
Abstract
Many dental homecare products are marketed, several of which have been evaluated using a “clean tooth” protocol (the teeth are scaled at the start of the trial). The efficacy of dental products in dogs that have not had their teeth professionally cleaned (“dirty tooth model”) has been studied far less often. Some dogs for which professional dental cleaning is indicated will not have their teeth cleaned because of anesthetic risk or for other reasons. In this study, 6 dental homecare products were evaluated against a negative control group; none of the dogs received professional dental cleaning at the start of the study. The home care protocols tested were: brushing every other day using a toothpaste, feeding a dental chew once daily (VF), adding a water additive in the water daily (AQ), brushing once a week + VF daily, brushing once a week + AQ daily, VF + AQ daily. Dental deposits (plaque and calculus) and periodontal health were assessed on awake dogs, before and after receiving the assigned homecare regimen for 8 weeks. Results were compared with an untreated control group. Dental deposits were reduced by regular mechanical action (brushing or VF daily). Periodontal health status was improved when AQ daily was combined with either brushing once a week or VF daily. Two scoring techniques useful for determining a recommendation from a veterinarian to commence home oral hygiene or recommend dental scaling as a necessary first step are described.
Keywords
Introduction
Maintaining good oral health is a component of good general health and well-being; regular oral hygiene is necessary to keep a dog's teeth and gingiva healthy. It is estimated that most dogs develop some form of periodontal disease (PD) by 1 year of age. 1
Plaque starts to adhere to the dental pellicle within 24 h following scaling and mineralization of plaque to form dental calculus starts approximately 3 days following scaling. Plaque in the subgingival sulcus can allow anaerobic bacteria to thrive, resulting in gingivitis, which can evolve into periodontitis (loss of connective tissue attachment and alveolar bone).1,2 The prevalence and severity of PD increase with age, particularly in small-breed dogs. 3
Periodontal disease is underestimated and undertreated, partly because of a lack of awareness by owners, and because most dogs with moderate or even severe PD continue to eat until halitosis, dental pain and other outward signs resulting from severe PD become obvious to the owner. 1 When severe, PD can be painful and can lead to deleterious local consequences, such as tooth loss, oronasal fistula, or pathological jaw fracture. Bacteremia occurs, which is associated with deleterious changes in distant organs.1,2 Although PD is a multifactorial disease, frequent and regular dental homecare using efficacious products can help prevent or slow down the progression of the disease.
As in humans, tooth brushing is the “gold standard”; however, owner compliance in dogs is low, even when recommended by a veterinarian, 4 as it involves interaction between the owner and the dog, and often the dog may not cooperate and allow brushing. Many dental homecare products for dogs and cats that do not require brushing are now available on the market. Options requiring less interaction between the owner and the dog include dental diets and dental chews designed to help remove dental deposits by mechanical action, or use of chemical anti-calculus or anti-plaque retardants incorporated in or on the surface of canine diets or dog treats, or gels or sprays spread on the gingiva, and drinking water additives. Some of these products have a proven plaque and calculus retardation effect when evaluated using a clean tooth model, and have been awarded the Seal of Acceptance of the Veterinary Oral Health Council (VOHC) based on trials conducted under VOHC protocolsa that include professional teeth scaling on day 0, with assessment of plaque and calculus accumulations compared with a negative control group at 28 days post-scaling. The VOHC trial protocol requires that the dogs are anesthetized during the trial. Efficacy of dental products in dogs that have not had their teeth professionally cleaned (“dirty tooth model”) has been studied far less often.5–7
Some dogs cannot be anesthetized due to their general health condition or for other reasons. In order to help veterinarians identify an appropriate dental homecare protocol for their patients, especially for those patients who cannot be anesthetized for professional teeth cleaning, this study was performed using dogs that did not have their teeth professionally scaled, to determine whether dental homecare alone could help remove dental deposits and maintain or improve oral health. Six oral hygiene regimens were evaluated and compared with a negative control group.
