
Abstract
Introduction
As populations around the world increasingly transition towards older age distributions, recent decades have seen rapid growth in a variety of fields in research on aging, including in the medical sciences, biological and health sciences, and social sciences. An emerging focus within this literature, in addition to the traditional target of reducing disease or disability, has been to foster positive aspects of aging or “successful aging.” One particular focus is on resilient aging, which integrates insights from across research disciplines to enhance the ability of individuals to experience stronger positions of health and wellbeing as they age. The approach aligns well with the idea that moving forward in the field of aging will require a multidisciplinary, multi-level response. This paper builds on the previous literature and conceptual frameworks by proposing an expanded framework for conducting empirical research on resilient aging. The conceptual framework we propose explicitly incorporates the role of economic factors as resources that contribute to resilience, in addition to social and psychological factors emphasized in the existing literature, while also introducing the idea of reinforcing cycles of resilience.
The remainder of the paper is organized as follows. The Conceptual Framework section first provides background from the existing literature on the concept of resilient aging and prevailing frameworks for analysis. It then develops a justification for the expanded conceptual framework proposed here. We highlight wellbeing and health as outcomes of interest and introduce the explicit role of economic resources as an important component of resilience. The Evidence From the Literature section presents empirical evidence from the literature that supports the conceptual arguments. It first discusses papers that focus on the influence of economic resources on health and wellbeing, and then consider papers that emphasize the reverse, that is, the influence of health status on economic resources. We include examples from Mexico and other low- and middle-income countries, as well as from high-income countries. The Translating Concepts to Empirical Applications section first illustrates the concepts of our proposed framework by considering a hypothetical scenario that compares how two individuals, one with low resilience and one with high resilience, experience the cycles of the framework following a health shock. We then outline data requirements for applying the ideas of the conceptual framework in empirical analyses and discuss the state of data availability. We conclude with a brief summary of key points in the Conclusion section.
Conceptual Framework
This section presents the conceptual framework that we use to model individual resilience, building upon the work of others. While we discuss data needs for application of the framework below, we do not present a detailed statistical model. Rather, the purpose of this paper is to emphasize the conceptual foundations of our framework and to encourage their incorporation into applied research on resilient aging. The specifics of integrating these concepts into empirical applications will depend, inter alia, on country context, data availability, and research objectives. Our framework pursues two major goals, which are developed more fully below: 1) expand the existing frameworks to explicitly include economic factors, and 2) incorporate explicitly the idea that resilience affects health, and vice-versa, that health in turn affects the resources that come together to form resilience.
In brief, resilience has been recognized as the ability to “bounce back” after adversity. Much of the early literature referred to children overcoming trauma, or the influence of childhood trauma on adult behavior (Beutel et al., 2017; Wingo et al., 2010; Zhou et al., 2016). Literature that is more recent started to refer to resilience in old age or resilient aging, focusing largely on recovering from shocks in terms of both physical and psychological dimensions of function which are associated with health setbacks (Windle, 2011). Previous authors also focus on how life experiences influence resilience in old age, thereby emphasizing the approach of the life course in the study of resilient aging. Several “positive” concepts such as successful aging and recovery emerged, giving importance to constructs such as mastery, self-esteem, social support, and purpose. The work environment, civic participation, or social engagement with family or a social network can provide opportunities to gain or secure these positive qualities of life. Moreover, these views focus on maintenance and enhancement of function in late life instead of only focusing on “recovery” from setbacks. In addition, these views imply a capacity to learn in old age, finding meaning in life, openness to new experience, and expanded life space; all these aspects add to resilience. In this approach, social and psychosocial resources facilitate “bouncing back” from a crisis or shock as well as maintaining health status (In Fry & Keyes, 2010; Kim et al., 2021).
We argue for an expansion of this framework typically proposed in the literature, with the explicit consideration of economic factors and the role they play in the ability to recover from a shock. We believe that such incorporation will help capture and understand better the likely consequences of adversity, as economic resources play a critical role in the capacity to recuperate from setbacks and maintain health status. This aspect can be especially critical during old age, when individuals no longer have the capacity or opportunity to earn income from labor.
We begin with the concepts used by previous authors in resilience research. First, “resilience” is the capacity to adapt in a beneficial manner to setbacks of any kind, either shocks to their health, social, or economic wellbeing (Kim et al., 2021). To consider resilience as a construct, authors have highlighted the importance of heterogeneity in risks and abilities acquired and accumulated through lived experiences, and how as a result, resilience itself changes over an individual’s life course. Hence, resilience is recognized as a dynamic construct resulting from a variety of types of “resources.” The heterogeneity in these resources is what leads to disparities in resilience among individuals in old age.
These resources are theorized as measurable traits, which build over time and depend on experiences or events individuals undergo over their life. A stressor would have stronger or weaker negative effects on health depending on these resources. The most often mentioned groups of resources include aspects in the psychological and social areas. These resources exist at different levels: individual, in the network of family and friends, in the community of residence or work, and in society overall or in the country in the form of policies and services (Kim et al., 2021; Samper-Ternent, 2012). This multiplicity of levels and concepts make the empirical research on resilience demanding in data, and we will discuss this below in our empirical adaptation of the framework. Next, we discuss each group of resources in turn.
Psychological Resources
Different dimensions of psychological assets held by individuals can enhance the impact of health prevention and treatment programs to address the health needs of an increasingly aging population. Relevant to our framework, these resources can augment the ability to bounce back or recover from stressful situations or shocks. These resources are observed and measurable aspects at the individual level such as purpose in life, happiness, life satisfaction, optimism, and other personality traits (Aldwin & Igarashi, 2015).
Social Resources
In this group, social relationships with either family or social networks operate to foster coping mechanisms and help in perceiving stressful situations with a less catastrophic optic (Holt-Lunstad, 2018). These resources are aspects such as having positive social interactions of a variety of types, and can be measured objectively but also by perceived social support in the event of a crisis. Objective measures can include the size of the network such as number of children living nearby or close friends, and frequency of interactions. Indicators also include subjective measures such as perceived loneliness, social isolation, and extent of activity of one’s social network. An important feature of this group of resources is the perception of security or ability to count on the support of the network in case of a crisis.
The evidence sustains that a higher amount of these psychological and social resources is associated with healthier behaviors such as physical activity, diet, sleep, not smoking, and use of preventive health care, for example, (Kim et al., 2021). These behaviors are, in turn, associated with positive health outcomes and wellbeing. In addition, other authors (Kim et al., 2015) differentiate between states of wellbeing and the resources needed to foster wellbeing, and postulate concepts such as having life meaning and purpose in life as indicators of both psychological and social wellbeing in old age (Kim et al., 2014).
