
Abstract
Medical records of dogs with an initial histopathological diagnosis of odontogenic sarcoma were reviewed for information on signalment, body weight, medical history, clinical signs, physical examination and diagnostic imaging findings, surgical procedure performed, and histologic characteristics. Twenty dogs were deemed to fit the criteria following the rigorous histology review process. These tumors were characterized by hypercellularity of the spindle cell component with less intervening stroma, mitotic activity, and variable presence of odontogenic epithelium and hard substance (cementum/dentin/bone). Non-invasive or locally invasive hypercellular peripheral odontogenic fibroma is suggested by the authors to describe these tumors. There were no signs of recurrence of any of the masses following surgical excisions with varying margins.
Keywords
Introduction
Peripheral odontogenic fibroma (POF), formerly known as fibromatous epulis of periodontal ligament origin (FEPLO) is one of the most commonly diagnosed canine odontogenic tumors. The true odontogenic origin of POF is controversial as the precise origin of the fibroblast population is debated. 1 It is unclear if the fibroblasts arise from periodontal ligament versus mucoperiosteal/alveolar crest fibroblasts or other origin. 2 Nevertheless, POFs are mixed tumors in the oral cavity associated with tooth-bearing tissues, namely odontogenic epithelium, a mesenchymal component, and mineralized cemento–osseous matrix (osseodentinous matrix) is often present. 2 While POFs often contain 3 components (epithelium, mesenchyme, and cemento-osseous matrix), the defining feature of this lesion is mesenchymal/fibroblast proliferation, which resembles the periodontal ligament mesenchyme. 2 This mesenchyme is composed of stellate fibroblasts embedded within a fine fibrillar collagenous stroma resembling the periodontal ligament in the region of gingival attachment of the tooth. 2 Dilated, empty blood vessels are also noted within this mesenchyme. The amount of odontogenic epithelium and cemento–osseous matrix present in POFs varies greatly among dogs and does not seem to affect the prognosis or behavior of this lesion.
Hypercellular variants of POFs (HPOFs) have been identified histologically, in which the fibroblasts are increased in number, with less intervening collagenous matrix and in some cases, increased mitotic activity. The behavior of these lesions is not well understood, and the level of hypercellularity on histology can raise concern since hypercellularity can be a criterion for malignancy in some mesenchymal lesions in the oral cavity and other sites. Occasionally, extension into the periodontal ligament region is noted in the area of gingival attachment of the tooth, consistent with these lesions arising from tooth-bearing structures. Some lesions abut the alveolar bone, without invasive behavior. In rare instances, invasion of the alveolar bone is present, suggesting potential for locally invasive behavior in rare cases.
The authors suggest the terms noninvasive HPOF and locally invasive HPOF to describe these tumors. The authors aim to describe the clinical, radiographic, and histopathologic characteristics of these lesions to aid in the development of prognostic standards and proper treatment recommendations.
Materials and Methods
Case materials were reviewed for 20 dogs with gingival masses that had a histopathologic diagnosis of HPOF, atypical POF, POF with atypia, odontogenic sarcoma, periodontal fibrosarcoma, low-grade soft tissue sarcoma, or low-grade fibrosarcoma. The biopsy specimens had been submitted to a histopathology servicea between 2010 and 2021. The specimens were obtained from dogs treated at a private dentistry and oral surgery referral practice as well as from dogs treated by regional referring veterinarians. Cases without available clinical follow-up after incomplete resection (debulking) of the mass were excluded from the study. Cases either without any or with scant odontogenic epithelium on histopathology evaluation were also excluded. Other odontogenic mixed tumors (eg, ameloblastic fibromas, amyloid producing odontogenic tumors) were also excluded. The cases were reviewed by 2 board certified veterinary pathologists, MDS and BP.
Information acquired from the medical records included breed, age, sex, tumor location, histopathologic characteristics, type of surgery, and outcome (recurrence). Additional clinical information such as intraoperative photographs, dental radiographs, weight of the patient, preoperative history, clinical signs, physical examination, radiographic findings, and surgical procedure was available for some dogs. Postoperative result clinical information about recurrence was obtained by verbal and electronic mail communication with the primary or referring veterinarian (6 to 36 months postoperative period).
Results
The signalment of each dog, tumor location, treatment, and period of reoccurrrence is reported in Table 1. HPOF (noninvasive and locally invasive) was diagnosed in dogs with ages from 3 to 14-years old (mean age of 8.6 years). There was no obvious sex predisposition. Nine dogs were Labrador Retrievers and Golden Retrievers, and a variety of small and large breed dogs were also represented. Eight of the tumor cases occurred in the maxilla while 12 occurred in the mandible. The rostral maxilla was affected in 63% (5/8) of maxillary cases, while the rostral mandible was affected in 75% (9/12) of mandibular cases.
Clinical Data.
In this study, 50% of the dogs (10/20) were treated by a definitive surgery (ie, maxillectomy or mandibulectomy). The other half of the samples obtained were for biopsy purposes and were treated by debulking. No recurrence was seen in any dog, with the follow-up period ranging from 6 to 36 months. There were no significant long-term postoperative complications recorded in these dogs, whether or not they received definitive surgery.
Clinical images were available for 6 dogs (cases #6, #7, #9, #14, #16, #20). Dental radiographs were available for review in all 6 dogs and a CT scan was obtained in 1 patient (case #9). In the dental radiographs, 2 dogs had osteolysis of the alveolar bone (Figure 5B), 2 dogs had displaced tooth/teeth (Figure 3B), and 4 dogs had osteoproduction/proliferation adjacent to or within the tumor (Table 2, Figures 2B, 3B and 4B).
