
Abstract
Objective
This study evaluated the effectiveness of a novel multidimensional group intervention aimed at enhancing subjective cognitive and psychosocial functioning in community-dwelling older adults.
Methods
Sixty cognitively healthy adults aged 65–75 were randomly assigned to an experimental or control group. The 10-week intervention integrated five components: memory compensation, problem solving, emotion regulation, mindfulness, and locus of control. Validated self-report measures were collected at pre-test, post-test, and 12-week follow-up.
Results
Mixed repeated measures MANOVA and ANOVA revealed significant improvements in the experimental group across all targeted domains compared to the control group (p < .001). Gains were sustained at follow-up.
Discussion
This structured, skills-based program significantly enhanced perceived cognitive and emotional functioning in healthy older adults. Its emphasis on real-life application and personal agency supports its use in community-based aging interventions. Trial Registration: Neuroage Study (NCT01481246).
Keywords
Introduction
Contemporary perspectives on aging have shifted from a focus on “how to live longer” to an emphasis on “how to age well.” The importance of timely psychosocial and cognitive interventions to reduce disability in aging is widely acknowledged (Reynolds et al., 2022; WHO, 2015). A growing body of literature supports a biopsychosocial approach in promoting successful, active, and healthy cognitive aging. Central to these models is the preservation of functional capacity, particularly through cognitive and psychosocial well-being (Mendoza-Ruvalcaba & Arias-Merino, 2015; Estebari et al., 2014).
This study examines the efficacy of a novel multidimensional group intervention designed to enhance cognitive and psychosocial functioning in community-dwelling older adults aged 65–75. A previous publication (Chadjikyprianou & Constantinidou, 2023) described the intervention’s theoretical foundations, structure, and instructional methods, along with data on its feasibility and acceptability. Over 90% of participants reported satisfaction with skill acquisition, while 60–90% reported continued use of strategies at follow-up, along with positive lifestyle changes (e.g., diet and exercise).
Key Components of the Multidimensional Group Intervention
Τhe current intervention stands out for its structured integration of five interconnected components targeting age-related challenges—memory compensation, problem solving, emotion regulation, mindfulness, and locus of control—delivered through a cohesive, skills-based curriculum. Τhis approach offers a novel synthesis grounded in cognitive rehabilitation and clinical psychology. Importantly, the instructional design emphasizes active skill-building, contextual integration, and functional application, moving beyond purely educational formats. By linking cognition and emotion, the program aims to improve daily functioning through structured, contextualized skill-building.
Each session followed a progression from direct instruction (e.g., psychoeducation) to interactive methods (e.g., role-play and group discussion) and indirect learning (e.g., case studies and reflective practice), concluding with independent application through structured homework (as described in detail in our previous publication; Chadjikyprianou & Constantinidou, 2023). These instructional layers were designed to reinforce each other across cognitive and emotional domains. This hands-on, cumulative model offered a scaffolded approach with each week building upon prior sessions, increasing complexity and fostering sustained integration of skills supporting the translation of abstract strategies into meaningful, functional behaviors. The following sections provide an overview of the five core components of the program. Figure 1 summarizes their integration across the intervention structure. Active Components of the Intervention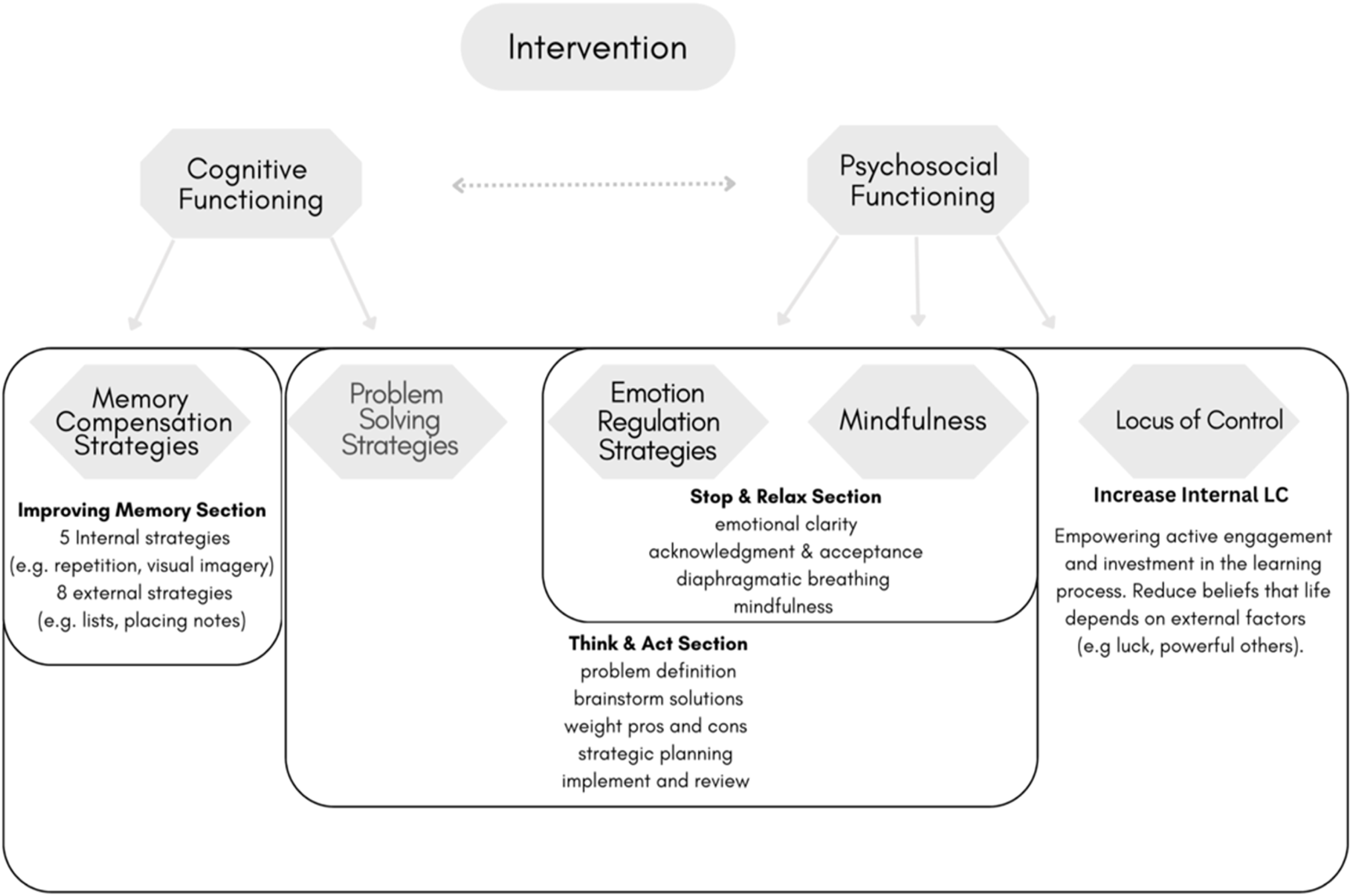
Cognitive Functioning
The present intervention targeted key areas of cognitive functioning often impacted by aging, with the goal of promoting adaptive self-regulatory strategies in everyday life. Memory and problem solving have been identified as key domains where older adults frequently report difficulties, even in the absence of objective cognitive decline (Chadjikyprianou et al., 2021; Drigas & Karyotaki, 2019).
Memory Compensation Strategies (MCS) were integrated as a key cognitive approach to teach participants methods for improving information encoding (Kinsella et al., 2016). Training included both internal strategies (e.g., visualization and mental rehearsal) and external supports (e.g., note-taking and lists), adapted from cognitive rehabilitation and educational psychology frameworks (Cicerone et al., 2019; Kinsella et al., 2016; Oxford, 1990). Emphasis was placed on applying strategies in meaningful, real-life situations to enhance participants’ sense of control and confidence in memory tasks.
Everyday problem solving was addressed through a five-step model presented in the “Think & Act” component. The intervention aimed to strengthen participants’ ability to approach real-life challenges using structured reasoning, planning, and decision-making. Problem solving was approached as a key element of executive functioning and was conceptually linked with emotion regulation, described in the following section.
