
Abstract
Objectives
The study investigated the health status of older migrants relative to their New Zealand-born peers. We adopted a holistic view of health (physical, mental, and social) and a structural approach to health disparities based on migrant status and socioeconomic position.
Methods
Using case–control matching based on age, gender, and education, the health status of 357 older migrants and 357 New Zealand-born older adults was compared.
Results
Older migrants reported significantly poorer social health. Health inequities were patterned by socioeconomic status. Working class older migrants had significantly poorer physical, mental, and social health than their New Zealand-born peers. Inequities in social wellbeing persisted even at the upper end of the social gradient.
Discussion
Migrant background is an important social determinant of health in older age. The reduced social wellbeing of economically advantaged migrants highlights vulnerabilities regardless of socioeconomic position and the need for targeted social policies.
Keywords
Introduction
Despite numerous social, economic, and cultural challenges accompanying immigration, research consistently shows that upon arrival to a new country immigrants have a significant advantage over the native-born population in many health indicators, including life expectancy, physical and psychological functioning, life satisfaction, and rates of non-communicable disease (Jatrana et al., 2018b; Markides & Rote, 2019; Ruiz et al., 2016; Vang et al., 2017). This phenomenon has become known as the immigrant paradox or the healthy immigrant effect (Markides & Coreil, 1986). While existing literature has predominantly focused on the superior health of Hispanic immigrants in the United States, similar effects have been documented in Canada, Australia, Aotearoa New Zealand, and many European countries (Hajat et al., 2010; Kennedy et al., 2015; Markides & Rote, 2019; Teruya & Bazargan-Hejazi, 2013; Vang et al., 2017).
Importantly, this initial health advantage seems to diminish over time. By the time immigrants reach later life, they often fare worse in health outcomes compared to their age-related native-born peers, including self-reported mental health (Elshahat et al., 2022; Ladin & Reinhold, 2013; Vang et al., 2017), quality of life (Nesterko et al., 2013; Sand & Gruber, 2018), rates of morbidity (Markides & Rote, 2019; Pasupuleti et al., 2016) and obesity (Alidu & Grunfeld, 2018), and healthy life expectancy (Boen & Hummer, 2019; Reus-Pons et al., 2017). These differences seem to remain significant even when controlling for age, country of origin, race or ethnicity, gender, marital status, educational attainment, and socioeconomic status (Pasupuleti et al., 2016; Sand & Gruber, 2018).
To explain what contributes to migrants’ negative health transition as they spend more time in the host country, much of the literature has focused on negative acculturation, positing that the more time immigrants spend in the host country, the more likely they adopt unhealthy behaviours and lifestyle choices of the native-born population (Alidu & Grunfeld, 2018). These include, but are not limited to, lower levels of physical activity (Teruya & Bazargan-Hejazi, 2013), increased alcohol consumption (Juárez et al., 2022), and reduced fruit and vegetable consumption (Lee et al., 2013; Popovic-Lipovac & Strasser, 2015). The validity of these findings, however, has been questioned because of the diverse range of definitions and measures of acculturation used across studies (Teruya & Bazargan-Hejazi, 2013). Furthermore, acculturation research has been criticized for predominantly focusing on individual level factors and failing to account for critical social, economic, and environmental determinants of health (Szabó, 2022).
Given these shortcomings, there has been a shift towards a structural framework, also known as the social determinants of health, which contends that social and environmental factors, such as socioeconomic status, working conditions, access to health care services, and discrimination, contribute to and perpetuate health inequities (Marmot et al., 2008). While the available evidence is still relatively limited, studies have found that differences between immigrants and native-born populations are partially explained by such conditions. For instance, it has been shown that labour migrants, those of lower socioeconomic position, and migrants who have experienced discrimination are more likely to experience poorer health outcomes (Boen & Hummer, 2019; Popovic-Lipovac & Strasser, 2015; Teruya & Bazargan-Hejazi, 2013). Studies also highlight the accumulative effects of exposure to one or multiple of these factors (Boen & Hummer, 2019; Jatrana, Pasupuleti, et al., 2014b; Jatrana et al., 2018b; Lee et al., 2013).