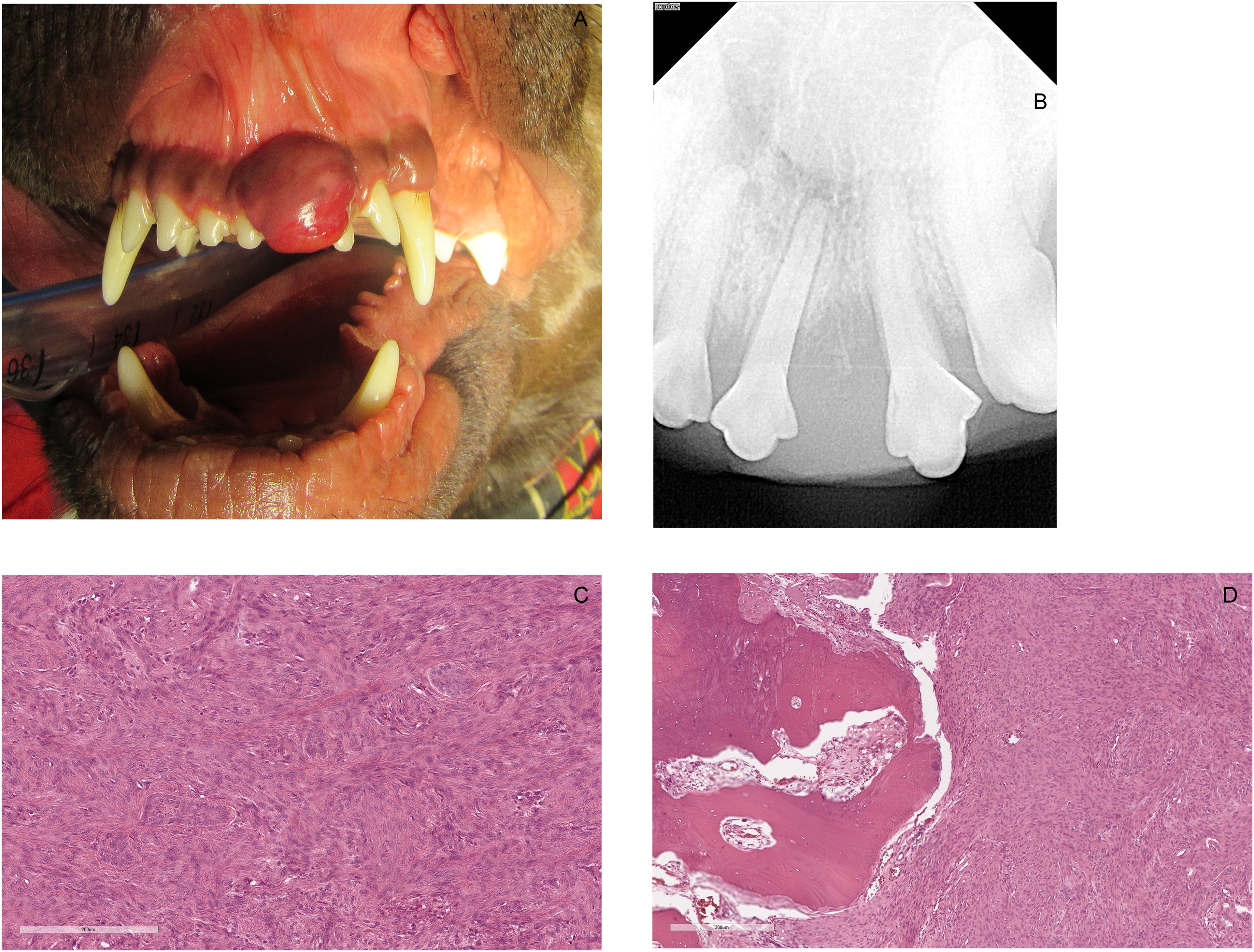
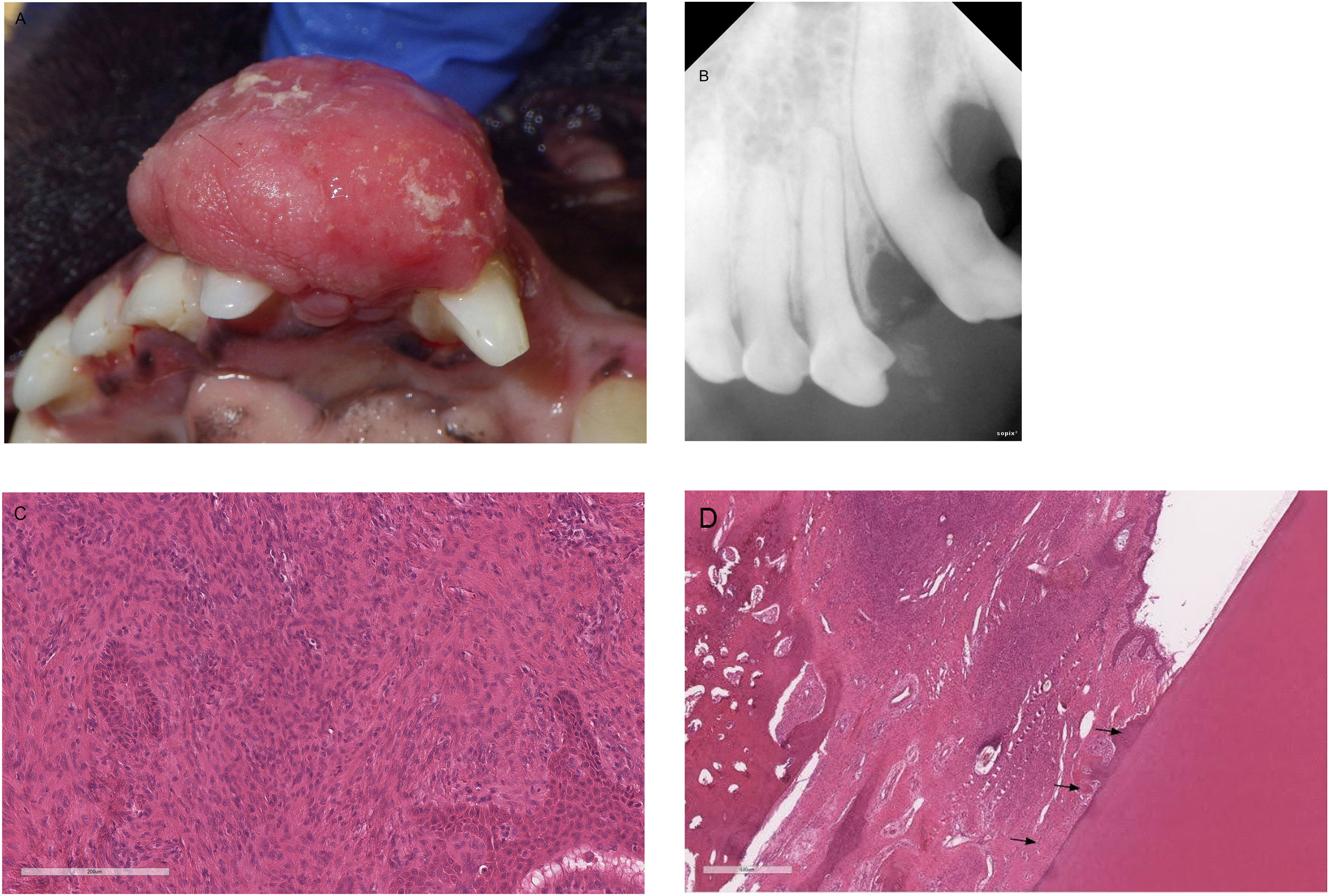
Case #16. (A) Photograph showing a red, round, ulcerated HPOF displacing the left maxillary first incisor tooth (201) mesially and second incisor tooth (202) distally. (B) Dental radiograph of the rostral maxilla showing focal osteolysis of the bone around teeth 201, 202 with periapical lucency and widened periodontal ligament space of 201 resulting in tooth displacement. (C) Photomicrograph showing a hypercellular region with odontogenic epithelium (H&E, 20×). (D) The lesion abuts the alveolar bone with invasion and regional osteolysis of the alveolar bone and lack of inflammation (H&E, 10×). Abbreviations: HPOF, hypercellular peripheral odontogenic fibroma; H&E, hematoxylin and eosin.
