
Abstract
The current study investigated how pain and BMI trajectories mediate the influence of family stress (1991–1994) on later-life impaired functionality (2017) in women. The study used prospective data from 244 mid-older rural Midwest Caucasian women who were in long-term marriages over a span of 27 years. Within the structural equation framework, the analytical model used latent constructs of family stress and trajectories of pain and BMI to predict later-life functionality. BMI and pain trajectories mutually influenced each other in forming a self-perpetuating cycle over time in mid-older women. Further, midlife family stress shaped BMI and pain trajectories, and these trajectories had consequences for later-life functionality, as defined by three kinds of impairments: physical, cognitive (subjective memory), and social (loneliness). The findings emphasize the need for policies and interventions that focus on reducing women’s stressful family circumstances in middle years to weaken and redirect their association with BMI and pain trajectories.
Today, most of the “baby boom generation” are in the latest stage of their life span, later adulthood. The wellbeing of these individuals, which is largely determined by their later-life functionality—the ability to perform daily activities in important domains—is a public health concern. Yet less is known about the life course processes leading to their later-life functionality.
Consistent with the biopsychosocial model of pain (Gatchel et al., 2007), social stress influences physical pain trajectories through neurological stress responses. Furthermore, previous stress-health research (Krueger & Chang, 2008; McEwen & Gianaros, 2010; Nazmi et al., 2009) has documented that social stress influences BMI trajectories through physiological and behavioral stress responses. More importantly, BMI and physical pain have been shown to influence each other mutually over time (Radojčić et al., 2021) and have consequences for health and functionality in later years (Eccleston, 1995; Hassing et al., 2010; Hergenroeder et al., 2011; Wickrama et al., 2021a; Yiengprugsawan et al., 2020). This possibility suggests a joint mediating life course process consistent with the life course perspective (Elder & Giele., 2009) in which stressful life experiences influence associated BMI and pain trajectories, which in turn contribute to functionality in later years. However, previous studies in this area have been largely fragmented and have not investigated such a life course process stemming from stressful life experiences that leads to later-life functionality.
Later-life functionality has several dimensions, including physical (e.g., physical limitations), cognitive (e.g., subjective memory impairment), and social (e.g., loneliness) impairments. Loneliness reflects deficiency in social relationships and poor social functioning, which are increasingly recognized as an important dimension of later-life functionality (Gyasi et al., 2022). Subjective memory impairment in later adulthood can influence older adults’ ability to function and live independently (von Gunten et al., 2005). Physical limitations in participating in life tasks are essential aspects of later-life functionality (Greyen et al., 2015). Previous studies have shown that these impairments are comorbid in later years, suggesting a shared underlying pathological condition (Covinsky et al., 2009) that may be reflected as a latent construct of functionality defined by multiple impairments. However, research has rarely focused on such a construct of later-life impaired functionality.
The present study focused specifically on married, mid-older (>40 ears) women. Intragroup investigations, more generally, and investigations of this specific group in particular, are important for several reasons. Women experience changes in bodily hormonal systems in their middle years that are consequential for their health/wellbeing trajectories (Dennerstein & Soares, 2008). In addition, feelings of stressful life experiences may be strongly associated with the depletion of psychological resources that may contribute to health problems, such as physical pain (Wickrama et al., 2021b). Furthermore, mid-older women typically experience a higher prevalence of pain and weight problems than men (LeResche & Drangsholt, 2001; Salk et al., 2017), which are likelier to be comorbid in women than in men (Rosa et al., 2021). However, an in-depth understanding of the life course processes involving BMI and pain trajectories leading to later-life functionality in women is lacking.
Literature Review
Family Stress and BMI Trajectories
We expect that family financial stress and marital stress of women in long-term marriages are strongly associated and have a shared variance, forming an underlying construct of family stress (Conger et al., 2010). Long-term exposure to family stress may contribute to physiological dysregulation in men and women which is observable through increased BMI over the middle and later years (Wickrama et al., 2018a; Wickrama, O'Neal, et al., 2018b).
In addition, family stress may influence BMI by initiating and sustaining unhealthy behaviors (Devine et al., 2003). Feelings of distress stemming from family stress may partly explain this connection. That is, many unhealthy behaviors, such as eating foods rich in sugar and fat that result in weight gain may reflect individuals’ stress coping mechanisms (Krueger & Chang, 2008). Furthermore, poor eating and sedentary behaviors have pro-inflammatory effects, which also result in a high BMI (Nazmi et al., 2009).
The life course perspective contends that early disadvantages lead to later adverse health outcomes particularly through shaping health-risk (e.g., bio-markers, symptoms, complaints, perceived health) trajectories over the life course (Elder & Geile, 2009). Accordingly, we expect that family stress influences not only contemporaneous levels of BMI but also subsequent changes (slope) of BMI. That is, the adverse influence of family stress on BMI may increase over time (an interaction with time).
Family Stress and Pain Trajectories
Research has shown that the prevalence of chronic pain is disproportionately higher among socioeconomically disadvantaged groups (van Hecke et al., 2013). The biopsychosocial model suggests that social factors, such as family financial hardship and marital problems, influence the development of physical pain (Chou et al., 2016; Wickrama et al., 2021b, 2022) through a brain-pain mechanism (Gatchel et al., 2007). We expect stress to be associated with individual pain experiences through brain-pain mechanisms. Neurophysiological research suggests that chronic stress may rewire the brain, resulting in changes in brain structure and functions. These alterations in the brain may have implications for the modulation of pain perception and sensations of physical pain (McEwen et al., 2015; Gatchel et al., 2007). In addition, stress may influence the development of pain through the depletion of psychological resources, such as sense of control in husbands and wives (Landau et al., 2015; Wu, 2016). Research suggests that reduced feelings of control may have an adverse impact on physical pain through neurological and physiological processes (McEwen & Gianaros, 2010; Randles et al., 2013).
