
Abstract
Although research has linked ageism and pain to increased stress in older adults, their influence on stress within the context of pandemics has not been adequately examined. Our objective was to investigate relationships among pain, ageism, and pandemic-related stress in older adults using structural equation modeling (SEM) and mediation analysis. We hypothesized that pain would exert a direct and/or indirect influence on pandemic-related stress, and ageism a direct influence. Data were collected from 486 North American older adults in January 2024. Participants completed measures of pain, ageism, and pandemic-related stress. SEM and mediation analyses yielded evidence suggesting ageism and pain influence pandemic-related stress, although ageism mediated pain’s impact on pandemic-related stress. This study underscores how pain and ageism can impact older adults’ psychological well-being during pandemics. Findings highlight a potential need for public health interventions to address ageism and pain during future waves of COVID-19 or other global health crises.
Introduction
Ageism is a pervasive social issue that disproportionately impacts the older adult population (Allen, Solway, Kirch, Singer, Kullgren, Moïse et al., 2022; Officer & de la Fuente-Núñez, 2018) and includes stereotypes, discrimination, or prejudice directed toward others or oneself based on age (Butler, 1969; World Health Organization, 2021). The COVID-19 pandemic intensified ageism toward older adults (Ayalon, 2020). Throughout the pandemic, COVID-19 was frequently mischaracterized in the media, public discourse, and government policy as an “older adult problem,” negatively portraying this age group as “frail” and “vulnerable” against the virus (Ayalon, 2020; Castillo et al., 2022; Fraser et al., 2020; Peckham et al., 2024). Indeed, some countries implemented stricter public health policies targeting older adults solely on the basis of age, without consideration of overall health status or other important risk factors for COVID-19 (e.g., presence of a chronic illness; Aloni & Ayalon, 2023). For example, in March 2020, the United Kingdom government recommended that all individuals aged 70 years and older self-isolate for at least 12 weeks, regardless of whether they had any pre-existing medical conditions (Fletcher, 2021; Public Health England, 2020). Research analyzing COVID-19-related coverage on social media revealed a marked increase in ageist content, including the trending Twitter (now X) hashtags #BoomerRemover and #CoffinDodger (Castillo et al., 2022; Jimenez-Sotomayor et al., 2020; Lichtenstein, 2021).
Ageism has deleterious consequences for older adults, including worsened mental, cognitive, and physical health (Chang et al., 2020), heightened pain severity (Levy et al., 2023), and lower quality of life (Chang et al., 2020). Moreover, ageism is linked to higher levels of stress (Kang & Kim, 2022; Lyons et al., 2018). Given the rise in ageism observed during the COVID-19 pandemic, ageism may also contribute to COVID-related stress in older adults. However, this association has yet to be explored empirically.
Pain is another contributor to stress and anxiety among older adults (Arola et al., 2010; Brennan, 2020, 2023) and is highly prevalent in this population (Yong et al., 2022; Zimmer et al., 2022). Pain is a subjective and multidimensional experience shaped by physiological, psychological, and social factors (Raja et al., 2020; Williams & Craig, 2016). Ageism is one of these social factors (Gignac et al., 2006; Levy et al., 2023); specifically, pain in older adults is often inadequately diagnosed and treated due to ageist stereotypes that view it as a normal part of aging which, in turn, can exacerbate pain experiences (Horgas, 2017; Molton & Terrill, 2014). The COVID-19 pandemic introduced further barriers to these pain management challenges due to efforts to limit virus transmission (e.g., closure of pain clinics, exercise facilities; El-Tallawy et al., 2020; Ziadni et al., 2022). As a result, individuals living with pain during the pandemic reported worsening pain severity (Chatkoff et al., 2022; Pagé et al., 2021), greater pain interference (Hruschak et al., 2021), and reduced control over their pain (Chatkoff et al., 2022). Furthermore, pain is often accompanied by social isolation, which was found to increase stress levels during the pandemic (Boyraz et al., 2020). These findings collectively suggest that it is important to test the reciprocal path between pain and ageism.
Pandemics are dynamic health crises that introduce numerous stressors, which can significantly impact psychological well-being (Taylor, 2022). COVID Stress Syndrome (Taylor et al., 2020a) provides a comprehensive framework for understanding and empirically measuring pandemic-related stress. According to Taylor et al. (2020a), COVID Stress Syndrome encompasses a range of interconnected emotional and behavioral responses to pandemics, including fear of contracting the virus, concerns about socioeconomic impacts, xenophobia (e.g., fear of virus transmission from “outsiders”), compulsive checking and reassurance seeking, and trauma-related responses (e.g., nightmares). These dimensions of COVID Stress Syndrome can be assessed using the widely validated COVID Stress Scales (CSS), which were deliberately designed to be easily adapted for measuring stress in future pandemic contexts (Taylor et al., 2020a, 2020b). Research using the CSS has shown that individuals with pre-existing mental and physical health conditions, such as anxiety, mood disorders, and chronic pain, report heightened levels of pandemic-related stress (Asmundson et al., 2020, 2022; Asquini et al., 2021). However, as noted by Hadjistavropoulos and Asmundson (2022), there remains a notable gap in research examining the impact of pandemic-related stress in older adults, a population at increased risk for adverse health outcomes post COVID-19 infection (Mueller et al., 2020).
Given the high prevalence of both ageism and pain affecting the older adult population (Dahlhamer et al., 2018; Lozon & Barratt, 2012), and their well-documented negative impacts on health and well-being (Chang et al., 2020; Fine, 2011), it is important to investigate how these factors may contribute to pandemic-related stress in this demographic. Understanding their impact could identify key targets for future interventions aimed at mitigating pandemic-related stress among older adults. The objective of this study is to address gaps in the literature regarding the theoretical interrelationships among pain, ageism, and pandemic-related stress in older adults. Drawing from the existing literature, we hypothesized a model wherein: (1) Pain influences pandemic-related stress directly and/or indirectly; (2) Ageism influences pandemic-related stress directly; and (3) Ageism is a mediator of pain and pandemic-related stress
Methods
Data Collection Procedure and Participants
This study received ethical approval from our institutional ethics board (#2023-417). Data were collected as part of a larger project (Arsenault et al., 2025) through online surveys distributed by Qualtrics Panels (https://www.qualtrics.com/) between January 18 and 22, 2024. The data previously published from the larger project strictly pertained to item response theory and confirmatory factor analyses of the CSS. Data pertaining to ageism and pain have not been previously published.
