
Abstract
Objectives
Assess the influence of physical function on balance and future falls in older adults with fear of falling (FOF) and whether activity restriction modifies the contribution to falls.
Introduction
Fear of falling (FOF), a heightened concern of falling during activities of daily living, affects approximately 38% of older adults and leads to an increased risk of future falls (Scheffer et al., 2008). In the general older adult community, falls are the leading cause of fatal injury (Burns & Kakara, 2018) and the most common cause of nonfatal trauma-related hospital admissions (“Web-Based Injury Statistics: Query and Reporting System (WISQARS). Atlanta, GA: Centers for Disease Control and Prevention, 2016.,” n.d.). Numerous fall risk factors have been examined in the general older adult community (Ambrose et al., 2013) resulting in interventions shown to reduce falls. Specific recommendations include the use of exercise to target physical function (e.g., strength, flexibility, proprioception) and multifactorial interventions which target an array of potential fall risk sources often in addition to physical function (e.g., environment, medications, psychological health) depending on individual patient needs (Guirguis-Blake et al., 2018). While these approaches are successful in the general adult community, it is not known whether utilization of exercise or multifactorial interventions are appropriate to reduce falls in older adults with a FOF given there is a limited understanding of how FOF increases fall risk.
We previously confirmed that reduced balance performance in older adults with a FOF is at least one source of increased risk of future falls (Garbin & Fisher, 2021). Importantly, this suggests that interventions aiming to improve balance are appropriate to reduce falls in this population. However, it is unclear whether balance training interventions should primarily emphasize physical function (e.g., strength, proprioception, pain) (Daubney & Culham, 1999; Hirase et al., 2020; Muehlbauer et al., 2015; Speers et al., 2002) or employ a multifactorial approach that also targets other potential sources of reduced balance performance (e.g., anxiety, depression, fear) (Brown et al., 2006; Deschamps et al., 2015; Huffman et al., 2009). Understanding the degree to which physical function is responsible for reduced balance experienced by older adults with a FOF, will inform existing interventions and advance future interventions to improve balance and, in turn, reduce falls in this population.
To date, there have been a small number of fall prevention intervention studies in older adults with a FOF that are exercise-based (Freiberger, Häberle, Spirduso, & Rixt Zijlstra, 2012; Haines et al., 2009), attempting to modify physical function characteristics, or multifactorial (Clemson et al., 2004; Zijlstra et al., 2013), focusing on various potential fall risk sources in addition to physical function. In comparing these intervention studies, those utilizing a multifactorial approach have had greater success at significantly reducing falls in older adults with a FOF relative to the studies that focus on exercise. However, it cannot yet be stated that the differing success of these intervention approaches is due to the approach taken given the myriad of factors that can also impact the success of an intervention study (e.g., sample size (Gates & Ealing, 2019), dose (Sherrington et al., 2017)). As such, it is necessary to step back and examine which fall prevention intervention approach is optimal (exercise vs. multifactorial) by elucidating the contribution of physical function on reduced balance and increased future fall likelihood experienced by older adults with a FOF and the degree to which balance and fall likelihood exists independent of physical function.
Heterogeneity within older adults with a FOF may also contribute to the varying success of different intervention studies that have attempted to reduce falls in this population. For example, within a group of older adults with a FOF some individuals may restrict their activity (e.g., participating in fewer activities outside of the home) while others do not. This activity restriction is associated with loss in physical function (Delbaere et al., 2004; Deshpande et al., 2008), suggesting that exercise interventions may be more effective for older adults with a FOF who restrict their activity than for those who do not restrict their activity. However, it is necessary to determine whether presence/absence of activity restriction modifies the degree to which physical function contributes to future fall likelihood. In this way, interventions can be optimized to reduce falls in these two types of FOF.