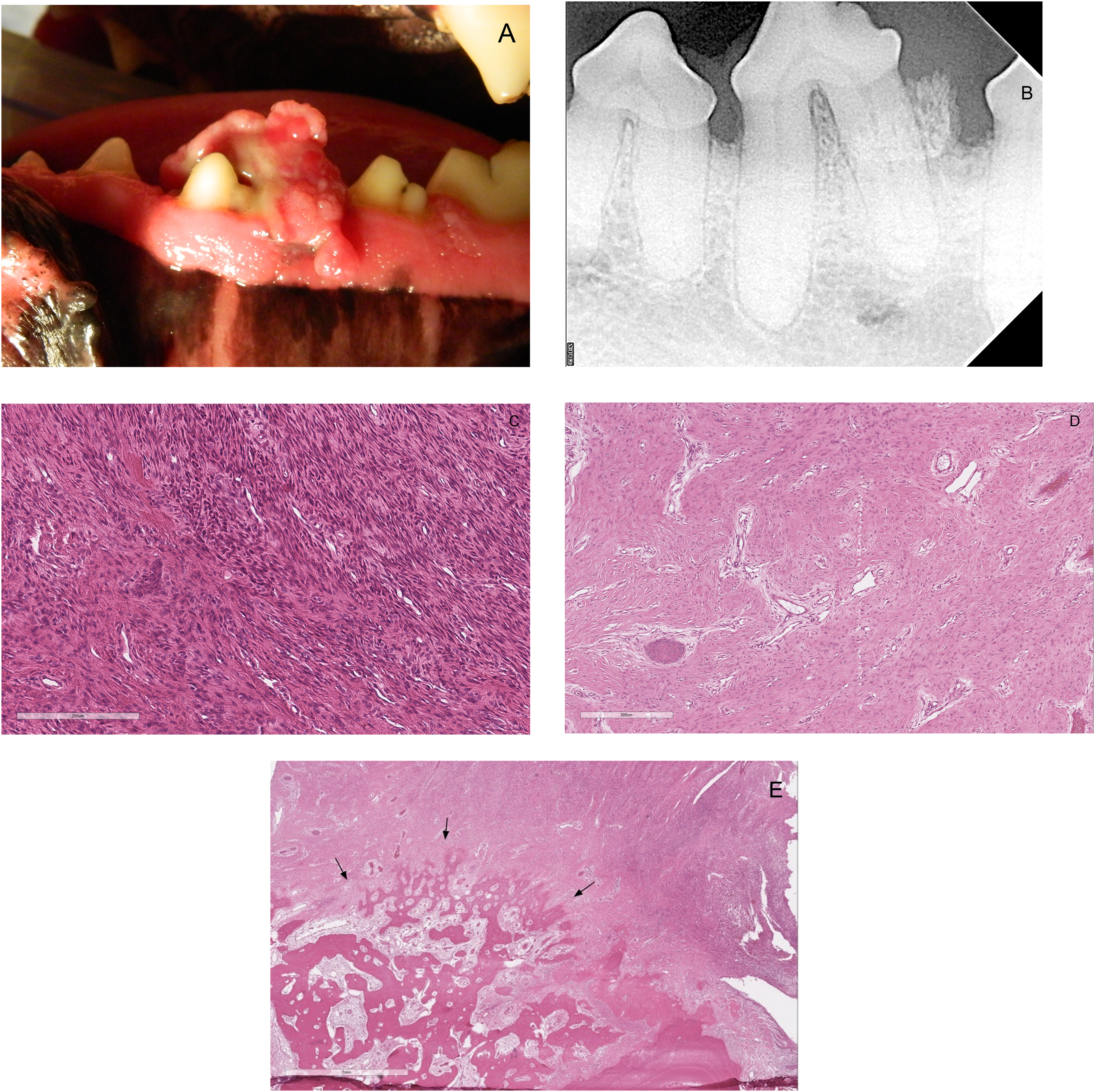
Case #14. (A) Photograph showing a pink, ulcerated, multilobulated, pedunculated HPOF located at the interdental space between the left mandibular third and fourth premolar teeth (307, 308), extending to the lingual aspect of 307. (B) Dental radiograph of the left mandible showed extrusion of 307 with osteoproduction around the coronal half of the distal root of 307. (C) Photomicrograph showing hypercellular region of the lesion with odontogenic epithelium (H&E, 20×). (D) Photomicrograph showing less cellular regions, reminiscent of a POF (H&E, 10×). (E) Photomicrograph showing the lesion abutting the alveolar bone with no evidence of deep invasion (arrows) (H&E, 