The sampling strategy and demographic verification process employed by Qualtrics Panels in this study are described elsewhere (Arsenault et al., 2025). Inclusion criteria comprised being a member of Qualtrics Panels, aged 65 years or older, residing in North America, and fluent in English. This sampling strategy resulted in an overrepresentation of White participants, likely due to their disproportionate presence in Qualtrics Panels. We address this limitation and its implications for sample representativeness below. All eligible participants provided informed consent by agreeing to the online form. Participants were compensated based on their specific agreement with Qualtrics Panels at the time in which they completed the survey.
Measures
Sociodemographic Questionnaire
We gathered the following self-report sociodemographic characteristics from participants: age, gender identity, race, ethnicity, marital status, level of education, employment status, household income, pain status, and COVID-19 history.
Geriatric Pain Measure (GPM–24)
Descriptive Statistics and Reliability Indices for Scores on the Geriatric Pain Measure (GPM–24) and Everyday Ageism Scale.
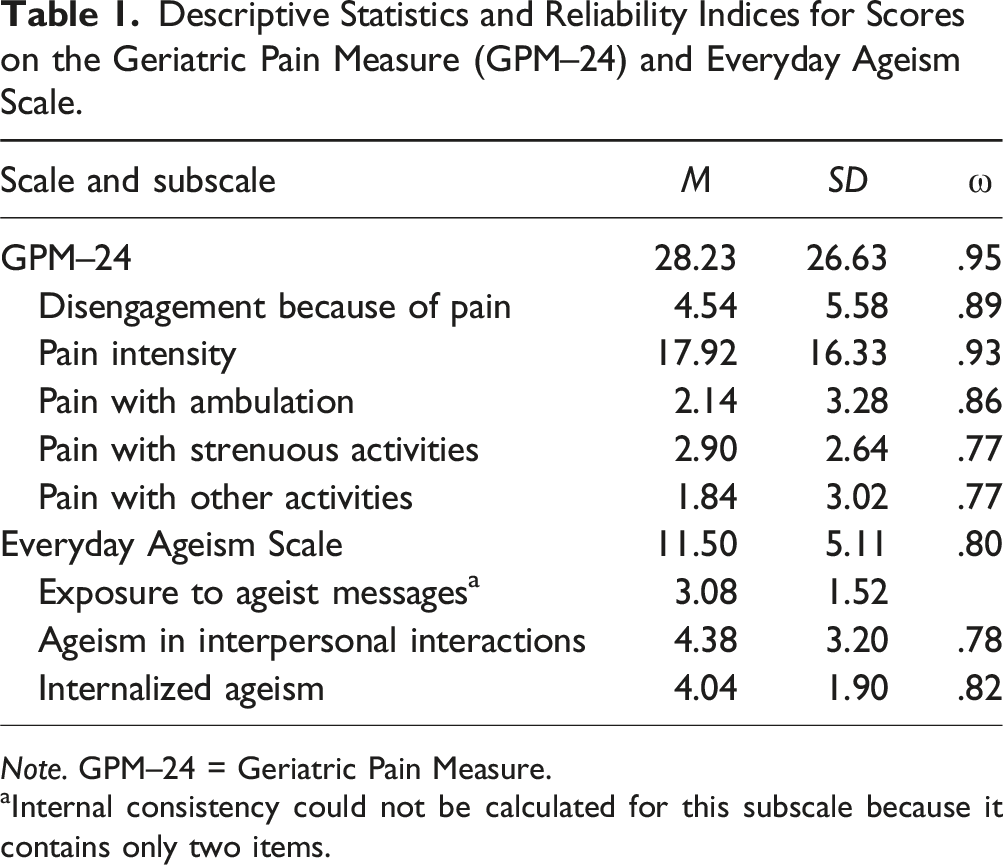
Note. GPM–24 = Geriatric Pain Measure.
aInternal consistency could not be calculated for this subscale because it contains only two items.
Everyday Ageism Scale
The Everyday Ageism Scale (Allen, Solway, Kirch, Singer, Kullgren et al., 2022) is a 10-item self-report questionnaire that assesses participants’ experiences with ageism in three subscales: (1) exposure to ageist messages (e.g., “I hear, see, and/or read jokes about old age, aging, or older people”); (2) ageism in interpersonal interactions (e.g., “People assume I have difficulty remembering and/or understanding things”); and (3) internalized ageism (e.g., “Feeling lonely is part of getting older”). Items in the exposure to ageist messages and ageism in interpersonal interactions subscales involve participants rating how often they have been exposed to everyday ageist events on a 4-point Likert scale ranging from 0 (never) to 3 (often). For the internalized ageism subscale, participants are asked to indicate their agreement with age-based stereotypes on a different 4-point Likert scale ranging from 0 (strongly disagree) to 3 (strongly agree). Individual subscale and total scores were obtained by summing the responses to applicable items. Subscale scores may range from 0 to 6 for exposure to ageist messages, 0 to 15 for ageism in interpersonal interactions, and 0 to 9 for internalized ageism. Total scores may range from 0 to 30. Higher scores reflect more frequent experiences of ageism. The Everyday Ageism Scale has shown acceptable overall internal consistency (α = .77) and acceptable subscale reliability (α = .75–.78; Allen, Solway, Kirch, Singer, Kullgren et al., 2022). Reliability for the exposure to ageist messages subscale cannot be computed due to consisting of only two items. In the current study, internal consistency for the overall scale and its subscales ranged from acceptable-to-good (Table 1).
COVID Stress Scales (CSS)
The CSS (Taylor et al., 2020b) is a 36-item self-report questionnaire that measures stress in response to pandemics over five scales: (1) fears of danger and contamination (DANCON); (2) fear of socioeconomic consequences (SEC); (3) xenophobia (XEN); (4) compulsive checking and reassurance seeking (CHE); and (5) traumatic stress symptoms (TSS). The most suitable factor structure of the CSS has been shown to vary across populations. For instance, the five-factor model has been supported in North American (Taylor et al., 2020b), Polish (Adamczyk et al., 2021), and Persian (Khosravani et al., 2021) samples, whereas a six-factor model that distinguishes DAN and CON as separate subscales has been supported in Serbian (Milic et al., 2021), Peruvian (Noe-Grijalva et al., 2022), and Swedish (Carlander et al., 2022) samples. More recently, the six-factor model was supported in an older adult population (Arsenault et al., 2025). Considering these findings, we applied the six-factor structure of the CSS for all statistical analyses in the current study.
