
Abstract
Introduction
Physical Activity (PA) and its links to frailty, quality of life (QoL), and other comorbidities in older Ugandans living with HIV remain under-explored.
Methods
We analyzed data from three annual assessments of older people living with HIV (PLWH) and age- and sex-similar people not living with HIV (PnLWH). We fitted linear generalized estimating equations (GEE) regression models to estimate the correlates of PA, including demographics, frailty, QoL, HIV, and other comorbidities.
Results
We enrolled 297 PLWH and 302 PnLWH. Older age (b = −157.34, 95% CI [-222.84, −91.83]), living with HIV (b = −979.88 [95% CI: −1878.48, −81.28]), frailty (b = −3011.14 [95% CI: −4665.84, −1356.45]), and comorbidities (b = −2501.75 [95% CI: −3357.44, −1646.07]) were associated with lower overall PA. Higher general QoL (b = 89.96 [95% CI: 40.99, 138.94]) was associated with higher PA.
Conclusion
PA interventions may support wellbeing of older people in the region, and tailored interventions should be explored.
Introduction
Engaging in physical activity (PA) brings numerous positive health benefits for older adults, and has been linked to reduced comorbidities associated with aging, such as cardiovascular diseases, cancers, worsened mental health, and cognitive problems. (L. Cheng et al., 2021; Erlandson et al., 2018; Reiner et al., 2013) Additionally, higher levels of PA have been associated with markers of positive aging, such as favorable lipid profiles, improved bone density, and reduced falls. (Vogel et al., 2009) However, extant research on the benefits of PA among older people has primarily been generated from the Global North.
Sub-Saharan Africa is expected to have the fastest growth in older adults globally by 2050 (Velkoff & Kowal, 2006) and is home to nearly 4 million people living with HIV (PLWH) aged 50 or older. Uganda in particular, reported that those aged 45–59 had the highest HIV prevalence of any age group in 2016 (Sherwood-Martin, 2023). Though the widespread scale-up of antiretroviral therapy (ART) has prolonged life expectancy, PLWH are at an increased risk of experiencing multiple poor health indicators associated with aging that have been shown to benefit from PA in the Global North, including frailty, depression, and diminished quality of life (QoL) (Dianatinasab et al., 2020; Heissel et al., 2019). Among older PLWH, PA is also associated with lowering abdominal adiposity, improving walking capacity and visuospatial ability, and improving physical and mental function (Chetty et al., 2021; Shim & Noh, 2022; Webel et al., 2023; Winston et al., 2021). As the population of PLWH ages in the Global South, scalable strategies to help augment QoL are an urgent priority (Siedner, 2019).
However, it is important to consider possible contextual differences in PA between the Global South and Global North. In the Global South, most PA is done for work or travel, not for recreational purposes, and resulting in very high activity levels (Guthold et al., 2011; Guwatudde et al., 2016). While high PA is generally associated with health benefits, excessive PA—particularly in occupational settings—has been shown to have negative health outcomes in other the Global North. (Kim et al., 2012; Li et al., 2013; Paluska & Schwenk, 2000) Whether or not a similar pattern exists among PLWH and people not living with HIV (PnLWH) residing in Uganda remains unexplored.
To address the gap in knowledge about PA among older PLWH in Uganda, we examined long-term trends in PA, frailty, QoL, comorbidities, and depression in a cohort of older PLWH and PnLWH. We hypothesized that PA would be lower among PLWH than PnLWH and that frailty, low QoL, comorbidities, and depression would be associated with lower levels of PA.
Methods
Study Sample and Data Collection
We analyzed three annual waves of data from the Quality of Life and Aging with HIV in Rural Uganda Study, described in detail previously (Siedner, 2019). Briefly, we first recruited individuals over 50 years old, living with HIV, and on ART for at least three years from one of two public health clinics in Uganda. We then used household census data to recruit PnLWH from the same communities matched on age (within quartiles), sex, and clinic catchment area (Takada et al., 2019). The first wave of the study occurred remotely, as it was during the COVID-19 pandemic lockdown (2020), with subsequent data collection occurring in person, annually in 2021 and 2022.