2×). Abbreviations: HPOF, hypercellular peripheral odontogenic fibroma; POF, peripheral odontogenic fibroma; H&E, hematoxylin and eosin
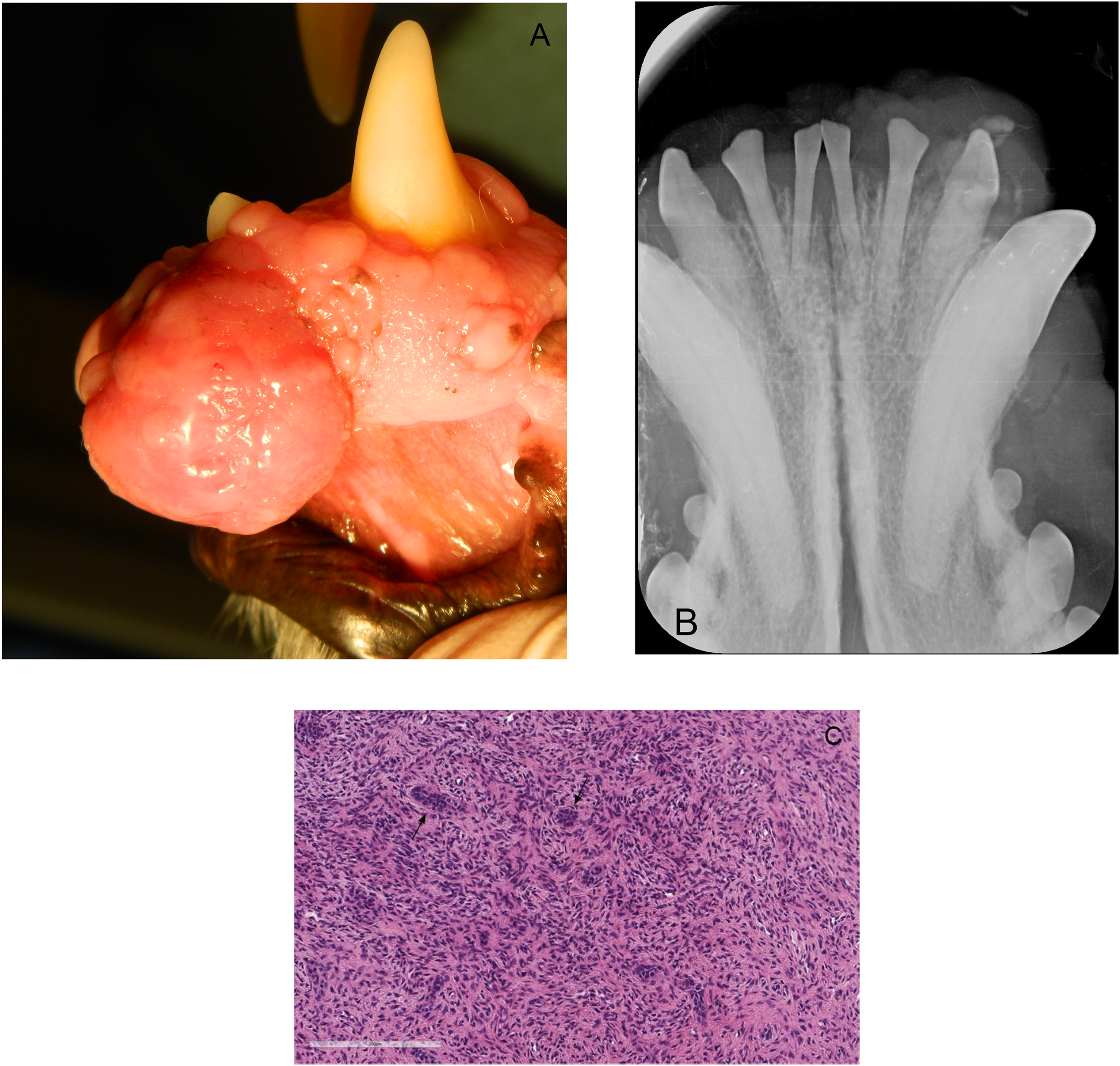
Case #6. Photograph showing a pink, semifirm, pedunculated, HPOF approximately 20 × 20 × 10 mm, located on the gingiva between the left mandibular second and third incisor teeth (302, 303). (B) Dental radiograph of the rostral mandible showed an osteoproliferative mass without obvious osteolysis of the alveolar bone or tooth displacement. (C) Photomicrograph showing hypercellular region with odontogenic epithelium (arrows) (H&E, 20×). Abbreviations: HPOF, hypercellular peripheral odontogenic fibroma; H&E, hematoxylin and eosin.
Summary of Radiographic Findings of 6 Dogs.