It is unclear how much physical function contributes to balance performance and future fall risk in older adults with a FOF and whether balance and future fall risk persists regardless of physical function. In fact, given that there is a psychological basis of FOF (Van Haastregt et al., 2008; Young & Mark Williams, 2015), some may view only physical function contributing to reduced balance and increased falls in this population as counterintuitive. Therefore, this study aimed to examine the extent to which physical function influences (1) reduced balance performance and (2) increased future fall likelihood in older adults with a FOF and (3) determine whether heterogeneity within FOF, based on presence or absence of activity restriction, modifies the impact of physical function. Accomplishing these aims will support advancement of targeted and effective intervention studies for older adults with a FOF. Specifically, this work will clarify whether interventions should prioritize exercise or a multifactorial approach. We hypothesized that reduced balance performance and increased future fall likelihood experienced by older adults with a FOF would both be influenced by physical function and exist independent of physical function (Figure 1) given the greater relative success of prior multifactorial interventions. Upon stratification based on activity restriction, we hypothesized that physical function would influence fall likelihood in older adults with activity restricting FOF more than those with non-activity restricting FOF. These analyses will be accomplished using two datasets, the Baltimore Longitudinal Study of Aging (BLSA) and National Health and Aging Trends Study (NHATS). Two datasets were used as they each offer unique advantages. Notably, BLSA contains more robust measurements to quantify balance performance while measures within NHATS allow for stratification of FOF based on activity restriction. Additionally, NHATS data is collected annually which facilitates analyses examining future fall likelihood. Model of the hypothesized sources of fall risk in older adults with a fear of falling. Solid lines indicate associations that have been established while dashed lines indicate associations that will be assessed in this study and the datasets utilized (BLSA = Baltimore Longitudinal Study of Aging; NHATS = National Health and Aging Trends Study).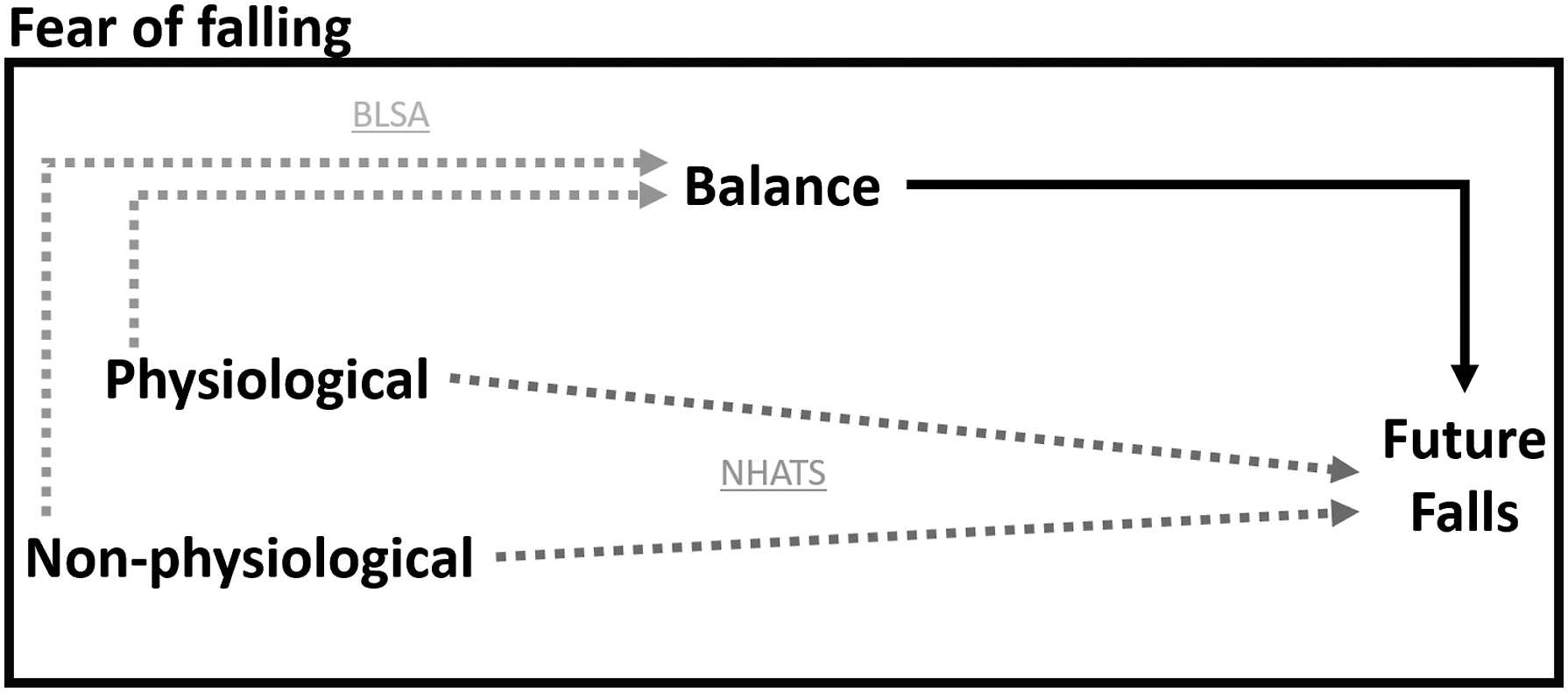
Methods
Data from BLSA were utilized to assess the influence of physical function on reduced balance performance in older adults with a FOF due to its physical function-related variables and its assessment for balance performance. FOF heterogeneity was not assessed with the BLSA dataset as its definition of FOF is already a subtype, specifically activity restricting FOF. Furthermore, sources of future fall risk were not assessed using this dataset given the inconsistent time to follow-up that exists for its longitudinal variables. As such, all BLSA data utilized in this study were cross-sectional. The NHATS dataset addresses each of the limitations in the BLSA dataset. Longitudinal data from NHATS occur in 1-year follow-ups. This facilitated analyses examining the sources of future fall likelihood without the large potential confound of inconsistent time to follow-up. The impact of heterogeneity within FOF was also assessed via the NHATS dataset as it first probes the presence of FOF and subsequently asks if this FOF resulted in activity restriction. Further information on these two datasets is provided below.
