
Abstract
Objectives:
There is little nationally representative information about factors associated with longevity among older Brazilians.
Methods:
Baseline survey data from the Brazilian longitudinal Study of Aging (ELSI-Brazil) were linked to vital statistics systems. Mortality rates and life expectancy estimates were calculated and compared to official sources. Cox Proportional Hazards models and Population Attributable Fractions (PAFs) identified significant predictors of mortality.
Keywords
Introduction
There is considerable evidence that biological, economic, environmental, and social factors are associated with mortality among aging cohorts (Liao et al., 2018; Puterman et al., 2020). But the bulk of this evidence has come primarily from higher-income settings. In most low- and middle-income countries, the study of mortality continues to rely on vital statistics that, although essential, do not provide sufficient information to assess underlying sociodemographic and health-related factors linked with the risk of morbidity, disability, or mortality (National Academies of Sciences & Medicine, 2018). The accelerated aging of populations in middle income countries has led to the development of a series of cohort studies of ageing (many of which are patterned after the US Health and Retirement Study) in countries such as Brazil, China, India, Indonesia, Mexico, and South Africa. These studies provide an important opportunity to better understand the mechanisms and consequences of risk factors over the life course and to assess whether the same factors associated with mortality and longevity that have been identified in higher income setting apply to these middle-income country contexts (Lee et al., 2021).
Understanding determinants of the aging process is essential for guiding investments in improving health and the policy environment. This is particularly relevant in Brazil, which has the world’s sixth largest population (over 212 million) with 17.8 million adults (8.5%) aged 65 and over. In 2020, life expectancy was estimated at 76 years, placing it squarely within the median for the Latin America and the Caribbean region. While the socio-economic context of the country continues to fluctuate, its nominal GDP (1.87 trillion) has been ranked within the top 10 globally for several years. Hallmark features of Brazil’s social and economic contexts include its high level of income inequality (Gini 48.9 in 2020, making it the 16th highest in terms of income inequality). Brazil is also known as a leader in innovative social policies, including a universal health system, a large conditional cash transfer program, and a national pension program, among others. These investments have already made changes to population health outcomes (Hone et al., 2017, 2019), although their cumulative impact on older adults has yet to be fully understood.
In recent decades, Brazil has also made improvements in enhancing the completeness and quality of vital statistics and other data systems (Marinho et al., 2019). But such systems still have limitations with respect to age reporting, documentation of education, and other socioeconomic variables on death certificates (Júnior et al., 2021), accurate identification of specific causes of death, and subnational variations in completeness and quality (Marinho et al., 2019; Teixeira et al., 2019; Turra et al., 2016). Even with improvements in the quality of vital statistics, there would still be gaps in understanding the aging process in Brazil because many relevant risk factors are not routinely collected in this data system (e.g., biological, socioeconomic, and social factors).
In this study, we aim to begin to fill these gaps in knowledge by assessing rates and predictors of all-cause mortality derived from the Brazilian Longitudinal Study of Aging (ELSI-Brazil), a nationally representative population-based cohort study of Brazilian adults aged 50 years and older.
Methods
This study uses data from the first wave of the ELSI-Brazil survey. The ELSI-Brazil sampling plan combined stratification of primary sampling units (municipalities), census tracts, and households. The baseline sample comprised 10,000 older adults (9412 participated), residing in 70 municipalities from all five Brazilian geographic regions. Details of the ELSI study (See http://elsi.cpqrr.fiocruz.br) have been described elsewhere (Lima-Costa et al., 2022).
The period under examination extends from the participant’s completion of the ELSI-Brazil baseline interview (May 2015 to October 2016) to completion of the second wave (July 2019 to March 2021). The flow diagram (See Online Appendix Figure 1) shows the construction of the analytic sample. Of the 9412 baseline participants, 6172 (65.6%) were retained for the second wave, 2533 were lost to follow-up and 707 had died (with a date of death informed by proxy). Using a probabilistic linkage method that included the participant’s name, sex, birth date, municipality of residence, and their mother’s name, information on those who died and those lost to follow-up was linked to the Brazilian Mortality Information System (SIM). The linkage algorithm identified that 263 (10.4%) of those lost to follow had died and among the 707 deaths reported by proxy, 609 (89.9%) were confirmed with a specific cause of death identified through this linkage. The number of baseline participants who died therefore totaled 970 (707 + 263).