As in the case of BMI, we expect that family stress not only influences contemporaneous levels of pain but also subsequent changes (slopes) in pain due to the cumulative influence of family stress on pain. That is, the adverse influence of family stress on pain may increase over time (an interaction with time).
Dynamic Association between BMI and Pain Trajectories During Mid-Later Years
Research suggests that higher BMIs and pain levels are significant comorbidities. Okifuji and Hare (2015) proposed several potential mechanisms underlying these comorbidities, including mechanical factors, chemical mediators, and lifestyle factors, that may be responsible for their comorbidity. Regarding mechanical factors, research has shown that increased loading on joints and the spine and defective structural changes due to higher BMI may result in bodily pain (e.g., Ding et al., 2005). With regard to chemical mediators, higher BMI can be considered markers for systemic inflammation (elevated C-reactive protein (CRP) and leptin and a deficiency in vitamin D) that have been shown to contribute to pain (Pereira-Santos et al., 2015). Regarding lifestyle factors, physical inactivity and a sedentary lifestyle have been shown to increase both BMI and pain (Strøyer & Jensen, 2008).
Conversely, weight gain may occur as a result of chronic pain. Distress stemming from functional limitations associated with pain may lead to overeating (Janke et al., 2012). Moreover, research has shown that both obesity and chronic pain are associated with feelings of distress (e.g., Tietjen et al., 2007). Adverse effects of chronic pain, such as a sedentary lifestyle, poor sleep, and side effects of medications, may also contribute to greater BMI (Knustson & Cauter, 2008). Additionally, pain has been shown to increase insulin resistance, which may contribute to an increase in BMI through metabolic imbalance (Greisen et al., 2001).
In particular, longitudinal studies suggest that high levels of BMI contribute to the development of pain over time, forming increasing pain trajectories. For example, obese individuals, particularly those who are inactive, have a greater risk of developing chronic arm and low back pain over several years compared to those who were not obese (Mork et al., 2013). Similarly, these findings suggest that individuals with chronic pain tend to gain weight over time, forming increasing BMI trajectories (Radojčić et al., 2021). Thus, we also expect that the initial level of BMI trajectories influence the slope of pain trajectories and vice versa forming a self-perpetuation cycle of BMI and pain.
BMI Trajectories and Later-Life Functionality
Overweight and obesity have been shown to have adverse impacts on multiple dimensions of individuals’ functionality, including physical, cognitive, and social impairments (Hassing et al., 2010; Hergenroeder et al., 2011). First, obese women score lower on physical functional capacity (Hergenroeder et al., 2011. Second, previous research has shown that even when controlling for cognitive decline due to aging, BMI is negatively associated with global cognitive performance, including short-term memory (Hassing et al., 2010). Third, recent research (e.g., Rotenberg, 2017) has reported that obese participants demonstrated lower emotional trust in close others, less disclosure to close others, and greater loneliness compared to normal-weight or overweight participants. As previously discussed, we expect that physical and cognitive impairments and loneliness have a shared variance, with the potential of forming a shared construct of functionality in later years.