Economic Resources
Although the group of social resources mentioned above implicitly considers access to resources such as health care, and social support including financial support from the social network (Thomas et al., 2017), the applied research does not focus on economic wellbeing as an explicit component that contributes to resilience. We advocate for the explicit incorporation of this group of resources in our framework, as economic wellbeing is closely linked to health and the ability to recover from health shocks. These are resources such as financial assets, real estate and other physical assets, as well as financial security such as insurance. The latter include health insurance, catastrophic health insurance, property insurance, and life insurance, operating as safety nets that also promote the perception of a strong capacity to recover from a shock (Kharazmi et al., 2021). In low- and middle-income countries with poorly developed financial markets, this safety net may also be offered, albeit informally, by a heavy reliance on family and social networks (Thomas et al., 2017). In addition to financial assets and insurance, related characteristics such as educational achievement, income, labor force participation, occupation, or job characteristics over the life course can serve as economic resources that contribute to resilience in old age.
Similar to previous authors, we recognize the important role of the life course in the conceptual framework, as psychological, social, and economic resources increase or build up, and decrease or erode over the life course, rendering resilience a dynamic construct that changes over time. Similarly, we consider the reverse effect, whereas in addition to each of the three groups of resources influencing health and wellbeing, health, in turn, is continuously influencing individuals’ capacity or ability to augment the psychological, social, and economic resources that constitute resilience. In Figure 1, we represent our conceptual framework, adapted and modified from previous literature (Kim et al., 2021; Samper-Ternent, 2012). We share with previous authors the emphasis on psychological and social resources as well as the life course approach, and we add an explicit focus on economic resources as part of resilience, and economic wellbeing as part of the outcomes. Box A represents resilience, as a dynamic construct based on the individual’s psychological, social, and economic resources. Over the life course, this is a changing ability to maintain wellbeing and bounce back after a shock. Within this box, resources influence each other, so that, for example, psychological resources reinforce the social and economic resources available to an individual; and vice-versa, the economic and social resources strengthen the psychological resources available to withstand a shock. Arrow B represents the influence of resilience, or the resources that form resilience, leading to healthier outcomes such as healthy behaviors, physical and mental health, physical and cognitive function, and wellbeing in general. Arrow C represents that, in turn, health outcomes and wellbeing influence the resources available for resilience. Expanded conceptual framework for models of resilient aging.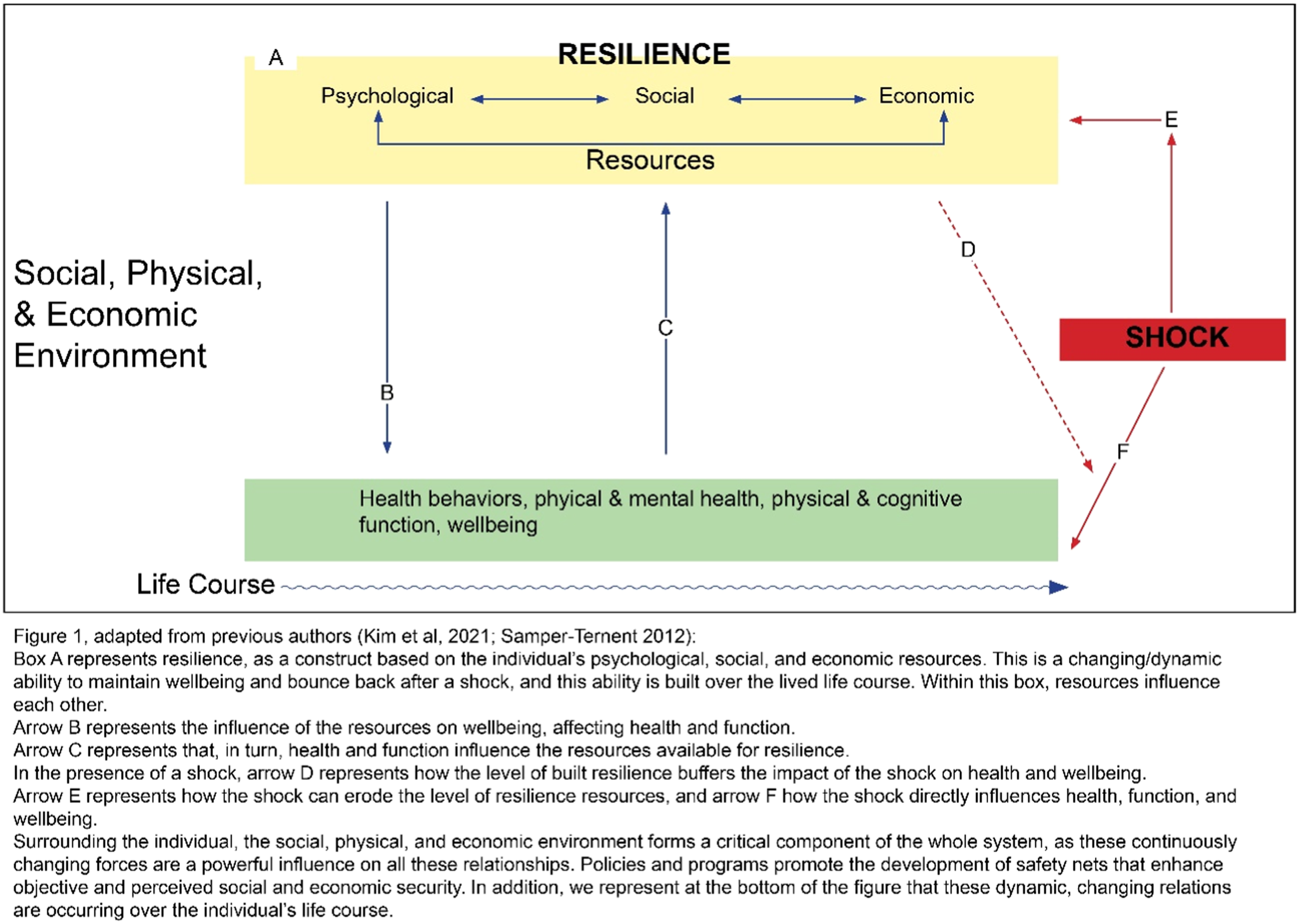
Arrow D represents that, in the presence of a shock, the level of built resilience acts as a mediator, buffering the impact of the shock on health outcomes and wellbeing. Arrow E represents how the shocks also can erode the level of resilience resources, while arrow F signifies how the shock directly influences health, function, and wellbeing.
Similar to other authors, and surrounding the individual, we denote that the larger social, physical, and economic environment or context forms a critical component of the whole system, as these continuously changing forces are a powerful influence on the resilience-wellbeing relationships. Policies and programs can promote the development of safety nets and opportunities that enhance objective and perceived social and economic security of individuals, for example, through old age pensions, universal health insurance, or universal access to education. Such features of the larger context in which individuals live and age have been characterized as components of macro-resilience (World Bank, 2021). In addition, and as previously mentioned, we represent at the bottom of Figure 1 that these dynamic, changing relations are occurring over the individual’s life course, resulting in accumulated resilience and wellbeing in old age.
