
Abstract
Introduction
In recent decades, the ability to balance the demands associated with the role of caregiver of an aging parent, family member, or friend with the responsibilities of paid work has become an issue for a significant proportion of the workforce (Duxbury & Higgins, 2017). Population aging in industrialized nations teamed with declines in fertility, delayed childbearing, an increase in cohabiting unions/dual-income households, and the shift from institutional to community-based health care (Calvano, 2015; Smock & Schwartz, 2020; Wysocki et al., 2015) has exacerbated this issue. The number of individuals providing unpaid care to aging relatives (referred to in this paper as caregivers) has increased dramatically over the past several decades with recent estimates showing that 10.6% of the population of Australia, 21.3% of the total population of the U.S.A., and approximately one in five of the citizens of the EU, the U.K., and Canada engaged in this form of caregiving (International Alliance of Carer Organizations, 2021). Although data on caregiver prevalence in the workforce is sparse, recent research (Henderson & Johal, 2022) estimates that three of every four employees have some form of responsibility for the care of an elderly family member, a trend that is projected to continue as global populations age.
The adverse consequences of this form of caregiving for both the employee and employer are well documented. Research has shown that employees who provide eldercare on an informal basis are more likely than those employees not engaged in this role to report higher levels of anxiety, depression, fatigue, headache/body-ache, poor sleep, reduced appetite, cardiovascular disease, and mortality (Connor & Taylor, 2022; Park, 2021). Employed caregivers also report lower job satisfaction, higher turnover, and reduced productivity compared to their non-caregiving peers (Duxbury & Higgins, 2017; Xiang et al., 2022).
Although eldercare is a growing concern for many employees, much of the research in the work-life area focuses on the impact of child caregiving on individual and work outcomes (Burch et al., 2019; Halinski et al., 2019). Conversely, research in the caregiving field focuses on caregivers from a public health perspective and does not highlight the economic impacts of care provision on caregiver employment status or the impact caregiving has on work outcomes (Schultz et al., 2020). This is unfortunate given recent evidence showing that caregiving is likely to surpass childcare as a pressing concern for organizations and their employees within the next decade (Schultz et al., 2020; Burch et al., 2019).
Three classes of stressors have been studied in relation to caregiver outcomes (Pinquart & Sörensen, 2003b): (1) caregiver characteristics (e.g., gender, ethnicity, and socio-economic status), (2) the caregiving context (e.g., where the care-recipient lives), and (3) care-recipient characteristics (e.g., health conditions). Various researchers have explored the link between the first two sets of stressors and a variety of caregiver outcomes (Pinquart & Sörensen, 2005, 2003b; Calvano, 2015; Duxbury & Higgins, 2017; Schultz et al., 2020). Studies exploring the relationship between the last class of stressor (care-recipient characteristics) and caregiver well-being are, however, relatively rare. Moreover, those studies that have been done tend to be limited in scope and generalizability focusing on the impact on the caregiver of caring for an elderly dependent with only one illness—most commonly dementia (Etters et al., 2008) or cancer (Girgis et al., 2013). Only a few papers were identified that either compared the impact of different care-recipient health conditions on caregiver outcomes (see Kim & Schulz, 2008; Stetz & Brown, 2004) or examined the impact on the caregiver of proving care to someone suffering from multiple health conditions at the same time (Schoen et al., 2009).
The research program described in this article, a three-stage initiative to develop and validate a measure to identify the demands imposed on those who combine a paid job with informal care of an elderly dependent (i.e., employed caregivers) with a variety of health conditions, was undertaken to address this issue. The need for such a measure can be appreciated when one considers the following. First, while the negative association between caregiver burden and caregiver well-being for employed caregivers has been established, we have little understanding of how demands placed on the caregiver vary according to the health condition(s) of the care recipient. Second, the few studies that do compare caregiver outcomes across a range of care-recipient illnesses or conditions suggest that divergent care-recipient conditions affect caregivers differently (Kim & Schulz, 2008; Bobinac et al., 2010). Our review of the extant literature suggests that a measure such as the one described in this paper that identifies and quantifies the demands arising from a wide range of care-recipient health conditions would help researchers and practitioners to clarify the relationship between care-recipient health, caregiver burden, and caregiver well-being and employment outcomes. In summary, the measure developed and tested in this study addresses the above issues by providing researchers and practitioners with a measurement tool that can be used to test models linking care-recipient health conditions to caregiver burden, caregiver burden to organizational outcomes such as absenteeism, intent to turnover and presenteeism, and caregiver burden to caregiver well-being outcomes such as perceived stress, depressed mood, and physical health. It will also facilitate identification of identify factors modifying each of these relationships such as caregivers’ abilities, strategies, and access to resources. As such, this measure should have utility for researchers who are exploring the etiology of caregiver well-being as well as practitioners who are charged with designing programs to help employed caregivers cope with work-caregiving conflict.
The paper proceeds as follows. We begin by distinguishing between the different forms of caregiving identified in the research literature. Next, we examine research linking the demands associated with different eldercare-recipient health conditions and caregiver well-being (specifically caregiver burden, depression, and stress). The research methodology used to develop and test the measure (Hinkin, 1995, 1998) is then summarized and results presented in three sections: (1) item identification; (2) scale construction and item reduction; and (3) validation and testing of the scale (Hinkin, 1995, 1998). The paper concludes with a discussion of key findings along with suggestions on how the measure can be used by researchers and practitioners alike.
Literature Review
Many of the findings reported in the caregiving literature regarding the challenges faced by caregivers and the impact of interventions introduced to help caregivers cope with their situation are mixed—a finding that Shultz et al. (2020) in their systematic review of the caregiving literature attribute to the fact that many studies do not take caregiver context into account. Schultz et al. (2020, p. 635) point out that “Caregivers represent a broad and diverse group of individuals. They span all ages and are heterogeneous across multiple dimensions” (Schultz et al., 2020, p. 635). Following Schultz et al.’s (2020) recommendations, we begin our literature review with a brief overview of the different forms of caregiving, specifying who we sampled and why.
We then provide a brief overview of the three research streams that informed the development and testing of the measure presented in this paper. We begin by summarizing research done identifying the types of health conditions typically reported by recipients of eldercare. We then turn our attention to how researchers have archetypally measured the demands associated with each of these various health conditions. Finally, we report on research that has been done linking the demands associated with care-recipient health conditions and employee well-being.
Classification of Caregivers
Talley and Crews (2007) describe a triadic model of caregiving which identifies three factors used to classify caregiving: formal (nurses, physicians, psychologists, and therapists), informal (immediate family and extended family), and care recipient (age and illness). Schultz et al. (2020) identify three distinct groups receiving informal care: (1) children with chronic illness and disability who are typically cared for by young adult parents; (2) adult children suffering from conditions such as mental illness who are cared for by middle-aged parents; and (3) older individuals who are cared for by their spouses or their middle-aged children. They state: “Each of these populations poses unique challenges to caregivers given the variability in health conditions, symptomatology, health and social service support systems, and the life course stage of the care recipient and caregiver” (Schultz et al., 2020, p. 635).
In our study, for the purposes of maintaining homogeneity of our sample, we focus exclusively the unique demands employed individuals face when they informally provide caregiving to elderly dependents. We do not consider the challenges faced by those who provide eldercare on a formal basis (i.e., paid care provided by a professional), those who care for a disabled child or adult, or those who only provide care for their children. While there is considerable overlap between the care of a disabled dependent and care for an elderly dependent (many older adults may become disabled because of their health condition), end-of-life care is generally not a consideration for most people who care for a disabled dependent. Care for children with disabilities can be a daunting undertaking and as Isa et al. (2016) point out, the demands this role places on caregivers can vary widely and is strongly related to the child’s disability factors (i.e., physical disability and cognitive disability).
Research has also pointed out that caring for an elderly dependent is quite different from caring for children. As Halinski et al. (2019, p. 100) point out: “Caring for children spans many years and has a predictable pattern (i.e., the need for childcare typically decreases slowly over time as children become more independent). Caregiving, on the other hand, is less predictable and varies widely in duration. While parents have nine months to prepare for the birth of a child, caregivers are usually thrust into the role without warning or planning because of an accident or sudden illness.” Childcare and eldercare also often elicit different emotions in the caregiver. Those who provide eldercare typically report feelings of guilt and sadness as the caregiver must deal with frequent uncomfortable realities (i.e., declines in health over time followed by the ultimate death of a loved one). While the provision of childcare can often be quite challenging (especially when combined with work), it is also a source of joy, happiness, and purpose as the parent watches children grow and develop (Halinski et al., 2019). While childcare is typically associated with reduced burden as children gain independence, caregiving only fully concludes when the elderly dependent dies (Kossek et al., 2001).
Care-Recipient Health Conditions
Butler-Jones (2010, p. 21) lists (in no particular order) the most prevalent health issues of the elderly as follows: circulatory and respiratory diseases, cancers, high blood pressure, heart disease, arthritis, diabetes, Alzheimer’s disease and other dementias, and “difficulty with [daily] activities.” Most empirical research that includes information on the care-recipient’s health condition focuses only on caregivers of individuals diagnosed with Alzheimer’s disease or other forms of dementia. This stream of research is primarily driven by the growing numbers of dementia patients requiring care (Burton et al., 2012). Research shows that caring for a dependent with a cognitive disability such as dementia (1) places a high degree of burden on employed caregivers (WHO, 2021; Calvano, 2015; Etters et al., 2008) and (2) is more stressful and burdensome than caring for someone with a physical disability (Bainbridge et al., 2006). These findings reinforce our assertion that it is important that researchers and practitioners understand how a variety of care-recipient health conditions can differentially affect caregiver outcomes.