Psychosocial Functioning
Psychosocial functioning was addressed through emotion regulation (ER), which plays a central role in coping and psychological well-being during aging. ER is considered one of the “hot” (top-down) components of executive functioning and, in this intervention, was targeted through the “Stop & Relax” sessions, guided by the model of Gratz and Roemer (2004). Participants practiced recognizing and accepting emotions, using breathing techniques to manage arousal, and applying problem-solving strategies from the “Think & Act” section to support emotional clarity and regulation.
Mindfulness was also integrated into “Stop & Relax” to help participants remain present and non-reactive during emotional or cognitive challenges. Defined as sustained, non-judgmental attention to internal and external experience (Kabat-Zinn, 2021), mindfulness has been linked to improvements in ER and perceived cognition (Jha et al., 2019; Nien et al., 2020). In this intervention, mindfulness is served as a tool for emotional awareness and self-regulation. Though research on mindfulness in aging is limited, combining it with ER was hypothesized to yield stronger effects than either alone.
Finally, the program aimed to strengthen internal locus of control—the belief in one’s ability to influence life outcomes. Research suggests that perceived control often declines in later life due to cumulative biological, cognitive, and social changes (Cerino et al., 2023; Robinson & Lachman, 2017). By encouraging engagement and personalization of strategies, the intervention sought to foster personal agency and empowerment, counteracting perceived loss of control in later life.
The primary hypotheses of the study were twofold. First, it was hypothesized that participants who received the intervention would exhibit significantly greater improvement across all outcome variables—namely, memory compensation strategies, problem solving, emotion regulation, mindfulness, and internal locus of control—than those in the control group who did not receive the intervention. Second, it was expected that the observed treatment gains would be maintained over time, specifically at the 12-week follow-up assessment.
Methods
Participants
Sixty-nine individuals were initially recruited from the community through flyers and outreach and were subsequently enrolled in a larger longitudinal project on aging that evaluated cognitive performance and psychosocial functioning over time (Neuroage, NCT01481246; Chadjikyprianou et al., 2021). As part of this project, participants completed baseline assessments, which were used to determine eligibility for the present substudy.
Inclusion criteria were as follows: 1. Native Greek speakers. 2. Age 60 or older. 3. Good general health with no history of neurological disorders (e.g., head trauma, stroke, or neurodegenerative disease). 4. No current or past psychiatric diagnosis according to the DSM-5. 5. Normal-range performance on neurocognitive tasks based on NEUROAGE normative data (≥−1 SD from the normative mean across all domains). 6. Absence of subjective cognitive complaints, assessed during baseline screening through a structured interview conducted by a trained psychologist.
Of the 69 individuals screened, nine were excluded: three reported subjective cognitive complaints during the structured interview, one had a current psychiatric diagnosis, and three demonstrated below cut-off performance on the neurocognitive screening battery. Two additional individuals who met all criteria declined to participate in the intervention. Although the lower eligibility criterion was age ≥60, only two individuals aged 60–64 expressed interest in participating, but both were excluded during baseline screening as they did not meet the inclusion criteria. Beyond these cases, there was no additional interest from this age group, and the final sample therefore consisted of participants aged 65–75. The 60 participants were then randomly assigned to the experimental (n = 30) or control group (n = 30). Both the substudy and the larger project received approval from a national bioethics committee (Protocol No. ΕΕΒΚ/ΕΠ/2008/26). All participants provided written informed consent prior to participation.
Recruitment targets were guided by feasibility and effect sizes from similar interventions (Constantinidou, 2019; Davodi et al., 2023). Post hoc inspection of observed effect sizes in the current study indicated large effects, which suggests that the study was sufficiently powered to detect meaningful treatment-related differences.
The experimental group included 19 women, and 11 men aged 65 to 75 years (M = 69.03, SD = 3.04), while the control group included 21 women and 9 men aged 65 to 75 years (M = 70.12, SD = 3.51). Educational attainment, measured by total years of formal education, ranged from 8 to 17 years (experimental: M = 11.70, SD = 2.11; control: M = 11.76, SD = 2.02). The two groups were matched on demographic characteristics and cognitive status, as assessed by the Mini-Mental State Examination (experimental: M = 28.31, SD = 1.80; control: M = 28.06, SD = 1.95). Figure 2 presents the Consort diagram for participant flow. Consort Flowchart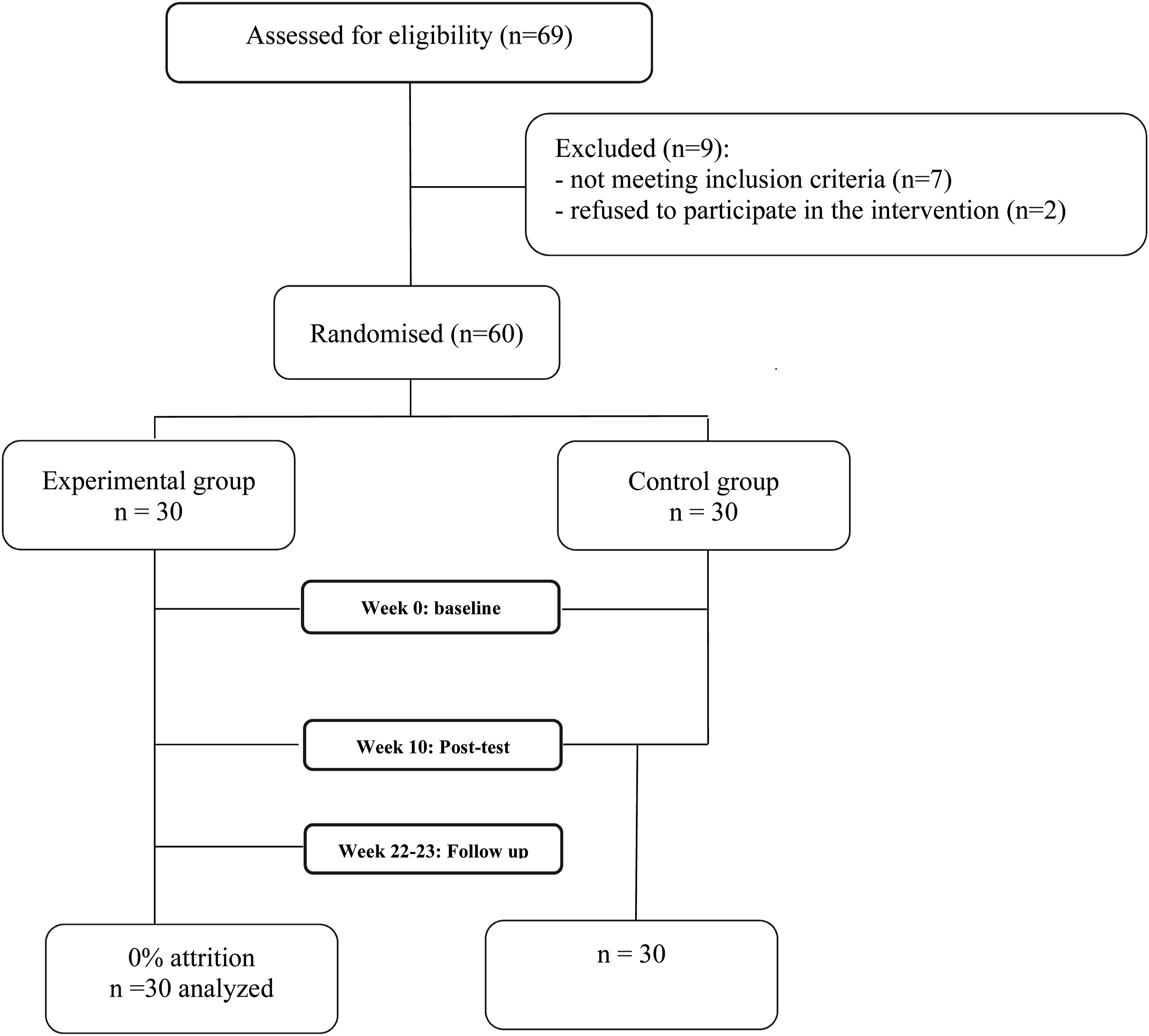
Measures
At baseline, all participants completed a neurocognitive screening to confirm eligibility. Key domains such as memory, executive functioning, and language were assessed. For further description on the screening protocol, see Chadjikyprianou et al. (2021). Dependent variables to assess treatment effectiveness consisted of validated self-report questionnaires administered pre- and post-intervention for both groups and at 12-week follow-up for the experimental group only.
