
Abstract
Objectives
In Germany, roughly 8.3 million people are in need of care, but only one-third of them receive state care benefits. The study investigates whether the individual network of a care-seeking person, as well as its resources, interact with health status on the likelihood of accessing formal care services.
Methods
German data from the Survey of Health, Ageing and Retirement in Europe (SHARE) from 2015 were used in several Firth logistic regressions with interaction terms.
Results
Health limitations are a significant predictor for the probability of receiving formal care benefits. As moderating factors, caregivers from the immediate family as well as caregivers with lower levels of education tend to contribute to an increase in this probability.
Discussion
Findings are based on a limited data set and indicate the importance of further research in this area to examine the mechanisms of access to formal care more precisely.
In view of aging societies and the resulting normality of needing care at an older age, the necessity of care provision for those who require a considerable amount of assistance with daily tasks either permanently or over a prolonged period of time continues to increase. At the same time, both the rise in women’s employment rates and changes in private living arrangements with declining family sizes and an increase in single households lead to a lack of private caregivers. Availability and access to public care services is thus becoming increasingly important in most OECD societies. In this context, the growing demand of long-term care can be met in different ways, and depends on societies’ social, moral and ethical norms, government policy, and other country-specific circumstances such as economic conditions, the tax regime, and labor market structures (Colombo et al., 2011; Ngai & Pissarides, 2009; Wissenschaftliche Dienste des Deutschen Bundestages, 2020). Among European countries alone, the type and extent of social benefits vary considerably: From a mainly familial accountability, in particular in southern and southeastern European countries, to the concept of collective—often state—responsibility, as is the case especially in northern European and Scandinavian countries (Colombo et al., 2011; Wissenschaftliche Dienste des Deutschen Bundestages, 2020).
All of these models of care provision can produce, reproduce, and perpetuate social inequality—both for those who provide care (professionally or privately) 1 and for those who rely on care. Social inequality can be understood as a socially conditioned and structurally embedded inequality of individual opportunities to live and act in order to satisfy generally accepted life goals in a society (Hradil, 1987; Huinink & Schröder, 2008). 2 It is displayed through inequality characteristics such as education, income, and social connections. With regard to people in need of care, social inequality describes unequal access to care services based on these characteristics, which subsequently hinders a dignified life with social participation. In fact, the need for care itself can be regarded as a characteristic of inequality; factors such as income, occupation, and social origin entail certain living conditions and particular lifestyles that result in a (pre-)determined state of health.
Whereas social inequality with regard to gender, education, income, and determinants of health and disease is a popular subject and highly discussed all over the world, less academic interest has been shown toward social inequalities affecting the elderly in need of care. This is particularly true for the German context. Germany can be considered as an example for the majority of (particularly central) European countries in which state care services are available, but direct relatives also have an obligation to support their elderly family members (Haberkern & Szydlik, 2008). Basic and primary care of relatives in need of care is chiefly to be provided by the family, yet the state care insurance system assumes joint responsibility. If the family cannot ensure proper care, the social welfare system provides various care benefits to those officially recognized as in need of care. In Germany, these include financial, material, and service-related benefits, which are granted on application. 3
More than 8 million people in Germany are in need of care. However, official care statistics only represent individuals who have been officially recognized as in need of care, showing that 2.9 million people receive benefits in accordance with the German Social Security Code (SGB XI) (Statistisches Bundesamt, 2017). The majority of them (2.08 million) were cared for at home with over half of those (1.38 million) by relatives alone (see Figure 1, left, for a breakdown of cases). In contrast, the number of individuals in need of care who are not officially recognized as such was estimated at 5.4 million in 2011 (see Figure 1, right). These individuals did not receive any benefits from long-term care insurance; rather, roughly 3.26 million of them received assistance exclusively through informal care, and 2.16 million received neither government-sponsored care nor informal assistance in 2006 according to the OECD (Geyer & Schulz, 2014). Overview of the number of individuals in need of care in Germany and their care arrangements.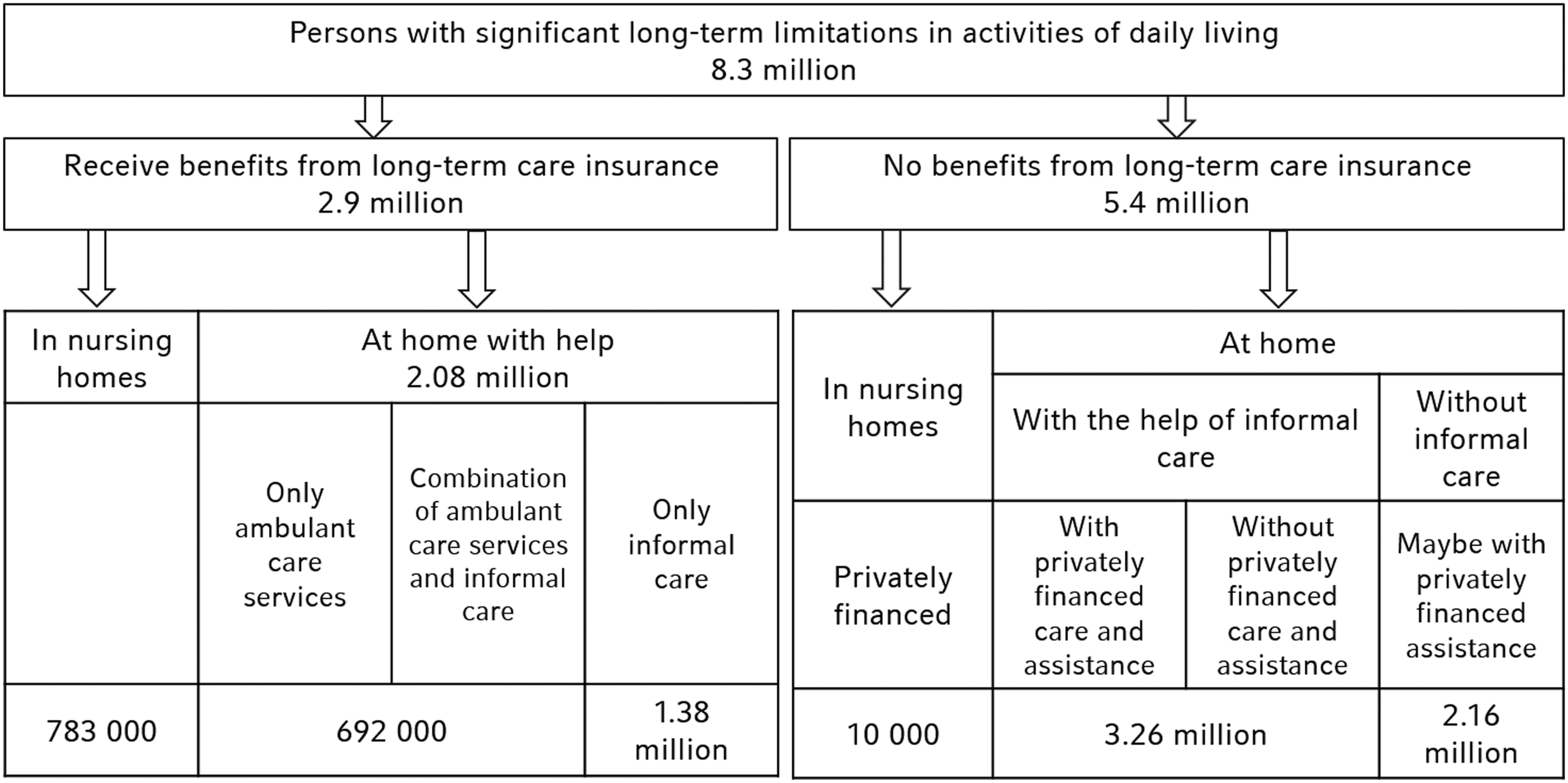
Given these numbers, one might ask how those in need of care who receive long-term care insurance benefits differ from those who do not receive benefits. This study investigates this question not only with regard to the characteristics of those in need of care, but with special regard to their network capital.
State of Research
The majority of existing research dealing with the relationship between the need for care, care arrangements, and care services originates from the field of gerontology. The initial focus has been on which factors influence the use of (formal) care services (Betini et al., 2017; Borrayo et al., 2002; Chappell & Blandford, 1991; Crets, 1996; Kempen & Suurmeijer, 1991; Logan & Spitze, 1994; Steinbeisser et al., 2018; Tennstedt et al., 1990). These studies consistently conclude that “need factors”—meaning the actual need for care—are the most important predictors for the use of care services. However, demographic and socio-economic characteristics (e.g., age, education, and income) also have a positive effect not only on the actual use of formal services (Geerlings et al., 2005; Paraponaris et al., 2012), but also on the knowledge of them (Ward et al., 1984). Women are more likely to use formal care services than men (Alkema et al., 2006; Steinbeisser et al., 2018).