Pain Trajectories and Later-Life Functionality
Chronic pain has been shown to have adverse impacts on multiple dimensions of individuals’ functionality. A recent study showed that those who reported “low to medium” pain and “severe” pain belonged to the most vulnerable group with the worst functional health outcomes compared with those with no pain (Yiengprugsawan et al., 2020). Studies have also shown that elderly adults with more severe pain had poorer performance on memory tests compared to elders with no or less pain that may be attributed to the fact that pain is mentally distracting and limit social engagement (Eccleston, 1999).
The Present Study
There are three study objectives. Figure 1 presents a graphical depiction of the model used to address these research objectives. Theoretical framework: Later-life functionality in married women.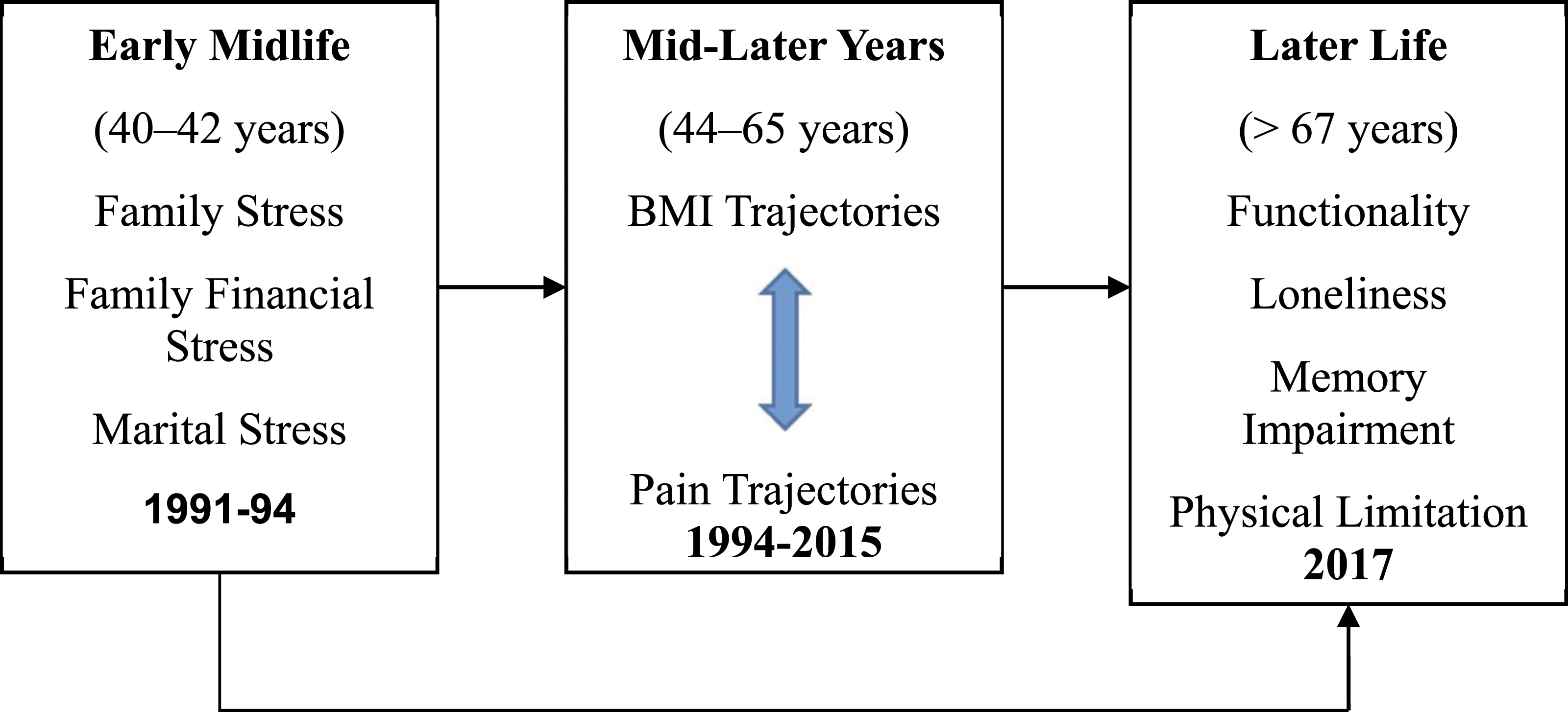
The first objective was to investigate (a) the existence of a global construct of family stress as indicated by multiple indicators including family financial and marital stresses in middle years; (b) the existence of a global construct of functionality in later years in married women as indicated by multiple indicators including physical limitation, impaired memory and loneliness; and (c) the association of these global constructs over mid-later years.
The second objective is to investigate the comorbidity and the self-perpetuating process of BMI and pain trajectories over the mid-older years.
The third objective is to investigate the mediating effect of BMI and pain trajectories on the association between midlife family stress and later-life functionality in married women.
To accomplish these objectives, prospective data were examined from 244 women in enduring marriages (more than 40 years) over a period of 27 years (1991–2017).
Methods
Sample
The data used to accomplish these study objectives are from the Iowa Youth and Family Project (IYFP, 1989–1994), which was later continued as two panel studies: the Midlife Transitions Project (MTP) (2001) and the Later Adulthood Study (LAS) (2015–2017). Together, these projects provide data over 27 years on rural families from a cluster of eight counties in north-central Iowa that closely mirror the economic diversity of the rural Midwest. The IYFP began in 1989 as a study of rural couples with children, at least one of whom was a seventh-grader in 1989 (Conger & Elder, 1994). The present study was limited to wives who were consistently married from 1991 to 2017 (n = 244) and participated in 1991, 1994, 2001, 2015, and 2017 data collections.
The sample was limited to women still married in 2017 because the study primarily focused on later-life functionality of women who were continuously married. That is, to estimate the overall model with pain and BMI trajectories and the functionality of continuously married women (1991–2017), we needed prospective data from those women during that period. The study sample of continuously married women included 61% of the total married women in 1991. This means that 39% of the women had disruptions in their marriages during the period 1991–2017 and were thus excluded from the study.
Comparison of Background and Initial Status Between the Total sample (1991), Dropped-out (1991–2017) and Stayers (2017).
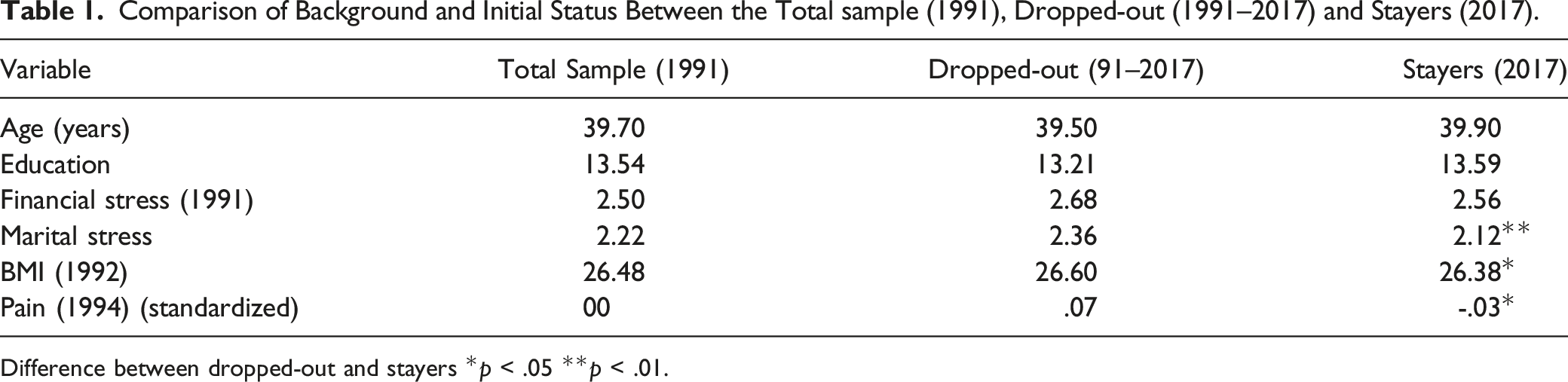
Difference between dropped-out and stayers *p < .05 **p < .01.