Items in the DAN (e.g., “I am worried our healthcare system is unable to keep me safe from the virus”), CON (e.g., “I am worried that people around me will infect me with the virus”), SEC (e.g., “I am worried about grocery stores running out of cold or flu remedies”), and XEN (e.g., “I am worried about coming into contact with foreigners because they might have the virus”) scales are rated on a 5-point Likert scale ranging from 0 (not at all) to 4 (extremely). Items in the CHE (e.g., “Sought reassurance from friends or family about COVID-19”) and TSS (e.g., “I thought about the virus when I didn’t mean to”) scales use a different 5-point Likert scale, where ratings range from 0 (never) to 4 (almost always). Scale scores can be calculated by adding participants’ responses to the relevant items, and total scores by summing the scores of all six scales. Scale scores can range from 0 to 24, and total scores from 0 to 144. Higher values reflect more severe levels of pandemic-related stress. The CSS have demonstrated strong psychometric properties (α = .83–.94; Taylor et al., 2020b), and robust cross-cultural reliability and validity (Rachor et al., 2023). Our data revealed that the reliability of the individual scales ranged from good-to-excellent (ω = .85-.93), and the total CSS had excellent reliability (ω = .96; Arsenault et al., 2025).
Data Analysis
Descriptive Statistics and Internal Consistency
All descriptive and reliability statistics were conducted using IBM SPSS 28.0.0.0. Descriptive statistics were calculated for scores on the GPM–24 (Ferrell et al., 2000) and Everyday Ageism Scale (Allen, Solway, Kirch, Singer, Kullgren et al., 2022). To assess the internal consistency of each measure, we used McDonald’s Omega coefficient. McDonald’s Omega is considered a more robust measure of reliability