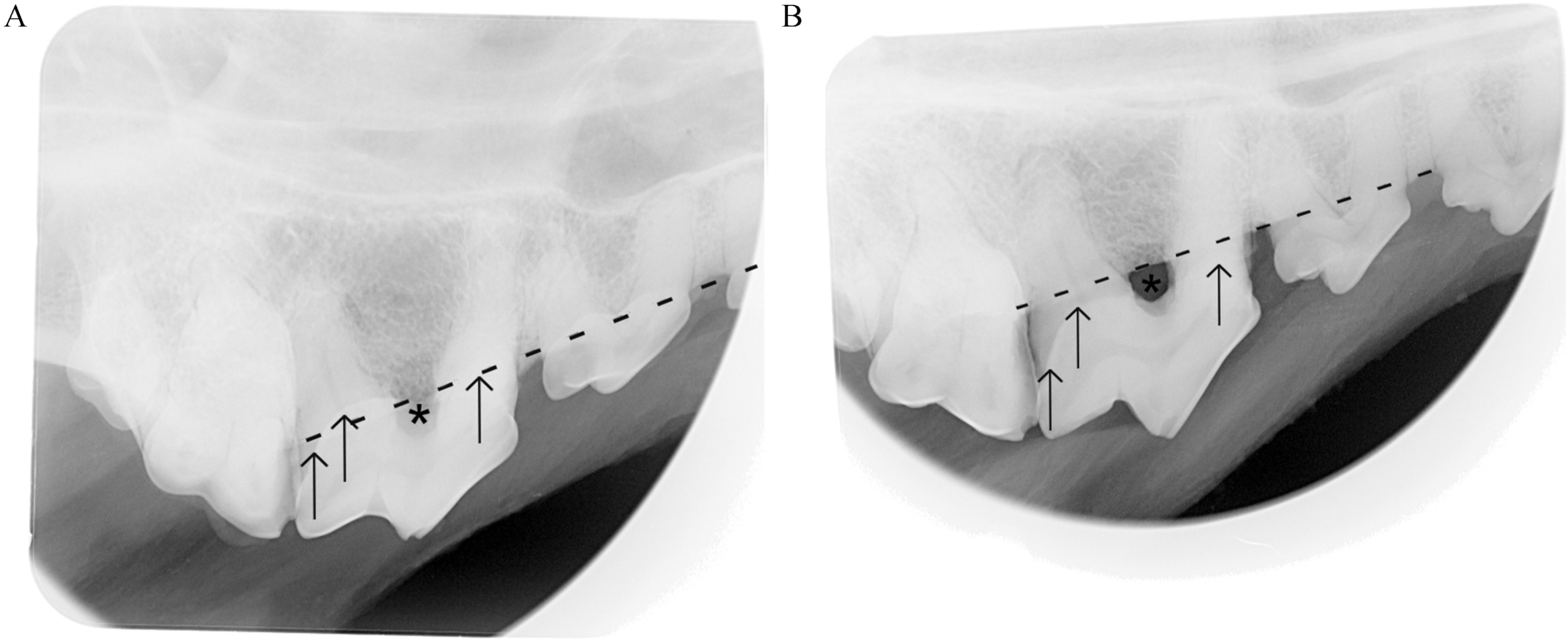
Radiographic views centered on the maxillary fourth premolar tooth (PM4) using a simplified bisecting angle technique (A) and a modified interproximal technique (B). Both views were acquired on the same head following creation of 37.5% bone defect surrounding the maxillary PM4. Notice the furcation (asterisk) is covered by the crown of the tooth on the SBA view (A), and that the level of the alveolar margin (dashed line) appears closer to the cementoenamel junction (CEJ, arrows) than on the MIP view (B). On the MIP view, exposure of the furcation is more easily detected, and the crown of the tooth is not superimposed over the alveolar margin, making the distance between the CEJ and the alveolar margin more visible.
Accuracy of the Simplified Bisecting Angle and Modified Interproximal Radiographic Techniques, According to Distance from CEJ to Alveolar Margin.