In 1991, the women were in their early middle years. Their mean (range) age was 39.70 years (31–55 years). On average, the women had been married for 19 years and had three children. The median age of the youngest child was 12 years. The mean number of years of education was 13.54 years. Owing to the few minorities in the rural area studied, all the participating families were white.
Data collected in 1991, rather than 1989, were used as the first time point of the present study due to the availability of study variables. This research was approved by the University of Georgia Institutional review board (STUDY 00001438). (STUDY 00001438).
Measures
Marital Stress
Consistently married mothers reported on their spouse’s perceived hostile behavior, destructive conflict resolution behavior, and marital instability in 1991, 1992, and 1994. At each time point, a composite measure was computed using standardized measures. The average of 1991, 1992, and 1994 composite measures were used as the measure of early-midlife marital stress.
Hostile marital behaviors were measured in 1991, 1992, and 1994. Married mothers indicated how often (1 = always; 7 = never) during the past month her partner engaged in 15 hostile behaviors (Matthews et al., 1996). Sample items included “get angry at you,” “shout or yell at you,” and “make you feel guilty.” Responses were reverse coded and averaged with higher scores representing a higher level of hostility (the range of Cronbach’s α was 0.89 to .90 for mothers across years).
Eight items assessed mothers’ reports of their spouses’ destructive conflict resolution behaviors in 1991, 1992, and 1994 (e.g., “criticizes you or your ideas for solving the problem,” “ignores the problem,” and “seems uninterested in solving the problem”) (Matthews et al., 1996). All items were scored on a 7-point Likert scale ranging from 1 = always to 7 = never with higher scores indicating more destructive problem-solving behaviors. Mean scores were computed. The internal consistencies varied from 0.79 to 0.90 from 1991 to 1994.
To create the measure of marital instability, or divorce proneness, we used a modified version of the five-item short form of the Marital Instability Index (Booth et al., 1983), a scale that has demonstrated validity and reliability. In 1991, 1992, and 1994 women were asked questions such as how recently either of them suggested getting divorce and discussed the possibility of getting divorce with a close friend, thought about divorce, (1 = not in the last year, 4 = within the last three months). Mean scores were computed. The internal consistencies varied from 0.64 and 0.71 from 1991 to 1994.
Family Financial Stress
Financial stress was measured in 1991, 1992, and 1994 using a four-item scale developed by Conger and Elder (1994). Respondents reported their perceived financial strain to items such as “we have enough money to afford the kind of food we need” and “we have enough money to afford the kind of medical care we need” with responses ranging from 1 (strongly disagree) to 4 (strongly agree). Internal consistencies of this measure varied from 0.75 to 0.78. The average of 1991, 1992, and 1994 composite measures were used as the measure of early-midlife financial stress.
Body mass index (BMI)
Respondents reported their height and weight in 1994, 2001, and 2015. From this information, their BMI, the ratio of weight to height squared ([lbs*703]/inches2), was calculated for each occasion. The baseline BMI (1992) distribution was as follows: <25 kg/m2 52.00%, between 25 and 30 kg/m2 26.60% and 30 kg/m2 21.40%.
Physical Pain and Physical Limitation
Recent studies have documented that simple self-assessment questions on physical limitations (Amiard et al., 2019) and physical pain (Bemmel et al., 2019) are useful tools with acceptable validities for evaluating physical limitations and physical pain in adult populations. In the present study, we use self-reports measures of physical limitation and physical pain.
Physical Pain
The degree of physical pain was assessed in 1994, 2001, and 2015 using two items from the Rand Health Science Program in Health Survey 1.0 (Hays et al., 1993). On a 6-point scale ranging from 1 (none) to 6 (very severe), respondents indicated how much bodily pain they experienced in the four preceding weeks. Also, on a 5-point scale ranging from 1 (not at all) to 5 (extremely), respondents indicated how much pain interfered with their normal work. Responses were standardized and averaged. The correlation between the two items ranged from 0.68 and 0.70 over the measurement occasions.
Physical Limitations
In 2017, the 10-item Physical Impairment Scale of the Rand 36-Item Health Survey 1.0 (Hays et al., 1993) captured impairment for vigorous (e.g., running or lifting heavy objects) and moderate activities (e.g., moving a table, pushing a vacuum cleaner, lifting or carrying groceries) ranging from 1 = No, not limited at all to 3 = Yes, limited a lot. Responses were averaged to create a measure of overall physical limitations. Cronbach’s alpha for the measure was 0.80.
Subjective Memory Impairment
Using the revised, shortened Everyday Memory Questionnaire (R-EMQ), three aspects of memory performance were assessed in later life (2017), including “retrieval,” “attentional tracking,” and “visual reconstruction” (Royle & Lincoln, 2008). The 13 items indicated SMI in the previous month. Sample items included “having to check whether you had done something that you should have done” and “forgetting when it was that something happened; for example, “was it yesterday or last week” (1 = Once or less in the last month, 5 = Once or more in a day). A mean score was computed with higher scores indicating more SMI. The scale’s internal consistency was 0.93.
Loneliness
Participants completed the UCLA Loneliness Scale (Russell et al., 1978) in 2017. The 20-item scale was designed to measure one’s subjective feelings of loneliness as well as feelings of social isolation on a 4-point scale (1 = Never; 4 = Often). Items were averaged. The scale’s internal consistency was 0.80.
