
Abstract
Objectives
The aim of this study is to understand the demographic and situational characteristics of men over 55 who have used a community support service.
Introduction
Health care utilisation practices and patterns amongst men experiencing mental health struggles are complex (Sagar-Ouriaghli et al., 2019). Although men’s mental health has received greater academic and policy attention in recent years, there is still limited research carried out in the UK that explores men’s engagement in mental health services. Furthermore, most research on men’s mental health and use of social services has tended to look at men in general, with few studies examining service use factors within subgroups of men (Addis & Mahalik, 2003; Galdas et al., 2005).
Mental health service use in older people requires further attention. The Adult Psychiatric Morbidity Study (2014) found that older people with Common Mental Disorders (CMDs) had the lowest rates of psychological therapy and unmet treatment requests which could suggest that older people may find it difficult to ask for what they need or may not even be aware of what mental health support is available to them (McManus et al., 2016, p. 100). In addition, older men with CMDs are less likely than women to be using treatment in part due to the longstanding stigma or reluctance to talk about mental health or to seek mental health help (McManus et al., 2016, pp. 100–101). Qualitative research has also found that older men may hold traditional masculine attitudes which view expressions of distress and help seeking as a weakness (Apesoa-Varano et al., 2015).
Past research has attempted to categorise predictors of help seeking attitudes, behaviours, and service use into conceptual models, for example, the Andersen Behaviour Model of Health Service Utilization (1968) has been extensively applied across sociological exploring health service use studies of Andersen (1995); Babitsch et al. (2012); Gagne et al. (2014); Parslow & Jorm (2000); Roberts et al. (2018). The framework has allowed for the discovering of conditions or factors that either facilitate or impede the use of health care services. The model suggests that an individual’s access to, and use of health services is shaped by: A) Predisposing factors (a consequence of sociodemographic characteristics such as age and gender, social structure, attitudes and beliefs). B) Enabling factors that facilitate or impede service utilisation (such as personal/family situation and the quality of social relationships, finances, travel, community enabling factors which include available health personnel and facilities, and other additions such as genetic factors and psychological characteristics). C) Need factors (objective measures and subjective perceptions of health needs, from functional and health problems that generate the need for health care services)
Recent systematic reviews examining the factors associated with the use of health services for mental health and emotional problems (notably CMD and major depression) have applied Andersen’s Behavioural Model of Health Services framework (Magaard et al., 2017; Roberts et al., 2018). Roberts et al. (2018) identified several studies that focused on the association between Andersen’s predisposing, enabling and need factors and help seeking for CMDs, finding need factors to be most associated with service use for CMD symptoms. Notably, having previously sought mental health treatment was generally associated with the increased likelihood of seeking treatment (Gwynn et al., 2008; Iza et al., 2013). Magaard et al.,’s (2017) systematic review investigating the individual and contextual characteristics associated with professional help seeking for emotional problems found that being a young or an older adult, being male, belonging to certain ethnic groups and having lower educational status were predisposing factors that were most likely to decrease help seeking behaviour. Using Andersen’s (1995) behavioural model in their analysis, Parslow and Jorm (2000) found that when controlling for variables associated with need for mental health services (e.g. psychological distress or diagnosed mental disorder), the sociodemographic variables strongly associated with service use were, being female, level of education and being separated.
In this paper, predictor variables are grouped according to Andersen’s Behavioural Model of Health Services Use (Andersen, 1995), as identified in the methods section. Like Magaard et al. (2017), this paper agrees with Andersen’s reasoning that social support can facilitate or impede help seeking behaviour and therefore assist as an enabling resource (Andersen, 2008), thus placing social support as an enabling factor in this analysis. Furthermore, previous research has found that being exposed to stressful life events can trigger distressful moods and depression (Kessler, 1997) and that the more life events experienced, the more likely one is to use mental health services (Sherbourne, 1998). As Andersen’s (1995) model describes above, enabling factors are those that facilitate or impede service utilisation, with examples including personal/family situation, quality of relationships, and finances. In the APMS14 there are several stressful life events variables that represent personal/family situations, social relationships, finances, and psychological characteristics which can both facilitate and impede help seeking. With limited research on the impact of life events on service use amongst older men, this research will also explore the influence of stressful life events as an enabling factor.
