
Abstract
Canine acanthomatous ameloblastoma (CAA) has been reported to be the most prevalent odontogenic tumor in dogs. The most common location of this tumor is the rostral mandible. Symphyseal-sparing mandibulectomy has been shown to be an effective technique to maintain mandibular continuity and promote early return to function. In this retrospective study, 35 dogs with CAA associated with a mandibular canine tooth were evaluated following a symphyseal-sparing rostral mandibulectomy. Dogs with intraoperative transection of the canine tooth root and subsequent root fragment extraction were included. The objective of this study was to evaluate outcome following excision of CAA with mid-root transection. Data retrospectively evaluated in this study included the following: narrowest tumor margin, narrowest tumor margin at the border associated with the transected canine root, tumor size, and prevalence of local recurrence. This study showed that 82.86% of CAA were completely excised with tumor-free margins (N = 29). The median narrowest overall tumor-free margin was 3.5 mm (interquartile range [IQR] 2.0-6.5 mm) and the median tumor-free margin associated with the border of the transected canine root was 5.0 mm (IQR 3.1-7.0 mm). Follow-up data was obtained in 25 cases via phone interviews with referring veterinarians and clients. No local tumor recurrence was reported in cases with incomplete tumor excision (N = 5). All dogs with follow-up data survived at least 1 year following surgery. It was concluded that segmental or rostral mandibulectomy with wide margins to include the entire mandibular canine tooth with subsequent mandibular instability may not be warranted for dogs with CAA associated with this tooth.
Keywords
Introduction
Canine acanthomatous ameloblastoma (CAA) has been reported to be the most common tumor of odontogenic origin in dogs. CAA account for as many as 45% of all odontogenic tumors in dogs. 1 CAA is classified as a tumor of odontogenic epithelium without odontogenic mesenchyme that is distinguishable from conventional ameloblastoma in biological behavior and histological pattern.2–4 It is believed that CAA arises from the remnants of odontogenic epithelium in the gingiva, although they have been reported to arise intraosseously as well.3,5,6 CAA is known to cause destruction of the underlying bone. 7 The aggressiveness and invasiveness of CAA into the associated jaw bone has been found to be highly variable while at the same time it is histopathologically highly uniform. 6
The most common location of CAA is the rostral mandible with 41.0% to 51.2% reported to be at this location.1,7,8 It is generally considered to be a benign locally invasive neoplasm that does not metastasize.5,7 The typical treatment of choice for CAA of the rostral mandible includes wide surgical excision with at least a 1 cm gross margin of normal tissue. 5 Other modalities for treatment include radiation therapy and intralesional bleomycin. 9
The goal of wide surgical excision is to achieve histopathologically tumor-free margins. Previous studies have reported local recurrence of CAA as high as 91% if only simple marginal excision (without bone/tooth removal) is performed. This supports having a goal of tumor-free margins during the surgical planning process.10,11 Multiple studies have shown that wide surgical excision of CAA with 1-2 cm margin of normal tissues results in low risk of local recurrence (0%-4.6%).10–14 A recent article found no local recurrence of CAA tumors even with tumor-free margins as low as 1 mm or less indicating that even narrow tumor-negative margins may be successful in preventing local recurrence. 8
Typically, unilateral or bilateral rostral mandibulectomy is performed to excise CAA of the rostral mandible. Rostral mandibulectomies can result in excision of the mandibular symphysis resulting in mandibular drift and traumatic occlusion causing palatal trauma.11,12,15 Crown reduction and vital pulp therapy may be recommended for the contralateral mandibular canine tooth if present to avoid painful malocclusion and associated palatal trauma. 14 Other treatments for mandibular drift that have been previously described include elastic training, mandibular fixation, and mandibular reconstruction techniques. 16 The goal of this study was to report the results of a curative intent surgical procedure to completely excise CAA associated with the mandibular canine tooth while maintaining the integrity and stability of the remaining rostral mandibles.
Materials and Methods
Cases were identified by searching medical records at the Center for Veterinary Dentistry and Oral Surgery, Gaithersburg, MD for dogs diagnosed with CAA that received a rostral mandibulectomy between 2007 and 2020.