Outcome Measures
Our outcome of interest was PA, which we measured using a modified International Physical Activity Scale (Lee et al., 2011). It was adapted to the Ugandan context, where activities that would be undertaken in this population were added to the questionnaire. (Mabweazara et al., 2023) This scale assesses self-reported physical activity over the past seven days, characterized by both intensity (i.e., low, moderate, and vigorous) and duration in minutes per week. These values are then converted into metabolic equivalents of task (METs), with one MET equal to the amount of oxygen consumed while sitting at rest (3.5 mL O2 per kg body weight times minutes) (Jetté et al., 1990). One minute of vigorous activity is converted into 8.0 METs; 1 minute of moderate activity was defined at 4.0 METs; 1 minute of walking was defined at 3.3 METs. (Haskell et al., 2007) For our primary outcome of interest, we considered METs as a continuous measure.
Exposure Measures
Our primary independent variable was HIV status. As described above, PLWH were enrolled directly from clinic. Individuals without HIV were tested annually to confirm their status prior to each study visit. Health-related QoL was measured using the EQ5D visual analogue scale (EQ-VAS), which asks respondents to report their current health on a scale of 0–100 and has been used previously in this population (Cheng et al., 2021; Olivieri-Mui et al., 2023; Quach et al., 2023; Rautenberg et al., 2023a, 2023b; Stanton et al., 2024). We also assessed age-related QoL using the Control, Autonomy, Self-Realization and Pleasure (CASP19) scale (Hyde et al., 2003). This scale asks participants four to five questions in each section (Control, Autonomy, Self-realization, or Pleasure), with a total of 19 items and a total possible score of 57. Frailty was measured using the Fried Frailty phenotype as described previously (Fried et al., 2001). Comorbidities were assessed by self-report, and included the following conditions: high blood pressure, diabetes, high cholesterol, heart attack or heart failure, kidney problems, stroke, cancer, chronic obstructive pulmonary disease (COPD), asthma, pneumonia, and tuberculosis.
Additional covariates of interest included: age, sex, marital status, income, employment, household asset ownership (Filmer & Pritchett, 2001), moderate to severe alcohol use, depressive symptoms, and body mass index. Alcohol consumption was measured using the 3-item consumption subset of the Alcohol Use Disorders Identification Test (AUDIT-C) (Bush et al., 1998) and was classified as low versus moderate to severe risk per standard cutoffs. Depressive symptoms were measured using a version of the depression subscale of the Hopkins Symptom Checklist (Derogatis et al., 1974) modified for the Ugandan context, (Bolton & Ndogoni, 2001; Mushavi et al., 2020) with probable depression defined as a score >1.75 (Ashaba et al., 2018). BMI was calculated based on height and weight, measured by study staff at the second visit.
Ethical Considerations
All study participants provided informed verbal consent over the phone during the first year of data collection, and written consent for subsequent waves. Study procedures were reviewed and approved by the institutional review committees at Mbarara University of Science and Technology and Mass General Brigham. The study also received clearance to conduct the study from the Uganda National Council for Science and Technology and the Research Secretariat in the President’s Office.
Analysis
Descriptive statistics were tabulated by HIV status and were compared using chi-squared tests, t-tests, or Wilcoxon Rank-Sum tests as appropriate. Longitudinal linear generalized estimating equations (GEE) regression models were fitted to the data with total number of METs per week as a continuous outcome. The preliminary model included age (continuous), HIV status (binary), EQ-VAS score (continuous), CASP19 score (continuous), depression (binary) frailty status (categorical, with robust, pre-frail, or frail as options), the presence of comorbidities (binary), and visit number (categorical). Interaction terms between HIV status x visit and frailty status x visit were also considered to determine if the relationship between HIV status or frailty and PA changed over time. Variables were retained in the final model if they were statistically significant (p
Results
Descriptive Statistics of Cohort at Baseline by HIV Status.