Other research has sought to identify sociodemographic and social circumstantial measures associated with mental health service utilisation. Focussing specifically on the interaction between age, gender, marital status, and education on help seeking attitudes, Mackenzie et al. (2006) recognise how previous work has found that older adults and men are much less likely to seek professional help when needed. Their findings challenged growing ageist assumptions and found that older adults’ help seeking attitudes were generally more positive than younger adults, and this was most notable in single participants (p. 579). A consistent finding across research examining help seeking factors is that individuals who are single, separated, or never married are more likely than married individuals to seek help from mental health professionals (Doherty & Kartalaova-O’Doherty, 2010; Kessler et al., 2005; MacKenzie et al., 2006).
Much previous qualitative and quantitative research focussing specifically on men’s use of mental health services has explored the influence of masculine beliefs or attitudes (Addis & Mahalik, 2003; Galdas et al., 2005) with few studies examining contextual/situational factors and help seeking behaviours. Doherty & Kartalaova-O’Doherty (2010) examined the sociodemographic and health status factors that predict help seeking for self-reported mental health problems for males and females from a GP. They found that out of sociodemographic factors, marital, employment and educational status were negatively associated with help seeking behaviours for male respondents with self-reported mental health problems. Yousaf et al.,’s (2015) systematic review of studies on help seeking in men categorised factors as either psychological (e.g. cognitive or emotional) or contextual (e.g. health service related and sociodemographic). Their review included studies where contextual sociodemographic factors such as low educational status, young age and never married status were identified as factors negatively associated with medical help seeking behaviours (Doherty & Kartalova-O’Doherty, 2010; Koopmans & Lamers, 2007).
Several of the studies described have examined the influence of factors such as gender and age on general and mental health care utilisation for mental health problems, however, there are limited studies that have explored the factors associated with service utilisation for a specific subgroup of a population, for example, focussing solely on men of a certain age. Furthermore, studies have focused on clinical health settings such as the General Practitioner (GP) and clinical mental health services, with limited research exploring community-based support services. The current study aims to enhance the understanding of older men’s service utilisation by exploring the demographic and situational factors/characteristics of men 55 years plus who have used a community care service. Community care and support services are broadly explored because in addition to addressing specific health needs, such services support social wellbeing generally, in which predisposing and enabling factors may have more influence. In the hope to add to the vast amount of qualitative research that has focused on masculine beliefs, attitudes, and behaviours, the following research question is addressed in this article: Under what social circumstances do older men (55+) use community support services?
Method
Secondary Data: The APMS 2014 Survey
Data from the Adult Psychiatric Morbidity Survey (APMS) 1 2014 – a general population survey of adults living in private households in England, United Kingdom – was used in this study. A main objective of the survey is to estimate the prevalence of psychiatric morbidity according to diagnostic category, including assessment of common mental disorders, psychosis, autism, substance misuse and dependency, and suicidal thoughts, attempts, and self-harm (McManus et al., 2016). The survey series is carried out every 7 years and was designed to be representative of the whole population in England (data is not collected from Wales, Scotland or Northern Ireland). Further details on the APMS 2014 methodology, sampling strategy and how weighting was carried out to account for selection probability and non-response are available elsewhere (see McManus et al., 2016).
In brief, APMS 2014 adopted a multi-stage stratified probability sampling design where one adult aged 16 or over was randomly selected for interview in each eligible household in England. The final dataset consisted of a sample of 7546 individuals and a comprehensive list of measures (over 1000 variables) (see McManus et al., 2016).
The APMS series 2 has a wide range of variables and so can be used to explore various issues relating to mental health. Many studies using APMS 2007 and APMS 2014 survey data have focused on specific subgroups, for example, UK armed forces veterans (Roberts et al., 2019), informal carers (Stansfeld et al., 2014), and black ethnic minorities (Qassem et al., 2015), to name a few. To the author’s knowledge, however, there have been no studies using any of the APMS series that has concentrated entirely on male respondents in the sample.
As well as assessment of psychiatric disorders, the APMS 2014 survey also collected demographic and socioeconomic characteristics and information on treatment and health service use, stressful life events, discrimination, social relationships, and social support.