Implementation of Memory Compensation Strategies Scale (MECSS)
The MECSS (Chadjikyprianou, 2022) was developed to evaluate the frequency and type of compensatory memory strategies used in daily life. It includes 20 items rated on a five-point Likert scale (0 = never, 4 = very often), forming two subscales: Internal strategies (11 items), capturing the use of mnemonic techniques, and External strategies (9 items), reflecting the use of environmental aids. Subscales demonstrated high internal consistency (Cronbach’s α = .89–.92).
Problem-Solving Inventory (PSI)
The Greek version of the PSI (Heppner & Petersen, 1982; Kourmousi et al., 2015) consists of 35 items (including three filler items) designed to assess individuals’ self-perceived problem-solving ability and style in everyday contexts. The inventory focuses on cognitive appraisals of problem-solving competence rather than actual performance. Each item is rated on a six-point Likert scale (1 = strongly agree, 6 = strongly disagree), with total scores ranging from 32 to 192. Lower scores indicate more functional and adaptive problem-solving appraisal. In the present study, internal consistency was high (Cronbach’s α = .88).
Difficulties in Emotion Regulation Scale (DERS)
The Greek version of the DERS (Gratz & Roemer, 2004; Mitsopoulou et al., 2013) was administered to assess perceived difficulties in emotion regulation. The scale consists of 36 items rated on a five-point Likert scale (1 = almost never, 5 = almost always), with higher scores indicating greater difficulty. It includes six subscales: lack of emotional clarity, lack of emotional awareness, impulse control difficulties, difficulties in goal-directed behavior, non-acceptance of emotional responses, and limited access to emotion regulation strategies. A total score is also computed to reflect global emotion dysregulation. The DERS aligns conceptually with third-wave cognitive-behavioral approaches, which emphasize the role of experiential avoidance in emotional disturbance. Internal consistency for all subscales was acceptable to high (Cronbach’s α = .81–92).
Mindful Attention Awareness Scale (MAAS)
The Greek version of the MAAS (Brown & Ryan, 2003; Mantzios et al., 2015) is a 15-item scale assessing dispositional mindfulness, defined as awareness and attention to present-moment experience. Items are rated on a six-point Likert scale, with higher scores indicating greater mindfulness. Internal consistency in the current study was high (Cronbach’s α = .86).
Multidimensional Locus of Control Inventory (MLCI)
The Greek version of the MLCI (Kourmousi et al., 2015; Levenson, 1973) was used to assess locus of control beliefs across three dimensions. The instrument includes 24 items rated on a six-point Likert scale ranging from -3 (strongly disagree) to +3 (strongly agree) and yields three subscale scores: Internality (beliefs that outcomes depend on one’s own actions), Powerful Others (perceived control by authority figures or institutions), and Chance (beliefs that life events are determined by luck or fate). Raw subscale scores are summed and adjusted by adding a constant of +24 to avoid negative totals. Higher scores on each subscale reflect stronger endorsement of the respective locus of control orientation. In the present study, internal consistency for all three subscales was high (Cronbach’s α = .82–.84).
Study Design and Intervention Protocol
The study employed a randomized pre–post design with follow-up. Sixty participants were randomly assigned to either the experimental (n = 30) or control group (n = 30). The experimental group was further randomly allocated into five small groups (n = 6 each) who received the intervention in a small-group format. Control group participants completed the neurocognitive screening and all dependent measures but did not receive any intervention. They were re-assessed after a 10-week interval which was the duration of the intervention received by the experimental group.
The intervention consisted of 10 weekly 90-minute sessions and followed a hierarchical structure, in which foundational content introduced early on supported the acquisition of more complex strategies in later weeks. This dosage was selected to balance theoretical and practical considerations. Evidence from recent reviews of cognitive interventions in healthy older adults suggests that a 10-week duration is close to the average length of effective programs (Bhome et al., 2018; Chiu et al., 2017). Regarding session length, studies typically report an average of approximately 66 minutes, with durations ranging from 45 minutes to 2 hours (Sanjuán et al., 2020). Drawing on this evidence and our theoretical framework, we implemented 10 90-minute sessions, which provided sufficient time to integrate both cognitive and psychosocial components while maintaining feasibility and participant engagement. For a detailed overview of the intervention protocol and the multidimensional instructional methods, see Chadjikyprianou and Constantinidou (2023).
The intervention sessions were co-led by a doctoral-level licensed and certified academic Speech-Language Pathologist with expertise in adult cognitive-communication disorders, and a licensed psychologist and doctoral student in Clinical Psychology with expertise in cognitive aging, who jointly facilitated all sessions. In addition, a graduate-level researcher attended each session to monitor adherence to the protocol and confirm that all groups followed the same content and procedures.
Statistical Analyses
All statistical analyses were conducted using IBM SPSS Statistics (Version 29), with the significance level set at α = .05. Independent t-tests assessed baseline group equivalence. Mixed repeated measures MANOVA and ANOVA were used to test intervention effects, with time (pre-test, post-test, and follow-up where applicable) as the within-subject factor and group as the between-subject factor.
Results
Group Performance at Baseline
Means and Standard Deviations for Dependent Variables at Pre-Test, Post-Test, and Follow-Up
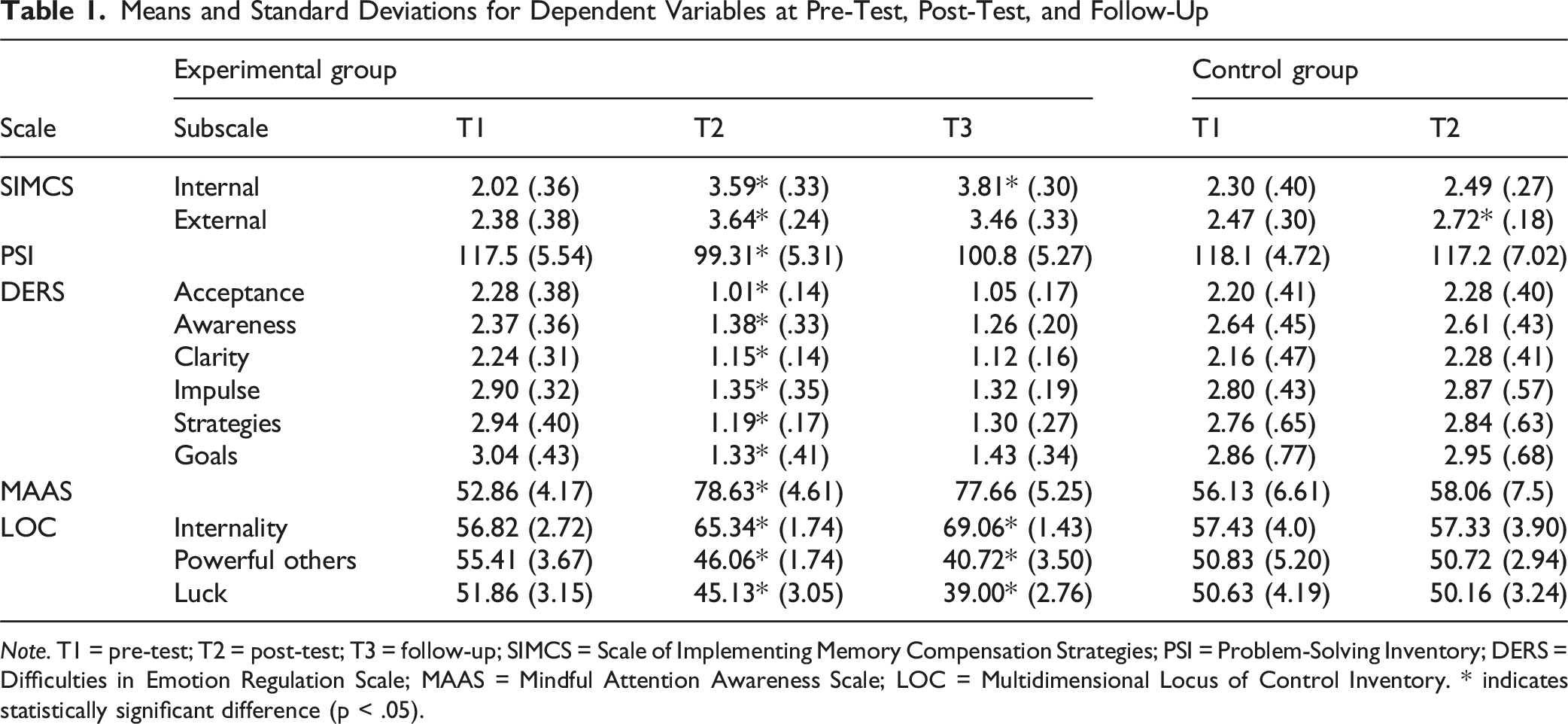
Note. T1 = pre-test; T2 = post-test; T3 = follow-up; SIMCS = Scale of Implementing Memory Compensation Strategies; PSI = Problem-Solving Inventory; DERS = Difficulties in Emotion Regulation Scale; MAAS = Mindful Attention Awareness Scale; LOC = Multidimensional Locus of Control Inventory. * indicates statistically significant difference (p < .05).