Data Analysis
Analyses were performed using structural equation modeling (SEM) and Mplus software (version 8.0; Muthén & Muthén, 1998-2018–2017). First, using multiple indicators of family stress and later-life functionality, we examined latent constructs of family stress and later-life functionality and the correlation between these two latent constructs. Second, using three repeated measures (1994, 2001, and 2015), we examined linear trajectories of pain and BMI estimating latent growth curves (LGCs) in a parallel process model, more specifically a parallel trajectory model with mutual influences between the level of one trajectory and slope of the other (Wickrama et al., 2016). We examined mutual influences of the level of one trajectory on slope of the other. Finally, we incorporated predictors (family stress) and outcomes (later-life functionality) into the BMI-pain parallel trajectory model.
A range of fit indices was used to evaluate model fit, including the χ2 test of model fit, the comparative fit index (CFI), and the root mean square error of approximation (RMSEA). For the χ2 fit statistic, the model is thought to fit the data well when the x2 divided by the degrees of freedom is below 3.0 (Carmines & McIver, 1981). When the CFI value is near or greater than 0.95 and the RMSEA value is close to or less than 0.06, this suggests that the model fits the data well (Hu & Bentler, 1999). Some data were missing for a specific wave of data collection (nearly 9% of the data). Full information maximum likelihood (FIML) was utilized to test the hypotheses with all available data.
Results
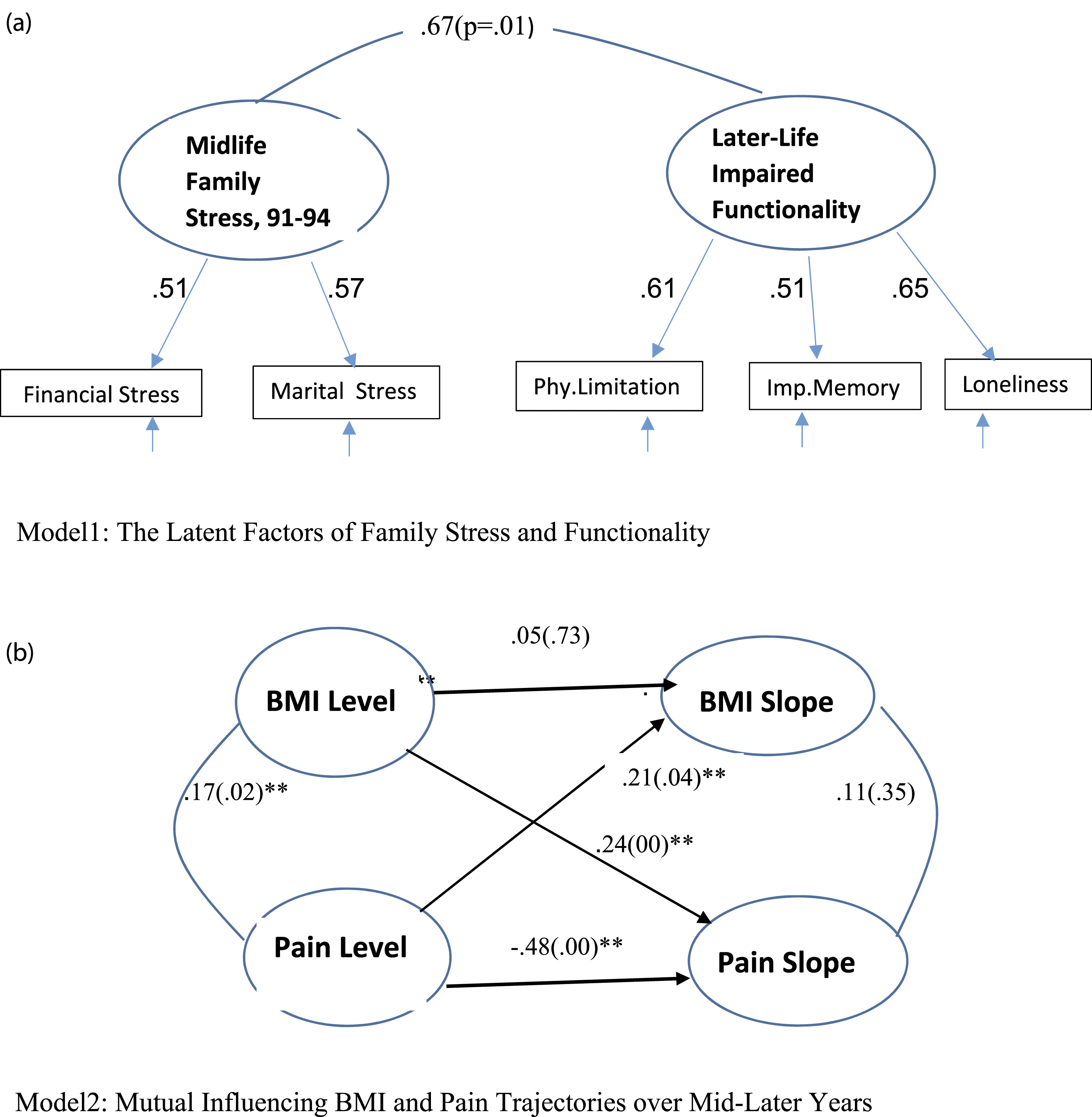
Confirmatory Factor Analysis for Family Stress and Functionality
Bivariate Correlations Among Study Variables.