Selection of variables for descriptive statistics and multivariable models was guided by the domains present in the WHO framework for Healthy Aging (Lloyd-Sherlock et al., 2019; World Health Organisation, 2017). These domains include the following: demographic factors (age, sex, self-reported skin color), socioeconomic status (years of formal schooling; per capita household income, home ownership, and occupational classification). Health status measures included fair/poor self-rated health, measured Body Mass Index (in categories), cognitive health (late memory word recall), and chronic conditions (self-reported prior medical diagnosis of cardiovascular disease—heart attack, angina or congestive heart failure, diabetes, stroke, cancer, depression, and measured hypertension (>140/90). Functional ability includes Activities of Daily Living (ADL) limitations, Instrumental Activities of Daily Living (IADL) limitations, and measured grip strength (average of two highest values) (de Souza Moreira et al., 2022). We also assessed behavioral factors (current or ever smoker vs. never), social support (partnered vs. single), and the physical environment (geographic region, and urban vs. rural residence).
Descriptive statistics comparing those who survived to those who did not were calculated as survey weighted proportions and means. Differences between groups are tested using Chi-Squared tests with a Rao–Scott correction for proportions and t-tests for differences between means. A multinomial logistic model was used to test differences between characteristics of those who were lost to follow-up with respect to those who died and those who were retained.