Evidence From the Literature
In this section we summarize examples from the literature, for Mexico and elsewhere, in support of the arguments in our conceptual framework. It is not our goal to provide a thorough literature review but, rather, to present select examples that serve two purposes: (1) they illustrate the importance of economic resources as determinants of health outcomes among the aging, and (2) when considered as a whole, they underscore the bi-directional relationship between economic resources and health outcomes. We rely heavily on examples from Mexico, both because it figures importantly in our research and, among low- and middle-income countries, it currently has the richest data for the study of resilience in aging. We selected studies that document the relationships of interest and represent: populations in other low- or middle-income countries in addition to Mexico and in high-income countries, a variety of dependent variables, and publications in Spanish as well as English. Despite the use of these criteria, the papers included in our summary should not be viewed as providing a comprehensive or representative introduction to this literature.
Papers Summarized: Economic Resources as Determinants of Health Outcomes.
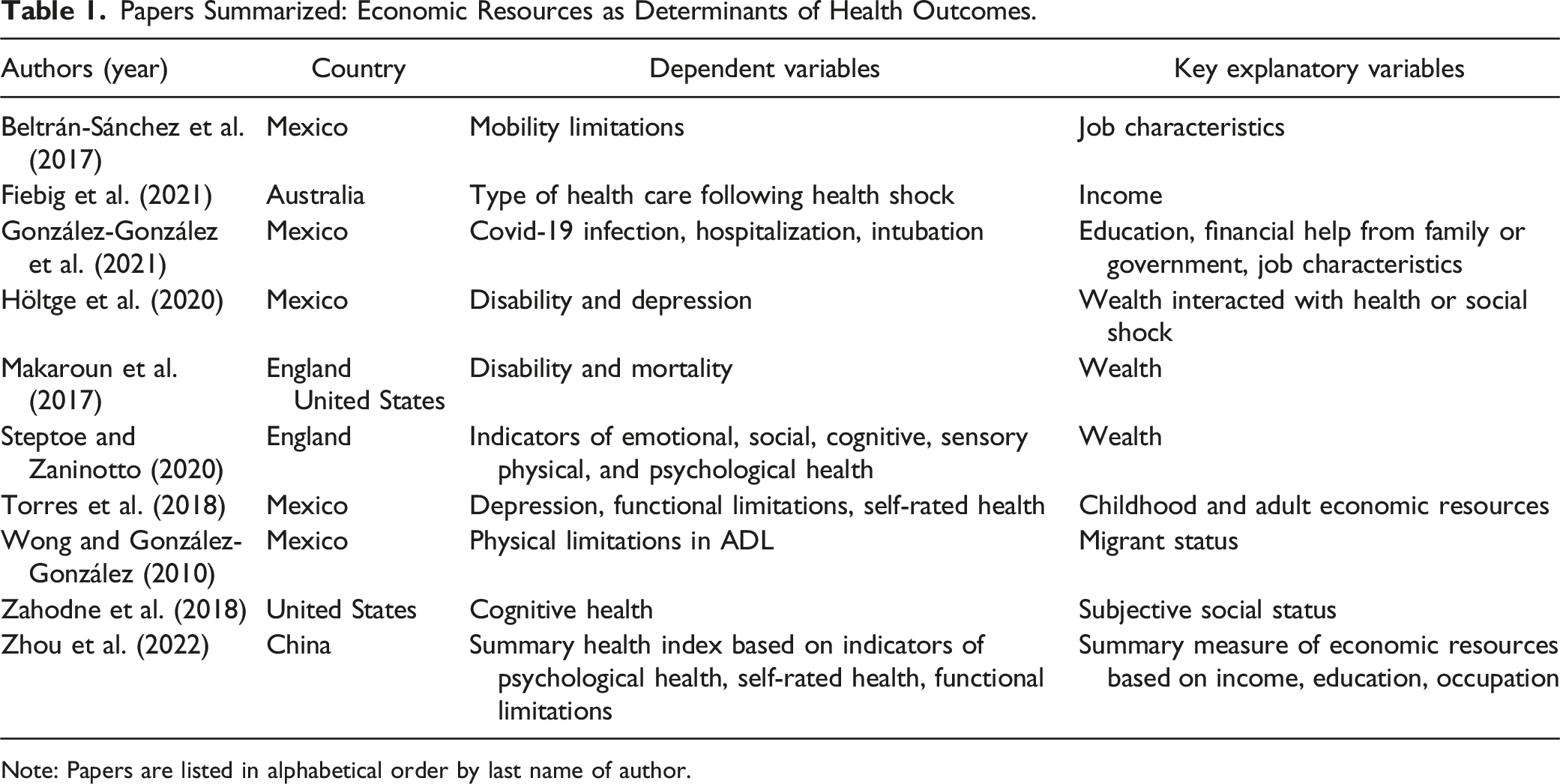
Note: Papers are listed in alphabetical order by last name of author.
Papers Summarized: Health Status as Determinants of Economic Resources.