Population aging and the shift of health care services into the community has made cancer patients another cohort that features in much caregiver research studies (Girgis et al. 2013, Burton et al., 2012). Caring for someone with cancer has been shown to be more burdensome than caring for the frail elderly (Kim & Schulz, 2008) and more disruptive to social engagement than caring for someone with AIDS (Stetz & Brown, 2004). Other studies (Burton et al., 2012) note that those suffering from chronic obstructive pulmonary disease (COPD), congestive heart failure and kidney failure, and the aftereffects of a stroke also commonly rely on family members to provide care during long periods of difficult or deteriorating health. Although these chronic diseases affect large numbers of people (Burton et al., 2012; Butler-Jones, 2010), little is known about how caring for a dependent with these chronic illnesses compares (in terms of caregiver burden and well-being) to caring for a dependent with dementia, cancer, or other health conditions.
Other care-recipient health conditions that have been the subject of individual studies in the eldercare caregiving literature, albeit even less frequently than the chronic diseases discussed above, include diabetes, HIV/aids, vision impairment, and Parkinson’s disease (e.g., Bambara et al., 2009; Cahill & Valadéz, 2013; Leroi et al., 2012; Li et al., 2004).
Measuring the Demands Associated with Different Care-Recipient Health Conditions
How have researchers quantified the demands associated with the various care-recipient health conditions identified above? To answer this question, we reviewed the empirical literature in this domain and identified any studies that included a mention of one or more specific care-recipient health conditions. We note three types of references: (1) a specific health condition was the sole focus of the study, (2) the health of the care recipient was included as part of the demographic data collected for the study, or (3) less commonly, the study was a comparison of outcomes across a variety of different care-recipient illnesses. In virtually all cases, the illnesses and health conditions were identified by asking either the caregiver or the care recipient for relevant information. Caregiver demands were measured separately and independently from the identification of the care-recipient’s health condition. We found no cases where respondents were asked to identify the demands specifically associated with a particular care-recipient health issue.
In Kim and Schulz’s (2008) comparative analysis of the impact of different care-recipient illnesses on caregiver well-being, the sample included carers of persons with cancer, dementia, diabetes, and frail elderly as identified by the caregivers’ answers to the question “What would you say [is/was] the main problem or illness of your care-recipient?” (p. 488). Physical, emotional, and financial demands were measured with questions such as: “How emotionally stressful would you say that caring for your care-recipient [is/was] for you?”. Similarly, Slaunwhite et al. (2017) used a survey question that asked caregivers to report their care-recipient’s primary health problem to identify carers of those who had mental health issues from those who did not. Stetz and Brown (2004) selected their sample in a manner designed to ensure that all caregivers were providing care to someone with cancer and/or AIDS. Of note, none of these studies included questions linking the demands specifically to the care-recipient’s specific health condition (i.e., all measured demands as an omnibus, higher level construct).
Demands Associated with Care-Recipient Health Condition and Employee Well-being
Most of the empirical research examining the relationship between caregiving and caregiver well-being focuses on caregiver burden and/or some combination of two generic measures of psychological well-being—depressed mood and perceived stress (Adelman et al., 2014; Pinquart & Sorenson, 2003b; Sales, 2003; Sherwood et al., 2005). Caregiver burden measures the impact felt by caregivers from the physical, emotional, social, and financial demands of caregiving (Zarit et al., 1986). Two moderately correlated components of caregiver burden have been identified by Montgomery et al. (1985): objective caregiver burden or OCB (i.e., the tasks the caregiver provides when caring for an elderly dependent) and subjective caregiver burden or SCB (i.e., the emotional or psychological burdens of care). Research has shown that both forms of burden are distinct and important even though many empirical studies use an overall measure of burden that sums component indicators into a single caregiver burden score.
Although our review of the extant literature suggests that very few studies have compared caregiver demands or well-being outcomes across multiple specific care-recipient illnesses or conditions, there is some support for the idea that caregiver burden (both forms) and psychological well-being are influenced by a care-recipients’ health condition. Sales’s (2003) examination of the extent to which the characteristics of different chronic illnesses can influence caregiver well-being determined that, in keeping with the multidimensional nature of caregiver burden, the psychosocial impacts of the care-recipients’ illnesses on caregivers can also take different forms. Sales (2003) findings show that while generic measures allow cross-disease comparisons, the specific challenges that may impact both the objective and subjective burdens of a particular illness may be missed. Bobinac et al.’s (2010) more recent study exploring this idea ascertained that care-recipients’ illnesses will have significant and differential effects on caregivers arising from different sources: from caring for an elderly dependent (e.g., time spent, difficult activities, and social isolation) and on caring about an elderly family member (i.e., emotional concern for their welfare). These studies reinforce the need for a measure such as the one developed in this paper.
Empirical research in this domain also provides support for the idea that care-recipient illness may differentially impact caregiver well-being (Kim & Schulz, 2008; Stetz & Brown, 2004; Kim & Schulz, 2008). For example, in studies comparing the well-being of caregivers to that of non-caregivers, a greater difference was found between the two groups when caregivers were all carers for dementia patients, suggesting that dementia caregivers may experience greater stress, depression, lower subjective well-being and self-efficacy, as well as poorer physical health than their non-dementia counterparts (Pinquart & Sörensen, 2003a).
Only one study was found that contradicted this small cohort of research that has demonstrated the differential impact of care-recipient health conditions on caregiver well-being. In a study focused only on older spousal caregivers of older care recipients in hospices, Haley et al. (2001) found no differences in depression between cancer and dementia caregivers.
This study addresses the above issues by developing a measure that allows researchers to link care-recipient health to caregiving demands and by testing a model that examines how different care-recipient illnesses and symptoms differentially impact caregiver burden and caregiver well-being.
Methodology
We followed the scale development protocol as outlined in Hinkin (1995, 1998, and 2005) and summarized in Figure 1, to develop and validate our measure of the demands associated with various care-recipient health conditions (referred to in the rest of the paper as the Care-recipient Health Demands Scale or CRHD). The decision to use this methodology is supported by a recent review of Likert scale development advances (Jebb et al., 2021). In the sections below, we outline the results obtained for the following phases of Hinkin’s methodology: (1) item identification, (2) scale validation, and (3) analysis of psychometric properties of the measures. Hinkin’s (2005) scale development protocol.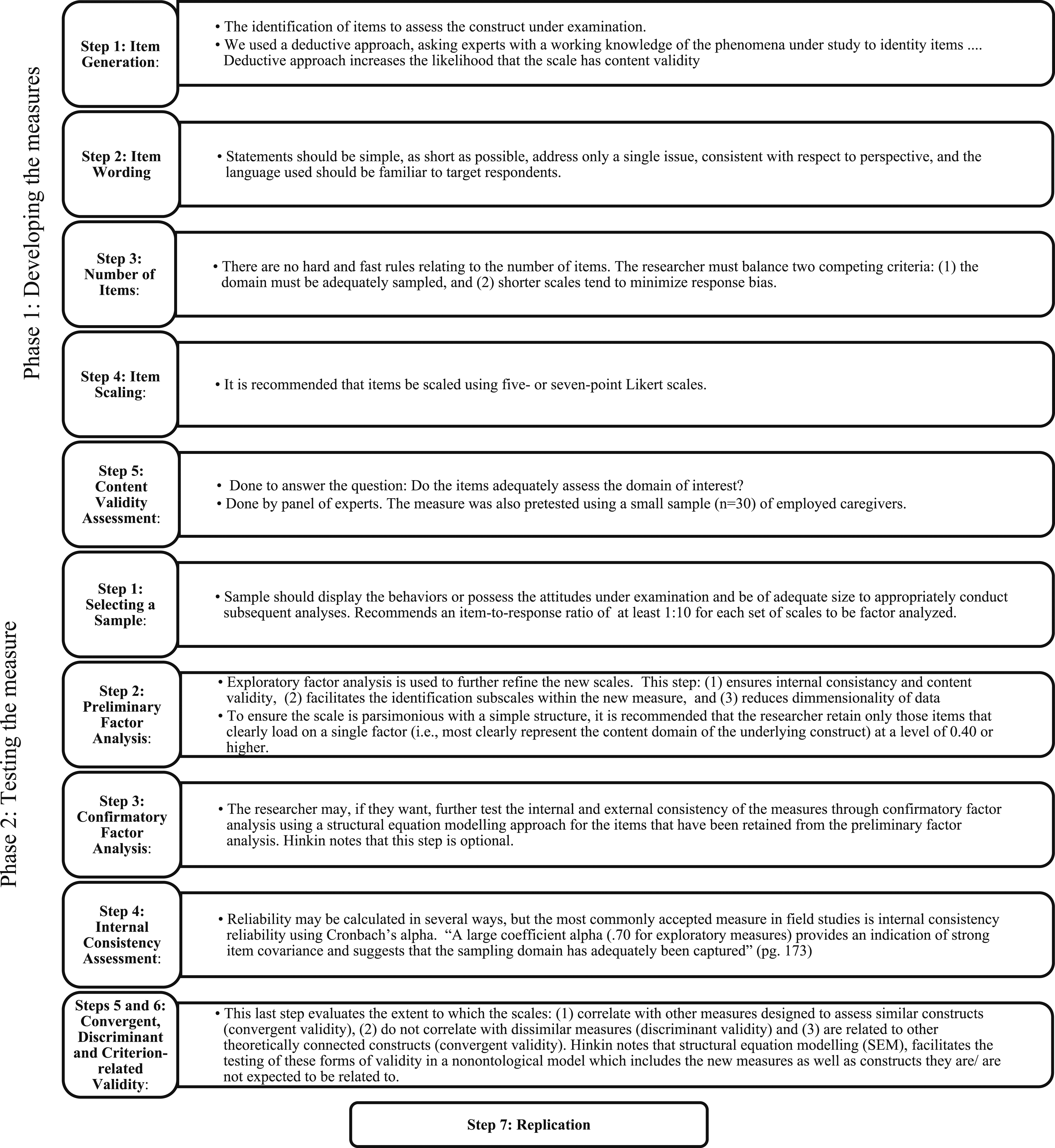
Phase 1: Item Identification
The first stage of scale development is the creation of a list of items to assess the construct under examination. The goal of the researcher is to develop items that will result in measures that sample the theoretical domain of interest to demonstrate content validity (Hinkin, 1995, 1998). In this study Hinkin’s advice was operationalized as follows.