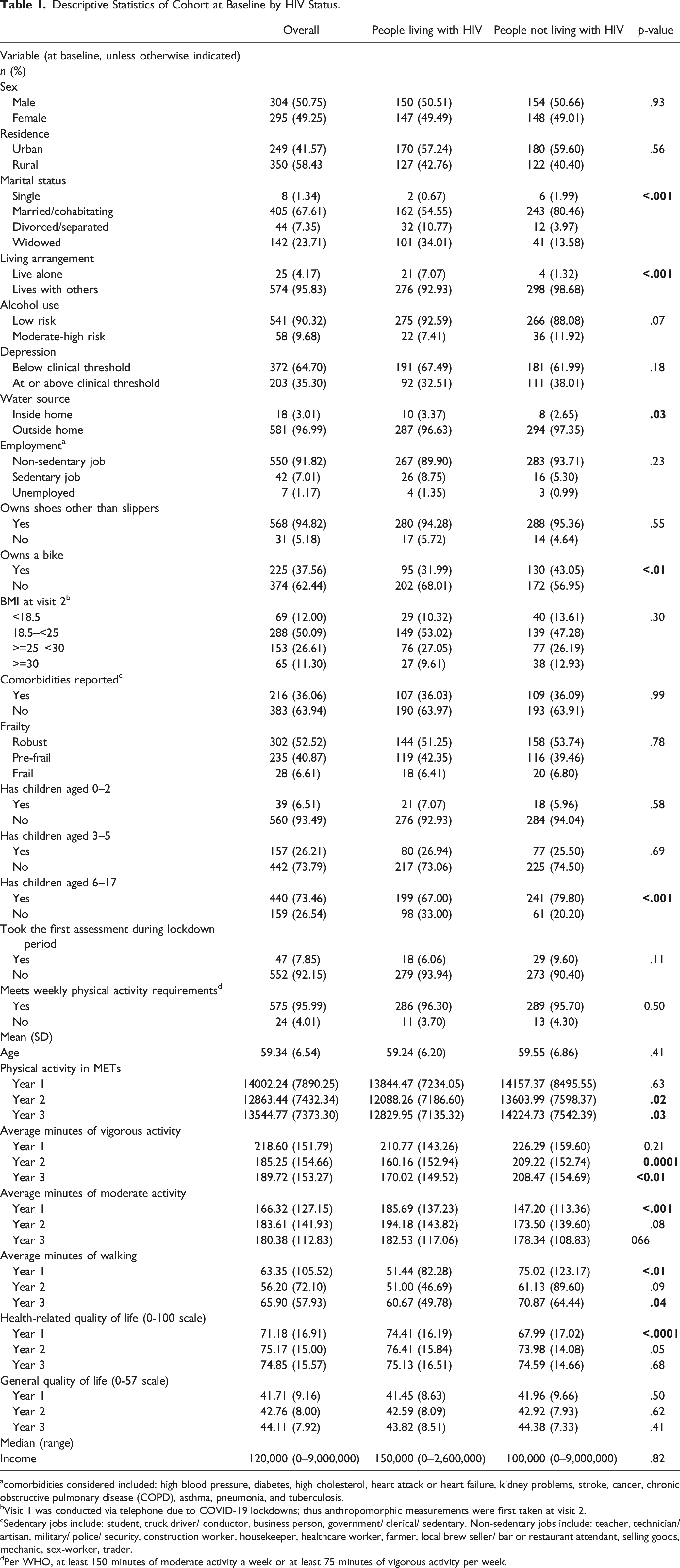
acomorbidities considered included: high blood pressure, diabetes, high cholesterol, heart attack or heart failure, kidney problems, stroke, cancer, chronic obstructive pulmonary disease (COPD), asthma, pneumonia, and tuberculosis.
bVisit 1 was conducted via telephone due to COVID-19 lockdowns; thus anthropomorphic measurements were first taken at visit 2.
cSedentary jobs include: student, truck driver/ conductor, business person, government/ clerical/ sedentary. Non-sedentary jobs include: teacher, technician/ artisan, military/ police/ security, construction worker, housekeeper, healthcare worker, farmer, local brew seller/ bar or restaurant attendant, selling goods, mechanic, sex-worker, trader.
dPer WHO, at least 150 minutes of moderate activity a week or at least 75 minutes of vigorous activity per week.