Baltimore Longitudinal Study of Aging Measurements
The BLSA is a National Institute of Aging sponsored prospective study focused on understanding healthy aging. This study began in 1958 and continuously enrolls adults aged 21 years or older. Every 2 years, participants undergo medical, physical, and psychological testing (Ferrucci, 2008). The BLSA database was selected for this study due to the high-quality physical function testing performed on participants. For this analysis, we screened data collected on 5772 observations from 2006 to March, 2020. We excluded 3829 observations due to missing data and further reduced the dataset by 461 observations to only include adults aged 65 years and older. Lastly, we removed any observations that were of the same participant on different data collection dates to ensure there were no duplicate participants across visits and that data were purely cross-sectional. This resulted in a final sample size of 680 participants (Supplemental Figure 1).
Balance performance was quantified via total seconds on the Health ABC Physical Performance Battery (HABCPPB) (Simonsick et al., 2001). The HABCPPB is a variant of the Short Physical Performance Battery Scale (SPPB) that augments the difficulty of the test by having participants perform a single limb stance task for 30 seconds in addition to the original standing tasks of semi-tandem and tandem for 30 seconds each. As aforementioned, within the BLSA dataset the only measure of FOF was for a specific subtype of activity restricting FOF. This activity restricting FOF was confirmed if a participant answered “yes” to the question of “In the past 12 months, did you limit your activities, for example, what you did or where you went because you were afraid of falling?” Variables related to physical function utilized from the BLSA dataset include: age, race, sex, body mass index, grip strength (via hand held dynamometer), knee stiffness in the past 12 months, foot pain, proprioception, knee extensor torque, and knee flexor torque. Lower extremity torque measurements were measured utilizing an isokinetic dynamometer (Biodex Multi-Joint System-PRO with Advantage Software V.4X, Biodex Medical Systems, Inc., Shirley, NY, USA) (Hartmann et al., 2009). Some of the physical function-related variables are non-modifiable (age, race, sex) and, consequently, are not targeted outcomes for interventions. However, these variables are still included within the analyses as they serve as proxies for differences in physical function that may otherwise not be captured. For example, a higher age may capture whole body strength deficits that could be attenuated via strengthening exercises.
National Health and Aging Trends Study Measurements
NHATS is a longitudinal cohort study that began in 2011 and includes annual collection of survey and functional test data on a nationally representative sample of Medicare beneficiaries (Montaquila et al., 2012). NHATS is sponsored by the National Institute of Aging (grant number NIA U01AG32947) and was conducted by Johns Hopkins University (Montaquila et al., 2012; “National Health and Aging Trends Study. Produced and distributed by www.nhats.org with funding from the National Institute on Aging (grant number NIA U01AG32947),” n.d.). Data collection procedures were approved by the John Hopkins University Institutional Review Board. For this study, data were utilized from Waves 1 and 2 of NHATS. The Wave 1 interview included 8245 older adults (from an initial selection of 12,411 individuals). At Wave 2, 1170 participants were not interviewed (T2; 12 months after T1) secondary to refusal, death, and general unavailability, thus reducing the cohort sample size to 7075 older adults. Participants were also excluded if they were not community-dwelling and if there were data missing for the presence of FOF, future falls, or any physical function-related variables. The exclusion of these participants resulted in a final sample size of 4376 participants (Supplemental Figure 2).
The presence of a future fall was assessed by asking at T2 (approximately 1 year after T1) the question “Since [Last interview month and year] have you fallen down?” A fall was defined as “…any fall, slip, or trip in which you lose your balance and land on the floor or ground or at a lower level.” The presence of FOF at T1 was reported if a participant answered “Yes” to the question of “In the last month, did you worry about falling down?” Subsequently, participants that answered “Yes” were identified as having activity restriction if they also answered “Yes” to the question of “In the last month, did this worry ever limit your activities?” Variables related to physical function from the NHATS dataset include: age, sex, race (White, Black, Hispanic, Other), self-reported pain, self-report of lower-extremity limited strength/movement, self-report of upper-extremity limited strength/movement, hand grip strength recorded via a hand grip dynamometer, and score on the NHATS Expanded SPPB section of chair stands (proxy for lower extremity power) and peak air flow (proxy for respiratory fitness). The Expanded SPPB chair stand and peak air tests were scored on a 0–4 scale with a lower score indicating worse performance.