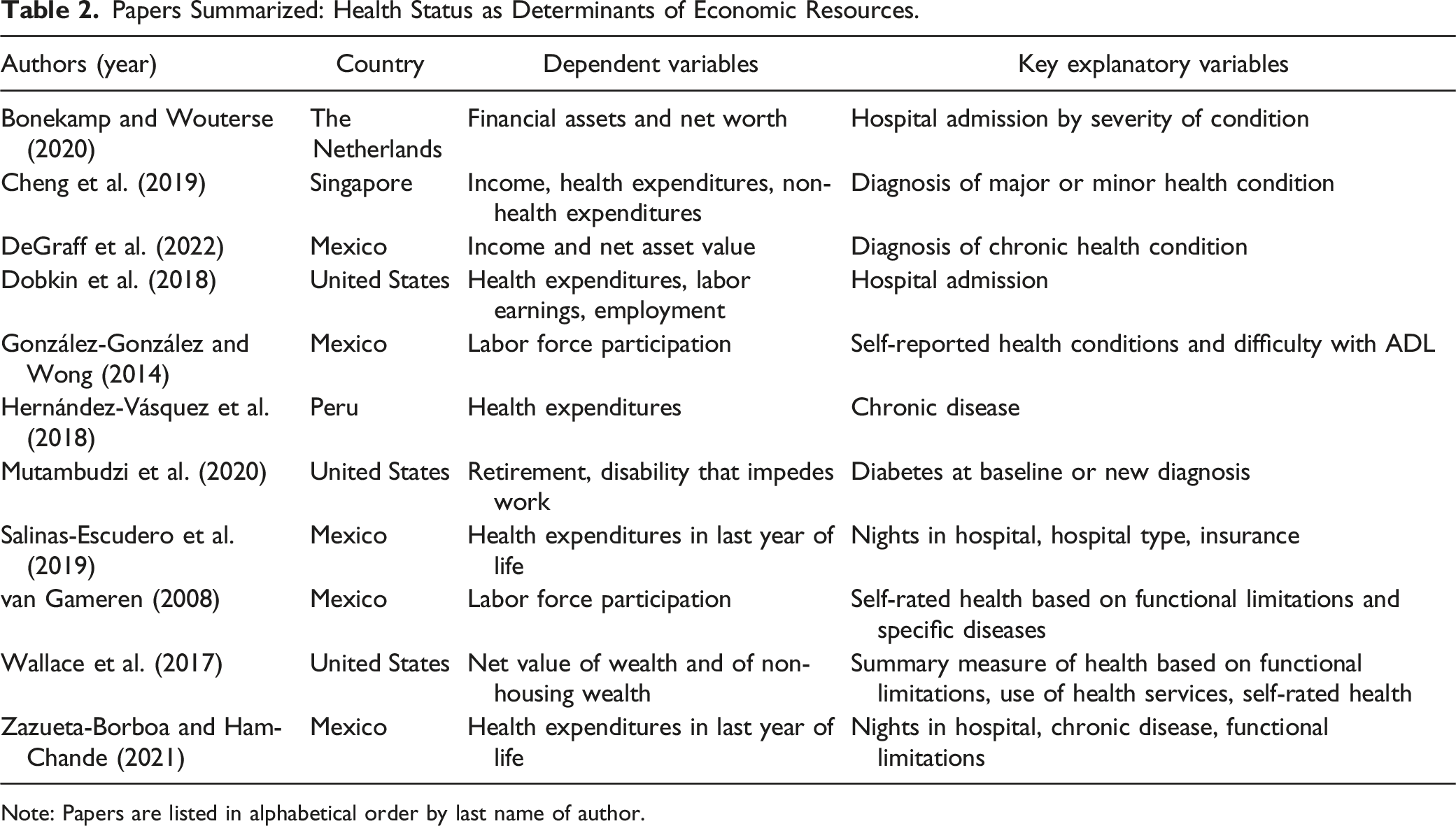
Note: Papers are listed in alphabetical order by last name of author.
Economic Resources as Determinants of Health Outcomes
Torres et al. (2018), using multiple waves from the Mexican Health and Aging Study (MHAS) for 2001, 2003 and 2012, model the determinants of 11-year trajectories for three health outcomes: depressive symptoms, functional limitations, and self-rated health. Based on a life course framework, the key explanatory variables are measures of childhood economic resources (access to a toilet at age 10 and any formal education) and adult economic resources (asset ownership index or asset value, and occupation or income). Alternative specifications employ consolidated lifetime measures of economic dynamics, wherein individuals are sorted into four categories based on whether their childhood and adult economic resource measures are low or high. The authors find significant effects of the separate childhood and adult economic resource measures for most of the health outcomes studied. These results support the argument that not only do better economic conditions in late life contribute to better health but, even after controlling for current economic resources, better economic conditions in childhood further contribute to better health late in life. Moreover, results for the consolidated lifetime measures of economic resources provide the additional insight of a gradient, where those who transition from low to high economic resources over the life course, or the reverse, are generally predicted to have better health outcomes in later life than those who remain in the low category, and worse health outcomes than those always in the high category. Taken as a whole, these findings also suggest that not only do recent negative economic shocks contribute to worsened health among the aging, so do economic shocks sustained earlier in the life course.
Zhou et al. (2022), for the case of China, also focus on economic determinants of psychological health, functional limitations, and self-rated health, but adopt a different conceptual and methodological approach. Using data from the 2018 wave of the Chinese Longitudinal Healthy Longevity Survey for individuals aged 60 or older, the authors construct a single comprehensive health index from 32 indicators of these three broad categories of health. Similarly, the primary explanatory variable of their models is a single comprehensive measure of economic resources. It is constructed from measures of total family income, years of education, and occupation at time of retirement, with the latter two including information for both the respondent and spouse if currently married. They find significant positive effects of the economic resources measure on health outcomes, with age-based models suggesting that this effect is concentrated among those younger than 80.
Beltrán-Sánchez et al. (2017), using data on individuals aged 50 or older from the 2001 wave of the Mexican Health and Aging Study, focus on the effects of the physical demands of different types of occupations on later-life functional limitations. The authors note that commonly considered economic characteristics such as education and wealth are likely associated with the physical characteristics of work and, thus, implicitly capture any effects of the latter on health outcomes in reduced form. However, a key argument informing their analysis is that physical characteristics of work have distinct effects on functional limitations in later life and, thus, warrant explicit consideration. Further, they note that this pathway is especially important to examine in a country such as Mexico that has less well-developed occupational safety and health regulations than most high-income countries. The authors construct a measure of mobility limitations based on degree of functionality for each of nine activities. The key explanatory variables are a set of job category variables, based on similar physical demands of occupations. They estimate models to alternatively include among the covariates the job variables, common indicators of economic resources, or both. The results support the statistical significance of the job category variables in models of functional limitations, even after also controlling for other measures of economic resources, suggesting that job characteristics have consequences for health later in life.
Wong and González-González (2010) similarly use data from the first wave of the MHAS and focus on physical limitations in activities of daily living among those aged 60 or older in 2001. The characteristic of primary interest is whether the individual is a return migrant from the United States. The authors note that conceptual arguments can be made in either direction regarding whether return migrants would have better or worse health outcomes than non-migrants in old age, especially in light of possible selection with respect to who returns to Mexico. Model results suggest that, among women but not men, return migrants are more likely than non-migrants to experience limitations in daily activities. While focused on the role of migration, the analysis controls for other common measures of economic resources. These results indicate that more education is associated with less disability for both men and women.
González-González et al. (2021), using the most recent MHAS data from 2018, examine the economic characteristics of the population aged 50 and older that are associated with higher risks of testing positive for Covid-19, or being hospitalized or intubated for such disease in Mexico. They find that older adults who have completed six or fewer years of schooling, or who receive government transfers or financial assistance from family were generally more likely to experience these negative health shocks. In addition, in keeping with Beltrán-Sánchez et al. (2017), the authors examine the role of job characteristics in view of potential work-related differences in the risk of exposure. The results suggest that those who work without a fixed physical place—itinerant workers, those who go from door to door, those working in improvised physical spaces or in vehicles—were at greater risk for some of these Covid-19 outcomes. The authors also note a selection process with respect to another key economic resource, the extent of health insurance coverage. Those who have better health insurance were over-represented among hospitalized patients who have tested positive for Covid-19. This finding suggests that those with better health insurance are in a stronger economic position to seek health care, including hospital care, when infected, thereby supporting greater resilience in the face of infection from Covid-19.