The extent to which an individual’s network impacts the use of formal care services has also been investigated in previous research. Results show that a lack of informal care and weak family networks increase the likelihood of accessing formal care services (Chappell & Blandford, 1991; Chou et al., 2015; Crets, 1996; Kempen & Suurmeijer, 1991; Lee & Penning, 2018; Logan & Spitze, 1994; Tennstedt et al., 1990). Furthermore, children decrease the likelihood of using formal services, while friends as caregivers increase this likelihood (Logan & Spitze, 1994; Weaver & Roberto, 2017). The same is true for knowledge of care services to be applied for (Ward et al., 1984). However, studies on the influence of the educational attributes of network capital on potential care-seeking individuals are scarce. Pot et al. (2001) investigated the influence of the characteristics of caregivers on the institutionalization of persons with dementia, finding that these persons are more likely to be institutionalized if the caregiver is more highly educated.
Most research to date has examined either the degree of care dependency or the network composition as factors affecting the utilization of formal care services. Studies that considered both aspects did not include a possible interaction between care dependency, network (capital), and care arrangement. Moreover, thus far hardly any study has addressed the possibility that caregiver characteristics—specifically, their knowledge capital—might have an impact on access to formal care services. In addition, most research in this area stems from the United States and Scandinavia; for Germany, access to care has barely been examined. The goal of this paper is therefore to uncover to what extent the factors of need for care, network capital, and education of network capital influence the receipt of state care benefits in Germany.
Theoretical Background and Hypotheses
In mature industrial nations such as Germany, where social structures are shaped by the rule of law and the welfare state, access to formal care services are based on a concept of equality. Each individual is inherently assumed to have a basic human need for care over the course of their lifetime, and it is understood that this requirement varies with demographic and socio-economic circumstances (Hanratty et al., 2007). Grant of formal care services should therefore be independent from socio-economic factors (such as income, wealth, or education) and social factors (such as having a family or being part of a network), but only related to the individual’s degree of need. Therefore, the first hypothesis examined in this research paper is:
Hypothesis 1: With increasing health impairments, the probability of receiving state care services increases as well.
Interaction of Health Status and Caregiver Network Position
An important possible aid in the access to formal care is the individual’s network. Granovetter (1973) states in his theory of the “strength of weak ties” that contacts in an individual’s outer network are a valuable source of information not provided from the inner network. Interpersonal ties are characterized by the amount of shared time, emotional intensity, and reciprocal services (Granovetter, 1973), resulting in ties belonging to the inner network to be stronger than those belonging to the outer network. It can therefore be assumed that close networks operate in more similar ways and contain more contacts with shared knowledge and experience in comparison to members of the wider network, whose perspectives are usually more divers. These diverse perspectives refer to political, moral, and emotional attitudes, and likely include the view on whether care should be provided by family or (at least supported by) the state. Close family members such as partners or children are therefore likely to have knowledge comparable to that of the individual in need of care. Contacts from the wider network such as friends or neighbors operate in their own close contexts, which contain and negotiate different content.
Coleman’s theory of social capital (1988) describes a person’s social capital as a resource of action based on reciprocity norms, revealing social capital to be a relationship characteristic rather than an individual. The more intense a social tie (i.e., the more reciprocal actions have already taken place, or the more consequential these actions taken were), the stronger the reciprocal norm functions. It can be assumed that more frequent and intense exchanges occur with a partner and especially one’s own children than with friends, acquaintances, or neighbors. More distant network members will therefore be less willing to take on unpaid, intensive care tasks for a person in need of care, while immediate relatives are less likely to expect compensation for their care work.
As a consequence, and according to both Granovetter and Coleman’s theories, the caregiver’s network position as the social capital of a person in need of care acts as an accelerator or decelerator of access to state care services (see Figure 2). The wider network should then be able to build a bridge to formal care services more quickly than the close network due to different knowledge resources and lower sense of commitment:
Hypothesis 2: Depending on the degree of need for care, the probability of receiving long-term care insurance benefits is lower for individuals with a caregiver in their close family circle than for those with a caregiver outside of the family circle.
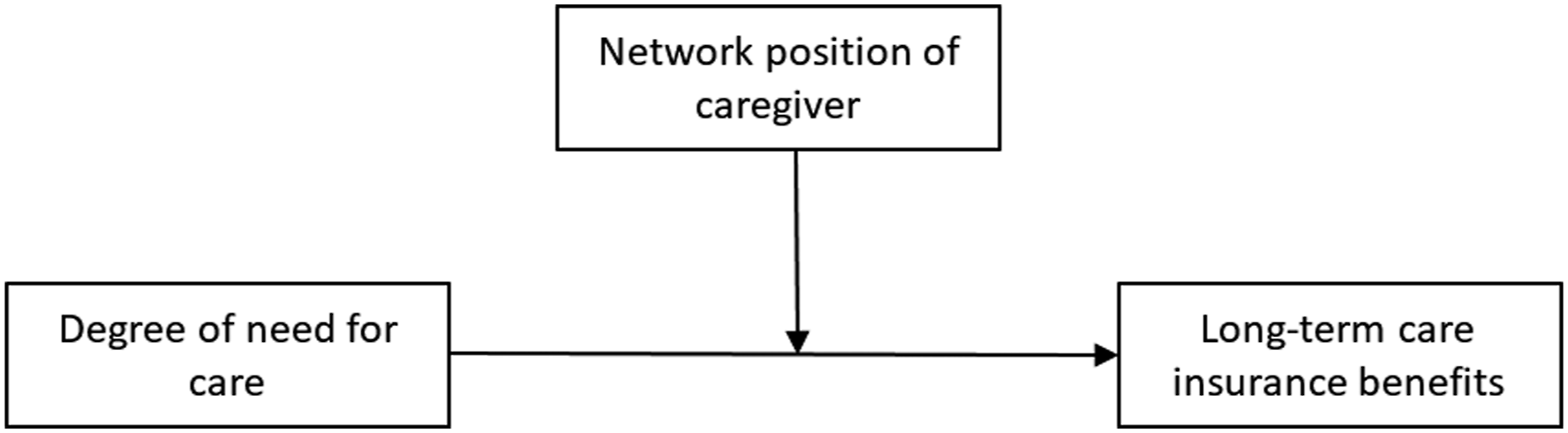
Visualization of the assumed interaction effect of the caregiver’s network position on the relationship between the need for care and receipt of care services.
Interaction of Health Status and Caregiver’s Educational Attainment
Not only differences in the type of content, but also in the amount and depth of knowledge between the individual in need of care and their caregiver can have important impact on the correlation between health status and formal care receive. This knowledge of the caregiver, based on his/her formal education and socializing structures, is known by the sociological term “cultural capital”.
According to Bourdieu (1983), cultural capital is one of three forms of capital a person can hold. In addition to economic capital, which can be directly converted into currency or property, as well as social capital (see above), Bourdieu introduces cultural capital as a term for the intertwined nature of an individual’s educational success and educational opportunities (Bourdieu, 1983). Cultural capital can exist in three forms: (1) internalized, as a permanent disposition of the organism towards the environment, (2) objectified, as cultural goods (e.g., books, encyclopedias, paintings, and instruments), and (3) institutionalized, in the form of educational degrees, qualifications, or certificates (Bourdieu, 1983).
Education implies the internalization of educational effort, which can also take place unconsciously and is passed on, for example, through social inheritance. Both the time spent actively learning and the adoption of family cultural capital during adolescence can be described as the “duration of educational acquisition”, which in turn can be transformed into educational attainment (Bourdieu, 1983). Accordingly, high incorporated cultural capital often manifests itself in high educational qualifications as its institutionalized form. The educational attainment of a caregiver can thus be used as a proxy for their cultural capital.
It can be assumed that well-educated individuals are less willing to provide care for someone in their network than those with lower educational attainment, given their respective career options (Blaumeiser et al., 2001).
In addition, the access to formal care services in Germany is strongly related to the knowledge of and skills with administrative processes (Bauer & Büscher, 2008; Behrens, 2008). Not only is it necessary to know of the possibility of applying for a service, but also to know how to access and submit the application. In addition to the application itself, a detailed documentation of daily physical or cognitive limitations may need to be provided. The individual in need of care is then assessed by an expert from the health insurance fund to determine the degree of need for care. In case of rejection, an appeal can be filed, which is a similarly highly formalized process and bound by relatively short deadlines. If the application is persistently rejected, the applicant (or his or her caregiver) may still take legal action before the social court. As the entire procedure is easier to manage with a basic knowledge of the administrative processes and an understanding of the requirements and documents to be provided, the assumption is plausible that those with higher education are more likely to submit an application and be successful. This is particularly true for the knowledge of the caregiver, who acts as an intermediary between the individual in need of care and the state (Figure 3). Visualization of the assumed interaction effect of the caregiver’s educational level on the relationship between the need for care and receipt of care services.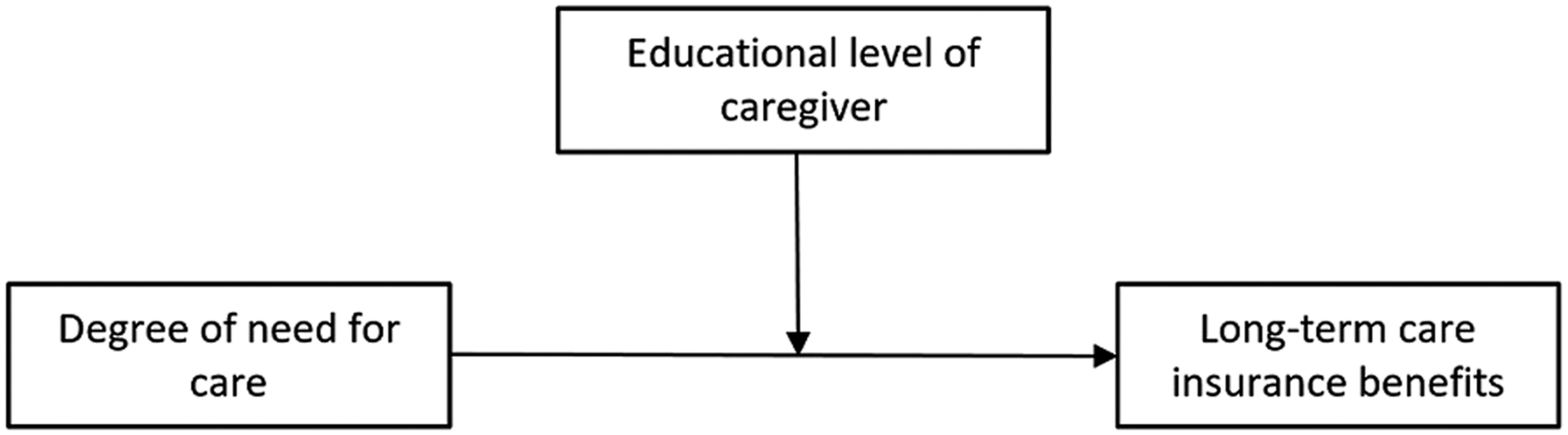
The caregiver’s educational attainment therefore also functions as a resource that the person in need of care can benefit from. As the caregiver’s education is inextricably linked to the caregiver him-/herself, their cultural capital is transformed into the social capital of the person in need of care. In order to keep the mechanisms distinct, henceforth the only terms used will be the caregiver’s network position and the caregiver’s level of education, both of which represent the social capital of the person in need of care.
