
Abstract
Introduction
The threat of illness from COVID-19 and the public health measures implemented to contain the pandemic were possible sources of stress for older people (Arpino et al., 2021; Kasar & Karaman, 2021). In this study, we consider the effects of coping strategies used by older adults to mitigate the early stressors of the pandemic in Aotearoa/New Zealand (NZ).
Globally, confinement potentially induced feelings of anxiety and isolation (Ammar et al., 2021; Brooks et al., 2020). Additionally, stressors such as job loss and food insecurity may also have long-term repercussions in terms of mental and emotional well-being (Officer et al., 2022). As age was related to more severe outcomes of COVID-19 infection (Fang et al., 2020), the public health measures were expected to exacerbate loneliness and anxiety disproportionately among the older adult population (ESCAP, 2022; Verhage et al., 2021). Cross-sectional studies during the pandemic indicated an increase in self-reported depression and anxiety symptoms among older people (e.g., Falvo et al., 2021; Kurniawidjaja et al., 2022; Meng et al., 2020).
Following findings that older people were often less emotionally vulnerable than younger people (e.g., Dragioti et al., 2022), several studies have examined the role of coping strategies in mitigating the effects of stress on mental and emotional well-being. Qualitative studies identified coping strategies such as staying busy, seeking social support, having a positive attitude (Fuller & Huseth-Zosel, 2021), physical exercise, playing music (Chan et al., 2022), use of technology for social connection, and prior life experience (Greenwood-Hickman et al., 2021) aiding older adults in mitigating stress. However, such studies have included non-representative samples and the theoretical approach to the role of “coping” was not described.
The transactional model (Lazarus & Folkman, 1984) conceptualizes stress and coping as a series of dynamic transactions between the individual and an environmental stressor (Biggs et al., 2017) which occurs in three interrelated phases: cognitive appraisal, coping, and the outcome. Appraisal leads to the stressor being defined as benign, irrelevant, or stressful. A situation threatening loss or harm to well-being (such as potential COVID-19 infection) is appraised as stressful (Lazarus & Folkman, 1984). Following appraisal, coping is defined as an individual “constantly engaging in cognitive and behavioral modifications to manage external and internal demands of the stressor” (Lazarus & Folkman, 1984, p. 141). Coping strategies have been broadly categorized as active or passive coping strategies.
Active coping strategies, including seeking support (information and emotional) from social contacts and engaging in physical activity (Faulkner et al., 2020; Heffer & Willoughby, 2017), have been associated with better adaptation to the stressor and a positive effect on emotional well-being (Oker et al., 2022). During the COVID-19 pandemic, higher social support was associated with lower anxiety and lower financial distress (Chen et al., 2021; Liu et al., 2021; Sharif Nia et al., 2021) and with positive emotional well-being (Wilson et al., 2020) including more rapid improvement in anxiety symptoms (Fluharty et al., 2021). Isolation from social contacts during the pandemic negatively altered the perception of social support and increased COVID-19-related worries (Szkody et al., 2021). However, very little work has explored the role of social support among older people.
Physical activity has been well-established as an active coping strategy during stressful life events (Kim & McKenzie, 2014). Salman et al. (2021) reported that individuals who engaged in less physical activity during the pandemic also experienced low mood and loneliness, while individuals who engaged in physical activity reported enhanced physical and emotional well-being (Wright et al., 2021).
Passive coping strategies such as substance use (alcohol use or tobacco smoking), avoidance, and denial, aid in avoiding the stressor (Little, 2018) and are commonly used to provide momentary relief from stress-related emotions (Biggs et al., 2017) but have an overall negative impact on emotional well-being (Gurvich et al., 2021) including during times of crisis (Brown & Nicassio, 1987). International studies (e.g., Foster et al., 2021; Rao et al., 2022) reported increased alcohol consumption and hazardous drinking among older adults induced by the pandemic and public health measures. There is little evidence regarding changes in smoking behavior among older adults, although qualitative interviews indicated that pandemic-related stressors were associated with increased smoking and reduced motivation to quit (Cordon et al., 2021).
The third stage of the transactional model is the health outcome which may be negative or positive according to the cognitive appraisal and coping strategies used (Walinga, 2014). One outcome that has been widely researched in the coping literature is emotional well-being including anxiety. A systematic review of 103 early studies worldwide (Kan et al., 2021) revealed that older adults were significantly more likely to suffer from anxiety. The transactional model suggests a clear pathway from a stressor, through appraisal and the coping strategies utilized, to anxiety symptoms.