Effects of the Intervention on the Dependent Measures
Memory Compensation Strategies
A mixed repeated measures MANOVA on the Implementation of Memory Compensation Strategies Scale showed a significant effect of time, F (1, 58) = 400.03, p < .001, partial η2 = .90, observed power = 1, a main group effect, F (1, 58) = 35.48, p < .001, partial η2 = .51, observed power = 1, and a significant time x group interaction, F (1, 58) = 212.48, p < .001, partial η2 = .81, observed power = 1. A three-way interaction between group, time, and subscales was also significant, F (1, 58) = 11.94, p < .001, partial η2 = .76. These findings indicate that changes in memory compensation strategies over time differed by group and subscale.
Pre-planned pairwise comparisons showed that, in the experimental group, scores increased significantly from pre- to post-test on both the internal subscale (mean difference = 1.57, 95% CI [1.43, 1.72], p < .001) and the external subscale (mean difference = 1.26, 95% CI [1.12, 1.39], p < .001). In the control group, a small but significant increase was found only in the external subscale (mean difference = 0.25, 95% CI [0.12, 0.39], p < .001), while internal strategy use remained unchanged (p > .05).
For the experimental group, follow-up data collected at 12 weeks post-intervention showed a significant time x subscale interaction, F (2, 28) = 8.29, p < .001, partial η2 = .41. Internal strategy use continued to increase from post-test to follow-up (mean difference = 0.22, 95% CI [0.04, 0.40], p = .03), whereas the use of external strategies showed no significant change (p = .15). Figure 3 is graphic display of the clear upward trend from pre- to post-test for both subscales in the experimental group. Mean ascores of the experimental and control groups on internal and external memory compensatios strategies accross the three assesment points: pretest (T1), posttest (T2), and follow-up (T3). Note. High scores indicate greater use of memory compensation strategies. Error bars represent ±1 SD. Asterisks (*) indicate statistically significant change from the previous time point (p<. 05)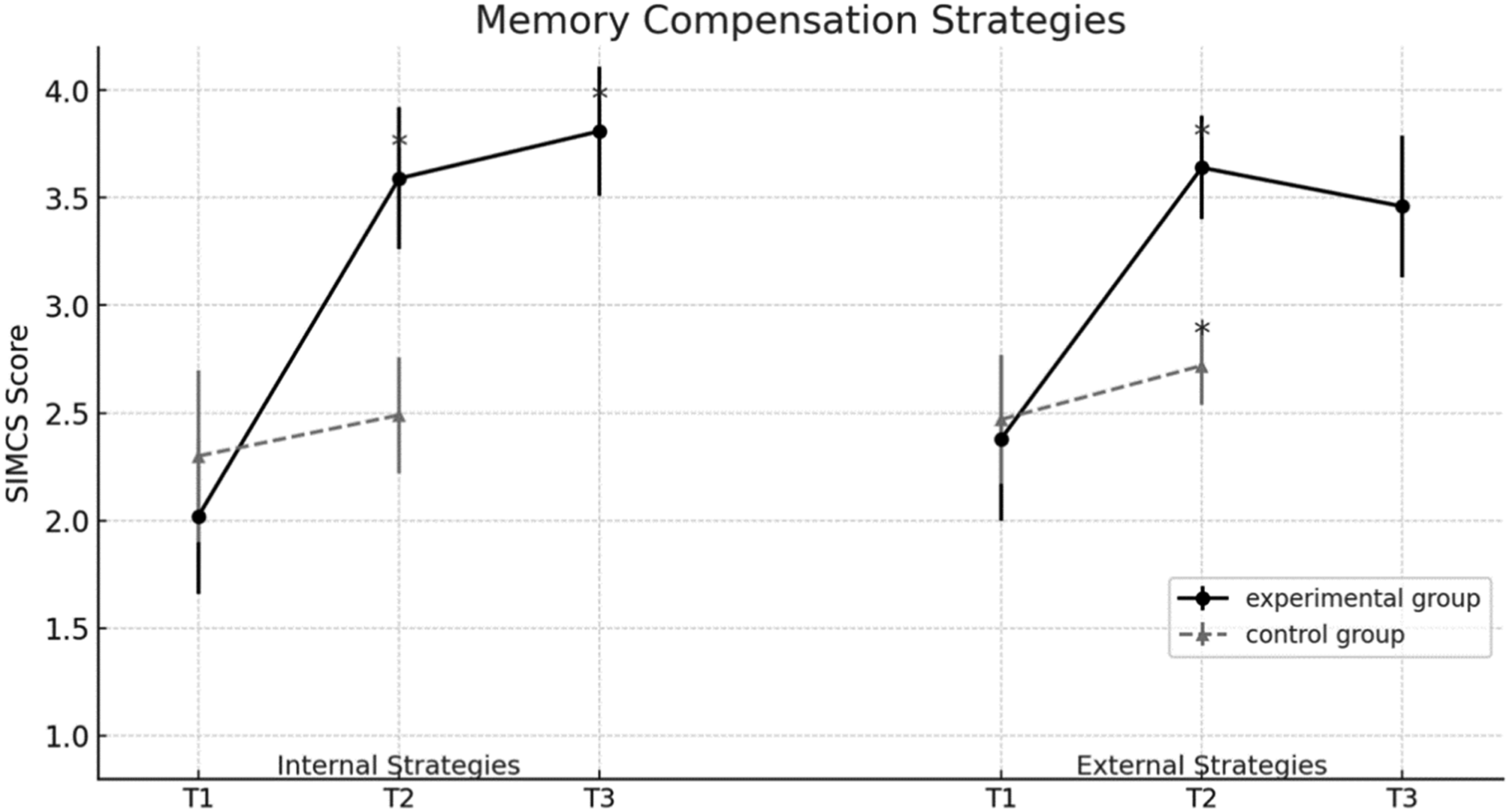
Problem Solving
A mixed repeated measures ANOVA on the Problem-Solving Inventory revealed a significant main effect of time, F (1, 58) = 91.60, p < 0.001, partial η2 = .61, observed power = 1, a main effect of group, F (1, 58) = 50.53, p < 0.001, partial η2 = .52, observed power = 1, and a significant time x group interaction, F (1, 58) = 75.70, p < .001, partial η2 = .56. These results indicate that changes in perceived problem-solving ability over time differed between the experimental and control groups.
Pre-planned pairwise comparisons confirmed a statistically significant reduction in PSI scores for the experimental group from pre-test to post-test (mean difference = 18.90, 95% CI [15.9, 21.8], p < .001), reflecting improved perceived problem-solving ability. In contrast, no significant change was observed in the control group (p = .54).