Medical records were then reviewed to select cases where CAA was associated with either the left (304) or right (404) mandibular canine tooth (Figure 1A and B). Histopathology reports for each case were reviewed to confirm a CAA diagnosis. Intraoperative photographs, dental radiographs, and surgery reports for each case were reviewed to determine if a portion of the mandibular symphysis remained intact postmandibulectomy (Figure 2). Photographs and dental radiographs were also reviewed to determine if the root of 304 or 404 was transected during the initial mandibulectomy followed by extraction of the remaining root fragment (Figure 3A and D). The operating veterinarians elected to use this symphyseal-sparing surgery technique in cases where it was possible to maintain symphyseal stability and obtain at least 0.5 cm gross surgical margins in cases with no bone involvement. In cases with bone involvement on dental radiographs at least 1 cm gross surgical margins were obtained. Planned gross surgical margins ranged from 0.5 to 2.0 cm based on this treatment algorithm and surgeon preference. Thirty-five cases met the inclusion criteria for this study.
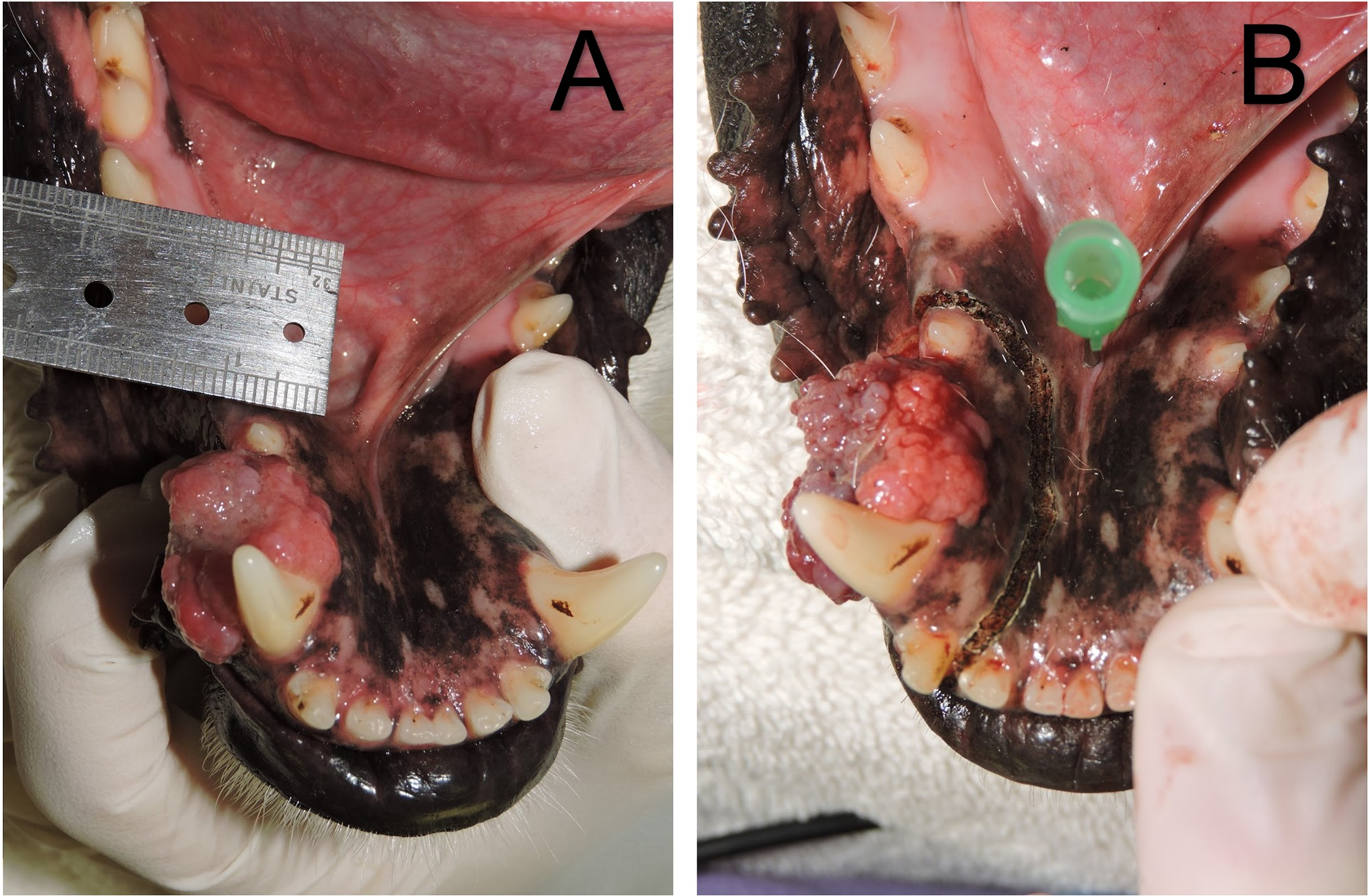
(A) A canine acanthomatous ameloblastoma associated with the right mandibular canine tooth (404). (B) An example of incision for surgery where an 18-gauge needle is marking the caudal aspect of mandibular symphysis.