than Cronbach’s alpha, as it is less affected by sample size or the number of items on a scale (Dunn et al., 2014; McNeish, 2018). We considered reliability values between .70 and .80 as acceptable, values between .80 and .90 as good, and values of .90 or higher as excellent.
Structural Equation Modeling (SEM)
Structural equation modeling (SEM) analyses were conducted using IBM SPSS Amos 28.0.0.0. SEM is a multivariate statistical technique used to verify a specified theoretical model by testing relationships between multiple unobserved (i.e., latent), observed (i.e., measured), and error (i.e., exogenous) variables (Byrne, 2016; Wright, 1934). In the current study, pain, ageism, and pandemic-related stress were modeled as the latent variables, and each of the individual subscales on the GPM–24 (Ferrell et al., 2000), Everyday Ageism Scale (Allen, Solway, Kirch, Singer, Kullgren et al., 2022), and CSS (Taylor et al., 2020b) represented the observed variables. We selected SEM as our statistical approach because our study involved modeling several latent variables (i.e., ageism, pain, and pandemic-related stress). SEM is particularly well-suited for this type of analysis because it allows us to model these latent constructs while accounting for measurement error, thereby enhancing measurement accuracy (Christ et al., 2014). Moreover, given the complexity of the relationships in our study, including potential mediation effects, SEM provided a comprehensive and robust framework for testing our hypotheses.
We also considered several possible covariates that might influence the relationships among pain, ageism, and pandemic-related stress: age, education, race, gender, and history of COVID-19 infection. As shown in Supplemental Table 1, the pair-wise Pearson correlation coefficients between these