The Healthy Immigrant Effect in Aotearoa New Zealand
Aotearoa New Zealand is a culturally diverse society with 27% of the total population born overseas and immigration being one of the primary sources of population growth (Statistics New Zealand, 2020b). The older adult population, that is, people aged 65 years or older, is similarly culturally diverse. According to the latest census data, 28% of older adults were born outside of Aotearoa New Zealand. The most common birthplaces in this age group are the United Kingdom and Ireland (43%), Asia (19%), the Pacific Islands (11.4%), Continental Europe (9.5%), the Middle East and Africa (5%), Australia (4.9%), and North America (2.6%). Although most older migrants (73.5%) have been living in Aotearoa New Zealand for over 20 years, there are large differences in length of stay across groups. Older adults from Asia (48.8%) and the Middle East and Africa (53.1%) are more likely to be recent migrants, residing in the country for less than 20 years (Statistics New Zealand, 2020a).
Although the healthy immigrant effect has not been studied extensively in Aotearoa New Zealand, there is evidence for some immigrant groups arriving with a health advantage. Using mortality data from the New Zealand census between 1996 and 2004, Hajat et al. (2010) found a mortality advantage for European and Asian immigrants aged 18 to 74 compared to their New Zealand-born counterparts of the same ethnic group. In line with findings from the international literature, this advantage seemed to diminish with longer length of residence. For immigrants from the Pacific, however, there was no mortality advantage evident in the data. More recently, Jatrana et al. (2014a) reported similar findings, such that Asian immigrants had both an all-cause and cause-specific mortality advantage over their same-ethnic, New Zealand-born peers. While all-cause mortality advantage reduced with increasing length of residence, some immigrant groups (e.g. Indians) maintained a cancer-specific mortality advantage over time. In a follow-up study, Jatrana et al. (2018a) highlighted socioeconomic disparities in household income, education, and neighbourhood deprivation as key factors associated with changes in mortality across groups.
Research examining the healthy immigrant effect in other indicators of health in Aotearoa New Zealand has been scarce. Apart from a study by Kokaua et al. (2009) demonstrating a lower prevalence of mental disorders among adult migrants from the Pacific compared to their New Zealand-born peers and those who migrated as young children, there has been virtually no research comparing mental health outcomes between immigrants and New Zealand-born adults (Elshahat et al., 2022). With respect to physical health and chronic conditions, Baker et al.’s (2019) prospective study of disability post-injury found a lower prevalence of multiple chronic conditions and disability pre-injury among immigrants, compared to New Zealand-born adults aged 18–64, providing some evidence for the healthy immigrant effect.
The Present Study
In addition to the general lack of research investigating the health of the immigrant population in Aotearoa New Zealand, the few studies available have either excluded older adults from the analyses or capped the age range at 74, which means our understanding of the health status of immigrants in older age in Aotearoa New Zealand is very limited. To that end, the primary objective of the present study was to compare the health of older immigrants in Aotearoa New Zealand to their New Zealand-born peers. When determining the comparison sample, we considered systemic health inequities based on ethnicity in the Aotearoa New Zealand context. As a result of colonization, Māori, the indigenous people of Aotearoa New Zealand, continue to experience pervasive health disparities compared to non-Māori (Hobbs et al., 2019). Consequently, the health status of older immigrants was assessed against the health status of non-Māori, New Zealand-born older adults of the same age, gender, and education.
Health was assessed holistically, incorporating aspects of physical, mental, and social wellbeing (World Health Organization, 1948). Based on previous findings related to the diminishing health advantage of immigrants over time, we expected to find older migrants to be in similar or worse health than their New Zealand-born peers. Further, as increasing research draws attention to socioeconomic conditions as potential drivers of health disparities between immigrant and the native-born population over time, we adopted a structural view, probing differences in health between older immigrants and their New Zealand-born peers based on socioeconomic position. Specifically, we expected health to be worse for people at the lower end of the socioeconomic gradient and health disparities to be larger for older migrants.