Radiograph showing minimal but intact caudal mandibular symphysis after mandibulectomy for a canine acanthomatous ameloblastoma tumor.
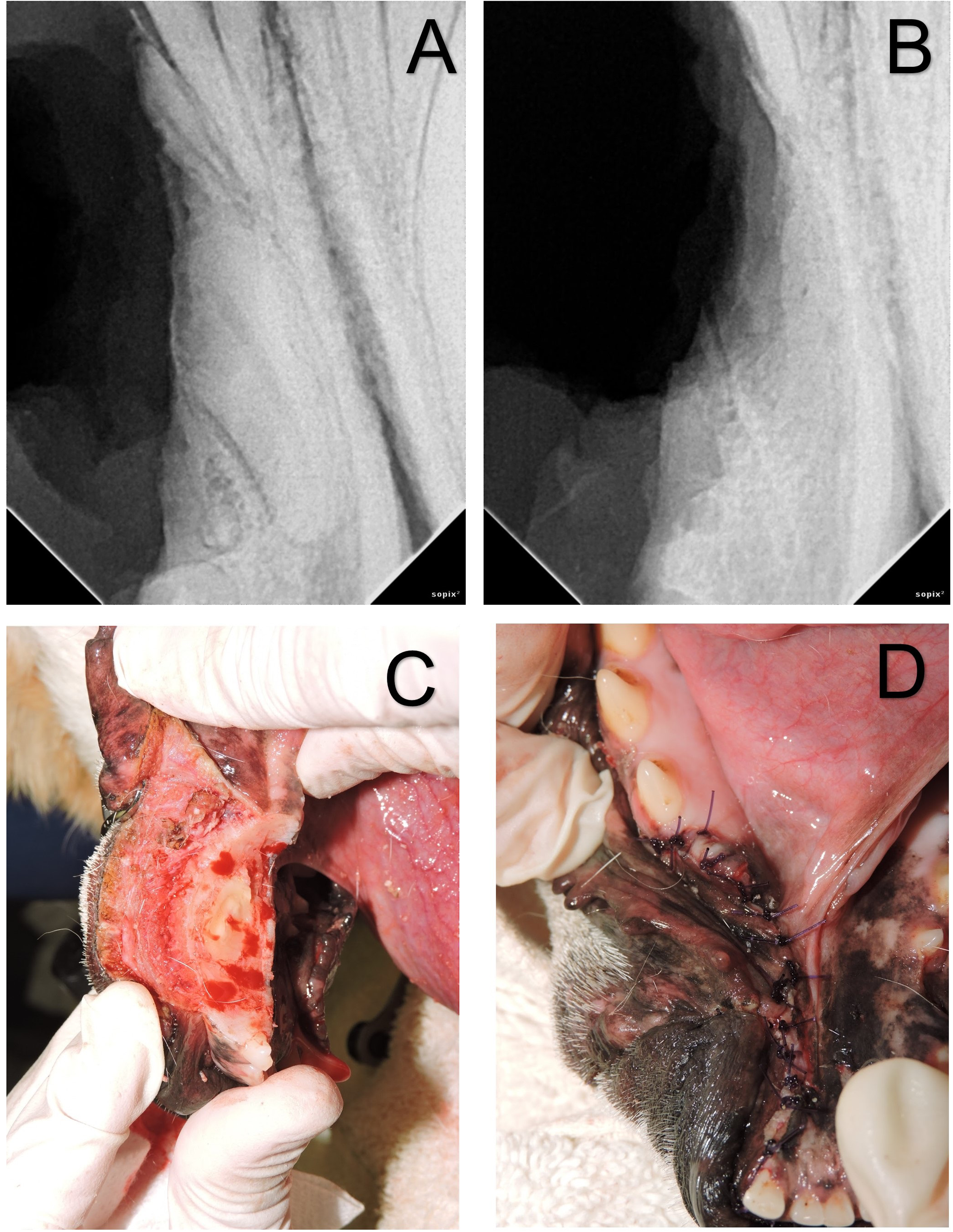
(A) Radiograph showing transected roots of right mandibular third incisor, canine, and first premolar teeth (403, 404, and 405) postmandibulectomy. (B) Radiograph showing complete extraction of transected roots. (C) Picture of remaining 404 root after mandibulectomy. (D) Final closure after mandibulectomy and root extractions.