variables and pain, ageism, and pandemic-related stress were small, indicating no evidence of potential confounding bias as a result of omitting them from the SEM. To illustrate, we present SEM 5 in Supplemental Figure 1, which includes history of COVID-19 infection as an added covariate. The inclusion of this variable did not produce any noteworthy changes in the relationships among pain, ageism, and pandemic-related stress (see Supplemental Figure 1).
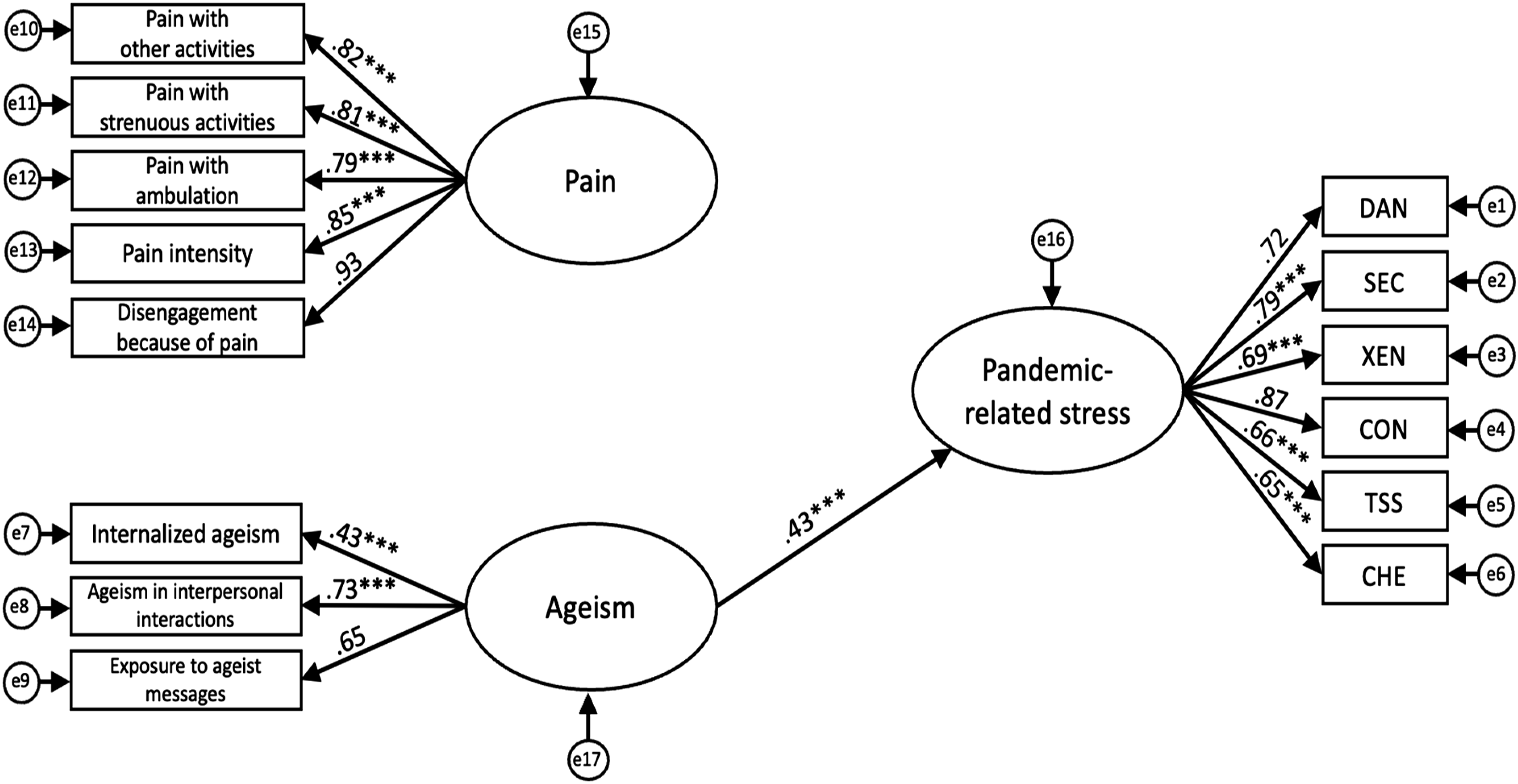
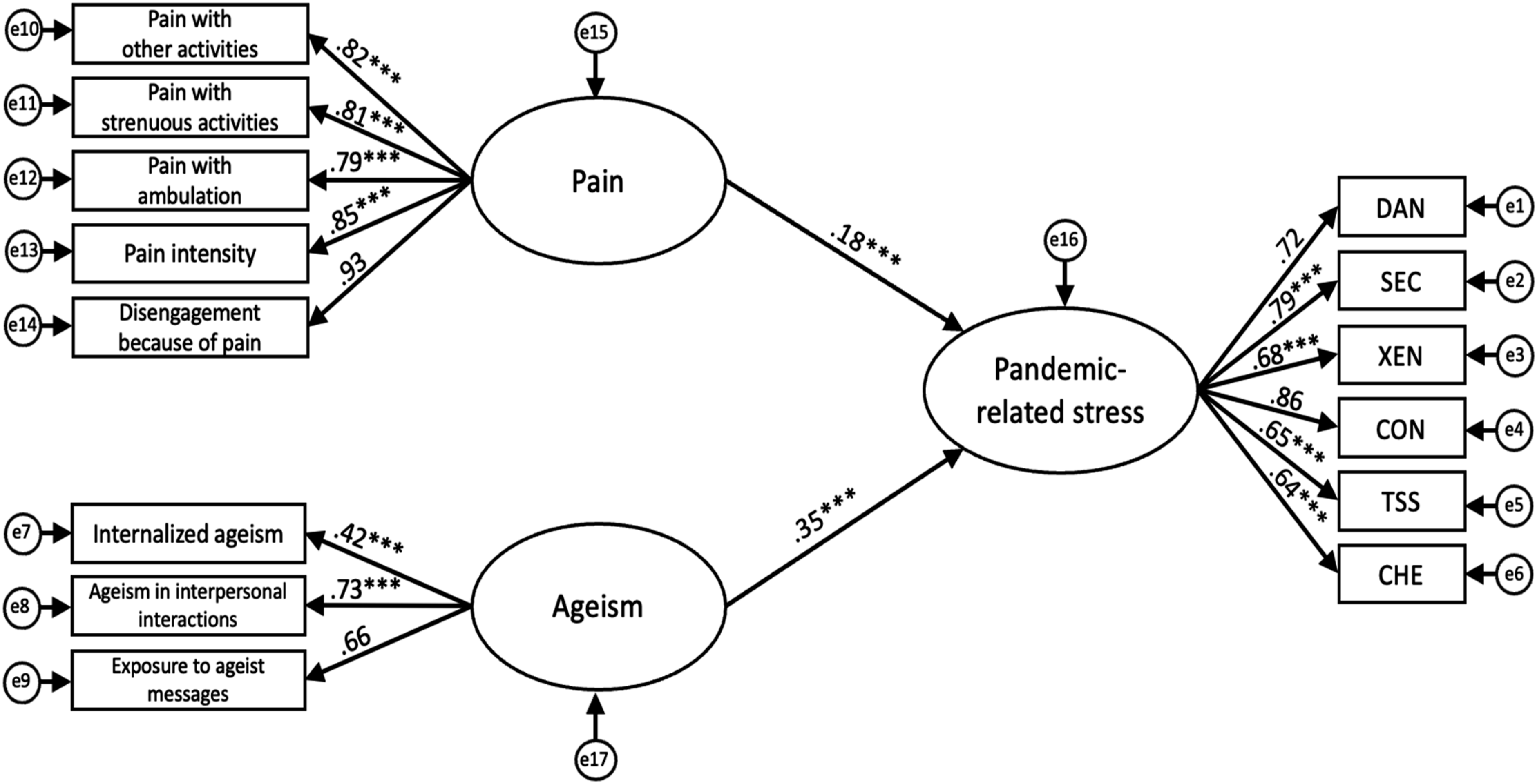
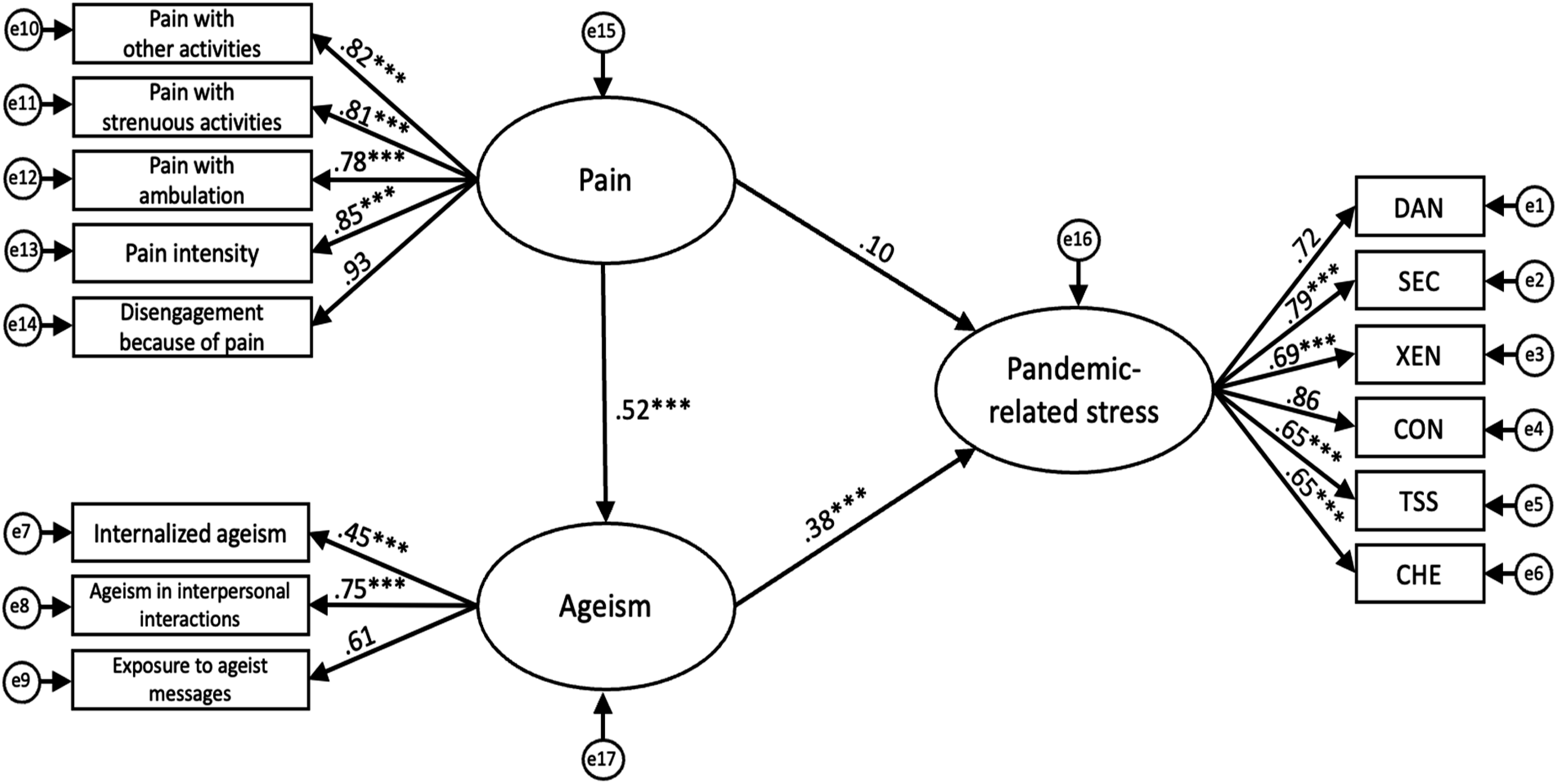
We fitted several SEMs to examine the relationships between these variables and better understand how different pathways may influence older adults’ levels of pandemic-related stress: (1) SEM 1 examined the direct effects of pain on pandemic-related stress (Figure 1). (2) SEM 2 examined the direct effects of ageism on pandemic-related stress (Figure 2). (3) SEM 3 examined the simultaneous direct effects of pain and ageism on pandemic-related stress (Figure 3). (4) SEM 4 examined the potential mediating effect of ageism in the relationship between pain and pandemic-related stress by adding a pathway between pain and ageism (Figure 4). (5) SEM 5 expanded on SEM 4 by controlling for the effect of previously contracting COVID-19 (see Supplemental Figure 1).
Several guidelines have been proposed regarding the minimum sample size for SEM, including 100–200 total cases (Boomsma, 1985), at least 10 cases per variable (Nunnally, 1967), and five to 10 cases per parameter (Bollen, 1989). Our sample size of 486 exceeded each of these recommended guidelines, making it well-suited for performing SEM analysis. While a sample of this size is deemed satisfactory by SEM standards (Wolf et al., 2013), it is not considered excessively large.