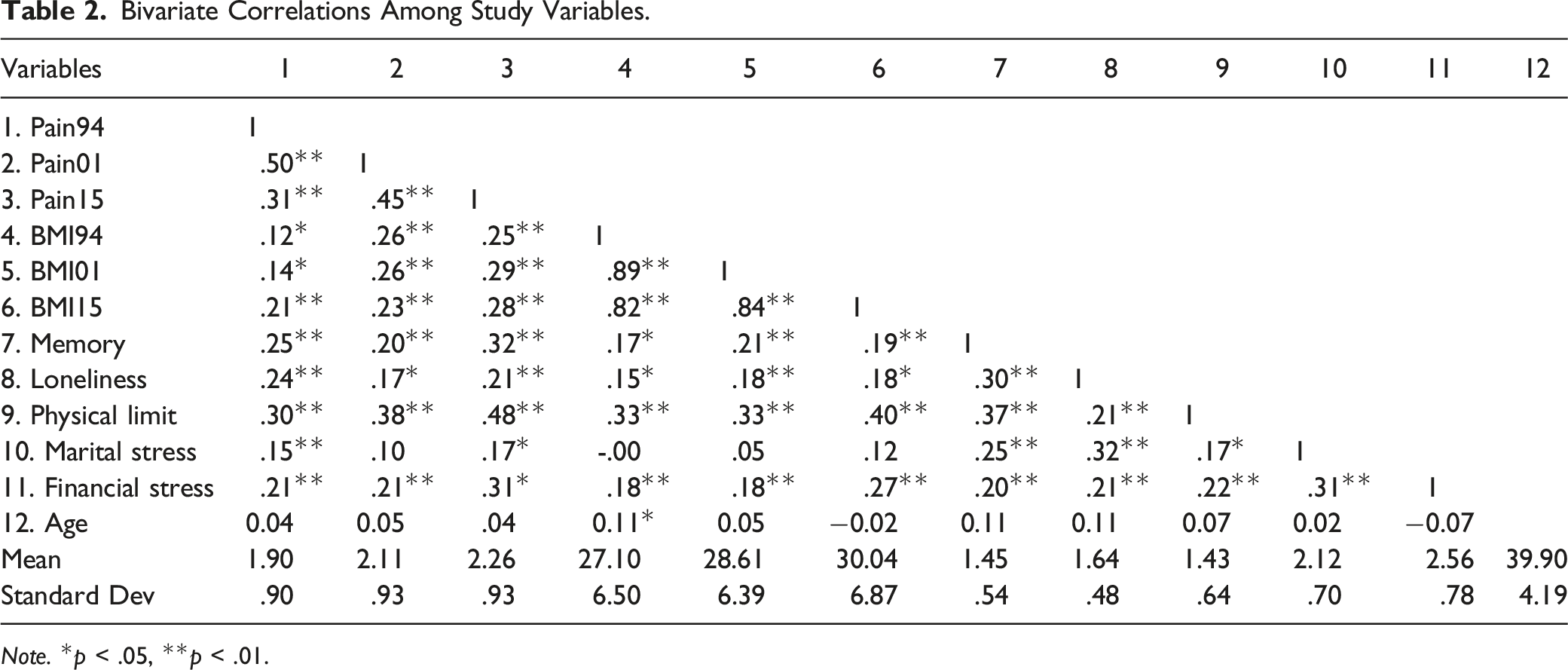
Note. *p < .05, **p < .01.
Preliminary models: Confirmatory latent factors and growth trajectories.
Parallel Process Trajectory Model
Before estimating parallel process trajectory model, we estimated univariate trajectories of BMI and pain, separately. The results showed that linear growth curves showed acceptable fit well with data for both BMI (x2(1) = 4.10, RMSEA = 0.07, CFI = 0.98) and pain (x2(1) = 2.84, RMSEA = 0.06, CFI = 0.99). Both trajectories showed increasing linear trends over time. Means (variance) of the level and slope for BMI growth curve were 27.19, p = 01, (25.90), p = 0.10 and 1.12, p = 0.04, (0.11), p = 0.03, respectively and means (variance) of the level and slope for pain growth curve were 1.92, p = 0.01, (0.54), p = 0.03 and 0.15, p = 0.01, (0.10), p = 0.04, respectively.
The parallel process trajectory model of BMI and pain (Model 2) presented in Figure 2 panel B showed an acceptable fit to the data (x2(7) = 20.00, RMSEA = 0.08, CFI = 0.98). The initial levels of BMI and pain were significantly correlated (r = 0.17, p = 0.03). However, correlation between BMI slope and pain slope was not significant (r = 0.11, p = 0.33). Importantly, the initial level of BMI significantly predicted slope of pain (0.24, p = 00) and the initial level of pain predicted slope of BMI (0.21, p = 0.04) in this model, showing cumulative mutual influences between BMI and pain over time. This suggests a self-perpetuating process between BMI and pain over mid-older years for married women (objective 2).