Demographic analyses include calculation of death rates by age and sex and making comparisons to official statistics as published by WHO in 5 year age groups (World Health Organization, 2022). We additionally calculate life expectancy estimates at each age (ex) and compare results with official data from the Brazilian Institute of Geography and Statistics (IBGE) available in 1 year age groups (Brazilian Institute of Geography and Statistics, 2022). Life expectancy calculations rely on the assumptions that those who died did so on average half-way between consecutive ages (Preston et al., 2001). The life table is based on standard assumptions that the death rate is constant after age 80 and that there were no person-years lived above age 100 in the population.
To understand the role of different factors on mortality, we employ Cox proportional hazards regression models. Because some variables were missing (up to 5% for some measured variables), we implemented multiple imputation via chained equations to create 20 datasets, then used Stata’s “svy” and “mi” commands to perform the survey-adjusted cox regression model drawing from the imputed datasets (StataCorp., 2021). The use of multiple imputation precludes the use of standard goodness of fit test measures (such as AIC/BIC or likelihood ratio tests), so variables introduced in the nested multivariable models were those that presented statistically significant differences among those who died and those who did not, as identified through descriptive (bivariate) analyses.
Finally, we calculate the Population Attributable Fractions (PAFs) for variables found to be statistically significantly associated with mortality in the Cox proportional hazards models. The PAF combines both the strength of the association of the risk factor with mortality as well as the prevalence of the risk factor in the population to derive an estimate of the impact on mortality if that risk factor were to be eliminated (Mansournia & Altman, 2018).