Turning to examples from high-income countries, Zahodne et al. (2018) focus on determinants of cognitive health in later-life, using longitudinal data on participants aged 65 and older in 2006 from the Health and Retirement Study (HRS) in the United States. While their conceptual framework and empirical models include common indicators of economic resources (measures of education, occupation, income, and wealth), the authors argue that subjective perceptions of inequality can have distinct effects on a range of health outcomes. They operationalize this concept by defining an indicator of subjective social status (SSS) derived from respondents’ self-assessment of where they sit on a 10-rung ladder of social status. Cognitive health is represented by measures of initial episodic memory (based on word recall) at baseline and subsequent decline in episodic memory as assessed in 2012. Model results suggest that independent of objective measures of economic resources and other controls, lower SSS is significantly associated with worse memory at baseline, but not with any greater loss of memory over time.
Using data for individuals aged 52 or older from the English Longitudinal Study of Aging (ELSA), Steptoe and Zaninotto (2020) examine the impact of wealth on indicators of ability or wellness across six health domains: physical, sensory, physiological, cognitive, emotional, and social. They consider both possible associations at baseline in 2004, and associations with changes in health status between baseline and follow-up in 2012, for each of several indicators of each health domain. The analysis controls for, among other variables, educational attainment, measures of childhood economic resources, and indicators of chronic health conditions at baseline. The authors conclude that individuals with lower wealth have lower health status at baseline, and experience significantly greater declines in health over time, for each of the health domains considered. These results suggest that negative wealth shocks exacerbate health declines among the aging.
Similarly, using HRS and ELSA data for the United States and England, respectively, Makaroun et al. (2017) consider the relationship between wealth at baseline for those aged 54–76, and two health outcomes: disability, as measured by difficulty with any of the activities of daily living, and mortality. The authors estimate the hazard of experiencing disability or death over a 10-year period from 2002 to 2012 by wealth quintile, controlling for education, income, and demographic characteristics. They conclude that a consequence of lower wealth is a greater risk of disability and death in subsequent years. Returning briefly to Mexico, a similar study by Hӧltge et al. (2020) uses MHAS data from 2001 to 2012 to examine trajectories of disability and depression. Their key focus is the effect of a health shock (a serious fall) or a social shock (death of spouse) on these trajectories, but they also consider interactions with wealth. The authors conclude that those with greater net worth at baseline are more resilient in that they experience more favorable trajectories following a shock.
Lastly, Fiebig et al. (2021) examine whether differences in economic resources contribute to differences in the increased use of primary care, specialist care, and non-urgent emergency care following a health shock in Australia. Using data collected by the Sax Institute for a sample of individuals aged 45 and older in the state of New South Wales, they focus on the role of income in the context of a new diagnosis of diabetes or heart disease. For diabetes, they find significant differences in type of care responses by income, with low-income patients increasing their use of general practitioner services more than high-income patients, and the opposite pattern for specialist care with respect to income. For heart disease, the difference in responses by income in the use of general care is not statistically significant. However, the increase in the use of specialist care following diagnosis of heart disease is greater for low-income patients than for high-income patients, likely in part because high-income patients already make greater use of specialist care prior to a health shock. There is no evidence of increased use of non-urgent emergency care for either health shock or income level. The authors note that the health implications of these differing patterns depend, in part, on how substitutable general practitioners and specialists are in the context of these diseases.
Before considering examples from the literature that focuses on the opposite causal direction, that is, health status influencing economic resources, we briefly mention a few threads that run through many of the papers summarized above. Each of these points is explicitly addressed in some of the papers, and all points are important to conceptual and methodological research in this area. First, it is important to think carefully about timing. Collectively, the studies discussed above consider potential effects of economic resources on health that originate in childhood or during the working years and cumulate across the life cycle, or are contemporaneous at older ages, or have lagged effects at older ages.
Second, researchers should be mindful about possible selection issues when interpreting results if the estimated models are not adjusted for sample selection. Using Wong and González-González (2010) as an example, as the authors note, it is important to consider whether the return migrants in their sample are representative of all migrants to the United States. Only those who return are available to be included in the data. If those who return are not representative with respect to characteristics that also might impact later-life health outcomes (e.g., income and wealth, access to health care during the period of migration, characteristics of jobs, underlying health conditions, or attitudes toward risks), estimates of the effects of migration on health outcomes could be biased in the sense that they also reflect the selection process. Similarly, when using longitudinal data for individuals in later life, sample attrition due to death (and other reasons) could potentially lead to selection bias, particularly when following individuals for a relatively long period.
Third, having access to health insurance and the extent of its coverage is a characteristic that can mediate causal relationships between other economic resources and health outcomes. Fourth, the potential heterogeneity of empirical results by age should be taken into account. Many datasets geared towards analysis of older populations include information for individuals aged 50 and older which is a very broad age range. Researchers often select a narrower age range considered most relevant for their focus, or they conduct parallel analyses by smaller age groups to allow for differences by age to be detected. Fifth, it is also often important for statistical analysis to allow for possible differences between females and males in the effects of economic resources on health, as well as between urban and rural locations. These two observed characteristics tend to be associated with fundamentally important but unobserved, or not well measured, social, cultural, and economic characteristics.
Lastly, and especially relevant to our overarching conceptual argument, several of these papers explicitly discuss the possibility that there is some form of reverse causality at work. In other words, even if not typically addressed in the statistical analysis, authors argue that the same or related health outcomes under study, in turn, have an influence on subsequent economic resources.