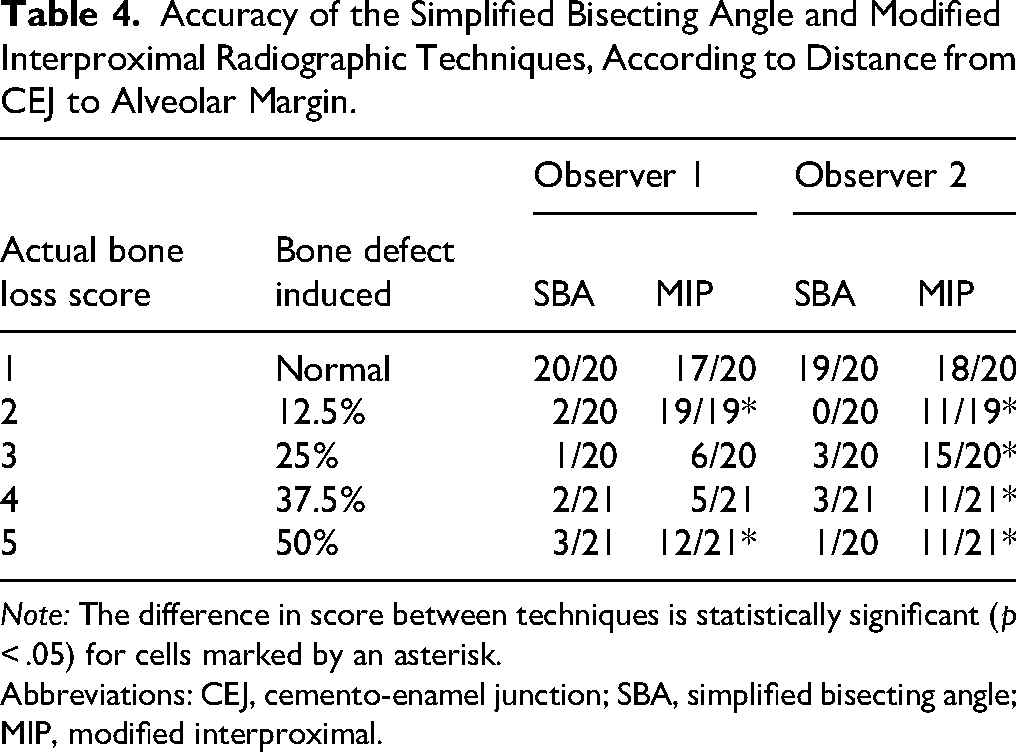
Note: The difference in score between techniques is statistically significant (p < .05) for cells marked by an asterisk.
Abbreviations: CEJ, cemento-enamel junction; SBA, simplified bisecting angle; MIP, modified interproximal.
Accuracy of Radiographic Technique in the Assessment of Furcation Involvement.
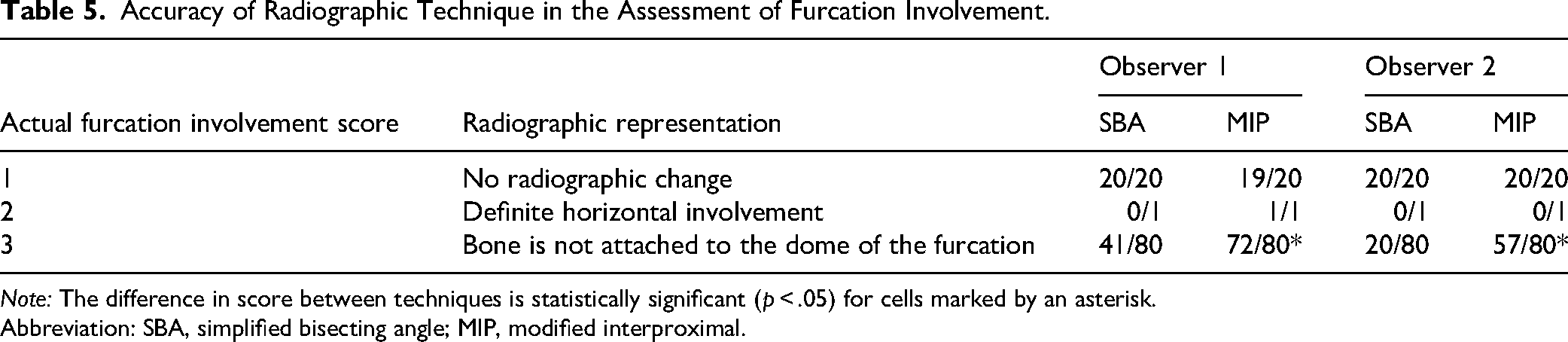
Note: The difference in score between techniques is statistically significant (p < .05) for cells marked by an asterisk.