Material and Methods
Animals
125 client-owned dogs were recruited for the study. All procedures performed during the study were conducted according to standard veterinary care procedures and following Polish Regulations (Art.1 ust.2 pkt1 Dz. U.2015 poz. 266). The study was approved by the Virbac Ethical Review Committee (Approbation numbers: EU-ERC/2O2O11-08).
The dogs were well-behaved, of any breed, any age, and any sex/neuter status. Breeds included: Cavalier King Charles Spaniel; Alaskan and Siberian Husky; Jack Russell Terrier; Maltese Terrier; German Shepherd; Newfoundland; Greyster; Miniature Spitz; Labrador; Welsh Corgi; Shih Tzu, Chihuahua and Pinscher. They were required to be in good general health and have all 8 target teeth present (maxillary third incisor [103, 203], canine [104, 204], third and fourth premolar [107, 207, 108, 208]). Dogs with severe PD (tooth mobility on palpation, full furcation involvement, >50% loss of attachment), having systemic disease, on prescribed medications, or pregnant, were excluded. Dogs that would not allow their teeth to be brushed, were unwilling to chew a dental chew, or that refused to drink water containing an additive, were also excluded.
Design and Randomization
The study lasted 16 weeks. During the entire study period, the dogs were fed the diet they were fed by the owner prior to the study.
On day 0, the body weight was recorded and the dental deposits and periodontal health (PH) status of the 8 target teeth were evaluated and recorded. These observations were all performed by the same board-certified veterinary dentist who used magnification and a headlight loupe. No instruments were used in the mouth and no radiographs were obtained.
During the first 8-week wash-out period, the owners were not allowed to use any dental homecare products (toys, treats, etc.). After 8 weeks with no oral hygiene, the dogs were re-examined and randomized into 7 groups based on PH statusb. Average body weight per group was then calculated; no significant differences existed between the groups for body weight.
During the second 8-week period (test period), the owners agreed to follow one of the following assigned protocols:
Brushing every other day using the toothbrush and toothpastec that has proven efficacy on oral bacteria,
8
“BR-CET” group, n = 15. The owners were taught to use the brushing technique described by VOHCa. One dental chewd given daily. This dental chew is designed to control plaque and calculus accumulation
9
and has been awarded the VOHC Seal of Acceptance; “VF” group, n = 15. Drinking water additivee given daily. This water additive contains pomegranate, which is known for its anti-aggregative and antioxidant effects
10
and for its effects against canine oral bacterial species.
11
“AQ” group, n = 15. A recent study has shown AQ is effective in controlling plaque and calculus accumulation after a professional dental cleaning.
12
Brushing once a week + one VF chew daily. “BR + VF” group, n = 15. Brushing once a week + AQ water additive daily; “BR + AQ” group, n = 15. One VF chew daily + AQ water additive daily; “VF + AQ” group, n = 15. Negative control, no oral hygiene permitted; “Control” group, n = 35.
On weeks 8 and 16, the target teeth (103, 203, 104, 204, 107, 108, 207, and 208) were observed and scored for deposits and PH, as described above, by the same blinded investigator. The scores for the most severely affected tooth on week 8 were analyzed by comparison with the scores in the same teeth at 16 weeks. In some dogs, there was more than one tooth scored as “worst” at 8 weeks; the mean of the scores of those specific teeth at 16 weeks in those dogs was used in the analyses. The scores for deposits and PH were analyzed independently.
Evaluation of Dental Deposits
Scoring was performed using undisclosed, visually evident plaque and calculus as follows: 0 = none; 1 = <25% of the buccal crown affected; 2 = 25-50% of the buccal crown affected; 3 = 50-75% of the buccal crown affected; 4 = >75% of the buccal crown affected.
Evaluation of Periodontal Health Status
Scoring was performed as follows: 0 = healthy (no gingivitis evident); 1 = gingivitis only (no apparent alveolar bone loss); 2 = early periodontitis (loss of less than 25% estimated root height); 3 = moderate periodontitis (up to 50% loss of estimated root height). Dogs with severe periodontitis had been excluded prior to randomization.