4
Hypothesis 3: Depending on the degree of need for care, the probability of receiving financial benefits from long-term care insurance is greater for those with a highly educated caregiver than for those whose caregiver has lower educational attainment.
Data and Method
Data
Data from the Survey of Health, Ageing and Retirement of Europe (SHARE) are used for the following analyses. 5 SHARE is a multidisciplinary, cross-national panel database of micro data on health, socio-economic status, and social and family networks of individuals aged 50 and older (SHARE-ERIC, 2020). The panel began in 2004 (wave 1) with 11 European countries and has since been conducted biennially. Currently, all 26 continental EU member states as well as Switzerland and Israel are part of the SHARE project (Bergmann et al., 2019). The SHARE target population consists of all individuals aged 50 years and over at the time of sampling with their main residence in one of the respective SHARE countries. Detailed information on the target population, sampling design, and data collection concept can be found in Supplemental Appendix A.
For regular SHARE interviews, two types of questionnaires can be distinguished: The baseline questionnaire for respondents who participate in a SHARE interview for the first time, and the longitudinal questionnaire for respondents who previously participated. The regular question modules relate to the areas of health and related limitations, employment and income (finances), network and support, and activities and (life) expectations. Basic demographic information (e.g., marital status, country of birth, education) as well as some information regarding the parents and (ex-)spouses are also posed in each wave. A “coverscreen” module at the beginning of each interview collects basic demographic information about each individual currently living in the household. This makes it possible to provide a partner identifier as well as a couple identifier for each wave (even if the partner has never participated in the survey).
The present study is based on German data from wave 6 (2015 survey), which is the only dataset that contains all the data required for this study. Data from previous waves were additionally used to acquire baseline data. 6 The initial sample in wave 6 for Germany consists of 4412 individuals. Observations with missing values for dependent and/or independent variables are excluded from this analysis. Missing value analysis reveals that non-response is a problem only in the case of household income and assets. Both were collected from only one household participant and were imputed to the partner in the data preparation process when possible. Missing values due to non-response are consequently doubled. A total of 241 (household income) and 847 (assets) observations have missing values, and were thereby excluded from the analysis sample. Further limitations in the data and resulting sample restrictions are presented in the sections on variables and analysis below. An overview of missing values and the reduction of case numbers can be found in Supplemental Appendix E.
Variables
Coding Information for All Included Variables.
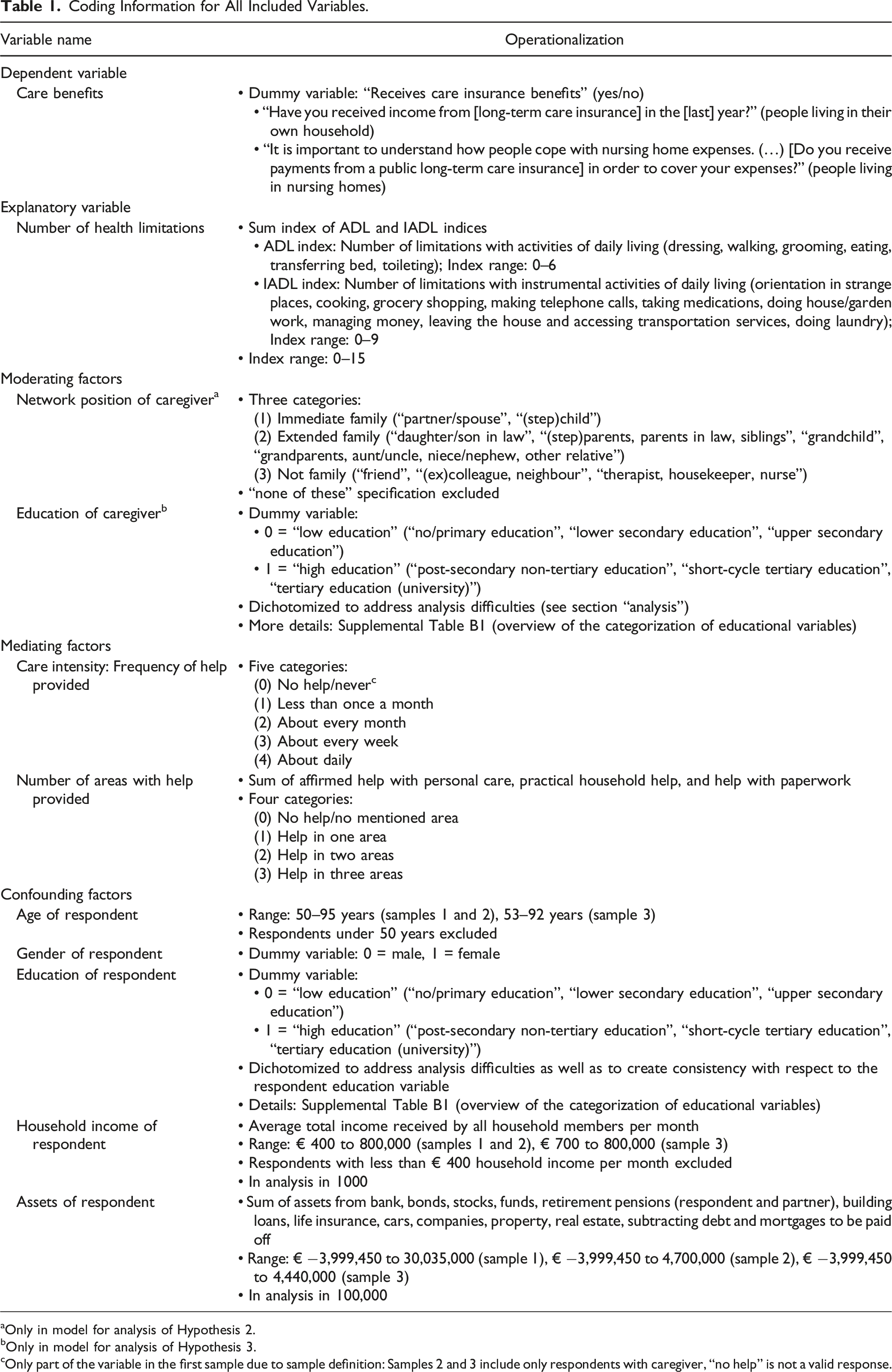
aOnly in model for analysis of Hypothesis 2.
bOnly in model for analysis of Hypothesis 3.
cOnly part of the variable in the first sample due to sample definition: Samples 2 and 3 include only respondents with caregiver, “no help” is not a valid response.
Dependent Variable
The dependent variable in all analyses is care benefits, which provides information on whether the respondent receives financial payments from state-funded long-term care insurance. This question is included as one of several income sources of the respondents in the prior year. Respondents living in a nursing home are asked with which income sources they cover their nursing home expenses, including the valid response “public long-term care service”. 7
Independent Variable
The main independent variable in all analyses is the number of health limitations. It is a sum index of the ADL (“Activities of Daily Living”) index and the IADL (“Instrumental Activities of Daily Living”) index, which are both included in the SHARE data. Both indices are adequate and often-used measures to reflect individual constraints. They are also collected as proxies for the health status evaluated throughout the care application procedure (Medizinischer Dienst des Spitzenverbandes Bund der Krankenkassen e.V. (MDS), 2016).