At the 12-week follow-up (experimental group only), no significant differences were found compared to post-test scores (p = .23), indicating sustained improvements. Figure 4 graphically depicts the results. Mean scores of the experimental and control groups on problem-solving strategies across the three assessment points: pretest (T1), posttest (T2), and follow-up (T3). Note. Lower scores indicate better problem-solving ability. Error bars represent ±1 SD. Asterisks (*) indicate statistically significant change from the previous time point (p<. 05)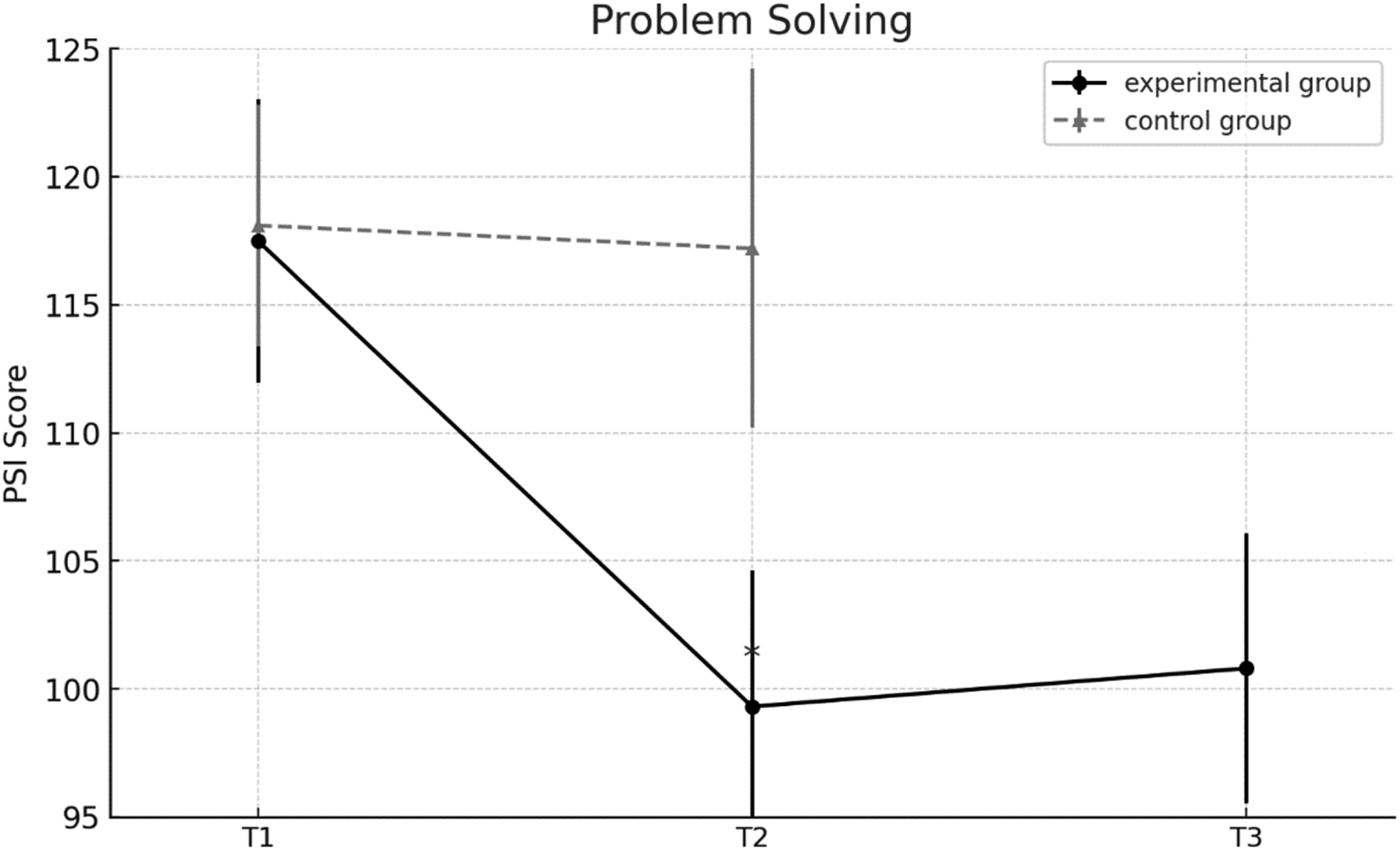
Emotion Regulation
A mixed repeated measures MANOVA on the Difficulties in Emotion Regulation Scale (DERS)—in which higher scores indicate greater difficulties in emotion regulation—revealed a significant effect of time, F (1, 58) = 390.55, p < 0.001, partial η2 = .87, observed power = 1, a main group effect, F (1, 58) = 53.56, p < 0.001, partial η2 = .48, observed power = 1, a significant time x group interaction, F (1,58) = 623.73, p < 0.001, partial η2 = .91, observed power = 1, and a three-way interaction between group, time, and the six subscales, F (5, 54) = 21.08, p < 0.001, partial η2 = .59, observed power = 1. These findings indicate that emotion regulation changes over time varied by group and across subscales.
Pre-planned pairwise comparisons for the experimental group showed statistically significant reductions across all six subscales from pre- to post-test (p < .001): acceptance (−1.27, 95% CI [−1.46, −1.08]), awareness (−0.99, 95% CI [−1.20, −0.78]), clarity (−1.09, 95% CI [−1.25, −0.93]), impulse control (−1.55, 95% CI [−1.73, −1.37]), strategies (−1.75, 95% CI [−1.91, −1.59]), and goal-directed behavior (−1.71, 95% CI [−1.93, −1.49]). These reductions reflect substantial improvements in emotional self-regulation. No significant changes were observed in the control group (p > .05).
Follow-up analyses for the experimental group revealed a significant time × subscale interaction, F (2, 28) = 23.40, p < .001, partial η2 = .92. No further changes were observed from post-test to follow-up (p > .05), indicating that the improvements were maintained.