Abbreviation: SBA, simplified bisecting angle; MIP, modified interproximal.
Sensitivity and Specificity Calculated for Bone Defect Scores.
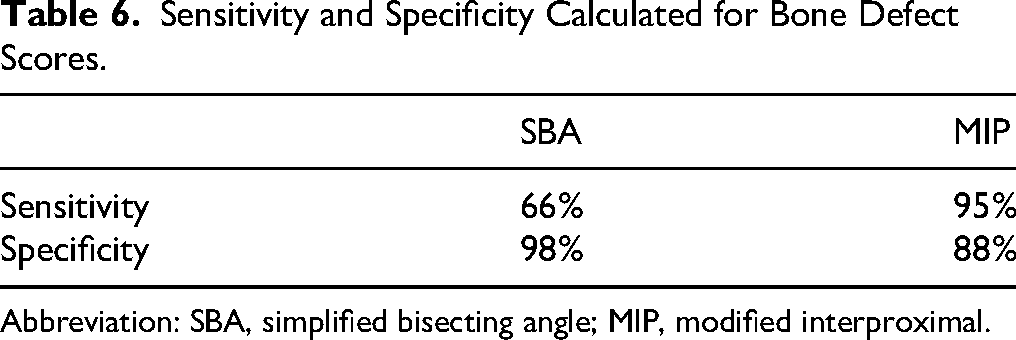
Abbreviation: SBA, simplified bisecting angle; MIP, modified interproximal.
Sensitivity and Specificity Calculated for Furcation Involvement Scores.
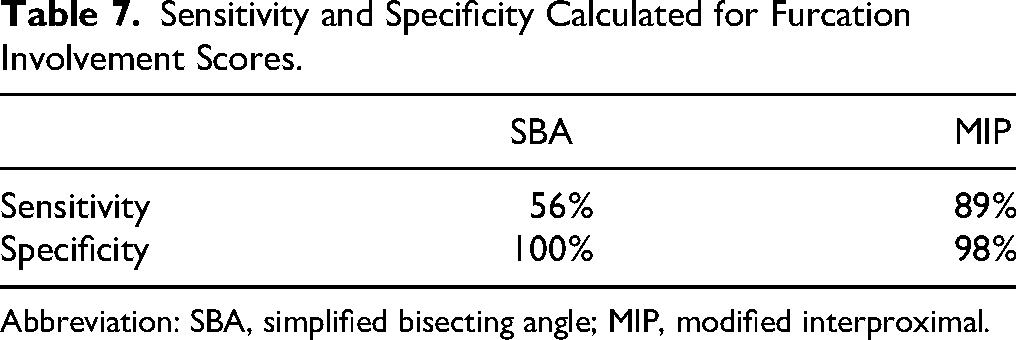
Abbreviation: SBA, simplified bisecting angle; MIP, modified interproximal.
Discussion
The objective of this study was to establish agreement, accuracy, sensitivity, and specificity of the novel MIP technique, in the detection of bony defects surrounding the PM4, and to further compare it to the established SBA technique. As hypothesized, this study showed that the MIP view consistently performed equally or better than the currently employed SBA technique, in the evaluation of the severity of bony defects and furcation involvement in dogs. The almost perfect agreement of scores between the two sittings of Observer 1 for both techniques and for one of two sittings for Observer 2, the other showing substantial agreement, suggests consistency in interpretation of radiographic scores of bone defects and of furcation involvement, regardless of radiographic technique. Moreover, the substantial agreement between the two observers indicates that bone defects were perceived on radiographs relatively similarly despite a widely different number of years of experience between the two observers. Results were similar for Observers 1 and 2, and although differences in interpretation exist, trends were observed in the same direction. Interobserver agreement was lower for Furcation Involvement Scores. The vast majority of disagreements occurred with Grade 3 furcation involvement.