Research Aims
Aotearoa/NZ’s first confirmed case of COVID-19 was reported on February 28th, 2020. The public health response was described as going “hard” and “early” to eliminate the virus’s transmission in the community (Ministry of Health, 2020). Initial measures included enforced lockdown, no public gatherings, strict adherence to small household “bubbles,” work from home, and closure of education facilities, and these were not eased until June 2020 (Jefferies et al., 2020). Despite the successful implementation of the public health response and reduced burden of disease, the public health measures may have negatively impacted older people’s mental and emotional well-being.
The aim of the current study was two-fold; to explore whether older adults in Aotearoa/NZ perceived the COVID-19 pandemic as stressful and to investigate whether coping strategies (social support, physical activity, alcohol, and smoking) used moderated the impact of perceptions of stress on anxiety among older adults.
Was the COVID-19 pandemic perceived as a source of stress by older adults in Aotearoa/NZ?
Were there any changes in older adult’s coping strategies and anxiety between 2018 (pre-COVID) and 2020 (post-first lockdown)?
Coping strategies will moderate the relationship between stress and anxiety symptoms for older adults in 2020.
The relationship between perceived stress and anxiety symptoms will be weaker for those reporting higher social support and physical activity (active coping strategies) during 2020.
The relationship between perceived stress and anxiety symptoms will be stronger for those reporting higher alcohol use and regular tobacco smoking (passive coping strategies) during 2020.
Method
Data were collected in 2018 (pre-COVID-19) and 2020 (post-first COVID-19 lockdown) as part of the New Zealand Health, Work, and Retirement (NZHWR) longitudinal Study (Allen et al., 2019). The NZHWR has biennially surveyed a cohort of New Zealanders aged 55+ (randomly selected from the NZ Electoral Roll) since 2006. The NZHWR oversamples participants of Māori descent to represent Aotearoa/NZ’s indigenous population adequately.
Demographic Characteristics of the Study Sample in 2020 (N = 3275).
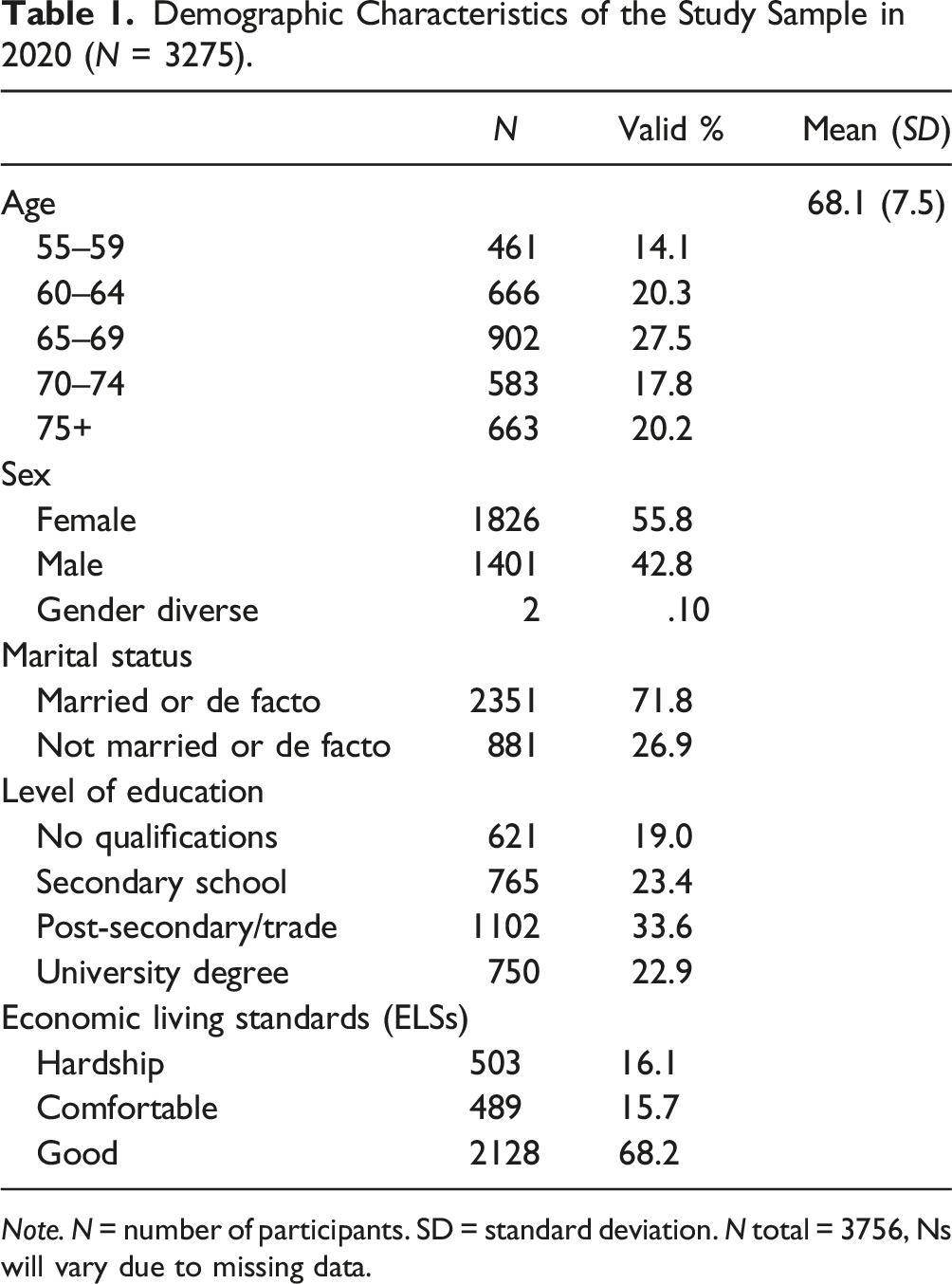
Note. N = number of participants. SD = standard deviation. N total = 3756, Ns will vary due to missing data.