Correlates of PA Throughout the Study
The median weekly METs was 14002.24 (standard deviation [SD] 7890.25) at baseline for the entire cohort. Those living with HIV had lower mean weekly PA output in terms of METs in years 2 (PLWH: 13844.47 [SD: 7234.05], PnLWH: 14157.37 [SD: 8495.55], p = .02) and 3 of the study, (PLWH: 12829.95 [SD: 7135.32], PnLWH: 14224.73 [SD: 7542.39], p = .025). Additionally, those living with HIV reported fewer mean daily minutes of vigorous activity in year 2 (PLWH: 160.16 [SD: 152.94]; PnLWH: 209.22 [SD: 152.74], p = .0001) and year 3 (PLWH: 170.02 [SD: 149.52]; PnLWH: 208.47 [SD: 154.69], p < .01), and fewer mean daily minutes of walking in year 1 (PLWH: 51.44 [SD:82.28]; PnLWH: 75.02 [SD: 123.17], p < .01) and year 3 (PLWH:60.67 [SD: 49.78], PnLWH: 70.87 [SD:64.44], p = .046). Those living with HIV reported more mean daily minutes of moderate activity during year 1 of the study (PLWH: 185.69 [SD: 137.23], PnLWH: 147.20 [113.36], p < .0012).
Changes in PA Over Time
Trends in Physical Activity Throughout Study Period.
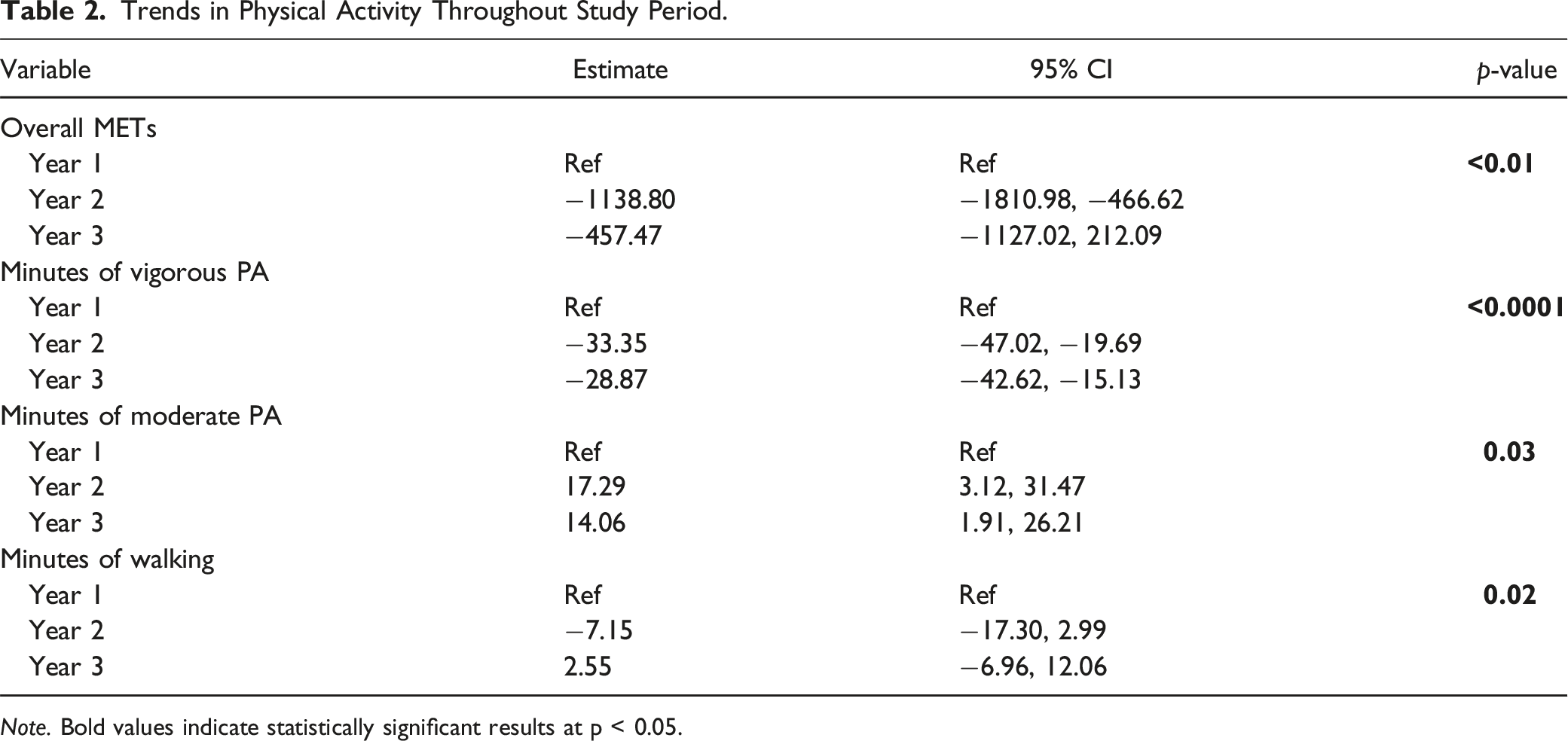
Note. Bold values indicate statistically significant results at p < 0.05.