Measures
Dependent Variable – Measure of Community Support Service Use
As part of a wider study that explores specifically older men’s use of community self-help/support groups, the research interest is in older men’s use of community support groups. However, due to low cases within the dataset (12 men aged 55 years plus reported using a self-help/support group), this article will take a broader look at community care and support services. A derived variable ‘anycdar’ (have you used any of these community care or day activity services in the last year – coded = Yes, No) was selected as the key indicator of use of community support services. It was derived based on survey respondents having used any of the following community services: community mental health centre, day activity centre, sheltered workshop, psychiatrist, psychologist, community psychiatric nurse (CPN), community learning difficulty nurse, other nursing services, social worker, self-help/support group, home help/home care worker, outreach worker/family support.
Predictor Variables
The APMS 2014 contains several possible predictor variables that could be considered as predisposing, enabling and need factors, as described in the theoretical framework section. Variables were recoded or merged to make variables with multiple values as binary and relevant as possible, for example, marital status was recoded from 6 values to just 2 values. Factors which have previously been found to influence help seeking behaviour were coded with higher values.
Predisposing Factors
Variables included age (in older age categories), marital status, ethnicity, and education status. Age was measured in categorical groups (55–64, 65–74, 75–84, 85+ years). Marital status was recoded to be categorised as: 1 = In a relationship (including, married, cohabiting) and 2 = Single (including widowed, divorced, separated). Education level was categorised as: 1 = Degree and professional qualification, 2 = A Levels, 3 = GCSE or equivalent, 4 = Foreign or other, 5 = no qualifications. Ethnic origin was recoded to just two categories: 1 = White, 2 = BME and mixed ethnic group.
Enabling Factors
Included employment status (1 = In employment, 2 = Unemployed, 3 = Economically inactive), whether respondent perceives themselves to have money problems (0 = No – No problems at all, 1 = Yes – Slight problems, definite or very severe problems), the number of significant stressful life events respondent experienced (1 = 0-1 stressful life events, 2 = 2+ stressful life events), and whether they get on well with family and other relatives (0 = no, 1 = yes).
This stressful life events variable was derived from 21 different stressful life events. 3 The APMS14 used the standard measure ‘LTE: List of Threatening Experiences’ to assess stressful life events. Previous research has found that the LTE is a valid and reliable measure of stress in mental health (Mortrico et al., 2013). Some life events are more stressful than others and maybe more powerful predictors of use of community mental health services. One way to examine this is to run relative risk ratios for each of these stressful life events to see which one or ones are most likely to predict use of community support services. Associations between these separate variables and the dependent variable were checked and those found to be significantly associated with the dependent variable were merged into a variable that totalled together the number of stressful life events a respondent had experienced ranging from 0–7 life events. 4 This was transformed into a binary variable using a median split, which resulted in two groups: 0-1 stressful life events experienced and 2 or more of these stressful life events experienced.
Need Factors
Included whether the respondent had a CMD present, defined as a score of 12 or more on the Clinical Interview Schedule-Revised (CIS-R), whether respondent self-reported having ever experienced a CMD ever (0 = no, 1 = yes), good/fair or poor health in general, whether respondent had spoken to the GP about a mental, nervous or emotional problem in the last 12 months (0 = no, 1 = yes) and whether they were currently receiving counselling for a mental, nervous, or emotional problem (0 = no, 1 = yes).
Statistical Analysis
All data analyses were performed using IBM SPSS (version 28). To generate nationally representative estimates, the complex study design and sample weighting were taken into account in all the analyses. Female respondents were excluded from the dataset and the remaining male respondents were filtered by age 55 and above, leaving 1253 to be included in the analyses. Descriptive statistics were obtained in relation to all potential variables of interest. Chi-squared tests were carried out between chosen predictor variables and the community support services dependent variable. Variables that were significantly related at the p < .05 level were included in the binary logistic regression analyses. Then, hierarchical logistic regression analyses were used to explore the associations between different factors and the use of community support services among men over 55 because of the dichotomous nature of the dependent variable. Multicollinearity was checked, and found not to be a problem, with the Variance Inflation Factor (VIF) for all variables below 2 and tolerance values higher than .5.