Method
Design and Participants
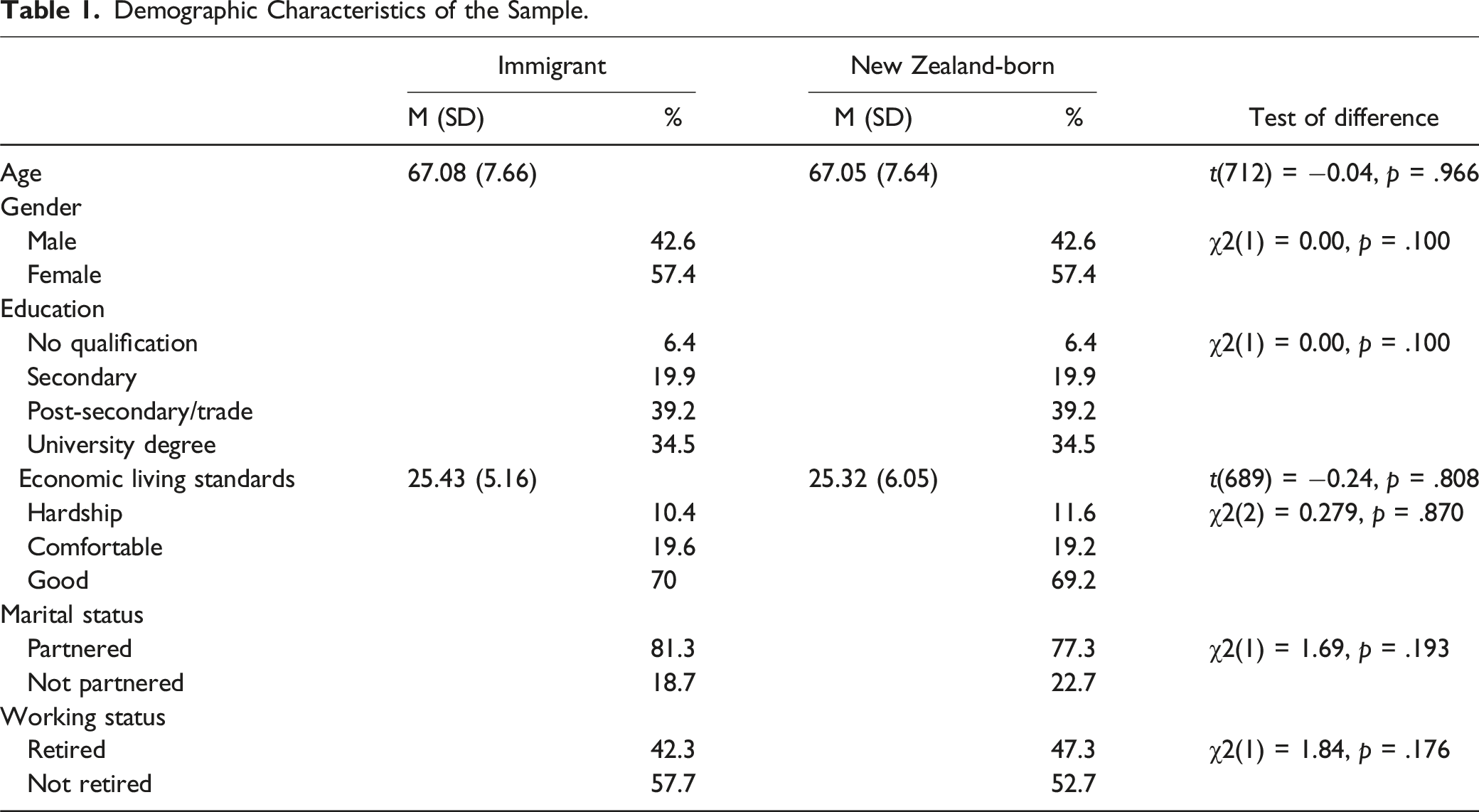
Demographic Characteristics of the Sample.
Measures
Control Variables
Gender (0 = male, 1 = female), marital status (0 = not married or in de facto relationship, 1 = married or in de facto relationship), retirement status (0 = not retired, 1 = retired), and education (0 = secondary education or lower, 1 = post-secondary education) were used as demographic control variables.
New Zealand-Born versus Migrant Background
Migrant background was operationalized as being born outside of Aotearoa New Zealand and immigrating to Aotearoa New Zealand after the age of 18. The variable was coded as 0 = migrant/not born in Aotearoa New Zealand and 1 = New Zealand-born.