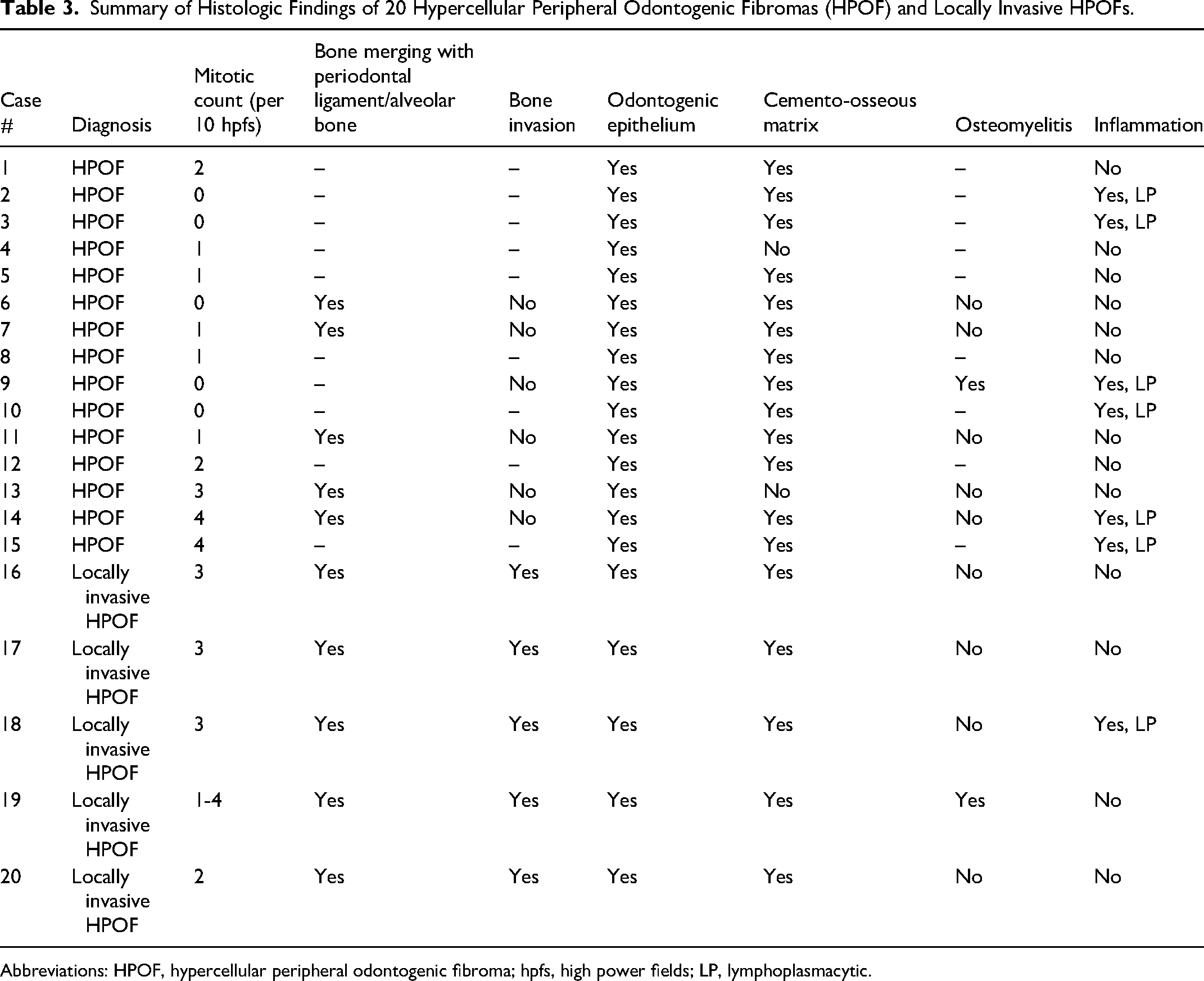
The histologic findings are reported in Table 3. All cases displayed hypercellularity of the fibroblastic component (Figures 1A-C, 2C, 3C, 4C, and 5C) and variable amounts of odontogenic epithelium. The odontogenic epithelium exhibited occasional squamous differentiation in some regions. Despite the hypercellularity of the fibroblastic component, nuclear pleomorphism was minimal. In some lesions, there were fewer cellular regions, reminiscent of a “classic” POF (Figure 4D). The mitotic count (10× high power fields) was variable, ranging from 0 to 4. In 10/20 dogs, the lesion extended to the periodontal ligament region and/or adjacent to the alveolar bone, at the region of gingival attachment to the tooth (Figure 3D). In 5/20 dogs, there was evidence of bone invasion merging with the alveolar bone and periodontal ligament region (Figure 6A-C), with some lesions causing osteolysis and/or tooth resorption. In total, 18/20 lesions contained variable amounts of cemento-osseous matrix, ranging from bright eosinophilic amorphous matrix to distinct regions of osseous metaplasia (Figures 1C, 6B and 6C). 2/20 cases had concurrent osteomyelitis, and 2/20 cases had few regional multinucleated giant cells near regions of ulceration. 7/20 cases had moderate lymphoplasmacytic inflammation multifocally within the fibroblastic proliferation (not bone).