Statistical Analysis
All analyses were performed utilizing R 3.6.0 statistical software (Team, 2019). Older adults were grouped based on the presence or absence of activity restricting FOF (BLSA) and presence or absence of FOF (NHATS). Within the NHATS database, individuals with a FOF were further stratified based on whether they reported their FOF restricted their activities. Summary statistics were performed on the groups (older adults without FOF, with FOF, with non-activity restricting FOF, and with activity restricting FOF) and are reported as percentages for categorical variables and means with standard deviations for continuous variables. Differences were subsequently assessed between groups within each dataset via t-test, Kruskal–Wallis, or Chi-square depending on normality and variable type. Differences were also assessed between analyzed participants and the participants removed due to missing data to determine whether removal of missing data resulted in a biased study sample.
Baltimore Longitudinal Study of Aging
The difference in balance performance in older adults with and without activity restricting FOF was assessed via a linear regression model before and after controlling for physical function. Specifically, a multiple linear regression model was created with balance ability as the response variable and presence/absence of activity restricting FOF as the main predictor. This created a regression equation of


National Health and Aging Trends Study
The effect of FOF on future fall likelihood was assessed using binary logistic regression with presence of T1 FOF as the predictor variable and report of a fall in the past year at T2 as the response variable. Determination of whether the presence of FOF increased the likelihood of future falls independent of physical function was made by subsequently creating a multiple binary logistic regression model that included the physical function-related variables within the NHATS database. The predictor variable of FOF was then stratified into activity restricting FOF and non-activity restricting FOF. The effect of each of these types of FOF on future fall likelihood was assessed before and after controlling for physical function-related variables. The primary outputs of interest for these models include odds ratios with 95% CIs.
Results
Baltimore Longitudinal Study of Aging
Summary Statistics for Older Adults With and Without a FOF Within the BLSA Dataset (n = 680).
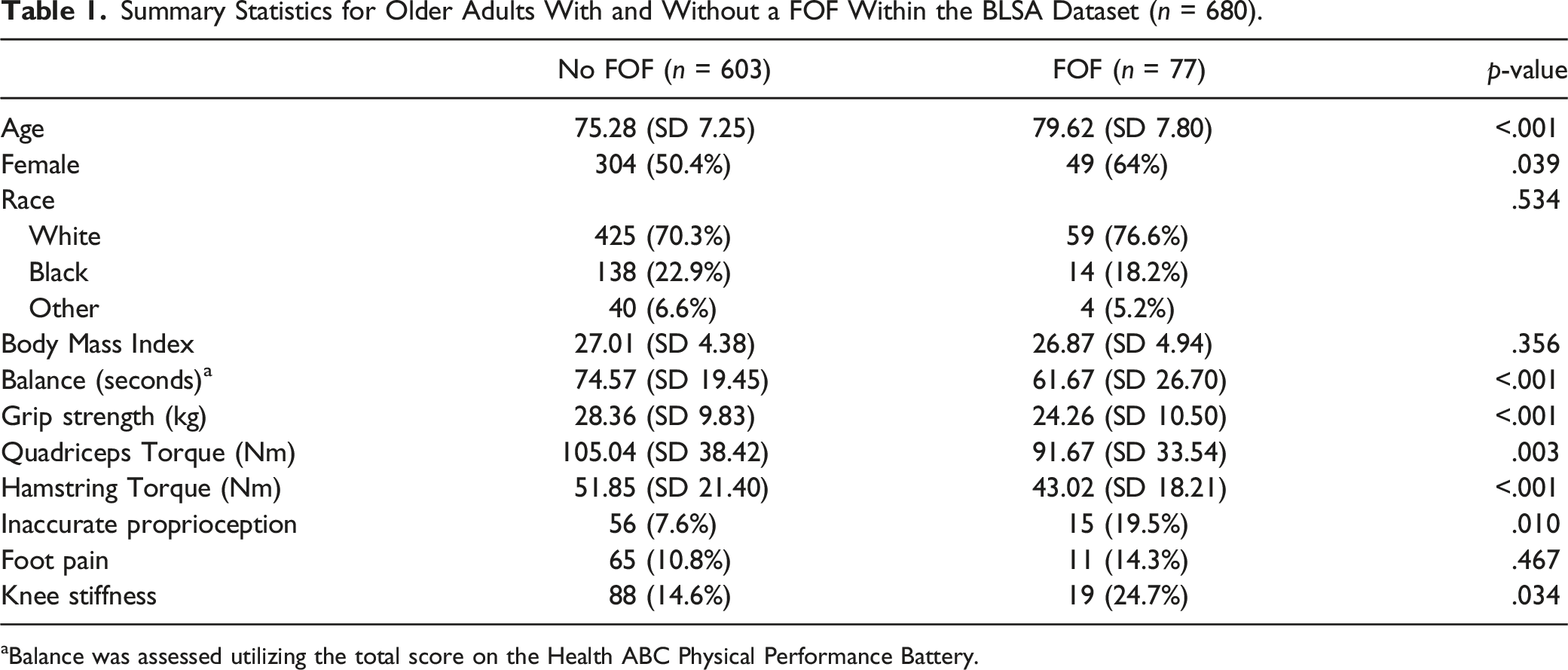
aBalance was assessed utilizing the total score on the Health ABC Physical Performance Battery.