The ELSI-Brazil study was approved by the Committee on Research Ethics of the Fundação Oswaldo Cruz, Minas Gerais (CAAE: 34649814.3.0000.509).
Results
Characteristics of Those Who Died With Those Who Survived.
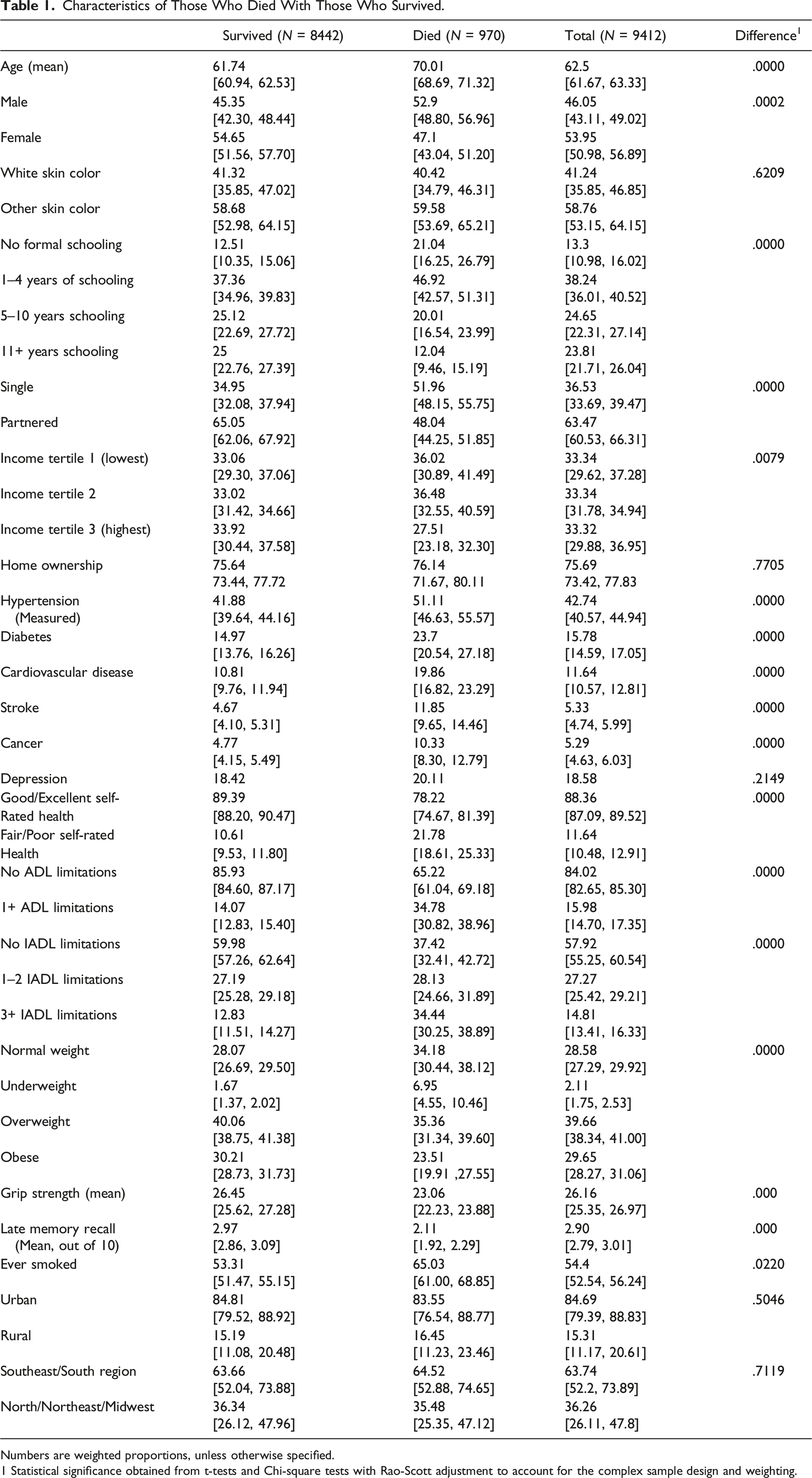
Numbers are weighted proportions, unless otherwise specified.
1 Statistical significance obtained from t-tests and Chi-square tests with Rao-Scott adjustment to account for the complex sample design and weighting.
The Online Appendix Tables 1 and 2 focus on characteristics of those lost to follow-up. It shows that, as compared to either those who died or those who were retained, those lost to follow-up were less likely to be in the older age groups, more likely to be single, less likely to own a home, more likely to have competed Middle or High School, and more likely to reside in the South or Southeast regions of the country, than those who were retained. In the fully adjusted multinomial logistic regression model (Online Appendix table 2), there was no statistically significant difference between those retained and those lost to follow up in terms of any health status indicator.
Comparison of Death Rates by Age, Sex, Data Source, and Year.
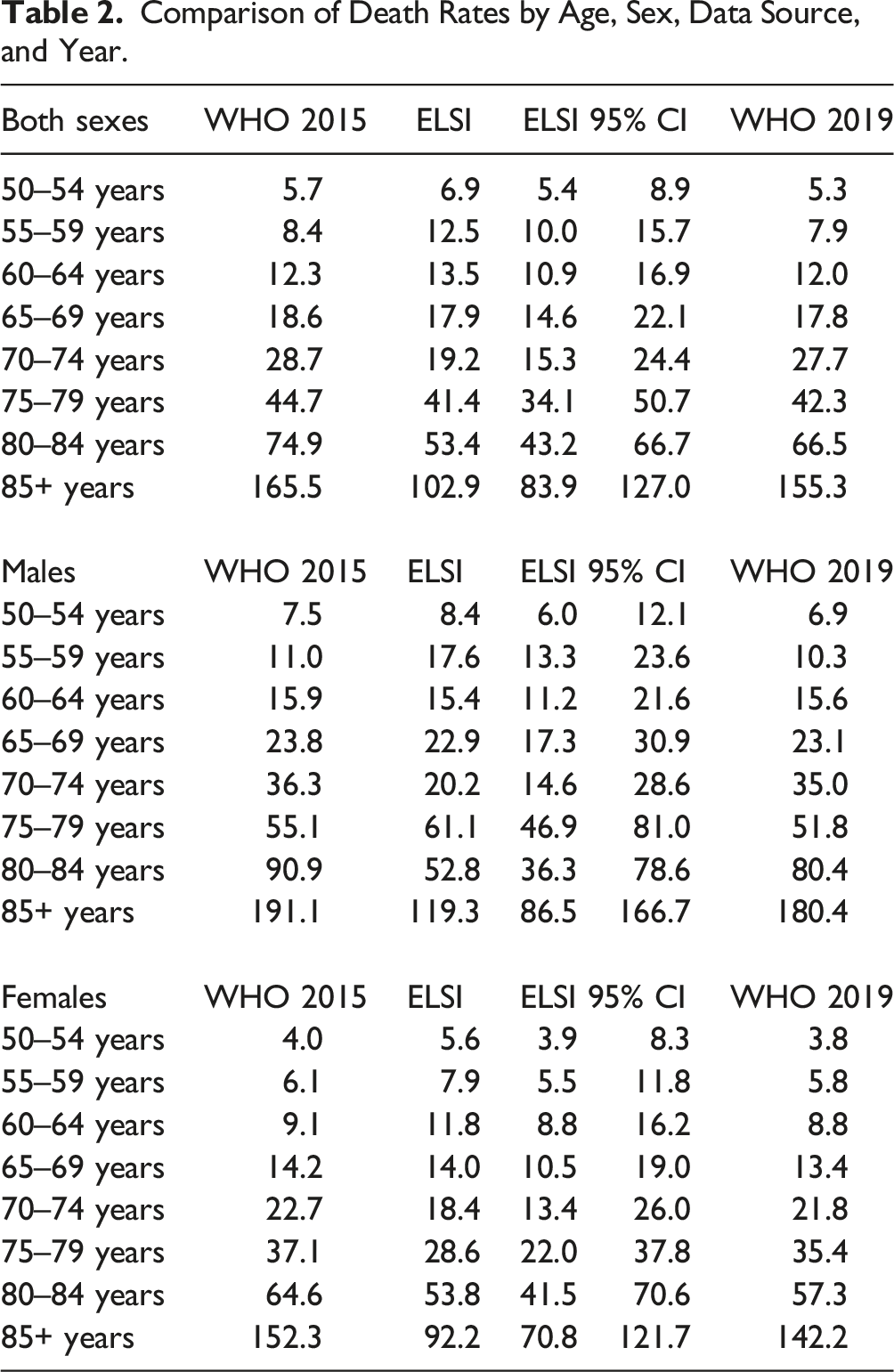
To assess mortality at a finer level of detail, Online Appendix Figure 2 plots single-years of age-specific death rate estimates from ELSI along with their 95% confidence intervals against values from the IBGE at the beginning (2015), middle (2018), and end (2020) of the period. For both men and women and for nearly every age, the IBGE estimates lie within the ELSI confidence intervals. The notable exception is among those aged 80+ where the ELSI estimates were significantly lower than official figures.