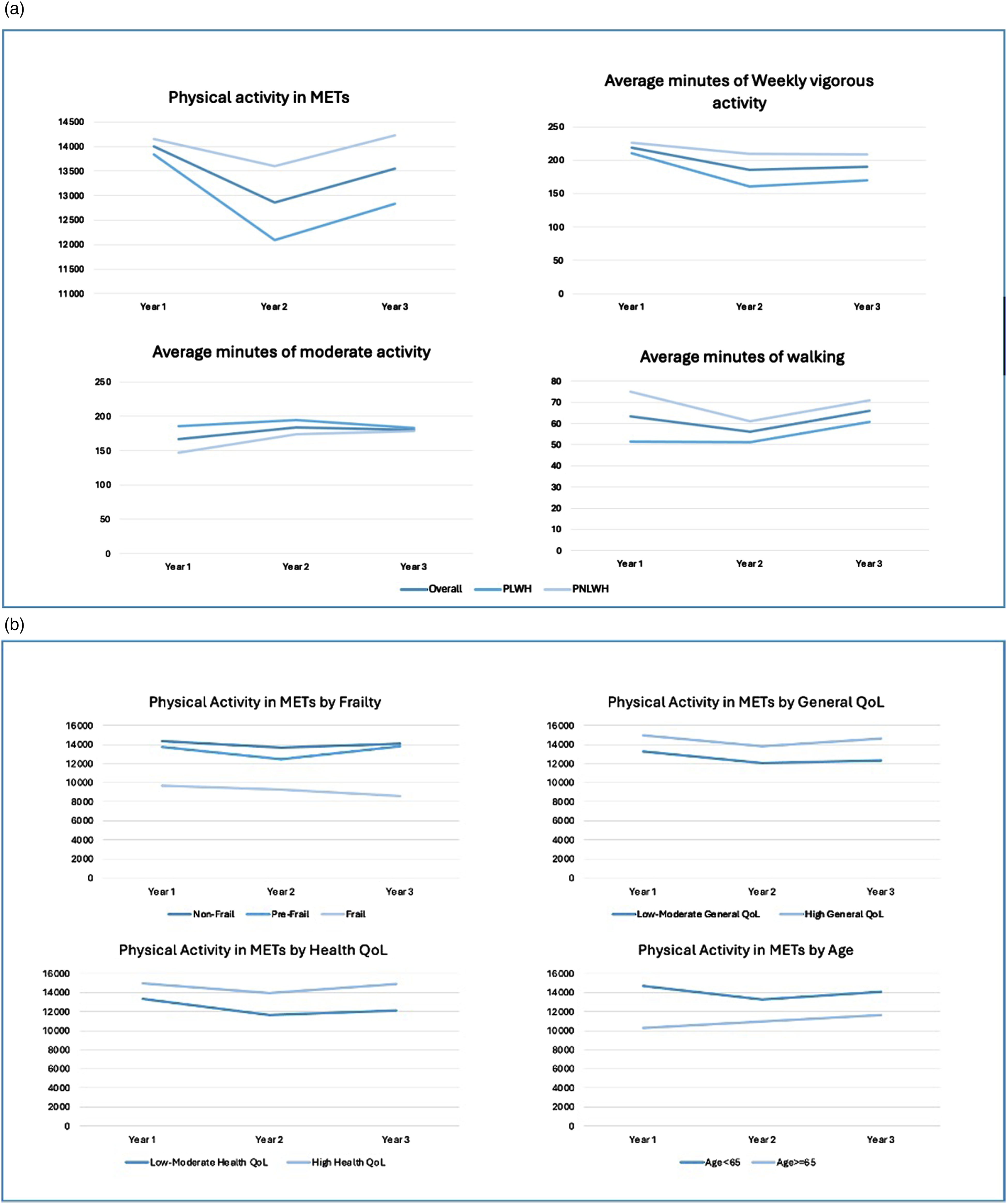
(a) Trends in activity type by HIV status and study year (b) Trends in activity type by frailty, QoL, age, and study year. Caption: The figure demonstrates changes in types of PA throughout the study and changes in overall PA by frailty status, general QoL, health-related QoL, and age. Overall, vigorous PA and walking declined in year two and rebounded in year three; moderate PA, though was highest in year 2. Among nearly all groups and PA declined in year 2 and rebounded in year 3.