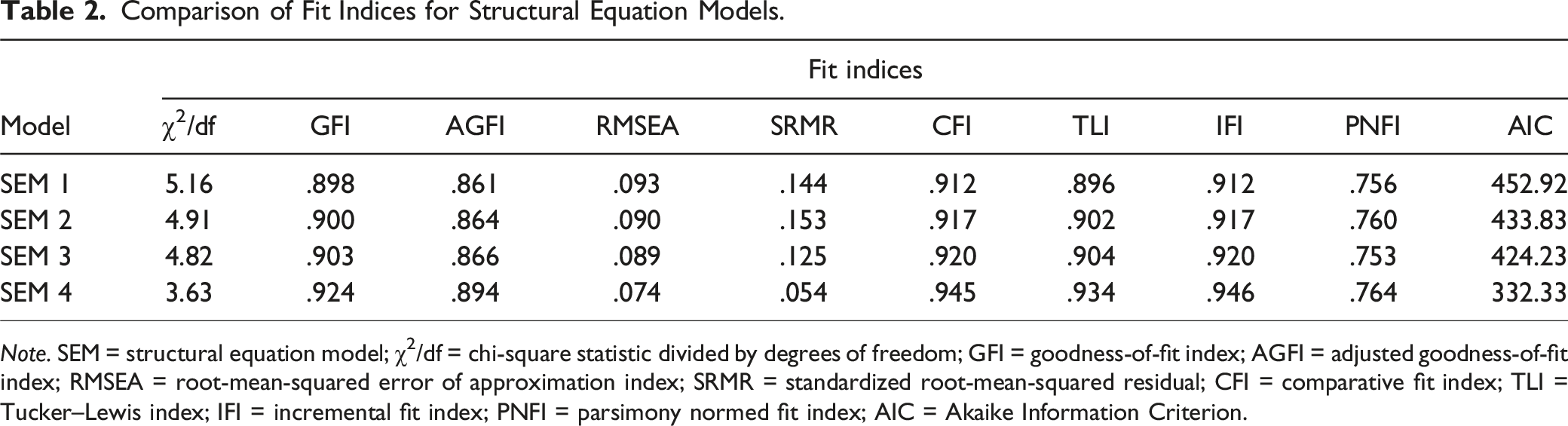
The following fit indices were used to test our hypothesized models, as recommended in the literature (Hu & Bentler, 1998, 1999; Schermelleh-Engel et al., 2003): chi-square statistic (χ2) and degrees of freedom (df), goodness-of-fit index (GFI), adjusted goodness-of-fit index (AGFI), root-mean-squared error of approximation index (RMSEA), standardized root-mean-squared residual (SRMR), comparative fit index (CFI), Tucker–Lewis index (TLI), incremental fit index (IFI), Akaike Information Criterion (AIC), and parsimony normed fit index (PNFI). The chi-square statistic, GFI, AGFI, RMSEA, and SRMR are absolute fit indices which evaluate how closely a hypothesized model fits the data in comparison to a “perfect” model (Byrne, 2016). The chi-square statistic is known to be sensitive to larger sample sizes and is thus best evaluated as a ratio of χ2/df. According to Cole (1987), ratios of ≤2 and ≤5 indicate good and acceptable fit, respectively. GFI and AGFI values ≥.95 indicate good fit, and RMSEA and SRMR values ≤.05 indicate good fit (Hu & Bentler, 1995). CFI, TLI, IFI, and AIC are comparative fit indices which evaluate how well the hypothesized model fits the data in comparison to null or alternative models (Byrne, 2016). CFI and TLI values ≥.95, and IFI ≥.90 indicate good fit (Bollen, 1989; Hu & Bentler, 1999). AIC compares the relative fit of different models for a given dataset while balancing model fit and complexity (i.e., number of estimated parameters; Akaike, 1978). Models with lower AIC values are considered to have better relative fit compared to alternative models (Brown, 2015). PNFI is a parsimony-adjusted fit index that assesses how well the hypothesized model fits the data while simultaneously accounting for the model’s complexity (Byrne, 2016). A PNFI value ≥.50 indicates good fit (Schermelleh-Engel et al., 2003).
Results
Participant Characteristics
Detailed sociodemographic characteristics of all participants (N = 486) and their scores on the CSS (Taylor et al., 2020b) are reported elsewhere (Arsenault et al., 2025). The sample had a mean age of 71.62 years (SD = 5.20). A total of 50.4% of participants identified as cisgender female, 46.5% as cisgender male, and 0.6% as non-binary. Table 1 presents descriptive statistics for scores on the GPM–24 (Ferrell et al., 2000) and Everyday Ageism Scale (Allen, Solway, Kirch, Singer, Kullgren et al., 2022). Participants had a mean total score of 28.23 (SD = 26.63) on the GPM–24, reflecting mild pain on average. The mean total score was 11.50 (SD = 5.11) on the Everyday Ageism Scale, indicating relatively low levels of experienced ageism.
Structural Model Fits
To evaluate the hypothesized relationships among pain, ageism, and pandemic-related stress, we conducted a series of SEMs (see Figures 1–4). Table 2 presents a comparison of conventional fit indices across the different models. Among the tested models, SEM 4 demonstrated the best fit with the data, as indicated by multiple conventional fit indices: χ2/df = 3.63, GFI = .924, AGFI = .894, CFI = .945, TLI = .934, IFI = .946, SRMR = .054, RMSEA = .074 [CI .064–.083], PNFI = .764. This model also yielded an AIC of 332.34, which was substantially lower than that of the independence model (AIC = 3738.51). Hypothesized model depicting direct effect of pain on pandemic-related stress. Note. e = error term; DAN = fear of danger; SEC = fear of socioeconomic consequences; XEN = xenophobia; CON = fear of contamination; TSS = traumatic stress symptoms; CHE = compulsive checking and reassurance seeking. Latent variables are shown in ellipses and observed variables are shown in rectangles. Values represent standardized path coefficients. ***p < .001. Hypothesized model depicting direct effect of ageism on pandemic-related stress. Note. e = error term; DAN = fear of danger; SEC = fear of socioeconomic consequences; XEN = xenophobia; CON = fear of contamination; TSS = traumatic stress symptoms; CHE = compulsive checking and reassurance seeking. Latent variables are shown in ellipses and observed variables are shown in rectangles. Values represent standardized path coefficients. ***p < .001. Hypothesized model depicting direct effects of pain and ageism on pandemic-related stress. Note. e = error term; DAN = fear of danger; SEC = fear of socioeconomic consequences; XEN = xenophobia; CON = fear of contamination; TSS = traumatic stress symptoms; CHE = compulsive checking and reassurance seeking. Latent variables are shown in ellipses and observed variables are shown in rectangles. Values represent standardized