Results
Sample Characteristics
From the data of 1253 male respondents over 55 years, only 8.1% (n = 102) men over 55 reported using a community service (community care or day activity service) in the last year. There were only a small number of men over 85 years of age, with 41.1% being aged 55–64, 34% 65–74 years, 19.5% 75–84 years and 5.4% 85+ years. The majority of respondents were married or in a relationship (74.3.%) and economically inactive (64.1%), with 34.8% of men over 55 years in employment at the time of survey. Only 4.4% of the sample were BME or mixed ethnic group, with the most being of white ethnicity (95.1%).
Characteristics of Older Men (Age ≥55 Years) Who Reported Using Any Community Care or Day Activity Services in the Last Year.
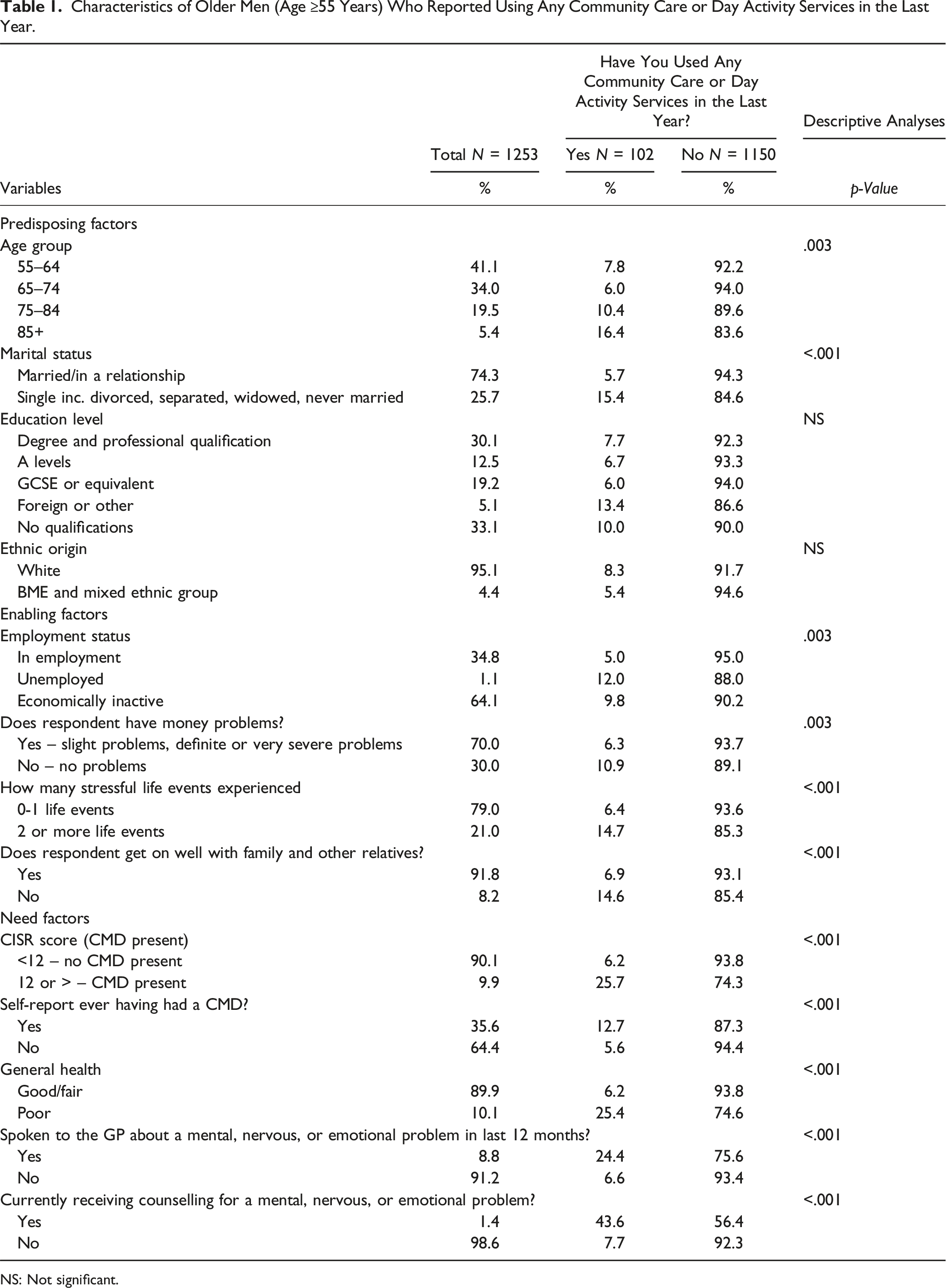
NS: Not significant.