Data collected for analysis from medical records and pathology reports included tumor location, tumor size based on largest gross tumor dimension, presence of preoperative CAA biopsy result, presence of tumor associated mandibular bone involvement, age of patient at the time of surgery, patient breed, weight, and sex. All mandibulectomy samples were evaluated by a board-certified veterinary pathologist and archived reports for each tumor were reviewed. The narrowest tumor-negative margin was recorded and analyzed in reports where this information was available. Based on recent research showing no local recurrence even with narrow margins, tumor-negative margins were defined as any sample where the tumor cells did not extend to the margin of the specimen. 8 In pathology reports where tumor-negative margin lengths were not specifically noted, a sample was considered to have tumor-negative margins if the pathologist indicated that the tumor was completely excised or indicated that tumor-free margins were present. Of particular interest was any notation addressing whether tumor cells were present at the sectioned root of 304 or 404. The narrowest caudal, ventral, or distal tumor-free margin was recorded where available and analyzed to evaluate tumor-negative margin status at the site of the sectioned mandibular canine. Follow-up data was collected through telephone interviews with the referring veterinarians and owners. Local tumor recurrence, whether or not the patient was currently alive or deceased, and cause of death were recorded. Age, weight, and breed were summarized using mean (standard deviation [SD]), median (interquartile range [IQR]), and N, respectively. Narrowest tumor-negative margins and tumor size via the largest recorded dimension of the tumor were evaluated using median IQR and mean SD, respectively. Whether or not the mandibulectomy procedure resulted in tumor-negative margins, presence of preoperative CAA biopsy result, presence of tumor associated bone involvement, tumor location, and local tumor recurrence were evaluated by N (%). All dogs had a 2-week postoperative oral examination at our facility to assess wound healing.
Results
The average age of patients in the 35 cases reported here was 9.53 years (SD ± 2.46). The median weight of all cases was 29.7 kg (IQR 22.05-35.55). The distribution of patient sex in this study was 51.43% neutered males (N = 18), 42.86% neutered females (N = 15), 2.86% intact males (N = 1), and 2.86% intact females (N = 1). There was a wide distribution of breeds in this study. The most common breeds represented were mixed-breed dogs (N = 7), Labrador Retrievers (N = 4), and Golden Retrievers (N = 3). Other less common breeds included American Foxhound, Australian Shepherd, Beagle, Border Collie, Boxer, Chesapeake Bay Retriever, Cockapoo, Dalmatian, English Bulldog, German Shepherd, Jack Russell Terrier, Malamute, Pit Bull, Shetland Sheepdog, Shih Tzu, and Weimaraner (N = 1-2).
Evaluation of tumor data showed that 16 of the tumors were located at 304 (45.7%) and 19 were located at 404 (54.3%). After mandibulectomy, 29 of 35 samples (82.86%) were found to have tumor-negative margins. All tumor-positive margins were located at the apical aspect. The histopathology report in 6 cases indicated tumor-negative margins without documenting margin width. Of the cases with quantified tumor-negative margins, the median narrowest margin was 3.5 mm (IQR 2.0-6.5 mm). The median narrowest caudal, ventral, or distal tumor-negative margin was 5.0 mm (IQR 3.1-7.0 mm). The gross tumor dimensions were noted in the medical record for 26 of 35 cases. The average measured largest tumor dimension of these cases was 2.07 cm (SD ± 0.65) and 65.38% of these cases had a tumor dimension ≥2 cm. Five cases had a history of previous marginal excision for CAA by the referring veterinarian and were presented to the Center for Veterinary Dentistry and Oral Surgery for definitive surgery. Incisional biopsy results suggestive of CAA were available preoperatively in 16 cases (45.71%). One additional case had a fine-needle aspirate (FNA) performed on the mass prior to referral that was also indicative of CAA, while another case had a biopsy report from 10 months previously that indicated gingival hyperplasia at the current tumor site. Surgery reports noted bone involvement associated with the tumor on intraoperative dental radiographs in 31 of 35 cases (88.57%). Bone involvement was noted in the surgery report in 4 of the 6 cases with tumor-positive margins and 27 of 29 cases with tumor-negative margins. Excisional biopsy using the symphyseal-sparing mandibulectomy technique as described 15 was done in the remaining 17 dogs with no previous biopsy or FNA.