Statistical Analysis
Due to the ordinal nature of the data, non-parametric tests were used. The analyses were performed in the R environment.f To compare the intra-group scores between week 8 and week 16 for the parameters assessed (dental deposits and PH status), Wilcoxon signed-rank tests were used. To assess the significance of the inter-group comparisons observed between week 8 and 16, Kruskal-Wallis tests were used for each parameter on the difference of scores observed between week 8 and week 16 for each dog (score on week 16 − score on week 8). When significant differences were detected, multiple comparisons using the Dunn Test were performed with Benjamini and Hochberg (BH) correction for multiple testing. Results are expressed as median (Q1; Q3) of the scores at each time point or median of the change of scores between time points. The α threshold for significance was set at 0.05.
Results
Characteristics of the Dogs
The mean (±SD) body weight and ages of all dogs were 16.3 ± 13.0 kg and 58.4 ± 38.3 months, respectively.
The characteristics of the dogs in each group are summarized in Table 1. The changes in dental scores from 8 to 16 weeks for coverage by plaque and calculus (deposits), and PH status of the worst tooth/teeth at 8 weeks were calculated.
Summary of the Characteristics of Dogs in Each Group at Day 0.
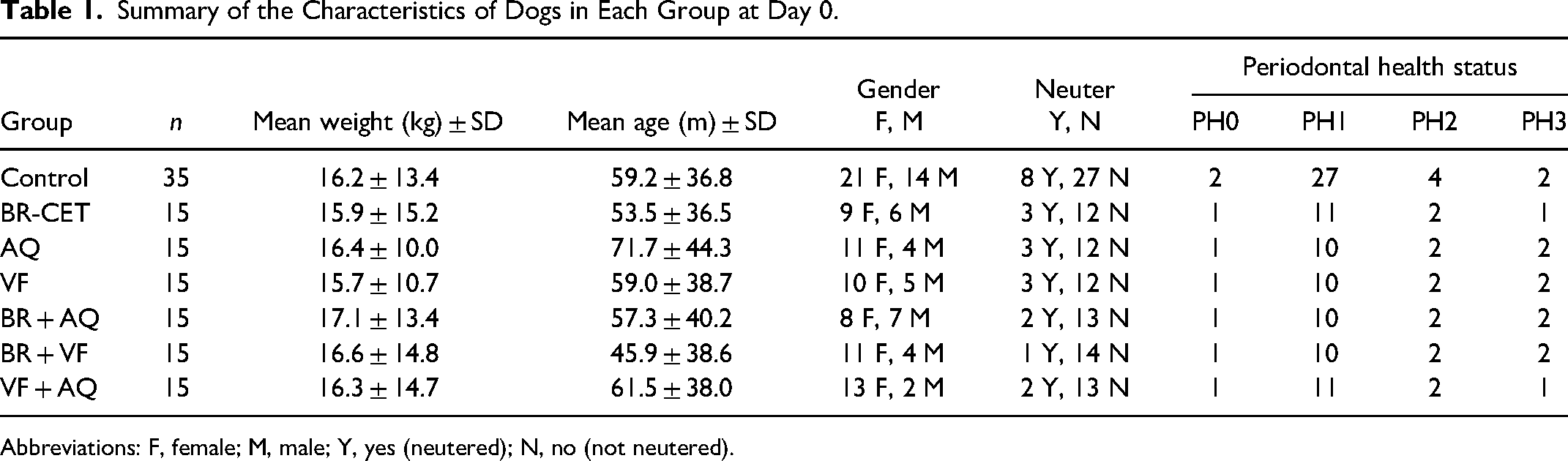
Abbreviations: F, female; M, male; Y, yes (neutered); N, no (not neutered).
Deposits (Plaque and Calculus)
When comparing the 8- to 16-week changes within each group (Table 2), dental deposits were significantly reduced by week 16 in all groups (P < 0.05).
Scores Obtained for Each Oral Care Regimen at Weeks 8 and 16 and the Difference of Scores Between These Time Points Assessed in Each Dog.