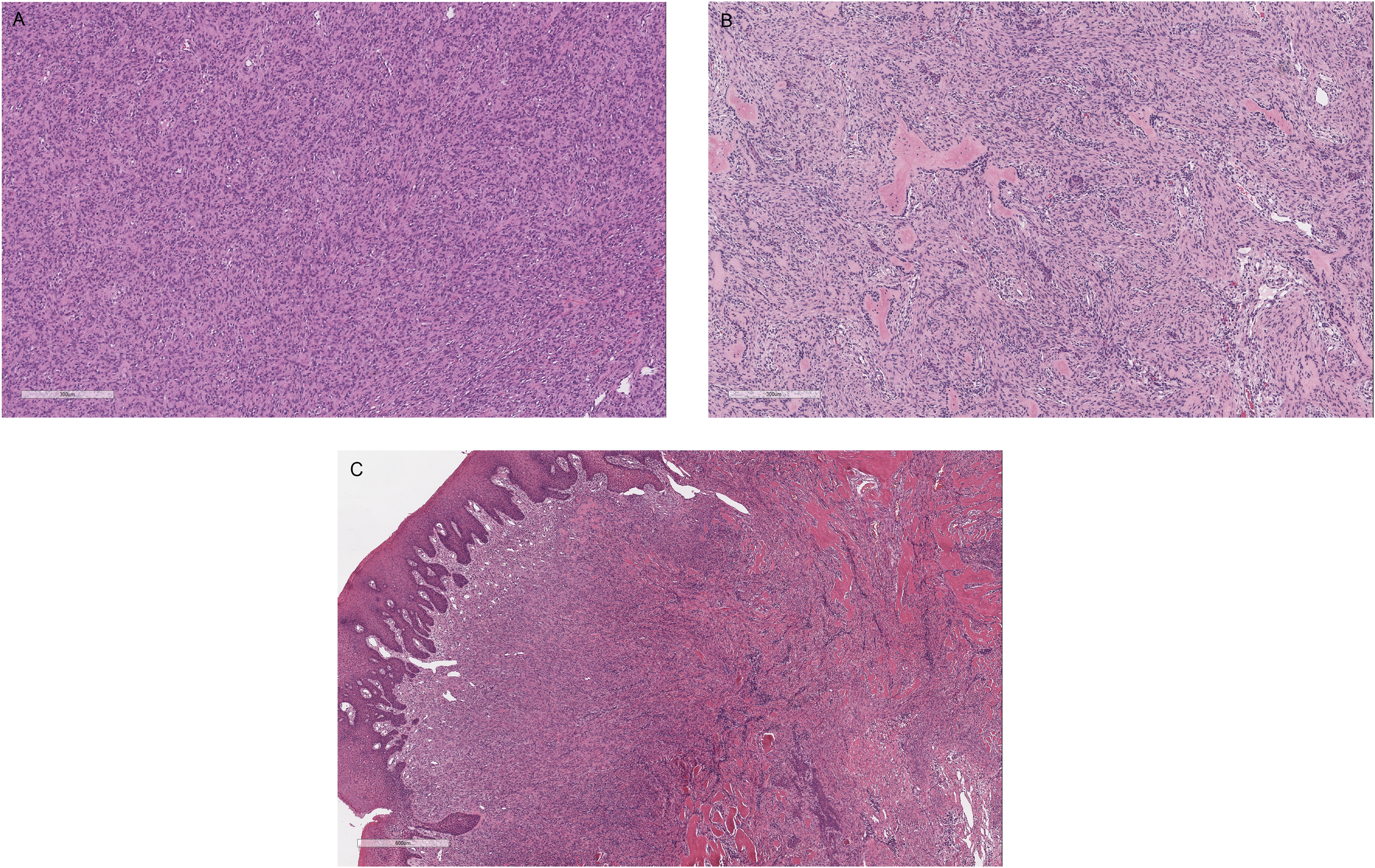
Photomicrographs of HPOFs. (A) Case #17 (H&E, 10×), (B) Case #11 (H&E, 10×) and (C) Case #8 (H&E, 4×). The lesions are subjectively hypercellular compared to most canine POFs. Abbreviations: HPOF, hypercellular peripheral odontogenic fibroma; POF, peripheral odontogenic fibroma; H&E, hematoxylin and eosin.
Case #7. (A) Photograph showing a round, irregular, pink HPOF located at the rostral left maxilla extending from the left maxillary first to third incisor teeth (201, 202, 203). (B) Dental radiograph of the left rostral maxilla showed displacement of the crowns of teeth 202 and 203, and osteoproduction within the mass at the distal aspect of 202. (C) Photomicrograph showing the hypercellular region with odontogenic epithelium (H&E, 20×). (D) Photomicrograph showing the lesion extends to the periodontal ligament region at the gingival attachment of the tooth (arrows) (H&E, 4×). Abbreviations: HPOF, hypercellular peripheral odontogenic fibroma; H&E, hematoxylin and eosin.
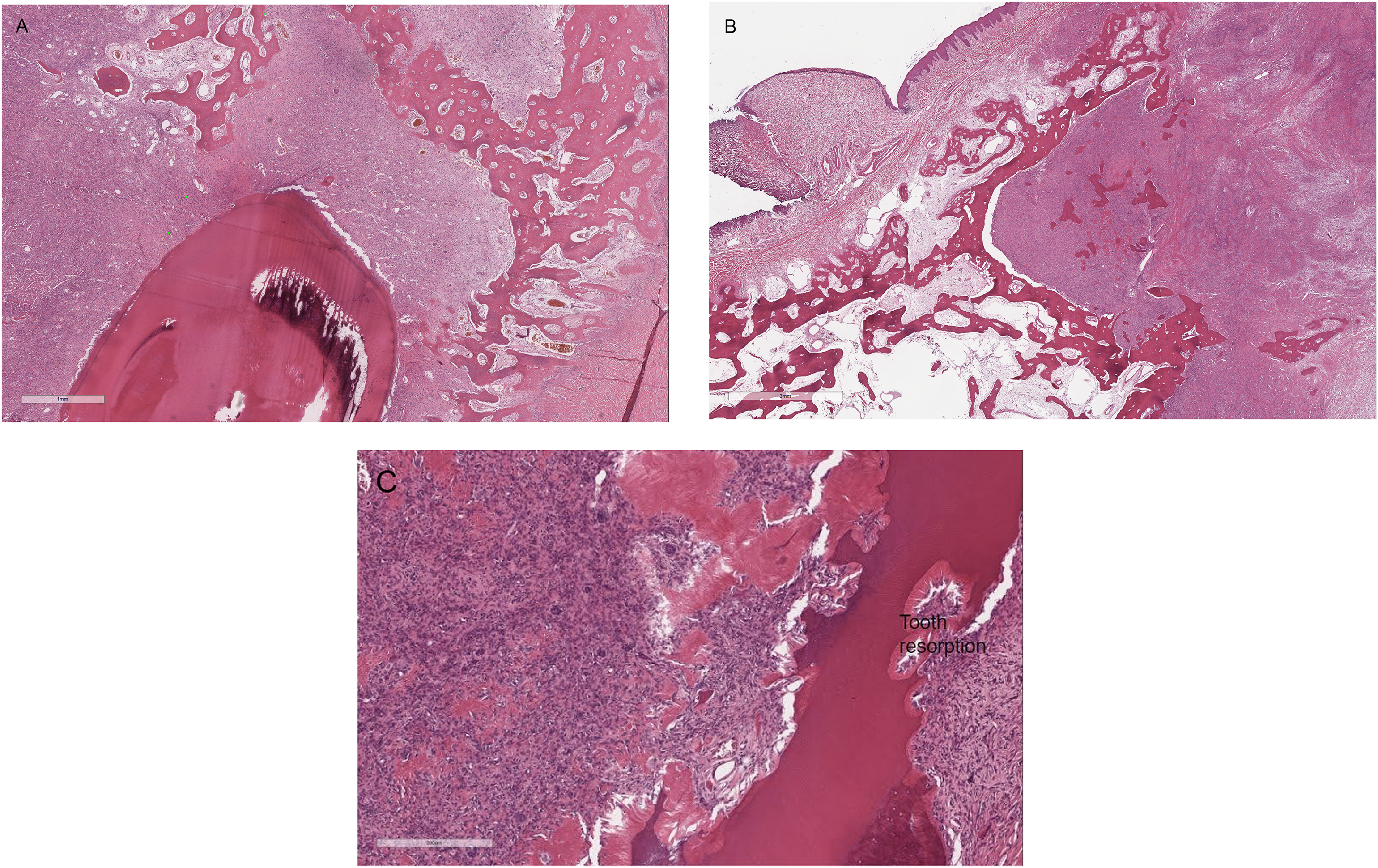
Photomicrographs showing bone invasion and lysis of the alveolar bone. (A) Case #17. (B) Case #18. (C) Case #20. Tooth resorption was also noted.