All dogs showed no complications and had wound healing 2 weeks postoperatively. There was no trauma evident from the ipsilateral maxillary canine tooth contacting the peri-surgery area. Follow-up data was obtained in 71% (25 of 35) of the dogs in this study. The 1-year survival rate in these dogs was found to be 100% for the 25 dogs with follow-up data. Seven of these dogs were still alive at the time of data collection. The cause of death was obtained for 13 of the 18 deceased dogs and euthanasia was unrelated to CAA in all of these cases. Euthanasia dates or confirmation of alive status at the time of data collection were confirmed in 23 of 25 dogs. Median follow-up time for these 23 cases was 940 days with a range of 424 to 2282 days. No local recurrence or peri-surgery area trauma was reported by the referring veterinarian based on oral examination at any time during the follow-up period. Follow-up data was obtained for 5 of the 6 dogs with a tumor-positive margin and no tumor recurrence occurred in any of these cases a minimum of 1-year postoperatively based on oral examination by the referring veterinarian.
Discussion
In this study, patients with CAA with tumors of the rostral mandible specifically associated with the mandibular canines were evaluated following symphyseal-sparing rostral mandibulectomy. Similar to previous studies, a majority of the cases were adult to geriatric, medium to large breed dogs. 1 There was no sex predilection in this study. Due to the number of breeds included in this study, the study population was too small to determine if any breed disposition were present. Mixed-breed dogs, Golden Retrievers, and Labrador Retrievers were the most common breeds represented but this is likely due to the common prevalence of these breeds in the general dog population. However, there are other studies that have found significant breed predilection for CAA in Golden Retrievers.1,8
In this study 82.86% of cases had tumor-free margins of at least 0.5 mm after symphyseal-sparing mandibulectomy was performed. Conventionally gross margins of 1-2 cm and excision of the entire periodontium of the affected tooth has been the treatment of choice for CAA.17,18 This surgical recommendation would make it difficult or impossible to spare the mandibular symphysis in cases of 304 of 404 involvement leading to instability of the rostral mandibles and mandibular drift as a potential postoperative complication involving palatal trauma or causing difficulty in prehending food.12,13,15 This study indicates that even with transection of 304 or 404 during mandibulectomy complete excision of a CAA associated with a mandibular canine is achievable in cases where suspected tumor margins are not in close proximity to the apex. It is also important to consider that after mandibulectomy and canine root fragment extraction, most veterinary dentists and veterinary surgeons perform osteoplasty prior to closure which may extend the tumor-negative margin and not be subject to evaluation.
Traditionally, it is recommended to avoid transection through the alveoli of teeth during a mandibulectomy to excise an oral tumor due to concerns that tumor cells may infiltrate apically along the periodontal ligament.17,18 In this study only procedures where the canine tooth root was transected during mandibulectomy were included to evaluate how transection through the alveolus might affect tumor-negative margins and local recurrence rates. This study showed no evidence of local tumor recurrence in cases with follow-up data using this rostral mandibulectomy technique. This supports the possibility that CAA does not consistently migrate extensively along the periodontal ligament and that avoiding transection of tooth roots during excision of CAA may not always be warranted especially when considering the potential complications associated with instability of the rostral mandibles. In cases where there is a preoperative diagnosis of CAA and it is possible to obtain 1 cm gross margins around the tumor, avoidance of alveolus transection may not be as critical as previously thought in order to obtain positive surgical outcomes.