We began by inductively generating a comprehensive list of care-recipient health conditions which could be used to measure the perceived extent to which each of these conditions impacts or places a burden on caregivers of elderly dependents. Our goal in generating this list was to represent the breadth and specificity of the illnesses afflicting elderly care recipients. Three steps were used in the list creation process: (1) a review of the caregiving literature, (2) an analysis of the results of a qualitative study on caregiving strain undertaken by the authors, and (3) a final review by experts in the field of caregiving and eldercare.
The literature was reviewed using the Google Scholar database and the following search terms: “care-recipient” with “illness” “condition” and “health,” as well as “care receiver” with “illness,” “condition’ and “health.” Article examination was restricted to those published in English that dealt with informal caregiving of elderly family members or friends. We then examined the qualitative data from our National Study on Work Life and Caregiving (Duxbury & Higgins, 2017) which involved 111-hour long in-depth interviews with male and female employed caregivers. Responses to interview questions that spoke to the challenges these caregivers faced that could be related to the condition of the person they were caring for generated a second comprehensive list of care-recipient health conditions. We used this list to corroborate and augment the initial list compiled from the literature review.
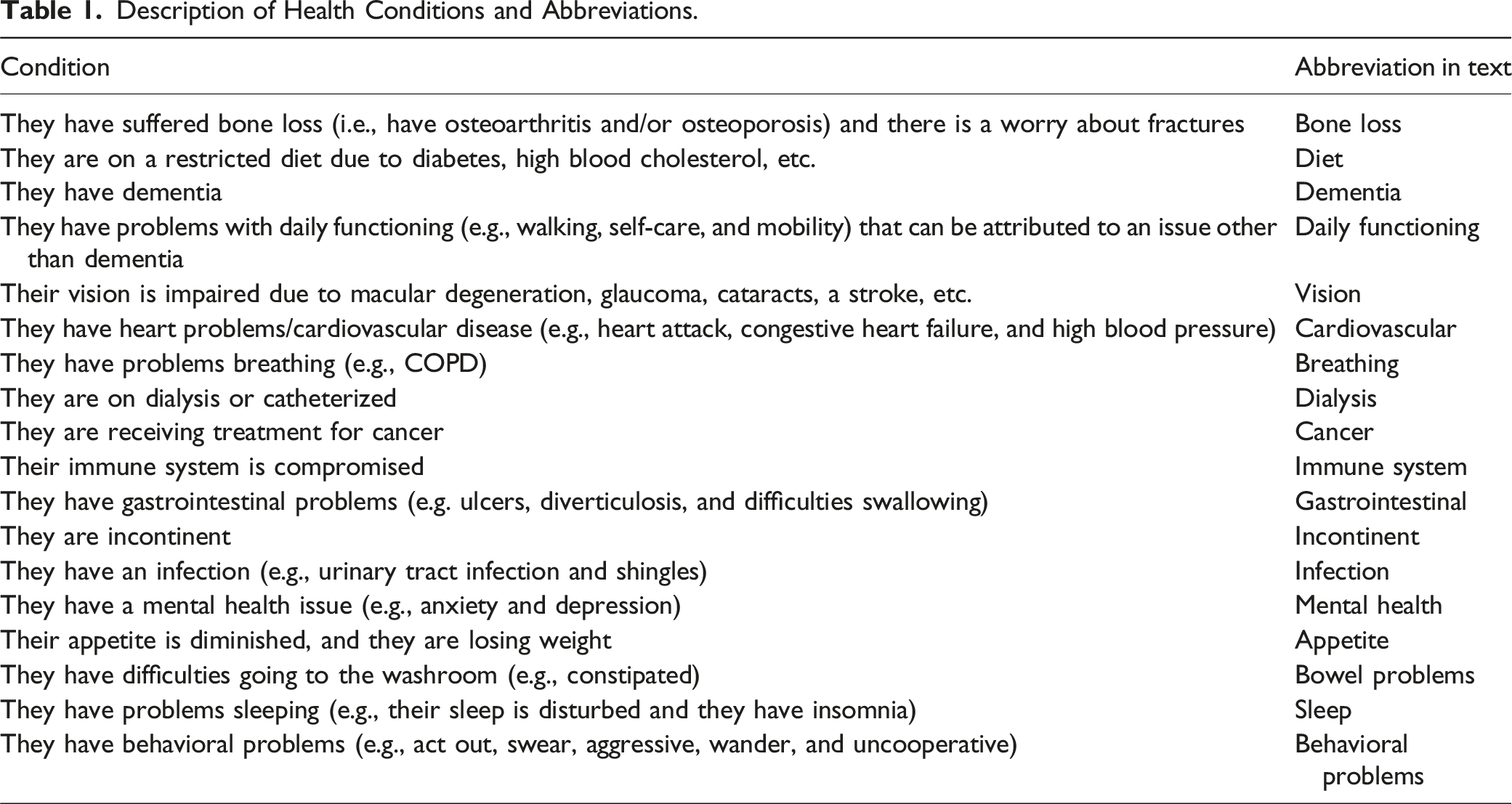
Description of Health Conditions and Abbreviations.
Phase 2: Scale Validation
Phase 2 of Hinkin’s (1998) approach requires the researcher to include the generated items within a questionnaire and then use the survey data to examine the psychometric properties of the new measures. The CRHD scale was constructed to allow us to collect two pieces of information from our respondents: (1) whether the person they were caring for suffered from each of the 18 listed conditions and (2) the caregiver’s assessment of the demands placed on them of caring for someone with this health issue. The question was worded as follows: A person’s caregiving experiences are likely to vary depending on the medical and physical condition of the person that they are caring for. Below is a list of physical and mental health conditions that are common in the elderly. For
The questions were answered on a 5-point Likert-type scale (1 = not applicable, 2 = almost no demands, 3 = a few demands, 4 = moderate demands, and 5 = high demands). The finalized measure was then pretested on a small sample (n = 30) of employed caregivers. Follow-up interviews with our respondents detected no problems with the measure (i.e., wording was clear, order of items was fine, and response burden manageable).
Sample
Description of the Sample (n = 1696).
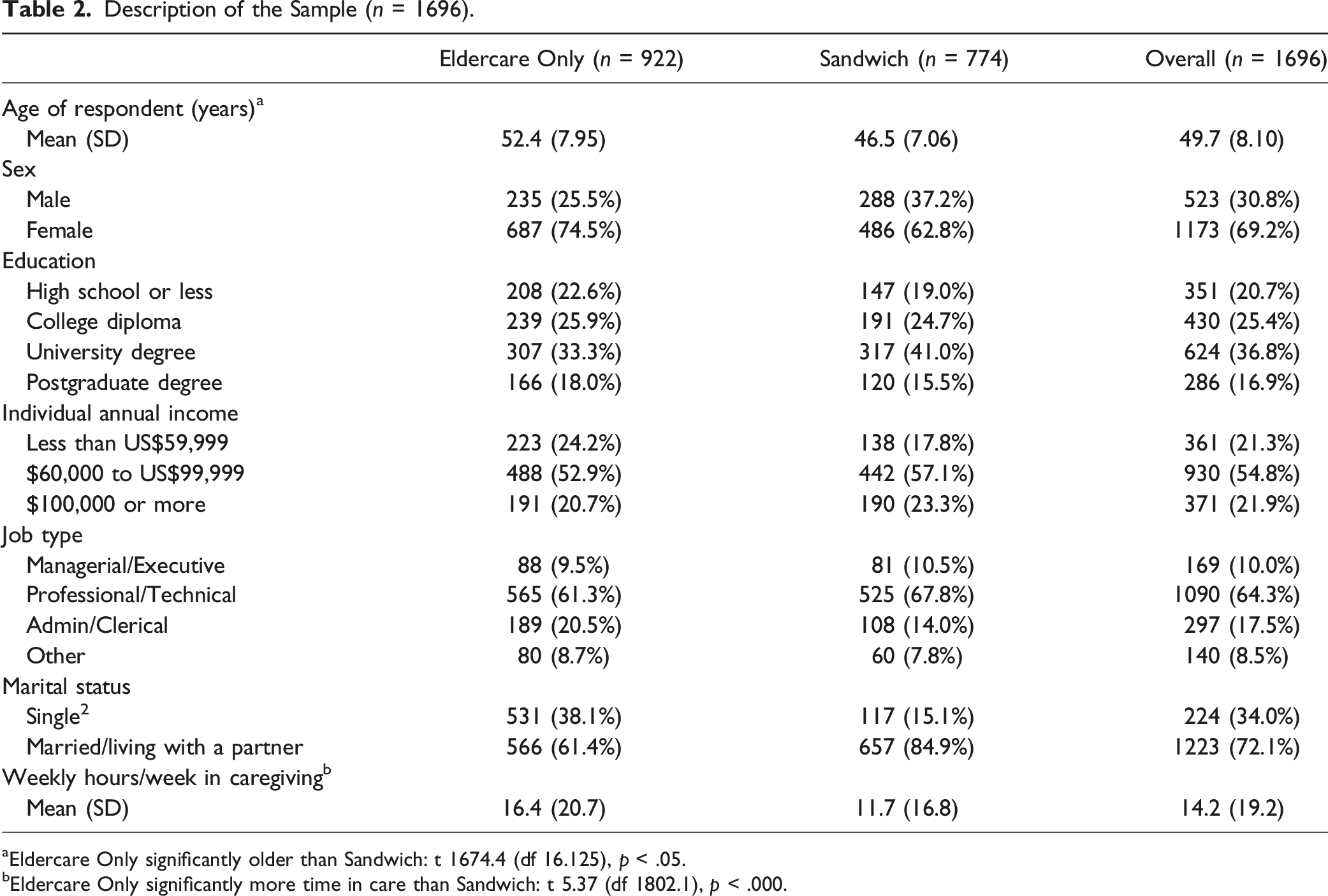
aEldercare Only significantly older than Sandwich: t 1674.4 (df 16.125), p < .05.