Health Status as Determinants of Economic Resources
DeGraff et al. (2022), using the first three waves of the MHAS data from 2001, 2003 and 2012, examine the effects of health shocks on subsequent income and assets in Mexico among those aged 50 or older at baseline. Health shocks are measured by a diagnosis between 2001 and 2003 of any of five chronic diseases or conditions: cancer, diabetes, heart disease, respiratory problems, or stroke. The economic resources variables are defined at the individual level as the change (in real terms) between 2001 and 2012 in several income and asset measures: total income, income by source (labor earnings, income from family, pension), total net asset value, and components of asset value (housing, business assets, financial assets). A key objective of the analysis is to assess whether there are differences in the impact of health shocks by whether individuals are economically vulnerable, with vulnerable status measured by lack of formal education and/or health insurance at baseline. Model results indicate no significant effects of health shocks on asset values, likely because most assets in Mexico are highly illiquid (e.g., housing) and, thus, not easily drawn upon to meet health expenditures or offset health-related loss of income. Regarding income, while in general the results do not provide evidence of significant effects of health shocks overall, negative effects are evident among those identified as more economically vulnerable, or less resilient, at baseline. Negative effects among the vulnerable are estimated to be most pronounced for labor earnings and among males. The analysis also finds no evidence of such effects in the short run (2001–2003), underscoring the importance of multi-wave longitudinal data for understanding these relationships.
van Gameren (2008) uses the first wave of the MHAS to examine the relationship between health status and labor force participation of those aged 50 or older in 2001, among those ever employed. This relationship is likely a key pathway for the effects of health shocks on subsequent income discussed above, though the analysis in this study is contemporaneous. Labor force participation is measured in reference to the week prior to interview. Health status is measured using self-rated health, but to lessen any biasing effects due to potential endogeneity of this measure in the cross-section, it is first estimated as a function of self-reported objective health characteristics such as functional limitations and diagnosis of specific diseases or health conditions. Controlling for several additional demographic and economic characteristics, the model for current labor force participation suggests that better health status increases the probability of the respondent being in the labor force, which better positions individuals to have a higher level of economic resources and, thus, greater resilience.
González-González and Wong (2014) also use MHAS data for Mexico to examine the effects of health status on labor force participation among the population aged 50 and older and in the labor force in 2001. Unlike van Gameren (2008), the authors directly utilize several self-reported measures of specific diseases or health conditions at baseline to represent health status, including arthritis, diabetes, heart attack, hypertension, and stroke, as well as difficulty with activities of daily living. Also unlike the study above, the authors estimate effects on subsequent labor force participation in the week prior to the survey in 2012, rather than on current labor force participation in 2001. They find evidence of significant negative effects of worse health status in 2001 on future labor force participation, also concluding that the effects differ somewhat by gender. For men, those who reported hypertension or diabetes at baseline were less likely to be in the labor force in 2012. For women, those who reported diabetes or arthritis were less likely to be in the labor force in 2012.
We mention two papers that focus on determinants of out-of-pocket health expenditures (OOPE) in the last year of life among Mexicans aged 50 and older. Salinas-Escudero et al. (2019) use MHAS data to construct a sample of those who died between 2001 and 2012, while Zazueta-Borboa and Ham-Chande (2021) do similarly for those who died between 2001 and 2015. The focus on the last year of life is motivated by the fact that out-of-pocket health expenditures tend to be much greater in the last year of life than in prior years, often contributing to extreme economic hardship for the individuals and their families. While the concept of resilience in aging is perhaps less relevant for the last year of life, possible similar implications for the quality of life during that time are relevant. In addition, the findings of these studies likely extend to earlier years of old age, at least to some degree.
Both studies find that the number of hospital nights is a key determinant of OOPE. Salinas-Escuerdo et al. also conclude that access to social insurance and use of public rather than private hospitals act to reduce OOPE. Zazueta-Borboa and Ham-Chande’s results in addition suggest that the number of chronic diseases and the degree of functional limitations are both associated with greater OOPE, though hospital time has a larger impact even after controlling for these underlying health conditions. They also note the challenge of accurately measuring out-of-pocket health expenditures in a country such as Mexico where such expenses might be covered by family members other than the respondent and their spouse.
In another example of how health influences economic resources, Hernández-Vásquez et al. (2018) examine how out-of-pocket health expenditures at older ages vary by health and economic characteristics in Peru. Using cross-section data from the 2017 National Household Survey on Living Conditions and Poverty, they focus on experience with OOPE during the year prior to interview for all respondents aged 60 and older (not only those who were in the last year of life). Controlling for several demographic and economic characteristics, but not including hospital stays as above, they find that individuals with chronic diseases are more likely to incur some OOPE as well as experience larger expenditure amounts. They do not find significant effects on OOPE of individuals’ functional limitations. In addition to examining how health conditions impact OOPE among the aging population in Peru, the authors also consider the influence of health insurance in possibly mediating such effects. While they find that the public insurance program for those in poverty reduces out-of-pocket health expenditures relative to those with no insurance, other forms of public health insurance are associated with larger OOPE than experienced by the uninsured. The authors explain that this pattern could be due to dissatisfaction with the quality of care available through public insurance, resulting in individuals seeking alternative, uncovered care options. Results also suggest that individuals covered by private health insurance are not significantly different from those with no insurance in their experience of out-of-pocket health expenditures. This finding could be explained, for example, by differences across these two groups in their use of health care or by inadequate protection for some forms of private insurance.
Turning to examples for high-income countries, Dobkin et al. (2018) examines the effect of a health shock, measured by hospital admission, on several measures of economic resources among those with health insurance in the United States. Using HRS data from 1992 to 2012, they estimate event study models for the effects of hospital admission for three age groups: 50–59, 60–64, and 65 and older. The measures of economic resources considered include out-of-pocket health expenditures, employment, and labor earnings, among others. For all three age groups, a hospital admission is associated with increased OOPE in the 3 years following admission, with the effect being most pronounced in the first year. In addition, for the two younger age groups, a hospital admission is strongly negatively associated with the probability of being employed and with labor earnings. Importantly for the impact on economic wellbeing, they note that while a large share of the earnings loss is insured through social security among those aged 60–64, this is generally not the case for the younger age group.
Cheng et al. (2019), using 2015/16 data for individuals aged 50 and older in Singapore, also analyze the effects of health shocks on several measures of economic resources. The data are longitudinal on a monthly basis, following individuals for 12 months, allowing for a detailed examination of the timing of health shock effects in the short run. Health shocks are measured by new diagnosis of selected diseases or conditions which they categorize as major (cancer, heart disease, or stroke) or minor (arthritis, diabetes, hypertension, or psychological issues). The economic measures considered are household income, out-of-pocket health expenditures, and non-health expenditures. The policy context for the analysis is noteworthy in that the Singapore health insurance system, in addition to including government-funded and employer-provided components, includes self-insurance through compulsory health savings accounts. Also using an event study approach, model results suggest that major health shocks have a substantial positive effect on out-of-pocket health expenditures for each of the first 4 months following diagnosis and continuing at longer intervals throughout the 12-month period. In contrast, the effects of minor shocks on health spending are smaller and of shorter duration. They also find that major health shocks to men, but not women, are negatively associated with household income with a lag of 5 to 10 months from diagnosis. Major health shocks, especially cancer, to either men or women negatively affect non-health spending in the first 5 months following diagnosis. In general, minor health shocks are found not to be significantly associated with income or non-health spending.