path coefficients. ***p < .001. Hypothesized final model depicting relationships between pain, ageism, and pandemic-related stress. Note. e = error term; DAN = fear of danger; SEC = fear of socioeconomic consequences; XEN = xenophobia; CON = fear of contamination; TSS = traumatic stress symptoms; CHE = compulsive checking and reassurance seeking. Latent variables are shown in ellipses and observed variables are shown in rectangles. Values represent standardized path coefficients. ***p < .001. Comparison of Fit Indices for Structural Equation Models. Note. SEM = structural equation model; χ2/df = chi-square statistic divided by degrees of freedom; GFI = goodness-of-fit index; AGFI = adjusted goodness-of-fit index; RMSEA = root-mean-squared error of approximation index; SRMR = standardized root-mean-squared residual; CFI = comparative fit index; TLI = Tucker–Lewis index; IFI = incremental fit index; PNFI = parsimony normed fit index; AIC = Akaike Information Criterion.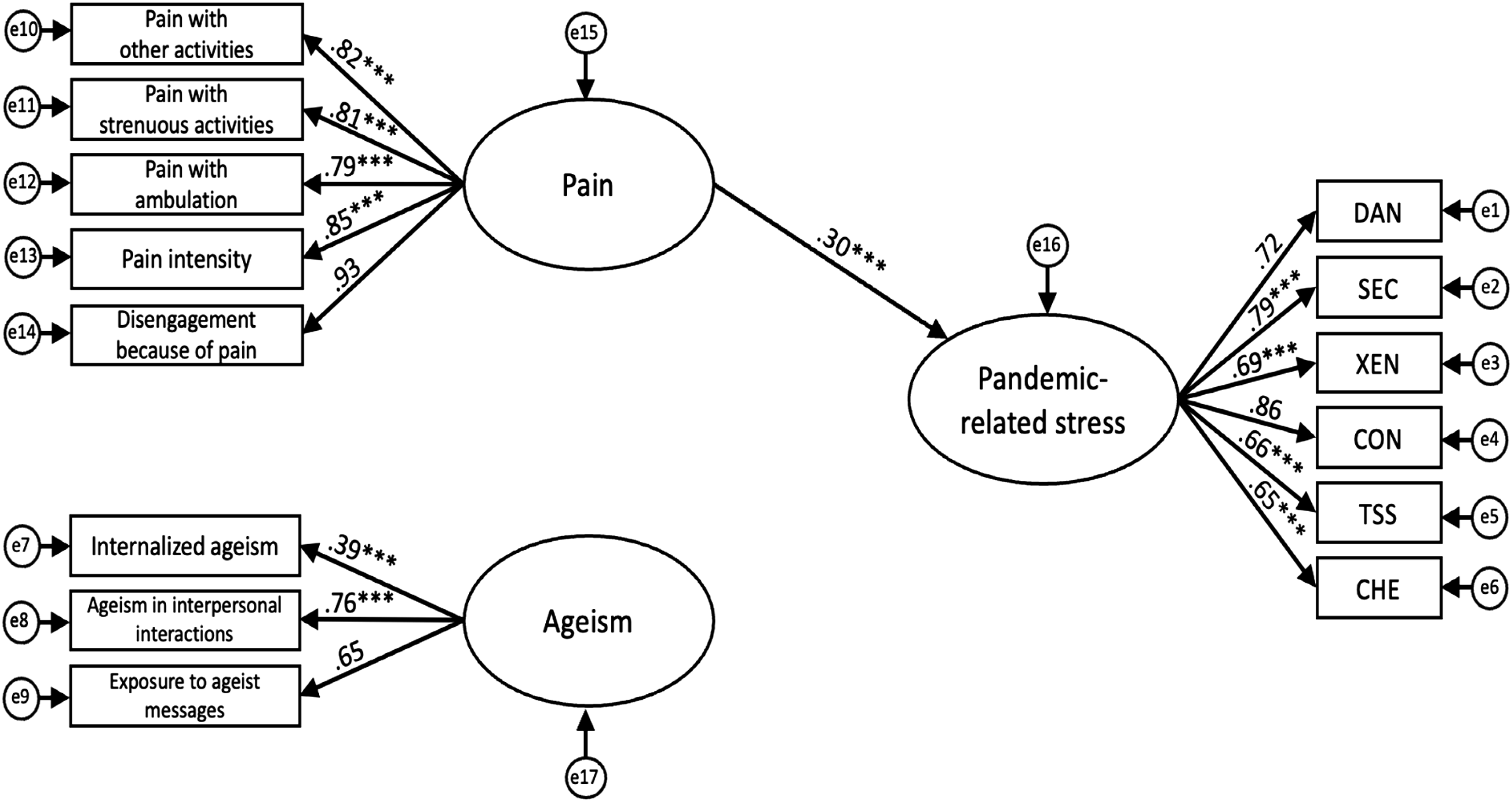
Estimates of Structural Models
The standardized path coefficients for our hypothesized structural models are presented in Figures 1–4. Across all models, factor loadings for the non-fixed observed variables of the latent constructs were statistically significant (refer to Figures 1–4). SEM 1 tested the direct effect of pain on pandemic-related stress, excluding ageism (Figure 1). Consistent with our hypotheses, pain significantly influenced pandemic-related stress, β = .30, p < .001. SEM 2 assessed the direct effect of ageism on pandemic-related stress, excluding pain (Figure 2). As anticipated, ageism also had a significant direct effect, β = .43, p < .001. SEM 3 included both pain and ageism as predictors of pandemic-related stress, without specifying a direct path between them (Figure 3). In this model, the direct effects of pain (β = .18) and ageism (β = .35) on pandemic-related stress were reduced but remained statistically significant (p < .001). Building on SEM 3, SEM 4 introduced a direct path from pain to ageism (Figure 4). This final model revealed that pain significantly predicted ageism, β = .53, p < .001, and in turn, ageism had a significant effect on pandemic-related stress, β
Discussion
To the best of our knowledge, this is the first study to construct and examine hypothetical models exploring how older adults’ experiences of ageism and pain might directly or indirectly impact their levels of pandemic-related stress. Older adults faced increased ageism during the COVID-19 pandemic, including targeted and derogatory social media content, and the widespread characterization of this age group as “vulnerable” (Ayalon, 2020; Lichtenstein, 2021; Peckham et al., 2024). Additionally, older adults reported exacerbations of pre-existing pain (Wang et al., 2024) and pain interference (Hruschak et al., 2021) due to COVID-19. Pre-pandemic research has established that both ageism (Kang & Kim, 2022) and pain (White et al., 2014) are significant predictors of stress in older adults. Our findings expand and provide support for the existing literature by demonstrating how ageism and pain uniquely contribute to older adults’ levels of stress specifically within the context of pandemics.
Direct Influence of Ageism on Pandemic-Related Stress in Older Adults
Across our hypothesized models, ageism was found to have a direct effect on older adults’ levels of pandemic-related stress, even when accounting for the influence of pain. These results are consistent with a growing body of research demonstrating the widespread and detrimental effects of ageism on older adults’ mental and physical health (Chang et al., 2020). In the context of our study, these results may be explained by extensive public health messaging and societal narratives framing older adults as particularly vulnerable to COVID-19 (Aloni & Ayalon, 2023; Peckham et al., 2024), which could have amplified participants’ fears of danger and contamination. Additionally, much of the ageist content in the media suggested that older adults’ lives were less valuable than those of younger individuals (Jimenez-Sotomayor et al., 2020; Skipper & Rose, 2021), reinforcing negative stereotypes and potentially contributing to traumatic stress symptoms measured by the CSS (e.g., nightmares; Taylor et al., 2020b). Taken together, our findings suggest that addressing ageism in future waves of COVID-19 or other global health crises, whether through the delivery of evidence-based interventions or more age-inclusive policies, may help mitigate its negative impacts on older adults’ psychological well-being.