Bone Defect IS was significantly lower than AS, highlighting a tendency for both observers to underestimate the distance between the CEJ and alveolar margin. This was true for both observers, and is reflected in similar studies.10,23,24,30 Furthermore, the delta value between IS scores for MIP technique was not statistically different from AS, indicating that interpretation of the MIP technique was close to reality, which was not the case for SBA technique. Similarly, IS was shown to be smaller than AS for Furcation Involvement Scores, again indicating a trend towards underestimation of disease, although the bias was more pronounced with the SBA technique. Again, the discrepancy between actual and interpreted severity of disease was more pronounced with the SBA technique.
In accordance with the authors’ hypothesis, the MIP technique provided superior accuracy in the evaluation of bone defects surrounding the maxillary PM4. Observers consistently underestimated the distance between the CEJ and alveolar margin by at least one increment (12.5% bone loss) with SBA technique. Accuracy and sensitivity were improved with MIP technique. Sensitivity for SBA technique is insufficient, and a clear bias towards underestimation exists. Detection of mild or moderate defects was poor. The degree of bony defect severity could be underestimated by as much as four scores with the SBA technique (Figure 5). This correlates with a 37.5% horizontal bone defect that may go undetected based on radiography alone. Greater delta values were more often encountered when distance between the CEJ and alveolar margin was greater. This systematic bias could lead to severely afflicted teeth being overlooked by the clinician and therefore retained. MIP technique offers a superior method for evaluation of furcation involvement since sensitivity was 89%.
The lack of difference in IS between Observers 1 and 2 was unexpected since Observer 2 has more years of experience compared to Observer 1. It is possible that during the process of acquiring images and creating the stepwise bone defect lesions on all maxillary PM4 that Observer 1 had gained experience in recognizing the various increments of bone defects, improving overall scoring performance with both techniques when compared to the experienced observer. This may introduce a bias in the current study, as the results obtained by Observer 1 showed significant difference between techniques, although this learning should have occurred equally for both techniques. In the same line of thought, this could mean that the MIP technique is more intuitive, and that learning may occur more quickly with this technique. Observer 1 in this case is the mentee of Observer 2 which could have led to an artificially increased agreement between observers. Considerable exposure to dental radiography during a 3-year residency program may provide a trainee with a sufficient level of expertise to interpret bone loss lesions surrounding the maxillary PM4 at a level equivalent to that of a veterinary dental specialist. This result has also been reflected in some human studies, where, unexpectedly, years of experience of the dental specialist did not affect interpretation of dental radiographs. 9
It is widely accepted that the diagnosis of PD is made by combining clinical findings (periodontal probing) with radiographic evaluation3,7,9–12 and that neither technique alone can accurately define the extent of bone loss. Studies have been performed to determine the clinical relevance of radiographic findings in veterinary medicine.4,5 One frequently cited study stated that radiographic findings revealed that the extent of PD was greater than expected clinically in 26% of cases. 4 This may reflect the low sensitivity of periodontal probing when used alone. In the present study, results show that experienced observers tend to underestimate the distance between the CEJ and alveolar margin on radiographs, which parallel the severity of PD. Considering that both diagnostic tools may overlook some lesions, albeit maybe not in the same situations, any improvement in the accuracy or sensitivity of any method is greatly welcome in order to properly diagnose PD stage and take appropriate action.
Results from this study are difficult to compare to previous publications. It is generally accepted that CT renders a higher diagnostic yield than dental radiographs, as validated in human medicine.17,31,32 Although many veterinary studies have compared dental radiographs to different algorithms obtained with CT or CBCT,8,17 few, if any, have included a gold standard comparable to the current study. Furthermore, radiographic techniques are rarely standardized, and most results are presented for the entire dentition, which does not capture the inherent difficulties presented by the caudal maxilla, namely tooth root superimposition and crowding.