Summary of Histologic Findings of 20 Hypercellular Peripheral Odontogenic Fibromas (HPOF) and Locally Invasive HPOFs.
Abbreviations: HPOF, hypercellular peripheral odontogenic fibroma; hpfs, high power fields; LP, lymphoplasmacytic.
Discussion
POFs are benign, often amenable to debulking surgery although en bloc resection may be necessary in some cases that anchor in the region of gingival attachment to the tooth. In this series, we have described a HPOF, characterized by subjective increased cellularity of the fibroblast population (compared to most POFs) and variable mitotic activity. There is a lack of consensus on how to diagnose these lesions, and little is known about their behavior. The authors propose the terms noninvasive HPOF and locally invasive HPOF to describe these tumors.
In a retrospective study of 152 dogs with POF, the mean age was 8.5 years and the lesion ratio of maxilla to mandible was 1.7:1. 3 The mean age of dogs with HPOF (non-invasive and locally invasive) in this case series was 7.3 years and the lesion ratio of maxilla to mandible was 1.25:1.Radiographically, POF may have osseous metaplasia (osteoproduction within the mass) with lack of osteolysis, since the lesions are not invasive. 4 Radiographic information was not available for noninvasive variants of HPOF.
In this case series, dental radiographs of locally invasive HPOFs displayed osteolysis (2/6), displacement and/or extrusion of associated dentition (2/6), and osteoproduction/osteoproliferation within the mass (4/6). Histologically, POFs contain a fine fibrovascular stroma with stellate fibroblasts, and variable amounts of odontogenic epithelium and “hard” tissue (cemento-osseous matrix), with lack of pleomorphism and little to no mitotic activity. Histologically, HPOFs had mixed epithelial and mesenchymal components similar to POFs, however, they had hypercellularity of the fibroblastic component, and in some cases mitotic activity or rarely, evidence of local bone invasion. The amount of epithelium and cemento-osseous matrix varied between the lesions, similar to the variability seen in “classic” POFs. Of note, some lesions contained moderate superimposed lymphoplasmacytic inflammation, which can potentially contribute to a hypercellular phenotype.
The noninvasive HPOFs examined herein were amenable to local excision as they were “classic” less cellular, POFs, with rare instances of suspected local recurrence (1/16, case #9). Case #9 was a biopsy from the recurrence of the gingival mass; however, the original biopsy is not available to confirm the diagnosis of the original mass. Some lesions abut the alveolar bone and extend into the periodontal ligament region, without deeper invasive behavior, consistent with the idea that these lesions arise from tooth-bearing structures. In rare instances, invasion of the alveolar bone was present, suggesting potential for locally invasive behavior in rare cases. The locally invasive cases were similar histologically to the noninvasive HPOFs with a similar degree of hypercellularity and mitotic activity, therefore they could not be distinguished based on histopathology alone. Clinical behavior and imaging are required for differentiation. The level of hypercellularity and local bone invasion (not mere merging of the alveolar bone or extension into the periodontal ligament region) can be interpreted as locally invasive behavior akin to a low-grade spindle cell sarcoma, hence some terms used to describe the locally infiltrative lesions by pathologists in the past have ranged from low-grade sarcoma to odontogenic sarcoma, periodontal fibrosarcoma and peripheral odontogenic fibrosarcoma. However, a consensus on how to diagnose these tumors was not available. When the bone invasion is present, the authors propose the term locally invasive HPOF, which clearly denotes the behavior and avoids the controversy of the cell of origin and potential confusion with other soft tissue sarcomas that can arise on the gingiva.
While the high level of hypercellularity in some lesions may raise a concern for potential locally invasive behavior (only noted in a few cases herein), follow-up of the majority of lesions did not reveal recurrence after incomplete excision (debulking). When invasive behavior was noted (5/20), there was no evidence of recurrence after complete excision. Therefore, hypercellularity should not be used as a sole criterion to classify these lesions as invasive. It is the pathologist's responsibility to comment on the hypercellularity and the need for clinical differentiation given the varied behavior. While HPOF lesions could have a degree of hypercellularity resembling the hypercellularity seen in other types of sarcomas in the oral cavity and other anatomic sites, the behavior of the majority of lesions is not invasive except for a small subset. Given that these hypercellular lesions contain similar elements to POFs (odontogenic epithelium, mesenchymal proliferation, and often cemento-osseous matrix), the authors suspect these lesions are a variant of the more common noninvasive POF, although advanced diagnostic tools to support this hypothesis are not yet available. Importantly, lesions without odontogenic epithelium or only scant odontogenic epithelial cells were excluded from the study, to avoid misclassification of soft tissue sarcomas arising from other fibroblasts in the region and overinterpretation of potentially hyperplastic epithelium in the vicinity of an affected periodontal ligament, respectively.