bEldercare Only significantly more time in care than Sandwich: t 5.37 (df 1802.1), p < .000.
Respondents were largely married, middle-aged middle-income females working in managerial/professional positions. On average, respondents spent a substantive amount of time each week in eldercare activities (14.2 hours). Those in the sandwich generation sample were significantly younger (M = 46.5) than those in the eldercare-only sample (M = 52.4) and more likely to report that they were married/partnered at the time the study was done. Those in the eldercare-only sample (M = 16.4 hours) spent significantly more hours in care per week than those in the sandwich sample (M = 11.7 hours week).
Research continues to show that caregiving is gendered (Duxbury & Higgins, 2017). In recognition of this fact, we disaggregated the data by sex (male/female) and undertook gender analysis using paired t-tests. Categorial variables were coded as numeric values based on the categories shown in Table 2 (i.e., education given a value of 1, 2, 3, or 4; income a value of 1, 2, or 3; marital status a value of 1 or 2). Gender was not significantly associated with age, education, or marital status. Male respondents tended to have higher income (M = 2.27 (0.58), F = 1.89 (0.66), p > .000) and participated in significantly fewer hours of weekly care (M = 12.1 (16.2), F = 15.1 (20.3) p > .000) than their female counterparts. Sex was, therefore, included as a control variable in all subsequent analyses.
Data on the percent of our sample providing care to a recipient with each of the 18 items was analysed using paired t-tests. Categorial variables were coded as numeric values based on the categories shown in Table 2 (i.e., education given a value of 1, 2, 3, or 4; income a value of 1, 2, or 3; marital status a value of 1 or 2). Gender was not significantly associated with age, education, or marital status. Male respondents tended to have higher income (M = 2.27 (0.58), F = 1.89 (0.66), p > .000) and participated in significantly fewer hours of weekly care (M = 12.1 (16.2), F = 15.1 (20.3) p > .000) than their female counterparts. Sex was, therefore, included as a control variable in all subsequent analyses.
Proportion of Sample Caring for People with Each of the Following Conditions (n = 1696).
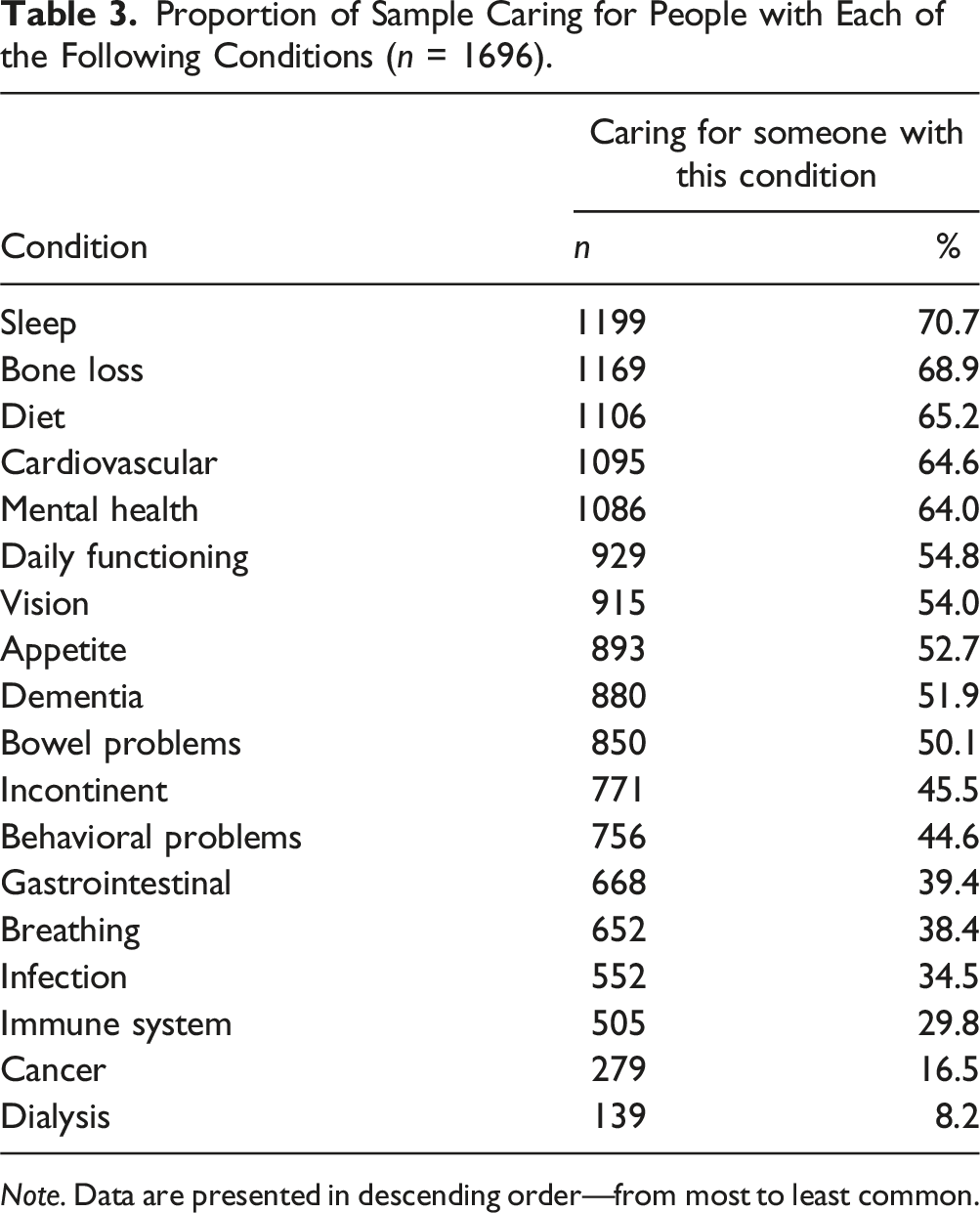
Note. Data are presented in descending order—from most to least common.