As illustrated in Figure 5, a composite DERS score (average of all six subscales) was also calculated for visual presentation. The graph shows a sharp decline in emotion dysregulation for the experimental group from pre- to post-test, with gains sustained at follow-up. The control group exhibited no meaningful changes across time. Mean scores of the experimental and control groups on emotion regulation difficulties across the three assessment points: pretest (T1), posttest (T2), and follow-up (T3). Note. Lower scores indicate fewer difficulties in emotion regulation. Error bars represent ±1 SD. Asterisks (*) indicate statistically significant change from the previous time point (p<. 05)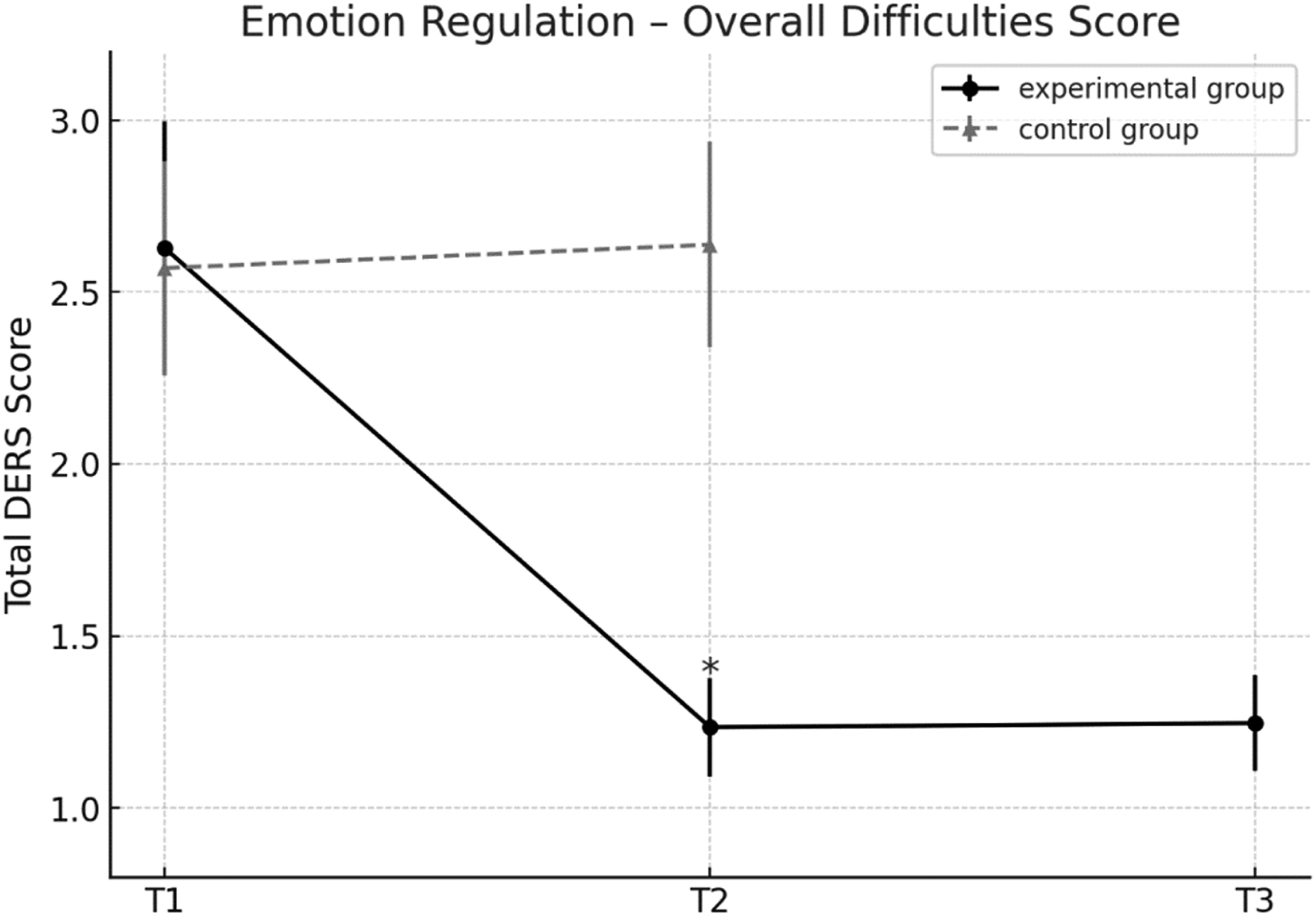
Mindfulness
Α mixed repeated measures ANOVA on the Mindful Attention Awareness Scale (MAAS), a measure in which higher scores indicate greater dispositional mindfulness, showed a statistically significant effect of time, F (1, 58) = 175.15, p < 0.001, partial η2 = .75, observed power = 1, a main effect of group, F (1, 58) = 50.53, p < 0.001, partial η2 = .52, observed power = 1, and a significant time x group interaction F (1, 58) = 129.66, p < 0.001, partial η2 = .69, observed power = 1. These results indicate that changes in mindfulness over time differed significantly between the two groups.
Pre-planned pairwise comparisons showed a significant increase in mindfulness scores for the experimental group from pre- to post-test (mean difference = 25.77, 95% CI [23.45, 28.09], p < .001). No significant change was observed in the control group (p = .20).
Follow-up data for the experimental group showed no significant difference between post-test and follow-up scores (p = .39), suggesting that gains were maintained over time. Figure 6 illustrates the changes in the experimental group from pre- to post-test, with these gains sustained at follow-up. Mean scores of the experimental and control groups on mindfulness attention awareness across the three assessment points: pretest (T1), posttest (T2), and follow-up (T3). Note. Higher scores indicate greater mindful awareness. Error bars represent ±1 SD. Asterisks (*) indicate statistically significant change from the previous time point (p<. 05)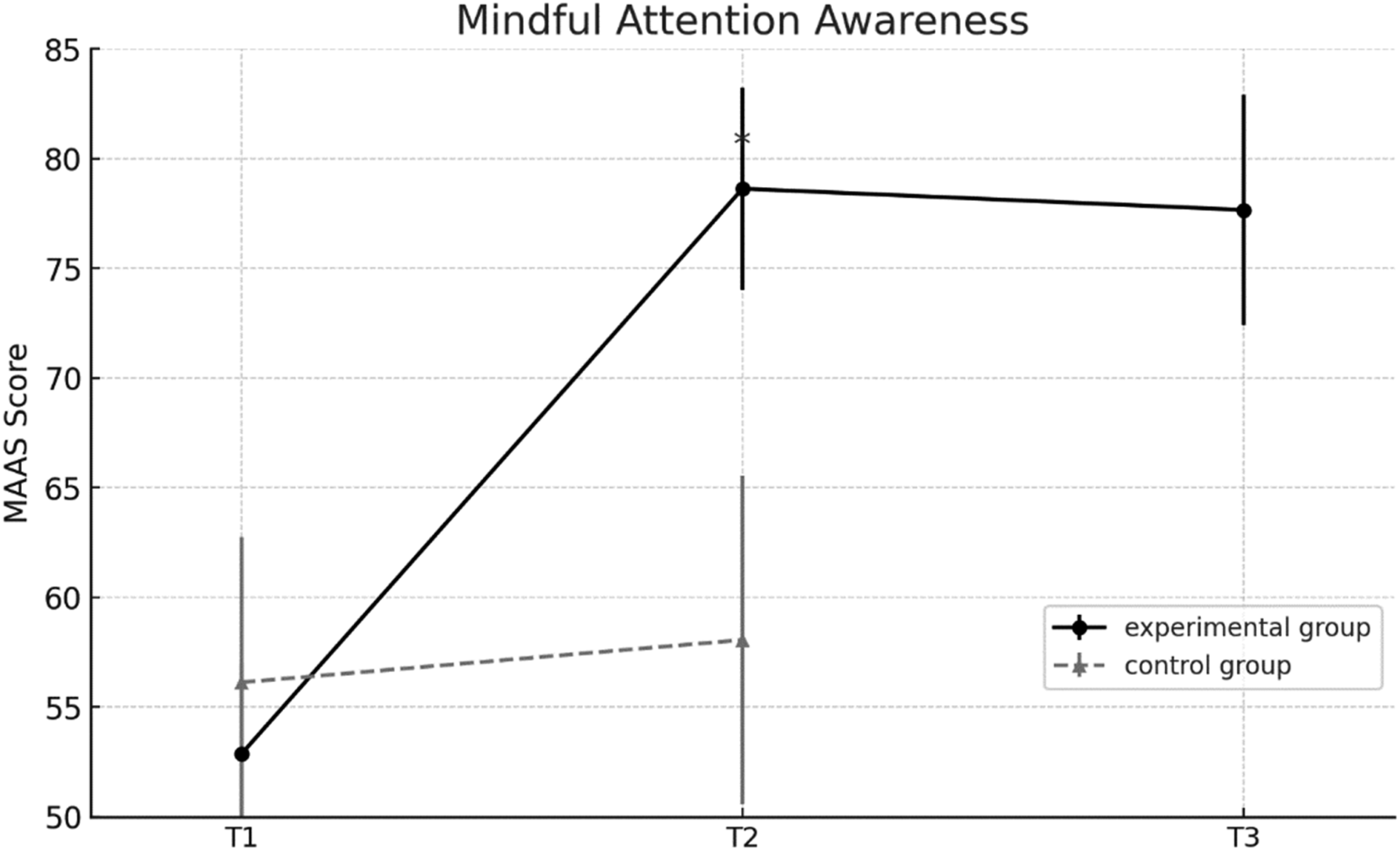
Locus of Control
A mixed repeated measures MANOVA on the Multidimensional Locus of Control Inventory showed an effect of time, F (2, 56) = 52.50, p < .001, partial η2 = .69, a main group effect, F (1, 57) = 4.57, p < 0.001, partial η2 = .39, and a three-way interaction between time, group, and subscales, F (4, 54) = 329.6, p < .001, partial η2 = .96,. These results indicate differential changes in locus of control dimensions across groups.
Pre-planned comparisons in the experimental group revealed increases in internality (mean difference = 8.51, 95% CI [7.75, 9.28], p < .001) and decreases in powerful others (−9.34, 95% CI [−10.27, −8.41], p < .001) and luck scores (−6.72, 95% CI [−7.47, −5.97], p < .001). No significant changes were observed in the control group.