We provide two examples of papers that include a focus on the effects of a health shock on wealth in high-income countries. Bonekamp and Wouterse (2020) use data from 2006 to 2017 for individuals aged 65–94 in the Netherlands. Health shocks are represented by hospital admission in the prior year for any of six categories of disease or health conditions that vary in their severity, with each compared to a group with no hospital admissions for these causes in the prior year. The measures of economic resources considered include savings, total financial assets, and total net worth. The authors discuss the potential endogeneity of the health shock measures and, to reduce any biasing effects, use a difference-in-difference approach with control groups constructed from individuals who experience the same health shock at a future date. Model results show almost no significant effects of the various health shocks on any of the wealth measures and, when significant, any such effects are very small. Here it is important to emphasize the social insurance context of the Netherlands. As the authors note, income is substantially protected in old age through a universal pension program, and out-of-pocket health care expenditures are very low due to a system of universal health insurance. The latter is highly comprehensive in coverage, including, for example, long-term in-home or nursing home care.
In contrast, for the United States with its very different institutional context regarding social protections, Wallace et al. (2017) find significant negative effects of health shocks on the wealth of the aging population. They use data from the HRS from 1992 to 2010, selecting married couples where at least one member was age 51–61 at baseline. The analysis sample is defined by retirement of the male, either at baseline or by the time of any of the biennial follow-up interviews. The authors use item response theory to develop a measure of health based on responses to 21 questions about physical health, encompassing limitations in the activities of daily living and other functions, use of non-routine health services, and self-rated health. Two wealth measures are constructed from data on the net value of seven distinct components of wealth, one measuring total wealth and one measuring non-housing wealth which has greater liquidity. The two wealth measures are used to estimate long-run and short-run effects, respectively, of changes over time in the health measure. As above, the authors discuss the possible endogeneity of the health change measures, as well as possible selective sample attrition, and utilize several statistical methods to minimize any biasing effects. They document the frequency of large negative changes in health status among the retired men and spouses in their sample. Model results provide evidence of modest negative effects of health shocks on wealth in the short run, with much larger negative effects in the long run. Based on these results, the authors suggest that the level of health care insurance among the older population in the United States is sub-optimal.
Lastly, Mutambudzi et al. (2020) focus on short-term and longer-term effects of diabetes in the United States on retirement and on disability that impedes work. They use five waves of HRS data from 2004 to 2012 and a sample of employed individuals aged 50 or older at baseline to estimate multinomial logistic models across the three work status outcomes. The key explanatory variables indicate three categories with respect to diabetes: free of disease throughout, diagnosis between 2006 and 2012, or already diagnosed at baseline, with models also controlling for a variety of economic and demographic characteristics. Results suggest that long-term diabetes increases the risk of disability, but a recent diagnosis does not. Regarding retirement, the evidence suggests that both recent and long-term diabetes increase its probability, with results for the former being more robust to alternative specification. They also find that the effects of diabetes on retirement are stronger for Hispanics. The authors speculate that this difference by ethnicity could be due to any of several disadvantages among the Hispanic population in the United States such as lack of health insurance, less knowledge about diabetes self-management, and inadequate access to prevention and control programs.
In closing this section, we note that the conceptual and methodological threads mentioned above—timing of effects, sample selection, the insurance context, differences by age or across other demographic groups, and endogeneity including reverse causality—are also relevant to understanding the effects of health status on economic resources. As illustrated by the studies summarized above, the context of health insurance and other social protections are perhaps even more heavily emphasized in research on the effects of health on economic resources than the reverse. An additional thread often found in studies of health effects on economic resources, particularly in the context of low- and middle-income countries, is the potential role of the extended family. Adult children or other relatives might help to mitigate negative economic consequences of adverse health events by, for example, covering some health expenditures or providing in-home care at no financial cost. Finally, we reiterate the earlier point about reverse causality. Considering the two sets of studies together, these examples provide empirical evidence illustrating our overall conceptual argument that causality runs in both directions between health status and economic resources, creating a mutually reinforcing cycle—a cycle of resilience for some, but a cycle of vulnerability for others.
Translating Concepts to Empirical Applications
We offer a hypothetical scenario to illustrate the main elements for empirical applications of the proposed expanded framework. It is not our intent to conduct empirical analysis here but, rather, to offer ideas for how to think about conducting empirical analysis of resilience among the aging. In the example that follows, we define a list of variables to represent components of the conceptual framework. The list of variables is broad, but not necessarily comprehensive or definitive. After setting initial conditions, we introduce a shock and then follow its impact through the cycle of the conceptual framework. While the example considers the implications of a health shock, the framework could similarly be applied to empirical analysis of an economic (or social, or psychological) shock.
We postulate a hypothetical scenario that builds upon examples from previous literature to illustrate the ideas represented in the conceptual framework. We begin by recognizing that, because resilience is dynamic and changing, the availability of longitudinal data is crucial. Thus, we assume that we can follow individuals over time. Assume two persons, individual A and individual B. We assume that the two individuals have many characteristics in common, for example, same age, sex, area of residence, marital status, and no longer active in the labor force. They will also experience the same health shock that will result in hospitalization for both. We next define the characteristics that are critical for resilience, the components of social, psychological, and economic resources. We assume these resources are at levels such that individual A has higher resilience than individual B. Individuals like A have relatively high educational attainment, and enjoyed a better occupational position with health care benefits through their employed life. They received reasonable and steady income and were able to accumulate assets. They have a retirement pension and health insurance during old age. Individuals like B, on the other hand, have lower levels of these resources and experienced more disadvantage through the life course, resulting in less healthy lifestyles, a higher number of chronic diseases, more physical and cognitive limitations in old age, and a less secure economic position.
In the face of a similar health shock that leads to hospitalization, person B suffers more negative effects in several ways: a) in their economic position because of higher out-of-pocket payments, and the need to draw down savings or increase debt, b) in their psychological resources, because these economic implications for B will be more stressful, and c) in their social resources because the shock will imply that the social network will have to be activated and respond to the shock to a larger extent than for person A. Thus, persons A and B end up being affected very differently by the same shock. Moving forward over time, the greater impact of this shock for B contributes to worse health, ability to function, and overall wellbeing, and even a higher vulnerability to being hospitalized again compared to person A. Thus, the higher level of resilience for A acted as a protective shield against the consequences of the shock to a larger extent than for B.
In summary, beginning with a similar health shock, lower resilience for B implies greater negative impacts on economic, social, and psychological resources. In turn, these greater negative impacts lead to a higher likelihood of another health shock and poorer health and wellbeing outcomes for B. In contrast, the advantageous position of resources that contribute to resilience for person A provides a buffer that mitigates the negative impact of the shock. Thus, the cycle following the shock is dampened for A in comparison to B. Note that the two cases presented here, and the influences depicted by following them over time, illustrate the arrows of the conceptual framework in Figure 1 and its reinforcing cycles of resilience or vulnerability.