The ADL index (Katz et al., 1963) describes the number of limitations to activities in daily life, illustrating difficulties with everyday self-care activities such as dressing, walking, grooming, eating, getting in and out of bed, and using the toilet—all fundamental activities for maintaining independence. The IADL index (Lawton & Brody, 1969) describes the number of limitations with instrumental activities in daily live, such as housekeeping, food preparation, the ability to handle finances, and shopping. The modified versions of the ADL and the IADL indices used in the SHARE questionnaire include six and nine activities, respectively (see Table 1) (Steel et al., 2003). Respondents are asked if they have any difficulties with each one of these activities that they expect to last longer than 3 months. The indices sum up all affirmative answers, resulting in a score ranging from 0 to 6 (ADL) and from 0 to 9 (IADL). The higher the respective index, the more difficulties with the respective activities and the lower the mobility and the autonomy of the respondent (Mehrbrodt et al., 2019).
Both index variables are combined into one index variable sum of health limitations by adding the respective values, with a range from 0 (no limitations at all) to 15 (many limitations). 8
Moderating Factor 1: Network Position of the Caregiver
Possible caregivers were reported via the questions if anyone living inside or outside the household regularly helped the respondent with personal care, household tasks, or paperwork. If the answer was “yes”, respondents were asked to report who that was (resulting in 28 categories created by SHARE). In total, up to seven caregivers could be named from inside and outside the household, respectively. A maximum of two caregivers from within the household and three caregivers from outside the household were named in the data.
To test the presumed impact of a caregiver’s network position on the association between health limitations of the respondent and receiving formal care services, the sample was restricted to individuals with only one caregiver. SHARE caregiver categories were first grouped into 10 categories of the variable caregiver in terms of equal network proximity to the respondent, and finally (due to analytical challenges, see section “Analysis” below) categorized more broadly into the three categories: “immediate family”, “extended family”, and “not family” (Table 1 includes the 10 preliminary as well as the three final categories).
Moderating Factor 2: Education of the Caregiver
In SHARE, except for the respondent’s education, education level was only collected for respondents’ partners and children. The partner’s educational information is furthermore only available if the partner lives in the same household as the respondent and has completed his or her own questionnaire (and is thus in turn a respondent). When first entering the SHARE panel and completing the baseline questionnaire, respondents were asked for their highest obtained school degree and any vocational and/or higher education degrees. Respondents could indicate several vocational or higher education degrees, from which the highest was selected and coded accordingly. If the partner did not want or could not participate, the respondent was asked about the number of years their partner spent in education. The number of years the respondent’s partner spent in education are collected as his or her sum of years in full-time education and vocational training, which are then converted into the corresponding category (see Supplemental Table B1). Both questions (i.e., respondent’s own education and partner’s years in education) are only posed in the baseline questionnaire when the respondent enters the panel. This data was therefore imputed to subsequent waves of participation. If the partner lives outside of the household, no partner education data are available. The new variable education of respondent was generated as a combination of school education and further education, and follows the construction of the International Standard Classification of Education (ISCED) (Stuck et al., 2019). 9 Resulting categories are listed in Table 1.
In contrast to the partner‘s educational level, children’s education is asked only up to a certain age in each survey wave. Full educational information is recorded in the first interview. In subsequent waves, only changes in children’s schooling (up to age 22) or further education (up to age 32) are reported. For children’s education, the ISCED variables already coded by SHARE are used. If no education information is provided due to no change, children’s education information is imputed over the waves. Given changes in the collection of the education variables by SHARE as well as the coding of the ISCED 10 between waves 4 and 5, both types of coding had to be merged into the new variable “child education”. For an overview of the original education categories, the associated ISCED indices, and the coding of the new education variables, see Supplemental Table B1.
In a final step, the education of the caregiver was summarized, whereas the caregiver was either the partner or one of the children. The education information was entered into the new variable education of caregiver, which was then dichotomized in a last step to address the mentioned analysis difficulties. The final variable consists of the two categories: “low education” and “high education” (details in Table 1).
Mediating Factors
An individual’s need for care affects both the frequency and the extent of the required care tasks. Whereas lesser limitations might require support only once a week with minor tasks (e.g., shopping), more severe limitations might require help with more extensive tasks daily (e.g., washing and dressing). The extent of care and the frequency of care in turn affect the likelihood of receiving formal care benefits. The higher both are, the more the applicant is classified as being dependent and thus to be granted formal care benefits. Additionally, as caregiving responsibilities increase, the caregiver is also likely to support the application for formal caregiving services. This is initially independent of the caregiver’s network position, since care intensity simply reflects the variation of care effort with care dependency and its impact on the probability of formal care service use. Thus, care intensity (i.e., the frequency of care provided and the number of care tasks provided by the caregiver) represents a mediating role in the analysis model. The corresponding variables act as mediating factors between the need for care and the receipt of care benefits. 11
Confounding Factors
Control variables in all analyses are respondent gender, age, education level, and financial status (household income and assets). All of these variables are possible confounding factors that are likely to influence both the degree of need for care and the receipt of care services.
Gender and age are so-called “predisposing factors” according to the Andersen-Newman model (Andersen & Newman, 1973): These factors are understood as a genetically determined susceptibility to the development of a poor health status (e.g., older age goes hand in hand with more severe physical complaints, and men are more inclined toward frailty in old age than women). At the same time, both characteristics could have an effect on the receipt of care benefits if and when men and women or younger and older applicants are treated differently when applying for care. For example, since women outlive their husbands (Laenderdaten.info, 2019), they are more likely to have to request benefits. And based on gender theories (Garfinkel, 1967; West & Zimmerman, 1987), applying for care services is likely perceived by men as undermining their masculine role which probably reduces their willingness to apply for formal care. With age, however, the likelihood of illness and restricted mobility and mental capacity increases overall, which makes an age-dependent treatment of care applications independent of the actual degree of impairment plausible. Combined with the assumption that the health state of older applicants deteriorate faster than that of younger applicants, may result in precautionary approval of an application for care benefits.
Education level and financial status are also (according to previous studies using the Andersen-Newman model) predisposing, or enabling, factors. As enabling factors, they provide access to care services (Andersen & Newman, 1973). As predisposing factors, they make the use of care services more likely (Andersen & Newman, 1973). On the one hand, health status varies with socio-economic status (a.o., Brunello, et al., 2013; Schöllgen et al., 2010). Individuals with a low socio-economic status have a higher risk of falling ill due to less knowledge of healthy lifestyles as well as the financial means to live by them. They are also less likely to attend preventative check-ups or receive necessary treatments, and are more likely to work in conditions that trigger (chronic) diseases (Behrens, 2008). These aspects contribute to a higher likelihood of being in need of care earlier or to a greater extent than those with a higher socio-economic status. On the other side, low income levels could increase receptiveness to applying for state-funded care benefits, whereas higher income provides more differentiated options. While those with higher economic status do not necessarily rely on financial state support but might be able to afford private care services instead, those with low income and/or assets lack this possibility. Less socio-economic resources thus increase the probability to apply for long-term care in case of need (Unger et al., 2015). Higher educational level, again, enables applicants to better understand the application processes, whereas a lack of formal education may leave individuals in need of care behind (see section “Theoretical background”).
Analysis
According to the postulated three hypotheses, this analysis of SHARE data includes three steps. The first is to examine the basic relationship between the need for care and the receipt of care benefits, taking into account both confounding and mediating factors. To analyze whether a caregiver makes a difference in the application or receipt of care, the base analysis sample is restricted to individuals with none or at most one caregiver. The base sample contains a total of 2604 observations.
In a second step, a possible moderating impact of the caregiver’s network position is investigated. To test Hypothesis 2 (i.e., the probability of receiving formal long-term care correlates positively with the social network distance between the person in need of care and their caregiver, both depending on the degree of the respondent’s need for care), the base sample is restricted to respondents with one caregiver only. The number of cases in this second sample is thus drastically reduced to 417 observations.
Finally, the third step examines whether the education of a caregiver from the inner network moderates the relationship between care needs and financial care benefits. In order to test Hypothesis 3 (the probability of receiving long-term care benefits correlates positively with the caregiver’s level of education, depending on the respondent’s degree of need for care) the sample is further restricted as SHARE only collects data on the education of the respondent’s partner and children. For this analysis, only respondents who indicated their partner or one of their children as caregiver are available, resulting in a third analysis sample of 203 observations.
The dependent variable in all analyses is the receipt of financial care insurance benefits. As it is a dichotomous variable, logistic regressions are used. With logistic regression, however, a problem called “separation” (Albert & Anderson, 1984) can occur, caused due to small sample sizes, rare events, or unbalanced or highly predictive risk factors. Separation is when one or more explanatory always or never occurs with the event of the dependent variable, meaning that they perfectly predict the outcome of interest. As a result, estimates of traditional maximum likelihood logistic regressions do not converge, manifesting in infinite coefficients and standard errors (Karabon, 2020; Zorn, 2005). While the problem of separation is not unknown, it is often unreported and instead attempted to be solved by modifying the model or replacing, transforming, or excluding the affected variables (Heinze, 2006; Zorn, 2005). However, none of these practices is appropriate in terms of a neat analytical approach (Heinze, 2006; Heinze & Schemper, 2002). An adequate alternative is the Firth logistic regression method (Firth, 1993), superior to other methods in terms of handling, significance, and efficiency (Heinze, 2006; Karabon, 2020; Wang, 2014). The basic idea of the Firth procedure is to introduce a bias term into the standard likelihood function that converges towards 0 as the sample size increases to infinity. The bias term therefore counteracts the small sample bias. The result is a penalized likelihood whose estimates will typically be smaller in absolute value than standard maximum likelihood estimates, as are their standard errors (Heinze & Schemper, 2002). Since the separation problem occurs with the moderating variables in the present analysis, Firth logistic regressions are used.