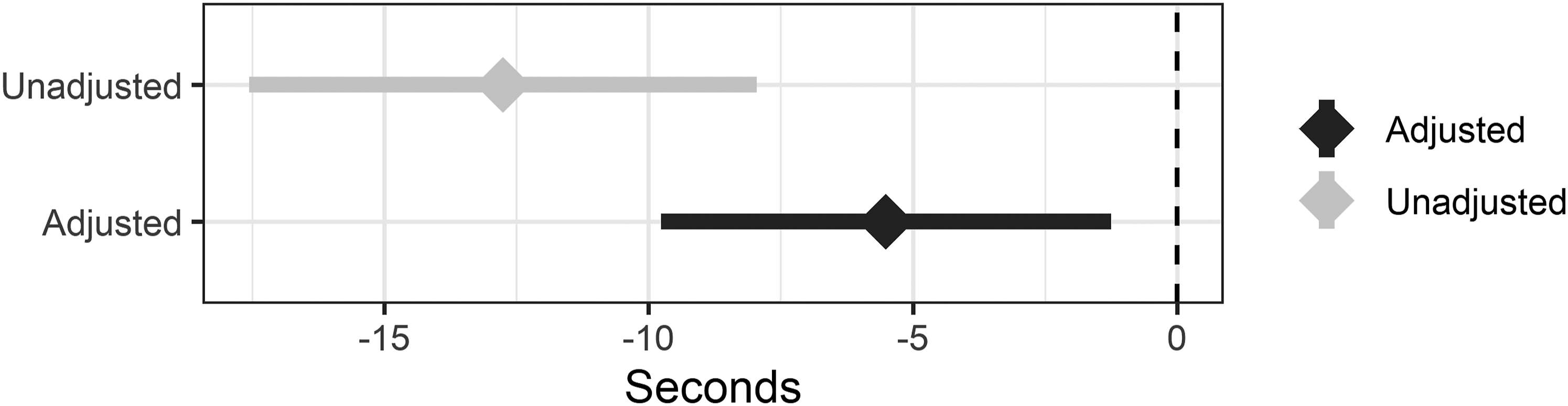
Difference in balance performance between groups. Negative scores reflect worse balance performance for older adults with a FOF. Diamonds and bars represent the difference between groups point estimates and confidence intervals, respectively. Unadjusted differences are represented as light gray while differences adjusted for physical function-related variables (age, race, sex, body mass index, grip strength, knee stiffness in the past 12 months, foot pain, accuracy of a proprioception test, knee extensor torque, and knee flexor torque) are represented as the dark gray.
Comparisons between the BLSA analyzed sample and missingness group are presented in Supplemental Table 1. Individuals removed from the BLSA dataset due to missing data were older and performed worse on tests of balance, grip strength, quadriceps strength, and hamstring strength.
National Health and Aging Trends Study
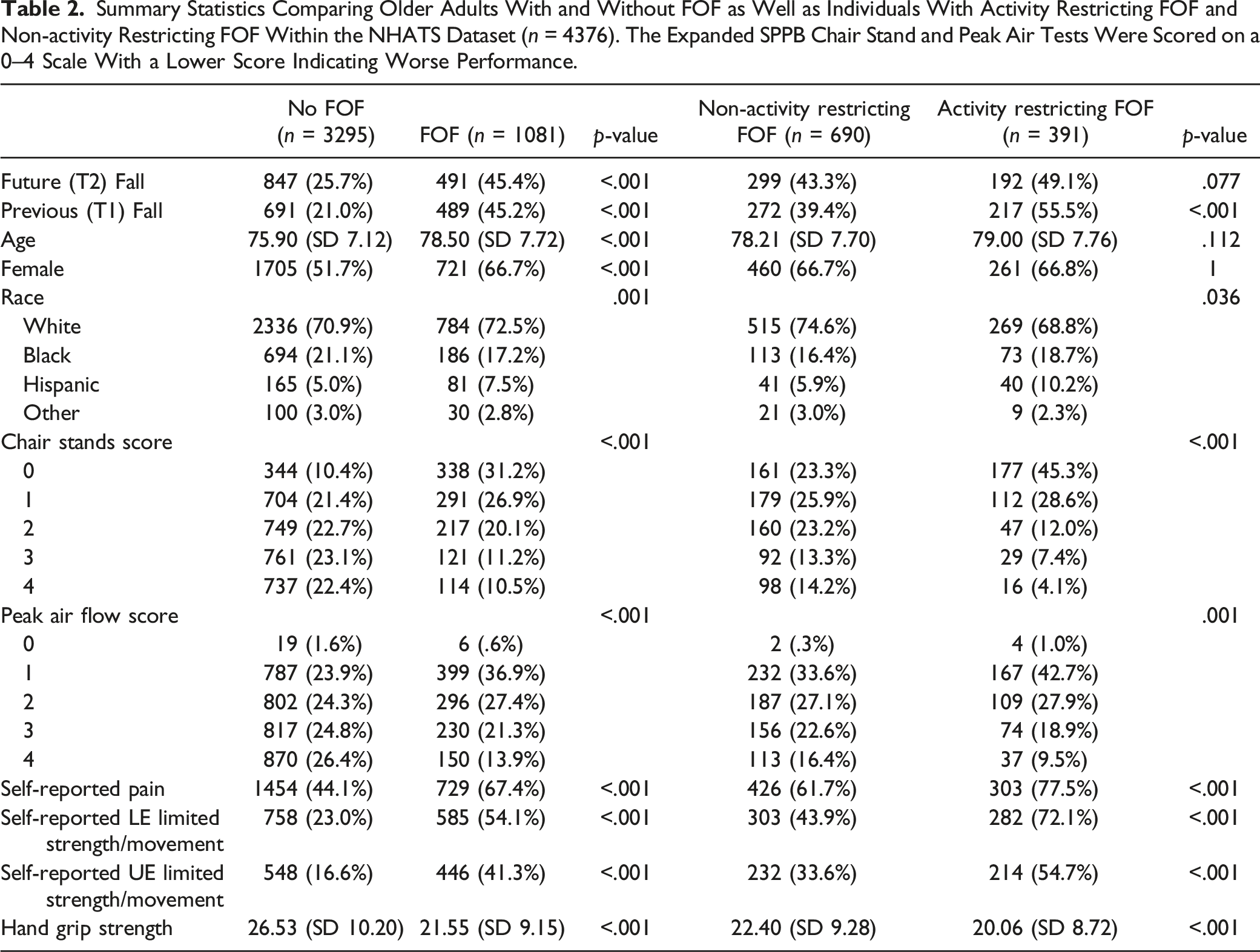