When comparing life expectancy at each age (ex), for most ages, the ELSI estimate lies between the 2015 and 2020 IBGE estimates, except for slightly lower estimates in younger ages (50–55) and older (75–80+ years) as can be seen in Figure 1 and Online Appendix table 3. Comparison of life expectancy at age x (ex) for both sexes combined, by data source.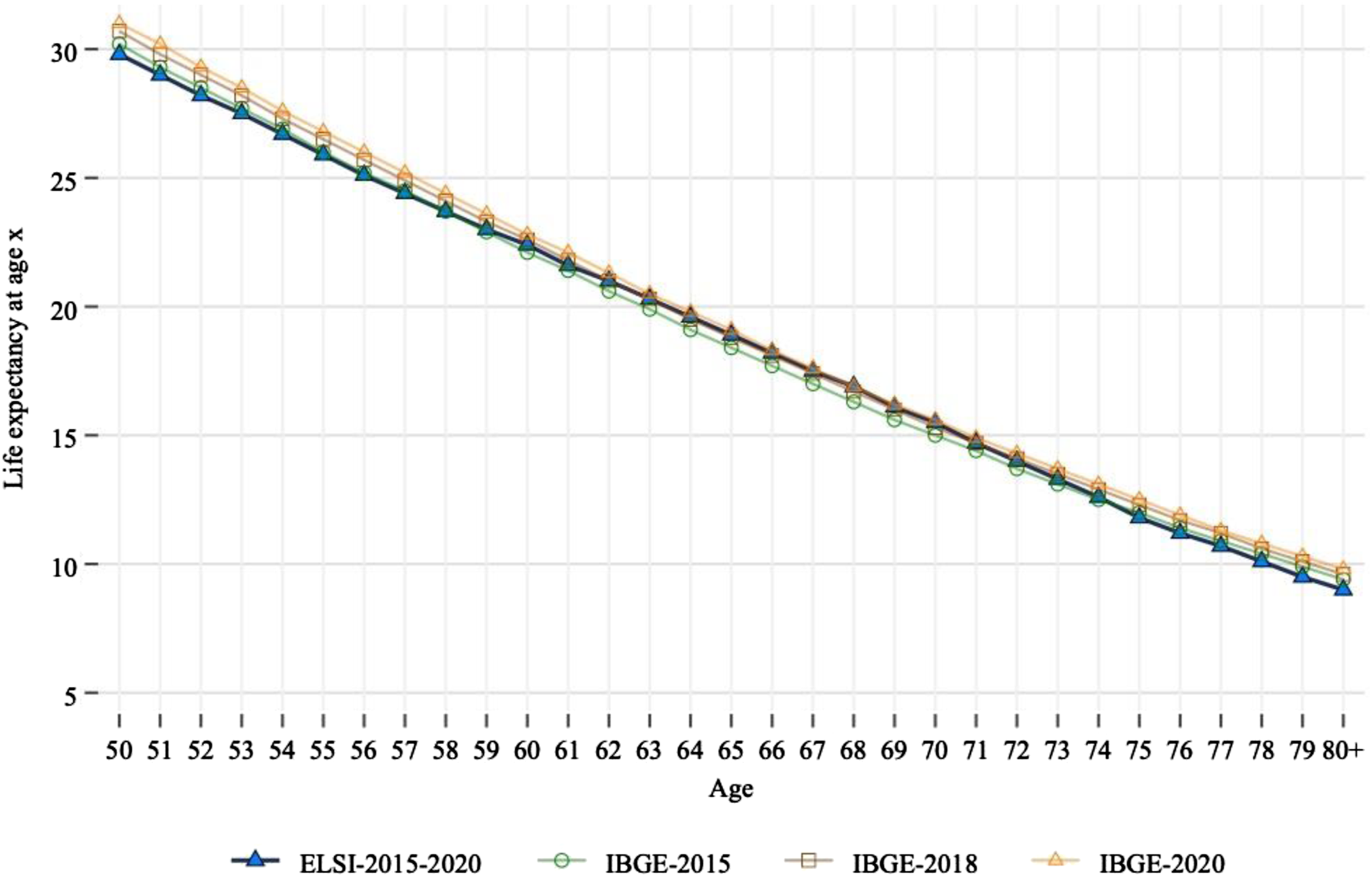
Results From Cox Proportional Hazards Models.
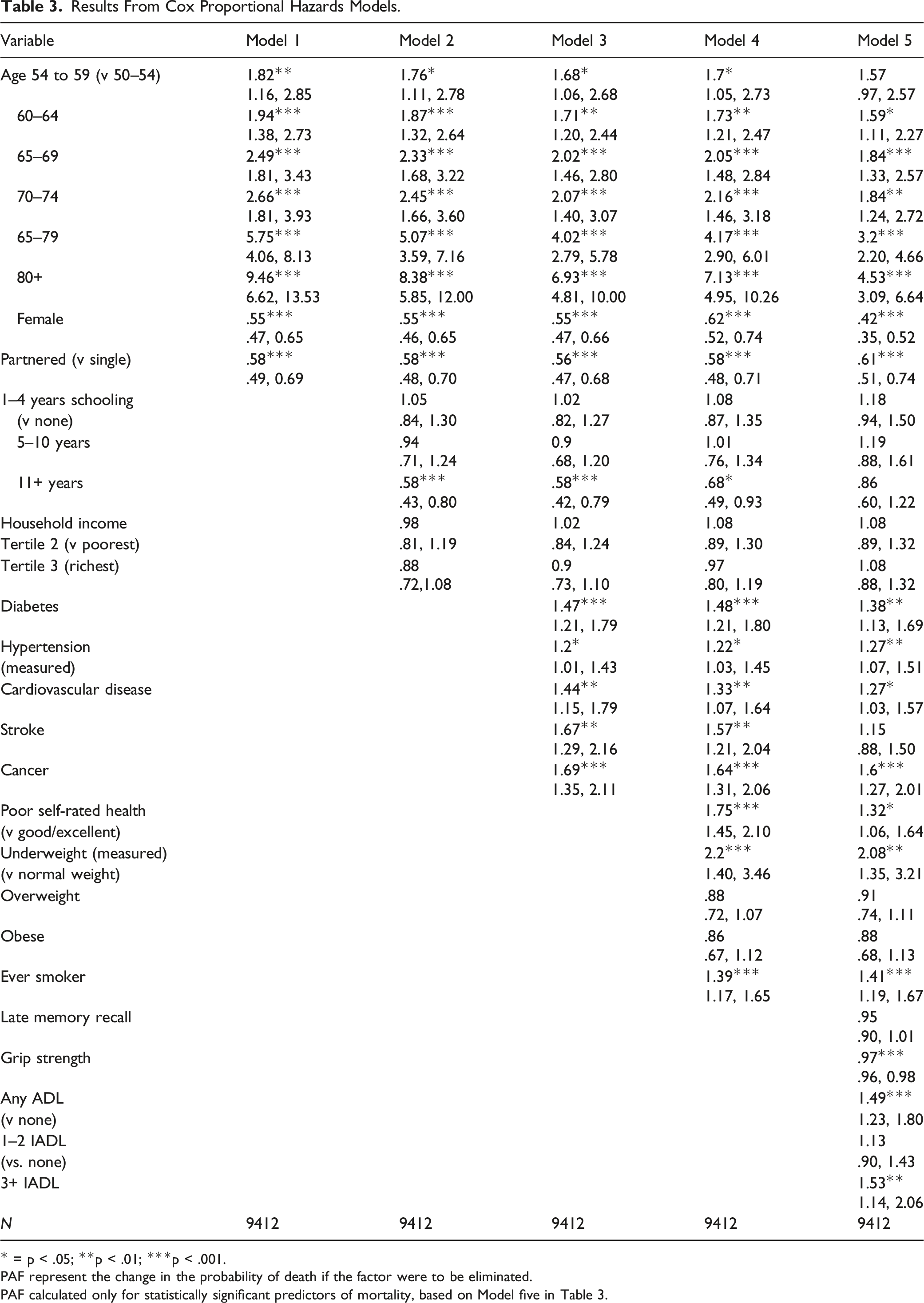
* = p < .05; **p < .01; ***p < .001.
PAF represent the change in the probability of death if the factor were to be eliminated.
PAF calculated only for statistically significant predictors of mortality, based on Model five in Table 3.
Figure 2 presents PAF estimates for those variables found to be statistically significant predictors of mortality in the Cox proportional hazards models (Model 5 in Table 3). These measures represent the change in the probability of death if the factor were to be eliminated, thus combining the relative risk of death but also the prevalence of the condition within the population. Two factors (11 or more years of schooling and being partnered vs. being single) both had positive PAFs, meaning that if they were to be eliminated, then mortality would increase in the population. In contrast, the largest population attributable fraction leading to lower mortality would come from, in descending order of magnitude, elimination of underweight, cancer, diabetes, 3+ IADL limitations, fair poor self-rated health, cardiovascular disease, low grip strength, any ADL limitation, hypertension, and smoking. Population Attributable Fraction (PAF) estimates and 95% confidence intervals.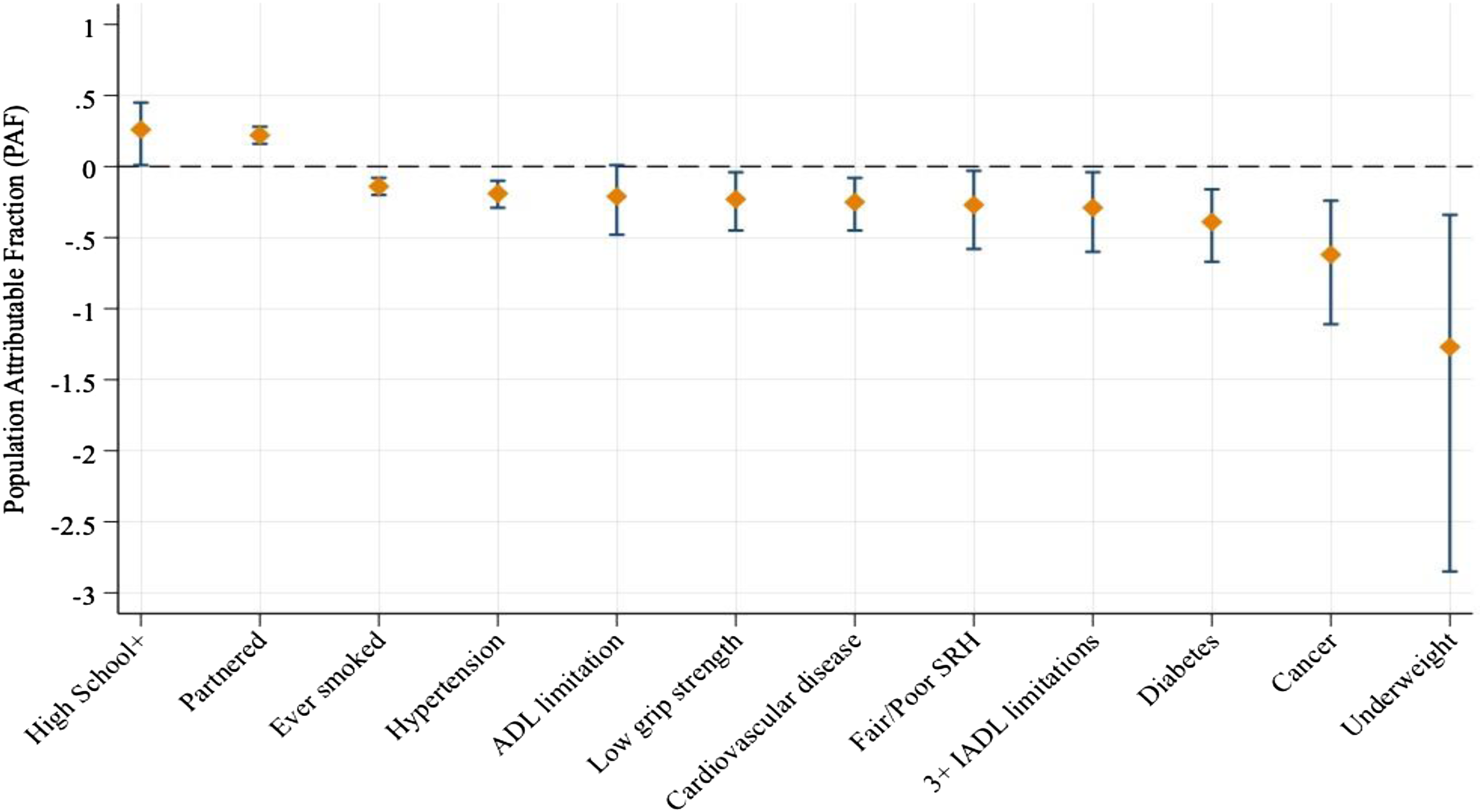
Discussion