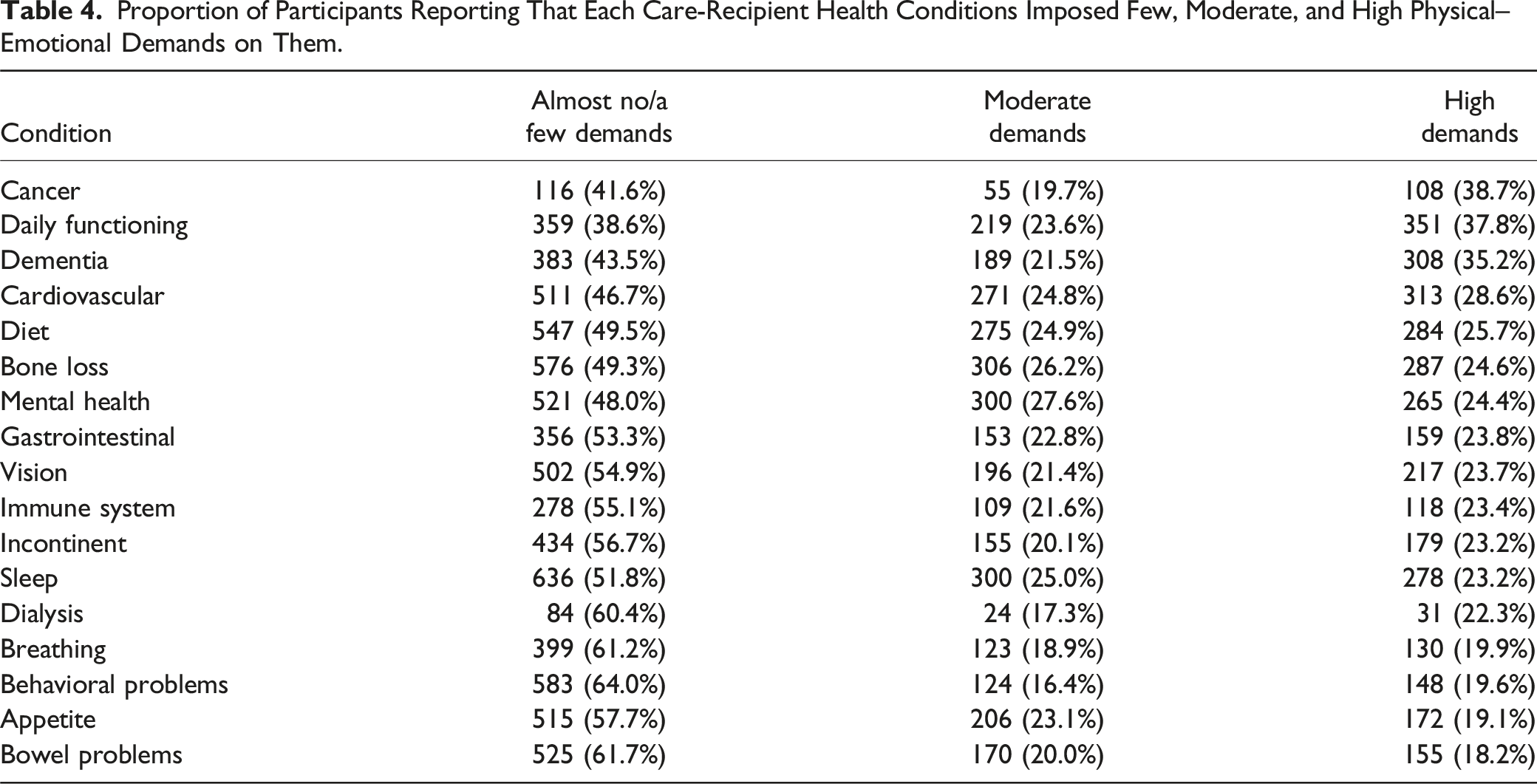
Proportion of Participants Reporting That Each Care-Recipient Health Conditions Imposed Few, Moderate, and High Physical–Emotional Demands on Them.
Item Reduction
Exploratory factor analysis (EFA) using maximum likelihood (Tucker & McCallum, 1997) was used in this study to reduce our list of 18 care-recipient health conditions into a smaller pool of factors (i.e., latent variables) to be used in the scale validation phase of the research. The Kaiser–Meyer–Olkin (KMO) Measure of Sampling Adequacy (MSA) was applied to the 18 health conditions to test for suitability for factor analysis. This test assesses proportion of variance among variables, where MSA should be above 0.8 in order to proceed with factor analysis (Shrestha, 2021). The overall MSA of 0.85 supported the use of factor analysis.
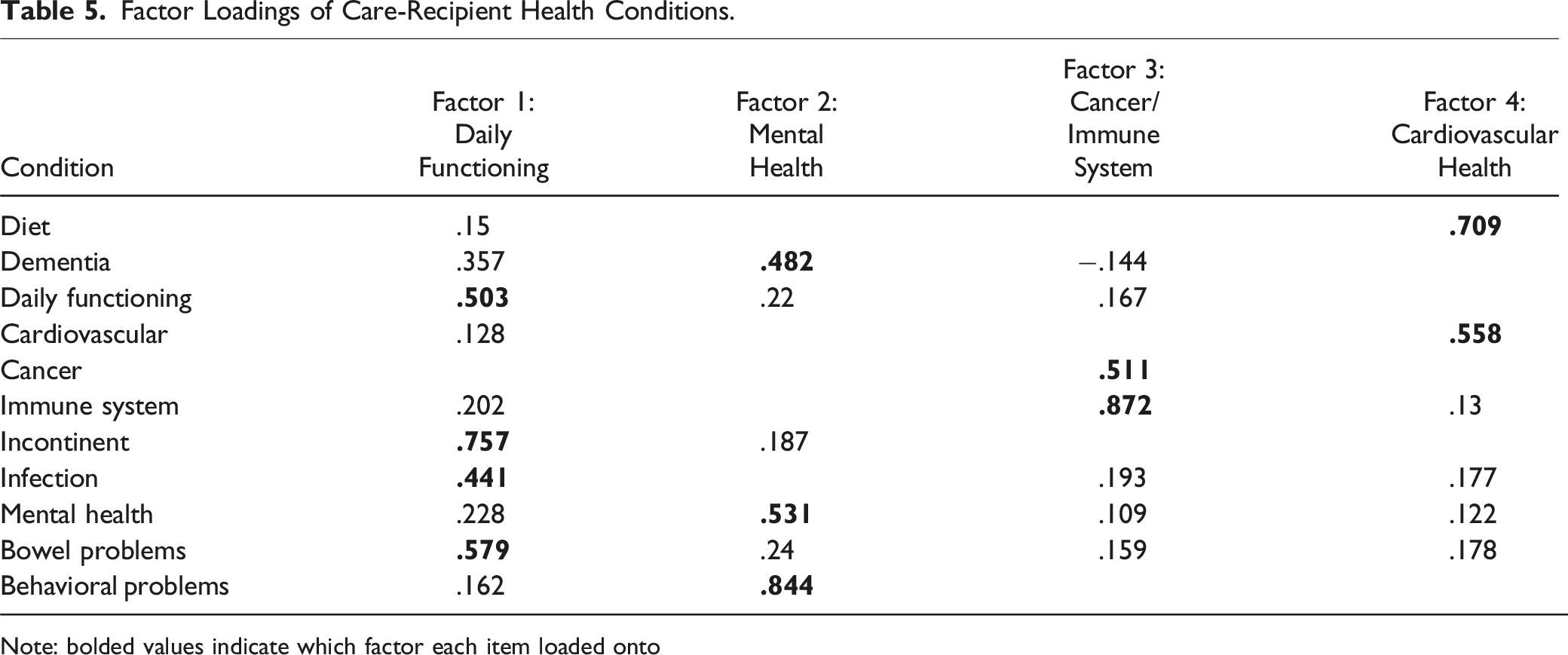
A factor analysis was performed using the factanal package in R version 4.2.2. As advised by Hinkin (1995), items which either did not load with any of the four factors at 0.4 or higher or which demonstrated high levels of cross-loading (i.e., loadings of .35 or higher on two or more factors) were removed from the analysis. Seven items did not load uniquely and were removed: dialysis, breathing, gastrointestinal, bone loss, appetite, vision, and sleep.
Factor Loadings of Care-Recipient Health Conditions.
Note: bolded values indicate which factor each item loaded onto
Two items loaded on the third factor, which was named “Cancer and Immune System.” The fact that these two items loaded on the same factor is consistent with data showing that people with cancer who receive chemotherapy are more likely to get infections because of their weakened immune system. Finally, two items, cardiovascular and diet, loaded on the fourth factor which we named “Cardiovascular Health Issues.” Again, the fact that these two conditions loaded on the same factor is not surprising given that many people with cardiac disease are placed on restricted diets (i.e., low fat and low salt).
Phase 3: Analysis of Psychometric Properties of the Measures
The final steps of Hinkin’s (1995; 1998) approach to scale development requires the researcher to assess validity (i.e., the accuracy of a measure). Best practice dictates that researchers who wish to demonstrate construct validity do so by establishing nomological validity (Hagger et al., 2017). This is done by connecting the construct that they are trying to validate to constructs that are linked to it in ways that are predicted by theory. In the section below, we first summarize the theory we used to develop the model used to test the CRHD scale and outline the hypothesis to be tested. We then outline the methodology used to test our hypothesis/validate our measure.
Conservation of resources (COR) theory put forward by Hobfoll (1989) was used to develop the nomological model used to establish construct validity. “The [COR] model’s basic tenet is that people strive to retain, protect, and build resources and that what is threatening to them is potential or actual loss of these valued resources” (Hobfoll, 1989, p. 516). According to the COR model, stress occurs in response to changes in the environment where (1) there is a threat to key resources, (2) when key resources are lost, and (3) when the investment of resources does not result in an overall gain of resources (Hobfoll, 1989; Hobfoll et al., 2018). COR theory is used in this paper to explain how a reduction of resources (the loss of time or energy due to caregiving) can result in declines in well-being (measured as general stress or burnout) of the caregiver.