Measures
Demographic Variables
Age was measured in years in 2020. Gender was coded as: 1 = male; 2 = female or gender diverse for analysis. Marital status was coded as a dichotomous variable: 1 = married or in a de facto relationship; 2 = unmarried or not in de facto relationship.
Economic living standards (ELSs) were assessed with the Economic Living Standards Index short form (ELSI-SF; Jensen et al., 2005) which aims to represent financial aspects of well-being. Scores range from 0 to 31, with scores ranging from 31 to 25 interpreted as “good,” 24–17 as “comfortable,” and 16–0 as “hardship.” The higher the score, the better the ELS (Jensen et al., 2005). In the present sample, M = 25.37, SD = 5.51, and alpha = .88.
Perceived Stress
Perceived stress induced by COVID-19 was measured using three items that assessed perceptions of the impact of the pandemic by asking:
“To what degree would you say the COVID-19 pandemic has had a negative impact on your overall: a. Physical health, b. mental health, and c. economic health.” Responses were recorded on a 5-point Likert scale ranging from 1(not at all impacted) to 5 (extremely impacted). These self-reported perceptions were used to indicate perceived stress and labelled: Physical Stress, Mental Stress, and Economic Stress.
Coping-Related Measures
Social Support was measured using the Social Provision Scale (SPS; Cutrona & Russell, 1987). SPS includes 24 items which are rated on a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). An overall score was calculated by summing scores on all items; a higher total score indicates higher perceived social support. In the present sample, M = 80.41, SD = 9.96, and alpha = .92.
Physical Activity was measured with one item adapted from the English Longitudinal Study of Ageing (Smith et al., 2015). The item categorized physical activity into vigorous, moderate, and mild on a 4-point Likert scale ranging from more than once a week (1) to hardly ever or never (4). The responses for the moderately active category (e.g., dancing and walking at a moderate pace) were used to compute a categorical dummy variable aligning with the current health guidelines recommending moderate physical activity every day as a universal goal (Yang, 2019). The dummy variable conceptualized the responses of more than once a week as high level of physical activity (1) and the responses of once a week, hardly ever, or never as low level of physical activity (0).
Alcohol Consumption was assessed with AUDIT-C (Bush et al., 1998), a brief alcohol screening instrument designed to identify hazardous drinking, by assessing the frequency and quantity of alcohol use. The three questions (How often did you have a drink containing alcohol in the past year? How many drinks did you have on a typical day when you were drinking in the past year? How often did you have six or more drinks on one occasion in the past year?) measure the frequency of drinking and typical quantity consumed, as well as the frequency of heavy drinking on occasions (Higgins-Biddle & Babor, 2018) on a Likert scale ranging from 0 to 4. The total score ranges from 0 to 12; the higher the AUDIT-C score, the higher the frequency and/or quantity of consumption. In the present sample, M = 3.54 and SD = 2.27. For females, M = 2.94 and SD = 1.91 and for males M = 4.27 and SD = 2.41.
Smoking was measured with one item, which asked participants, “If you currently consider yourself a regular smoker, how many do you think you would smoke on an average day?” For analysis, a dichotomous categorical variable was computed with the response of not a regular smoker (0) and all other responses denoted as a regular smoker (1).
Anxiety
Anxiety symptoms were measured using the short form of the Geriatric Anxiety Inventory (Byrne & Pachana, 2011; GAI – SF which comprises five items that assess anxiety symptoms in the past seven days. A forced choice response format (agree = 1; disagree = 0) for each item is summed to yield total scores ranging from 0 to 5 in which the higher scores mean higher levels of anxiety symptoms. In the present sample, M = .81, SD = 1.40, and alpha = .84.