Testing the Comprehensive Mediational Model (Objective 3)
Next, as shown in Figure 3 (Model 3), the predictor, family stress, latent construct and the outcome, impaired functionality latent construct, were added to the parallel process model of BMI and pain trajectories. This mediational model showed an acceptable fit to the data (x2(32) = 53.20, RMSEA = 0.05, CFI = 0.98). The following description presents the results from the left to the right of the model. The initial levels of BMI and pain were positively predicted by family stress latent construct (β = 0.20, p = 00 and β = 0.40, p = 01). That is, women who experienced more midlife family stress averaged higher initial levels for BMI and pain trajectories. Also, women who experienced more family stress generally reported a greater increase in their pain over time (β = 0.37, p = 0.01) suggesting a cumulative influence of family stress on pain. However, women who experienced more family stress did not experience a significant increase in their BMI over time (β = 0.06, p = 0.60). In this model, as in Model 2, the initial level of BMI significantly predicted slope of pain (β = 0.17, p = 0.01) and the initial level of pain predicted slope of BMI (β = 0.29, p = 0.01) showing the existence of a self-perpetuating process between BMI and pain. Model 3: Midlife family stress and later-life Impaired functionality in women: Mediation role of mutual influencing BMI and pain trajectories. Note. Standardized coefficients (p values are in parentheses), Age influenced on BMI level, pain level, BMI slope, pain slope, and functionality were 0.13(0.05), 0.11(0.15), −0.24(0.02), −0.01(0.91), and −0.01(0.83).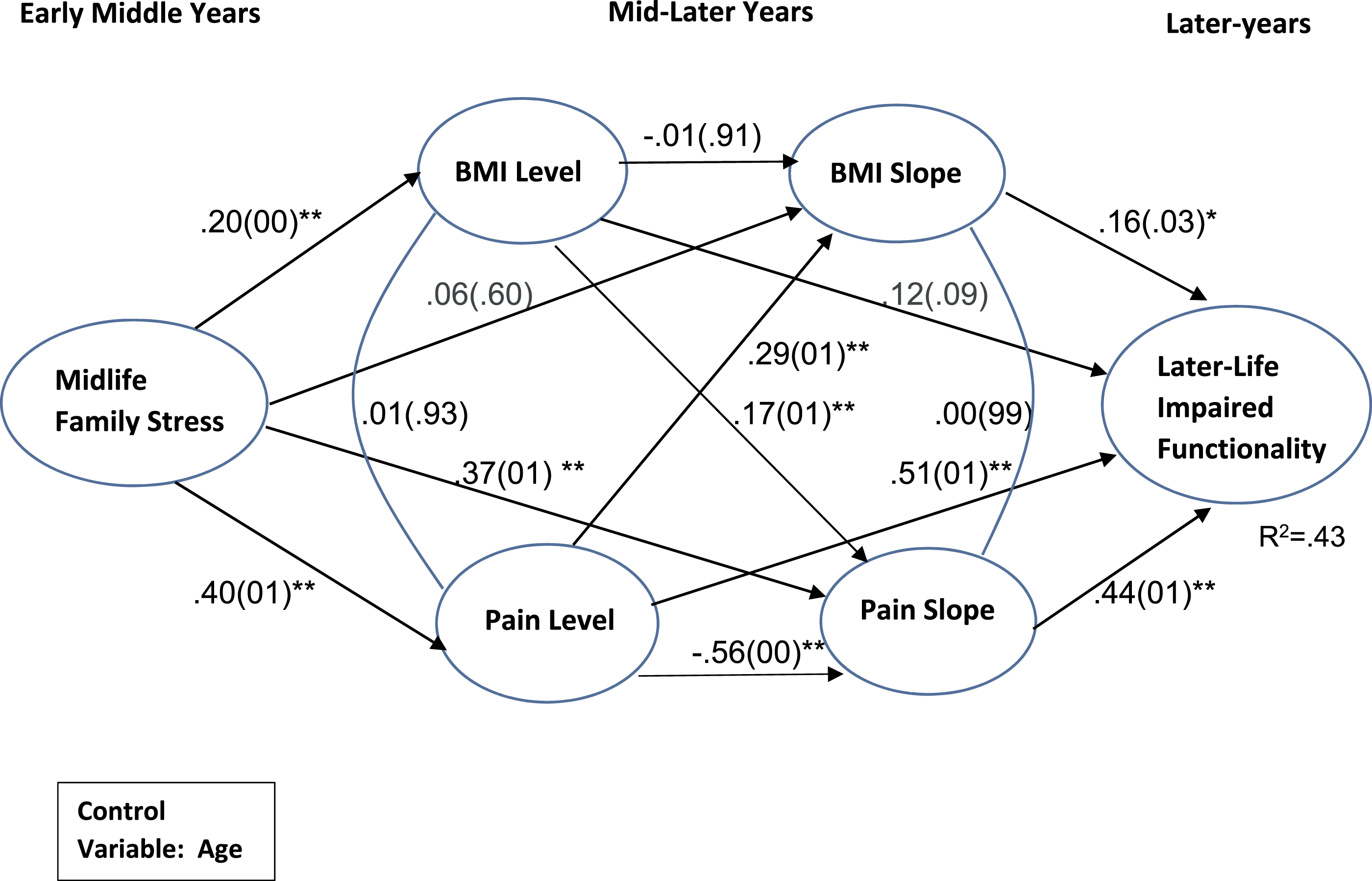
Regarding later-life functionality outcomes, the initial level of women’s pain (1994) significantly predicted their impaired functionality (β = 0.51, p = 0.01) in 2017. The initial level of women’s BMI (1994) marginally predicted their impaired functionality (β = 0.12, p = 0.09). The rates of change (slopes, 1994–2015) in both BMI and pain trajectories significantly predicted impaired functionality (β = 0.16, p = 0.03 and β = 0.44, p = 0.01) in 2017. All growth factors of BMI and pain trajectories explained 43% variance of later-life impaired functionality in married women. In this model, the direct effect of family stress on later-life impaired functionality was not significant (not shown in Figure 3). The loadings of indicators of family stress and later-life impaired functionality remained essentially the same as in previous CFA model 1 presented in Figure 2(A).
We tested indirect effects of the comprehensive model using bootstrap procedure available in Mplus (version 8). The indirect effect from family stress on impaired functionality through the level and slope of pain trajectories were significant (β = 0.21, CI: .02,.42), and β = 0.18, CI: .01,.49), respectively). Indirect effect of family stress through the level of BMI trajectories on impaired functionality was significant (β = 0.05, CI: 0.01, 0.24). The total indirect effect from family stress on impaired functionality was (β = 0.44, CI: 0.14, 0.94). In sum, the results of the comprehensive model provided evidence supporting objective 3.
Discussion
Previous theoretical and empirical research has documented associations among women’s stressful life experiences, BMI and pain trajectories, and later-life functionality. However, these studies have been largely fragmented and have not investigated the dynamics of BMI and pain trajectories, and their mediating roles in linking stressful life experiences to later-life functionality in women within a single analytical framework. To fill this research gap, the present study addressed three study objectives.