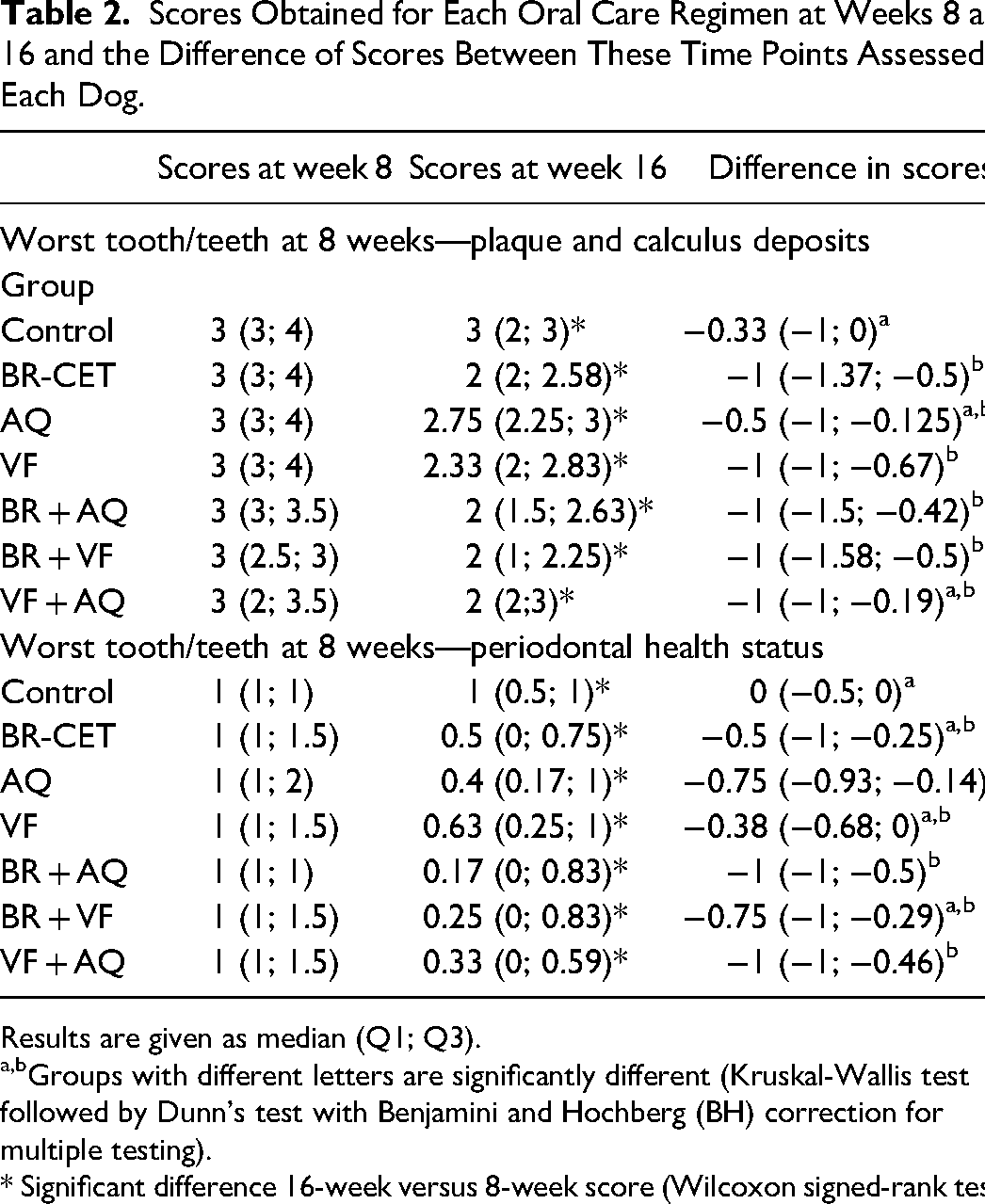
Results are given as median (Q1; Q3).
Groups with different letters are significantly different (Kruskal-Wallis test followed by Dunn's test with Benjamini and Hochberg (BH) correction for multiple testing).