Hierarchical Logistic Regression
The hierarchical logistic regressions focused on participants who responded Yes or No to using a community care or day activity service in the last year. The variables ‘highest education qualification’ and ‘ethnic group’ were excluded as they were found to not be significantly related to the use of a community care or day activity service within the descriptive analyses. Predisposing factors were included in block 1, enabling factors in block 2, and the variables related to need factors in block 3. The first model assessed predisposing factors, and an additional group of characteristics was added to each subsequent model until the final model was reached that included predisposing, enabling, need, and external environmental and personal health practice factors. The a priori alpha level was .05.
Logistic Regression ENTER METHOD (No vs. Yes).
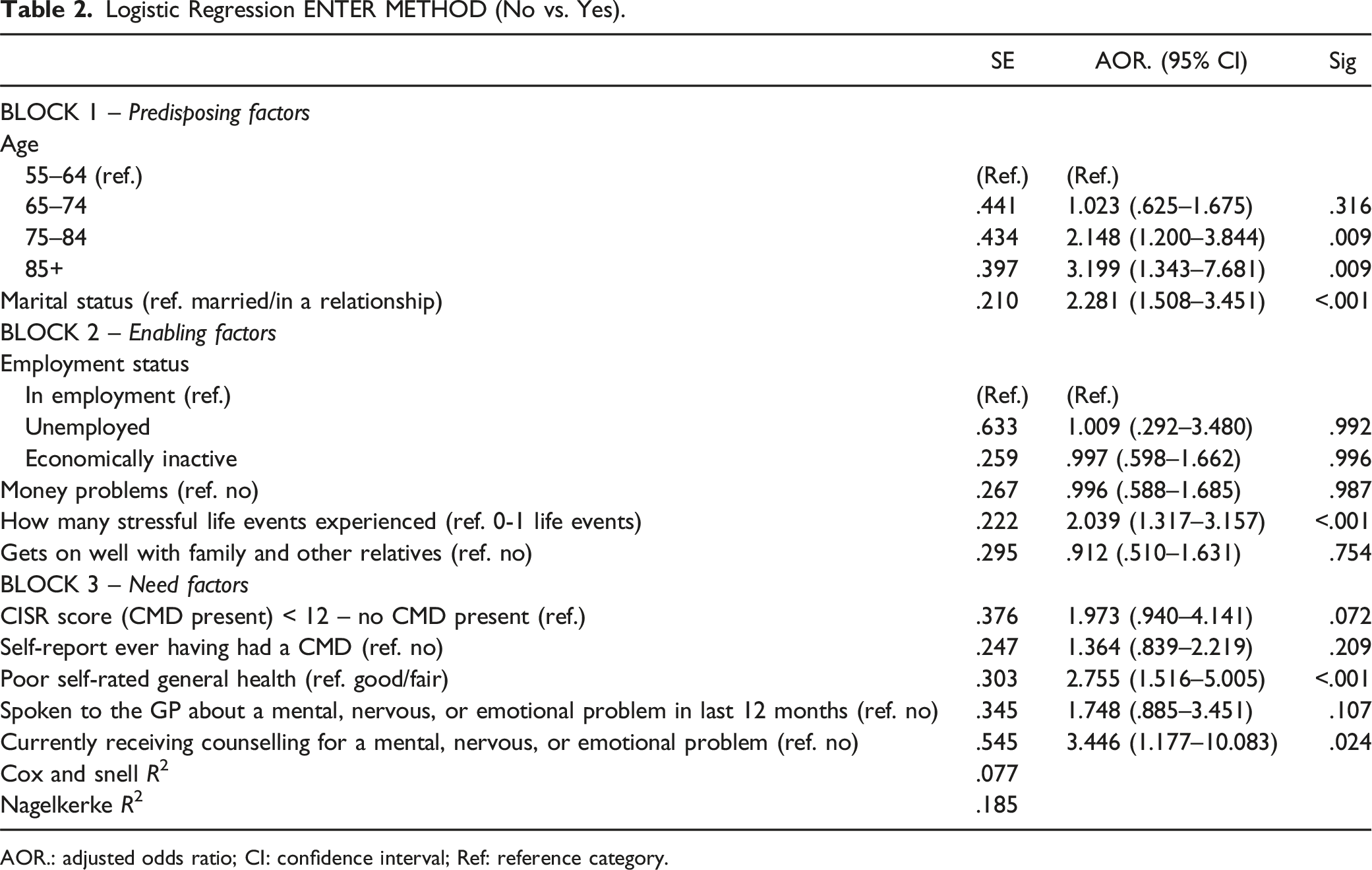
AOR.: adjusted odds ratio; CI: confidence interval; Ref: reference category.