Correlates of PA
GEE Model With METs per Week as Continuous Outcome.
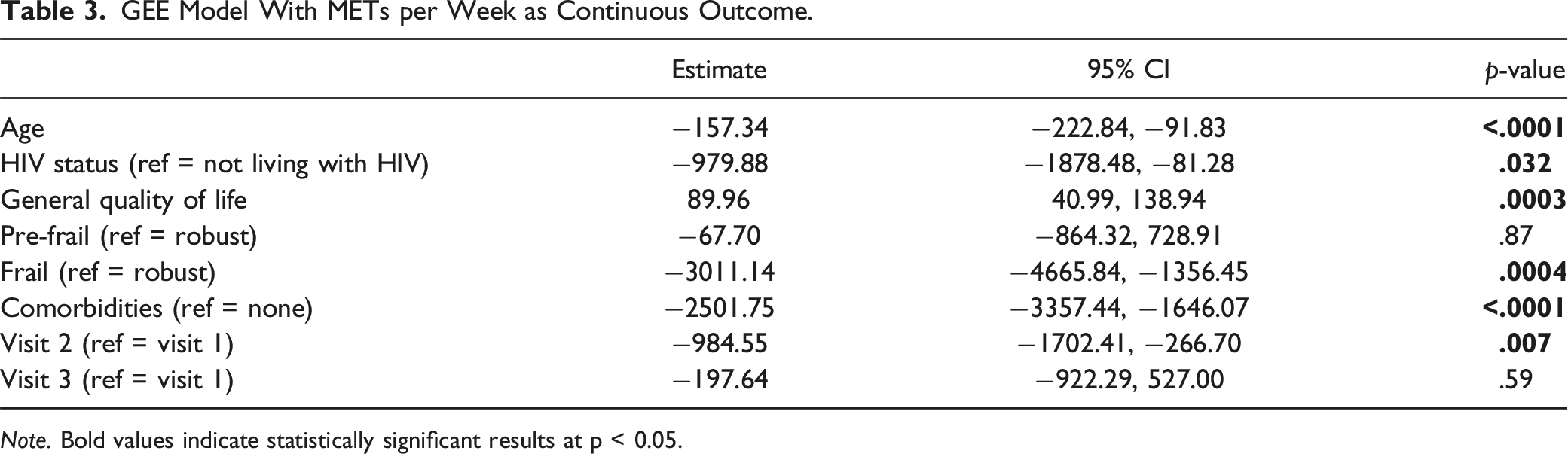
Note. Bold values indicate statistically significant results at p < 0.05.
Discussion
In this well-characterized 3-year cohort study of older age people in rural Uganda, our findings revealed that older PLWH were less likely than their counterparts without HIV to engage in PA. We also identified key health and well-being indicators associated with PA levels. Most notably, individuals with comorbidities and frailty were significantly less likely to engage in PA.
Our data underscores the potential for PA interventions to promote healthy aging, including for PLWH on ART. For example, we found that those reporting comorbidities—of which the most prevalent conditions were high blood pressure (21%), high cholesterol (7%), and diabetes (6%)—reported reduced PA. We similarly found reduced PA levels among PLWH and those with the frailty phenotype. These findings demonstrate that the groups who might benefit the most from PA are less likely to engage in optimal levels (Angulo et al., 2020; Colberg et al., 2016; Mann et al., 2014; Rêgo et al., 2019; Xu et al., 2023). We cannot precisely determine whether reduced PA is contributing to these co-morbidities, or vice versa, where comorbidities and frailty may have emerged from reduced levels of PA earlier in life, or where individuals may have reduced their rates of PA in response to these conditions. In either instance, though, programs to help encourage PA for those who might most benefit from it should be considered for development and evaluation in such settings. Although few if any programs are active at scale, there are numerous pilot programs of PA interventions among PLWH, which may be adapted to this specific context and sub-populations.