Analyses
All analyses were conducted in IBM SPSS version 28.0.1.1 (15). Data were screened for missing values and outliers and met the assumptions of multiple regression for normality, linearity, independence of residuals, homoscedasticity, and multicollinearity. Missing data values for all variables were below the acceptable threshold of 5% (Schafer, 1999).
To answer research questions 1 and 2, paired t-tests were used to test the null hypothesis that there were no changes in coping strategies and anxiety between 2018 (pre-COVID) and 2020 (post-COVID).
Hierarchical regression was utilized to explore the relationship between perceived stress and anxiety and the moderating effects of coping strategies on the relationship between stress and anxiety in older adults. Anxiety was the DV and the IVs were entered in four blocks:
The first block included age and ELSI-SF (correlated with the DV) as controls.
The second block included Physical Stress, Mental Stress, and Economic Stress scores.
The third block included the four coping strategies: Social Support, Physical Activity, Alcohol, and Smoking.
The fourth block included 12 interaction terms (each stress variable multiplied by each coping variable) to test the moderation effect of the coping strategies on perceived stress.
Unstandardized Beta coefficients with corresponding p values were utilized to assess the contribution of the variables in the model at every step.
The ModGraph-I program (Jose, 2013) was used to plot the interaction terms to visualize significant moderation effects.
Results
Perceived Stress During the COVID-19 Lockdown
Perception of Stress on Various Domains of Health After First COVID-19 Lockdown Relaxation.

Changes in Older Adult’s Coping Strategies and Emotional Well-Being
Paired t-tests revealed no differences in Social Support, Alcohol, and Physical Activity between 2018 and 2020. The mean scores for Smoking were 1.89 in 2018 and .11 in 2020 (t (1975) = 136.14, SEM = .013, p < .001) indicating a reduction in smoking levels.
There was no change in the mean scores of Anxiety between 2018 and 2020.
Hypothesis 1: Coping Strategies Will Moderate the Relationship Between Stress and Anxiety
Summary of Hierarchical Regression Analysis for Variables and Moderators Predicting Anxiety Scores (GAI).
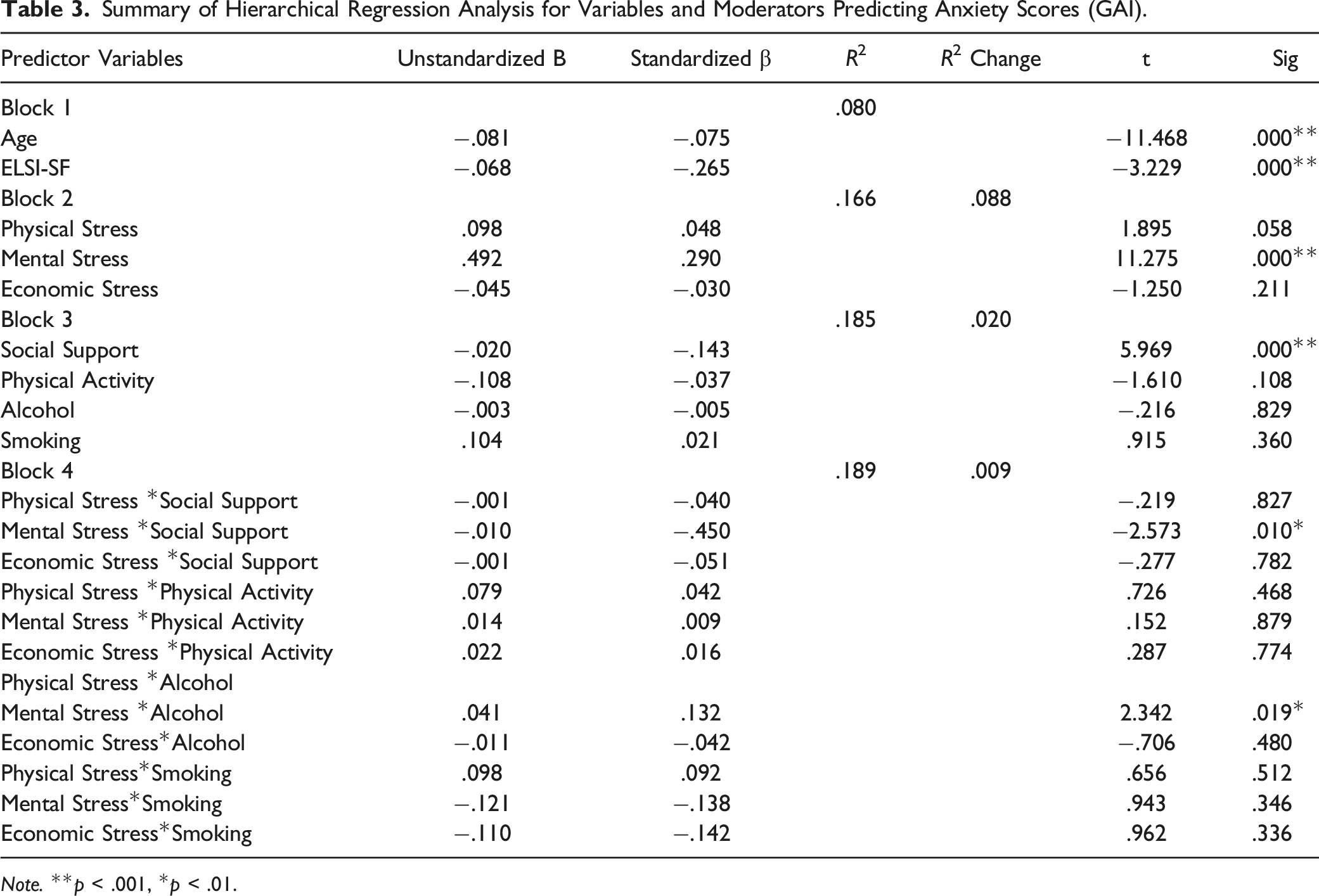
Note. **p < .001, *p < .01.