Concerning the predisposing factors (BLOCK 1), age groups and marital status were significant within the model. Older men aged 75 years and above were more likely to report having used a community care or day activity service in the last year. Older men aged 85+ were over 3 times more likely to have reported using a community care or day activity service in the last year (adjusted odds ratio (AOR) = 3.199, p < .0.5) compared to older men aged 55–64 years. Men who were single/unmarried/divorced were over twice as likely to have used a community care or day activity service in the last year than those who were married or in a relationship (AOR = 2.281, p < .0.5).
Concerning the enabling factors, only one of the independent variables (the number of stressful life events experienced) contributed significantly to the model. Participants who reported experiencing two or more of the seven significant stressful life events used in this study were twice as likely to have used a community care or day activity service in the last year than those who had only experienced one or none (AOR = 2.039, p < .05). Employment status, reporting of money problems and getting on well with family and relatives were not significant within the hierarchical logistic regression model.
Need related factors were the strongest predictors of community care or day activity service use for men over 55. As we might expect, those or were currently having counselling or therapy for a mental, nervous or emotional problem (AOR = 3.446, p < .05), were more likely to have used a community care or day activity service in the last year. Currently having counselling was the strongest predictor in the model with an odds ratio of 3.446, meaning that men who were currently having counselling were 3 and half times more likely than those who were not currently having counselling to have also used a community care or day activity service in the last year. Self-reported general health was also a significant predictor having used a community care or day activity service in the last year (AOR = 2.755, p < .05). Men who reported poorer general health were nearly 3 times as likely to have used a community care or day activity in the last year compared to those men with Good or Fair general health. Having a CMD present, or self-reported ever having a common mental disorder in their lives was not significant within the binary regression model and neither was having previously sought help from the GP about a mental, nervous, or emotional problem in the last 12 months.
Discussion
Findings presented are consistent with previous data on mental health service use amongst older males. To the author’s knowledge, this is the first study to explore factors that predict men’s (aged 55+) use of community care or day activity services such as community mental health centre, day activity centre, sheltered workshop, psychiatrist, psychologist, community psychiatric nurse (CPN), community learning difficulty nurse, other nursing services, social worker, self-help/support group, home help/home care worker, outreach worker/family support. Exploring the use of a wider range of community support services amongst a specific age group of men is important for the planning and development of health and social care services. The findings indicate that being over 85, single, divorced, or widowed, having experienced several certain stressful life events, poorer general health, and currently having counselling or therapy are strongly connected to use of community care or day activity services.