In this study, we demonstrate that ELSI-Brazil can be used to provide measures of mortality and life expectancy for older Brazilians. These estimates largely coincide with official statistics, with the important exception of underestimating mortality among the oldest age groups (80 and above) and slightly overestimating mortality among the youngest age groups. These differences do not appear to be driven by characteristics of those lost to follow-up and may instead be a function of the difficulty of recruiting older, sicker adults into the survey. Importantly, estimates of life expectancy by age were close to official estimates for both sexes.
Specific factors associated with mortality largely align with the literature. As expected, women tend to have lower mortality risk, with an overall higher life expectancy at every age as compared to men. Higher educational attainment was negatively associated with mortality and showed a PAF of .28, suggesting it is an important determinant of longevity. This is consistent with previous analyses that have quantified the importance of educational attainment for mobility (Nascimento et al., 2018) and changes in life expectancy, especially for Brazilian women (Turra et al., 2016). Interestingly, there was no evidence of a mortality gradient by educational attainment, perhaps because there is a low average level of education especially among older members of the cohort—half the sample had 4 years or less years of formal schooling, as previously reported (Andrade & Lopez-Ortega, 2017). While there has been evidence of a more pronounced SES gradient for self-rated health and ADL limitations among older Brazilians (Lima-Costa et al., 2012), to date, there have not been sufficient data to assess the individual-level relationship between mortality and educational attainment in a nationally representative sample of older adults.