This study found that radiographs helped understand the extent of bone defects, analogous to PD. Recent studies,8,17 comparing radiographic and CT findings report contradictory results as to whether radiographs overestimate or underestimate PD. In the present study, descriptive data showed that compared to the gold standard of macroscopic standardized experimentally induced bone defects, distance between the CEJ and alveolar margin was overestimated 0.5% of the time with SBA technique and underestimated in 73% of instances. This contrasts with the MIP technique where distance is overestimated 3% of the time and underestimated only 34% of the time. This underscores that sensitivity is much improved with MIP. Out of the six cases where distance was overestimated for MIP, five cases were of normal bone height. It is likely that clinical findings would not have led to a change in treatment plan in these circumstances. This reflects the usefulness of the MIP technique in a clinical setting. As shown in Tables 4 and 5, the difference between techniques is observed mainly in mild bony defects (score of 2) and in severe bony defects (score of 5). Since it has been shown that radiographs reveal that bone loss is more severe than clinically anticipated in up to 26% of instances, 4 performing the MIP technique may improve detection of periodontal lesions allowing appropriate treatment to be instigated. The decision is even more critical in borderline cases, when extraction is being considered. The use of MIP technique may prevent the retention of extensively damaged teeth by providing more accurate information to the clinician.
Although this project focused on the maxillary PM4, interpretation of disease for the M1 and M2 is also considered difficult in a clinical setting, for the same reasons. The MIP view may have the potential to aid in the correct diagnosis of bony defects affecting these teeth. Further studies evaluating its usefulness for maxillary molars are warranted.
This experimental model of incremental induction of bone defects offered many advantages. Unlike spontaneous lesions of PD, which present a very wide spectrum of bone loss, this experimental model allowed establishment of an unequivocal bony defect %, facilitating data analysis. The creation of horizontal bony defects used in this study mimics the most common pattern of bone loss in PD in companion animals 8 and was selected for this reason. It is possible that a vertical pattern of bone loss or dogs with spontaneous lesions of PD may have produced different results. Aside from subjective clinical experience, there is no data available qualifying the patterns of natural PD in dogs, in various regions of the mouth. Naturally occurring lesions combine both horizontal and vertical bone loss to varying degrees, and the alveolar margin may be irregular. The edge of natural bone loss may be more gradual than that seen in the model in this study. The creator of the model tried to taper the edge of the artificial lesions, although it remained sharper than a natural lesion, increasing its visibility on dental radiographs and this would have affected both radiographic techniques equally. Ultimately, sequential lesioning allowed progressive severity assessment in each cadaver, reducing the overall sample requirement.
A Williams periodontal probe was used to measure increments between scores for bone defects. This instrument exhibits markings at 1, 2, 3, 5, 7, 8, 9 and 10 mm, with markings missing at 4 and 6 mm. Although this instrument only measures with mm-level precision, it has been widely utilized in numerous studies.10,24 The shortest root measured in this study was 12 mm. A 12.5% difference in the height of the bone margin represented 1.56 mm. The observers were tasked with distinguishing lesions based on a 12.5% increase in bone loss. With a tolerance of 50% of the interval between marks on the periodontal probe indicating the intended bone removal, the increment remained within a range of 1.6 ± 0.5 mm, ranging from 1.1 to 2.1 mm. This distance increased as the size of the dogs increased. While one might speculate that the accuracy of discrimination improved with larger dogs, this aspect was not addressed in the study. In retrospect, the use of an electronic caliper could have helped reduce variability in the amount of bone removed. However, since the defects were manually created using dental burs, some degree of imprecision in standardizing the lesions is to be expected. The authors estimate this would represent less than 0.25 mm, or ¼ of the distance between markings on the periodontal probe, as this would be visible to the operator wearing loupes while creating the lesions. The caliper could also have been employed to measure the full root lengths, which exceeded 10 mm, thereby improving measurement accuracy. It is possible that minor variations occurred during the creation of individual defects, although these would not have been cumulative, as each increment was produced and measured independently of the preceding one from the CEJ. The authors consider that such variations are unlikely to have affected the study's results, since the observers evaluated the radiographs based on predetermined stages rather than by directly measuring the lesions.