Another challenge of non-linear regressions is the interpretation of interaction terms. Ai and Norton (2003), as well as Mize (2019) point out that although many studies use interaction terms in logistic regressions, an adequate interpretation is often missed. The estimated coefficients of a logistic regression as a single value cannot represent the effect on the predicted probabilities, as these are not constant. Since effects can differ drastically depending on which data range the predicted probability is in (Mize, 2019), a suspected interaction effect cannot be detected in logistic regression models “simply by looking at the sign, magnitude, or statistical significance of the coefficient” (Ai & Norton, 2003, p. 129). In addition, the factors entered in logistic regression models interact by the estimation method alone, even if an interaction term is not explicitly included in the model. Thus, even without interaction, the factors depend on each other, so that the prediction of one variable depends on the level of the other variable. However, to avoid type I errors, including interaction terms are nonetheless necessary for correct estimates of interactions (Mize, 2019). Consequently, for the analysis of Hypothesis 2 and Hypothesis 3, the proposed moderating variables were included in the models as interaction terms. Results are interpreted with Average Marginal Effects (AMEs) 12 and predicted probabilities. The former estimate the extent to which a factor has the same effect on the probability of the outcome for the different groups; the latter show how outcomes differ under specific conditions (Long & Mustillo, 2018).
Results
Descriptive Results
Descriptive Results.
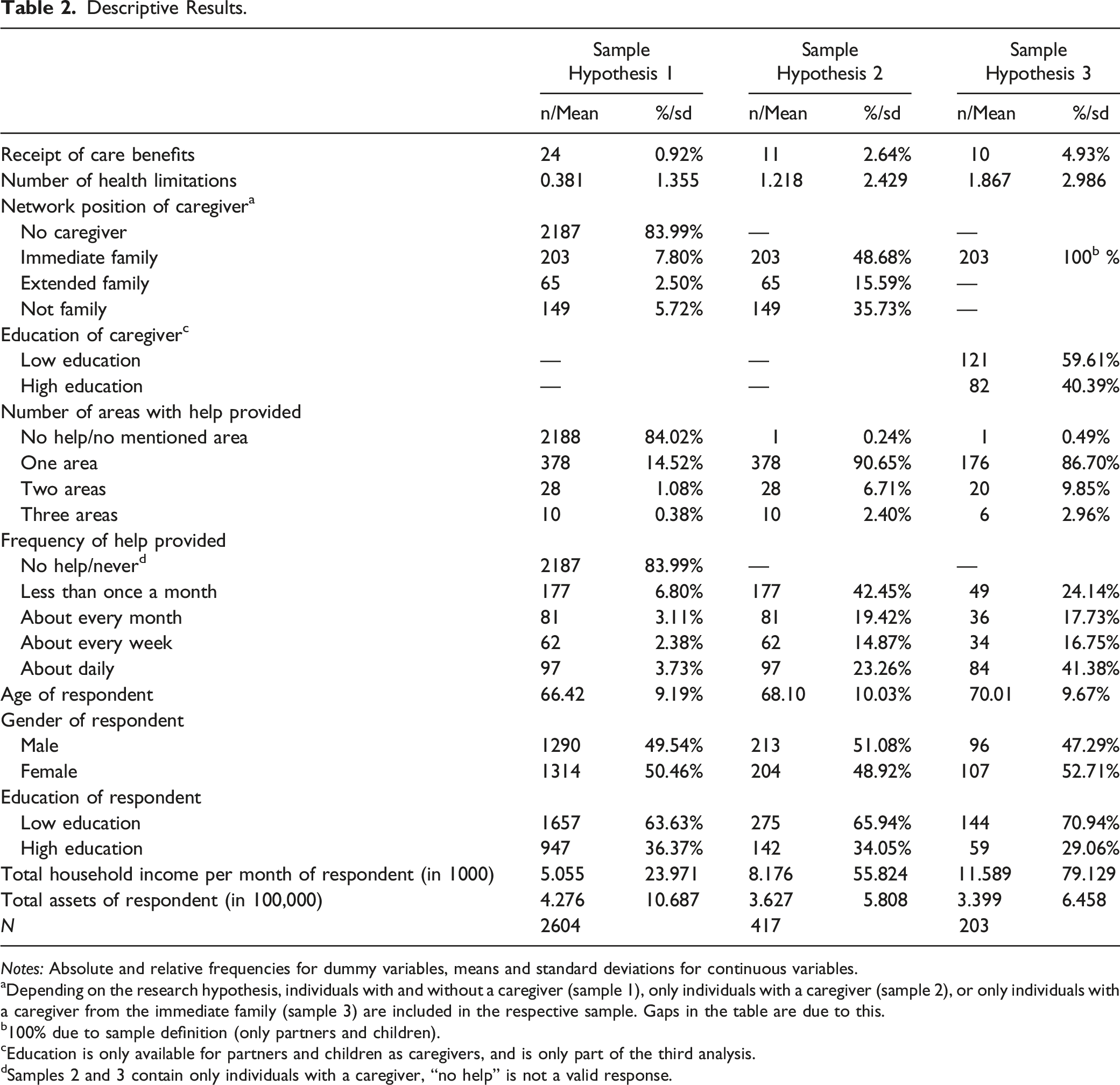
Notes: Absolute and relative frequencies for dummy variables, means and standard deviations for continuous variables.
aDepending on the research hypothesis, individuals with and without a caregiver (sample 1), only individuals with a caregiver (sample 2), or only individuals with a caregiver from the immediate family (sample 3) are included in the respective sample. Gaps in the table are due to this.
b100% due to sample definition (only partners and children).
cEducation is only available for partners and children as caregivers, and is only part of the third analysis.
dSamples 2 and 3 contain only individuals with a caregiver, “no help” is not a valid response.
The proportion of those receiving state care benefits is low in all three samples, ranging from just under 1% (total sample) to just under 5% (most restrictive sample). This seems surprisingly low given that the second and third samples only include respondents who report having a caregiver. The proportion of those suffering from at least one limitation in executing ADL or IADL 13 increases from sample 1 (with or without a caregiver, 14%), via sample 2 (with a caregiver, 34.7%), to sample 3 (with partner or child as caregiver) (not shown in Table 2). The fact that less than half of the respondents with a caregiver state that they have limitations could indicate that minor impairments are not perceived as such or are not freely disclosed. Another indication that minor health restrictions do not justify the use of state care benefits or that these are not (yet) approved is the mentioned proportion of under five percent of respondents receiving financial state care benefits even in the most restrictive sample.
On average, respondents in the total sample have 0.381 health restrictions, implying that a large share of participants did not indicate any restrictions at all. The percentage of those who stated that they do not have a caregiver and correspondingly do not receive support in any of the areas queried at any time is correspondingly high (84%). In contrast, the average number of health restrictions in the two reduced samples that only include respondents with a caregiver rises to 1.2 and 1.9, respectively. In both samples, help is provided for the most part in one task area (90.7% and 86.7%, respectively) and mainly by the immediate family (sample 2: 48.7%). While the majority of help provided to respondents with a caregiver (sample 2) is performed less than once a month (42.4%), this largest ratio shifts to daily assistance when only respondents with a partner or child as a caregiver are considered (sample 3) (41.4%). It seems that immediate family members thus provide more intensive care than more distant family members or friends, neighbors or acquaintances. Caregivers’ educational level is more or less equally distributed, with a slight tendency toward lower education (just under 60%).
Multivariate Results
Hypothesis 1
AMEs of Firth Logistic Regression Estimates of the Association Between Health Limitations and the Receipt of Care Benefits; Nested Models (Without and with Confounding and Mediating Factors, Respectively).