Chronic conditions and other risk factors were also largely consistent with the literature, such as those based on data from the Study of Aging and Health (SABE) (Bernardes et al., 2021). Measured hypertension, poor self-rated health, and previous medical diagnoses of cardiovascular disease, stroke, and cancer were all predictive of greater mortality risk, similar to results found in a study of mortality risk among older adults in four countries (Costa Rica, England, US, Taiwan) (Goldman et al., 2016). A study using another Brazilian aging cohort based in a small town (Bambuí) compares results with those obtained from the English Longitudinal Study of Aging (ELSA) and found that hypertension and diabetes were strongly associated with 6 year mortality, with smoking identified as an important contributing factor (de Oliveira et al., 2016). Given the higher prevalence and greater mortality risk among Brazilians (as compared to British older adults), the authors found that such factors had a greater contribution to population attributable risks in Brazil than in England. Another study compared older adults who participated in a different Brazilian cohort, Siga-Bagé (based in Southern Brazil) and ELSA. Kessler et al (2020) confirmed that mortality risk was generally higher among Brazilian as compared with English older adults and identified smoking as an important modifiable risk factor. Unlike this study, Kessler et al did not find that hypertension or diabetes were statistically significantly related to mortality risk. They did, however, find that obesity was not associated with mortality, but did not assess underweight (Kessler et al., 2020). This study found underweight to be one of the strongest predictors of mortality at older ages. This is perhaps due to its relationship with frailty, which has been found to be associated with increased mortality risk among older Brazilians in the SABE study (Fhon et al., 2018).