Nomological Model
The nomological model used to establish the validity of our measures is shown in Figure 2. The constructs included in our model (SCB, OCB, perceived stress, and depressed mood) appear in many studies exploring the relationship between caregiving and caregiver well-being (e.g., Adelman et al., 2014; Pinquart & Sorenson, 2003b; Sales, 2003). Theoretical framework used establishes nomological validity. Note: Path coefficients are displayed on the lines between variables, and significant relationships are represented by a solid blue line, with dotted lines depicting non-significant relationships.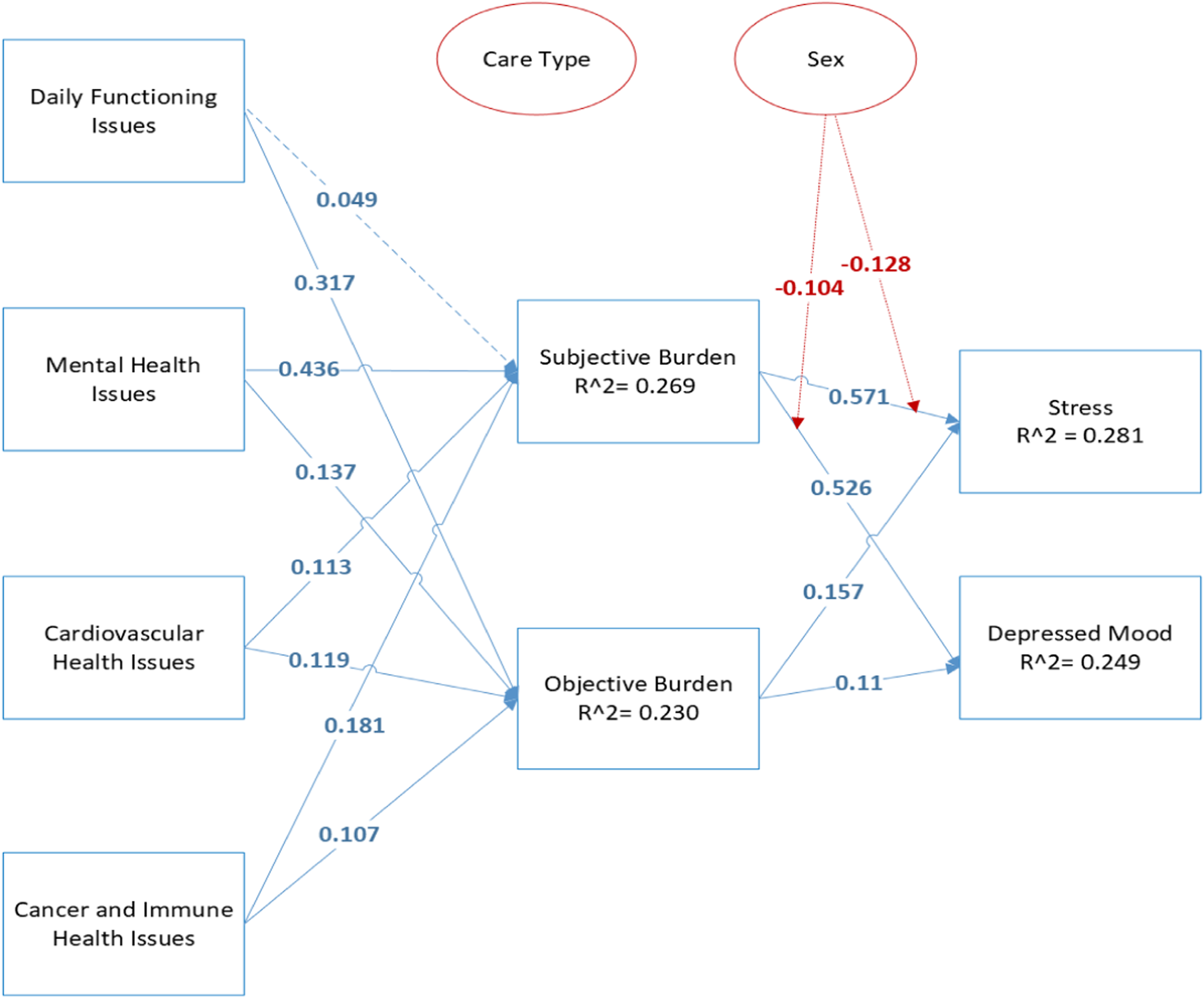
Our model posits that daily functioning problems, mental health problems, cancer/immune issues, and cardiovascular health (as measured using CRHD subscales) measure the physical/emotional demands imposed on the caregiver from caring for an individual with each of these health conditions. We posit that these demands will predict SCB and OCB which will, in turn, predict employee well-being. Justification for these assertions is provided below.
Subjective (i.e., the emotional or psychological burdens of care) and objective (i.e., the tasks the caregiver provides when caring for an elderly dependent) caregiver burdens measure the impact felt by caregivers from the physical, emotional, social, and financial demands of caregiving (Zarit et al., 1986). Based on COR, we expect that greater the demands (i.e., time, energy, and emotions) that caring for someone with daily functioning problems, mental health problems, cancer/immune issues, and cardiovascular health places on the caregiver in a typical month, the greater the likelihood that an employee will experience SCB and OCB as their resources are drained. Accordingly, we hypothesize that:
Daily functioning problems will be positively associated with (a) SCB and (b) OCB.
Mental health problems will be positively associated with (a) SCB and (b) OCB.
Cancer/immune system problems will be positively associated with (a) SCB and (b) OCB.
Cardiovascular conditions will be positively associated with (a) SCB and (b) OCB.
Two indicators of employee well-being, perceived stress and depressed mood, were included in the model. Stress can be defined as a negative physical and psychological reaction to a lack of fit between individuals and their environment while depressed mood is a mental state characterized by sadness, a loss of motivation, and feelings of hopelessness (Dole & Duxbury, 2015). COR theory implies that the greater the subjective/objective burden (i.e., physical, emotional) on the caregiver, the greater the likelihood that an employee will experience a decline in well-being as resources are depleted. This expectation is consistent with work by Lazarus (1991) who argues that stress can be viewed as a cognitive-phenomenological process in which individuals evaluate the demands placed on them by their environment (i.e., SCB and OCB) to determine if they pose a threat to individual well-being and, if so, whether they possess the ability and resources to deal effectively with the threat. Work by Pearlin et al. (1990) can also be used to justify this relationship. The authors argue that (1) the demands faced by caregivers (often in the form of emotional and social support) increase concomitant with the frailty of care recipients and (2) the higher the caregiving demands, the greater the likelihood that the caregiver will become exhausted (i.e., resources depleted) and experience higher levels of depressed mood and stress. These relationships have been consistently documented in research that investigates the relationship between eldercare demands (typically measured as hours in caregiving per week) and caregiver stress and depression (see Calvano, 2015; Duxbury et al., 2022; Duxbury & Higgins, 2017). The above literature supports the following hypotheses:
SCB will be positively associated with (a) perceived stress and (b) depressed mood.
OCB will be positively associated with (a) perceived stress and (b) depressed mood.
Finally, the literature supports the need to control for both gender and caregiver type (i.e., eldercare only and sandwich generation) when testing our model. Much of the research in this domain supports the idea that women caregivers report higher levels of caregiver burden and negative well-being outcomes than their male counterparts (Dole & Duxbury, 2015; Duxbury & Dole, 2015; Adelman et al., 2014). While there is less consensus on the impact of having one (eldercare-only) versus two (childcare and eldercare) caregiving roles on well-being, what is available supports the need to control for caregiver type (Duxbury et al., 2022; Duxbury & Higgins, 2017).
Measures
Measurement of Constructs in the Model.
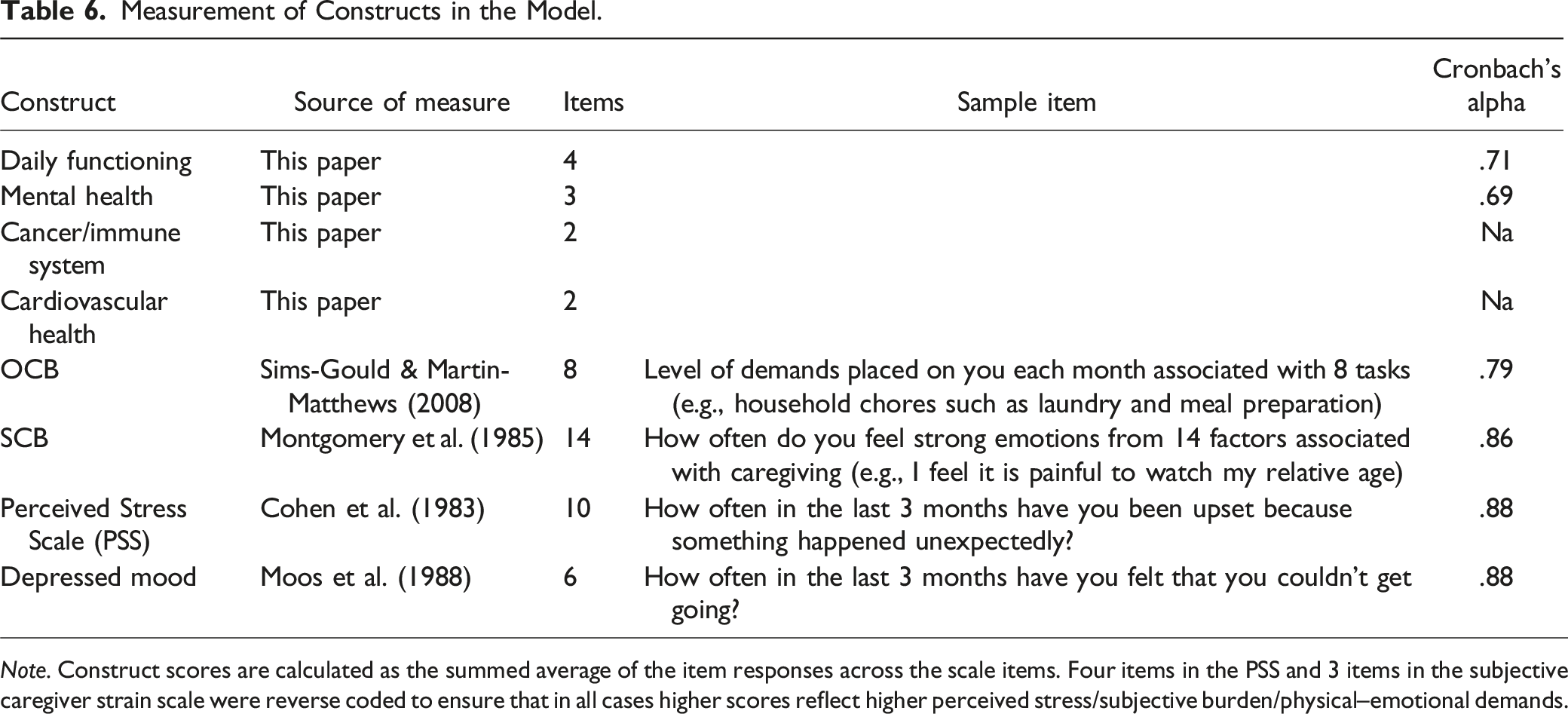
Note. Construct scores are calculated as the summed average of the item responses across the scale items. Four items in the PSS and 3 items in the subjective caregiver strain scale were reverse coded to ensure that in all cases higher scores reflect higher perceived stress/subjective burden/physical–emotional demands.