Socioeconomic Status
The Short-form Economic Living Standards Index (ELSI-SF) was used to assess socioeconomic status (Jensen et al., 2005). The ELSI-SF is a non-monetary measure of socioeconomic status, which was specifically developed for the Aotearoa New Zealand context. It assesses financial restrictions in social participation (e.g. not being able to visit the hairdresser once every 3 months because of cost) and living conditions (e.g. not having electricity because of cost), economizing behaviours (e.g. not picking up prescriptions because of cost), financial problems (e.g. inability to pay for accommodation or utilities), overall satisfaction with living standards, and self-reported adequacy of income. A total score is created by summing all 25 items (range: 0–31), with higher scores indicating better economic living standards. As per recommendations by Jensen et al. (2005), the total score can be further divided into levels reflecting levels of hardship (range: 0–16), levels of comfortable (range: 17–24), and levels of good (range: 25–31) living standards.
Self-Rated Mental and Physical Health
The Optum™ SF-12v2® Health Survey was used to assess self-rated physical and mental health (Ware et al., 2008). Physical and mental health components were calculated based on normative scores for the Aotearoa New Zealand population derived from the 2008 New Zealand General Social Survey and the 2006–2007 New Zealand Health Survey (Frieling et al., 2013).
Symptoms of Depression and Anxiety
Depression symptoms were assessed with the 10-item Center for Epidemiological Studies Depression scale (CESD-10; Andresen et al., 1994). Participants were asked to rate how often they had experienced symptoms, such as ‘I could not get going’, in the previous week on a four-point scale (1 = rarely or never and 4 = mostly or always). A total score is created by summing all item scores (range: 10–40). The scale yielded acceptable reliability of α = 85. Anxiety symptoms were assessed with the 5-item Geriatric Anxiety Inventory (GAI-SF Byrne & Pachana, 2011). Participants indicated their agreement or disagreement with items, such as ‘I worry a lot of the time’. A total score is created by summing all item scores (range: 0–5). The scale yielded acceptable reliability of α = .84.
Social Provisions
The Social Provisions Scale (SPS) was used to assess participants’ access to and capacity to provide social support (Cutrona & Russell, 1983). The scale has 24 items covering six dimensions of relational provisions: attachment, social integration, reassurance of worth, reliable alliance, guidance, and opportunity for nurturance. Agreements with items, such as ‘There is someone I could talk to about important decisions in my life’, are rated on a 4-point scale (1 = strongly disagree to 4 = strongly agree) and are combined into a summary score (range: 24–96). The scale yielded acceptable reliability of α = .93.
Loneliness
The short-form, 6-item De Jong Gierveld Loneliness Scale was used to measure social and emotional aspects of loneliness (De Jong Gierveld & Van Tilburg, 2006). Participants were asked to rate the extent to which items, such as ‘I experience a general sense of emptiness’ (emotional loneliness) and ‘There are enough people I feel close to’ (social loneliness), applied to the way they felt using a 3-point scale (1 = no, 2 = more or less, and 3 = yes). Social loneliness items are reverse scored. Responses of ‘more or less’ and ‘yes’ receive a score of ‘1’, and ‘no’ responses receive a score of ‘0’. A summary score is derived for emotional (range: 0–3) and social (range: 0–3) loneliness, with higher scores indicating greater loneliness. Both subscales yielded acceptable reliability (emotional: α = .63; social: α = .84).
Data Analysis
Case–control matching was conducted in SPSS using random matching based on gender and education, and a fuzz factor of 1 was allowed for age. After random matching was completed, differences between the two samples were examined using an independent samples t-test for age and chi-square tests for gender and education. Next, bivariate correlations were calculated among the study variables to test the interrelatedness of the self-reported health measures as well as the associations of length of residence and age with self-reported health outcomes. Hypotheses were tested with path analysis in Mplus8 using robust maximum likelihood estimation. The primary analysis examined the predictive effects of migrant background on self-reported health outcomes, while controlling for demographic variables, including age, gender, education, marital status, retirement status, and economic living standards. Next, analyses were stratified by socioeconomic position.
Results
Correlations Among Study Variables by Sample.