Stress measures added in the second block significantly explained an additional 8.8% of the variance (F (3, 1743) = 61.53, p < .001). Only Mental Stress contributed significantly.
Four coping strategies in the third block explained an additional 2.0% of the variance in anxiety scores (F (4, 1739) = 10.77, p < .001). Only Social Support contributed significantly to the total variance explained.
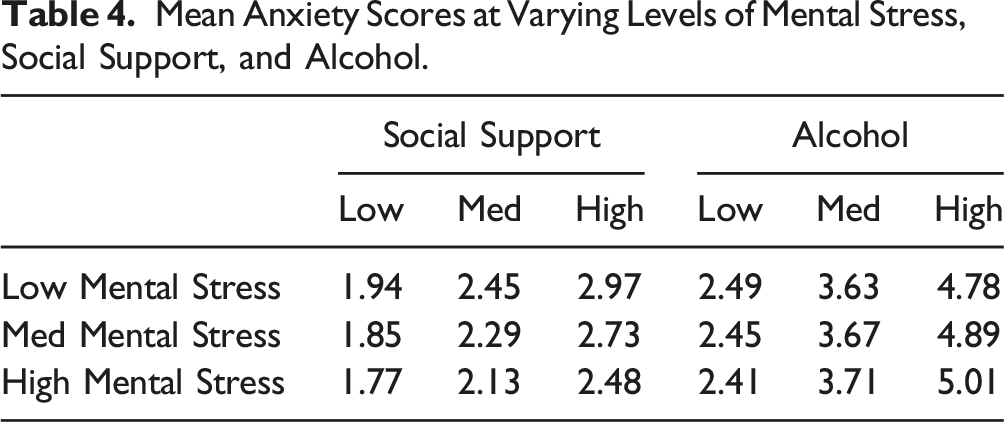
Mean Anxiety Scores at Varying Levels of Mental Stress, Social Support, and Alcohol.
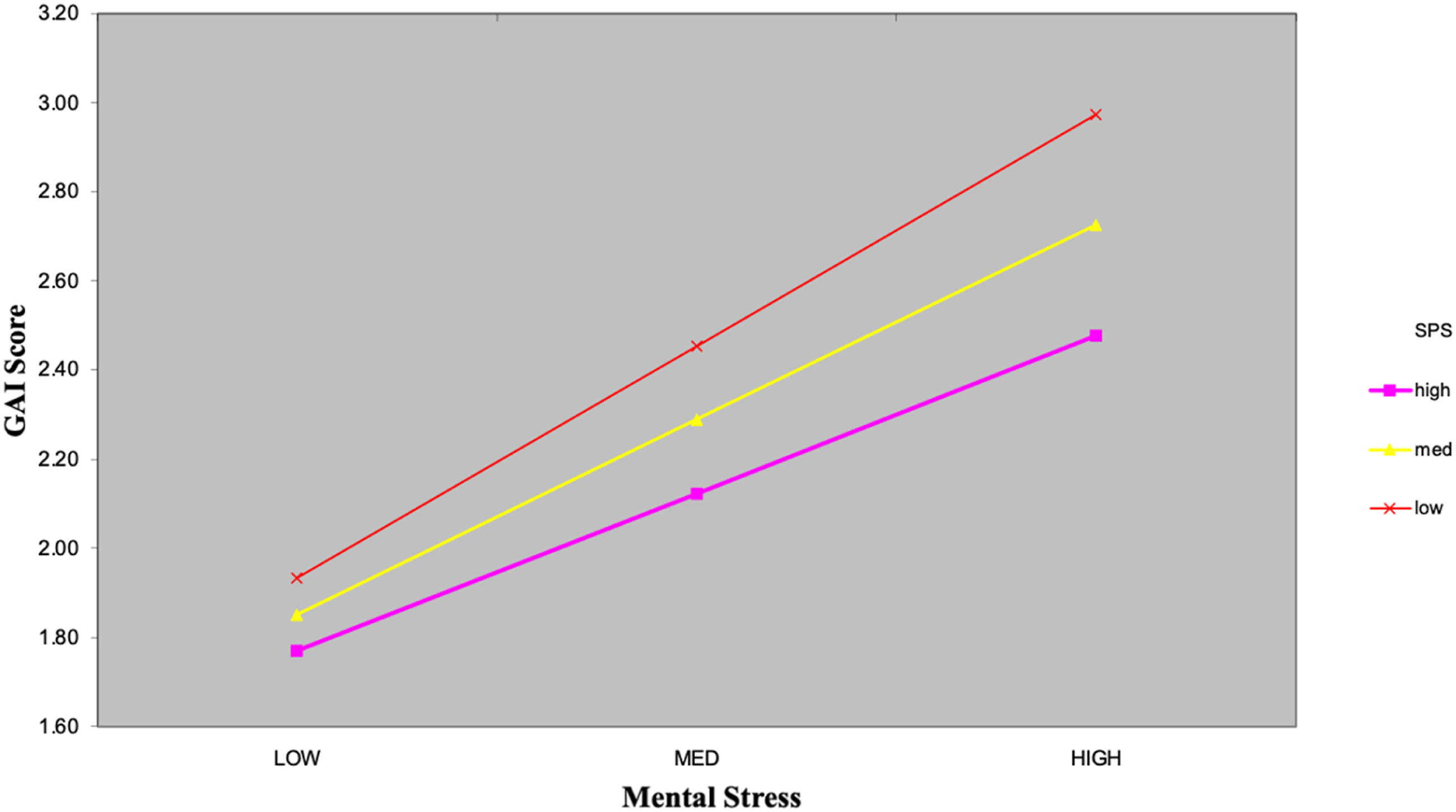
Moderation of the effect of mental stress on anxiety by social support.
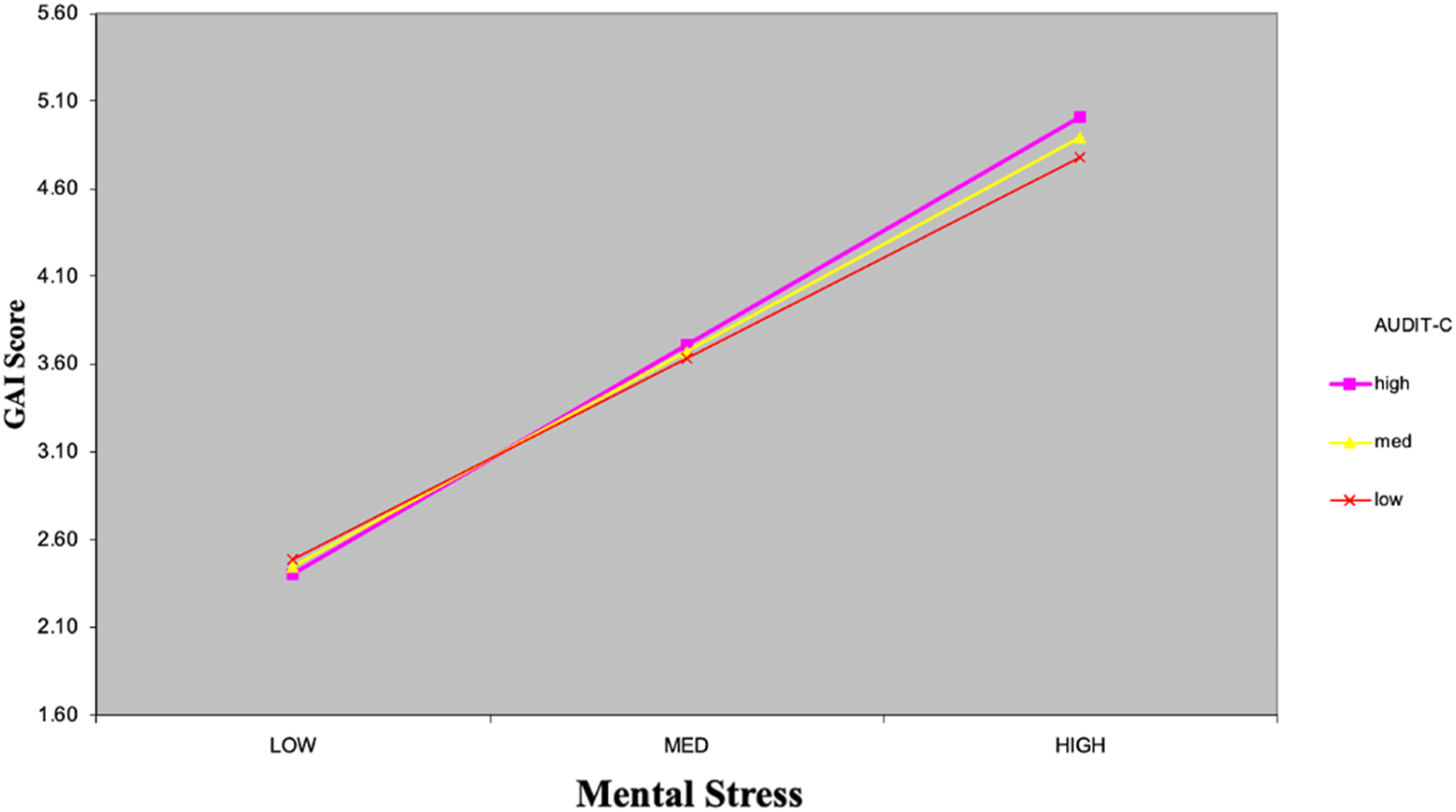
Moderation of the effect of perceived mental stress on anxiety by alcohol consumption.