Additionally, our findings highlight that PA declines with age, which is consistent with other studies (Milanović et al., 2013). In this study, PA declined in year two compared to year one, it did not decline in year three compared to year one. This may be due to the timing of the study, with year one beginning in October 2020. Previous assessments in this cohort have demonstrated that individuals expanded their farming in response to the pandemic during the first year of the study. (Olivieri-Mui et al., 2023) The high levels of PA at baseline may be due to increased farming activities, and decline in PA in year two of the study may represent individuals returning to baseline farming trends. Additionally, though the study dates did not overlap with COVID-19 restrictions in the regions where the study participants resided, the high levels of COVID-19 spread in April and May of 2021 due to the Delta variant may have decreased outdoor activity, and thus PA levels, in year two.
As demonstrated in studies from elsewhere in the world, increased PA was associated with better general QoL in both PLWH and PnLWH enrolled in this study (Bize et al., 2007; Rejeski & Mihalko, 2001). This evidence from older people in Uganda adds to the potential benefits of PA-promoting interventions, including for PLWH who are on ART long term.
We found generally high levels of PA reported by this cohort. Approximately 96% of the present cohort met World Health Organization PA recommendations compared to 8%–44% in cohorts of similar age from the United States and Europe (Keadle et al., 2016; Kruger et al., 2007). We hypothesized that generally high levels of PA are driven by contextual factors that encourage or require PA among the study population. For example, most participants reported not having a water source within their homes and the majority were also employed in non-sedentary jobs, such as agriculture or construction. This is consistent with literature demonstrating higher levels of PA in agrarian societies and lower-income settings where subsistence farming remains common, and the impact of the built environment on PA levels in sub-Saharan Africa. (Asai et al., 2018; Guwatudde et al., 2016; Kolbe-Alexander et al., 2015; Racine et al., 2012) By contrast, in high-income countries, where the majority of PA is recreational in nature, far higher levels of inactivity are reported in low-income groups (Guthold et al., 2011; Watson et al., 2016) than were seen in the present study.
There were several strengths and limitations of the current analysis. Strengths include longitudinal observation with a relatively large sample direct measurement of frailty via physical tests (such as gait speed and grip strength), data missingness was rare and longitudinal retention as high, with approximately 95% of individuals retained for all three years of observation. A major limitation was the use of self-reported measures for PA, which are known to over-estimate PA compared to direct measurement with pedometers. (Prince et al., 2008) Nonetheless, we have no reason to suspect that measurement bias interacted with HIV serostatus, and the strong association between PA, frailty, age, and measurements of sedentary lifestyle, such as unemployment, offers some measure of internal validity. As with all observational studies there is potential for confounding, which may have occurred if unmeasured factors related to both HIV (or other co-morbidities) and PA explain the relationship between both variables. Finally, our cohort is comprised mainly of rural and peri-urban individuals from an agrarian society, so generalizability should be considered within this context.
In conclusion, our results demonstrate relatively high levels of PA in rural Uganda, but that individuals living with HIV and those with age-related health difficulties, such as frailty and comorbidities, are less likely to continue to engage in PA, despite its known benefits. In future work, contextually relevant PA interventions could be developed and tested among older people and PLWH who do not meet the WHO recommendations. However, ensuring that optimal levels of PA are maintained in this population, including minimizing excessive PA, is important to the maintenance of overall health. Moreover, HIV program developers and public health practitioners could consider the role for PA for health promotion among these groups in the region.
Footnotes
Acknowledgments
We would like to thank the research participants in Uganda and the study team from Mbarara and Kabwohe in Uganda, and the Medical Practice Evaluation Center in the US for making this work possible.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ACT reports receiving a financial honorarium from Elsevier, Inc for his work as Co-Editor in Chief of the Elsevier-owned journal SSM-Mental Health. MLG reports past grant funding from Gilead Sciences, Inc, which ended in December 2022. The other authors declare no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (K24DA061696-01), National Institute on Aging (R01AG059504), National Heart, Lung, and Blood Institute (K24HL166024), National Heart, Lung, and Blood Institute (R01HL141053).