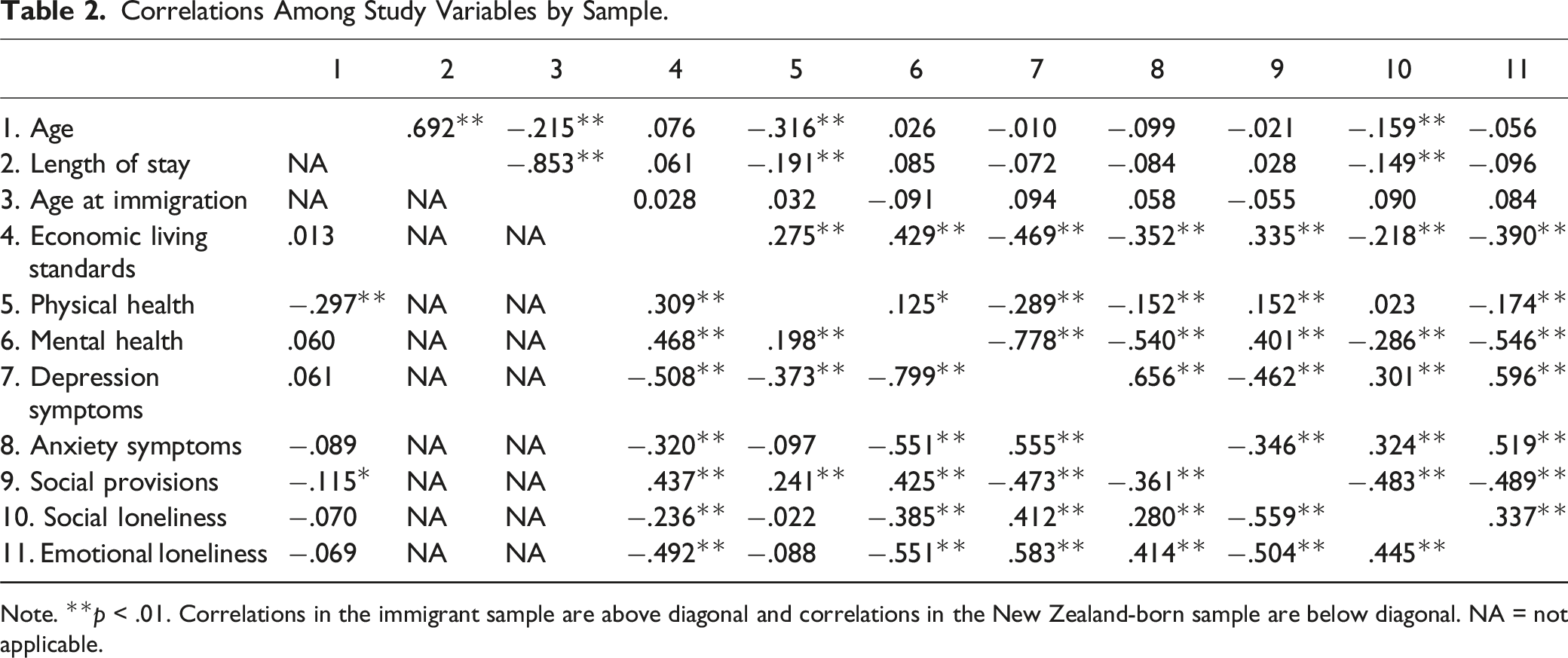
Note. **p < .01. Correlations in the immigrant sample are above diagonal and correlations in the New Zealand-born sample are below diagonal. NA = not applicable.