* Significant difference 16-week versus 8-week score (Wilcoxon signed-rank test).
When comparing the change in scores between the different groups, the changes in the following groups were significantly different from the change in the control group (P < 0.05; Table 2; Figure 1):
Dental brushing every other day (“BR + CET”) Dental chew daily alone (“VF”) Brushing once a week + water additive daily (“BR + AQ”). Brushing once a week + dental chew daily (“BR + VF”).
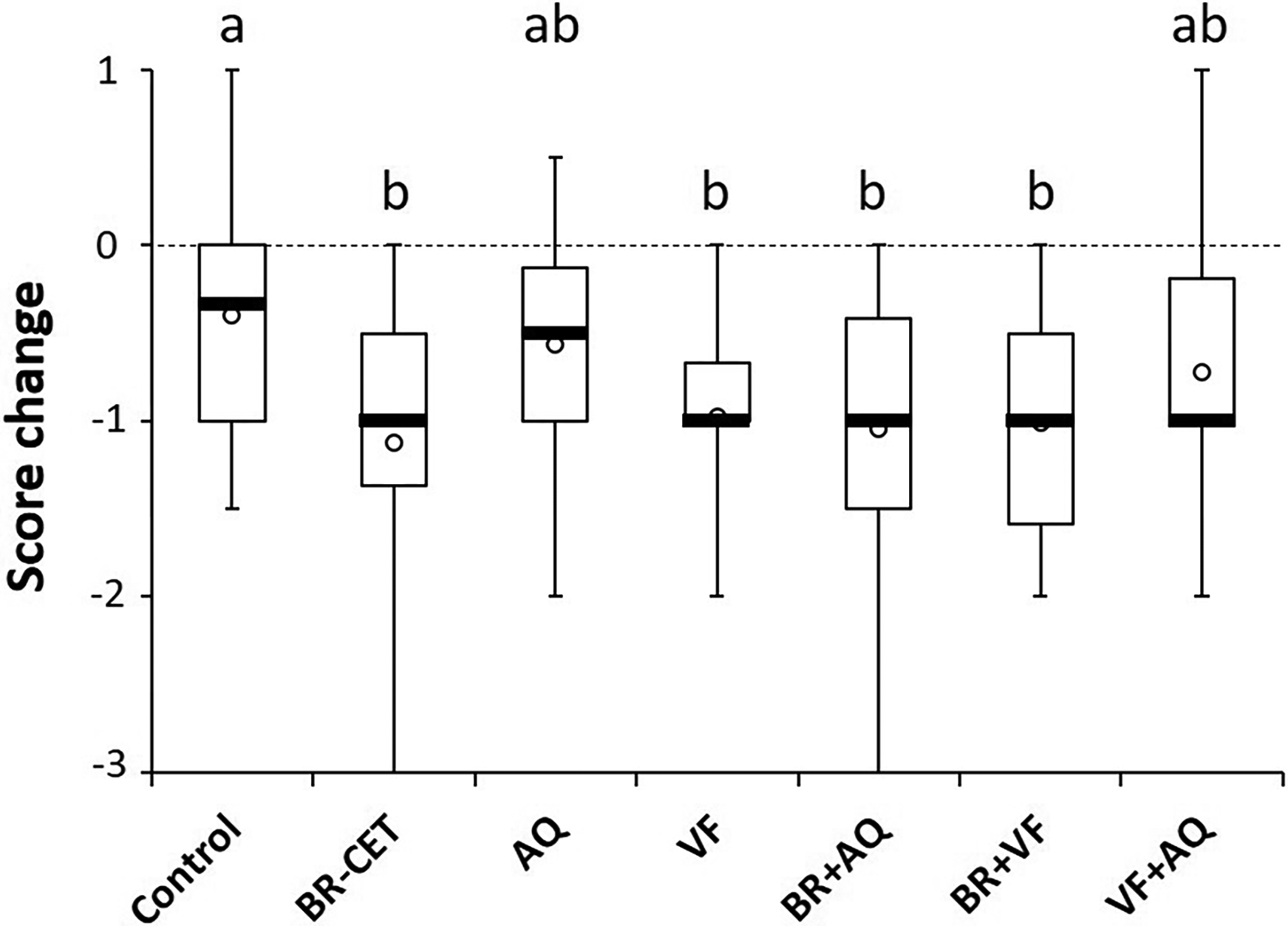
Box and whisker plots showing the changes in deposit scores in each group. Difference of scores between week 8 and week 16 were assessed in each dog and the repartition of the difference is shown in this plot. a,bGroups with different letters are significantly different (P < 0.05; Kruskal-Wallis test followed by Dunn's test with Benjamini and Hochberg (BH) correction for multiple testing).