Data Analysis
Partial least squares structural equation modeling (PLS-SEM) using the seminr package in R was used to test the hypothesized model (see Figure 2). The guidelines articulated by Hair et al. (2014) were followed throughout this stage of the analysis. Indicator reliability was assessed by examining indicator loadings or the outer loadings of the measurement model. With one exception (SCB), all indicator loadings were greater than 0.7 as required by Hair et al. (2014). Three items within the SCB scale had loadings less than 0.4 and were removed from the analysis to achieve sufficient indicated reliability. As shown in Table 6, the internal consistency of each latent variable was considered satisfactory (0.7 or above as suggested by Stevens, 1992). Composite reliability, a measure of internal validity, was sufficient with all constructs having values above 0.60 as suggested by Fornell & Larcker (1981). The average variance extracted (AVE) is a strict criterion for measurement model validity, where values above 0.5 are generally considered suitable (Fornell & Larcker, 1981). Most AVE values of the latent constructs in our model were above the accepted 0.5, with the exception of stress, objective burden, and subjective burden, which had AVE values ranging from 0.405 to 0.481. In their original 1981 paper, Fornell and Larker note that AVE should be considered a conservative estimate of validity with limitations when used in models with complex multi-variate relationships. In this study, the high composite reliability (>0.6) of our constructs indicates that convergent validity has been achieved in the three cases where constructs have AVE below 0.5. As such, it was decided to proceed with our analysis. The PLS-SEM was bootstrapped with 1000 resamples to obtain the significance of each path. Sex and care-type were controlled for in the model.
Determination of Reliability and Construct Validity
Discriminate Validity
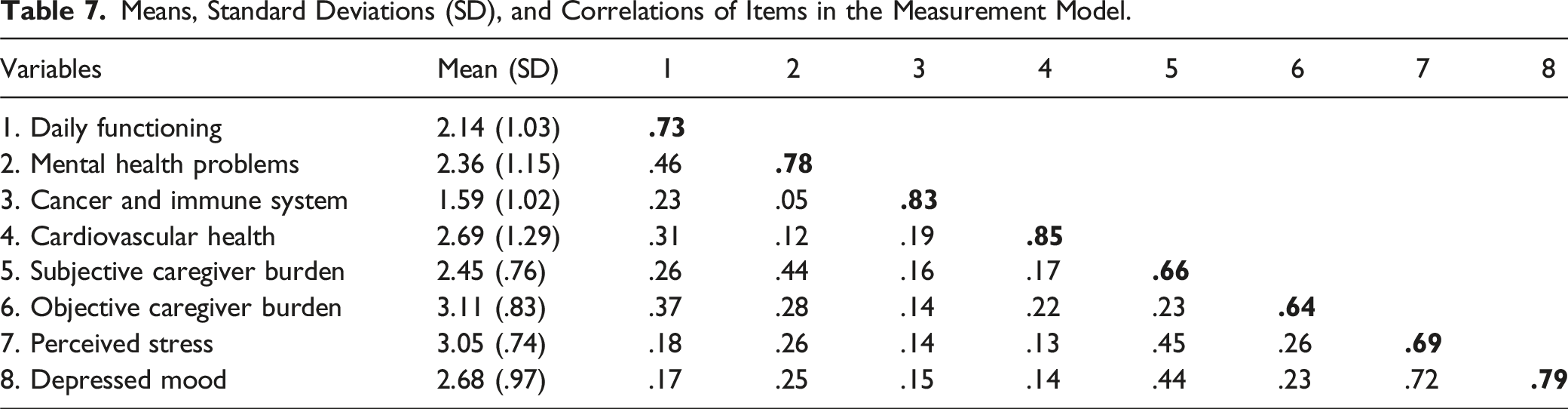
Means, Standard Deviations (SD), and Correlations of Items in the Measurement Model.
Predictive Validity
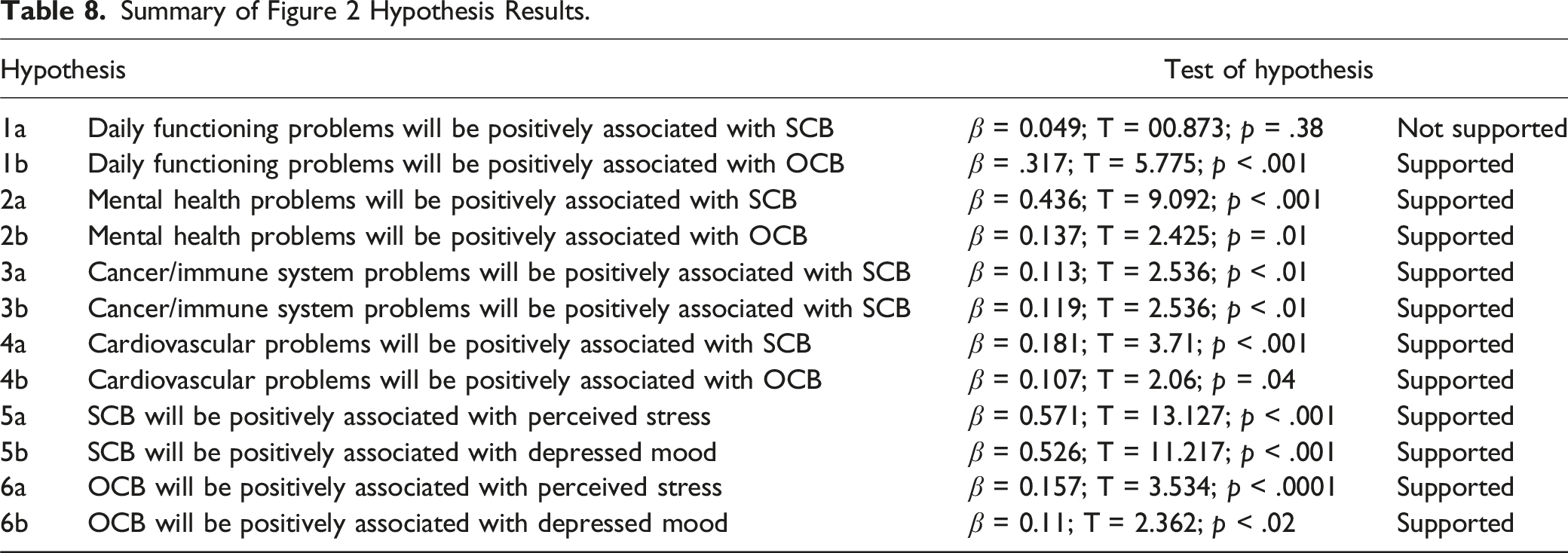
Summary of Figure 2 Hypothesis Results.
Construct Validity
The results from our analysis of the structural model used to establish construct validity of our measures including path coefficients and significance levels are shown diagrammatically in Figure 2. Results of hypotheses testing are provided in Table 8. The results from this phase of the analysis lend support to the construct validity of the CRHD.
Our analysis provided moderately strong support for our theoretical framework. Our predictors explained 26.9% of the variance in SCB, 26.9% of the variance in OCB, 28.1% of the variance in perceived stress, and 24.9% of the variance in depressed mood. As noted in Table 8, all but one of our hypotheses were supported by our data. Three of the four CRHD subscales (i.e., those quantifying the demands placed on the caregiver of caring for someone with mental health problems, cancer/immune system problems, and cardiovascular problems) are all significantly associated with increased perceptions of burden for the caregiver. Providing care to someone experiencing daily functioning problems was also a significant predictor or OCB but not, as hypothesized, SCB. The fact that H1a is not supported by data is unexpected given research in the area suggesting that conditions such as daily functioning issues tend to generate high caregiver burden (Kawaharada et al., 2019). It may be that caregivers view care provision associated with daily functioning as “spending time with a loved one” during the end stages of life; in prior qualitative interviews with caregivers, end-of-life caregiving has been described as “meaningful” and “a privilege” (Woodman et al., 2016).
Discussion
The research was designed to address the lack of evidence linking the relationship between care-recipient health and caregiver well-being. To achieve this goal, we undertook a comprehensive research project that had two distinct phases. In Phase 1 of the research, using an extensive literature review process and a panel of key stakeholders and content matter experts, we identified 18 care-recipient health conditions that encapsulated the breath of caregiver duties pertaining to specific recipient health conditions. These 18 items included a range of common eldercare health issues such as mental health issues, cancer, breathing problems, and difficulties with daily functioning.
In the second phase of this research, we developed and empirically validated a research instrument that allows researchers and practitioners to (1) identify whether the caregiver was providing care to an individual who suffered from one or more of 18 health conditions common in the elderly and (2) quantify the demands imposed on the caregiver of caring for someone with this health issue. Factor analysis determined that 11 of these 18 health conditions could be grouped into four different constructs each of which measures the demands placed on the caregiver of caring for someone suffering from several closely related health conditions.