It is important to note that all atypical HPOFs should not be classified as locally invasive HPOF lesions automatically since there is a continuum of lesions histologically and the majority of hypercellular lesions are not invasive and therefore do not require more aggressive treatment. However, in cases of recurrence or clinical suspicion of bone involvement, imaging is recommended to assess possible bone involvement which could alter the treatment plan. In some cases, however, it is important to note that radiographic evidence of bone involvement may be reflective of concurrent periodontal disease, or osteomyelitis, instead of true bone invasion by the lesion, therefore clinical discretion is advised. In cases where the pathologist is uncertain about the potential for local invasion, monitoring of the surgical site for recurrence and/or imaging for evidence of bone involvement may be prudent since histologic differentiation is difficult.
A diagnosis of hypercellular noninvasive and locally invasive POF in dogs is uncommon, not only given the rarity of the neoplasm, but also potentially because the accurate histological distinction between noninvasive and locally invasive mesenchymal lesions in the oral cavity of dogs can be problematic (eg, histologically low-grade, biologically high-grade fibrosarcoma of dogs). 5 Furthermore, there seems to be a lack of consensus among human medical pathologists when determining the malignancy criteria for odontogenic tumors 6 which likely extends to veterinary pathology. Over the years, as our diagnostic capabilities improve with the advancement in imaging, microscopic and molecular technology, many lesions have been stratified into more specific categories, which in turn has improved the specificity of therapeutic approaches and prognostic evaluations. 7
Differential diagnoses for locally invasive HPOF include ameloblastic fibroma, fibrosarcomas arising from other fibroblasts in the gingiva/tooth-bearing regions, and low-grade well-differentiated osteosarcoma. Ameloblastic fibromas also have a mixed epithelial and spindle cell component, however, they have a more prominent or dominant odontogenic epithelium component than the one seen in HPOFs, with plexiform, anastomosing trabeculae of odontogenic epithelium. Instead, locally invasive HPOFs have isolated islands or thinner anastomosing strands of odontogenic epithelium similar to the “classic” POF. Differentiating locally invasive HPOF from low-grade well-differentiated osteosarcoma may be difficult in lesions with abundant cemento-osseous matrix, however the presence of odontogenic epithelium is of paramount importance. Caution is also advised to avoid interpreting trabeculae of hyperplastic surface mucosal epithelium or isolated islands of hyperplastic odontogenic epithelium in the periodontal ligament region as evidence of lesional odontogenic epithelium.
Due to the periodic reclassification of nomenclature in the scientific community, the nomenclature involving POF has been evolving and is still controversial. In veterinary medicine, POF was also reclassified in the 1980s, and fibromatous and ossifying epulides were placed together, as FEPLO. 8 POF is the preferred term for some in veterinary medicine currently, since it is more specific than the term epulis, however other veterinarians still prefer the term FEPLO. POF is rather commonly diagnosed in dogs; in one published retrospective study of 280 oral biopsies in dogs, 21% of the samples were diagnosed with 9 while in another published retrospective study of 152 dog, 31% of the dogs had POF. 3
Radiographic osteolysis, poorly defined margins of the lesion, and external inflammatory root resorption are some of the indications of aggressive or neoplastic bone lesions.10–15 When an incisional biopsy result is unavailable prior to the definitive surgery, preoperative dental radiographs may be helpful to suggest an aggressive lesion and to guide treatment decisions. However, it is important to note that radiographic evidence of bone lesions may be reflective of concurrent periodontal disease, osteomyelitis, and other reactive changes in the alveolar bone, instead of true bone invasion by the lesion, therefore clinical discretion is advised.
In addition, many cases of noninvasive HPOFs had to be excluded from the study because of lack of follow-up, which may give the impression that locally invasive lesions are common (5/20); however, many more noninvasive HPOFs are likely to exist than invasive variant. Osteolysis of alveolar bone, displaced or extruded dentition, and/or osteoproduction/proliferation were seen in 6 cases that had dental radiographs available. One patient whose CT images were also available to review showed lack of bony changes.
A limitation of the study is the lack of imaging data for the majority of cases, given that debulking surgery was performed without imaging. The cases in this study are dogs treated at a private dentistry and oral surgery referral practice as well as cases seen by regional referring veterinarians. Thus, only a subset of cases (6/20) have dental radiographic and/or advanced imaging images available for review, while the remaining cases from regional veterinary practices lack dental radiographs. The authors acknowledge that a major limitation of this study is therefore the lack of dental and/or advanced imaging of two-thirds of the histopathologic cases. Correlation of radiographic and histopathologic changes is important for the understanding of these oral tumors and further study is recommended.
The goal of this case series is to aid in the correct diagnosis and timely, appropriate treatment of HPOFs and locally invasive variants. Features of POFs that should raise concern for pathologists include hypercellularity, mitotic activity, and local invasiveness, and should prompt a cautionary comment and diagnosis of HPOF. Histopathology alone cannot differentiate between noninvasive and locally invasive HPOFs and assimilation of clinical and imaging information is very important for these hypercellular oral lesions. In this study, dogs responded favorably to local excision (debulking) of the majority of HPOFs and complete resection was curative for locally invasive lesions. It is unclear if merging of the lesion with alveolar bone or extension into the periodontal ligament region could potentially lead to local recurrence, therefore monitoring may suffice in the absence of definite local bone invasion. Excisional biopsy or marginal resection of suspected HPOF is an adequate treatment option, depending on clinical and imaging findings. Complete resection may be pursued if the lesion recurs, based on imaging results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Material
Antech Diagnostics, Irvine, California.