Periodontal Health Status
Periodontal health status improved between 8 and 16 weeks in all groups (P < 0.01; Table 2). The inter-group comparisons showed that only the change of scores in the groups BR + AQ and VF + AQ was significantly different from the change observed in the control group (P < 0.01; Table 2; Figure 2).
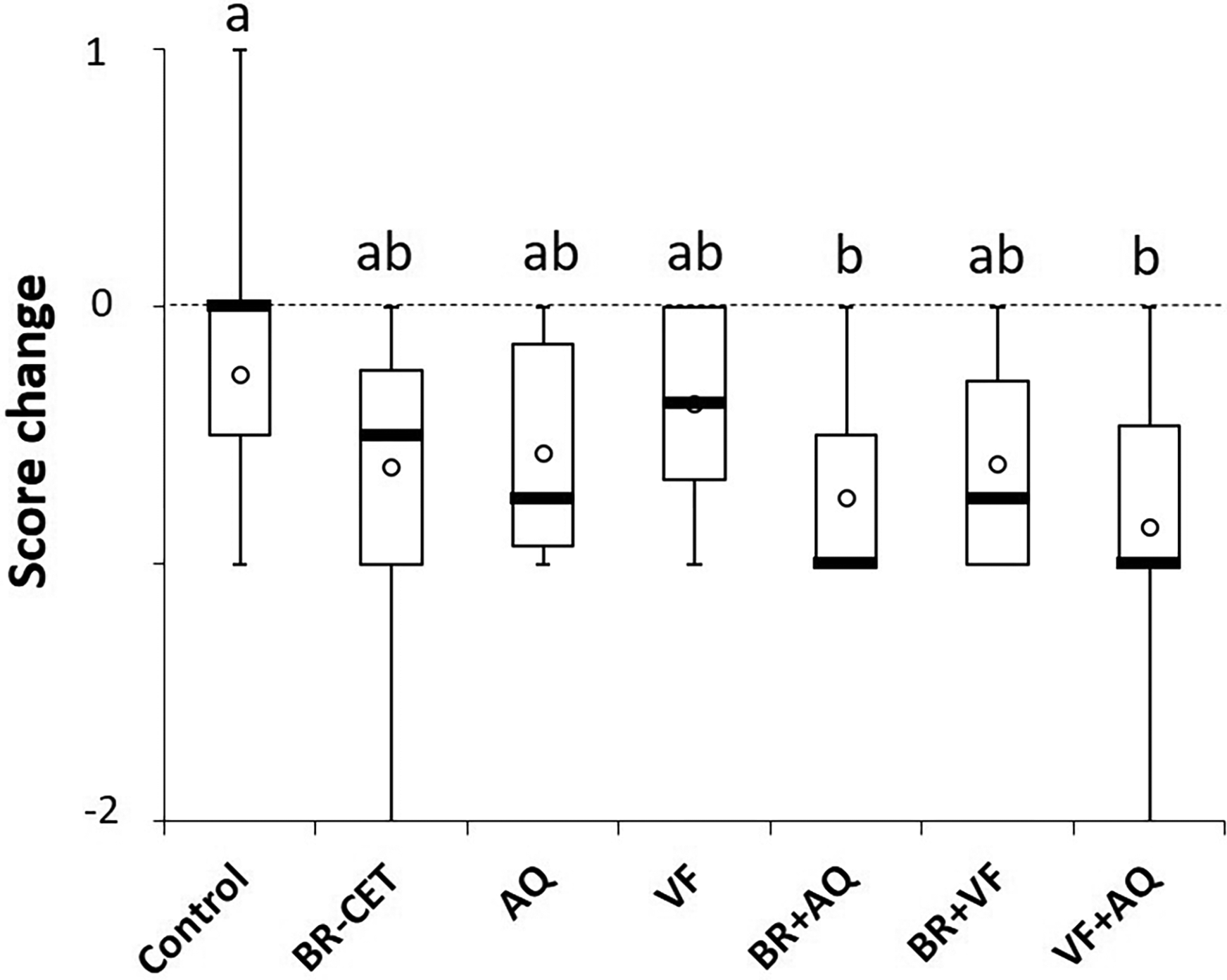
Box and whisker plots showing the changes in periodontal health scores in each group. Difference of scores between week 8 and week 16 were assessed in each dog and the repartition of the difference is shown in this plot. a,b Groups with different letters are significantly different (P < 0.01; Kruskal-Wallis test followed by Dunn's test with Benjamini and Hochberg (BH) correction for multiple testing).