The data requirements for the empirical applications of resilience among older adults are demanding. Measures on several dimensions are required, some of which are retrospective regarding past events occurring over the life course, and some are prospective in nature, requiring repeated observations as follow-ups. In the past, such longitudinal studies on aging were available only for the populations of high-income countries (Ferraro & Kelley-Moore, 2003; Kaiser, 2013; Suzman & Harper, 2013). Over the last two decades, more studies have produced this type of data in the field of aging, including for low- to middle-income countries. Some of these longitudinal studies have the added feature that they are comparable to the Health and Retirement Study (HRS) in the United States allowing for cross-national comparisons.
These longitudinal data sets, such as the Mexican Health and Aging Study (MHAS), are well-suited for empirical applications and analysis of resilience and vulnerability. They include many dimensions of life (e.g., physical health, economic, social, psychological) and cover a long period of time with several waves of observation, capturing the cycles of shocks and their likely consequences. Examples of analyses that use longitudinal data, including several that use MHAS data, and focus on parts of the cycle are provided in the synthesis of literature above. A detailed description of the MHAS, along with study profiles, can be found in Wong et al. (2017) and at the MHAS website, www.MHASweb.org, where the data can also be accessed. Study profiles and data descriptions for similar longitudinal data sets in other countries are available as follows: Bӧrsch-Supan et al. (2013) for SHARE in Europe, Gómez-Olivé et al. (2018) for HALSI in South Africa, Perianayagan et al. (2022) for LASI in India, Raina et al. (2019) for CLSA in Canada, Sonnega et al. (2014) for HRS in the United States, Steptoe et al. (2013) for ELSA in England, Zhao et al. (2014) for CHARLS in China, and Lima-Costa et al. (2022) for ELSI in Brazil, among others. These surveys are rich in the kind of data that is required for analysis of resilience among the aging. 1
An additional source for scholars interested in empirical research on resilient aging is the Gateway to Global Aging Data (www.g2aging.org), a web-based resource funded by the National Institutes of Health (NIA/NIH), for harmonizing and providing information on how to access multidisciplinary longitudinal data on aging, health, and retirement from the international family of Health and Retirement surveys. This resource includes many of the studies mentioned above, and can guide researchers regarding where to obtain the data for each country study, which variables are available in each study, and which of the variables are comparable across studies.
Here we outline the main variables for the empirical analysis of resilient aging, all of which are available in the MHAS and in most of the similar longitudinal studies mentioned.
Health Status
• Self-reported global health • Diagnosed chronic diseases • Physical function limitations • Cognitive function • Depressive symptoms
Shocks
Health Shocks
• Hospitalizations • Falls with major consequences such as surgery • New diagnosis of major chronic diseases (e.g., cancer, heart disease, lung disease) • New diagnosis of Covid-19
Economic Shocks
• Loss of income sources or substantial reduction in income • Major damage to property due to accident or natural disaster • Forced migration due to civil conflict or violence • Reduction in asset value • Unexpected expenses
Social Shocks
• Recent divorce • Recent widowhood • Recent loss of a child • Recent loss of another close relative or friend
Psychological Shocks
• Recent trauma, such as victim of recent crime or accident affecting health or family situation • Having to change residence, for example, to live with children or in a nursing facility, in order to manage daily life
Resources for Resilience
Economic Resources
• Health insurance • Life insurance • Financial assets • Real estate and business assets • Consumer durables • Income by source (labor, family support, pensions, returns on financial assets) • Educational achievement
Social Resources
• Social activities such as volunteer work, helping with family care, hobbies, sports activities • Frequency of contact, size of network living nearby (family, including children and grandchildren, and friends) • Family and friends who can be counted on in emergencies
Psychological Resources
• Sense of control • Connectedness vs loneliness • Personality traits • Life satisfaction
In addition to outlining the relevant categories of variables that are available in the MHAS and other data sets mentioned above, we also underscore the importance of the longitudinal nature of these data. Longitudinal studies allow us to apply the conceptual framework through follow-up interviews, wherein at wave-1 we observe characteristics representing health status and the resources that form resilience, and then can follow individuals through the reinforcing cycles of the framework. In wave-2, for example, we can observe if a shock has occurred since wave-1. Then, the effects of the shock on health and wellbeing can be observed in wave-3. In turn, the health effects observed in wave-3 can be examined for effects on the level of resources for resilience observed in wave-4, and so on. Furthermore, as illustrated by some of the literature reviewed herein, depending on the timing of the interview waves such data sets can be used to examine whether any of the hypothesized effects of the cycle of resilience are immediate or lagged in nature, or are short-lived or long-lasting.
Conclusion
In conclusion, we have presented a conceptual framework to study resilience that builds on previous frameworks, adding the role that economic resources play as part of resilience, and incorporating the idea that there is a reverse influence of health outcomes, behaviors, and wellbeing on the resources that form resilience. We presented illustrative findings from the literature to support these points. We believe that the state of the field is rich in data to conduct empirical research on resilience in old age, and we illustrated the measures that are available for this work using as an example one of the longitudinal studies on aging, the Mexican Health and Aging Study. This empirical work—which focuses on micro-resilience—should help identify the groups that are most vulnerable or least resilient in cases of shocks, to inform the design of policies and programs to potentially anticipate and ameliorate the consequences of such shocks in the future and, thereby, strengthen the macro-resilience of society.
Our contribution has extended the literature by explicitly adding the role of economic resources to a conceptual framework on resilience, and by highlighting evidence using a variety of data sources documenting the critical role of economic resources in resilience of the aging. This evidence provides a close view of examples from the empirical literature on aging, allowing us to appreciate the wide variety of outcomes and variables representing the economic resources that contribute to resilience, even if these authors are not always using the term ‘resilience’. We encourage researchers to examine resilience in aging with empirical data using this expanded conceptual framework, given the richness of longitudinal data sources described above that the field now offers, which ought to support this line of research in both high-income and low- and middle-income countries.
In particular, the current pandemic is a major shock with consequences in several areas, and the existing longitudinal studies should provide data to better understand the level of resilience among older adults to withstand a shock of this nature. We hope that this paper provides motivation and general guidance to conduct research along these lines, as there is much to contribute empirically about resilience in aging in low- and middle-income countries, both in specific countries and using cross-national comparisons.
Footnotes
Acknowledgments
A previous version of the paper was presented as keynote address at the 2021 Annual Meeting of the International Conference on Aging in the Americas. The authors appreciate the comments from the conference audience as well as the contributions from the anonymous reviewers. We acknowledge support from the Mexican Health and Aging Study, which is partly sponsored by the National Institutes of Health/National Institute on Aging (R01AG018016) in the United States and the Instituto Nacional de Estadística y Geografía (INEGI) in Mexico. We also acknowledge support from the Texas Resource Center for Minority Aging Research (NIA/NIH P30AG059301).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.