The study did not employ a guide to standardize patient positioning, film, or tube head placement, relying instead on careful visualization and positioning by the researchers. While such a guide could have enhanced image consistency, its use would not replicate real-world clinical practices. In veterinary practice, the bisecting angle technique has been adapted for evaluating periapical pathology and PD in animal patients. Unlike in human dentistry, where a parallel view is preferred for assessing bone loss due to reduced distortion, this approach is impossible in many oral regions of dogs, primarily due to the absence of a palatal vault. The bisecting angle technique in veterinary dentistry does not mandate a specific angle; rather, the film and tube positioning must align with the individual patient's anatomy. To aid practitioners in capturing images more effectively, a simplified technique has been developed, employing a predetermined angle and plate position. For the MIP, the choice of a 70-degree angle was informed by extensive clinical experience, ensuring practicality in plate and tube placement, akin to the simplified technique. This angle was found optimal as it diverges sufficiently from the 45-degree angle to provide a distinct view while ensuring the apices remain within the field of view.
For this study, the MIP technique was performed in lateral recumbency. However, acquisition of this radiographic projection can be achieved in other positions. The only requirement is that the plate is angled 70 degrees from the median plane of the palate and the tube directed perpendicular to the film in a ventro-medial direction.
Full-mouth radiographic surveys have been advocated in veterinary dentistry since the late 1990's and are now considered the standard of care.1,3,5,14,15 Benefits of improved diagnostics, considering the prevalence of undetected lesions 5 outweigh the effects of radiation exposure to the patient. Exposure of veterinary personnel to radiation must also be considered when requesting additional radiographic views; therefore, the MIP technique could be reserved for selected cases in which PD is suspected or anticipated. Many radiographic protocols can be used and adapted to every patient's needs. The MIP technique has been shown to perform better than the SBA technique. When confronted with severe lesions and debating root planing against extraction, the MIP view may aid in determining proper treatment and prognosis.
For standardization of the radiographic view, and to avoid technical difficulties associated with dental anatomy of brachycephalic dogs, only mesaticephalic or dolicocephalic large breed dogs with a healthy periodontium were used.
This experimental model of bone defect induction was used because it made possible the comparison between the two techniques for their ability to discriminate between standardized lesions. It is repeatable and it can be done using fewer subjects than working with natural lesions and progressive disease. A study on natural lesions would be indicated to support the conclusion of this study.
In conclusion, the MIP technique is a useful tool in the evaluation of bony defects in the caudal maxilla of dogs, and is more accurate, sensitive and specific than the modified bisecting angle technique. If the MIP technique performs similarly in spontaneous lesions associated with bone loss as a result of PD, it will improve confident decision making by dental professionals. Based on this experimental study model, the MIP technique is recommended as an additional projection to the full-mouth survey performed in dogs.
Materials
(a) Williams periodontal probe (PCPUNC128 X6), Hu-Friedy Mfg. Co., LLC, Chicago, IL, USA.
(b) Phosphor plates, CR7 Vet, Durr Medical, Bietigheim-Bissingen, Germany.
(c) Belmont Phot-XIIS 628-1-G CIR: 47, Takara Belmont Corporation, Tokyo, Japan.
(d) Randomness and Integrity Services Ltd, Dublin, Ireland, https://www.random.org.
(e) Synapse 5, FujiFilm, Tokyo, Japan.
(f) Horos, The Horos Project 2022, Nimble Co LLC d/b/a Purview, Annapolis, MD, USA.
(g) BenQ PD3200, BenQ Corporation, Taipei, Taiwan.
(h) Apple, Cupertino, CA, USA.
(i) RadiAnt DICOM Viewer Software, Version 2021.1., Medixant, Poznan, Poland (https://www.radiantviewer.com).
(j) SAS System for Windows, Version 9.4, SAS Institute, Cary, NC, USA.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fonds du centenaire, (grant number SFMVA023).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.