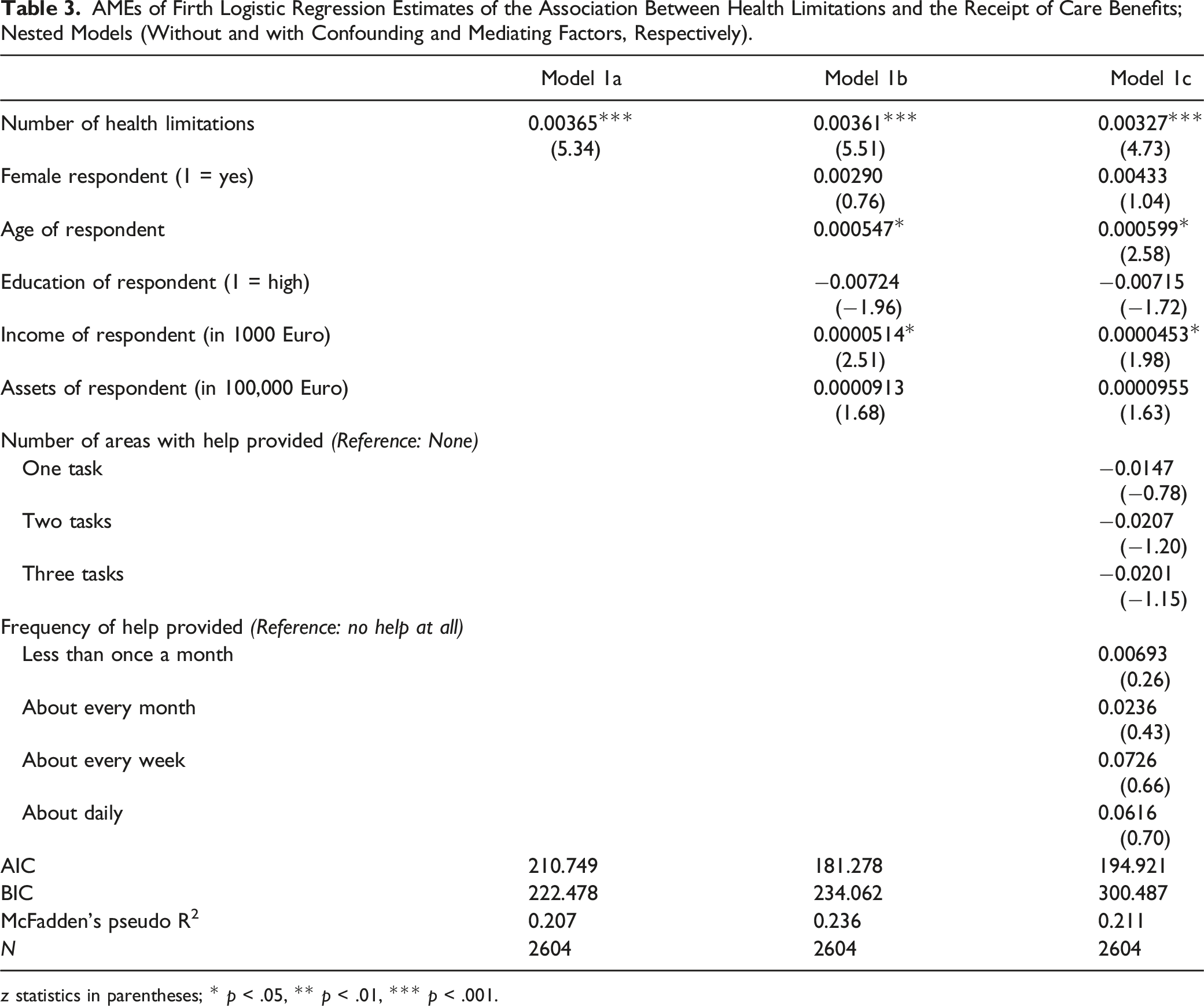
z statistics in parentheses; * p < .05, ** p < .01, *** p < .001.
The predicted probabilities of receiving care benefits range from 1.1% for an individual with only two health limitations to just over 60% for persons with extensive health limitations (15 limitations) (see Figure 4). The likelihood ratio test is highly significant, indicating that the factors included in the model are suitable predictors of the dependent variable.
14
Hypothesis 1 can thus be clearly confirmed. Predicted probability of the receipt of care benefits based on the number of health limitations. Model with confounding variables only. (N = 2604).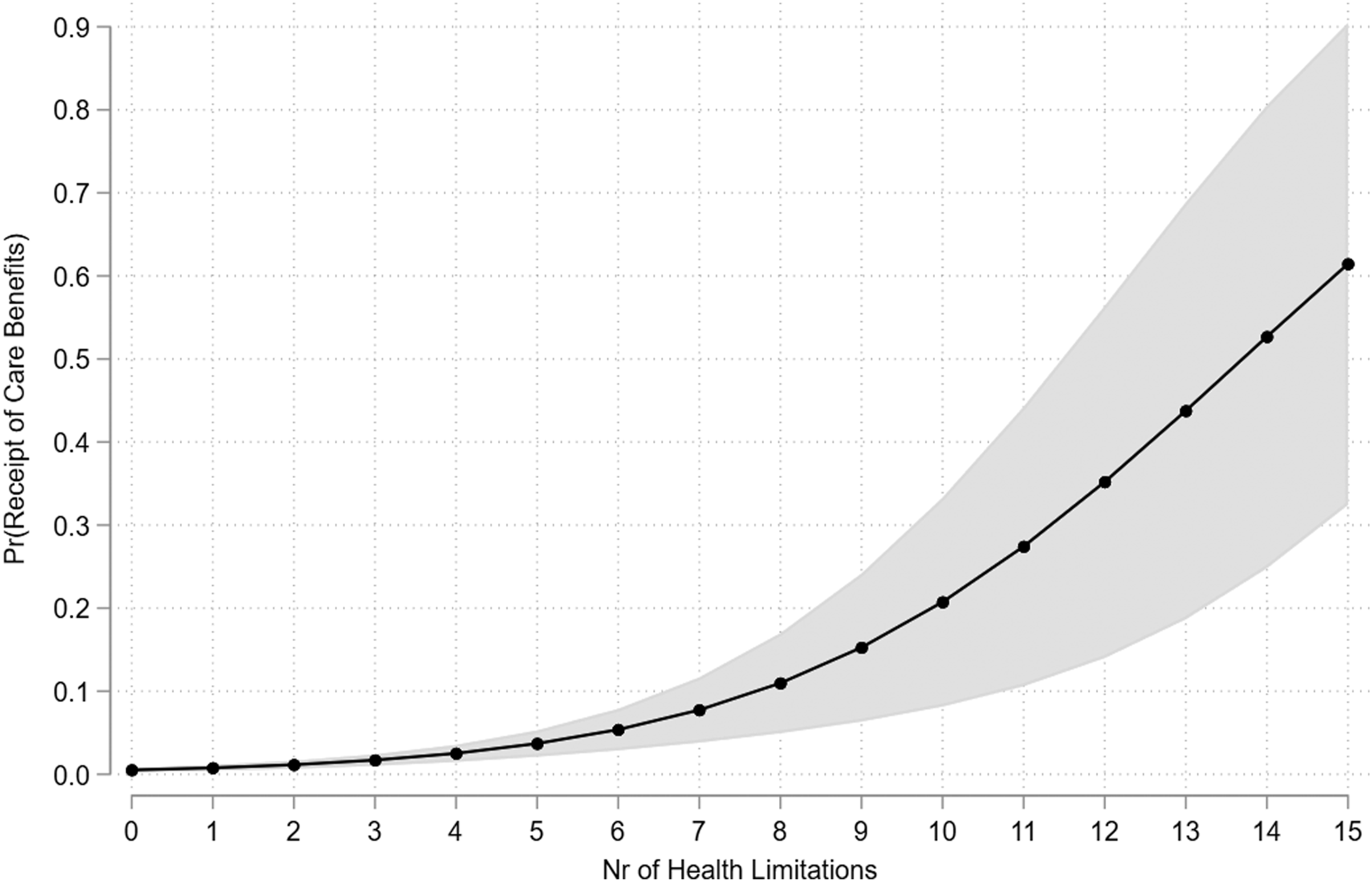
Hypothesis 2
Next, the moderating influence of the caregiver’s network position is estimated by including a corresponding interaction term. Results are illustrated in Figure 5. For interpretation, Average Marginal Effects (AMEs) and predicted probabilities are used (see explanation above). Predicted probability of the receipt of care benefits by network position of the caregiver and the number of health limitations; overall (plot 1) and group comparisons (plots 2, 3, and 4). All models with confounding variables only. (N = 417).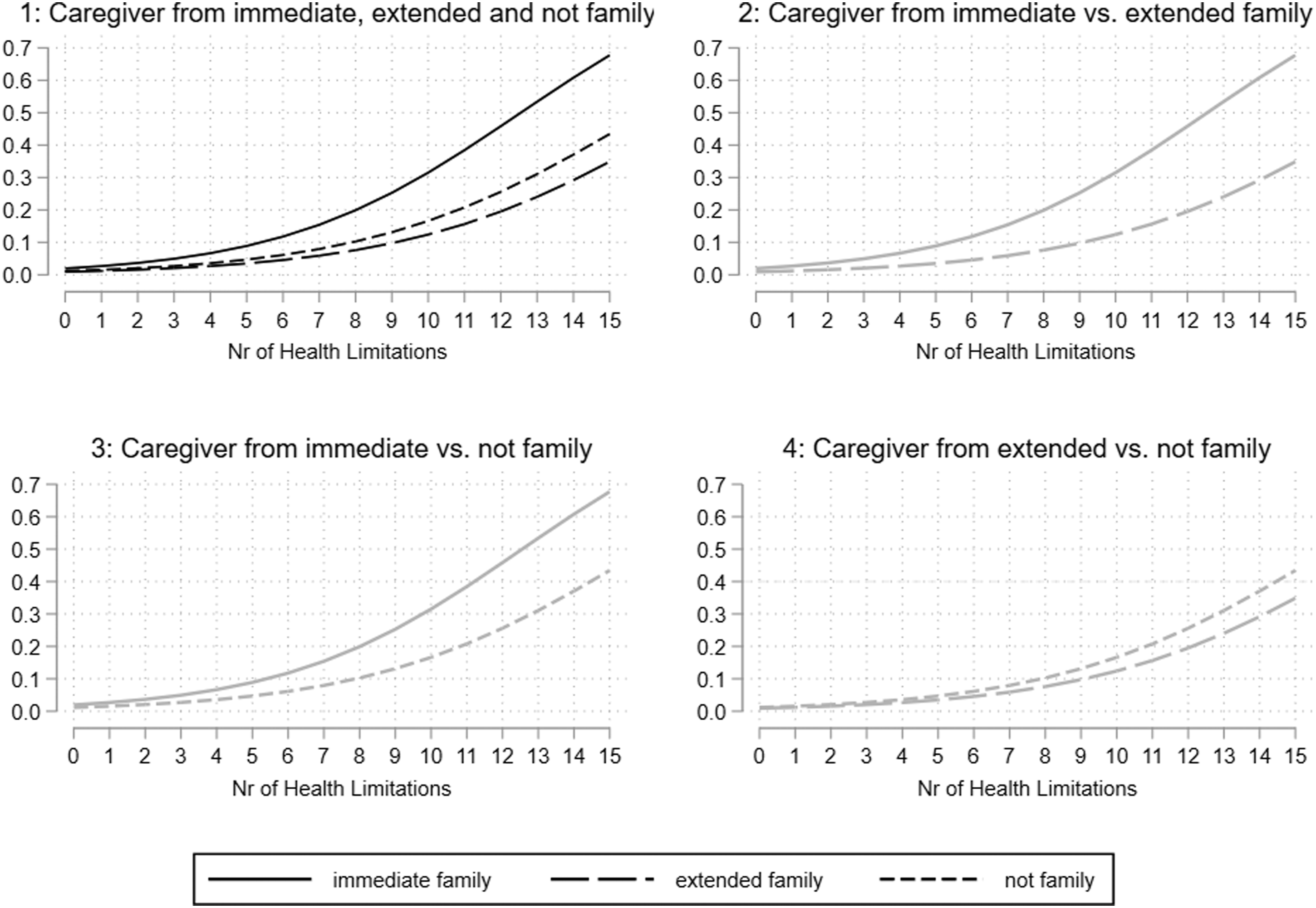
Starting with the health limitation side of the interaction effect, AMEs show that, on average, each additional health limitation significantly increases the predicted probability of receiving care benefits by 1.7 percentage points (p < .001) if the caregiver is a partner or child and by 0.5 percentage points if the caregiver is part of the extended family or (not significant). There are no significant differences in the AMEs of health limitations on the receipt of care between groups. The predicted probabilities are shown in plot 1 of Figure 5.