When we look at the results obtained using the four subscales of the CRHD, we note that caregivers of individuals with cardiovascular health issues who are on special diets perceive the highest demands on their time and emotional energy (M = 2.7) while those caring for someone with cancer/a compromised immune system perceive fewer demands (M = 1.6). The demands caregivers perceive that are imposed on them when caring for someone with the other two clusters of health conditions, mental health problems including dementia (M = 2.4), and challenges in execution of daily functioning activities (M = 2.14) are in between these two extremes. We speculate that these differences in demands on the caregiver’s time and energy may be in part attributed to the amount of support caregivers in each of these groups receive from the formal health care system people. Future research in this area is, however, needed to help us understand why caregiver demands vary with the care-recipients’ health circumstances.
Examination of how measures performed in the nomological model that was used to validate our scale engenders several important observations. First, caring for someone with daily functioning issues (a cluster of health problems associated with aging that include difficulties walking, engaging in daily self-care activities, infections such as shingles, cystitis, and incontinence, and constipation) is a significant predictor of objective but not subjective caregiver burden. Caring for someone with these types of issues imposes physical (β = .317) but not emotional (path not significant) demands on the caregiver. Second, while caring for someone with mental health challenges (dementia, anxiety, depression, behavioral problems including acting out, swearing, and engaging in uncooperative, aggressive behavior) imposes both emotional and physical demands on the caregiver; in this case, the demands are more likely to be emotional (β = 0.436, p < .001) than physical (β = 0.137, p < .01). Similar findings were obtained for the relationship between caring for someone with a cardiovascular health condition and caregiver burden. Again, we note that the demands facing those caring for someone with this set of conditions are more likely to be emotional (β = 0.181, p < .001) than physical (β = 0.107, p < .04). Third, caregivers of elderly individuals with cancer whose immune system is compromised are equally likely to find such caregiving physically (β = 0.113, p < .01) and emotionally (β = 0.119, p < .01) demanding. It should, however, be noted that the paths between caring for someone with these conditions and both types of burden are lower than observed with the other health conditions.
In summary (1) caregivers of individuals with mental health issues were the most likely to experience SCB (emotional strain from caregiving), (2) caregivers who provided help with daily functioning were the most likely to experience OCB (i.e., physical strains from caregiving), (3) the relationship between caring for someone with daily functioning issues and SCB was not significant, and (4) the relationship between caring for someone with cancer/immune system problems and SCB is stronger than the relationship observed between providing this type of care and OCB. Finally, our study (see Figure 2) provides strong support for the idea that SCB (i.e., the emotional dimension of caregiving) is a more important predictor of employee well-being (stress and depression) than is OCB, a finding that has been reported in other studies (Duxbury & Higgins, 2017). This is important as it points to the need for programs that provide emotional support to informal caregivers.
Conclusions
The research summarized in this paper was motivated by researchers’ need for a tool to help them (1) understand how caregiver recipient characteristics impact caregiver well-being, (2) determine how often caregivers are providing care for an individual with more than one illness, and (3) identify the demands placed on the caregiver of caring for someone experiencing health conditions other than dementia and cancer. The results from this study indicate that we have accomplished these goals and reinforce our assertion that it is important that researchers and practitioners understand how the condition of the care recipient can differentially affect caregiver outcomes. Our research also provides strong support for the idea that caregiver burden (both forms) and psychological well-being is influenced by a care-recipients’ health condition. The following conclusions are supported by the data.
First, the measure developed and tested in this paper provides researchers and practitioners with a tool that can be used to enhance our understanding of the relationship between care-recipient health and caregiver burden/well-being. Our measure allows researchers to capture the diversity of the caregiving experience—both in terms of the most common types of care being provided by caregivers to care recipients as well as the demands inherent in caring for someone with a particular health condition. As such, it should have utility for researchers who are exploring the etiology of caregiver well-being as well as practitioners who are charged with designing programs to help employed caregivers cope with work-caregiving conflict. Second, our analysis determined that certain health problems of the elderly tend to occur together which supports the need to expand our research agendas to examine the challenges of caring for someone with several different health problems at the same time. Third, our research shows that the emotional, physical, and time-related demands placed on the caregiver vary according to the health condition(s) of the care recipient.
Our measures give key stakeholders a tool that they can use to better understand the relationship between the different health conditions and the type of burden (emotional vs. physical) imposed on the caregiver. Our scale allows researchers to examine this relationship in a multitude of ways. They can either look at the data on how the caregivers rated the demands imposed on them by the 18 different conditions included in our measure or they can use the four subscales of the CRHD to identify demand by co-occurring health conditions. The value of the information that this tool can provide researchers and practitioners can be expected to increase concomitant with the number of caregivers in our population.
Finally, Schultz et al. (2020) noted that many interventions studies within the caregiving literature were parsed based on (1) the underlying disease of the care recipient, (2) delivery mode (i.e., technology-based vs. human; individual or groups), or (3) intervention target (i.e., caregiver and/or care recipient; family; home environment; workplace). Our measurement tool enhances researchers’ ability to evaluate these different interventions and delivery modes on a more comprehensive set of underlying disease(s) experienced by the care recipient.
Limitations and Directions for Future Research
This paper has several limitations. First, two of our subscales include only two items, which may limit construct validity. Second, 7 of the 18 care-recipient health conditions were removed from the analysis due to poor loadings. While the poor performing items were generally observed to be uncommon health conditions (i.e., dialysis), or multidimensional conditions that are symptoms of various comorbidities (i.e., poor sleeping and weight loss) that were unlikely to load on just one factor, the fact that they were not included in our scales is a potential limitation of this study as our findings did not reflect theorized conceptions put forward by our review and panel of experts. Additional research with different samples will increase our understanding as to whether our results are sample specific or in fact provide an accurate representation of key care-recipient conditions that need to be considered in future research.
Third, our study focused on family members with full-time employment (who are relatively well-paid and well-educated) who provided informal caregiving to elderly dependents. As such, the tool developed in this study is limited to only caregivers (albeit a large and growing group of people) who fulfill these criteria. We encourage other researchers to follow the research methodology outlined in this paper to develop measures that can be used to further our understanding of the relationship between care-recipient health and the well-being of other types of caregivers (e.g., those caring for disabled children or adults, older caregivers who are no longer in the labor market, social workers, councilors, and those with less education and lower incomes). Development of a diverse set of measures will allow researchers to better understand how caregiver context impacts caregiver outcomes such as stress and depression. Development of a measure such as the one presented in this paper but targeted at formal caregivers (e.g., those working in long-term care facilities, psychologists, social workers, nurses, and doctors) would, for example, support research exploring the relationship between care-recipient health and the demands placed on those professionals whose job it is to care for the elderly. Such information could also help hospitals and long-term care facilities with staffing decisions.
Finally, our measure asked respondents to assess the level of demands (i.e., time, energy, and emotional) that caring for someone with each of the conditions included in our measure places on them in a typical month. Unfortunately, this wording (which was done to reduce respondent burden and provide researchers with an omnibus measure of caregiver demands associated with care-recipient health) means that we cannot explore either the relationship between care-recipient condition and the incidence of each of these indicators of demands. Nor can we determine the extent to which each of these forms of demand predicts different outcomes. Future research in this area is needed to explore these issues.
There are a variety of ways that researchers can build on and use the measures developed in our study. While we embedded our measures within a model derived from the well-being literature to test their validity, we encourage researchers to include our measures in other theoretically driven nomological networks which will not only help to validate the measures but could provide insights into the relationship between care-recipient health, caregiver strain and key outcomes of interest to employers (e.g., absenteeism, intent to turnover, and use of Employee Assistance Programs) and therapists (marital satisfaction and family conflict) as well as theoretically relevant moderators and mediators of the relationship between demands and outcomes (e.g., flexible work arrangements, meditation, and cognitive behavioral theory protocols).
Implications for Practitioners
Schultz et al. (2020) concluded their review of the caregiving literature with two observations of relevance to this study. First, they found that findings regarding the impact of different interventions are mixed and depend very much on the context surrounding the individual’s caregiving situation. Second, they point out that intervention efficacy is likely to be enhanced when tailored to the specific needs of the caregiver. The measure presented in this paper gives practitioners a tool they can use to evaluate the links between the care-recipient’s health conditions/the demands these conditions impose on the caregiver (i.e., the context of care) and the efficacy of various types of interventions (e.g., psychosocial, meditative, cognitive behavioral theory, and respite care) at managing caregivers’ response to caregiving. Information gathered from research using this tool will prove valuable to health care practitioners (psychologists, social workers, therapists, and physicians) as they seek to help eldercare providers cope with the demands (emotional and physical) this labor of love imposes on them.
The tool developed in this study also allows practitioners to evaluate the extent to which various types of training benefit caregivers dealing with different care-recipient health conditions. Such information should help the caregiver themselves identity potential or actual “resilience” strategies to help them manage the demands of the role as well as the health care practitioners whose job it is to counsel caregivers and offer viable ways forward to those in distress.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the SSHRC/CIHR Partnership Grant FRN: HWP – 146001 (CIHR); 890-2016-3018 (SSHRC) entitled: “Mobilizing a Caregiver-Friendly Workplace Standard: A Partnership Approach” and a CIHR grant through the Canadian Consortium of Neurodegeneration and Aging (CCNA).