Related to the first study objective, the results of the current study confirmed the existence of significantly correlated latent constructs of family stress and later-life impaired functionality reflecting underlying common conditions of multiple stressors/impairments. Improved understanding of family stress and later-life impaired functionality would provide important insights for family-marital therapists and clinical care practitioners regarding whether to emphasize care/therapy for constituent stressors/impairments separately or common conditions reflecting all indicators simultaneously.
With regard to the second study objective, consistent with previous research findings (Okifuji & Hare, 2015), the levels of BMI and pain were contemporaneously associated in the middle years. However, their linear changes (slopes) were not significantly associated suggesting divergent trajectories of BMI and pain over mid-older years. Importantly, the initial level of BMI positively influenced change in pain, while the initial level of pain positively influenced change in BMI over time. These longitudinal mutual cumulative influences resulted in a self-perpetuating cycle of BMI and pain in women over their mid-later years. That is, high levels of BMI and pain in the middle years put women at risk of increasingly adverse trajectories of BMI and pain over their mid-later years. These findings regarding the relationship between BMI and pain trajectories may inform preventive measures and therapeutic strategies for pain.
Related to the third study objective, the results showed that family stress positively influenced trajectories of BMI (the level) and pain trajectories (both the level and slope). As the level of trajectory of an attribute reflects the severity of the problem, and slope reflects the deterioration or recovery over time, these independent influences elucidate how family stress contributes to weight and pain problems over the mid-older years. The influence of family stress on pain trajectories is consistent with the biopsychosocial model of pain, which suggests that social stressors may activate brain regions, resulting in neurological conditions leading to physical pain (Chou et al., 2016). Importantly, the influence of family stress on subsequent changes in pain reflects the cumulative nature of this influence, suggesting that the influence of family stress on pain strengthens over time—an interaction between family stress and time. Future studies should further elucidate the responsible cumulative mechanisms through which family stress influences changes in pain.
These results showed that family stress contemporaneously influences the level or severity of BMI. This is consistent with stress-health research, which posits that stress influences BMI through physiological and behavioral responses (McEwen & Gianaros, 2010). Importantly, family stress influences the levels of both BMI and pain trajectories, which in turn initiate a self-perpetuating cycle of BMI and pain. This highlights the need to identify factors that can weaken the associations between family stress and the levels or severity of BMI and pain in early middle years.
Both BMI and pain trajectories over mid-later years predicted the functionality of women in later life, as defined by physical impairments, subjective memory impairment, and loneliness. The levels and slopes of BMI and pain trajectories uniquely influenced the impaired functionality of women in later years. This indicates the importance of considering both severity (the levels) and increases/decreases (changes over time) in BMI and pain trajectories as unique contributors to impaired later-life functionality.
Several factors potentially limit the scope and generalizability of these results. First, the sample comprised only European-American middle-aged women who were mothers living in the rural Midwest. Moreover, this cohort of rural women experienced the economic downturn of the rural farm crisis in the late 1980s (Conger & Elder, 1994). Thus, although the findings enhance our understanding of early midlife family stress, pain and BMI trajectories, and later-life impaired functionality, caution is warranted in generalizing these results. Studies testing similar models with more diverse samples are needed. Future samples should include both men and women, as well as greater racial/ethnic diversity and variation in geographic location. Likewise, the study sample was limited to women in long-term marriages. Second, the present study used self-reporting measures. Replication using more objective measures (e.g., welfare receipts, and clinical measures) is needed. Third, unmeasured confounding constructs may contribute to the associations found in the present study. Two likely constructs to include in future research are additional sociodemographic characteristics, such as accessibility to health insurance, and other stressful experiences, such as work and parental problems. Fourth, because of the long measurement intervals, the present study may not fully reveal the continuity and intricacies of changes in BMI and pain trajectories. Fifth, although we have ensured the proper temporal order of constructs, there may exist reversed causation between constructs. Sixth, the present study did not investigate the synergistic influence of BMI and pain trajectories on impaired functionality. Finally, Survival bias might have potentially impacted our results. Women who experienced good health during the study period might have been more likely to have stable marriages and remained in the sample.
This study addressed several methodological concerns. First, we estimated the long-term trajectories of BMI and pain and used them as outcomes of family stress and predictors of impaired functionality within the same analytical framework. The comprehensive SEM model using shared latent constructs and growth factors of attributes allowed the investigation of higher-level health/wellbeing processes over the life course. Nevertheless, these findings highlight how family stress persistently influenced later-life functionality through long-term life course trajectories of BMI and pain in married women. Future interventions should not overlook social antecedents, particularly family stressors, as potential causes of physical pain and weight problems. Clinical implications also include the importance of considering the possible comorbidity and self-perpetuating process of BMI and pain in efforts to reduce the impaired functionality of women in later years. Weakening pain and BMI trajectories and their association may improve women’s later-life functionality and general quality of life at both the individual and population levels.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is currently supported by a grant from the National Institute on Aging (AG043599, Kandauda A. S. Wickrama, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies. Support for earlier years of the study also came from multiple sources, including the National Institute of Mental Health (MH00567, MH19734, MH43270, MH59355, MH62989, MH48165, MH051361), the National Institute on Drug Abuse (DA05347), the National Institute of Child Health and Human Development (HD027724, HD051746, HD047573, HD064687), the Bureau of Maternal and Child Health (MCJ-109572), and the MacArthur Foundation Research Network on Successful Adolescent Development Among Youth in High-Risk Settings.
IRB Approval
University of Georgia Institutional review board (STUDY 00001438).
Data availability
Data cannot be shared publicly because of confidential nature of respondents’ information. Data are available from the Principal Investigator of Later Adulthood Study, Kandauda Wickrama (