Discussion
This study was performed on dogs that did not receive a professional teeth cleaning at the start of the study. The decision to not include scaling was made because many dogs are not scaled regularly or even not at all, whether because of high anesthetic risk or other reasons. Information that would determine the need for periodontal treatment in these dogs or identifying home oral care products that are effective when the teeth cannot be scaled would be useful.
Two factors are required to determine appropriate procedures for periodontal management of dogs that will not undergo anesthesia. One is a credible method of determining the extent of existing abnormality—will instituting home care likely be of value, or is the patient sufficiently diseased that the recommendation must be to proceed with treatment (e.g., scaling, periodontal surgery, or extractions) even if the patient has a poor anesthetic risk?
The second is a means of determining which products will likely be effective, by comparing results over time with a negative control group.
The VOHC's product effectiveness trial protocolsa (Veterinary Dental Product Submission Protocols) take a firm science-based stance by requiring use of a “clean tooth” model (the teeth must be scaled under anesthesia on day 0), with plaque and calculus scoring also conducted under anesthesia (except when the Gingival Contour Plaque index is used in trained awake dogs). For the objectives undertaken in this trial, anesthesia was not permitted, so an awake oral examination system was required. There have been many dental trials, human and canine, conducted without using anesthesia for scoring. For humans, this is not usually a problem—even periodontal pocket measurements using probes, and a full dental radiographic examination, can be conducted in awake, informed human patients. Most awake dogs would likely not tolerate this extent of manipulation of the mouth. The literature on awake periodontal examination in dogs was reviewed; the most commonly reported technique is lifting the lip to observe or photograph the buccal surfaces of the teeth.5,7,13–18 Dental deposits are recorded on a chart as either a map showing areas covered, or by applying a qualitative subjective scoring index. An alternative for scoring plaque is the Gingival Contour Plaque Index, 19 which has been approved for use in trained, awake dogs in VOHC trials. Periodontal health assessment has been used in unanesthetized dogs in the past, typically using a Gingivitis index or Gingival Bleeding index.6,15,16
An epidemiological study of 29,702 Polish dogs was used to develop an Oral Health Index (OHI) for use in awake dogs; 17 the single time-point examination consisted of identifying the worst-affected tooth and recording the dental deposit coverage (plaque and calculus—scored from 0 = none to 2 = >50% coverage), and the PH (scored from 0 = no gingivitis to 2 = periodontitis). The size of lymph nodes was also scored and added to the OHI score.
The OHI was presented as a system that would assist in differentiating dogs that required commencement of home oral hygiene only, or that required professional examination, scaling, and possibly more extensive treatment such as extraction under anesthesia. The dental deposits and PH scoring methods in that study were adapted for use in the present study—the deposits score was expanded to a range of 0-4 and the PH score was expanded to 0-4, where 4 = severe periodontitis, including tooth mobility and full furcation involvement—dogs with a PH score of 4 at week 8 were excluded from the present study. Lymph node scores were not used in the present study.