Discussion
There were three main findings. First, COVID-19 was perceived, on average, to be slightly stressful in that the pandemic negatively impacted older adults’ physical, mental, and economic well-being. Second, there were no changes in social support, physical activity, and alcohol consumption before (2018) and after (2020) the first lockdown, although there was a significant reduction in smoking. Third, two coping strategies moderated the relationship between perceived stress and anxiety in 2020, with only social support being protective against stress. These findings highlight the impact of social support in mitigating the perceived negative impact of the COVID-19 pandemic on the emotional well-being of older adults. Here, we discuss each of these findings in turn and in relation to each other.
Our finding that there was no change in anxiety after the first lockdown in 2020, while there was a significant relationship between COVID-19-related perceived mental stress on measures of anxiety, suggests a relationship between trait-anxiety and perceptions of stress during the pandemic. Those who were already more likely to report anxiety symptoms in 2018 were also more likely to report mental stress and anxiety in the face of the pandemic. International research has reported mixed results regarding the perception of stress associated with the COVID-19 pandemic among older adults. Some older adults perceived the pandemic as stressful and feared even stepping outside, whereas others disagreed with the vulnerability label (Falvo et al., 2021; Verhage et al., 2021). These mixed results emphasize the heterogeneity of older adults and highlight the need to be aware of groups who are vulnerable to negative outcomes rather than labelling all older adults as vulnerable. Despite earlier fears for the mental health of older people, meta-analyses have shown that younger people were at higher risk of mental health effects than older people (Dragioti et al., 2022) while among older people, specific sub-populations were most at risk (Yan, et al., 2022).
The generally low perception of stress among older adults during the pandemic may be accounted for by those who were able to enjoy the early lockdown situations. Older adults in Aotearoa/NZ who were retired, able to work from home or eligible for wage subsidy, and were able to connect with family and friends, described their lockdown experience as enjoyable (Stephens & Breheny, 2022) while public health measures were often reassuring rather than alarming (Greyling et al., 2021). The present findings reinforce these early indications that older adults were generally resilient in the face of a potentially stressful time.
This primary appraisal for much of the population can also explain the lack of significant change in coping strategies such as physical activity, alcohol consumption, and social support. Although smoking levels did change, this was not in the direction predicted by the transactional model. This reduction in smoking behavior has been reported in the United States (Denlinger-Apte et al., 2022) and Japan (Koyama et al., 2021). Explanations for this change include the elimination of contextual situations such as bars or parties following the pandemic (Denlinger-Apte et al., 2022) or enforced stays at home with family (O’Donnell et al., 2021).
The coping strategies which did moderate the relationship between perceived stress and anxiety were social support and alcohol use. Those who reported greater social support reported the lowest anxiety scores at the highest level of perceived stress, while those with the lowest social support were increasingly more anxious as perceived stress increased. Other studies among younger populations in China (Liu et al., 2021), the United States (Szkody et al., 2021), and among nurses (Schierberl Scherr et al., 2021) have reported a moderating role of social support on the relationship between perceived stress during the COVID-19 pandemic and mental health symptoms. The present results show a similar relationship among older adults.