Adequate analysis of interaction requires to test both sides of the interaction. Thus, it should not only be considered to what extent the effect of health limitations on the probability of receiving care differs between respondents with an immediate, extended, or non-family caregiver, but also whether there are significant differences between the aforementioned groups at different levels of need for care (Mize, 2019, p. 107). The group differences in predicted probabilities are shown in plots 2 to 4 of Figure 5. Gray lines indicate non-significant and black lines significant results, demonstrating that none of the differences between types of caregivers is significant (see Supplemental Table C2 for an overview of predicted probabilities, AMEs and differences). However, Figure 5 shows that the increase is steeper for caregivers originating from the immediate family (from 4.9% with three limitations to 45.8% with 12 limitations) than for the other types of caregivers, whose increases are very similar (from about 2% to a maximum of 25% on the same values of health limitations). Predicted probability of the receipt of care benefits by educational level of the caregiver and the number of health limitations; interaction effect between caregiver’s education and number of health limitations. Model with confounding variables only. (N = 203).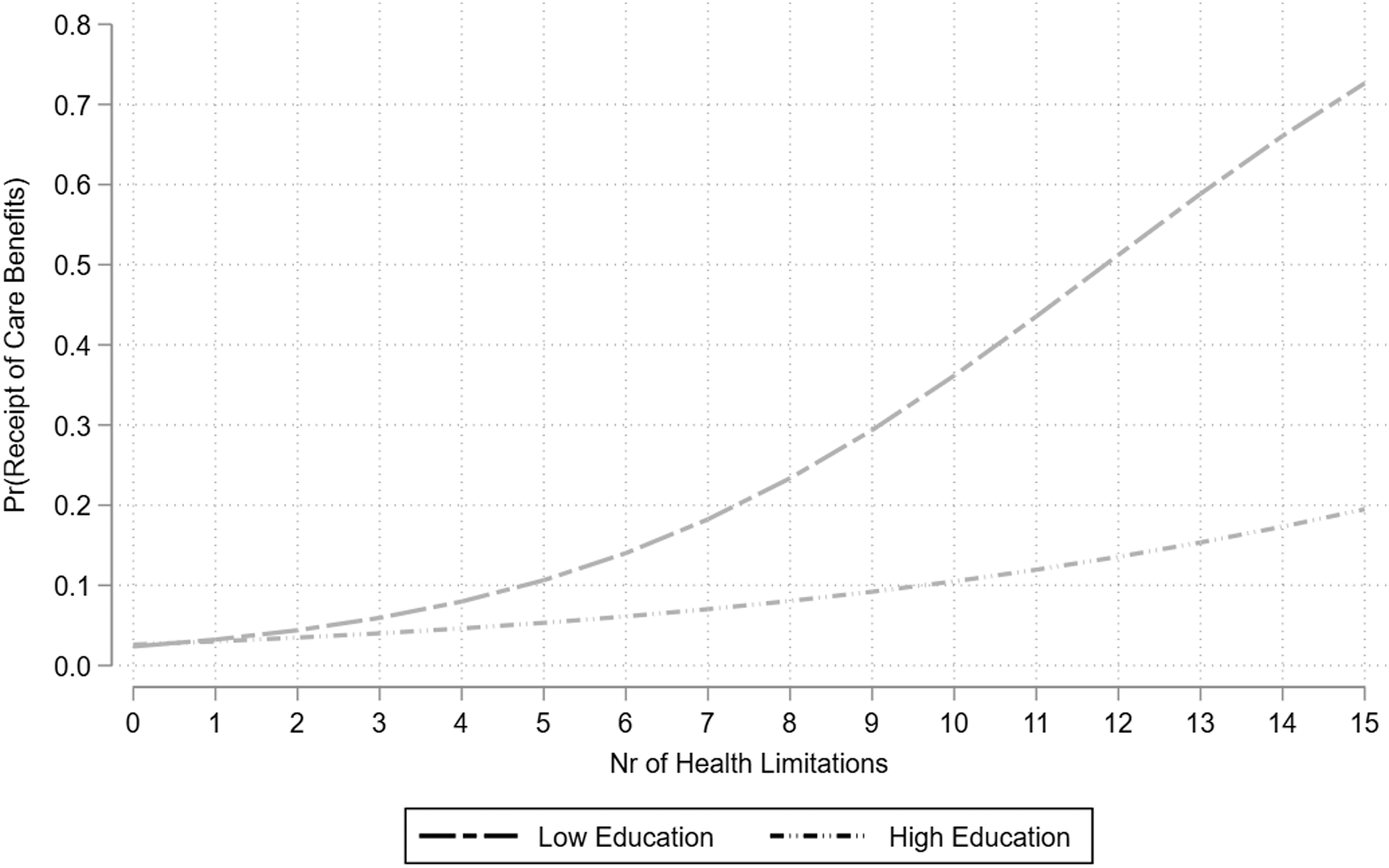
Hypothesis 2 can therefore not be confirmed. Although differences in the influence of health restrictions in the interaction with the caregiver’s network position are evident, these differences are not significant. Moreover, the results contradict the hypothesized assumption that with greater network distance, the bridge to formal care services is built more quickly. One argument for this would be that immediate family members provide more intensive care, which also leads to a greater likelihood of seeking out support through state-funded benefits. However, the inclusion of the mediating factors for care volume and care frequency to control for this circumstance weaken the effects, while neither direction nor relationship are fundamentally altered (see Supplemental Figure D1.1 and Supplemental Table D1.3). It seems more plausible that the effort required to apply for care and the associated formalities is more likely to be made by immediate family members than by more distant network members, which is still in line with the reciprocity hypothesis.
Hypothesis 3
Finally, the moderating influence of the caregiver’s educational capital on the probability of receiving state care benefits is tested. Predicted probabilities can be seen in Figure 6.
AMEs reveal an increase of probability of receiving care by 2.2 percentage point per additional limitation in the group of lower educated caregivers (p < .001) and of 0.5 percentage point in the group of higher educated caregivers (not significant).The gap between both groups is only significant at the 10% level (p = .067).
No significant gap in terms of the caregiver’s educational capital on the likelihood of receiving care is found for any group differences at the different levels of need for care (Figure 6). Although the lines spread out considerably as the need for care becomes higher (while both start at about 5% at three health limitations, the probability increases only slightly to 13.5% at 12 health limitations and a highly educated caregiver, but to a notably 51% at the same health level and a lower educated caregiver), the gray shading indicates the lack of significance in the group differences (see Supplemental Table C3 for all predicted probabilities).
In sum, Hypothesis 3 cannot be confirmed either. Depending on the caregiver’s educational level, differences in the development of the probability of receiving care benefits depending on health status are visible, but not significant. In addition, these results do not show the hypothesized effects: While it was assumed that highly educated informal caregivers facilitate access to state care services, this analysis demonstrates the opposite effect. Two possible reasons might account for this: First, not only is the assumption plausible that higher education corresponds with a demanding job and thus a time budget too restricted to handle the application process, but also that this discrepancy increases with increasing care requirements. Second, higher education usually corresponds with higher income and thus with the capability to finance private care—an option less available to caregivers with lower education who consequently rely on state-based care.