Summary Statistics Comparing Older Adults With and Without FOF as Well as Individuals With Activity Restricting FOF and Non-activity Restricting FOF Within the NHATS Dataset (n = 4376). The Expanded SPPB Chair Stand and Peak Air Tests Were Scored on a 0–4 Scale With a Lower Score Indicating Worse Performance.
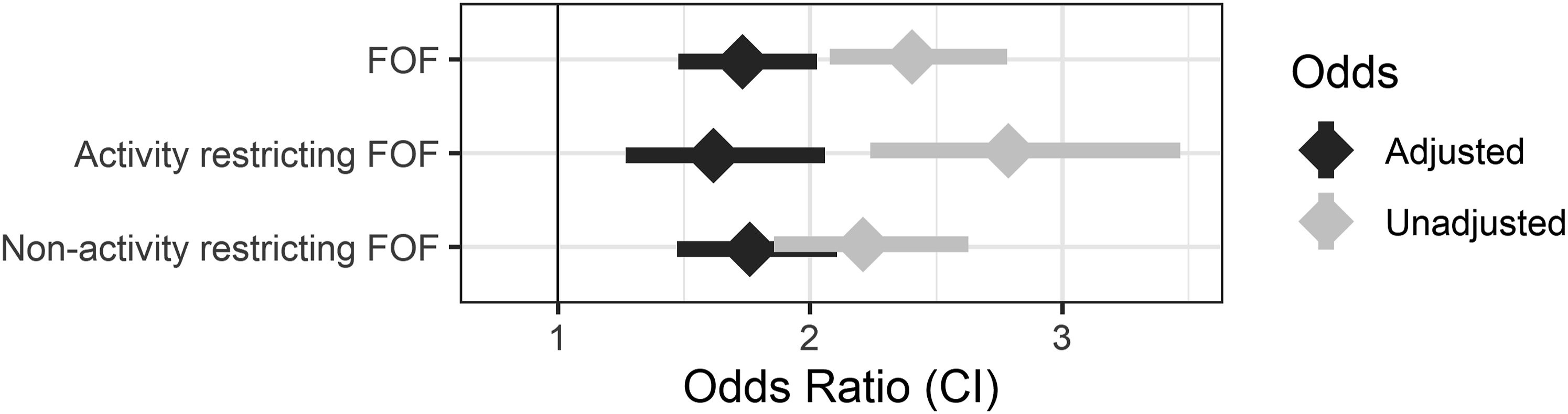
The effect of FOF, Activity restricting FOF, and Non-activity restricting FOF on future falls. Diamonds and bars represent the odds ratio point estimates and confidence intervals, respectively. Raw odds ratios are represented as light gray while odds ratios controlled for by physical function-related variables (age, sex, race, self-reported pain, self-report of lower-extremity limited strength/movement, self-report of upper-extremity limited strength/movement, hand grip strength recorded via a hand grip dynamometer, and score on the NHATS Expanded SPPB section of chair stands and peak air flow) are represented as the dark gray.