At 12-week follow-up, a significant time x subscale interaction emerged in the experimental group, F (4, 25) = 536.71, p < .001, partial η2 = .98, observed power = .91. Internality scores continued to increase (mean difference = 3.72, 95% CI [2.93, 4.51], p < .001), while powerful others (mean difference = −5.34, 95% CI [−6.99, −3.69], p < .001) and luck scores (mean difference = −6.13, 95% CI [−7.22, −5.10], p < .001) further declined, reinforcing a shift toward internal control.
As shown in Figure 7, the experimental group maintained a consistent shift toward internal control, while the control group remained stable across subscales. Mean scores of the experimental and control groups on locus of control subscales -internality, powerful others, and luck- across the three assessment points: pretest (T1), posttest (T2), and follow-up (T3). Note. Higher scores indicate stronger beliefs in each respective control domain. Error bars represent ±1 SD. Asterisks (*) indicate statistically significant change from the previous time point (p<. 05)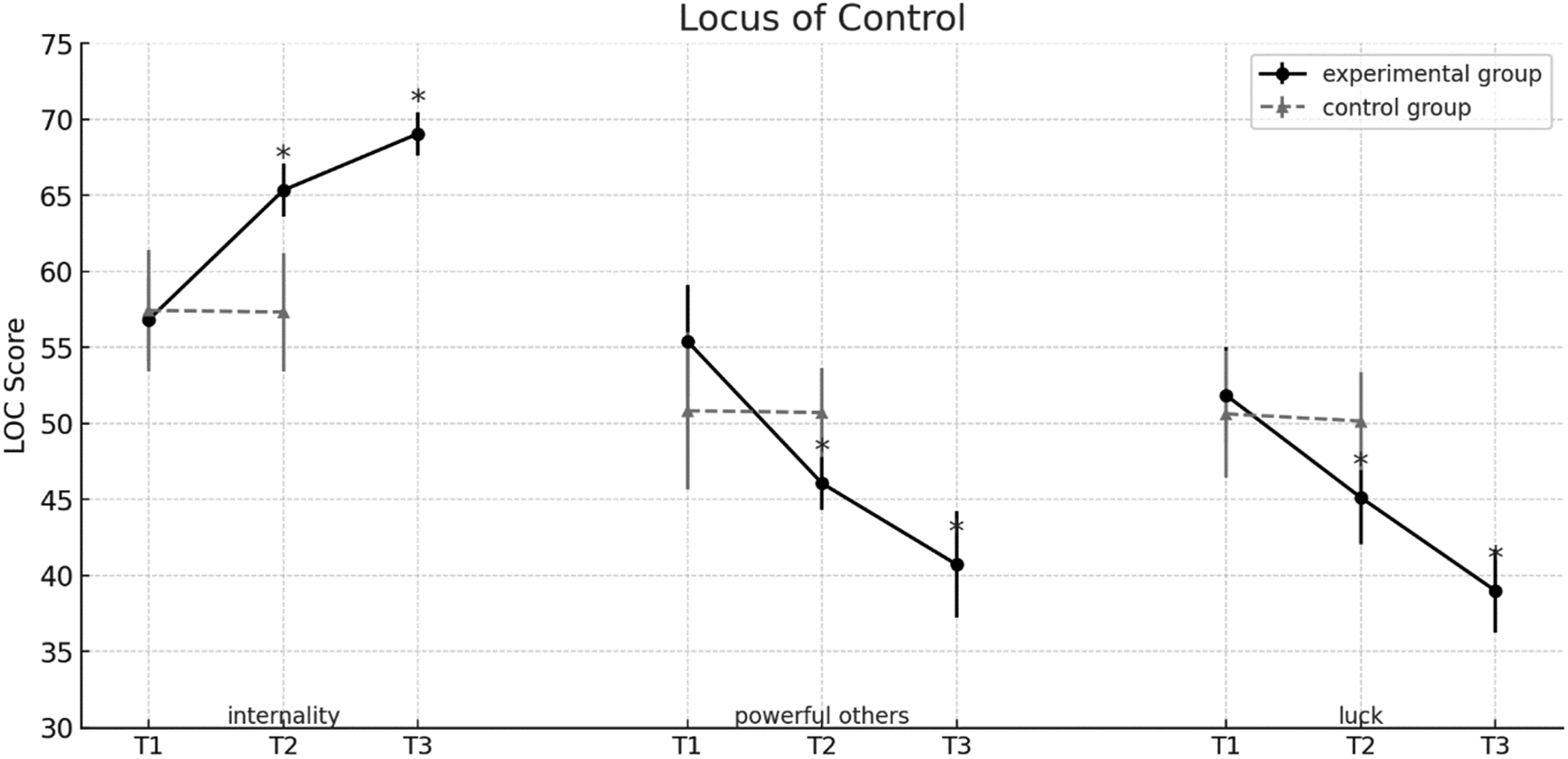
Discussion
The principal objective of the present study was to evaluate the effectiveness of a novel, multidimensional group intervention aimed at promoting perceived cognitive and psychosocial functioning in cognitively healthy older adults aged 65–75 residing in the community. Drawing from principles of cognitive rehabilitation and clinical psychology, the program targeted everyday cognitive strategies such as memory compensation and problem-solving while also enhancing emotion regulation, mindfulness, and a sense of personal control. To our knowledge, this is one of the first structured, theory-based, non-pharmacological interventions targeting healthy older populations that systematically integrates cognitive and emotional training in a coherent and skills-based framework.
Participants in the experimental group exhibited significantly greater improvements than those in the control group, and these gains were sustained at the 12-week follow-up. These findings align with a growing body of literature supporting the effectiveness of multidimensional approaches in enhancing cognitive and psychosocial outcomes in aging (Estebsari et al., 2014; Hsu et al., 2018; Nguyen et al., 2018). Its emphasis on functional skill application and perceived agency offers a practical, community-based framework that can support independent living and psychosocial resilience in older adulthood. The sections that follow explore in greater detail the functional domains addressed by the program.
Memory Compensation Strategies
Participants in the current intervention were actively engaged in addressing everyday memory challenges through structured scenarios during sessions and the application of internal and external Memory Compensation Strategies (MCS). Weekly diaries were used to monitor application, with prompts to support real-life implementation. Results showed a marked increase in the use of internal strategies across all assessment points, while external strategies improved significantly from baseline to post-test but did not show further significant change at follow-up. While the control group showed no change in internal strategies, they exhibited a small but significant improvement in external strategy use—possibly due to exposure to the self-report scale prompting reflection or strategy adoption. Interestingly, the experimental group continued to show gains in internal strategy use 12 weeks post-intervention. Throughout the program, internal strategies were emphasized as more cognitively demanding and central to memory function, though both were promoted as useful. Previous studies among healthy older adults and individuals with subjective memory complaints have reported a preference for external aids, as they are easier to integrate into daily routines (Bouazzaoui et al., 2010; Frankenmolen et al., 2017; Pizzonia & Suhr, 2022). The current findings extend this literature by demonstrating that older adults can improve their use of both strategy types through structured intervention, with sustained effects over time.
Problem Solving
A key objective of this study was to determine whether healthy older adults could benefit from targeted training in executive functioning through problem solving. Participants in the experimental group reported significantly improved perceptions of their problem-solving abilities, maintained at the 12-week follow-up. The control group showed no notable change.
Training was embedded in the “Think & Act” module, which introduced a five-step problem-solving model. Cognitive flexibility was emphasized during brainstorming, while planning and organization were targeted in subsequent stages where participants evaluated alternatives and formulated implementation plans. Weekly sessions included practice on realistic scenarios and at-home application to personal challenges. A distinctive feature was the integration of lifestyle domains such as nutrition and physical activity within the problem-solving framework. This allowed participants to apply executive strategies to health-related decisions, reinforcing practical relevance.
While most prior research has focused on clinical populations (e.g., Areán et al., 2010; Vasudev et al., 2022), the present study aligns with evidence from Nguyen et al. (2018), showing that even brief interventions can support decision making in healthy older adults. Notably, older adults, even when cognitively intact, often face age-related challenges in decision making and everyday problem solving (Chen et al., 2017; Thornton et al., 2013), which are commonly linked to executive dysfunction. The current results reinforce the notion that structured, theoretically grounded interventions can effectively support executive processes and everyday functioning in this population.