Direct and Mediating Effects of Pain on Pandemic-Related Stress
The pandemic also introduced unique challenges for individuals experiencing pain, with research documenting negative pain-related outcomes in this population following COVID-19 infection (e.g., heightened pain severity, interference with daily activities, reduced pain control; Chatkoff et al., 2022; Hruschak et al., 2021; Pagé et al., 2021). In line with our hypotheses, we found a positive direct relationship between pain and pandemic-related stress in older adults, even after accounting for the influence of ageism as a separate predictor. These findings are consistent with a previous study using the five-factor structure of the CSS (Taylor et al., 2020b), which identified correlations between pain and increased fears of danger and contamination (DANCON) in adults (Asquini et al., 2021). Our results underscore the importance of integrating both psychological and physical health care for the large portion of older adults who experience pain during pandemics. This integrated approach addresses the multifaceted nature of pain and aligns with well-established biopsychosocial models of pain (Gatchel et al., 2014; Hadjistavropoulos et al., 2011).
In our final hypothesized model, a significant indirect pathway emerged in which higher levels of pain were associated with greater experiences of ageism, which in turn contributed to pandemic-related stress. These findings support the interpretation that ageism acts as a mediating mechanism in the relationship between pain and pandemic-related stress, with pain indirectly influencing pandemic-related stress by increasing participants’ perceptions of ageism. We also conducted an analysis to examine whether pain mediated the path from ageism to pandemic-related stress; however, the data did not support this hypothesis. One potential explanation for the finding that pain increases perceived ageism is that healthcare providers who view pain as an inevitable part of aging can be less likely to diagnose and treat pain in older adult patients, reflecting externalized ageist attitudes (Collis & Waterfield, 2015; Gignac et al., 2006). This interpretation also aligns with Stereotype Embodiment Theory (Levy, 2009), which suggests that older adults who are frequently exposed to ageism (e.g., negative age stereotypes and negative self-perceptions of aging) are more likely to internalize and embody these attitudes. Within this framework, it is possible that participants in our study may have internalized ageist stereotypes that frame their pain as inevitable and expected parts of aging (Achterberg, 2019; Collis & Waterfield, 2015). Indeed, one study found that 87% of older adults anticipated experiencing more pain as they age (Sarkisian et al., 2002). Given these findings, educating both healthcare providers and older adults about ageism could be an important strategy for mitigating its negative effects on older adults living with pain.
Limitations
The present study has several limitations that should be acknowledged. First, due to the exclusively online format, our study may have unintentionally excluded individuals living in rural or remote areas without internet access, as well as non-Qualtrics Panels members. The majority of participants (92.8%) self-identified as White, which precluded us from examining race as a potential covariate in our analyses and further limits the generalizability of our findings to racialized older adults. A data collection approach that can engage more diverse subsets of the older adult population, including older adults demonstrating higher levels of pain, will be important for future studies to pursue. This study also relied exclusively on self-report measures, which could have introduced a degree of social desirability bias. Future research would benefit from supplementing the CSS (Taylor et al., 2020b) with clinical interviews or objective behavioral assessments to provide a more comprehensive understanding of pandemic-related stress and its impacts on older adults. Our cross-sectional design also restricts the ability to draw causal inferences. Future investigations would benefit from employing a longitudinal design, as this approach could examine temporal relationships and provide evidence of causality. Data for this study were collected in January 2024, nearly 4 years after the onset of the COVID-19 pandemic. While our focus was on examining pandemic-related stress specifically at the time of data collection, we acknowledge that the generalizability of our findings to older adults’ experiences during earlier waves of the pandemic is uncertain.
Future research in this area may also explore more flexible methodologies, such as directed acyclic graphs. Although more complex and computationally demanding, graphical models offer a powerful means of identifying both direct and indirect relationships, as well as potential causal loops that might not be easily captured through SEM alone. Such an approach could complement the findings from the current investigation. Finally, although the Everyday Ageism Scale (Allen, Solway, Kirch, Singer, Kullgren et al., 2022) demonstrated good reliability in our study, it is a newly developed measure that would benefit from further psychometric evaluation. Future research should assess its reliability and validity across culturally and gender-diverse groups to enhance its generalizability and ensure its applicability in diverse populations.
Conclusion
We aimed to verify the structural relationships among pain, ageism, and pandemic-related stress in older adults. In doing so, our results offer novel insights into how older adults’ experiences of pain and ageism are associated with their psychological responses to pandemics. Specifically, our structural models revealed the significant direct impact of pain and ageism on pandemic-related stress. Additionally, our models demonstrated that ageism mediates the relationship between pain and pandemic-related stress in older adults. Given that pain and ageism are key correlates of pandemic-related stress, they could be targeted in evidence-based interventions aimed at addressing the unique challenges faced by older persons during pandemics. Such interventions could not only help mitigate the disproportionate psychological burden of pandemics on older adults living with pain but also serve as a catalyst for challenging and transforming society’s ageist attitudes toward the treatment and care of older adults during global health emergencies. Future research is encouraged to investigate the model with more diverse populations and examine causal pathways, helping to inform interventions and policies that better address the complex needs of older adults during public health emergencies.
Supplemental Material
Supplemental Material - The Impact of Ageism and Pain on Pandemic-Related Stress in Older Adults: A Structural Equation Modeling and Mediation Analysis
Supplemental Material for The Impact of Ageism and Pain on Pandemic-Related Stress in Older Adults: A Structural Equation Modeling and Mediation Analysis by Kylie A. Arsenault, Ying C. MacNab, Gordon J. G. Asmundson, Thomas Hadjistavropoulos in Journal of Aging and Health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Saskatchewan Health Research Foundation (grant number 2908). KA was also supported by a Social Sciences and Humanities Research Council Canada Graduate Scholarship–Master’s.
Ethical Statement
Data Availability Statement
Data are available from the corresponding author upon reasonable request for a period of 7 years following publication subject to approval from our institutional research ethics board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.