This study has several strengths. It relies on nationally representative cohort data with rich information on demographic, health status, financial, and social domains that allowed us to investigate relationships with mortality hitherto unexplored in a national sample. Moreover, comparison of mortality and life expectancy estimates to official sources helps to establish the study results’ generalizability.
Study limitations include the fact that a number of questions are based on self-report and we cannot rule out the risk of recall bias that may have affected respondents’ ability to recall certain facts. Moreover, approximately 2% of responses were supplied via a proxy respondent, usually the respondent’s spouse or caretaker. Our sample is made up of community-dwelling older adults and excludes highly vulnerable and sick individuals including those residing in hospitals or other institutional settings. Sampling weights have been calculated to make estimates from ELSI data nationally representative based on demographic and geographic characteristics, but not in regards to the health status of the participants. The lack of participation of older, much sicker adults in the study, a limitation of many aging cohort studies, may explain why our estimates for mortality at the oldest ages were lower than official estimates.
Finally, the COVID-19 pandemic may have affected our results. Recent work estimated a .9 year reduction of life expectancy at age 65 between 2019 and 2020 due to the pandemic (Castro et al., 2021). Other work indicates that COVID had not only a direct impact on mortality in Brazil but also had an indirect effect through other causes of death (Fernandes et al., 2023). For example, mortality related to childhood (e.g., pregnancy and childbirth and puerperium) and adulthood (e.g., diabetes and hypertension) increased while death from some conditions with high prevalence among older adults such as malignant neoplasm, heart and stroke, and pneumonia actually declined (Fernandes et al., 2023). As noted above, the lack of participation of older and much sicker respondents in ELSI, combined with the indirect effect of COVID in reducing mortality risk from some major causes of death among older adults may have contributed to lower number of deaths in our study and a consequent underestimation of death rates at older ages. In this study, we do not analyze the specific contribution of COVID-19, although there were 42 deaths confirmed due to COVID-19 (ICD-10 B34.2) among those whose records were successfully linked. This represents 4.3% of all deaths. Given that the IBGE mortality and life expectancy estimates were projections based on pre-COVID-19 data and that older age is associated with COVID-19 mortality, our estimates of death at the oldest ages may indeed be undercounted.
In conclusion, this study demonstrated the value of ELSI as it allows for the assessment of mortality risk by factors that are not typically collected in other data systems such as vital statistics. The study adds value due to its being the only existing nationally representative aging cohort in the country. ELSI-Brazil therefore provides an opportunity to understand better the contribution of factors such as educational attainment, the household economic situation, health behaviors, and a range of health conditions—separately and in combination, on mortality, longevity, disability, and inequalities in each of these outcomes for a nationally representative sample of older adults. Future research can further advance the state-of-the-art by incorporating ELSI’s mortality data (including specific causes of death) with measures of physical functioning, cognitive performance, metabolic and other biomarkers, and genomic analyses (Lima-Costa et al., 2022). The study’s ultimate objective is to harness such research for promoting healthy aging among older Brazilians and to inform the overall provision and continuous quality improvement of health and social services essential to reaching this goal.
Supplemental Material
Supplemental Material - Socioeconomic, Disease Burden, Physical Functioning, Psychosocial, and Environmental Factors Associated With Mortality Among Older Adults: The Brazilian Longitudinal Study of Ageing (ELSI-Brazil)
Supplemental Material for Socioeconomic, Disease Burden, Physical Functioning, Psychosocial, and Environmental Factors Associated With Mortality Among Older Adults: The Brazilian Longitudinal Study of Ageing (ELSI-Brazil) James Macinko, Hiram Beltrán-Sánchez, Juliana Vaz de Melo Mambrini, and Maria Fernanda Lima-Costa in Journal of Aging and Health.
Footnotes
Acknowledgements
We thank the team from the Health Surveillance Secretariat (Secretaria de Vigilância em Saúde, in Portuguese) at the Brazilian Ministry of Health for performing linkage of the ELSI-Brazil data with vital statistics data (the National Mortality Information System, SIM).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first and second waves of ELSI-Brazil were supported by the Brazilian Ministry of Health (DECIT/SCTIE – Department of Science and Technology from the Secretariat of Science, Technology and Strategic Inputs [Grants: 404965/2012-1 and TED 28/2017]; and COSAPI/DAPES/SAS – Healthcare Coordination of Older Adults, Department of Strategic and Programmatic Actions from the Secretariat of Health Care [Grants: 20836, 22566, 23700, 25560, 25552, and 27510]. The funding sources had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication
Data availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.