Emotion Regulation
Emotion regulation strategies were integrated across both the “Stop & Relax” and “Think & Act” components of the intervention, targeting all six dimensions outlined by Gratz and Roemer (2004), with particular attention to challenges associated with cognitive aging. Participants in the experimental group reported statistically significant reductions in emotion regulation difficulties across all DERS subscales from pre- to post-intervention, namely, in acceptance, awareness, clarity, impulse control, goal-directed behavior, and access to strategies. These improvements were sustained at the 12-week follow-up, with no further changes observed, indicating lasting effects. The control group, by contrast, exhibited no significant improvements across subscales, confirming that changes were driven by the intervention.
In-session activities focused on recognizing, labeling, and accepting emotional experiences, supported by diaphragmatic breathing to reduce physiological arousal and enhance self-regulation. Participants also completed weekly emotional clarity diaries to reinforce awareness and emotional tolerance.
While previous studies with older adults have emphasized stress reduction and general well-being (Estebsari et al., 2014; Hsu et al., 2018; Shirani et al., 2019), the present study is the first, to our knowledge, to systematically implement DERS-based emotion regulation training alongside problem-solving instruction. The findings suggest robust, durable improvements in emotion regulation through this integrative approach.
Mindfulness
Mindfulness techniques were incorporated into the “Stop & Relax” component of the intervention, supporting emotional regulation through present-moment awareness and reduced reactivity (Gallegos et al., 2015; Lutz et al., 2014). Unlike cognitive restructuring in Cognitive Behavioral Therapy (CBT), mindfulness emphasizes non-judgmental acceptance of thoughts, emotions, and bodily sensations (Zhang et al., 2021).
Participants in the experimental group showed a statistically significant increase in mindful attention from pre- to post-intervention, with gains maintained at the 12-week follow-up. No significant changes were observed in the control group.
Although research on mindfulness in the context of aging remains limited, the present findings highlight its potential to enhance emotional awareness and self-regulation in older adults. The integration of mindfulness into this structured intervention appears to have contributed meaningfully to observed psychosocial gains, reinforcing earlier findings on its cognitive-affective benefits in late life.
Locus of Control
Locus of control (LC), once seen as a stable trait (Rotter, 1966), is now viewed as modifiable through experience and structured interventions (Lachman et al., 2015). This is especially relevant in older adulthood, where declining internal LC is often linked to functional and psychosocial challenges (von Humboldt et al., 2024).
Findings from this study demonstrate that a structured, multidimensional intervention can produce meaningful and lasting shifts in LC. The experimental group showed significant increases in internal LC and reductions in external attributions (i.e., powerful others and luck) both post-intervention and at 12-week follow-up. In contrast, the control group exhibited no significant changes, underscoring the stability of LC in the absence of intervention (Hovenkamp-Hermelink et al., 2019).
Active engagement with the program through strategy application and personal reflection likely contributed to the internalization of control beliefs and the translation of abstract psychological constructs into everyday behavior. The sustained effects suggest that this shift reflects deeper cognitive restructuring rather than short-term reactivity.
These results have important implications. Internal LC has been associated with higher self-efficacy, motivation, adaptive coping, and improved psychological outcomes in older adults (Constantinidou & Kennedy, 2022; Hovenkamp-Hermelink et al., 2019). Integrating LC-enhancing components into aging interventions may therefore strengthen engagement, foster resilience, and support functional gains. The observed changes highlight LC as a modifiable factor with substantial relevance for cognitive and emotional health in later life.
Limitations and Future Research
Despite encouraging results, several limitations should be noted. First, the relatively small sample, though adequate to detect large effects, was not determined via a priori power analysis, limiting generalizability and detection of smaller effects. In addition, the study relied on self-reported measures of cognitive and emotional functioning without objective post-intervention assessments. While self-reports offer ecologically valid insights into perceived change, future studies should combine subjective and objective measures to determine whether perceived gains are accompanied by measurable performance improvements. Evaluating the program in more diverse populations, including individuals with lower education or mild cognitive impairment, would further enhance its relevance.
Second, the absence of an active control group with matched group dynamics is a major limitation, as it prevents firm conclusions about whether the observed benefits reflect intervention-specific mechanisms or non-specific factors such as peer interaction or placebo effects. Future studies should therefore incorporate active control conditions (e.g., groups receiving general educational content or social activities) to disentangle specific intervention effects from non-specific influences. Relatedly, follow-up assessments were conducted only with the experimental group. While this provided useful information about maintenance of effects, it limited causal inferences and precluded direct comparisons with controls. This design decision was primarily driven by feasibility constraints, but future studies should include follow-ups for all study arms to more rigorously evaluate long-term outcomes.
Third, because the program was multicomponent, combining cognitive and emotional training elements, the present design does not allow us to isolate which components were most effective in driving the observed changes. Importantly, however, the intervention was intentionally conceived as an integrated cognitive-psychosocial package, based on the rationale that combined training may yield complementary and potentially synergistic benefits. This integrated approach is one of the program’s strengths, aligning with recent calls for holistic interventions in aging research. At the same time, we recognize the value of probing mechanisms of change. Future studies should therefore employ more extensive pre–post neuropsychological batteries, enabling exploratory associations between targeted domains and observed outcomes.
Finally, the complete absence of attrition across the 23-week study period warrants comment, given that psychosocial and cognitive interventions with older adults typically report attrition rates between 12% and 30% (Ngandu et al., 2022; Reijnders et al., 2017; Rosenberg et al., 2020; Zülke et al., 2024). Notably, however, other intensive cognitive rehabilitation programs have also reported no attrition (Constantinidou, 2019). High retention in this study may reflect multiple factors: participants were cognitively healthy, community-dwelling, and voluntarily enrolled, suggesting strong intrinsic motivation. The group-based format likely fostered social connectedness, consistent with cultural values in Cyprus emphasizing communal participation. Program acceptability also appears to have played a central role: in our earlier publication, more than 90% of participants reported being extremely satisfied with the meeting topics, 97% with the instructor’s organization and preparation, and 96.7% with the support provided (Chadjikyprianou & Constantinidou, 2023). Control group retention may similarly reflect intrinsic motivation to contribute to research, interest in repeated assessments, and the close contact maintained with the research team. While this strengthens internal validity, it also suggests that the sample may represent a particularly motivated and socially engaged group, limiting generalizability.
To support long-term impact, future versions could incorporate booster sessions or digital tools to sustain engagement. Despite limitations, this study offers an important step toward scalable, theory-based, and ecologically valid interventions. Integrating cognitive and emotional strategies within a structured, community setting provides a solid foundation for future refinement and broader application.
Conclusion
This study offers initial evidence for the effectiveness of a structured, multidimensional intervention in enhancing perceived cognitive and psychosocial functioning in healthy older adults. By combining cognitive rehabilitation and psychological strategies, the program supported improvements in domains essential for autonomy and daily functioning. Emphasizing experiential learning and real-life application, it appears well-suited for community and preventive contexts. Notably, the observed gains were sustained over time.
Overall, the findings highlight the value of integrated, non-pharmacological interventions in promoting healthy aging. Addressing cognitive and emotional domains within a unified framework may foster resilience, self-efficacy, and quality of life. These results support the importance of early, theory-driven approaches for preserving autonomy and psychological well-being in later life.
Footnotes
Acknowledgments
We thank all participants and their families for their involvement in the study, as well as the student researchers from the Neurocognitive Research Laboratory at the University of Cyprus for their support in the data collection process.
Ethical Consideration
The Neurocognitive Study for the Aging (Neuroage) has been reviewed and approved by the Cyprus National Bioethics Committee (protocol number: ΕΕΒΚ/ΕΠ/2008/26) and is registered with the Commissioner for Protection of Personal Data.
Consent to Participate
All participants provided written informed consent to participate in the study.
Author Contributions
AC conceptualized and designed the project, coordinated the data collection, analyzed data, and wrote the manuscript. FC conceptualized and designed the project, supervised the data collection/analysis, and wrote the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was co-funded by the European Regional Development Fund and the Republic of Cyprus through the Research and Innovation Foundation (Excellence/1216/0404).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the princiapl investigator (FC) upon reasonable request.