The transactional model suggests that social support might moderate the effects of perceived stress by promoting cognitive reappraisal. Social support networks providing information, advice, and guidance during a crisis may promote the reappraisal of the stressor as more controllable and manageable (Szkody et al., 2021). In a high social support context, individuals report a sense of understanding and safety that is further associated with emotional stability and positive reappraisal (Padhy & Angiel, 2021; Van Knippenberg et al., 2007). As the reappraisal alters the appraisal stage in the transactional model, it may also have a positive impact on emotional well-being (Holmstrom, 2015). The availability of informational and emotional support from social connections can promote cognitive reappraisal and alleviate negative emotions associated with the stressor.
Because there was no change in levels of social support after the first lockdown, it seems that older people bring their social support networks into a stressful situation (rather than respond to stress by seeking social support) and this accords with previous research and theorizing regarding convoys of support (Antonucci et al., 2014). However, this understanding of social support does not support its definition as an “active” coping strategy in terms of the transactional model. Although social support clearly moderates stress, its role in a stressful situation requires more nuanced theorizing. In practical terms, this finding does indicate that older people with lower social support may be targeted as a more vulnerable group in a pandemic situation.
Alcohol consumption was the only other proposed coping strategy that moderated the relationship between mental stress and anxiety among older adults. As predicted, at high mental stress levels during the COVID-19 pandemic, high alcohol consumption was associated with higher anxiety scores compared to moderate and low alcohol consumption, supporting the prediction that this is not a useful coping mechanism. Alcohol consumption has been previously associated with interfering with the cognitive processes involved in processing information and formulating an appraisal (Sayette, 1999). However, despite international evidence that risky drinking among older people increased (e.g., Rao et al., 2022) or that older people were more likely to buy alcohol for entertainment or emotional reasons during lockdowns (e.g., Foster et al., 2021), older adults in our sample did not increase alcohol consumption during the pandemic. The strengthening of the relationship between alcohol use and anxiety at high levels of perceived stress suggests that those with higher levels of alcohol use are another group in the population who are vulnerable to increased stress. However, this is a weak effect and must be replicated in future research. Given the marked differences observed between the consumption scores for males and females which is not unexpected (see French et al., 2014), further research could also fruitfully examine the gendered effects of perceived stress and alcohol use on anxiety. Previous research has demonstrated that older women are more likely to experience anxiety symptoms than men, and that consumption of alcohol is also associated with anxiety (e.g., Forlani et al., 2014). Such findings suggest complex interactions between stress, gender, and alcohol use among older people.
Limitations
The use of cross-sectional data to examine the moderating effects limits our interpretations of those effects. For example, it is equally likely that symptoms of anxiety could increase the consumption of alcohol, rather than alcohol use contributing to increases in anxiety; there is evidence that having a pre-existing anxiety disorder Garnett et al. (2021) or reporting mental distress in 2020 (Biddle et al., 2020), predicted increased alcohol use during the pandemic. Further research on the role of alcohol as a stress reliever among older adults will be required to untangle these relationships. The correlational nature of the results for the role of social support are not so problematic since the role of social support as a buffer of stress and in promoting mental health is more strongly established (Taylor, 2011).
Another important limitation is the measure of perceived stress utilized in this study. The measure of people’s understanding of the impact of the pandemic on their mental health is believed to indicate higher levels of perceived stress. However, this assumption requires further validation.
Those lost to the study in 2020 were more likely to report “comfortable” rather than “good” economic living standards, while the proportion in “hardship” remained the same. It is possible that the loss of participants who were more likely to report lower living standards also affected the mean scores of other study variables, particularly economic stress.
Conclusion
The current study provided limited support for the use of Lazarus and Folkman’s (1984) transactional model of stress and coping in accounting for the coping strategies of older people during the COVID-19 pandemic. The generally low perception of stress and no detectable changes in the emotional well-being of older adults between 2018 and 2020, aligned with the model. As the pandemic was not generally perceived as threatening or stressful at that time, no downstream changes in coping strategies or the potential outcome of increased anxiety were observed.
Two coping strategies, social support and alcohol consumption, moderated the relationship between perceptions of stress and anxiety. Rather than revealing the outcomes of individual coping strategy choices under stress, these findings point to the importance of recognizing the heterogeneity of older people prior to stress. Different groups of older people have different needs during a stressful period such as a pandemic.
Those who regularly use alcohol at higher levels may be at a greater risk of higher levels of poorer mental health. The strongest result showed that older people with low levels of social support are at the greatest risk of increased anxiety symptoms when they perceive that the pandemic is harmful to their mental well-being. These are the people who are more vulnerable and to whom additional support may be targeted in times of stress.
These findings highlight the heterogeneity of older adults. The implications for future public health responses are that, rather than treat older people as a single group in terms of age alone, interventions may be more appropriately targeted to those who are in need of support. Here, the needs of those with higher alcohol use and lower social support have been highlighted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The collection of data for this study was funded by the New Zealand Ministry of Business, Innovation, & Employment (MAUX1705).