Model Fit and Robustness Checks
All models were tested for model fit using the information criteria AIC and BIC, as well as McFadden’s pseudo R2. According to the values (see Table 3), the inclusion of the confounding but not the mediating variables in the analyses seems plausible. See Supplemental Appendix D for a brief discussion of the values.
To ascertain whether the results of the main analyses are largely stable with the data used, various robustness checks were conducted. First, the models corresponding to hypotheses 2 and 3 were each calculated both ways, with mediating and confounding factors and without. Second, the original samples were extended through samples in which educational status of children were only estimated in cases where the educational data was obviously not up to date (in the main analyses, only educational data that could be validly assumed to be correct was included). Third, all models were calculated with the dependent variable restricted to the IADL and the ADL index, respectively, as opposed to a sum index of ADL and IADL. Neither the effects nor the significance levels of the robustness analyses differed substantially from the main analyses. Results and discussion of the robustness analyses can be seen in Supplemental Appendix D.
Discussion
The purpose of this study was to examine the association of health limitations with the likelihood of receiving state-funded long-term care benefits, taking into account possible interactions with the caregiver’s network position and educational capital. Consistent with previous studies, a significant positive effect of need for care on the probability of receiving long-term care benefits was found, which remained stable even after controlling for both confounding and mediating factors. However, the hypotheses that this effect is strengthened by, first, increasing network distance and, second, higher education of the caregiver, could not be confirmed. On the contrary, the analysis suggests that immediate family members and caregivers with lower educational levels are more likely to form a bridge to formal care services.
The potential explanation for the first result—that immediate family members push for state support more quickly as they provide more frequent and more intensive care—could not be confirmed in the analysis. Rather, it appears that family members are more willing to take on the extra effort of applying for government care than individuals from the wider network. This again points to Coleman's reciprocity hypothesis and to the fact that care circulates particularly within the family. Family members give and receive care in a cycle of general reciprocity, which need not be explicitly stated. The nature of kinship as an emotional relationship tends to produce a subjective feeling of obligation to perform care within the family (Comas-d'Argemir & Soronellas, 2019). That such norms of reciprocity exist in caregiving relationships have been shown by a number of studies (e.g., Blieszner & Hamon, 1992; Lee et al., 2003; Silverstein et al., 2007). This also points to the complexity of caregiving as the intertwining of love, work, and relationships, which is discussed especially in the area of gender studies (Rummery & Fine, 2012).
For the second result—that caregivers with lower educational levels are more likely to form a bridge to formal care services—studies have shown that caregivers with lower socio-economic backgrounds perceive family caregiving as less negotiable than caregivers with higher socio-economic backgrounds (Conlon et al., 2014; Winqvist, 1999). High levels of education may thus also lower the willingness to spend more time than necessary on family caregiving and related application processes. Muresan (2017) shows that children with higher levels of education are more likely to provide financial and emotional support to their parents than personal care. Whether higher job demands actually have a negative effect on highly educated caregivers' willingness to provide care is debatable. However, empirical evidence shows that a child's high income negatively affects their actual care engagement and instead increases the likelihood of financial transfers (Couch et al., 1999; Shuey & Hardy, 2003; Szinovacz & Davey, 2008).
Overall, the present study assumes that the application procedure for long-term care benefits can represent a barrier for the receipt of state-funded care. This may be caused by personal characteristics of the applicants and/or their caregivers, but also by official regulations intended as a means to control and shorten access to benefits (Peeters, 2020; Reibling & Wendt, 2008). Care is thus primarily revealed in the dimension of equity issues: Do those in need of care have equal access to necessary care services? Or are there (structural) barriers that make access difficult or even impossible for some, while others do not face these barriers (and/or do not experience them as a barrier) due to their socio-economic and social disposition? The lack of utilization of state care services has consequences not only for those in need of care, but also for their caregivers. Providing care requires (sometimes far-reaching) adjustments in a caregiver's private and professional life. Often, employment must be reduced or even completely terminated, which not only affects a caregiver's current income situation, but ultimately also translates into lower pension returns (Reiter, 2018). As care work is still predominantly carried out by women, gender thus acts as a determinant of social inequality. Caretaking therefore reproduces and reinforces existing social inequality structures. Studies also point to further consequences of caregiving for caregivers, including lower life satisfaction (Geyer & Schulz, 2014), physical and mental health burdens (Pinquart & Sörensen, 2003; Stratmann et al., 2021; Zwar et al., 2020), lower life expectancy (Zwar et al., 2021), and higher levels of social isolation (Hajek et al., 2021).
Furthermore, the physical and emotional exhaustion that caregiving responsibilities entail can also affect the caregiving relationship itself. The unmediated confrontation with age, illness, suffering, and death, the mismatch between physical closeness and emotional distance, and the indispensable intimacy of (physical) care are often experienced by caregivers as stressful and demoralizing (Osterbrink & Andratsch, 2015). The care relationship thus becomes charged with tension and conflict. In the worst case, helplessness and excessive demands lead to verbal, psychological, emotional, and/or physical violence, or even to the withdrawal of the caregiver from the care relationship. As a result, the individual in need of care suffers (passive or active) neglect (Braun, 2012). External structures—for example, high barriers to the access of state supportive care services—can have a reinforcing effect on this. If caregivers feel left alone with the burden of care, aggression can intensify. To avoid this, it is essential that sufficient and accessible government support services exist to provide relief for caregivers and, in turn, the caregiving relationship to protect those in need of care. Linking informal and formal care services is of central importance here. Care work is often still exclusively located as a “work of love” (Bock & Duden, 1977; Graham, 1983) in the private sphere, and continues to be negotiated in most societies as “female” work without productive economic benefits. Debates in gender studies point to the problematic character of this perspective and the reproductive nature of care work (Tronto, 1993). Care thus becomes socially relevant work that transcends private and public spheres (Daly & Lewis, 1998), making it impossible to clearly separate them from one another. Accordingly, the state is seen as an important co-player in shaping the provision of care and addressing related gender issues. For a detailed discussion of this topic see, among others, Hochschild (1995), Geissler and Pfau-Effinger (2005), Held (2006), Engster (2007), Kremer (2007), Tronto (2013), Levitsky (2014).
For the entirety of the interpretation of the results presented in the previous paragraphs it is relevant to know that there is no data set specifically designed or existing for the research question presented here. The SHARE data used for the analysis are suitable for the study thanks to its particular data structure, but it is not perfectly adapted to the research question. For example, the dependent variable only depicts the receipt of financial long-term care insurance benefits. However, possible long-term care insurance benefits also cover, among other things, outpatient care services, care benefits in kind, coverage of the costs of care aids, day and night care, as well as support services for informal caregivers. None of these options are covered by the variable surveyed here. It can therefore be assumed that the proportion of those who have been classified as in need of care via the care application procedure is higher than has been recorded here. Another limitation is the vagueness of the dependent variable in its statement logic. Not receiving (financial) long-term care benefits can imply either not having applied for care benefits or having applied but not been granted them. Thus, it was impossible to control for this aspect.
In addition, the survey of health restrictions presents another difficulty. While part of the respondents might be unwilling to disclose their inadequacies publicly, other parts might be unable to participate at all due to their particularly high need for care. Apart from this, using an unweighted sum score to represent health limitations, as was done for the ADL and IADL variables as well as for the total variable derived from them, ignores the specific consequences single limitations might have on the individual need for care and could thus be criticized. For example, individuals who cannot dress themselves or go to the toilet independently may have a different need for help than those who lack orientation in unfamiliar places, even though their number of limitations is the same.
In light of these limitations, the present study should be considered to be a preliminary and orienting study, designed to provide scientific evidence for the need to further explore the discussed problem with a more adequate and purpose-built data set. In this regard, a larger sample size, more differentiated variables (see above), further possible influencing factors (e.g., the professional sector of respondent and caregiver as a relevant source of knowledge for the application process), as well as a more comprehensive survey (e.g., including educational capital of the wider network) could be ways to examine the mechanisms of access to care more precisely. In addition, this preliminary study only takes into account care recipients with one caregiver only. In order to limit the complexity, data sets with more than one caregiver were excluded from the analysis. However, a person in need of care is often supported by several caregivers. For example, children, friends, or neighbors may help the partner of the person in need of care who provides the primary care, or several children may share care in different areas or take turns providing care. The extent to which both the size and composition of such a care network influences the use of public care services is of great importance. Future studies should take more complex caregiver networks into account in order to better understand the mechanisms involved behind the link between care needs and the receipt of formal care services.
Supplemental Material
Supplemental Material - Bridge or Barrier? The Impact of Network Capital on the Receipt of Long-Term Care Services in Germany
Supplemental Material for Bridge or Barrier? The Impact of Network Capital on the Receipt of Long-Term Care Services in Germany by Ariane Baum in Journal of Aging and Health
Footnotes
Acknowledgments
The SHARE data collection has been funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782) and by DG Employment, Social Affairs & Inclusion. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see ![]() ).
).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.