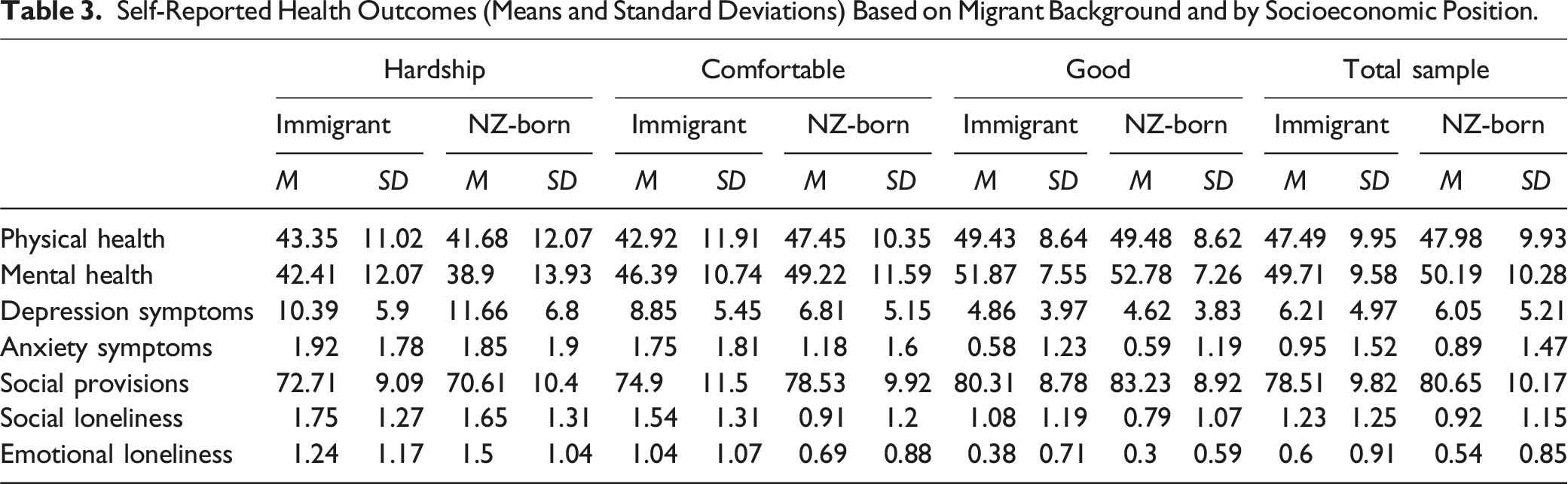
Self-Reported Health Outcomes (Means and Standard Deviations) Based on Migrant Background and by Socioeconomic Position.
Prediction of Health Outcomes in the Total Sample and Stratified by Socioeconomic Position.
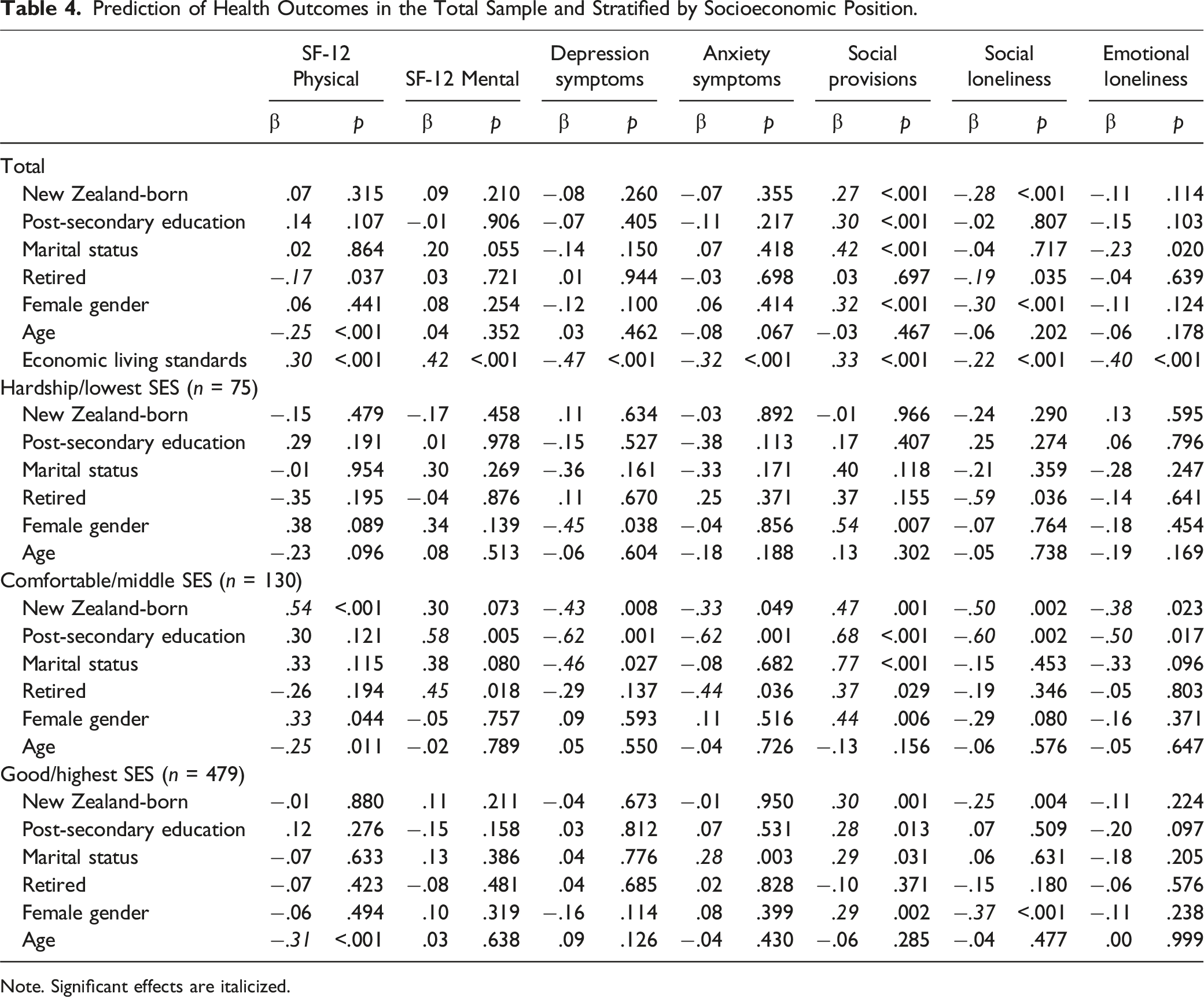
Note. Significant effects are italicized.
Analyses stratified by socioeconomic position yielded several significant differences between immigrant and New Zealand-born older adults (Table 4). Those reporting economic hardship had the worst outcomes on all measures, but having a migrant background did not have an additional significant effect on health in this group. Among those with a comfortable living standard, being New Zealand-born was associated with better physical health (β = .54, p < .001), lower levels of depression (β = −.43, p = .008) and anxiety (β = −.33, p = .049), higher levels of social provisions (β = .47, p = .001), and lower levels of social (β = −.50, p = .002) and emotional loneliness (β = −.38, p = .023). For those with good living standards, being New Zealand-born had significant effects on social wellbeing in terms of reduced social loneliness (β = −.25, p = .004) and increased social provisions (β = .30, p = .001).
Discussion
In recent years, increasing research from large immigrant-receiving countries, such as the United States, Canada, Australia, and many European countries, has exposed health inequities between migrant and native-born older adults (Markides & Rote, 2019). Informed by a holistic view of health and a structural model of inequities, the present study aimed to contribute to this emerging body of research by investigating the health status of older migrants in Aotearoa New Zealand compared to a matched sample of non-Māori, New Zealand-born older adults.
Findings demonstrate that both socioeconomic position and migrant background are important social determinants of poor health among older people in Aotearoa New Zealand. Having a migrant background emerged as a specific risk factor for compromised social wellbeing. The differences between migrant and New Zealand-born older adults in social wellbeing foreground the importance of early life relationships and the maintenance of social convoys over the life course for health in later life (Antonucci et al., 2014; Kahn & Antonucci, 1980; Webster et al., 2022). Immigrating to a foreign country as an adult can disrupt social networks, severing or weakening ties with existing social connections from one’s home country (Maleku et al., 2022). In turn, new migrants often find that forming new social convoys in a foreign environment is a difficult task (Ryan, 2011; Ryan et al., 2008), which can have lifelong implications for social wellbeing. Indeed, previous research in Aotearoa New Zealand has shown that older migrants commonly report restricted social networks, reduced social support, and increased social isolation (Park et al., 2019; Szabó et al., 2023).