The homecare protocols tested included either brushing every other day or the use of a dental chew or a water additive daily, either alone or in combination with weekly teeth brushing. The group of dogs that were brushed every other day was used as the positive control. Brushing every day was not included in order to improve compliance during the trial period, and because brushing every other day has been found to significantly retard plaque and calculus accumulation as well as gingivitis in dogs. 20
Although the plaque and calculus deposits and PH parameters tested are related, the authors considered them independently for analysis as it was assumed that some homecare protocols would be more effective on one score versus the other. The mechanical action that brushing or a dental chew provides can have an influence on the supragingival plaque and calculus but likely less so on the subgingival tissues. It may be the contrary for a water additive that could have a chemical effect within the gingival sulcus, as suggested in a previous study. 12
The study confirmed that the mechanical action resulting from brushing every other day or giving a dental chew daily was effective at reducing deposits and maintaining PH status. Surprisingly, giving the dental chew and water additive daily did not significantly reduce the deposits as expected when compared to the control group, despite the reduction in score between weeks 8 and 16. This may be due to a sample size or higher variability effect in this group.
Interestingly, only the combinations of brushing once a week plus water additive given daily or dental chew with water additive both given daily were able to produce a significant improvement of PH status compared with the control group, while the latter combination had no significant effect on deposits. Brushing once weekly by itself does not provide significant protection, as previously demonstrated, 20 and water additive alone did not produce significant improvement in deposits or PH, suggesting that both the mechanical action provided by the weekly brushing or daily dental chew and the chemical action provided by the water additive daily is required for better results on PH status in unscaled dogs. The water additive used in this study has been shown to reduce the gingival bleeding index in dogs that had their teeth scaled and polished prior to receiving the product every day for 1 month. 12 The results obtained from this previous study 12 and the one presented here suggest that the water additive can have beneficial effects on the gingiva and PH when the teeth are cleaned or in teeth with a low extent of deposit coverage but it is less or not effective when deposits are more extensive.
Overall, the only oral hygiene regime that can partly remove deposits and improve PH was weekly brushing combined with water additive daily. The low “n” per group resulting from inclusion of 6 oral health protocols and a negative control group could have resulted in greater variability in the results. Repeating this study using a larger number of dogs in the groups of interest is indicated.
Unscaled dogs with greater extent of deposits and poorer PH status will require alternatives to the homecare protocols tested here since none were effective in eliminating deposits and improving PH status to normal. If scaling under anesthesia is not possible, some possibilities not tested in this study would be to combine brushing every other day with both the dental chew and water additive daily or brushing daily along with either or both of these products.
This study has demonstrated that, in dogs that have not received professional scaling under anesthesia:
One dental chew per day, or brushing every other day, or both can partly remove dental deposits on dogs with dental deposits and no gingivitis. Brushing once a week and giving the water additive daily can help improve the PH of dogs and reduce the extent of deposits. A combination of several dental homecare protocols (such as brushing every day + dental chew + water additive daily) may help further reduce the extent of deposits and improvement in PH; this combination was not tested in this study.
This study and the documented results are not designed to encourage treatment of PD without scaling. Professional scaling should always be considered if the general health condition allows, to optimally prevent the local and systemic consequences of PD.2
Materials
VOHC website. https://vohc.org/. Accessed 10/26/2024. Research Randomizer, https://www.randomizer.org/ CET oral hygiene toothbrush and toothpaste, Virbac, France Veggiedent® FR3SH™ dental chew, Virbac, France Aquadent® FR3SH™, Virbac, France https://www.r-project.org/
Footnotes
Acknowledgments
The authors would like to thank the veterinary nurses who were members of the research team: Joanna Warzecha, Justyna Matusinska, and Natalia Hucko-Pietka.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Celine S. Nicolas is a Virbac SA employee, and Jerzy Gawor and Colin Harvey received financial support from Virbac SA. The remaining author declared that he has no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Virbac SA.