Lack of recurrence in cases with incomplete tumor excision may have been related to changes in the microenvironment, stimulation of the immune response to scavenge tumor cells during the wound healing process, alveolar bone removal associated with extraction of the canine tooth root fragment, and osteoplasty of alveolar cortical bone postexcision. These latter procedures may explain the lack of recurrence in cases with tumor-positive margins since remaining periodontal ligament and alveoloplasty/osteoplasty associated with extraction of the remaining root fragment would likely extend the excised margin beyond the ≤ 1 mm width that has been shown to be minimally required to positively prognosticate no recurrence. 8 All mucosal incisions in this study were made with either monopolar electrosurgery or CO2 laser. These surgical techniques have been shown to cause thermal damage in tissues at surgical margins which can alter histopathological margins. 19 This could be another explanation for lack of recurrence in cases with tumor-positive margins.
A previous study evaluated CAA tumor recurrence after dorsal marginal mandibulectomy. In this previous study, no local tumor recurrence occurred in any of the cases however, tumor margins were not evaluated and only tumors < 2 cm at the largest dimension were included for evaluation. 13 In the study reported here, 65.38% of the 26 cases where tumor dimensions were recorded had a tumor dimension ≥2 cm. This result indicates that even in cases with a larger tumor size, a more conservative mandibulectomy can achieve tumor-negative margins and have a positive long-term outcome for the patient. It is also important to note that tumor recurrence data in both this study and the previous study on CAA tumor recurrence was obtained via follow-up interviews with clients and referring veterinarians. 13 Unfortunately, this data only determines if there was obvious gross recurrence of CAA in these patients during the follow-up period for each case. Dogs reported in this study could have had subclinical, microscopic tumors present. Future studies using follow-up radiographs or cone beam computer tomography (CT) to determine existence of subclinical tumor recurrence would be needed to evaluate the recurrence rate more accurately in cases where CAA has been excised assuming these modalities are sensitive enough to provide such information in an area which has had previous surgery. A re-entry procedure and bone biopsy would undoubtedly be the most reliable method to determine subclinical local recurrence, but this is not practical or necessarily advisable based on the results of this study. Currently not enough high-level evidence exists to determine the recurrence rate for CAA and to establish what the gross margin should be for a curative intent surgery.
Excisional biopsy is routinely performed in humans with oral and maxillofacial lesions and has also been performed in dogs and cats.20–33 The principal differential diagnoses for the dogs of this study with CAA included squamous cell carcinoma (SCC) and peripheral odontogenic fibroma (POF). For patients without a preoperative histopathology report and without exact knowledge of the tumor type, clients were counseled on excisional and incisional biopsy procedures. Incisional biopsy is never contraindicated and is generally quite dependable although there is mild controversy regarding appropriate technique and accuracy.34–37 Generally, pathologists agree that greater sample volume generates a more accurate diagnosis. 38 The technique performed here was presented to clients as a method for excisional biopsy to confidently obtain a high volume of tumor for a histopathological diagnosis and to potentially be a curative procedure for CAA, POF, and even SCC depending on lesion size. The morbidity from the procedure was presented as being similar to a sequential multitooth extraction procedure since it would include the canine, ipsilateral first and second premolar, and a variable number of incisor teeth. The procedure described here removed bone and teeth en bloc compared to removing bone with a drill and bur while extracting teeth using periodontal elevators/luxators and extraction forceps. Therefore, symphyseal-sparing mandibulectomy was not considered to be a radical, potentially debilitating technique that should only be undertaken with the information gained by an incisional biopsy procedure. Clients were informed that if the tumor were incompletely excised based on histopathological analysis, a second revisional procedure could be done to excise remnant tumor cells. Overall, clients were presented with a cost-effective clinical scenario that had a relatively high incidence of success defined by tumor excision with negative margins and acceptable morbidity, similar to a sequential, multitooth extraction procedure.
Symphyseal-sparing mandibulectomy can obtain adequate tumor-negative margins for CAA associated with mandibular canine teeth. The results of this study support those of a previous study that indicated that even with a very narrow tumor-negative margin width, cases can have a positive postsurgical prognosis. 8 Limitations of this study include the small sample size, retrospective nature of the study, different pathologists reviewing samples, and interview-type follow-up data. It is concluded that segmental or rostral mandibulectomy with wide 2 cm margins that include the entire mandibular canine tooth may not be warranted, but rather it is more beneficial to maintain stability of the mandibles using the symphyseal-sparing technique for dogs with CAA associated with a mandibular canine tooth.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.