First, of predisposing factors, older ‘old’ men (85+) were more likely to have reported use of a community care or day activity service than men aged 55–64 years. This is consistent with studies that have found that older adults have more positive attitudes to help seeking than younger people (Mackenzie et al., 2006). In addition, it coincides with reports that increased age is related to higher need for mental health services, yet this may refer to the greater use of all medical services generally (Parslow & Jorm, 2000; Rabinowitz et al., 1999). As such, men in this age category are likely to have a higher need for support such as use of home help/homecare worker, other nursing services, social worker, and day activity centres, which were included within the derived dependent variable. Second, older men who were single, divorced, widowed, or never married, were twice as likely as those married or in a relationship to report having used a community support service in the last year. This aligns with previous research that found that respondents who were married and cohabiting had increased odds of not using mental health services (Byers et al., 2012). This is likely because of the support and companionship that is found in a spousal relationship. Often in couples, married or living together, there is a particular relationship that allows an individual to feel secure, safe, supported and loved (Hagerty et al., 2002). Thus, it may act as a buffer against emotional difficulties. Other research has suggested that respondents in relationships receive social, emotional and informal mental health support from their partners (Vogel et al., 2007), rather than needing to use professional services. In contrast, losing a spouse through death, separation or divorce can increase emotional distress (Peters & Liefbroer, 1997; Simon, 2002), pointing to an increased need for the support services found in the outcome variable, which also might explain the findings.
Third, looking at enabling factors, the likelihood of reporting use of a community care or day activity service in the last year increased when men over 55 has experienced two or more (of seven) stressful or traumatic life events such as serious illness or serious assault, major financial crisis, time in prison, bullying, violence in the home, sexual abuse, or being homeless at any time in their lives. The more of these traumatic life events they had experienced the more likely they were to have been in touch with a community support service. Given that the impact of such traumatic life events is likely to have a strong association with mental health and wellbeing over the life course (Marmot & Wilkinson, 2005), it is not surprising that this is a significant predictor. However, it is worth commenting on the lack of importance of death of a family member or close relative, and divorce or separation, as a life stressor for older men, particularly as previous qualitative research has found that being single (widowed or separated/divorced) and living alone contributes to feelings of loneliness (Willis & Vickery, 2022). One explanation for this could be that as the population ages and becomes more connected, both socially and economically, there has been an increase in older adults marrying and divorcing (ONS, 2017), resulting in it becoming a more normalised life event. Further, women generally live longer than men, meaning men are less likely to become widowers.
Unlike previous research (Doherty & Kartalova-O’Doherty, 2010), employment status and money problems were found not be significant enabling factors within the model. Some studies have previously found that male respondents who were unemployed or had long-term sickness were more likely to seek help than their employed male counterparts (Doherty & Kartalova-O’Doherty, 2010), and this is likely due to situations such as unemployment and long-term sickness lead to poorer physical and mental health (Ohrnberger et al., 2017) thus increasing the need for support. An interpretation of the findings is related to the age of respondents and the majority being economically inactive (at the time of survey), which is likely due to many participants falling into the retirement age category. It is perhaps surprising that getting on well with family and other relatives was found to not be a significant influence in the model, given the strong relationship previously found between social ties, social interactions and mental health (Turner & Brown, 2010). This highlights the nuances around help seeking attitudes compared with actual help seeking behaviour. It might be that men in these older age categories have fewer family ties, due to a variety of reasons including loss of spouse and close ties, geographical circumstance, and estrangement (Willis & Vickery, 2022).
Finally, consistent with previous studies (Gwyn et al., 2008; Iza et al., 2013; Roberts et al., 2018), need factors were the strongest predictors of having used of a community care or day activity service in the last year. Studies have found that having previously sought mental health treatment was generally associated with the increased likelihood of seeking further mental health support (Gwyn et al., 2008; Iza et al., 2013). Aligning with such previous research, this study found men over 55 years who were currently having counselling or therapy for mental, nervous or emotional problem were many times more likely to have also used a community care or day activity service in the last year compared to those who were not having counselling or therapy. As noted, the dependent variable (used any of the community care or day activity service in the last year) did include support such as psychologist, psychiatrist, community psychiatric nurse, support services which also offer types of counselling or therapy. Furthermore, such services, (as well as social workers and mental health day centres) may help older men to seek out alternative mental health support such as counselling and therapy, and thus be a contributing factor to the use of both services. In contrast to previous research (Doherty & Kartalova-O’Doherty, 2010), seeking help from a GP for a mental, nervous, or emotional problem was found to not be a significant predictor of community support service use in the model yet was found to have a significant association in the descriptive analyses.