Comparisons between the NHATS analyzed sample and missingness group are presented in Supplemental Table 2. Individuals removed due to missing data in the NHATS dataset were significantly different in all measures in a direction indicating greater frailty.
Discussion
Older adults with a FOF continue to fall at an alarming rate (Scheffer et al., 2008). It is critical that we improve our understanding of how FOF increases fall likelihood to support the advancement of effective interventions that reduce falls in this population. As such, this study employed two large nationally representative datasets to understand whether reduced balance performance and increased falls experienced by older adults with a FOF are due, in part, to reduced physical function. This study also assessed how heterogeneity within a sample of older adults with a FOF modified the influence of FOF on future falls and the effect of controlling for physiologic variables.
Variables related to physical function were significantly different between groups in both the BLSA (no activity restricting FOF vs. activity restricting FOF) and NHATS (no FOF vs. FOF) datasets in a direction suggesting that each cohort of older adults with a FOF were at a greater fall risk due to their physical function. Within the BLSA database, older adults with a FOF performed worse on the balance performance test (HABCPPB) by a considerable margin. When controlling for physical function, the difference between groups was attenuated but remained significant suggesting that the balance decrement experienced by this sample of older adults with a FOF cannot solely be attributed to deficits in physical capacity. Given the BLSA dataset defines FOF as FOF with activity restriction, this result is unsurprising. Older adults with a FOF that report activity restriction typically experience greater physical frailty (Deshpande et al., 2008) and conceptual models have posited that this frailty is a source of their reduced balance performance and increased risk of falls (Delbaere et al., 2004). Furthermore, research has indicated that older adults with activity restricting FOF also experience decrements in other areas, such as psychosocial function (Murphy et al., 2015; Painter et al., 2012; Van Haastregt et al., 2008), which can influence balance performance (Brown et al., 2006; Deschamps et al., 2015; Huffman et al., 2009).
In the NHATS dataset, the presence of FOF resulted in greater odds of a future fall. When controlling for physical function, the effect of FOF on future fall likelihood persisted but was reduced. These findings indicate that both physical function and additional sources unrelated to physical function are responsible for the increased fall likelihood experienced by older adults with a FOF. Consequently, this work supports the use of multifactorial fall prevention approaches that include exercise to improve physical function and also target other potential fall risk sources. The likely presence of multifactorial sources of fall risk detailed in our study agrees with previous research detailing a higher rate of future falls in older adults with a FOF with and without elevated fall risk due to deficits in physical function (Delbaere, Close, Brodaty, et al., 2010). Further, older adults with a FOF have been shown to exhibit physical (e.g., strength, flexibility, proprioception) (Daubney & Culham, 1999; Hirase et al., 2020; Muehlbauer et al., 2015; Speers et al., 2002) and psychological (e.g., anxiety, worry, depression) (Brown et al., 2006; Deschamps et al., 2015; Huffman et al., 2009) deficits known to increase fall risk in the general older adult community.
Upon stratifying older adults with a FOF based on presence or absence of activity restriction, it was observed that there was a significant difference in all physiologic variables excluding sex and age. Notably, older adults with activity restricting FOF exhibited worse physical function. Interestingly, both activity restricting and non-activity restricting FOF greatly increased the odds of a future fall. The increased future fall odds in both groups despite the presence of activity restriction resulting in probable greater physical frailty suggests that physical function’s influence on future fall likelihood may differ based on the presence/absence of activity restriction. Evidence for this differential influence was seen as the effect of activity restricting FOF on future fall odds greatly reduced when controlling for physical function while only a slight reduction was observed for the effect of non-activity restricting FOF. Activity restricting and non-activity restricting FOF did share a similarity in that the effect of both types of FOF on future fall odds persisted while controlling for physical function, suggesting that both groups have sources that increased future fall likelihood unrelated to their physical capacity. These findings align with the conceptualized framework of the role of FOF in fall risk (Hadjistavropoulos et al., 2011). Specifically, this study’s findings support the concept that FOF increases future fall likelihood secondary to multifactorial causes and that activity avoidance in FOF can lead to physical deconditioning, thus increasing the impact of physical fall risk factors on future fall likelihood.