Further, inequities in health, including social wellbeing, were patterned by socioeconomic position. Higher socioeconomic position was associated with better self-reported health outcomes in both groups, but New Zealand-born older adults derived more health benefits from increasing economic advantage compared to their peers of migrant background. This was particularly evident for the group in the middle of the socioeconomic gradient, likely to reflect working class older adults, including labour migrants. Older migrants in this group reported significantly poorer outcomes across all three domains and in almost every indicator of health than their age, gender, and education matched non-Māori, New Zealand-born peers. Numerous previous studies have shown that labour migrants, in particular, are at higher risk of experiencing poor health as they age than their native peers (Bolzman et al., 2004; Klokgieters et al., 2018; Lum & Vanderaa, 2010). Importantly, some of these inequities were not limited to the working class. We saw significant disparities in social wellbeing between older immigrants and older New Zealanders even in the most economically advantaged group, a finding that supports previous studies documenting diminished health return of higher socioeconomic status for migrants and ethnic minorities as a result of structural barriers and discrimination (Assari, 2018a, 2018b; Brandt & Hagge, 2020; Muñoz-Comet, 2016; Stephens et al., 2022).
At the lower end of the socioeconomic ladder, the figures indicate consequential health vulnerabilities for those living in hardship regardless of place of birth. Significantly diminished health outcomes in this economically most disadvantaged group are likely to denote the health impacts of a lifetime of socioeconomic deprivation (Harber-Aschan et al., 2020; Seabrook & Avison, 2012; Stephens et al., 2022; Torres et al., 2018). The sample size in this group, however, was relatively small, and as such findings should be taken with caution. Taken together, the findings provide support for using a structural model when investigating health inequities between migrants and native-born populations and highlight the need to adopt a holistic view of health, that incorporates social wellbeing alongside mental and physical health indicators.
Limitations
Findings should be considered in light of some limitations. For one, analyses were based on self-report data. Given that cultural groups vary in their interpretations of health symptoms, the use of self-report data may result in the under-reporting of health-related difficulties (Jatrana et al., 2014a, 2018; Teruya & Bazargan-Hejazi, 2013). Second, grouping ethnically diverse older adults together into a homogenous ‘migrant’ category in analyses poses challenges for interpretation of the data. There is significant variability across ethnic groups in socioeconomic position and educational attainment. Considering these factors are important axes of stratification, and the grouping of ethnic groups into a homogenous category is likely to result in an observed overall health disadvantage when in fact the health disadvantage may be only present for some ethnic groups but not for others. Third, approximately half of the migrant sample originated from the United Kingdom. Although most migrants in the 65+ age group in Aotearoa New Zealand come from the United Kingdom, Ireland, and Continental Europe (Statistics New Zealand, 2020b), these groups were significantly over-represented, whereas Asian and Pacific migrants were significantly under-represented. Finally, the analyses were cross-sectional, assessing the health status of older migrants and their New Zealand-born peers at one point in time, and as such our findings do not provide information on changes in health trajectories over time.
Strengths and Policy Implications
An important strength of the research is the use of case–control matching of New Zealand-born and migrant participants based on age, gender, and education, which allowed us to reduce the potential confounds introduced by demographic characteristics (Rose & Laan, 2009). This gives us stronger evidence that disparities found in health between the two groups can be attributed to having a migrant background. The structural approach taken in this research further highlighted how disparities differ across the socioeconomic gradient. In particular, older working and lower middle-class migrants arrived at older age in poorer health than their (age, gender, and education matched) New Zealand-born peers, reflecting not only the impact of lifetime inequities in work, education, and access to healthcare but also inequities in migrants’ ability to realize the benefits of socioeconomic resources and opportunities for their health. Finally, conceptualizing health holistically enabled us to highlight significant vulnerabilities in social wellbeing. While higher socioeconomic position was protective for physical and mental health, it did not mitigate disparities in social wellbeing between migrant and New Zealand-born older adults.
These findings have important implications for social policy. They bring attention to addressing the root causes of inequities in migrant health and the need for a two-pronged approach. On one hand, strategies aimed at reducing socioeconomic deprivation have the potential to improve health for all older people. On the other, we need focussed policy action promoting social integration and reducing barriers for migrants to realize health gains from their socioeconomic position over the life course.
Footnotes
Acknowledgments
Access to the data is available upon request from the Health and Ageing Research Team at Massey University at
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Royal Society of New Zealand–Te Aparangi (RDF-VUW-1901) and the Ministry of Business, Innovation and Employment, New Zealand (MAUX1705 – ‘Maximising workforce participation for older New Zealanders: Opportunities, Challenges and Prospects’).