Previous research has found that need factors such as having a CMD present are most associated with use of health services for CMD symptoms (Roberts et al., 2018). Respondents in this study with a CMD present (CISR score of 12 or more, based on the interviewer administered clinical interview schedule-revised questionnaire) were more likely to have used a community support service in the last year, and this is to be expected as these community services are aimed at supporting those experiencing a range of mental health issues, including depression and anxiety. However, this did not contribute significantly to the model.
The analyses here show that a man’s (55+) self-reported general health status affects the odds of using a community care or day activity service in the last year. Men with good/fair general health were less likely to have used a community care or day activity service in the last year, and those with poor general health are more likely to have. Physical general health and mental health are found to be strongly linked (Ohrnberger et al., 2017) and having an existing physical health problem increases the likelihood of also seeking mental health help from the formal health care system (Rabinowitz et al., 1999).
Limitations
Although this study is novel in its exploration of men over 55 from the Adult Psychiatric Morbidity Survey 2014, there are key issues that limit how much the findings can be generalised further. First, although the APMS14 was based on a national probability sample and involved high-quality self-completion questionnaires and face-to-face interviews, the dataset was not designed to explore the topic at hand. Community support and treatment use was only a small part of this large survey, meaning the questions asked and prominence given to exploring community support services would not be the same as if the author were carrying out the study themselves.
Second, the APMS 2014 is 9 years old. Older men’s characteristics and use of community support services might have changed in recent years, with the population ageing, and during and post-COVID-19, whereby several such services have been reduced or cut back. In respect to the survey’s limitation, bias due to non-participation is unavoidable. Although the APMS is a cross-sectional survey that uses a high-quality general population sample, being an essential source for prevalence and profiling, conclusions about causality cannot be validly drawn.
Despite this, the study ventured to make the best use of the available – albeit limited-data on the topic area of older men’s mental health and community support service use. While the dependent variable is not ideal in terms of specificity, it still provides a broader insight into community mental health support service use by older men than currently available from published research. Although there are increasingly more quantitative studies that have examined men’s (mental) health service utilisation, what this paper highlights is a need for studies to be conducted exclusively addressing the issue of older men’s (55+) contact with mental health community care and support services, specifically with a larger sample of men in that age cohort and using variables addressing cultural enabling factors, as well as demographic and situational variables. It further highlights areas for specific focus within qualitative research in the field of men’s mental health help seeking, for example, reasons older single men might be more likely to have used a community support service than those in a relationship.
Implications
The findings highlight the need for health and social care practitioners and professionals to consider demographics and social circumstances when supporting specific groups of men with service utilisation. Fundamentally, need factors are often seen as most important in influencing service use and will ultimately drive service provision targeted at specific groups. This study further highlights other really important factors, notably in the categories of predisposing and enabling factors, such as age, marital status and circumstance. That older men 75+ were more likely to have used a community care or day activity service in the last year than men aged 55–64 years was promising, suggesting that those older men who may have a higher level of support need were likely to have received it. The association between marital status and community support service use supports the use of low-cost interventions, such as self-help/support groups, day care activity services and mental health centres in providing support to single older men who might be at risk of loneliness, social isolation and exclusion (Steptoe et al., 2012). The low rate of self-help/support group use in men 55 years plus might, however, reflect the lack of availability and awareness of such support groups or that older men were less likely to use, or report, using them. This points to the need to assess whether there are enough and different types of community support services to meet the needs of older men who may be struggling with emotional problems. In conclusion, the findings and discussion presented suggest that more attention needs to be paid to mental health community support treatment and service use of men of specific age cohorts.
Footnotes
Acknowledgements
This article reports on independent research funded by the National Institute for Health Research, School for Social Care Research (NIHR SSCR). The views expressed in this publication are those of the author and not necessarily those of the NIHR SSCR, the National Institute for Health Research, nor the Department of Health and Social Care. Sincere gratitude to the funder for supporting this research and to NHS Digital for granting permission to use the APMS data. Many thanks also to the post-doctoral fellowship mentor, Dr. Demi Patsios, for his support throughout.
Author’s Note
This research was hosted by The School for Policy Studies, University of Bristol, UK.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a research grant from the NIHR School for Social Care Research, England 2021–2023 (Reference 102645/CM/UBDA-P188).
Data Availability Statement
The data that support the findings of this study are available from NHS Digital. Restrictions apply to the availability of these data.