Together, Hadjistavropoulos’ conceptualized model of FOF and the results of this study support the use of both exercise and multifactorial approaches for future intervention studies targeting fall prevention in older adults with a FOF. While both approaches may be effective at reducing falls, there is stronger rationale for multifactorial interventions that include exercise as reduced physical function does not appear to be the only source impacting future fall likelihood in older adults with a FOF. However, the results of this study also illuminated the importance of identifying if an older adult with a FOF is restricting their activity as individuals not restricting their activity may experience greater benefit from interventions targeting sources influencing future fall likelihood independent of physical function. Future research is necessary to expand on the findings of this study and identify the precise sources related to physical function using clinical measures (e.g., muscle strength of specific muscles, range of motion) as well as those unrelated to physical function (e.g., anxiety, depression, environmental factors) that increase fall risk in older adults with FOF, with and without activity restriction. Identification of these sources will further support intervention studies and, in turn, lead to a reduction in falls in the large population of older adults with a FOF.
While the results of this study demonstrate that heightened future fall likelihood in older adults with a FOF is not solely due to reduced physical function and that presence/absence of activity restriction can influence physical function’s contribution to future fall likelihood, intervention studies utilizing this knowledge are a necessary step prior to recommending specific treatments be adopted in the clinical setting. However, there is still information within our findings that can help guide clinical care. For instance, it is important to identify whether patients have FOF and if they are restricting their activity. Specifically, presence of FOF may be a useful screening tool to identify individuals that are appropriate for fall prevention interventions given FOF greatly increases fall risk. Further, understanding whether an individual is restricting their activity can help inform clinicians on likely impairments that should be assessed. Detailed questionnaires are available to probe FOF (Falls Efficacy Scale-International (Delbaere, Close, Mikolaizak, et al., 2010)) and activity restriction (Survey of Activity and FOF in the Elderly (Lachman et al., 1998)). However, single questions of “Are you afraid of falling?” and “If yes, have you restricted any activity because of this fear?” are also a valid method to determine FOF and activity restriction (Belloni et al., 2020). That said, the reliance on these single item questions is a limitation within this study and future studies should aim to utilize detailed and continuous measures of FOF and activity restriction. In doing so, researchers can examine how varying degrees of FOF and activity restriction impact fall likelihood and other health outcomes.
The use of two datasets provided a clear picture and each facilitated specific analyses. For example, the NHATS database allowed analyses into longitudinal falls data and stratifying FOF based on presence/absence of activity restriction while the BLSA dataset provided more robust and objective measures related to physical function and a sensitive balance measure. Yet, the utilization of two datasets also introduced potential limitations including a reduced ability to draw a generalized combined conclusion between the balance and future fall results. The use of these datasets also introduced the limitation of missing data and, subsequently, the exclusion of participants with missing data. This exclusion resulted in samples with lower frailty compared to the groups with missing data. The greater frailty of the missing data groups is unsurprising given a large portion of the missingness was found in tests of physical function which many of the participants were not eligible for or did not perform secondary to safety concerns (Kasper et al., 2012). However, this difference reveals that the study results are less applicable to older adults with frailty exceeding the study sample. Another limitation of this study is the categorization of some variables as measures of physical function. It could be argued that a report of pain can reflect a participant’s body structure/function as well as their perception. Nevertheless, we believe it to be appropriate to err on the side of caution and consider these variables as physiological as it increases our confidence in stating that the reduced balance performance and increased future fall likelihood experienced by older adults with a FOF persists independent of physical function.
This study demonstrated that there are multifactorial sources, both related and unrelated to physical function, responsible for reduced balance performance and increased future fall likelihood experienced by older adults with a FOF. Further, it was revealed that heterogeneity, specifically the presence or absence of activity restriction, within FOF can modify the extent to which physical function impacts future fall likelihood. Together, these results support the use of multifactorial interventions that include exercise to optimally reduce falls in older adults with activity restricting FOF while fall prevention strategies for those not restricting their activity may have greater benefit targeting potential sources of fall likelihood unrelated to physical function.
Supplemental Material
Supplemental Material - Examining the Role of Physical Function on Future Fall Likelihood in Older Adults With a Fear of Falling, With and Without Activity Restriction
Supplemental Material for Examining the Role of Physical Function on Future Fall Likelihood in Older Adults With a Fear of Falling, With and Without Activity Restriction by Alexander J. Garbin, PT, DPT, PhD, and Beth E. Fisher, PT, PhD, FAPTA in Journal of Aging and Health
Footnotes
Author note
The author Alexander J. Garbin changed institutions from the University of Southern California to the Veterans Affairs Eastern Colorado Geriatric Research, Education, and Clinical Center, Veterans Affairs Eastern Colorado Health Care System and University of Colorado since this work has been completed. The data that support the findings of this study are openly available in the National Health and Aging Trends Study at https://www.nhats.org/researcher. Data from the BLSA can be accessed pending approval of a pre-analysis plan ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This work contains data collected from the National Institute of Aging sponsored NHATS (grant number NIA U01AG32947) and the Baltimore Longitudinal Study of Aging.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.